Back to Journals » Journal of Pain Research » Volume 18
Predictive Factors of Acute Pain After Day Surgery: A Meta-Analysis
Received 9 May 2025
Accepted for publication 29 September 2025
Published 8 October 2025 Volume 2025:18 Pages 5249—5263
DOI https://doi.org/10.2147/JPR.S538046
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Karina Gritsenko
Hanqing Zhang,1,2 Xinglian Gao1
1Union Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, People’s Republic of China; 2School of Nursing, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, People’s Republic of China
Correspondence: Xinglian Gao, Union Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, 430000, People’s Republic of China, Email [email protected]
Objective: This study aims to provide evidence-based recommendations for optimizing postoperative pain management and enhancing recovery efficiency by identifying key predictors of acute postoperative pain in day surgery patients.
Background: As day surgery becomes more widespread, effective management of acute postoperative pain is crucial for successful recovery. A variety of studies have explored factors influencing postoperative acute pain. This study synthesizes existing evidence through a meta-analysis to clarify the primary predictors.
Methods: A comprehensive search was performed across multiple databases, including PubMed, CINAHL, Scopus, Web of Science, EMBASE, the Cochrane Library, and CNKI, to identify clinical studies examining factors associated with acute postoperative pain following day surgery. The search encompassed all relevant publications up to January 30, 2025. The systematic review and meta-analysis employed a fixed-effects model to analyze the data, with a random-effects model applied in cases of significant heterogeneity.
Results: Ten studies involving 11,865 patients were included. Significant predictors of acute postoperative pain, including: insufficient use of analgesics (OR = 2.12, P < 0.00001), age < 45 years (OR = 2.88, P < 0.00001), open surgery (OR = 5.05, P < 0.00001), education level ≤ middle school (OR = 2.06, P = 0.0001), preoperative fear and anxiety (OR = 2.18, P < 0.00001), higher preoperative pain expectation (OR = 1.74, P < 0.00001), and general anesthesia (OR = 1.91, P < 0.0001).
Conclusion: This study identified the main predictors of acute postoperative pain in day surgery, suggesting these factors should be incorporated into clinical assessments to optimize pain management and recovery. The main risk factors include analgesic usage, age, surgery type, education level, preoperative fear and anxiety, pain expectation, and anesthesia type. Effective preoperative management of these factors may reduce postoperative pain and enhance recovery.
Keywords: day surgery, predictive factors, meta-analysis, postoperative acute pain
Introduction
With the advancement of global medical technology and the innovation of health management models, day surgery has become an integral part of modern surgical practice. Its significant advantages include reduced patient hospitalization time, lower medical costs, decreased postoperative infection risk, and improved hospital bed utilization efficiency.1 However, the management of acute postoperative pain in day surgery remains a major challenge. Postoperative acute pain not only affects the quality of patient recovery and treatment outcomes but also contributes to higher medical costs.2,3 Therefore, assessing and managing the risk factors for postoperative acute pain is crucial in ensuring the safe and timely discharge of day surgery patients. Through risk prediction, healthcare providers can systematically identify and address various risk factors that may influence postoperative acute pain, such as patient age, anesthesia method, and surgery type.4,5 Given that day surgery patients need to be discharged early for recovery, the assessment and management of these risk factors are particularly important. If postoperative acute pain is not effectively controlled before discharge, it can result in various complications, prolong hospitalization, and potentially impair long-term recovery outcomes, creating both physical and psychological burdens.6,7
Despite existing studies exploring various risk factors for postoperative acute pain, their results often lack consistency. These discrepancies arise from differences in study design such as prospective versus retrospective approaches, patient population characteristics including age, comorbidities, and cultural factors, and analytical approaches like statistical models and pain assessment criteria.8,9 While some research indicates that older age may significantly contribute to the risk of acute postoperative pain in day surgery patients, other studies fail to find a significant association.10 Some studies have identified inadequate use of analgesics, limited educational attainment, and heightened preoperative fear and anxiety as notable risk factors. However, the extent to which these findings can be generalized across various surgical procedures and diverse patient populations remains insufficiently verified.11,12 We selected these specific risk factors for analysis because they are frequently reported, clinically modifiable, and relevant to perioperative care, unlike less actionable factors such as genetic or socioeconomic variables.
Therefore, This meta-analysis aims to comprehensively identify and assess the key risk factors that are significantly correlated with acute postoperative pain in the context of day surgery, clarifying the role of various predictive factors for postoperative acute pain in day surgery. The goal is to generate robust scientific evidence that will assist healthcare professionals in optimizing preoperative evaluations and postoperative pain management strategies and improve medical quality during predictive assessments and management, offering more efficient pain management for day surgery patients and enhancing their postoperative recovery quality, comfort, and satisfaction.
Methods
Registration ID
The protocol for this review has been registered in the International Prospective Register of Systematic Reviews (PROSPERO), with registration number CRD42024582981. This study adhered to the guidelines outlined in the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) statement, and the MOOSE (Meta-analysis of Observational Studies in Epidemiology) recommendations.
Search Strategy
Two authors conducted a comprehensive literature search using electronic databases to identify relevant studies. The search covered all records from the inception of each database up to January 30, 2025, focusing on literature that examined risk factors associated with postoperative acute pain in patients undergoing day surgery. The databases searched included PubMed, CINAHL, Scopus, Web of Science, Embase, the Cochrane Library, and CNKI. A combination of Medical Subject Headings (MeSH) and free-text terms was utilized to enhance the sensitivity of the search. The following keywords were used in various combinations: “Day surgery” OR “Ambulatory surgery” OR “Same-day surgery” OR “Day-case surgery” OR “Day case surgery” OR “Day operation” OR “Day-operation” OR “Day surgeries” OR “Day-surgery” AND “Postoperative pain” OR “Post-operative pain” OR “Acute pain after surgery” OR “Post-surgery pain” AND “Risk factors” OR “Predictors” OR “Determinants” OR “Risk assessment” OR “Risk prediction” OR “Predictive factors”. The search strategy was designed to be inclusive, with no limitations regarding study design, publication date, or geographic setting. However, only studies published in English were considered. Additionally, the reference lists of selected articles were manually screened to identify any further studies that met the inclusion criteria.
Inclusion and Exclusion Criteria
The inclusion criteria for this review were as follows: (1) Study Population: Patients undergoing day surgery; (2) Study Design: Cohort and cross-sectional studies that examine the risk factors associated with acute postoperative pain following day surgery; (3) Evaluation Metrics: Factors such as analgesic usage, age, surgery type, education level, preoperative fear and anxiety, expected pain from surgery, and anesthesia methods; (4) Data Availability: Studies that provided statistical data such as Odds Ratios (OR) and 95% Confidence Intervals (CI). Exclusion criteria included: (1) Study Design: Basic clinical research, editorials, animal studies, literature reviews, case reports, reprinted articles, and conference abstracts; (2) Content Issues: Studies with incomplete or unavailable data, statistical inaccuracies, results with errors that could lead to invalid references, or duplicate publications; (3) Access Issues: Studies that could not be accessed.
Data Extraction and Collection
In line with the established inclusion and exclusion criteria, the two authors initially screened 27,275 articles. These were organized using EndNote 21 software, after which titles were reviewed, and duplicates removed. The authors independently examined the titles, abstracts, and full texts of the remaining articles to extract relevant data. A third independent author verified the accuracy of the data extraction process. In instances where discrepancies arose, the senior author made the final decision. The following data were extracted from each included study: basic details (first author, publication year, study country), study design (type of study, sample size, inclusion/exclusion criteria), patient demographics (age, gender), surgical and anesthesia-related information (surgery type, surgery duration, anesthesia method), and factors influencing postoperative acute pain (such as analgesic usage, age, type of surgery, educational background, preoperative anxiety/fear, anticipated postoperative pain, and anesthesia type). Furthermore, where available, adjusted Odds Ratios (OR) and their 95% Confidence Intervals (CI) from multivariable regression analyses were recorded, alongside the variables included in these models. To resolve any ambiguities or missing data, the authors contacted the corresponding authors of the original studies. In total, 10 articles were ultimately included in the analysis.
Quality Assessment
The quality evaluation of the included studies was conducted independently by two authors. For cross-sectional studies, the Joanna Briggs Institute (JBI) Critical Appraisal Checklist was used, which includes eight questions: (1) Inclusion criteria, (2) Study population and setting, (3) Measurement of exposure, (4) Measurement of outcomes, (5) Measurement of study conditions, (6) Identification of confounding factors, (7) Strategies for handling confounding factors, (8) Statistical analysis methods. Each question has four options: Yes (Y), No (N), Unclear (U), Not Applicable (N/A). For cohort studies, the Newcastle-Ottawa Scale (NOS) was employed, which evaluates studies across three domains: (1) Selection bias (four items), (2) Comparability (one item), and (3) Outcome assessment (three items). The comparability domain could receive up to 2 points, while each remaining item was worth 1 point, yielding a maximum possible score of 9. Based on standardized cut-offs, studies were categorized as low quality (0–3 points), moderate quality (4–5 points), or high quality (6–9 points). Disagreement between the two authors were resolved through discussion, and when necessary, a third author was consulted to reach a consensus.
Data Analysis
The meta-analysis was performed using Review Manager (RevMan), version 5.4, developed by the Cochrane Collaboration. For continuous outcomes, either the mean difference (MD) or standardized mean difference (SMD) was selected as the primary effect size metric. In the case of dichotomous outcomes, the analysis employed odds ratios (OR) or risk ratios (RR), along with the corresponding 95% confidence intervals (CIs). To evaluate the degree of variability across studies, heterogeneity was assessed using the I² statistic. An I² value exceeding 50% suggested significant heterogeneity, prompting further subgroup and sensitivity analyses to explore potential sources and adoption of a random-effects model (REM) to account for between-study variability. Conversely, if I² was less than 50%, heterogeneity was considered low, and a fixed-effect model (FEM) was adopted for statistical synthesis. A p-value of less than 0.05 was regarded as indicative of a statistically significant result.
Results
Literature Screening
Based on the predefined search strategy, a total of 27,275 articles were initially identified. After a thorough screening and evaluation process, 1538 articles met the inclusion criteria and were ultimately retained for further analysis. After carefully reviewing the titles and abstracts, inclusion and exclusion criteria were applied. Upon full-text review, a total of 10 articles were ultimately included in the analysis.3,13–21 The screening process is shown in Figure 1.
 |
Figure 1 Flowchart of Literature Screening Process. |
Basic Characteristics of Included Studies
This meta-analysis encompassed 10 studies published between 2002 and 2022, involving a combined total of 11,865 participants. Among these studies, six were designed as cohort studies, while the remainder employed a cross-sectional methodology. Among all included studies, 4 articles reported the amount of analgesic usage,13,14,16,19 5 articles reported age,3,15–17,20 4 articles reported surgical types,14,16,19,21 3 articles reported education level,14–16 5 articles reported preoperative fear and anxiety,3,15,16,18,19 5 articles reported expected postoperative pain,3,15,16,18,19 and 3 articles reported anesthesia methods.3,14,15 The characteristics of the included studies are shown in Table 1.
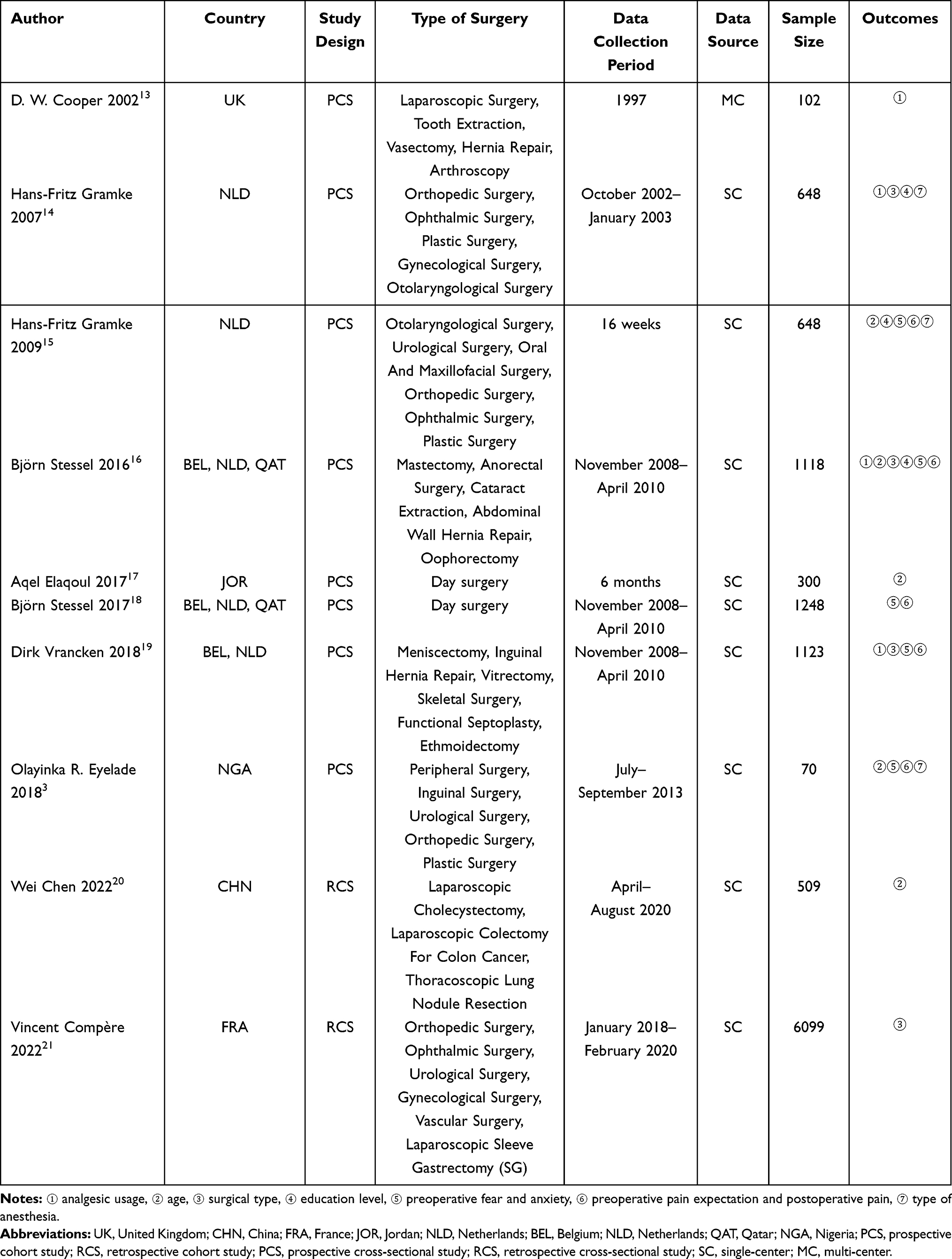 |
Table 1 Basic Characteristics of Included Studies |
Quality Assessment of the Studies
Our analysis included 8 PCSs3,13–19 and 2 RCCs.20,21 The evaluation method was changed to JBI assessment and NOS scoring. The evaluation results are shown in Tables 2 and 3.
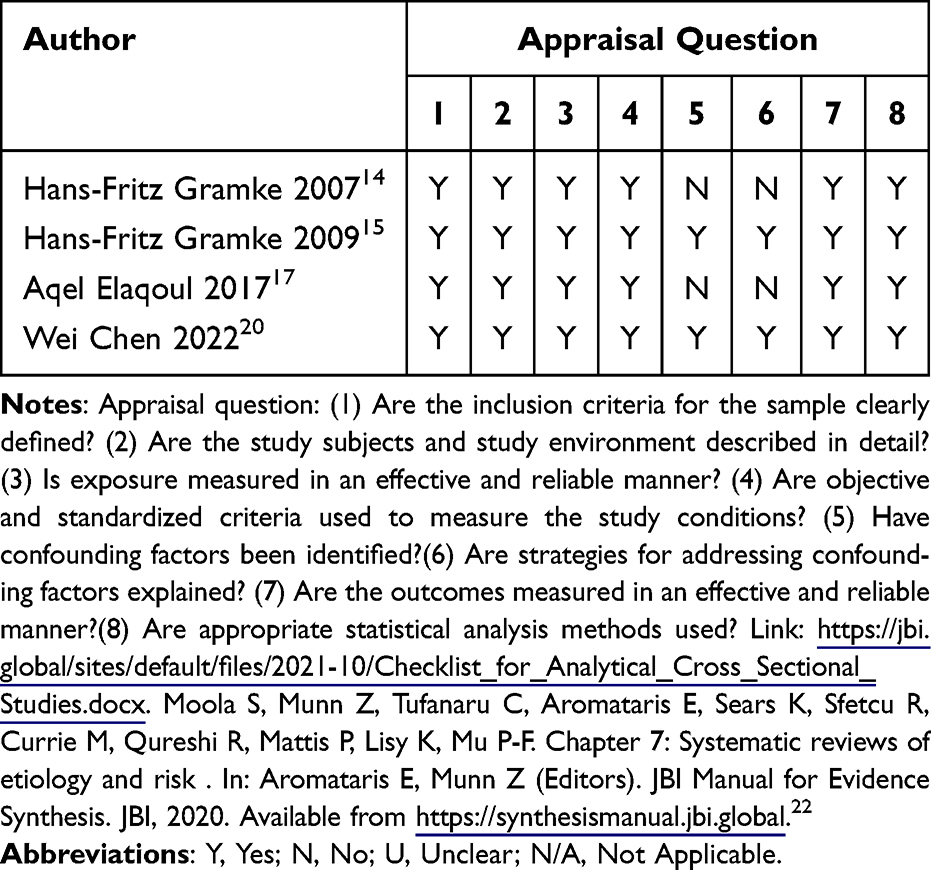 |
Table 2 Quality Appraisal |
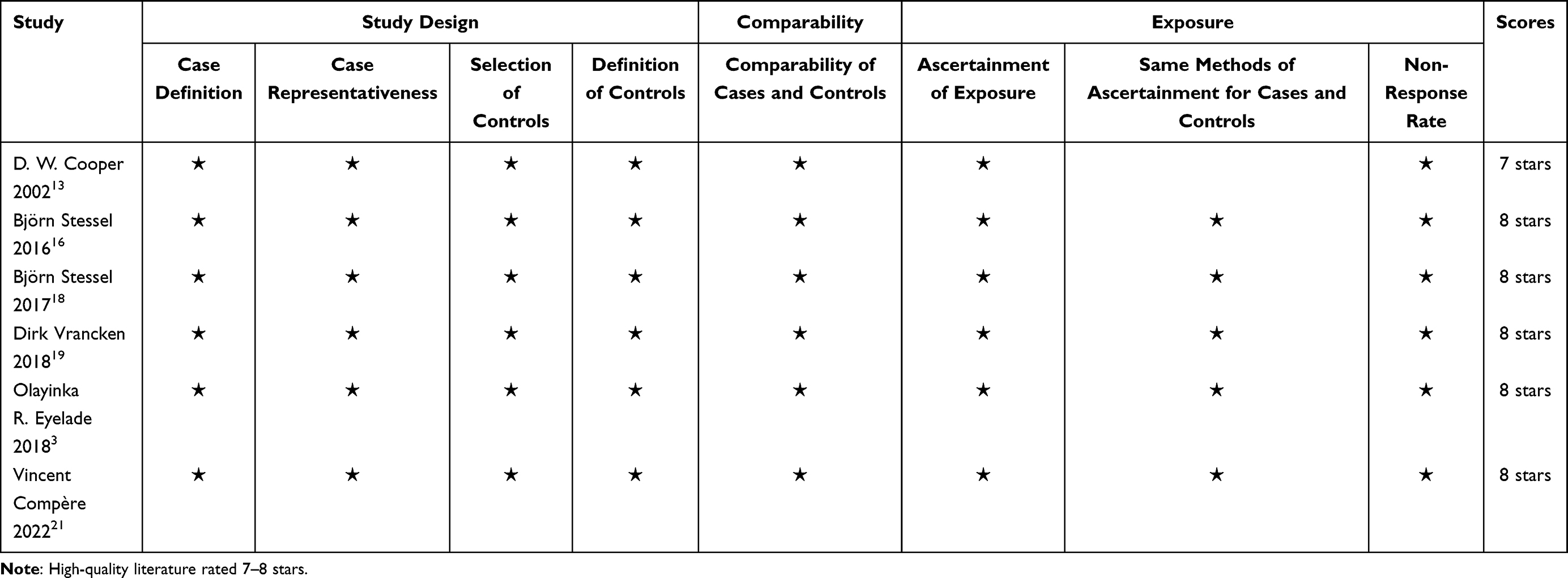 |
Table 3 NOS Scores |
Meta-Analysis
This meta-analysis summarizes the key risk factors and their statistical results in this study, including OR, 95% CI, p-value, and I². These factors showed significant statistical and clinical relevance in postoperative acute pain, as shown in Table 4.
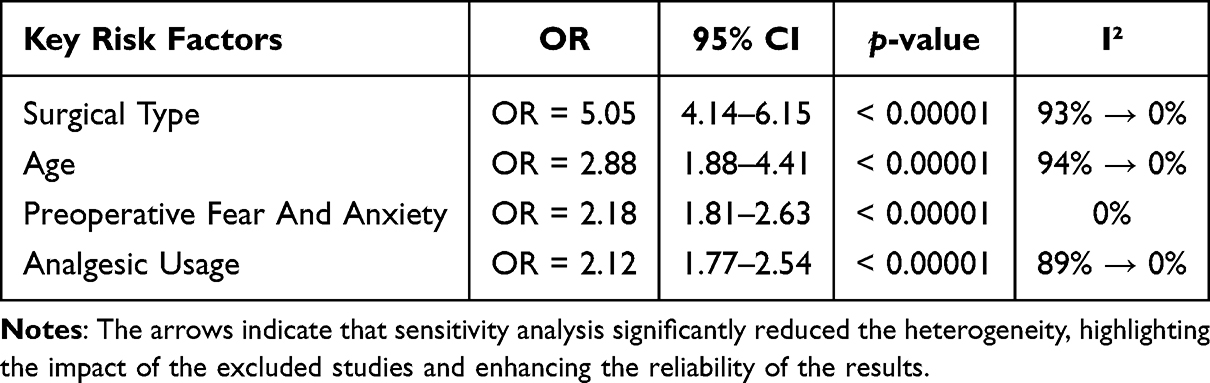 |
Table 4 Key Risk Factors |
Four articles provided data on analgesic usage.13,14,16,19 The meta-analysis indicated a substantial degree of heterogeneity among the included studies, with an I² value of 89%. Sensitivity analysis revealed that the exclusion of one study led to a marked reduction in heterogeneity, bringing the I² down to 0%. Employing the fixed-effects model (FEM), it was found that the difference in analgesic usage between the group without postoperative acute pain and the group with postoperative acute pain was statistically significant (OR = 2.12, 95% CI: 1.77–2.54, P < 0.00001), as illustrated in Figure 2.
 |
Figure 2 Forest plot of analgesic usage. |
Five articles provided data on age.3,15–17,20 The meta-analysis indicated substantial heterogeneity among the included studies, as evidenced by an I² value of 94%. Sensitivity analysis demonstrated that removing three studies led to a marked reduction in heterogeneity between the two groups, with the I² value dropping to 0%. Employing the fixed-effects model (FEM), it was found that there was a significant difference in age between the group without postoperative acute pain and the group with postoperative acute pain (OR = 2.88, 95% CI: 1.88–4.41, P < 0.00001), as illustrated in Figure 3.
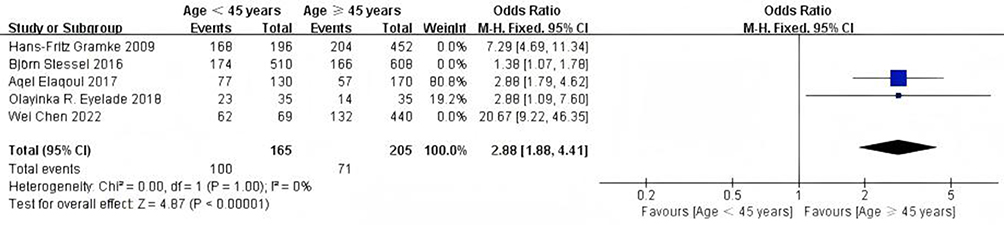 |
Figure 3 Forest plot of age. |
Four articles provided data on surgical type.14,16,19,21 The meta-analysis revealed substantial heterogeneity among the studies, with an I² value of 93%. Sensitivity analysis indicated that removing two studies significantly reduced the heterogeneity between the two groups, bringing the I² value down to 0%. Employing the fixed-effects model (FEM), it was found that there was a significant difference in surgical type between the group without postoperative acute pain and the group with postoperative acute pain (OR = 5.05, 95% CI: 4.14–6.15, P < 0.00001), as illustrated in Figure 4.
 |
Figure 4 Forest plot of surgical type. |
Three articles provided data on education level.14–16 The meta-analysis showed high heterogeneity between the studies (I² = 88%). Sensitivity analysis revealed that after excluding one study, the heterogeneity between the two groups decreased (I² = 61%). Employing the random-effects model (REM), the analysis revealed a statistically significant association between patients’ educational attainment and the incidence of postoperative acute pain. Specifically, individuals without acute postoperative pain were more likely to have a higher level of education compared to those who experienced such pain (OR = 2.06, 95% CI: 1.42–2.99, P = 0.0001), as illustrated in Figure 5.
 |
Figure 5 Forest plot of education level. |
Five studies reported data on preoperative fear and anxiety.3,15,16,18,19 The meta-analysis showed low heterogeneity between the studies (I² = 0%). Employing the fixed-effects model (FEM), the results indicated that there was a significant difference in preoperative fear and anxiety between the group without postoperative acute pain and the group with postoperative acute pain (OR = 2.18, 95% CI: 1.81–2.63, P < 0.00001), as illustrated in Figure 6.
 |
Figure 6 Forest plot of preoperative fear and anxiety. |
Five articles provided data on the comparison between preoperative pain expectation and postoperative pain.3,15,16,18,19 The meta-analysis showed low heterogeneity between the studies (I² = 27%). Using the fixed-effects model (FEM), it was found that there was a significant difference in the comparison of preoperative pain expectation and postoperative pain between the group without postoperative acute pain and the group with postoperative acute pain (OR = 1.74, 95% CI: 1.51–2.00, P < 0.00001), as illustrated in Figure 7.
 |
Figure 7 Forest plot comparing preoperative pain expectation and postoperative pain. |
Three articles provided data on anesthesia type.3,14,15 This meta-analysis showed substantial heterogeneity between these studies (I² = 94%). Sensitivity analysis showed that excluding one study markedly reduced heterogeneity, bringing the I² down to 0%. Employing the fixed-effects model (FEM), the results indicated that there was a significant difference in anesthesia type between the group without postoperative acute pain and the group with postoperative acute pain (OR = 1.91, 95% CI: 1.38–2.65, P < 0.0001), as illustrated in Figure 8.
 |
Figure 8 Forest plot of anesthesia type. |
In the meta-analysis, certain factors exhibited high heterogeneity. After sensitivity analysis and excluding some studies, the heterogeneity significantly decreased. To explain the reduction in heterogeneity, a summary of the excluded studies, including the authors, the specific reasons for exclusion, and the consequent effects on the overall analysis, as illustrated in Table 5.
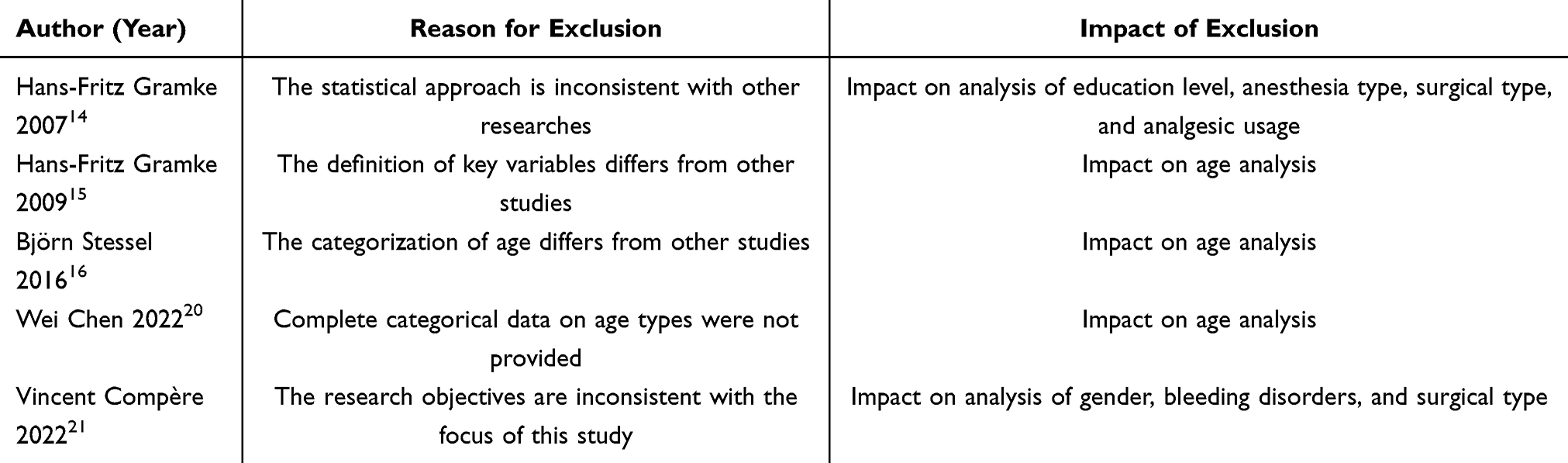 |
Table 5 Excluded Studies and Their Impact |
Discussion
This study conducted a meta-analysis to systematically assess the key predictive factors that influence acute postoperative pain following day surgery. The objective was to offer more robust evidence-based guidance for improving pain management and recovery in clinical settings. With continuous advancements in medical technology, day surgery has increasingly become an integral component of modern surgical practice due to its significant advantages in shortening hospital stays, reducing medical costs, and minimizing the risk of hospital-acquired infections.1 The widespread adoption of this model alleviates patients’ financial burden, enhances healthcare resource utilization and provides a more convenient treatment experience.23,24 However, the management of acute postoperative pain remains a key challenge affecting recovery and overall treatment outcomes in day surgery settings.25 Acute pain after surgery can hinder the recovery process, increase healthcare expenses, and adversely affect the patient’s surgical experience and quality of life.26 Therefore, identifying predictive factors associated with postoperative acute pain is of critical importance. By thoroughly analyzing these influencing factors, healthcare teams can implement more targeted analgesic strategies during the preoperative, intraoperative, and postoperative phases. Such targeted management can increase surgical success rates, improve postoperative recovery quality, minimize patients’ pain perception, enhance overall satisfaction, and ultimately optimize patient recovery outcomes.27,28
The study found that inadequate use of analgesics, patient age, open surgical procedures, lower education level, preoperative fear and anxiety, higher preoperative pain expectation compared to actual postoperative pain, and type of anesthesia are important factors influencing the occurrence of acute postoperative pain. Through a detailed evaluation of predictive factors, this study seeks to offer more effective clinical guidance, optimize postoperative pain management strategies, and support healthcare providers in making evidence-based decisions during preoperative assessments to reduce the incidence of acute postoperative pain in patients.
In sensitivity analyses addressing high heterogeneity (as detailed in Table 5), studies were excluded primarily due to inconsistent statistical methods, differing categorizations, or mismatched objectives. For instance, Hans-Fritz Gramke (2007 and 2009) were excluded for inconsistent statistical approaches, impacting analyses of education level, anesthesia type, surgical type, and analgesic usage, their removal reduced discrepancies and improved methodological alignment among remaining studies. Björn Stessel (2016) was omitted for differing age categorizations, allowing a more homogeneous dataset for age-related predictions. These exclusions reduced I² values, resulting in more reliable pooled estimates and strengthening the interpretability of our results without altering the overall evidence base.
Inadequate analgesia presents a significant risk for the occurrence of acute postoperative pain (OR = 2.12, 95% CI: 1.77–2.54). This conclusion aligns with existing literature, further confirming the critical role of perioperative pain management in preventing acute postoperative pain in patients.29 Studies indicate that insufficient analgesics increase pain incidence, intensity, and duration, related to medication type, dosage, timing, and patient differences.30 Therefore, it is essential in clinical practice to ensure that patients receive timely, adequate, and appropriate analgesic medications in the early postoperative period. Early pain control not only alleviates patient suffering but also effectively prevents the vicious cycle of pain, reducing anxiety and discomfort caused by worsening pain.31 Additionally, tailoring pain management based on patient condition and surgical type can reduce postoperative pain and prevent complications like chronic pain.32,33
Younger patients (under 45 years old) face a significantly higher risk of developing acute postoperative pain (OR = 2.88, 95% CI: 1.88–4.41). This phenomenon is likely closely related to multiple factors, including higher pain sensitivity, faster physiological metabolism, psychological factors, and social and cultural influences in younger patients.34,35 Younger individuals often have stronger central nervous system responsiveness and lower pain tolerance, exacerbated by high-stress states and higher pain expectations.36,37 Therefore, when assessing younger patients, physicians should not only consider their pain management needs and ensure the adequacy and timeliness of postoperative analgesia but also address the psychological aspects of pain perception. Furthermore, clinical practice should incorporate individualized pain management plans tailored to the needs of younger patients. Early postoperative pain intervention, appropriate management of pain expectations, and enhanced psychological support can help alleviate the impact of postoperative pain and optimize recovery quality for these patients as demonstrated by Tsui et al.38
Compared to minimally invasive procedures, patients who undergo open surgery are at a markedly increased risk of experiencing acute postoperative pain (OR = 5.05, 95% CI: 4.14–6.15). This indicates that the invasiveness of the surgery plays a critical role in the mechanisms underlying postoperative pain. Open surgery typically involves larger incisions, more tissue manipulation, and greater tissue damage, often accompanied by significant soft tissue destruction and inflammatory responses. This not only increases the risk of intraoperative bleeding but also leads to larger surgical wounds, exacerbating postoperative pain and complicating the recovery process, resulting in more intense and prolonged postoperative pain.39,40
For patients undergoing open surgery, in addition to pharmacological pain control in the early postoperative period, a comprehensive pain management strategy should be employed. This may include physical therapy, nerve blocks, and multimodal analgesia techniques such as analgesic pumps, to reduce pain perception and prevent the progression to chronic pain.41 Therefore, personalized pain management plans, including preoperative preparation and intraoperative monitoring, are crucial for rapid pain relief and improved recovery.33
Patients with lower education levels demonstrate a higher risk of developing acute postoperative pain (OR = 2.06, 95% CI: 1.42–2.99). These patients often lack sufficient knowledge about pain management, leading to increased anxiety and fear when facing postoperative pain, which in turn heightens their sensitivity to pain.42,43 Lower education correlates with more intense pain perception due to misconceptions and lack of confidence in pain management.44 Therefore, in clinical practice, it is important not only to develop pain management plans for these patients but also to focus on their preoperative education and psychological intervention. Various forms of preoperative education should be utilized, simplifying language and incorporating visual aids or video materials, to help patients understand the importance of postoperative pain management. This can assist in correcting misconceptions about the surgical process and pain management, effectively alleviating their fear and anxiety.45 At the same time, healthcare providers should offer personalized pain management guidance tailored to the patients’ cognitive levels and employ psychological interventions such as cognitive-behavioral therapy (CBT) for emotional support and psychological counseling.44 Building trust through communication can reduce anxiety, enhance compliance, and lower pain perception.46,47
Preoperative fear and anxiety are significant factors influencing the occurrence of acute postoperative pain (OR = 2.18, 95% CI: 1.81–2.63). Studies have shown that patients with preoperative fear and anxiety tend to be more sensitive to pain, which is closely related to their psychological state, fear of surgery, and expectations for postoperative recovery.48 These emotions trigger physiological responses that amplify pain and reduce tolerance.49,50 Healthcare providers can help patients manage these symptoms by incorporating preoperative training, such as deep breathing techniques, meditation, or progressive muscle relaxation, to alleviate physical tension and reduce postoperative pain perception.51 Cognitive-behavioral therapy (CBT) can also be used to alter patients’ cognitive patterns about surgery and pain, helping them cope with surgical pain in a healthier and more constructive manner.52 Preoperative assessment and emotional support can alleviate anxiety and promote better recovery.53
Patients who anticipate experiencing more pain before surgery than they actually feel afterward are significantly more prone to acute postoperative pain (OR = 1.74, 95% CI: 1.51–2.00). A patient’s expectation of pain largely influences their pain perception. Studies have shown that the higher the preoperative expectation of pain, the more sensitive patients are to pain postoperatively.54 Pain expectations, shaped by understanding and past experiences, can burden recovery if overly high.55,56 Furthermore, doctors should emphasize the effectiveness and safety of early postoperative pain management to patients. Through positive guidance, patients should be helped to establish realistic pain expectations and understand the pain management methods available, ensuring they have a clear understanding of the actual postoperative pain experience. This not only enhances treatment compliance but also reduces emotional fluctuations caused by pain.57 Thus, managing expectations through education is key to reducing pain risk and optimizing recovery.
Anesthesia type is a significant factor influencing acute postoperative pain. Research indicates that individuals receiving general anesthesia are at a notably increased risk of experiencing acute postoperative pain when compared to those who undergo regional or local anesthesia (OR = 1.91, 95% CI: 1.38–2.65). General anesthesia often results in delayed onset of postoperative analgesia, and the metabolism and clearance of anesthetic drugs can be slower, causing patients to experience more noticeable acute pain in the early postoperative period.58 General anesthesia may alter pain thresholds and intensify perception.59
In contrast, regional or local anesthesia typically provides better postoperative pain relief and shortens recovery time.60,61 Regional anesthesia works by blocking pain transmission in specific nerves using local anesthetics, offering effective pain control during surgery and continued analgesia postoperatively. This not only reduces the occurrence of acute postoperative pain but also helps patients recover their mobility more quickly.62 Local anesthesia avoids side effects like nausea from general anesthesia, especially for minor surgeries.63 However, when considering the type of anesthesia, physicians should tailor the choice based on the patient’s overall health status, the nature of the surgical procedure, and the anticipated requirements for postoperative recovery.59 For elderly patients or high-risk individuals with chronic diseases, regional or local anesthesia is often the preferred choice, as it provides effective pain relief while minimizing systemic side effects associated with general anesthesia.64 On the other hand, general anesthesia remains necessary for complex surgeries involving multiple anatomical areas.65 Combining techniques can enhance pain relief.63 In conclusion, the choice of anesthesia should be based on individualized patient assessment, taking into account pain management goals and recovery needs. Ensuring the rationality and effectiveness of the anesthesia plan is crucial for achieving optimal pain control and the shortest recovery time.66
In summary, this meta-analysis identified that patients with inadequate analgesia, those under 45 years of age, patients with preoperative fear and anxiety, individuals undergoing open surgery, and those receiving general anesthesia are all at high risk for developing acute postoperative pain and should be given special attention. For these high-risk groups, a comprehensive preoperative assessment should be conducted, taking into account factors such as age, anxiety levels, type of anesthesia, and surgical approach, to develop individualized pain management plans. Additionally, postoperative follow-up should be strengthened—especially for high-risk patients—through regular pain assessments and timely interventions to ensure they receive adequate pain relief throughout the recovery process.
Limitations of the Study
Some of the included studies exhibited considerable heterogeneity in terms of design, sample size, data quality, and research methodology, which may limit the generalizability of the results. Future research should further explore differences in surgical type, anesthesia methods, patient characteristics, and postoperative management. Although this study conducted an in-depth analysis of clinical variables such as age, surgical type, and anesthesia method on postoperative pain, it did not sufficiently examine the potential impact of social factors—such as levels of social and familial support—on postoperative pain. These social factors also play a critical role in pain perception and recovery. Moreover, future studies should focus on large-scale, multicenter, prospective research using multivariable regression analyses to clarify the independent effects and interactions among biological, psychological, and social risk factors. This would help refine pain management systems and provide patients with more precise and effective perioperative pain relief strategies.
Conclusions
This study systematically evaluated multiple risk factors influencing acute postoperative pain following day surgery and identified that inadequate analgesic use, age <45 years, open surgery, anesthesia type, lower education level, preoperative fear and anxiety, and higher preoperative pain expectations compared to actual postoperative pain are closely related to acute postoperative pain in patients.
Abbreviations
OR, Odds Ratio; CI, Confidence Interval; P, Significance Probability.
Acknowledgments
The author are grateful for the guidance from the corresponding author.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Jiang L, Houston R, Li C, et al. Day surgery program at west China hospital: exploring the initial experience. Cureus. 2020;12(7):e8961. doi:10.7759/cureus.8961
2. Keast M, Hutchinson A, Khaw D, McDonall J. Impact of pain on postoperative recovery and participation in care following knee arthroplasty surgery: a qualitative descriptive study. Pain Manag Nursing. 2021;23(4):541–547. doi:10.1016/j.pmn.2021.11.011
3. Salaudeen GO, Afuwape OO, Eyelade OR, Olapade-Olaopa EO. Effectiveness of postoperative analgesia in the management of acute pain in day-case surgeries. Ann African Med. 2018;17(3):140–144. doi:10.4103/aam.aam_53_17
4. Bekele Z, Ayana M, Haile M, Tesfaye A, Tasew A. Incidence and predictors of postoperative severe acute pain within 24 hours after cesarean section performed under spinal anesthesia at public hospitals in West Shoa, Ethiopia, 2022 prospective cohort study. Ann Med Surg. 2023;85(9):4239–4247. doi:10.1097/MS9.0000000000001031
5. Zhang H, Yang Y, Jiang L, Xu X, Zhang J, Zhang L. Predicting risk factors for acute pain after hepatobiliary and pancreatic surgery: an observational case control study. BMJ Open. 2024;14(8):e078048. doi:10.1136/bmjopen-2023-078048
6. Chen D, Zhang Y, Liu J, Chen Y. Postoperative acute pain trajectory and chronic postsurgical pain after abdominal surgery: a prospective cohort study and mediation analysis. Int J Surg. 2025;111(2):1968–1976. doi:10.1097/JS9.0000000000002218
7. McNaughton MA, Quinlan-Colwell A, Lyons MT, Arkin LC. Acute perioperative pain management of the orthopaedic patient: guidance for operationalizing evidence into practice. Orthop Nurs. 2024;43(1):10–22. doi:10.1097/nor.0000000000000998
8. Chow C, Yu C, Yu W, Yeung K, Schmidt L, Buckley N. Risk and protective factors in predicting pediatric acute postsurgical pain: a systematic review and meta-analysis. Health Psychol. 2023;42(10):723–734. doi:10.1037/hea0001293
9. Liu Q-R, Dai Y-C, Ji M-H, Liu P-M, Dong -Y-Y, Yang J. Risk factors for acute postsurgical pain: a narrative review. J Pain Res. 2024;17:1793–1804. doi:10.2147/JPR.S462112
10. Admiraal M, Van Zuylen M, Hermanns H, et al. The effect of preoperative disability, cognitive impairment, frailty and opioid use on acute postoperative pain in older patients undergoing surgery A prospective cohort study. J Pain. 2023;24(10):1886–1895. doi:10.1016/j.jpain.2023.05.013
11. Aliyev D, Asik I. Postoperative chronic pain syndrome and risk factors in patients with breast surgery. J College Physicians Surg--Pakistan. 2023;33(6):609–615. doi:10.29271/jcpsp.2023.06.609
12. Oh J, Lee W, Ki S, Suh J, Hwang S, Lee J. Assessment of preoperative anxiety and influencing factors in patients undergoing elective surgery: an observational cross-sectional study. Medicina. 2024;60(3):403. doi:10.3390/medicina60030403
13. Cooper DW, Garcia E, Mowbray P, Millar MA. Patient-controlled epidural fentanyl following spinal fentanyl at Caesarean section. Anaesthesia. 2002;57(3):266–270. doi:10.1046/j.1365-2044.2002.2366_1.x
14. Gramke HF, de Rijke JM, van Kleef M, et al. The prevalence of postoperative pain in a cross-sectional group of patients after day-case surgery in a university hospital. Clin J Pain. 2007;23(6):543–548. doi:10.1097/AJP.0b013e318074c970
15. Gramke HF, de Rijke JM, van Kleef M, et al. Predictive factors of postoperative pain after day-case surgery. Clin J Pain. 2009;25(6):455–460. doi:10.1097/AJP.0b013e31819a6e34
16. Stessel B, Fiddelers AA, Marcus MA, et al. External validation and modification of a predictive model for acute postsurgical pain at home after day surgery. Clin J Pain. 2017;33(5):405–413. doi:10.1097/ajp.0000000000000413
17. Elaqoul A, Obaid A, Yaqup E, et al. Postoperative pain among patients after day-case surgery. Plast Surg Nurs. 2017;37(4):130–136. doi:10.1097/psn.0000000000000206
18. Stessel B, Theunissen M, Marcus MA, et al. Prevalence and predictors of patient nonadherence to pharmacological acute pain therapy at home after day surgery: a prospective cohort study. Pain Pract. 2018;18(2):194–204. doi:10.1111/papr.12589
19. Vrancken D, Theunissen M, Joosten EA, et al. Procedure-specific pain intensity four days after day surgery and the relationship with preoperative pain: a prospective cohort study. Anesth Pain Med. 2018;8(6):e81366. doi:10.5812/aapm.81366
20. Chen W, Huang M, Dai Y. Analysis of the influencing factors of postoperative pain in day surgery patients under multimodal pain management. West China Med J. 2022;37(2):208–213. doi:10.7507/1002-0179.202012272
21. Compère V, Mauger A, Allard E, Clavier T, Selim J, Besnier E. Incidence of postoperative pain at 7 days after day surgery reported using a text messaging platform: retrospective observational study. JMIR Perioper Med. 2022;5(1):e33276. doi:10.2196/33276
22. Moola S, Munn Z, Tufanaru C, et al. Chapter 7: Systematic reviews of etiology and risk. In: Aromataris E, Munn Z, Editors. JBI Manual for Evidence Synthesis. JBI; 2020. Available from: https://synthesismanual.jbi.global.
23. Sah M, Bhattarai A. Day care laparoscopic cholecystectomy: a review. Scholars J Med Case Reports. 2024;12(3):292–297. doi:10.36347/sjmcr.2024.v12i03.015
24. Peng J, Zhao J, Cao D. Analysis of day surgery implementation in a large public hospital from the perspective of high-quality development. Hospital Administration Med Pract. 2024;3(2):1–6. doi:10.54844/hamp.2024.0050
25. Hah J, Cramer E, Hilmoe H, et al. Factors associated with acute pain estimation, postoperative pain resolution, opioid cessation, and recovery. JAMA Network Open. 2019;2(3):e190168. doi:10.1001/jamanetworkopen.2019.0168
26. Belay M, Yirdaw LT. Management of postoperative pain among health professionals working in governmental hospitals in South Wollo Zone, Northeast Ethiopia. Prospective cross sectional study. Ann Med Surg. 2022;80:104148. doi:10.1016/j.amsu.2022.104148
27. Kehlet H. Prediction of postoperative pain: are we missing the target? Anaesthesia. 2023;78(10):1301–1302. doi:10.1111/anae.16063
28. Armstrong R, Fayaz A, Manning G, et al. Predicting severe pain after major surgery: a secondary analysis of the Peri-operative quality improvement programme (PQIP) dataset. Anaesthesia. 2023;78(7):840–852. doi:10.1111/anae.15984
29. Coppes O, Yong R, Kaye A, Urman R. Patient and surgery-related predictors of acute postoperative pain. Curr Pain Headache Reports. 2020;24(4):12. doi:10.1007/s11916-020-0844-3
30. Heidari R, Najafzadeh M, Erfaniyan R, Razmpa E, Emami H, Heidari M. Evaluation of effective factors on pain in patients undergoing sleep apnea surgery. J Contemp Med Sci. 2022;8(1):47–50. doi:10.22317/jcms.v8i1.1095
31. Yu L, Zhang X, Jiang F, et al. Development and validation of nomograms to predict preoperative anxiety and postoperative pain in patients undergoing gynecological surgery: an observational analysis. J Affective Disord. 2023;15(339):227–236. doi:10.1016/j.jad.2023.07.058
32. Ishida Y, Okada T, Kobayashi T, Funatsu K, Uchino H. Pain management of acute and chronic postoperative pain. Cureus. 2022;14(4):e23999. doi:10.7759/cureus.23999
33. Kim Y-D. Association between postoperative pain management and long-term patient outcomes. J Korean Med Assoc. 2025;68(1):6–8. doi:10.5124/jkma.2025.68.1.6
34. Andreoletti H, Dereu D, Combescure C, Rehberg B. A systematic review and meta-analysis of three risk factors for chronic postsurgical pain: age, sex and preoperative pain. Minerva anestesiologica. 2022;88(10):827–841. doi:10.23736/S0375-9393.22.16489-8
35. Yang M, Riva‐Cambrin J. Prediction tools for postoperative pain. Pain Reports. 2021;6(1):e875. doi:10.1097/PR9.0000000000000875
36. Agnew J, Roy A, Hammer S, Strale F. Pain sensitivity increases more in younger runners during an ultra-marathon. Scandinavian J Pain. 2021;21(2):364–371. doi:10.1515/sjpain-2020-0032
37. Riecke J, Zerth SF, Schubert A, et al. Risk factors and protective factors of acute postoperative pain: an observational study at a German university hospital with cross-sectional and longitudinal inpatient data. BMJ Open. 2023;13(5):1–8. doi:10.1136/bmjopen-2022-069977
38. Tsui P, Gupta A, Cervoni C, Page C, Sonty N. Pain psychology and perioperative pain management. Perioperative Pain Control. 2021;9:117–133. doi:10.1007/978-3-030-56081-2_9
39. Nyktari V. Current minimally invasive surgery and chronic postsurgical pain S54. Signa Vitae. 2021;17(1):54. doi:10.22514/sv.2021.197
40. Shamim M. Diathermy vs. scalpel skin incisions in general surgery: double-blind, randomized, clinical trial. World J Surg. 2009;33(8):1594–1599. doi:10.1007/s00268-009-0064-9
41. Ramsay M. Postoperative pain management: is the surgical team approach finally getting it right? Ann Surg. 2019;270(2):209–210. doi:10.1097/SLA.0000000000003374
42. Nasir M, Ahmed A. Knowledge about postoperative pain and its management in surgical patients. Cureus. 2020;12(1):e6685. doi:10.7759/cureus.6685
43. Kasahun H, Agizew T, Temesgen M, Ashagrie H. Assessment of acute postoperative pain management and associated factors after elective surgery among adult surgical patients: a prospective cross-sectional study. IJS. 2022;7(1):e37. doi:10.1097/SR9.0000000000000037
44. Khalid A, Sadiqa A, Rehman NA, Bilal M, Inayat T. Association of preoperative pain-related education with postoperative patient care among in-hospital cardiac patients. Anaesth Pain Intensive Care. 2022;26(6):757–767. doi:10.35975/apic.v26i6.2046
45. O’Donnell KF. Preoperative pain management education: an evidence-based practice project. J Perianesth Nurs. 2018;33(6):956–963. doi:10.1016/j.jopan.2017.11.001
46. Darville-Beneby R, Lomanowska AM, Yu HC, et al. The impact of preoperative patient education on postoperative pain, opioid use, and psychological outcomes: a narrative review. Can J Pain. 2023;7(2):2266751. doi:10.1080/24740527.2023.2266751
47. Sinderovsky A, Grosman-Rimon L, Atrash M, et al. The effects of preoperative pain education on pain severity in cardiac surgery patients: a pilot randomized control trial. Pain Manag Nursing. 2023;24(4):e18–e25. doi:10.1016/j.pmn.2023.02.003
48. Tadesse M, Ahmed S, Regassa T, et al. Effect of preoperative anxiety on postoperative pain on patients undergoing elective surgery: prospective cohort study. Ann Med Surg. 2021;73:103190. doi:10.1016/j.amsu.2021.103190
49. McKnight R, Price J, Geddes J. Anxiety and obsessional disorders. Psychiatry. 2019;24:329–348. doi:10.1093/oso/9780198754008.003.0032
50. Jabur R, Gonçalves R, Faria K, Semczik I, Ramacciato J, Bortoluzzi M. Single-channel electroencephalography and its associations with anxiety and pain during oral surgery: a preliminary report. J Dental Anesthesia Pain Med. 2021;21(2):155–165. doi:10.17245/jdapm.2021.21.2.155
51. Ozhanli Y, Akyuz N. The effect of progressive relaxation exercise on physiological parameters, pain and anxiety levels of patients undergoing colorectal cancer surgery: a randomized controlled study. J Perianesthesia Nursing. 2021;37(2):238–246. doi:10.1016/j.jopan.2021.08.008
52. Meyer VM, Beydoun HA, Gyenai L, Goble NM, Hunter MM, McGill RJ. The effect of preoperative behavioral intervention on pain, anxiety, opioid use, and function in patients undergoing total knee arthroplasty: a randomized controlled study. Mil Med. 2023;188(5–6):e1010–e1017. doi:10.1093/milmed/usab424
53. Stamenkovic D, Rančić N, Latas M, et al. Preoperative anxiety and implications on postoperative recovery: what can we do to change our history. Minerva anestesiologica. 2018;84(11):1307–1317. doi:10.23736/S0375-9393.18.12520-X
54. Stuhlreyer J, Klinger R. The influence of preoperative mood and treatment expectations on early postsurgical acute pain after a total knee replacement. Front Psychiatry. 2022;13:840270. doi:10.3389/fpsyt.2022.840270
55. Disceken FM, Kose G. Association of preoperative pain beliefs with postoperative pain levels in abdominal surgery patients. J Clin Nurs. 2021;30(21–22):3249–3258. doi:10.1111/jocn.15831
56. Horn A, Kaneshiro K, Tsui B. Preemptive and preventive pain psychoeducation and its potential application as a multimodal perioperative pain control option: a systematic review. Anesthesia Analg. 2020;130(3):559–573. doi:10.1213/ANE.0000000000004319
57. Othin M, Sendagire C, Mukisa J, et al. Effect of preoperative information about pain on postoperative pain experience and patient satisfaction following orthopaedic surgery: a randomised controlled trial. Res Square. 2020;1:1–16. doi:10.21203/rs.3.rs-130942/v1
58. Fitzgerald H, Anderson E, Anderson L, Tracy A, Thomson J. Effectiveness of deep general anesthesia compared to the standard depth of general anesthesia on acute postoperative pain and patient safety: a systematic review protocol. JBI Database Systematic Rev Implementation Reports. 2019;17(10):2129–2135. doi:10.11124/JBISRIR-2018-004040
59. Hill K, Macfarlane A. Does regional anaesthesia improve outcome? Anaesth Intensive Care Med. 2018;19(11):619–623. doi:10.1016/J.MPAIC.2018.08.018
60. Wong H, Pilling R, Young B, Owolabi A, Onwochei D, Desai N. Comparison of local and regional anesthesia modalities in breast surgery: a systematic review and network meta-analysis. J Clin Anesthesia. 2021;72:110274. doi:10.1016/j.jclinane.2021.110274
61. Droog W, Walbeehm E, Konijn J, et al. A systematic review on long-term postsurgical pain outcomes; what is the effect of upper extremity regional anesthesia? Anesthesia Analg. 2023;137(2):365–374. doi:10.1213/ANE.0000000000006529
62. Levene J, Weinstein E, Cohen M, et al. Local anesthetics and regional anesthesia versus conventional analgesia for preventing persistent postoperative pain in adults and children: a Cochrane systematic review and meta-analysis update. J Clin Anesthesia. 2019;55:116–127. doi:10.1016/j.jclinane.2018.12.043
63. Mynka N, Kobelyatsky YY. Efficacy of a combination of regional methods of anesthesia with general anesthesia in corneal transplantation. Emergency Med. 2021;17(4):69–73. doi:10.22141/2224-0586.17.4.2021.237729
64. Reysner T, Wieczorowska-Tobis K, Kowalski G, et al. The influence of regional anesthesia on the systemic stress response. Reports. 2024;7(4):89. doi:10.3390/reports7040089
65. Shellito A, Dworsky J, Kirkland P, et al. Perioperative pain management issues unique to older adults undergoing surgery. Ann Surg Open. 2021;2(3):e072. doi:10.1097/AS9.0000000000000072
66. Godde K, Mude G, Barole N, Tenpe S. Modern anesthesia: a multidisciplinary approach to pain relief. Multidisciplinary Rev. 2024;8(4):e2025104. doi:10.31893/multirev.2025104
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.