Back to Journals » Vascular Health and Risk Management » Volume 16
Predictive Performance of Pender’s Health Promotion Model for Hypertension Control in Iranian Patients
Authors Gorbani F ![]() , Mahmoodi H
, Mahmoodi H ![]() , Sarbakhsh P
, Sarbakhsh P ![]() , Shaghaghi A
, Shaghaghi A ![]()
Received 23 April 2020
Accepted for publication 5 July 2020
Published 17 July 2020 Volume 2020:16 Pages 299—305
DOI https://doi.org/10.2147/VHRM.S258458
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Konstantinos Tziomalos
Fatemeh Gorbani,1 Hassan Mahmoodi,2 Parvin Sarbakhsh,3 Abdolreza Shaghaghi1
1Department of Health Education and Promotion, Faculty of Health, Tabriz University of Medical Sciences, Tabriz, Iran; 2Social Determinant of Health Research Center, Research Institute for Health Development, Kurdistan University of Medical Sciences, Sanandaj, Iran; 3Department of Biostatistics and Epidemiology, Faculty of Health, Tabriz University of Medical Sciences, Tabriz, Iran
Correspondence: Abdolreza Shaghaghi
Department of Health Education and Promotion, Faculty of Health, Tabriz University of Medical Sciences, Tabriz, Iran Tel +0098 41 333 57580-3
Fax +0098 41 333 40634
Email [email protected]
Objective: The main aim of this study was to investigate predictive factors of adherence to the hypertension control therapeutic and lifestyle recommendations in a sample of Iranian patients based on the constructs of Pender’s health promotion model.
Patients and Methods: The cross-sectional study was performed on the 380 hypertensive patients who were referred to the health centers, the emergency and internal diseases departments of the Bagheralolom Hospital, and the cardiologists’ offices in the city of Ahar, North West of Iran. Data were collected using a researcher designed questionnaire based on the Pender’s health promotion model. The Pearson correlation test, multivariate linear regression, and independent t-test were used for data analysis.
Results: Mean age of the recruited patients was 52.94 (SD=12.8). Perceived benefits, perceived barriers, situational influences, and interpersonal influences (adjusted R2= 0.525) explained 52.5% of the observed variation in adherence to hypertension control recommendations.
Conclusion: Successful hypertension control in patients with chronic morbidity need to be based on sound data about major determinants of the relevant health/illness behaviors. The study findings revealed that the Pender’s health promotion model could be applicable as a theoretical framework to identify major determinants of adherence to hypertension control recommendations. Future cross-cultural validation of the study findings in more representative and larger sample sizes could add to the legitimacy of the evidence surrounding self-care practices in hypertensive patients.
Keywords: hypertension, diseases control, Pender’s model
Introduction
Hypertension is a global public health issue with a major impact on the burden of cardiovascular and cerebrovascular disorders or subsequent possible premature deaths.1 Hypertension generally has no symptoms in the early stages; therefore, many undiagnosed patients may not seek treatment for their blood pressure (BP) control. Appropriate control of BP, however, could prevent costly medical procedures, ie, hemodialysis or cardiovascular surgeries for treatment of complications in hypertensive patients.1 Hypertension is also the leading precipitating factor in 51% of deaths from stroke and 45% of deaths attributed to ischemic heart disease (IHD) worldwide.2 The hypertension prevalence rate could vary widely from 10% to over 60% across countries3 and its rate was reported to be 26.21% in Iran.4
The relatively high prevalence of hypertension in low and middle income countries reflects the inadequacy of control measures in consequence of inherent insufficiencies within the healthcare provision systems.1 A higher hypertension associated mortality rate could be expected in these countries5 due to paucities in healthcare systems and self-management of the disease.6 Self-management of hypertension includes taking the prescribed medications, monitoring of blood pressure level, and following of the lifestyle modification recommendations given by the healthcare professionals (HCPs).7 The research evidence demonstrated that self-care practices are permissive for hypertension control but not implicitly adequate for a full accomplishment.8
Determinants of poor blood pressure control were reported in earlier studies9,10 but due to its potential in posing an immediate life threat in certain circumstances, various aspects of the disease and patients status must be considered very carefully in interventions to control the elevated BP. Lifestyle modifications to control hypertension should include medication adherence,11,12 dietary modification,13,14 adequate physical activity,15,16 stress control,17 smoking cessation,18 and establishment of an effortless and efficient communication milieu to provide information or the required consultation for hypertensive patients.19 Previous studies revealed that lifestyle modification for a better hypertension control profile can be achieved if a well-planned intervention based on the evidence based knowledge is chosen.20
The Pender’s Model of Health Promotion as a midrange model to envisage multiple predicting factors of health-related behaviors21 was used successfully in predicting lifestyle changes among patients with diabetes and in planning interventions for an improved diseases outcome.20,21 The model’s constructs can also be used in intervention studies to prevent other diseases’ risk factors or induce behavior change for health promotion purposes.22
To the best of our knowledge, no study was implemented earlier to inspect the pertinence of the model’s constructs in prediction of diseases control behaviors among Iranian hypertensive patients. The main aim of this study was to investigate the applicability of the Pender’s health promotion model in predicting the Iranian patients’ self-care practices for hypertension control.
Patients and Methods
Participants and Procedures
This cross-sectional study was performed on the 380 patients with hypertension in the city of Ahar, North West of Iran in 2016. Data were collected using a researcher designed questionnaire consisting of two sections. The first section included demographic questions and the second section consisted of questions about adherence to the hypertension control therapeutic and lifestyle recommendations (on-time medication taking, nutritional changes, physical activity enhancement, better stress management, and not smoking). The questions about the hypertension control behavioral profile were selected and arranged based on the constructs of Pender’s health promotion model. A convenience sampling method was utilized to recruit the study respondents from patients referred to the health centers, the emergency and general internal departments of the Bagheralolom Hospital, and also cardiologists’ offices in the city of Ahar, North West of Iran. All the study procedures were described to the selected patients and their right to withdraw from the study at any point or refuse to answer any particular question(s) was emphasized in very simple language. A written informed consent form was obtained from each of the respondents (signed with pen or fingerprint based on the attendees’ convenience) before their participation in the study. Patients were asked to self-complete the study questionnaires; however, the interviewer remained close to the patients to answer any question and also receive the completed questionnaires. For those participants who could not read the questionnaires, a face-to-face oral interview was performed according to the questionnaire items. Inclusion criteria to be entered into the study were having HBP for at least 1 year and not having any cognitive dysfunction which could interfere with the study conduction.
Questionnaire Development
An intensive literature review was performed to identify the reported predicting variables of hypertension control in previous studies. Thus, 30 items were identified that were arranged in six domains consistent with the Pender’s model constructs, ie, perceived benefit (6 items), perceived barriers (13 items); commitment to action (4 items), perceived self-efficacy (3 items), situational influences (2 items), and interpersonal influences (2 items).
The content validity of the structured questionnaire was tested qualitatively (based on the feedback forms of an expert panel consisting of health promotion and cardiology specialists) and quantitatively (based on the level of agreement among the panelists by calculation of the Content Validity Index (CVI) (values >0.79 were considered acceptable) and Content Validity Ratio (CVR) (values >0.62 were deemed to be acceptable). The test re-test reliability coefficient was also estimated based on the responses given by the 20 patients in 2 weeks interval ICC=0.88). The Alpha Cronbach’s internal consistency coefficient for the whole questionnaire was 0.82 and for its six subscales were in the vicinity of the acceptable range, ie, perceived benefit (6 items, α=0.72), perceived barriers (13 items, α=0.89), commitment to action (4 items, α=0.84), perceived self-efficacy (3 items, α=0.84);, situational influences (2 items, α=0.79), and interpersonal influences (2 items, α=0.78).
Data Analyses
The statistical analysis was performed using the Statistical Package for Social Sciences (SPSS) v. 17 for Windows (SPSS Inc., Chicago, IL). t-test was used to compare diseases control status in different socio-demographic strata. The Pearson correlation coefficient was calculated to assess the relation between the questionnaire’s subscales or Pender’s model constructs. Simple linear regression was applied to assess correlation between the patients’ subscales scores. In the univariate analysis, each variable (socio-demographic variables or Pender’s model constructs) was separately entered into the analysis process. The significant variables found in the univariate analyses were entered into multiple regression analysis. A backward elimination multiple linear regression was performed to find a set of best predictors for diseases control. The a priori level of significance was considered to be 0.05.
Results
Among the 380 patients who participated in this study about 55.0% were men and 77.9% were married. The reported educational level for 30.5% of the attendees was elementary or higher. About 9.5% of the study respondents proclaimed to be in full time employment, 40.8% reported to be cigarette ex-smokers, and 33.7% claimed to be current cigarette smokers (Table 1).
 |
Table 1 Association of the Socio-Demographic Characteristics and Mean Total Score of Hypertension Control Amongst the Studied Iranian Patients |
A statistically significant difference was observed in the hypertension control scores of men and women and those with or without a history of previous smoking or those who reported to be current smokers with non-smokers (Table 1).
Table 2 presents the observed correlation between the total and subscale scores of the inventory of hypertension control determinants classified based on the Pender’s health promotion model, ie, perceived benefits, perceived barriers, and commitment to action, perceived self-efficacy, situational influences, and interpersonal influences. Perceived benefits (r=0.617, P<0.01), commitment to action (r=0.628, P<0.01), perceived self-efficacy (r=0.411, P<0.01), situational influences (r=0.446, P<0.01), and interpersonal influences (r=0.393, P<0.01) indicated a positive correlation with the hypertension control overall scores but perceived barriers (r=−0.488, P<0.01) were found to be negatively correlated with the overall score (Table 2).
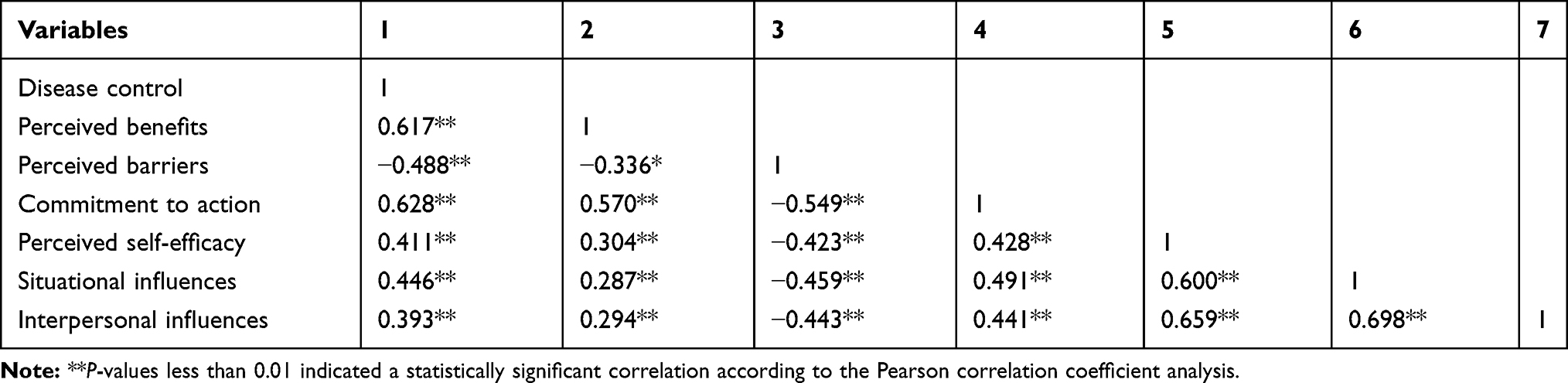 |
Table 2 Correlation Between Total and Subscale Scores of the Inventory of Hypertension Control Determinants Classified Based on the Pender’s Health Promotion Model Constructs |
Predictors of Diseases Control Among Hypertensive Patients
Based on the univariate regression analysis outputs, gender (R2=0.020, P<0.006), previous history of smoking (R2=0.029, P<0.001), being a current smoker (R2=0.024, P<0.001), perceived benefit to change behavior (R2=0.379, P<0.001, perceived barriers to change behavior (R2=0.236, P<0.001), commitment to action (R2=0.393, p<0.001), perceived self-efficacy (R2=0.167, P<0.001), situational influences (R2=0.197, P<0.001), and interpersonal influences (R2=0.152, P<0.001) could predict the diseases control overall behavioral pattern among the studied hypertensive patients (Table 3).
Analysis of the study data based on the backward elimination modeling also revealed that perceived benefit (beta=0.372, P<0.001) and barriers to change behavior (beta=−0.138, P<0.001), situational influences (beta=0.269, P<0.001), and interpersonal influences (beta=−0.144, P<0.001) could predict the overall hypertension control behavioral pattern among the studied patients (P<0.05). The model explained 52.5% of the observed variance in the mean score of hypertension control (R2=0.525, P<0.001) among the study respondents (Table 4).
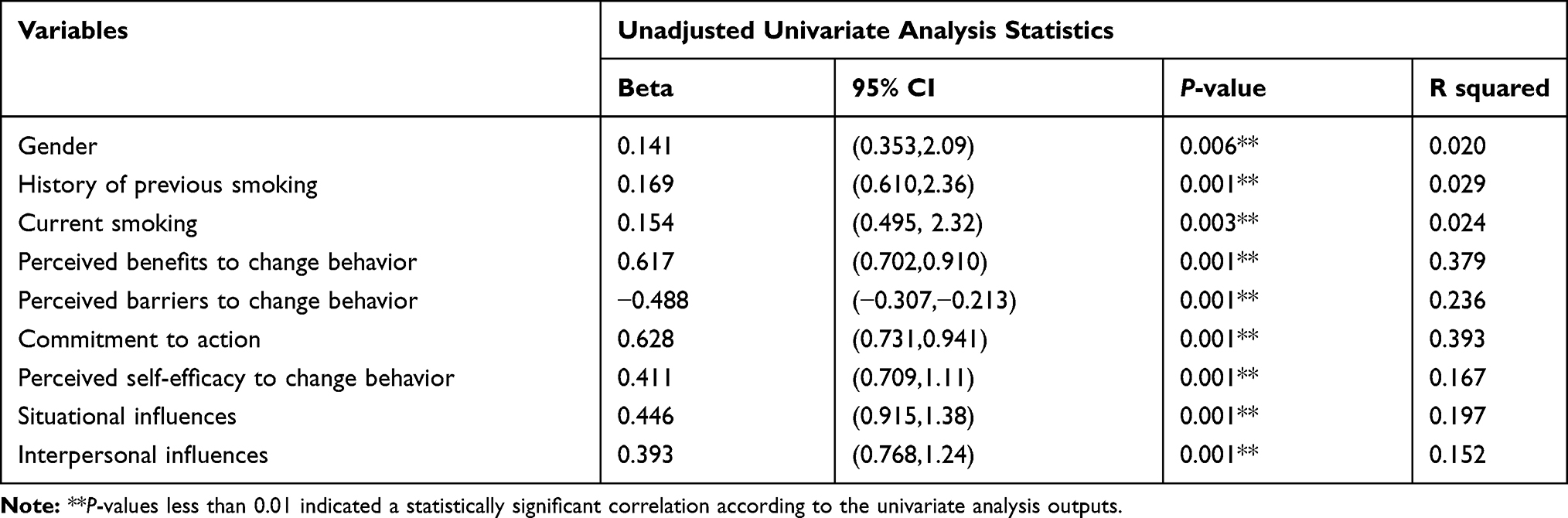 |
Table 3 Predictors of Hypertension Control Amongst the Studied Iranian Hypertensive Patients |
 |
Table 4 Main Determinants of Hypertension Control Amongst the Studied Iranian Patients |
Discussion
The main aim of this study was to envisage applicability of the Pender’s health promotion model for prediction of disease-specific control and management behaviors amongst the Iranian hypertensive patients. The study results showed that gender, history of smoking, and/or smoking status, perceived barriers and benefit, commitment to action, perceived self-efficacy, situational influences, and interpersonal influences are major predictors of diseases control behaviors among the studied hypertensive patients.
The study findings represented that the studied hypertensive Iranian women had more control over their blood pressure than their male counterparts. The result is in line with the observation in other studies on HBP patients.23 This might be related to the lower level of awareness or perceived severity and susceptibility to hypertension among this sub-group of populations. Intervention to enhance the perceived severity/susceptibility and benefit among hypertensive patients was indicated to improve the diseases control behavior among hypertensive patients.24 Women were also suggested to have an overall better health seeking profile than men in the conducted studies.25
A better disease control profile was observed in this study among those hypertensive patients that had no history of previous smoking or were not current smokers, which is consistent with the findings of the study of DeVore et al.26 However; a contrasting result was reported in other studies in relation to the association between smoking habit and blood pressure control among HBP patients.27 Perceived benefit in this study predicted 37.9% of the variance for diseases controls scores among hypertensive patients, which is in line with those of previous studies.28 One potential explanation for such a relation might be fear of the disease complications if no measure is taken and perceived self-efficacy for behavior change.
Perceived barriers predicted 23.6% of the variance in disease control scores and indicated a significant negative correlation with diseases control among the study participants. Association of perceived barriers with hypertension self-management behaviors was confirmed in other studies.29 It was suggested that patients with a low perception of barriers are more likely to adhere to their therapeutic plan or disease control protocols.30 Being knowledgeable about potential barriers of behavior change can help patients to find or seek solutions to overcome them. Therefore, one of the key aspects of intervention by HCPs for hypertensive patients could be provision of information about possible barriers to change and benefits of behavioral changes for a better self-care and disease self-management.
Our results showed that commitment to action is the main predictor of diseases control among hypertensive patients (R2=0.393). This finding is contrary to the findings of a previous study that suggested a reverse correlation between commitment to action and systolic blood pressure levels (SBP).31 This inconsistency may be attributed to differences in the socio-economic characteristics of the studied population samples or measurement divergences.
This study findings also showed that perceived benefit, perceived barriers, situational influences, and interpersonal influences could predict 52.2% variance of the hypertension control scores among the recruited patients. These results seem to be consistent with findings of another research which indicated that individual perceptions such as perceived sensitivity, perceived severity,32 perceived benefits, perceived barriers, guidance for action, and self-efficacy can be indispensable for behavior change among hypertensive patients.33
Limitations
Due to the small sample size and non-random nature of the participants’ recruitment, the obtained findings might not be generalizable to other HBP patients in Iran. Given that a sizable number of the study participants were recruited in the emergency department, the probability of responding bias warrants further scrutiny due to the possible interference of an incongruous interview space.
The relatively low literacy level of the recruited study attendees could also have caused imprecision and inaccuracy of the responses because of the respondents’ challenges, for instance in accurately recalling details pertaining to the hypertension control behaviors or misunderstanding questions, hence intentionally or unintentionally misrepresenting responses to the study questions.
The study results might also be misleading because of not correcting for some important baseline underpinning factors such as Glomerular Filtration Rate (GFR), glycemia, low-density lipoprotein (LDL) level, and previous myocardial infarction that were not measured in this study, mainly due to logistic restrains. As a consequence, the probability of recruitment of an unbalanced number of patients with a low or prominent performance profile of hypertension control and in consequence with a distinct profile of hypertension biomarkers or other baseline risk factors (selection bias) might not be ruled out completely.
The observed significant Pearson’s test statistic in conjunction with the weak correlation values in assessment of the relationship between the studied predicting and output variables might also represent homogeneity of the studied sample that allowed for little variance between individuals and the probability of false positive research findings. The other interpretation of the detected weak correlation might be the non-linear relationship between the studied variables that needs to be considered in future studies.
Conclusion
Successful hypertension control in patients with chronic morbidity needs to be based on sound data about major determinants of the relevant health/illness behaviors. Implementation of cogent interventions will be attainable in virtue of evidence-based knowledge that can be stipulated into mainstream health provision packages. Targeted model-based interventions are necessarily more explicit than the ad hoc change efforts in mitigating the output variables due to their inherent multidimensionality (ie, considering simultaneously in general the individual, social, built environment, and policy components), in that models pose a set of archetypal ingredients to support and guide patients-targeted optimal empowerment programs. The study findings revealed that the Pender’s health promotion model could be applicable as a theoretical framework to identify major determinants of adherence to hypertension control recommendations and, thus, planning tailor-made interventions to boost adherence to an antihypertensive regimented and monitored lifestyle for Iranian and probably other hypertensive patients. Situational and interpersonal influences along with perceived benefits and barriers were identified as preeminent determinants of adherence to the recommended therapeutic and lifestyle change in this study, but future cross-cultural validation of the study findings in more representative and larger sample sizes could add to the legitimacy of the evidence surrounding self-care practices in hypertensive patients.
Ethical Considerations
Approval for the study was obtained from the institutional level Medical Ethics Board of Trustees (MEBoT) within the Tabriz University of Medical Sciences (approval number: 5-4-3786-93-04-26).
Disclosure
The authors declare no conflicts of interests.
References
1. World Health Organization. A Global Brief on Hypertension: Silent Killer, Global Public Health Crisis: World Health Day 2013. World Health Organization; 2013.
2. World Health Organization. World Health Organization. (2009). Global Health Risks: Mortality and Burden of Disease Attributable to Selected Major Risks. Geneva; 2009.
3. Mills KT, Bundy JD, Kelly TN, et al. Global disparities of hypertension prevalence and controlclinical perspective: a systematic analysis of population-based studies from 90 countries. Circulation. 2016;134(6):441–450. doi:10.1161/circulationaha.115.018912
4. Aghaei Meybodi HR, Khashayar P, Rezai Homami M, Heshmat R, Larijani B. Prevalence of hypertension in an Iranian population. Ren Fail. 2014;36(1):87–91. doi:10.3109/0886022x.2013.832315
5. Sarki AM, Nduka CU, Stranges S, Kandala N-B, Uthman OA. Prevalence of hypertension in low- and middle-income countries: a systematic review and meta-analysis. Medicine. 2015;94:e1959–e. doi:10.1097/MD.0000000000001959
6. Vedanthan R, Bernabe-Ortiz A, Herasme OI, et al. Innovative approaches to hypertension control in low- and middle-income countries. Cardiol Clin. 2017;35:99–115. doi:10.1016/j.ccl.2016.08.010
7. Bokhour BG, Cohn ES, Cortés DE, et al. The role of patients’ explanatory models and daily-lived experience in hypertension self-management. J Gen Intern Med. 2012;27(12):1626–1634. doi:10.1007/s11606-012-2141-2
8. Warren-Findlow J, Seymour RB. Prevalence rates of hypertension self-care activities among African Americans. J Natl Med Assoc. 2011;103(6):503–512. doi:10.1016/s0027-9684(15)30365-5
9. Jarab A, Al Zabadi H, Hallak H, Khdour M, Al-Shahed Q, Mukattash T. Determinants of poor blood pressure control in hypertensive patients: findings from the baseline survey in west bank. Palestine. 2017.
10. Muleta S, Melaku T, Chelkeba L, Assefa D. Blood pressure control and its determinants among diabetes mellitus co-morbid hypertensive patients at Jimma University medical center, South West Ethiopia. Clin Hypertens. 2017;23(1):29. doi:10.1186/s40885-017-0085-x
11. Li YT, Wang HHX, Liu KQL, et al. Medication adherence and blood pressure control among hypertensive patients with coexisting long-term conditions in primary care settings: A cross-sectional analysis. Medicine. 2016;95:20. doi:10.1097/MD.0000000000003572
12. Ramli A, Ahmad NS, Paraidathathu T. Medication adherence among hypertensive patients of primary health clinics in Malaysia. Patient Prefer Adherence. 2012;6:613. doi:10.2147/PPA.S34704
13. Nguyen H, Odelola OA, Rangaswami J, Amanullah A. A review of nutritional factors in hypertension management. Int J Hypertens. 2013;2013. doi:10.1155/2013/698940
14. Schwingshackl L, Chaimani A, Hoffmann G, Schwedhelm C, Boeing H. Impact of different dietary approaches on blood pressure in hypertensive and prehypertensive patients: protocol for a systematic review and network meta-analysis. BMJ Open. 2017;7(4):e014736. doi:10.1136/bmjopen-2016-014736
15. Hegde SM, Solomon SD. Influence of physical activity on hypertension and cardiac structure and function. Curr Hypertens Rep. 2015;17(10):77. doi:10.1007/s11906-015-0588-3
16. Pescatello LS, MacDonald HV, Lamberti L, Johnson BT. Exercise for hypertension: a prescription update integrating existing recommendations with emerging research. Curr Hypertens Rep. 2015;17(11):87. doi:10.1007/s11906-015-0600-y
17. Nagele E, Jeitler K, Horvath K, et al. Clinical effectiveness of stress-reduction techniques in patients with hypertension: systematic review and meta-analysis. J Hypertens. 2014;32(10):1936–1944. doi:10.1097/HJH.0000000000000298
18. Ge Z, Hao Y, Cao J, et al. Does cigarette smoking exacerbate the effect of blood pressure on the risk of cardiovascular and all-cause mortality among hypertensive patients? J Hypertens. 2012;30(12):2307–2313. doi:10.1097/HJH.0b013e328359aa1f
19. Cappelletti ER, Greco A, Maloberti A, Giannattasio C, Steca P, D’Addario M. What hypertensive patients want to know [and from whom] about their disease: a two-year longitudinal study. BMC Public Health. 2020;20(1):308. doi:10.1186/s12889-020-8421-6
20. Holcomb K. Hypertension: Enhancing Lifestyle Management Through Patient Education and Pender’s Health Promotion Model. University of Massachusetts Amherst; 2017. Available from: https://scholarworks.umass.edu/cgi/viewcontent.cgi?article=1116&context=nursing_dnp_capstone. Accessed July 10, 2020.
21. Pender NJ. Health Promotion Model Manual. University of Michigan; 2011. Available from: https://deepblue.lib.umich.edu/bitstream/handle/2027.42/85350/HEALTH_PROMOTION_MANUAL_Rev_5-2011.pdf. Accessed July 10, 2020.
22. Hagerstrom GE. Personal factors, perceptions, influences and their relationship with adherence behaviors in patients with diabetes [dissertation]. Atlanta, GA: Georgia State University; 2010.
23. Heydari A, Khorashadizadeh F. Pender’s health promotion model in medical research. J Pak Med Assoc. 2014;64(9):1067–1074.
24. Chu SH, Baek JW, Kim ES, et al. Gender differences in hypertension control among older Korean adults: korean social life, health, and aging project. J Prev Med Public Heal. 2015;48(1):38. doi:10.3961/jpmph.14.043
25. Khorsandi M, Fekrizadeh Z, Roozbahani N. Investigation of the effect of education based on the health belief model on the adoption of hypertension-controlling behaviors in the elderly. Clin Interv Aging. 2017;12(233):eCollection 2017. doi:10.2147/CIA.S117142
26. DeVore AD, Sorrentino M, Arnsdorf MF, Ward RP, Bakris GL, Blankstein R. Predictors of hypertension control in a diverse general cardiology practice. J Clin Hypertens. 2010;12(8):570–577. doi:10.1111/j.1751-7176.2010.00298.x
27. Li G, Wang H, Wang K, et al. The association between smoking and blood pressure in men: a cross-sectional study. BMC Public Health. 2017;17(1):797. doi:10.1186/s12889-017-4802-x
28. Khodaveisi M, Fakhreazizi S, Mohammadi N, Tapak L. Assessment of knowledge, attitude and adherence to treatment in patients with heart disease in Iran. Int J Travel Med Global Health. 2019;7:142–146. doi:10.15171/ijtmgh.2019.29
29. Fix GM, Cohn ES, Solomon JL, et al. The role of comorbidities in patients' hypertension self-management. Chronic Illn. 2014;10(2):81–92. doi:10.1177/1742395313496591
30. Flynn SJ, Ameling JM, Hill-Briggs F, et al. Facilitators and barriers to hypertension self-management in urban African Americans: perspectives of patients and family members. Patient Prefer Adherence. 2013;7(741):eCollection 2013. doi:10.2147/PPA.S46517
31. Munro S, Lewin S, Swart T, Volmink J. A review of health behaviour theories: how useful are these for developing interventions to promote long-term medication adherence for TB and HIV/AIDS? BMC Public Health. 2007;7(1):104. doi:10.1186/1471-2458-7-104
32. Kamran A, Shekarchi A, Sharifirad G, Sharifian E, Shekarchi L. Evaluating dietary perceptions education program among rural hypertensive patients on commitment and adherence to healthy diet. J Hum Heal. 2015;1(1):7.
33. Larki A, Tahmasebi R, Reisi M. Factors predicting self-care behaviors among low health literacy hypertensive patients based on health belief model in bushehr district, South of Iran. Int J Hypertens. 2018;2018:eCollection 2018. doi:10.1155/2018/9752736
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.