Back to Journals » Open Access Emergency Medicine » Volume 14
Predictive Performance of the NEWS‒Lactate and NEWS Towards Mortality or Need for Critical Care Among Patients with Suspicion of Sepsis in the Emergency Department: A Prospective Observational Study
Authors Dadeh AA ![]() , Kulparat M
, Kulparat M
Received 22 July 2022
Accepted for publication 11 November 2022
Published 17 November 2022 Volume 2022:14 Pages 619—631
DOI https://doi.org/10.2147/OAEM.S382752
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Hans-Christoph Pape
Ar-aishah Dadeh, Matina Kulparat
Department of Emergency Medicine, Songklanagarind Hospital, Faculty of Medicine, Prince of Songkla University, Hat Yai, Songkhla, 90110, Thailand
Correspondence: Ar-aishah Dadeh, Department of Emergency Medicine, Songklanagarind Hospital, Faculty of Medicine, Prince of Songkla University, Hat Yai, Songkhla, 90110, Thailand, Tel +6674-451705, Fax +6674-451704, Email [email protected]
Objective: We aimed to evaluate the National Early Warning Score‒Lactate (NEWS‒L) and NEWS to predict 24-hour mortality as the primary outcome. The secondary outcomes were to predict 48-hour, 28-day, and in-hospital mortality rates, and the need for critical care in patient with suspicion of sepsis at the emergency department (ED).
Methods: A prospective observational study was performed in patients aged ≥ 18 years diagnosed with sepsis in the ED from March to November 2021. Area under the receiver operating characteristic curve (AUROC) analyses determined the predictive values of NEWS and NEWS‒L for 24-hour mortality.
Results: Ninety-two patients were enrolled (mean age 68 years, 48 [52.2%] males). Three (3.2%) patients died within 24 hours and 34 (36.9%) patients needed critical care during the ED stay. The median (interquartile range) NEWS and NEWS-L results were higher in the 24-hour non-survivors versus survivors: 12 (10.5, 12.5) versus 8 (6, 9) (p = 0.024) and 18.7 (15.2, 19.1) versus 10.6 (8.9, 13) (p = 0.036), respectively. The adjusted odds ratio (aOR) was 1.22 for the primary outcome as the NEWS-L increased by 1 unit without statistical significance (p = 0.228). The aOR values for the secondary outcomes ranged from 1.34 to 1.67 with statistical significance. A NEWS-L of 11 and a NEWS of 12 predicted 24-hour mortality with sensitivities/specificities of 100%/56% and 67%/91%, respectively. The AUROC values of NEWS-L for mortality at 24 hours, 48 hours, 28 days, and in-hospital patients, and the need for critical care were 0.860, 0.905, 0.813, 0.839, and 0.837, respectively.
Conclusion: NEWS-L is an accurate predictor for 24-hour mortality in septic patients in the ED. NEWS‒L performed better than NEWS for each outcome. NEWS‒L demonstrated good to excellent performance and was accurate in predicting sepsis related to adverse outcomes.
Keywords: National Early Warning Score, NEWS, NEWS-lactate, sepsis, mortality, need for critical care
Introduction
Based on statistics from high-income countries, global estimates of sepsis cases range from 19.4 to 31.5 million people with possibly 5.3 million deaths per year.1 In terms of hospitalization and hospital mortality, septic patients are a disproportionately high burden.2,3
Sepsis is described as a “life-threatening organ dysfunction induced by a dysregulated host response to infection” and organ dysfunction, as defined by a sequential organ failure assessment (SOFA) score of 2 in the Third International Consensus Definition for Sepsis and Septic Shock (Sepsis-3). In the absence of hypovolemia, septic shock is defined as the necessity for a vasopressor to maintain a mean arterial pressure of at least 65 mmHg and a serum lactate level of over 2 mmol/L (>18 mg/dL).4
The SOFA score, on the other hand, necessitates a number of laboratory values that are rarely available in the triage section of an emergency room. The time to receive test results can delay the diagnosis of a septic patient.5
For patients presenting to the emergency department (ED) with sepsis, various scoring systems have been developed and evaluated.6 The National Early Warning Score (NEWS) was created to predict the risk of cardiac arrest, intensive care unit (ICU) admission, and mortality in ward patients.7–9 A recent study by Churpek et al compared the accuracy of predicting in-hospital mortality in patients with suspected infection outside the ICU. They found that the discrimination was highest for NEWS, followed by the Modified Early Warning Score, quick SOFA, and systemic inflammatory response syndrome (p = 0.01 for all pairwise comparisons).10 Our hospital has used NEWS triaging for septic patients since 2018. A previous study conducted in our hospital defined NEWS ≥ 5 as sepsis and the patients were included into the hospital sepsis management protocol.11 This protocol was implemented as an alert protocol in the ED triage area to increase awareness of early sepsis detection. The full diagnostic criteria for sepsis using the SOFA score according to the Sepsis-3 definition are applied in patients with a NEWS ≥ 5.11,12
Hyperlactatemia has been linked to an increased risk of death in critically ill patients.13,14 At a cut-off value of 2 mmol/L, peripheral venous lactate can be used as a screening tool to rule out arterial hyperlactatemia in clinical practice. However, in the case of a peripheral venous lactate level > 2 mmol/L, hyperlactatemia should be validated via arterial sampling.15
According to the Surviving Sepsis Campaign Bundle: 2021, intravenous fluid is a resuscitation technique used to treat sepsis or septic shock to lower the serum lactate level. The serum lactate level should be measured every two to four hours if the initial blood lactate level is higher than 2 mmol/L prior to intravenous fluid infusion.15,16
The VitalPAC Early Warning Score‒lactate (ViEWS‒L) and NEWS‒Lactate (NEWS‒L) were found to be effective predictors of in-hospital mortality in adult ED patients by Jo et al17,18 However, limited data show early death in ED septic patients at 24 hours, which may reflect the quality of ED monitoring and treatment.
In this study, we aimed to evaluate the predictive performance of the NEWS‒L and NEWS in 24-hour mortality as the primary outcome. Furthermore, we aimed to evaluate the two early warning scores to predict the mortality rates at 48 hours, 28 days, and for in-hospital patients, and the need for critical care in septic patients. Also, we followed the patients admitted to the general ward and ICU.
Materials and Methods
Study Design and Setting
This study was a single-center prospective observational study conducted in the ED at the tertiary referral and academic 855-bed hospital and has ED volume over 48,000 patient visits per year. Approximately 75 adult septic patients visit this ED each month.
Selection of Participants
The data were collected from March to November 2021. The inclusion criteria for the study were patients aged ≥ 18 years old who visited the ED with an initial NEWS ≥ 5 and were diagnosed with sepsis. The exclusion criteria were pregnancy or lactation, referred patients, traumatic patients, incomplete information, palliative patients, or patients who refused resuscitation. The n4Studies tool was used to determine the sample size for the study population to evaluate two independent proportions and was calculated based on the Jo study.19,20 The final calculated sample size was 296 patients, which accounted for an expected drop-out rate of 10%.
Definitions of Variables
According to The United Kingdom, Royal College of Physicians 2012, the NEWS cut point of 5 is a middling score. Immunocompromised patients were those with underlying diseases such as viral infection, diabetes mellitus or malignancy disease with chemotherapy within the previous month, cirrhosis of the liver, or the use of immunosuppressive drugs.
Patients with suspicion of sepsis in our study were defined as patients who were clinically suspected of infection with a NEWS ≥ 5 and serum lactate > 2 mmol/L. The initial blood lactate level was considered admissible when blood was sampled within 60 minutes of ED arrival.
Lactate clearance was defined according to the following formula: (initial serum lactate level – serum lactate level within 2 hours) × 100/initial serum lactate level. ED length of stay was defined as the time from ED arrival to ED discharge or hospital admission.
The NEWS‒L is the sum of the NEWS (physiologic component) and the serum lactate level (mmol/L, laboratory component) (Table 1).19 For example, if the patient had a NEWS of 6 and serum lactate level of 3 mmol/L, the NEWS-L was 9. Initial serum lactate levels are typically determined at the study hospital using arterial blood; however, venous blood lactate levels can also be used followed only by a 2-hour arterial blood lactate after receiving treatments.
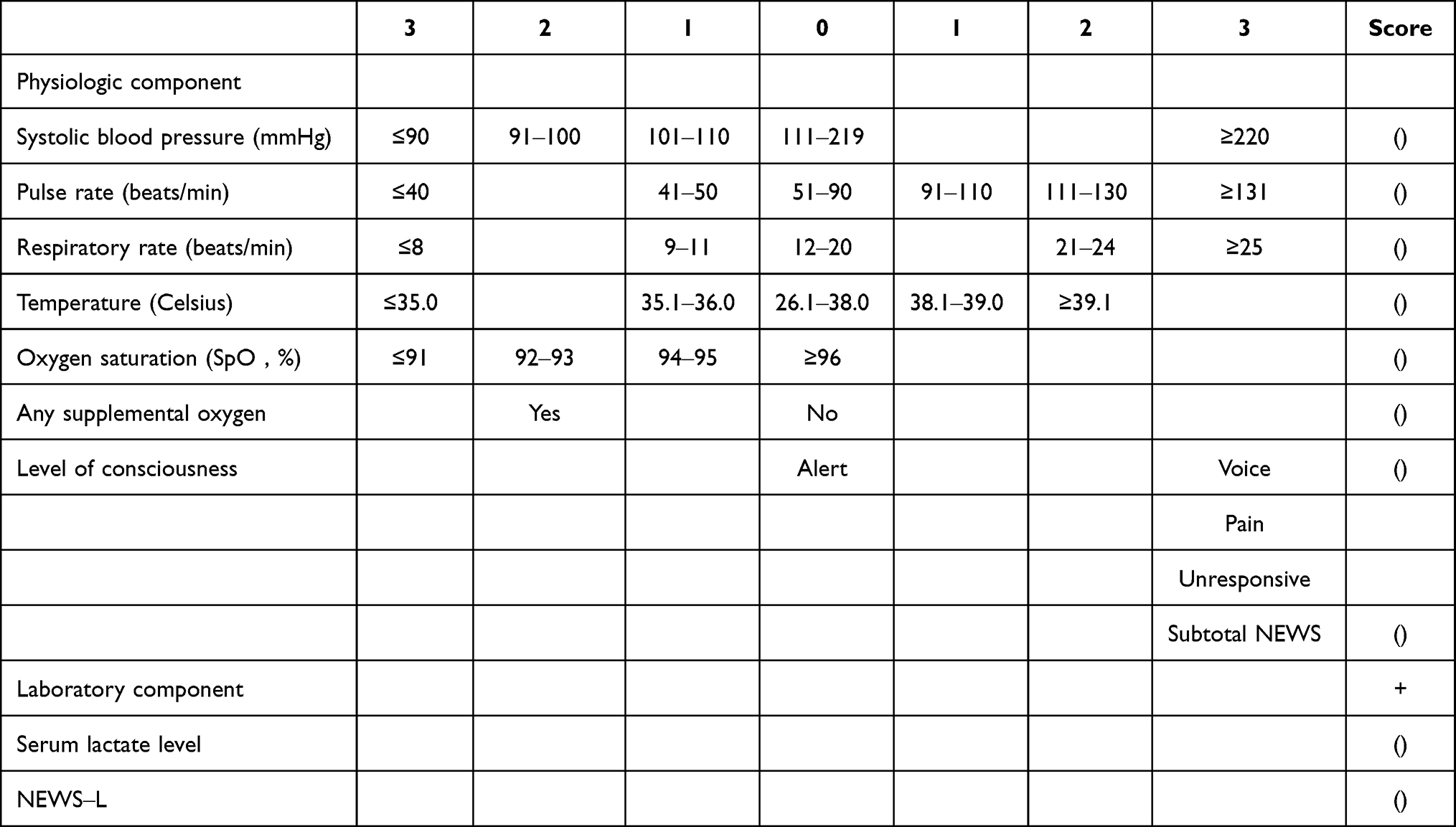 |
Table 1 NEWS and NEWS‒L Values. Adapted from Jo et al19 |
The need for critical care was defined practically and operationally by the use of either advanced airway or inotropic/vasopressor agents, or admission to the ICU, which is the primary location for providing invasive critical treatment including mechanical ventilation.
Data Collection
A case report form was developed and validated for the study and encompassed demographics, underlying diseases, medications related to immunocompromised status, Emergency Severity Index (ESI) level, initial NEWS, laboratory results (initial serum lactate, lactate level at two hours following treatments, culture results), SOFA score, treatments at ED, final diagnosis, ED disposition, need for critical care, and hospital outcome. Data were collected from the electronic medical records and ED data maintained by the study hospital. Following enrollment, patients were evaluated by the attending physicians. The initial lactate levels were measured and followed by arterial lactate measurements at two hours using a ABL800 Flex® blood gas analyzer (Radiometer Medical ApS, Denmark) using the amperometric assay. The attending physicians and medical teams were in charge of all medical treatments.
Outcome Measurements
The primary outcome was the predictive performances of the NEWS‒L and NEWS for 24-hour mortality. The secondary outcomes were the 48-hour, 28-day, and in-hospital mortality rates after admission, and the need for critical care.
Statistical Analysis
All data were loaded into EpiData version 3.1 and the statistical analysis was conducted using R software version 4.0.2 (The R Foundation, Vienna, Austria). Continuous variables with normal distribution were analyzed and reported as mean and standard deviation (SD). Non-normal variables are reported as median and interquartile range (IQR) while categorical variables are reported as percentages. The logistic regression analysis results are presented as an odds ratio (OR) with a 95% confidence interval (95% CI). The Student’s t-test for independent samples was used to compare the means of normally distributed variables. The Wilcoxon rank sum test was used for variables that were not normally distributed. The χ2 test or Fisher exact test was used where appropriate for categorical data. We adjusted for all possible confounders by identifying the essential predictive factors associated with increased 24-hour mortality. Independent factors with p-values < 0.20 identified during the univariate analysis were introduced into a multivariate logistic regression analysis model with backward stepwise selection. Sensitivity and specificity analyses were also performed for various cutoff values of the NEWS and NEWS‒L scores for 24-hour mortality. An area under the receiver operating characteristic curve (AUROC) analysis was used to determine the predictive values of the NEWS and NEWS‒L for mortality. Model discrimination was considered to be good if it yielded an AUROC of 0.7–0.8 and excellent if it yielded an AUROC of 0.8–0.9.21 Analytical results are described as OR with a 95% CI. A p-value < 0.05 was considered statistically significant.
Compliance with Ethical Requirements
The ethics committee of Prince of Songkla University approved this study (REC No. 63-357-20-4). The institutional review board of Prince of Songkla University is affiliated with the International Conference on Harmonization in Good Clinical Practice. According to our institutional review board protocol for delay of informed consent, the requirement for patient consent was done after complete treatment at the ED or when the patient could make the decision. In addition, consent was waived when the patients died because the participants had no more than minimal risk and the patients received standard treatment procedures. All study data were retained as confidential data in an encrypted file with a password and only the researcher and assistant could access the data.
Results
Demographic Data
During the study period, 315 adult patients with organ infection and NEWS ≥ 5 were enrolled. Nine-two patients met the enrollment criteria. The baseline characteristics of the study patients are presented in Table 2. Forty-eight (52.2%) patients were male and the mean age was 68 years. The three main comorbidities were diabetes mellitus (26.1%), chemotherapy session (31.5%), and immunosuppressive agent use (9.8%). The five significant variables between the non-survivors and survivors in 24 hours included the mean ± standard deviation (SD) values of heart rate (115.8 ± 18.8 bpm), respiratory rate (32.6 ± 7/min), central venous catheter use (1 ± 1.1 patient), and the median (interquartile range [IQR]) values of oxygen saturation (96% [92, 98]) and hospital length of stay (6.3 days [2, 10.9]). The ED disposition included 23 (25%) patients admitted to the ICU, 60 (67.4%) patients admitted to the general ward, and 8 (8.7%) discharged patients (Figure 1). The median ED length of stay (EDLOS) was 4.6 hours without statistical significance. The sources of infection in our study were pulmonary (29.3%), urinary tract (22.8%), intra-abdominal (21.7%), bacteremia (9.8%), skin and soft tissue (8.7%), and others (7.6%).
 |
Table 2 Demographic and Baseline Characteristics of the Study Patients |
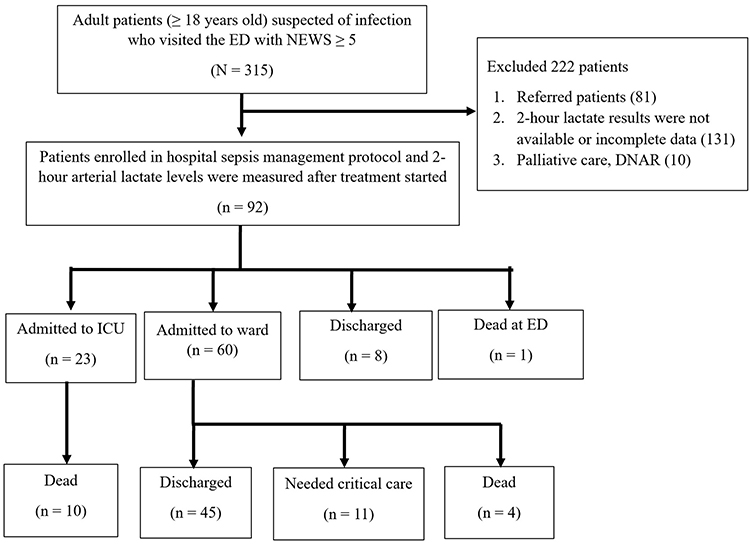 |
Figure 1 Study flow diagram of enrolled patients. |
NEWS‒L and NEWS to Predict Mortality and the Need for Critical Care
The median (IQR) results for NEWS were significantly higher in the 24-hour non-survivor group versus the survivor group with values of 12 (10.5, 12.5) versus 8 (6, 9) (p = 0.024), and for NEWS‒L the values were 18.7 (15.2, 19.1) versus 10.6 (8.9, 13) (p = 0.036), respectively. The initial lactate and lactate levels at 2 hours in 24-hour non-survivors were higher than survivors. Furthermore, lactate clearance in 2 hours was lower in 24-hour non-survivors but without statistical significance (Table 3). Three (3.2%) patients died within 24 hours, 5 (5.4%) died within 48 hours, 12 (13%) died within 28 days, and 34 (36.9%) needed critical care during the ED stay.
 |
Table 3 Comparison of NEWS, NEWS-L, SOFA Score, Lactate Levels and Lactate Clearance with 24-Hr Mortality of Sepsis Patients in the Emergency Department |
Multivariate analysis with logistic regression was performed and adjusted for age, sex, and ESI triage level. The adjusted OR (aOR) for the primary outcome was 1.22 as the NEWS‒L increased by 1 unit without statistical significance (p = 0.228). The aOR values for the secondary outcomes ranged from 1.34 to 1.67 with statistical significance (Table 4).
 |
Table 4 Multivariate Logistic Regression Analysis of NEWS-L for Mortality Prediction |
We excluded the results of NEWS‒L/NEWS less than 6 because no deaths occurred in these scores. Next, we selected the cut-off values of the NEWS‒L and NEWS from 6 to 16 individually in predicting 24-hour mortality. The sensitivities and specificities are shown in Table 5. Twenty-four-hour mortality could be predicted with a NEWS‒L of 11 with a sensitivity and specificity of 100% and 56% and a NEWS of 12 with a sensitivity and specificity of 67% and 91%. Thus, intensive monitoring in the ED should be provided in these patients.
 |
Table 5 Predictive Performance of NEWS and NEWS‒L for 24-Hour Mortality |
The AUROC values of NEWS‒L/NEWS for 24-hour, 48-hour, 28-day, and in-hospital mortality rates, and the need for critical care were 0.860/0.882, 0.905/0.809, 0.813/0.796, 0.839/0.822, and 0.837/0.770, respectively. For each outcome NEWS‒L performed better than NEWS. Generally, NEWS‒L demonstrated good to excellent performance to predict sepsis related to adverse outcomes (Figure 2).
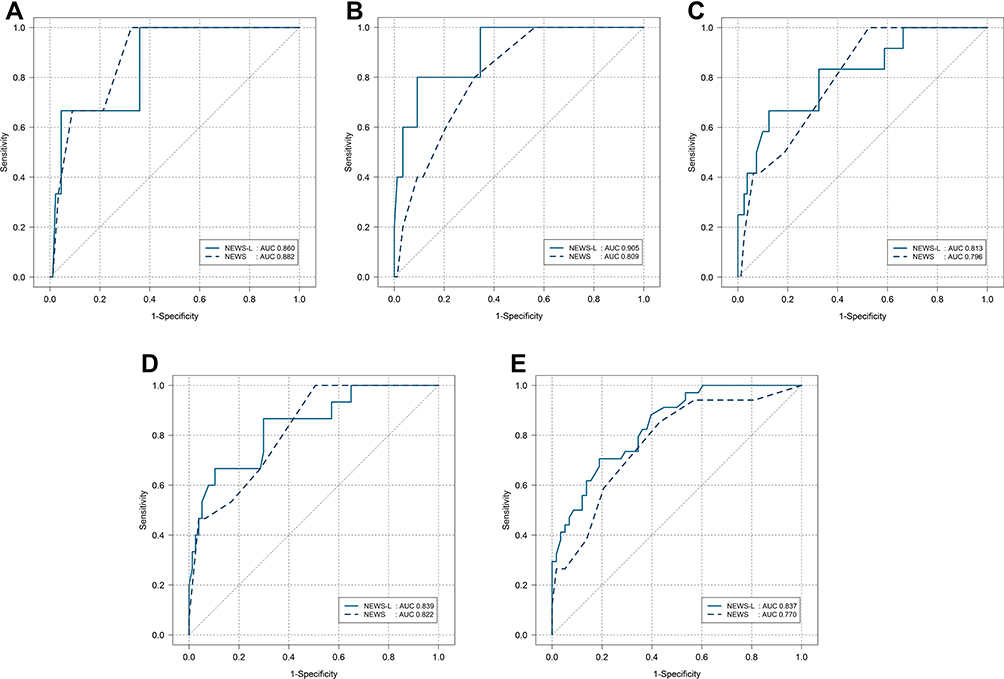 |
Figure 2 Receiver operating curves for patients with sepsis by NEWS and NEWS‒L: (A) 24-hour mortality; (B) 48-hour mortality; (C) 28-day mortality; (D) In-hospital mortality; (E) Need for critical care. |
Discussion
We evaluated the predictive performance of NEWS and NEWS‒L for several outcomes that included mortality status of patients at 24 hours, 48 hours, 28 days, and for in-hospital patients, and the need for critical care among adult septic patients in the ED. The main results of this study in multivariate logistic regression revealed that NEWS‒L was associated with 24-hour mortality (OR = 1.22). However, the predictive performance of NEWS‒L was significantly accurate for 48-hour, 28-day, and in-hospital mortality, and the need for critical care. NEWS-L could predict 24-hour mortality at a score of 11 with high sensitivity (100%) but low specificity (56%). NEWS could predict 24-hour mortality at a score of 12 with moderate sensitivity (67%) and high specificity (91%).
Since sepsis is a dynamic condition, any technique that relies only on a single measurement of a physiological parameter may be inaccurate in forecasting the progression of sepsis. Screening patients using both physiological data and rapid blood tests can help improve emergency patient treatment.5 Moreover, evaluating patients in an ED setting is always challenging. Implementation of effective diagnostic tools and appropriate treatment guidance is mandatory. NEWS is a well-validated tool in predicting unanticipated ICU admission, cardiac arrest, and mortality within 24 hours among ward and ED patients.22 A study by Brink et al showed NEWS was superior to other scoring systems in predicting mortality in ED septic patients.23 Furthermore, the discrimination power increased when combined with lactate level as in NEWS‒L.19 In recent literature, new studies are available on combining early warning scores (EWS) with different biomarkers including D-dimer, soluble urokinase plasminogen activator receptor, plasma midregional proadrenomedullin, and procalcitonin.24–28 Nevertheless, those biomarkers are not routinely measured in the ED setting, especially in limited resource facilities.
One large study included 198,755 vital signs datasets from general medical emergency patients. The ability of NEWS was tested to discriminate risk of cardiac arrest, unanticipated ICU admission or death within 24 hours between NEWS and other EWS. The conclusion was NEWS had a greater ability than other early warning scoring systems in distinguishing patients at risk in those specific combined adverse outcomes. The NEWS AUROC (95% CI) values within 24 hours were as follows: cardiac arrest 0.722 (0.685‒0.759), unanticipated ICU admission 0.857 (0.847‒0.868), death 0.894 (0.887‒0.902), and any of the outcomes 0.873 (0.866‒0.879).22 The NEWS AUROC values in predicting 24-hour mortality in this current study was 0.882, which was similar to a study by Smith et al.22
The overall ICU mortality rates in patients with sepsis and septic shock studied by Khwannimit et al in our hospital were 10.7% and 47%, respectively.3 Thirty-six percent of sepsis and septic shock patients admitted to the ICU came from the ED.3 Thus, it is imperative to identify high-risk patients in the ED and provide early resuscitation to decrease ICU mortality of septic patients. Effective early critical care intervention and implementation of an ED-based ICU were associated with a reduction of in-hospital mortality from 2.13% to 1.83% and ICU admissions from 3.2% to 2.7% among all ED patient visits.29 Furthermore, Nelson and coworkers found that 15% of all critical care was performed in the ED.30
In addition, in our ED the need for critical care was greater than ICU admission since the number of patients indicated for critical care were higher than patients admitted to the ICU (36.9% versus 25%). Our study revealed that the AUROC values in predicting the need for critical care for NEWS‒L and NEWS were 0.837 and 0.770, respectively. These results were lower than the study by Jo et al, which reported AUROC values for NEWS‒L and NEWS of 0.860 and 0.830, respectively, in patients who presented with disease infection.19 Identifying patients who need critical care using NEWS‒L may provide appropriate clinical intervention before deterioration of their condition.
The present study demonstrated that non-survivors had higher NEWS than survivors. Similarly, previous investigations reported that NEWS on ED admission was a predictor of adverse outcomes in adult ED patients irrespective of age and comorbidities.9,23,31–33 Our study confirmed the findings by Churpek et al that supported the introduction of NEWS in the ED.10 However, they studied patients in the ED and outside the ICU and suggested a NEWS threshold of ≥ 7. This threshold is also recommended by the Royal College of Physicians.7,8 The median NEWS in the present study was 12 in 24-hour non-survivors, which was similar to a NEWS of 11.5 in a former study.19
The lactate level on ED admission is associated with in-hospital and 30-day mortality in different patient populations.12,25,34 Many studies found that lactate clearance at two hours was probably sufficient in most acute conditions, which is currently recommended in resuscitation guidelines and significantly reduces ICU length of stay and in-hospital mortality. However, the present study revealed that only the initial lactate level and lactate clearance at two hours were insufficient in predicting 24-hour mortality.
Our study showed that the NEWS‒L in 24-hour non-survivors was higher than in NEWS‒L survivors. Therefore, NEWS‒L was associated with 24-hour mortality; however, no statistical significance was observed. The predictive performance of NEWS‒L is significantly accurate to predict mortality at 48 hours, 28 days, and for in-hospital patients, and the need for critical care. These results were compatible with previous studies.19,25 Jo et al found that NEWS‒L and ViEWS‒L were powerful predictors of in-hospital mortality in general ED patients.18,19 The results of many studies are contradictory. For example, Lee et al found that NEWS‒L was a moderately accurate predictor of in-hospital mortality in adult patients outside the ICU with sepsis.25 Also, Leung et al found that the combination of lactate level with NEWS did not improve the prognostic value of NEWS in predicting 7-day mortality in septic patients in the ED.26 The different results are possibly explained by different protocols used to diagnose sepsis and the various mortality outcomes.
Overall, the median NEWS‒L, NEWS, and lactate values of the non-survivors in our study were higher than previous studies. As a result, the proportion of need for critical care and the mortality outcome in our study were quite high. The differences can be explained by taking into account that this study collected data in the ED of a tertiary hospital where most of the patients had multiple comorbidities and used immunosuppressive medications. The number of non-survivors in our study was only three patients, which would be weak in an external validity analysis.
Other common physiological variables identified as significant factors in our study in the group of 24-hour non-survivors were: mean ± SD heart rate (139.3 ± 19 bpm), median (IQR) respiratory rate (46 [43,48] rate/minute), and the median (IQR) oxygen saturation (71 [63.5, 81.5] %). Delayed placement of invasive mechanical ventilation in patients having acute hypoxemic respiratory failure after failure of a high flow nasal cannula or non-invasive ventilation increased ICU mortality and poor patient prognosis.35,36
In our study, the median time of EDLOS was 4.6 hours without statistical significance. However, a study by Agustin et al concluded that clinical outcomes of sepsis patients were not significantly different between early and delayed ICU admission.37 On the other hand, a study by Zhang et al showed increased in-hospital mortality when septic patients were in the ED longer than 12 hours and subsequently required ICU admission.38
This study presents new knowledge on the early prognostic values of NEWS‒L related to short-term mortality (ie, 24 hours and 48 hours), which is limited in previous studies. Therefore, our study supports the growing evidence that suggests NEWS is a sensitive screening tool in the ED to predict early sepsis-related outcomes. The calculation of NEWS in our setting by triage nurses has additive value and reflects the practically of its use.
We must acknowledge the limitations of the present study. First, we aimed for 296 participants but only 93 (31.4%) patients were enrolled in the study. A larger sample and extended duration would improve a future study. Second, a total of 131 (41.6%) patients were excluded from the study due to the lack of documented 2-hour lactate levels. During the COVID-19 pandemic, the management of a patient under investigation who had respiratory tract symptoms required hospital admission within 2 hours. Therefore, a blood sample for lactate level could not be collected in all septic patients at 2 hours. Third, a subgroup analysis was not conducted to assess patients on beta-blockers or calcium channel blockers. These drugs might affect the heart rate and blood pressure response, which may affect NEWS. Finally, this study was conducted in a single-center tertiary care hospital. A multicenter study may increase the generalizability of the study.
Conclusions
Among septic patients in the ED, NEWS‒L is an accurate predictor for 24-hour mortality and performed better than NEWS for each outcome. Generally, NEWS‒L demonstrated good to excellent performance to predict sepsis related to adverse outcomes.
Data Sharing Statement
The prospective data used to support the findings of this study are available from the corresponding author upon request.
Acknowledgments
The authors are grateful to Kingkarn Waiyanak for article searches and retrieval, Nannapat Pruphetkaew, Epidemiology Unit, for statistical assistance, Glenn K. Shingledecker for his help in editing the manuscript, and the Faculty of Medicine for funding this research.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The Faculty of Medicine funded this research.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Fleischmann C, Scherag A, Adhikari NK, et al. Assessment of global incidence and mortality of hospital-treated sepsis current estimates and limitations. Am J Respir Crit Care Med. 2016;193:259–272. doi:10.1164/rccm.201504-0781OC
2. Paoli CJ, Reynolds MA, Sinha M, Gitlin M, Crouser E. Epidemiology and costs of sepsis in the United States-an analysis based on timing of diagnosis and severity level. Crit Care Med. 2018;46:1889–1897. doi:10.1097/CCM.0000000000003342
3. Khwannimit B, Bhurayanontachai R. The direct costs of intensive care management and risk factors for financial burden of patients with severe sepsis and septic shock. J Crit Care. 2015;30:929–934. doi:10.1016/j.jcrc.2015.05.011
4. Singer M, Deutschman CS, Seymour CW, et al. The third international consensus definitions for sepsis and septic shock (Sepsis-3). JAMA. 2016;315:801–810. doi:10.1001/jama.2016.0287
5. Worapratya P, Wuthisuthimethawee P. Septic shock in the ER diagnostic and management challenges. Open Access Emerg Med. 2019;11:77–86. doi:10.2147/OAEM.S166086
6. Smith GB, Prytherch DR, Schmidt PE, Featherstone PI. Review and performance evaluation of aggregate weighted ‘track and trigger’ systems. Resuscitation. 2008;77:170–179. doi:10.1016/j.resuscitation.2007.12.004
7. Royal College of Physicians. National Early Warning Score. NEWS: Standardising the Assessment of Acute-Illness Severity in the NHS: Royal College of Physicians. London: Royal College of Physicians; 2012.
8. Department of Health. National Early Warning Score, national clinical guideline no. 1; 2013 [cited March 27, 2021]. Available from: http://health.gov.ie/wp-content/uploads/2015/01/NEWSFull-ReportAugust2014.pdf.
9. Keep JW, Messmer AS, Sladden R, et al. National early warning score at Emergency Department triage may allow earlier identification of patients with severe sepsis and septic shock: a retrospective observational study. Emerg Med J. 2016;33:37–41. doi:10.1136/emermed-2014-204465
10. Churpek MM, Snyder A, Han X, et al. Quick sepsis-related organ failure assessment, systemic inflammatory response syndrome, and early warning scores for detecting clinical deterioration in infected patients outside the intensive care unit. Am J Respir Crit Care Med. 2017;195:906–911. doi:10.1164/rccm.201604-0854OC
11. Limapichat T, Pattanapong K. Normal saline solution or lactated ringer’s solution to enhance lactate clearance in septic patients after initial resuscitation in the ED: a retrospective cohort trial. Open Access Emerg Med. 2021;13:511–519. doi:10.2147/OAEM.S340691
12. Uffen JW, Oosterheert JJ, Schweitzer VA, Thursky K, Kaasjager HAH, Ekkelenkamp MB. Interventions for rapid recognition and treatment of sepsis in the emergency department: a narrative review. Clin Microbiol Infect. 2021;27(2):192–203. PMID: 32120030. doi:10.1016/j.cmi.2020.02.022
13. Casserly B, Phillips GS, Schorr C, et al. Lactate measurements in sepsis-induced tissue hypoperfusion: results from the Surviving Sepsis Campaign database. Crit Care Med. 2015;43:567–573. doi:10.1097/CCM.0000000000000742
14. Levy B. Lactate and shock state: the metabolic view. Curr Opin Crit Care. 2006;12:315–321. doi:10.1097/01.ccx.0000235208.77450.15
15. van Tienhoven AJ, van Beers CAJ, Siegert CEH. Agreement between arterial and peripheral venous lactate levels in the ED: a systematic review. Am J Emerg Med. 2019;37:746–750. doi:10.1016/j.ajem.2019.01.034
16. Evans L, Rhodes A, Alhazzani W, et al. Surviving sepsis campaign: international guidelines for management of sepsis and septic shock 2021. Crit Care Med. 2021;49(11):e1063–e1143. doi:10.1097/CCM.0000000000005337
17. Vincent JL, Quintairos E, Silva A, Couto L, Taccone FS. The value of blood lactate kinetics in critically ill patients: a systematic review. Crit Care. 2016;20:257. doi:10.1186/s13054-016-1403-5
18. Jo S, Lee JB, Jin YH, et al. Modified early warning score with rapid lactate level in critically ill medical patients: the ViEWS-L score. Emerg Med J. 2013;30:123–129. doi:10.1136/emermed-2011-200760
19. Jo S, Yoon J, Lee JB, Jin Y, Jeong T, Park B. Predictive value of the National Early Warning Score-Lactate for mortality and the need for critical care among general emergency department patients. J Crit Care. 2016;36:60–68. doi:10.1016/j.jcrc.2016.06.016
20. Ngamjarus C, Chongsuvivatwong V n4Studies: sample size and power calculations for iOS. The Royal Golden Jubilee Ph.D. Program. Songkla: The Thailand Research Fund & Prince of Songkla University; 2014.
21. Hanley JA, McNeil BJ. The meaning and use of the area under a receiver operating characteristic (ROC) curve. Radiology. 1982;143:29–36. doi:10.1148/radiology.143.1.7063747
22. Smith GB, Prytherch DR, Meredith P, Schmidt PE, Featherstone PI. The ability of the National Early Warning Score (NEWS) to discriminate patients at risk of early cardiac arrest, unanticipated intensive care unit admission, and death. Resuscitation. 2013;84:465–470. doi:10.1016/j.resuscitation.2012.12.016
23. Brink A, Alsma J, Verdonschot RJCG, et al. Predicting mortality in patients with suspected sepsis at the emergency department; A retrospective cohort study comparing qSOFA, SIRS and National Early Warning Score. PLoS One. 2019;14:e0211133. doi:10.1371/journal.pone.0211133
24. Eckart A, Hauser SI, Kutz A, et al. Combination of the National Early Warning Score (NEWS) and inflammatory biomarkers for early risk stratification in emergency department patients: results of a multinational, observational study. BMJ Open. 2019;9:e024636. doi:10.1136/bmjopen-2018-024636
25. Lee CT, Snyder AM, Edelson DP, Churpek MM. The prognostic value of lactate and comparison to other scoring systems in septic patients outside the intensive care unit. Am J Respir Crit Care Med. 2017;195:A2780.
26. Leung L, Hung KK, Lo RS, Yeung C, Chan S, Graham CA. Prognostic value of qSOFA, SIRS and News in the emergency department for predicting 7-day mortality: a prospective study. Ann Emerg Med. 2018;72:S3. doi:10.1016/j.annemergmed.2018.08.011
27. Nickel CH, Kellett J, Cooksley T, Bingisser R, Henriksen DP, Brabrand M. Combined use of the National Early Warning Score and D-dimer levels to predict 30-day and 365-day mortality in medical patients. Resuscitation. 2016;106:49–52. doi:10.1016/j.resuscitation.2016.06.012
28. Rasmussen LJH, Ladelund S, Haupt TH, Ellekilde GE, Eugen-Olsen J, Andersen O. Combining national early warning score with soluble urokinase plasminogen activator receptor (suPAR) improves risk prediction in acute medical patients: a registry-based cohort study. Crit Care Med. 2018;46:1961–1968. doi:10.1097/CCM.0000000000003441
29. Gunnerson KJ, Bassin BS, Havey RA, et al. Association of an emergency department–based intensive care unit with survival and inpatient intensive care unit admissions. JAMA Netw Open. 2019;2:e197584. doi:10.1001/jamanetworkopen.2019.7584
30. Nelson M, Waldrop RD, Jones J, Randall Z. Critical care provided in an urban emergency department. Am J Emerg Med. 1998;16:56–59. doi:10.1016/S0735-6757(98)90066-3
31. Alam N, Vegting IL, Houben E, et al. Exploring the performance of the National Early Warning Score (NEWS) in a European emergency department. Resuscitation. 2015;90:111–115. doi:10.1016/j.resuscitation.2015.02.011
32. Lee YS, Choi JW, Park YH, et al. Evaluation of the efficacy of the National Early Warning Score in predicting in-hospital mortality via the risk stratification. J Crit Care. 2018;47:222–226. doi:10.1016/j.jcrc.2018.07.011
33. Almutary A, Althunayyan S, Alenazi K, et al. National early warning score (NEWS) as prognostic triage tool for septic patients. Infect Drug Resist. 2020;13:3843–3851. doi:10.2147/IDR.S275390
34. Park YJ, Kim DH, Kim SC, et al. Serum lactate upon emergency department arrival as a predictor of 30-day in-hospital mortality in an unselected population. PLoS One. 2018;13:e0190519. doi:10.1371/journal.pone.0190519
35. Kang BJ, Koh Y, Lim CM, et al. Failure of high-flow nasal cannula therapy may delay intubation and increase mortality. Intensive Care Med. 2015;41:623–632. doi:10.1007/s00134-015-3693-5
36. Moretti M, Cilione C, Tampieri A, Fracchia C, Marchioni A, Nava S. Incidence and causes of non-invasive mechanical ventilation failure after initial success. Thorax. 2000;55:819–825. doi:10.1136/thorax.55.10.819
37. Agustin M, Price LL, Andoh-Duku A, LaCamera P. Impact of delayed admission to the intensive care unit from the emergency department upon sepsis outcomes and sepsis protocol compliance. Crit Care Res Pract. 2017;2017:9616545. doi:10.1155/2017/9616545
38. Zhang Z, Bokhari F, Guo Y, Goyal H. Prolonged length of stay in the emergency department and increased risk of hospital mortality in patients with sepsis requiring ICU admission. Emerg Med J. 2019;36:82–87. doi:10.1136/emermed-2018-208032
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Role of Procalcitonin in Predicting Mortality and Organ Dysfunction at Intensive Care Admission
Suranadi IW, Sinardja CD, Suryadi IA
International Journal of General Medicine 2022, 15:4917-4923
Published Date: 12 May 2022
Resistin Concentration in Early Sepsis and All-Cause Mortality at a Safety-Net Hospital in Riverside County
Bonenfant J, Li J, Nasouf L, Miller J, Lowe T, Jaroszewski L, Qiu X, Thapamagar S, Mittal A, Godzik A, Klein W, Nair MG
Journal of Inflammation Research 2022, 15:3925-3940
Published Date: 13 July 2022
Albumin Level is Associated with Short-Term and Long-Term Outcomes in Sepsis Patients Admitted in the ICU: A Large Public Database Retrospective Research
Cao Y, Su Y, Guo C, He L, Ding N
Clinical Epidemiology 2023, 15:263-273
Published Date: 3 March 2023
Multidrug-Resistant Bacteria on Critically Ill Patients with Sepsis at Hospital Admission: Risk Factors and Effects on Hospital Mortality
Maia MDO, da Silveira CDG, Gomes M, Fernandes SES, Bezerra de Santana R, de Oliveira DQ, Amorim FFP, Neves FDAR, Amorim FF
Infection and Drug Resistance 2023, 16:1693-1704
Published Date: 23 March 2023
LASSO-Based Identification of Risk Factors and Development of a Prediction Model for Sepsis Patients
Hong C, Xiong Y, Xia J, Huang W, Xia A, Xu S, Chen Y, Xu Z, Chen H, Zhang Z
Therapeutics and Clinical Risk Management 2024, 20:47-58
Published Date: 7 February 2024