Back to Journals » Infection and Drug Resistance » Volume 19
Predictive Factors for Upper Urinary Tract Stones Combined with Carbapenem-Resistant Enterobacteriaceae Associated Urinary Tract Infections
Authors Zhang X, Ji C, Chi Z, Hu W
Received 9 January 2026
Accepted for publication 15 June 2026
Published 30 June 2026 Volume 2026:19 589951
DOI https://doi.org/10.2147/IDR.S589951
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Oliver Planz
Xuming Zhang, Chaoyue Ji, Zhichao Chi, Weiguo Hu
Department of Urology, Beijing Tsinghua Changgung Hospital, School of Clinical Medicine, Tsinghua Medicine, Tsinghua University, Beijing, 102218, People’s Republic of China
Correspondence: Weiguo Hu, Email [email protected]; Chaoyue Ji, Email [email protected]
Introduction: This study investigates predictive factors for carbapenem-resistant Enterobacteriaceae (CRE) bacteriuria in patients with upper urinary tract stones, a population particularly vulnerable to complicated urinary tract infections amidst growing antimicrobial resistance.
Methods: A cross-sectional study was conducted on 2029 inpatients with upper urinary tract stones. Patients with CRE bacteriuria (n=31) were compared with a matched non-CRE group (n=124). Clinical data, stone characteristics, and admission laboratory parameters were analyzed. Univariate and multivariate logistic regression were employed to identify independent predictive factors and establish a diagnostic model.
Results: Escherichia coli and Klebsiella pneumoniae were the predominant CRE pathogens. Multivariate analysis identified three independent predictive factors for CRE bacteriuria: a history of fever within the past 3 months (OR=3.24, p=0.03), presence of an indwelling ureteral stent at admission (OR=12.97, p< 0.01), and a positive urinary nitrite test (OR=2.92, p=0.04). A diagnostic model incorporating these factors demonstrated good predictive accuracy, with an area under the receiver operating characteristic curve of 0.83.
Conclusion: A history of recent fever, indwelling ureteral stents, and positive urinary nitrite are significant independent predictive factors for CRE-associated urinary tract infections in patients with upper urinary tract stones. The developed diagnostic model demonstrates potential predictive value in an exploratory setting, which may inform future large-scale studies aimed at the early identification and management of these high-risk patients before definitive culture results are available.
Keywords: urolithiasis, carbapenem-resistant enterobacteriaceae, urinary tract infections
Introduction
Carbapenem-resistant Enterobacteriaceae (CRE) are defined by the US Centers for Disease Control and Prevention as Enterobacteriaceae resistant to at least one carbapenem antibiotic or producing carbapenemases.1 The most common types of carbapenem-resistant Enterobacteriaceae (CRE) are carbapenem-resistant Klebsiella pneumoniae (CRKP) and carbapenem-resistant Escherichia coli (CREco).2 The hazards of CRE are beyond dispute. The most comprehensive meta-analysis to date concluded that mortality rates among patients infected with CRE are markedly higher than those infected with carbapenem-sensitive Enterobacteriaceae, reaching more than double in some studies.3 In 2017, CRE was designated by the World Health Organization as one of three categories of resistant bacteria requiring the most urgent development of new antibiotics globally.4
Urinary tract infections(UTI) are among the most common infectious diseases in healthcare settings, affecting approximately 150 million people worldwide each year.5 UTIs encompass a wide range of types, including numerous benign forms (such as uncomplicated cystitis) and life-threatening variants (such as urosepsis). Diagnosis of UTIs currently relies primarily on clinical symptoms (such as frequent urination, urgency, dysuria, and fever) combined with laboratory investigations. These include routine urine analysis (leukocyte esterase, nitrite), urine culture, and antimicrobial susceptibility testing.6 A positive urine culture for pathogenic bacteria forms the cornerstone of diagnosis. The causative pathogens of urinary tract infections are predominantly Enterobacteriaceae, making the urinary tract one of the most common sites for CRE infections. Urinary tract stones are among the most common disorders of the urinary system, and their incidence has been increasing annually in parallel with improvements in living standards. The diagnosis of urinary tract stones primarily relies on imaging examinations such as ultrasound and non-contrast CT scans. CT currently represents the most accurate method for assessing stone burden, location, degree of obstruction, and hydronephrosis.7 The relationship between upper urinary tract stones and UTIs is complex and intertwined, with each condition potentially contributing to the other. When upper urinary tract stones act as a causative factor, they often lead to UTIs through mechanisms such as urinary tract obstruction or damage to the urinary epithelium. Patients with urinary stones demonstrate a significantly increased likelihood of developing UTIs compared to individuals without such conditions. One study followed over a thousand adult patients with upper urinary tract stones for up to seven years, ultimately finding a high rate of positive urine cultures at 28%.8
Upper urinary tract stones complicated by UTIs present a challenging clinical problem. In clinical practice, aggressive antimicrobial therapy forms the cornerstone of management, as a positive preoperative urine culture constitutes a high-risk factor for postoperative infection following stone surgery.9 Preoperative treatment should employ appropriate antibiotics based on urine culture and susceptibility testing results. For patients presenting with fever or signs of sepsis, surgery should only be considered once the infection has been effectively controlled.10 Current urine culture and susceptibility testing typically requires 2–3 days to yield results. Earlier identification of the infecting bacterial species would enable the guidance of empirical antibiotic therapy, thereby avoiding antibiotic overuse. It would also facilitate the isolation of patients with infections caused by resistant bacteria, preventing the nosocomial spread of such pathogens.
In recent years, multiple studies have reported risk factors for CRE-associated urinary tract infections, including prior hospitalization, invasive procedures, and broad-spectrum antibiotic use.11 However, predictive research specifically targeting the specialized population of upper urinary tract stone patients remains unexplored. Therefore, we envisage establishing a simple and practical predictive model using clinical and laboratory indicators available at admission, through a cross-sectional study approach, to assist clinicians in making preliminary judgements while awaiting urine culture results.
Methods
Study Setting
This study was conducted within the urology department of a university-affiliated tertiary hospital. Our institution is designated as one of China’s specialized centers for the prevention and treatment of urological stone disease and manages approximately 1500 patients with stone-related conditions annually. The study was approved by the Beijing Tsinghua Changgung Hospital Ethics Committee and was conducted in accordance with the Helsinki Declaration. The Ethics Committee deemed that participants’ informed consent could be waived in accordance with the relevant laws and policies. The ethical approval number for this study is 25256-4-01.
Study Design and Patient Population
Clinical data were rigorously collected from 2029 inpatients admitted to the general ward of the Department of Urology at Beijing Tsinghua Changgung Hospital between January 2017 and December 2023 for upper urinary tract stones, strictly adhering to inclusion criteria. A positive urine culture is defined as follows: in midstream urine samples, a bacterial colony count exceeding 105 CFU/mL in females or exceeding 104 CFU/mL in males; or a bacterial colony count of ≥1×104 CFU/mL in urine collected via an indwelling Foley catheter. Exclusion criteria are as follows: (1) Presence of immunodeficiency disorders or use of immunosuppressive medications. (2) Relevant clinical data was incomplete upon admission. (3) Admission to ICU prior to definitive urine culture results.
The patients enrolled were divided into two groups. The CRE group comprised 31 patients confirmed to have CRE-associated UTIs via antimicrobial susceptibility testing. The non-CRE group included 1940 patients whose test results indicated other bacteria, fungi, or Ureaplasma. Patients in the CRE and non-CRE groups were matched in a 1:4 ratio based on age, gender, and admission date. The reason we adopted a 1:4 ratio is that we had sufficient samples available, achieving a balance between attaining the most effective power and minimizing sample loss.12 Ultimately, 124 patients were included in the non-CRE group. The collected patient data encompassed three primary categories: (1) Personal characteristics: age, gender, presenting symptoms, comorbidities or prior medical history, and year of admission; (2) Stone-related parameters: cumulative maximum diameter, volume, presence of urinary obstruction, and presence of staghorn calculi; (3) Laboratory findings upon admission: complete blood count, urinalysis results, renal function indicators, urine culture and sensitivity outcomes, and infection-related biomarkers.
Definition of CRE
This study adheres to the Clinical and Laboratory Standards Institute (CLSI) guidelines for minimum inhibitory concentration (MIC) testing of carbapenem-resistant Enterobacteriaceae (CRE).13 The standard for reporting CRE is as follows: MIC ≥ 4μg/mL for doripenem, meropenem, and imipenem; or MIC ≥ 2μg/mL for ertapenem.
Statistical Analysis
All data were collated using Excel and subjected to statistical analysis via SPSS 23.0 and R software version 4.0.5. For univariate analysis, quantitative data meeting normality and homogeneity of variance criteria underwent independent samples t-tests, with descriptive statistics presented as mean ± standard deviation. Non-normally distributed quantitative data were analyzed using the Wilcoxon signed-rank test, with descriptive statistics expressed as median (interquartile range). Qualitative data were described using percentages, with intergroup comparisons performed via χ2 or Fisher’s exact test. P values < 0.05 were considered statistically significant. Significant variables underwent univariate logistic regression analysis. Multivariate analysis employed binary logistic regression to construct diagnostic models for independent predictive factors, alongside the generation of curves and nomograms and receiver operating characteristic curve (ROC).
Results
Clinical Characteristics
Information on all patients during hospitalization was reviewed via the hospital case management system. Urine culture results from the first three days following admission were collected, and the data were systematically recorded. The classification (family and genus) of each bacterial strain was confirmed by referencing the official websites of the National Microbial Science Data Centre and the National Pathogenic Microorganisms Resource Bank.
A total of 31 strains were detected in the CRE group, including 14 strains of Escherichia coli (45.2%), 12 strains of Klebsiella pneumoniae (38.7%), three cases of Enterobacter cloacae (9.7%), and two strains of Citrobacter (6.5%). None of the patients were co-infected with any other type of bacteria, as shown in Figure 1. A total of 160 bacterial strains were detected in the non-CRE group, the three most common types being Enterobacteriaceae (30.6%), Ureaplasma (17.5%) and Enterococcus spp. (14.4%).
 |
Figure 1 Urine culture results for CRE group and non-CRE group patients. |
Antimicrobial Susceptibility Testing
Due to the varying time requirements for each strain to undergo the antimicrobial susceptibility testing, the drugs utilized for each strain were not identical. Ultimately, a total of 25 drugs were employed for the drug sensitivity test. The CRE group strains had the highest resistance rate to Amoxicillin/Clavulanic Acid and Cefuroxime, with a resistance rate of 100%, and the lowest rate of resistance to Tigecycline with a resistance rate of 12.5% (Table 1).
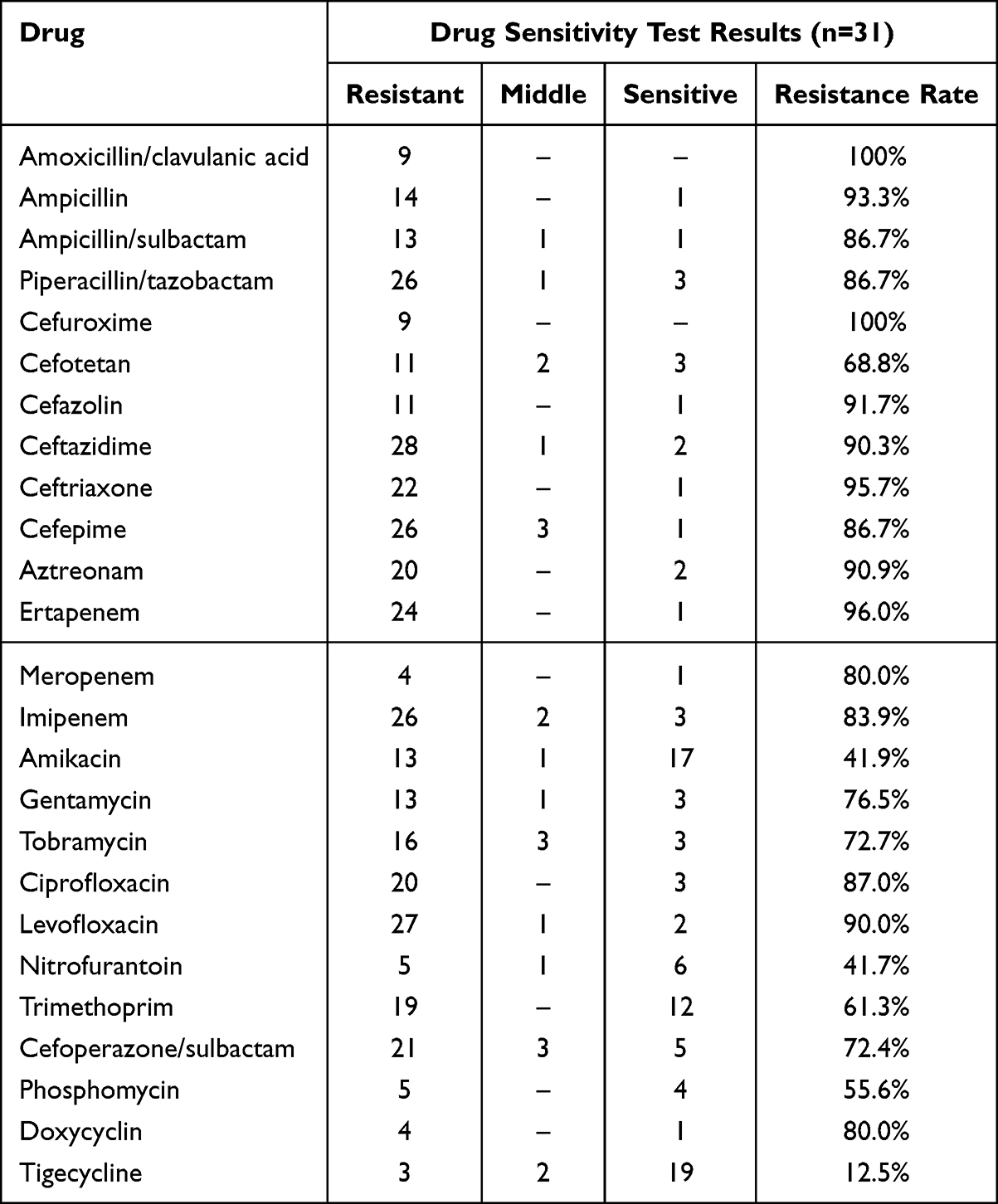 |
Table 1 Drug Resistance Rates of CRE Group |
Analysis of Predictive Factors
Patients with upper urinary tract calculi combined with CRE bacteriuria are mainly elderly people and women. In the results of univariate analysis, patients in the CRE group were more likely to have a history of fever in the past 3 months (P < 0.01) in terms of comorbidities or medical history and were more likely to have indwelling nephrostomy tubes (P=0.04), Ureteral stents (P < 0.01), or Foley catheters (P=0.04) at admission. The comparison of other basic personal information is shown in Table 2. In relation to stone load, patients in the CRE group exhibited higher cumulative maximum diameter and stone volume in comparison to those in the non-CRE group. However, subsequent statistical analysis revealed no significant differences between the two groups. About the characteristics of calculi, patients in the CRE group demonstrated a higher propensity for bilateral calculi, multiple calculi, and concurrent presence of calculi in both the kidneys and ureters when compared to those in the non-CRE group. Nonetheless, statistical analysis did not reveal any significant differences. With respect to complications caused by stones, the incidence of obstruction in the CRE group was higher, though this did not reach statistical significance. In terms of laboratory test indicators, the hemoglobin level of patients in the CRE group was lower than that in the non-CRE group, and the positive proportion of urine nitrite was significantly higher than that in the non-CRE group. All the above comparisons between the groups showed statistically significant differences (P < 0.01).
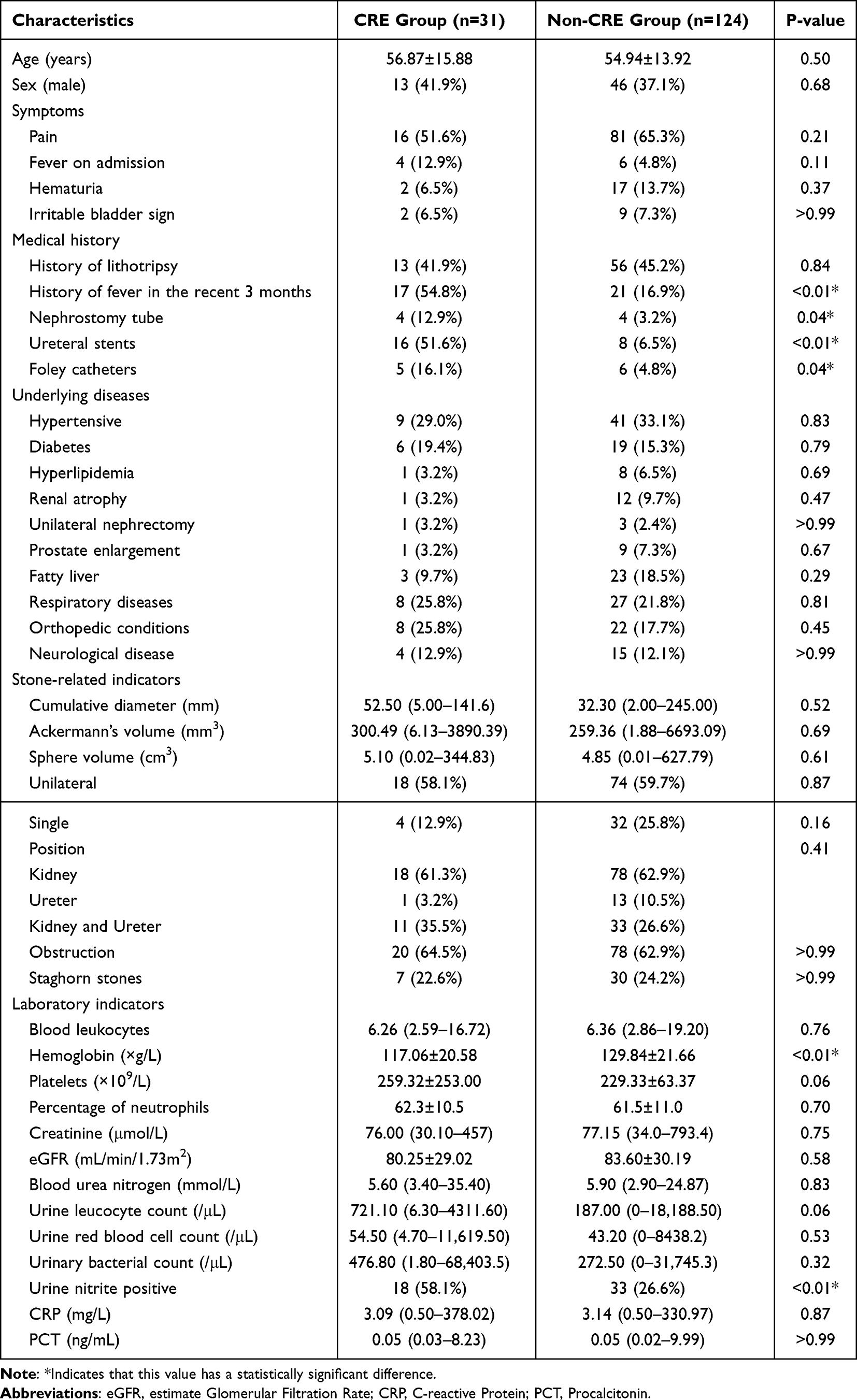 |
Table 2 Comparison with Patients’ Characteristics Between CRE and Non-CRE Groups |
Multivariate analysis was conducted using binary logistic regression to ascertain the presence of fever history in the recent three months, indwelling nephrostomy tube at admission, indwelling ureteral stents at admission, indwelling Foley catheters at admission, lower hemoglobin and urine nitrite positive (Table 3). Among them, there were statistically significant differences in the presence of a fever history in the recent 3 months, indwelling ureteral stents at admission, and urine nitrite positive. The relevant raw data for multivariate analysis can be found in the supplementary materials (Supplementary Table 1).
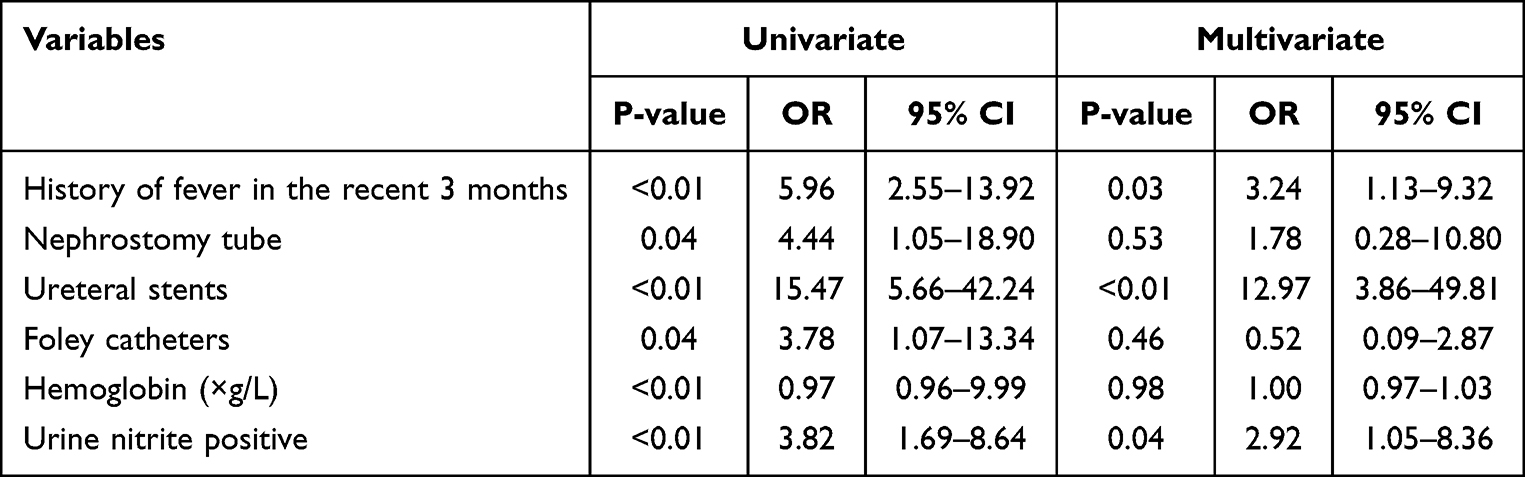 |
Table 3 Univariate and Multivariate Analysis of Predictive Factors for CRE Acquisition |
Construction of the Diagnostic Model
The three independent predictive factors were utilized to construct the diagnostic model and plot the nomogram (Figure 2). Subsequently, a receiver operator characteristic curve was generated (Figure 3), which had an area under the curve (AUC) of 0.83 (95% CI 0.74–0.92, P < 0.05), indicating that the model had good positive predictive properties. The calibration degree of the nomogram model was evaluated through calibration curves. In Figure 4, this was verified using the 1000-times Bootstrap resampling method. The results demonstrate that the calibration curve of the nomogram basically coincides with the ideal curve, indicating that the performance of the model approaches the ideal diagnostic performance.
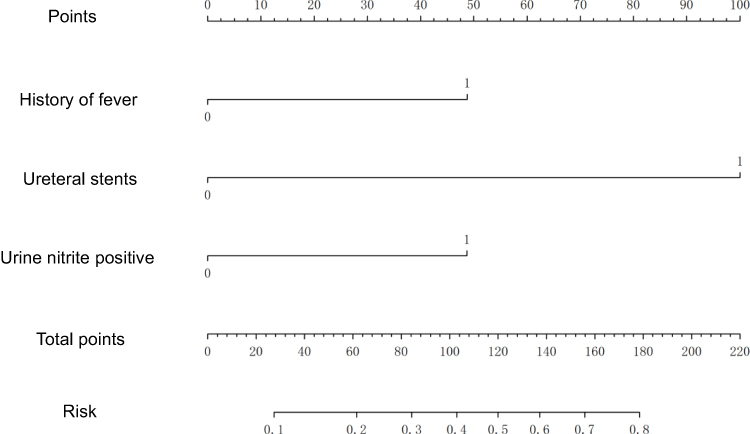 |
Figure 2 Nomogram prediction model for upper urinary tract stones with CRE-associated UTIs. |
 |
Figure 3 Receiver operating curve for predictive model of upper urinary tract stones with CRE-associated UTIs. |
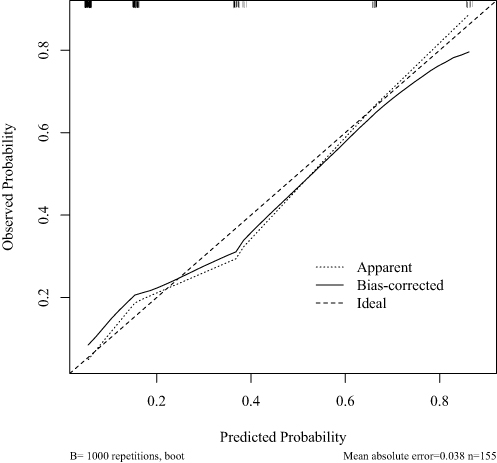 |
Figure 4 Calibration curve for predictive model of upper urinary tract stones with CRE-associated UTIs. |
Discussion
The detection rate of CRE in this study was 1.53%, significantly higher than the reported CRE infection incidence of 4.0 per 100,000 discharged patients in a multicenter study across 25 tertiary hospitals in China.14 This indicates that the high-risk subgroup of patients with upper urinary tract stones faces a markedly greater risk of urinary tract infection compared to the general hospitalized population. This may be associated with factors such as urinary tract obstruction, epithelial damage, and exposure to invasive procedures in such patients. This study classified the bacteria detected in the urine of the included patients and found that Escherichia coli and Klebsiella pneumoniae were the most common in the CRE group, accounting for more than 80% of the total. This is consistent with previous studies that CREco and CRKP are the two most common types of bacteria in CRE.13,15 The most prevalent strain identified within the non-CRE group was Escherichia coli, a finding that aligns with the predominance of Enterobacteriaceae as the most prevalent strain type in UTIs. A study revealed that Escherichia coli accounted for 85% of community-acquired UTIs and 50% of nosocomial-acquired UTIs.16
Antimicrobial susceptibility testing showed that CRE strains had the highest resistance to β-lactam antibiotics, and more than 80% to carbapenems with lower resistance to tigecycline and aminoglycosides. This finding is consistent with the global trend of CRE resistance, but it also highlights the dilemma of clinical treatment: the significant failure of carbapenems as the traditional “last-line-of-defence” drugs, and the wide range of adverse drug reactions and consequent economic problems associated with alternative drugs with lower resistance rates. When treating CRE infections, in vitro susceptibility testing serves as a key basis for selecting antimicrobial agents, though it is not the sole criterion. Clinical decision-making must comprehensively consider multiple factors including susceptibility results, resistance mechanisms, site and severity of infection, patient-specific characteristics, and drug availability.17,18 Firstly, in vitro antimicrobial susceptibility testing serves as the cornerstone for guiding antimicrobial therapy. Accurate susceptibility testing clearly identifies bacterial strains’ sensitivity to various antimicrobial agents, providing fundamental assurance against the use of ineffective drugs. However, for severe infections with high mortality risk (such as bloodstream infections), even when antimicrobial susceptibility testing indicates intermediate or only slight resistance to certain drugs, clinicians often employ strategies involving high doses, prolonged infusion, or combination therapy to enhance treatment success rates.19 When selecting medications, the patient’s renal function, hepatic function, age, and the potential toxic side effects of the drugs (such as the nephrotoxicity of polymyxin and the risk of subtherapeutic blood concentrations with tigecycline) must all be taken into account to avoid ineffective treatment and minimize adverse reactions.20,21 Although novel agents such as Cefiderocol and Aztreonam-Avibactam have been demonstrated to be effective against certain CRE isolates, these medications may not yet be widely available in all regions. Consequently, treatment decisions must be based on locally accessible drugs alongside continually updated clinical efficacy and safety evidence.1 Additionally, a variety of antibiotics with novel antimicrobial mechanisms have been developed in recent years, such as iron carrier antibiotics and macrocyclic nucleoside antibacterials that block bacterial MraY proteins,22 in the hope of playing their unique roles in the future antibacterial field.
In the results of the univariate analysis of this study, it was found that the proportion of patients with indwelling nephrostomy tubes, ureteral stents and Foley catheters at admission was significantly higher in the CRE group than in the non-CRE group. This result is consistent with previous studies, suggesting that invasive manipulation is a key risk factor for CRE infection.23 Catheter retention has been demonstrated to disrupt the uroepithelial barrier, and the rough surface of the catheter has been shown to provide a vehicle for the formation of bacterial biofilms. Once a biofilm has been formed, bacteria within the biofilm are significantly more permeable to antibiotics and resistant to host immune clearance than planktonic bacteria without biofilm formation. This process thus promotes bacterial colonization and infection.24 It has been shown that both Escherichia coli25 and Klebsiella pneumoniae26 have a strong ability to form biofilms, so how to eradicate biofilms will also be one of the directions for controlling catheter-associated UTIs, especially multidrug-resistant bacterial infections. According to existing studies, therapeutic strategies for biofilms include inhibiting the formation of their extracellular polymer matrix, inhibiting biofilm spreading, and interfering with the metabolism of microorganisms in the biofilm.27 More attempts and studies are needed in the future on how to translate these laboratory techniques into clinical techniques and apply them to patients. Notably, having an indwelling ureteral stent at admission was identified as an independent predictive factor in multivariate analysis with a significantly higher risk than other catheter types. Prolonged ureteral stenting can cause local inflammatory reactions, vesicoureteral reflux or localized urinary stasis, and prolonged bacterial contact with the urinary tract epithelium.28 This is consistent with our observation that the proportion of patients requiring long-term catheterization due to inoperability was significantly higher in the CRE group than in the non-CRE group. Therefore, the guidelines should be strictly followed to remove or repacle ureteral stents as soon as possible and to optimize the catheterization process.
In this study, a univariate analysis revealed that the CRE group exhibited significantly lower hemoglobin levels compared to the non-CRE group. A subsequent review of the literature identified a potential causal relationship between anemia and infection.29 Inflammatory anemia, otherwise referred to as anemia of chronic disease, is the most prevalent form of anemia in hospitalized and chronically ill patients. The underlying mechanism of this condition is associated with systemic immune activation, leading to impaired iron transport (including iron retention in macrophages and reduced dietary iron uptake, etc)., impaired iron- and liver-dependent erythropoiesis (which is considered to be associated with inflammation that inhibits the level of erythropoietin to the right), and shortened erythrocyte lifespan in the inflammatory milieu. Anemia, in turn, can lead to a decline in the body’s immune function,30 ultimately forming a vicious circle of “infection-anemia-infection”. Therefore, in clinical practice, anemia in combination with upper urinary tract stones suggests the possibility of chronic infection. Chronic infection may be caused by the obstruction of upper urinary tract stones, resulting in the accumulation of urine, or it may be caused by the stone itself as a foreign body, which becomes a “shelter” for bacterial proliferation,31 making it difficult to remove the bacteria inside the stone, and ultimately leading to incomplete treatment. This chronic infection, failing to address the root cause—namely, the removal of the stones—leads to prolonged antibiotic use, thereby selecting for drug-resistant bacteria. In the multivariate analysis, it was found that the proportion of patients in the CRE group with a history of fever in the recent three months was significantly higher. This similarly suggests that prolonged recurrent infections may be an important causative factor for bacteriuria in CRE.
In addition, urinary nitrite positive is an independent predictive factor. A large-scale study indicates that urinary nitrite testing demonstrates good predictive performance for positive urine cultures caused by Gram-negative bacteria. However, its predictive capability is poor for bacteriuria caused by Gram-positive bacteria.32 Escherichia coli is the primary bacterium responsible for positive urinary nitrite results. Studies indicate that among patients developing Escherichia coli infections following kidney stone surgery, the preoperative urinary nitrite positivity rate reached 64.5%. However, infections caused by Klebsiella pneumoniae exhibit a lower nitrite positivity rate.33 This indicates that a positive nitrite test is strongly associated with Escherichia coli infection, but may be less strongly linked to other Enterobacteriaceae such as Klebsiella species. Therefore, a positive urinary nitrite test primarily suggests a possible infection in the urine caused by Gram-negative bacilli such as Escherichia coli, which possess strong nitrate-reducing capabilities. However, it cannot detect all types of urinary tract pathogens.
This study has certain limitations. Firstly, we did not find any differences about stones burden. However, the CRE group exhibited a higher stone burden, suggesting that larger stones may more readily cause urinary tract obstruction, urine retention, and damage to the urinary epithelium, thereby creating a favorable environment for CRE colonization and biofilm formation.34,35 We consider that more calculation-related indicators, such as the stone system rating, need to be included in subsequent studies. Secondly, this study is constrained by its retrospective, single-center design and a very limited number of CRE cases, which increases the risk of overfitting and limits the generalizability of the proposed predictive model. Furthermore, the absence of key clinical variables, such as detailed previous antibiotic use and specific stone burden metrics, restricts the robustness of our findings. Therefore, our results should be interpreted as exploratory rather than definitive. Nevertheless, as an early report on CRE infection in this specific population, it provides preliminary data to inform future multi-center prospective studies.
Conclusion
In our preceding study, we conducted a review of the risk factors and therapeutic advances for CRE-associated UTIs.36 In this study, we direct our attention to patients with concomitant upper urinary tract stones. In this study, “history of fever in the recent 3 months”, “having an indwelling ureteral stent at admission” and “urinary nitrite positive” were selected as independent predictive factors for CRE infection in patients with upper urinary tract stones. These exploratory findings highlight potential risk factors that may help conceptualize future risk stratification for CRE-associated UTIs early in hospitalization. While these initial results do not yet warrant immediate changes to clinical protocols, they provide a foundation for future, larger-scale prospective studies. Such validation is necessary to determine whether predictive models can safely guide the early selection of targeted agents (such as tigecycline or amikacin) or the timely implementation of contact isolation measures. Ultimately, refining and validating this model could eventually assist in concentrating infection control resources on predicted vulnerable populations.
Abbreviations
CRE, Carbapenem-resistant Enterobacteriaceae; UTIs, Urinary tract infections; MIC, Minimum inhibitory concentration; CRKP, Carbapenem-resistant Klebsiella pneumoniae; CREco, Carbapenem-resistant Escherichia coli.
Data Sharing Statement
All data generated or analyzed during this study are included in this published article and its supplementary information files.
Ethics Approval and Consent to Participate
This study was approved by the Beijing Tsinghua Changgung Hospital Ethics Committee. The Ethics Committee agreed with that participants’ informed consent could be waived in accordance with the relevant laws and policies, including the National Health Commission- “Human beings biomedical research ethics audit method (2023), the State Drug Administration/National Health Commission” the quality control standard for clinical trials (2020) and the medical equipment quality control standard for clinical trials (2022), WHA-Helsinki declaration (2013) and CIOMS-the human body biomedical research international moral guideline ethical principles. The data of all patients in this study were provided anonymously without exposing the privacy of the patients.
Acknowledgments
We acknowledge Ms. Cao Han and Dr. Yuzhe Tang for their supporting work in this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
No funding was received for conducting this research.
Disclosure
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
References
1. Bologna E, Licari LC, Manfredi C, et al. Carbapenem-resistant enterobacteriaceae in urinary tract infections: from biological insights to emerging therapeutic alternatives. Medicina. 2024;60:214. doi:10.3390/medicina60020214
2. Yao Y, Falgenhauer L, Falgenhauer J, et al. Carbapenem-Resistant Citrobacter spp. as an emerging concern in the hospital-setting: results from a genome-based regional surveillance study. Front Cell Infect Microbiol. 2021;11:744431. doi:10.3389/fcimb.2021.744431
3. Zhou R, Fang X, Zhang J, et al. Impact of carbapenem resistance on mortality in patients infected with Enterobacteriaceae: a systematic review and meta-analysis. BMJ Open. 2021;11:e054971. doi:10.1136/bmjopen-2021-054971
4. Tacconelli E, Carrara E, Savoldi A, et al. Discovery, research, and development of new antibiotics: the WHO priority list of antibiotic-resistant bacteria and tuberculosis. Lancet Infect Dis. 2018;18:318–12. doi:10.1016/s1473-3099(17)30753-3
5. Tandogdu Z, Wagenlehner FM. Global epidemiology of urinary tract infections. Curr Opin Infect Dis. 2016;29:73–79. doi:10.1097/qco.0000000000000228
6. Kranz J, Bartoletti R, Bruyère F, et al. European Association of Urology Guidelines on Urological Infections: summary of the 2024 guidelines. Eur Urol. 2024;86:27–41. doi:10.1016/j.eururo.2024.03.035
7. Thongprayoon C, Krambeck AE, Rule AD. Determining the true burden of kidney stone disease. Nat Rev Nephrol. 2020;16:736–746. doi:10.1038/s41581-020-0320-7
8. Holmgren K, Danielson BG, Fellström B, et al. The relation between urinary tract infections and stone composition in renal stone formers. Scand J Urol Nephrol. 1989;23:131–136. doi:10.3109/00365598909180827
9. Köves B, Cai T, Veeratterapillay R, et al. Benefits and harms of treatment of asymptomatic bacteriuria: a systematic review and meta-analysis by the European Association of Urology Urological Infection Guidelines Panel. Eur Urol. 2017;72:865–868. doi:10.1016/j.eururo.2017.07.014
10. Bargagli M, Scoglio M, Howles SA, Fuster DG. Kidney stone disease: risk factors, pathophysiology and management. Nat Rev Nephrol. 2025;21:794–808. doi:10.1038/s41581-025-00990-x
11. Kitano H, Teishima J, Shigemura K, et al. Current status of countermeasures for infectious diseases and resistant microbes in the field of urology. Int J Urol. 2019;26:1090–1098. doi:10.1111/iju.14087
12. Hennessy S, Bilker WB, Berlin JA, Strom BL. Factors influencing the optimal control-to-case ratio in matched case-control studies. Am J Epidemiol. 1999;149:195–197. doi:10.1093/oxfordjournals.aje.a009786
13. Potter RF, D’Souza AW, Dantas G. The rapid spread of carbapenem-resistant Enterobacteriaceae. Drug Resist Updat. 2016;29:30–46. doi:10.1016/j.drup.2016.09.002
14. Zhang Y, Wang Q, Yin Y, et al. Epidemiology of carbapenem-resistant Enterobacteriaceae infections: report from the China CRE Network. Antimicrob Agents Chemother. 2018;62. doi:10.1128/aac.01882-17
15. Ma J, Song X, Li M, et al. Global spread of carbapenem-resistant Enterobacteriaceae: epidemiological features, resistance mechanisms, detection and therapy. Microbiol Res. 2023;266:127249. doi:10.1016/j.micres.2022.127249
16. Foxman B. Urinary tract infection syndromes: occurrence, recurrence, bacteriology, risk factors, and disease burden. Infect Dis Clin North Am. 2014;28:1–13. doi:10.1016/j.idc.2013.09.003
17. Tamma PD, Heil EL, Justo JA, et al. Infectious Diseases Society of America 2024 Guidance on the treatment of antimicrobial-resistant gram-negative infections. Clin Infect Dis. 2024:ciae403. doi:10.1093/cid/ciae403
18. Tumbarello M, Losito AR, Giamarellou H. Optimizing therapy in carbapenem-resistant Enterobacteriaceae infections. Curr Opin Infect Dis. 2018;31:566–577. doi:10.1097/qco.0000000000000493
19. Sheu CC, Chang YT, Lin SY, Chen YH, Hsueh PR. Infections caused by carbapenem-resistant Enterobacteriaceae: an update on therapeutic options. Front Microbiol. 2019;10:80. doi:10.3389/fmicb.2019.00080
20. Zavascki AP, Klee BO, Bulitta JB. Aminoglycosides against carbapenem-resistant Enterobacteriaceae in the critically ill: the pitfalls of aminoglycoside susceptibility. Expert Rev Anti Infect Ther. 2017;15:519–526. doi:10.1080/14787210.2017.1316193
21. Stoian IA, Balas Maftei B, Florea C-E, et al. Multidrug-resistant Acinetobacter baumannii: resistance mechanisms, emerging therapies, and prevention-a narrative review. Antibiotics. 2025;15:2. doi:10.3390/antibiotics15010002
22. Nakaya T, Yabe M, Mashalidis EH, et al. Synthesis of macrocyclic nucleoside antibacterials and their interactions with MraY. Nat Commun. 2022;13:7575. doi:10.1038/s41467-022-35227-z
23. Justo-Quintas J, Medina-Polo J, Gil-Moradillo J, et al. Infections by carbapenemase-producing enterobacteriaceae in a department of urology. A new challenge. Actas Urol Esp. 2018;42:170–175. doi:10.1016/j.acuro.2017.08.004
24. Imvrios G, Tzitzili E, Pyrpasopoulou A, et al. Association of Double-J stenting in renal transplant patients with urinary tract colonization and infections in a multidrug-resistant microbe endemic nosocomial environment. Transplant Proc. 2019;51:408–412. doi:10.1016/j.transproceed.2019.01.020
25. Sharma G, Sharma S, Sharma P, et al. Escherichia coli biofilm: development and therapeutic strategies. J Appl Microbiol. 2016;121:309–319. doi:10.1111/jam.13078
26. Guerra MES, Destro G, Vieira B, et al. Klebsiella pneumoniae biofilms and their role in disease pathogenesis. Front Cell Infect Microbiol. 2022;12:877995. doi:10.3389/fcimb.2022.877995
27. Koo H, Allan RN, Howlin RP, Stoodley P, Hall-Stoodley L. Targeting microbial biofilms: current and prospective therapeutic strategies. Nat Rev Microbiol. 2017;15:740–755. doi:10.1038/nrmicro.2017.99
28. Wang X, Ji Z, Yang P, Li J, Tian Y. Forgotten ureteral stents: a systematic review of literature. BMC Urol. 2024;24:52. doi:10.1186/s12894-024-01440-9
29. Weiss G, Ganz T, Goodnough LT. Anemia of inflammation. Blood. 2019;133:40–50. doi:10.1182/blood-2018-06-856500
30. Korman RM, Hetzel N, Knowles TG, Harvey AM, Tasker S. A retrospective study of 180 anaemic cats: features, aetiologies and survival data. J Feline Med Surg. 2013;15:81–90. doi:10.1177/1098612x12461008
31. Schmidt WC, Mousavi A, Li J, et al. Intercalated bacterial biofilms are intrinsic internal components of calcium-based kidney stones. Proc Natl Acad Sci U S A. 2026;123:e2517066123. doi:10.1073/pnas.2517066123
32. Choi MH, Kim D, Bae HG, et al. Predictive performance of urinalysis for urine culture results according to causative microorganisms: an integrated analysis with artificial intelligence. J Clin Microbiol. 2024;62:e0117524. doi:10.1128/jcm.01175-24
33. Yang Z, Lin D, Hong Y, et al. The effect of preoperative urine culture and bacterial species on infection after percutaneous nephrolithotomy for patients with upper urinary tract stones. Sci Rep. 2022;12:4833. doi:10.1038/s41598-022-08913-7
34. Borghi L, Nouvenne A, Meschi T. Nephrolithiasis and urinary tract infections: ‘the chicken or the egg’ dilemma? Nephrol Dial Transplant. 2012;27:3982–3984. doi:10.1093/ndt/gfs395
35. Ripa F, Pietropaolo A, Montanari E, et al. Association of kidney stones and recurrent UTIs: the chicken and egg situation. A systematic review of literature. Curr Urol Rep. 2022;23:165–174. doi:10.1007/s11934-022-01103-y
36. Zhang X, Miao S, Ji C, Hu W. Risk factors and treatment advances for carbapenem-resistant Enterobacteriaceae infections in the urinary tract. Front Cell Infect Microbiol. 2025;15:1724851. doi:10.3389/fcimb.2025.1724851
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.