Back to Journals » Journal of Inflammation Research » Volume 19
Predictive Factors for Resorption in Lumbar Disc Herniation: A Systematic Review
Authors Shen X, Dai F, Li Z ![]() , Jiang H, Liu J, Wang J, Yu P
, Jiang H, Liu J, Wang J, Yu P
Received 30 August 2025
Accepted for publication 14 December 2025
Published 8 January 2026 Volume 2026:19 559719
DOI https://doi.org/10.2147/JIR.S559719
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Ujjwol Risal
Xueqiang Shen,1– 3,* Feng Dai,1,* Zihang Li,1,* Hong Jiang,1 Jintao Liu,1 Jianwei Wang,2 Pengfei Yu1
1Department of Orthopedic Surgery, Suzhou TCM Hospital Affiliated to Nanjing University of Chinese Medicine, Suzhou, Jiangsu, People’s Republic of China; 2Department of Orthopedic Surgery, Wuxi Affiliated Hospital of Nanjing University of Chinese Medicine, Wuxi, Jiangsu, People’s Republic of China; 3Nanjing University of Chinese Medicine, Nanjing, Jiangsu, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Pengfei Yu, Email [email protected] Jianwei Wang, Email [email protected]
Purpose: In patients with lumbar disc herniation (LDH), the herniated intervertebral disc (IVD) can be spontaneously absorbed without surgical intervention (herein referred to as “resorption”). However, current studies provide unclear explanations of the mechanism of LDH resorption, and the summary of predictive factors is not comprehensive enough. This review aimed to summarize predictive factors associated with LDH resorption based on current evidence, thereby providing clinical guidance for therapeutic decision making.
Methods: A comprehensive literature search was performed using PubMed, Web of Science, Embase, and the Cochrane Library from database inception to July 2024. The search was performed using the terms “spontaneous”, “regression”, “resorption”, “remission”, “absorption”, “herniation”, and “disc”. Manual searches were also performed to broaden the literature search. Studies were included if they reported at least one potential predictor of resorption in patients with LDH and provided follow-up imaging assessments (CT/MRI) to define resorption outcomes, along with the criteria used to determine the presence or absence of imaging resorption. Two reviewers independently searched the relevant literature and the ROBINS-I tool were used to assess the quality.
Results: The literature search yielded 1115 publications, of which 22 were finally included. The review suggested that the probability of resorption in LDH can be predicted by five aspects: clinical factors, type and size of the LDH, composition of the herniated IVD, imaging features of LDH, and spinal physiology. One limitation of this review is the lack of high-quality prospective studies among the included research, which may affect the accuracy of the findings.
Conclusion: The probability of resorption in LDH can be predicted based on five aspects. This helps clinicians preferentially select LDH cases with a high probability of resorption for conservative treatment, which is of positive significance for improving the success rate of conservative treatment in patients with LDH. However, due to the lack of high-quality prospective studies for support, large-scale prospective studies are necessary to assess the accuracy of these predictive factors for LDH resorption.
Keywords: lumbar disc herniation, resorption, predictive factors, review
Introduction
Lumbar disc herniation (LDH) is one of the most common diseases in orthopaedics, predominantly affecting individuals aged 30–50.1 Additionally, low back pain is a leading cause of labour force loss and disability, posing a heavy socioeconomic burden,2 and its incidence is increasing annually. Computed tomography (CT) and magnetic resonance imaging (MRI) have revealed that the herniated part of the intervertebral disc (IVD) undergoes spontaneously regression. Scholars have described this process using terms such as “regression”, “resorption”, “remission”, and “resolution”.3–6 In this paper, we uniformly refer to this phenomenon as “resorption”, which refers to the spontaneous volume reduction of the herniated part of the IVD without surgical intervention, and this change can usually be observed through imaging.(Figure 1) During the last 20 years, in-depth studies have focused on resorption in LDH, making great progress in the understanding of this phenomenon. This reduction or disappearance of the herniated IVD without surgical intervention, accompanied by significant improvement in clinical symptoms, provides the most direct basis for the non-surgical treatment of LDH.7,8
 |
Figure 1 MRI images demonstrating LDH resorption. (A–C) MRI shows L5/S1 intervertebral disc protrusion. (D–F) After 4 weeks of non-surgical treatment, MRI shows significant resorption. |
The mechanism of resorption is not fully understood, and its occurrence is often influenced by the patient age, disease duration, and size and type of LDH. Therefore, this review aims to address the key research question: Can the probability of resorption be predicted using these relevant factors? The present review focuses on the factors influencing resorption in LDH, providing clinicians with a stronger evidence base for formulating individualized and rational conservative treatment.
Materials and Methods
Literature Search Strategy
Two authors independently performed a literature search of four databases (PubMed, Web of Science, Embase, and the Cochrane Library) in July 2024, following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guideline.9 The search terms were “spontaneous”, “regression”, “resorption”, “remission”, “absorption”, “herniation”, and “disc”. The reference lists of the included articles were manually searched to broaden the literature search.
Inclusion Criteria
We selected all peer-reviewed studies on factors associated with resorption in LDH, without restriction of regions, publication types, or languages. The key inclusion criterion was that the study must mention, analyze, or discuss at least one potential predictive factor for LDH imaging resorption in its results or discussion. Eligible studies were required to include patients diagnosed with LDH by MRI or CT, and interventions were not restricted, allowing conservative management, routine clinical care, or the absence of any specific treatment, provided that the natural course of resorption could be observed. No specific comparison group was required; studies comparing different herniation types, clinical characteristics, imaging features, or follow-up outcomes were all eligible. Regarding outcomes, included studies needed to report at least one predictor associated with resorption, covering clinical, imaging, pathological, or mechanistic domains. Study designs were limited to prospective or retrospective cohort studies, case-control studies, and cross-sectional analyses. In addition, eligible studies were required to provide follow-up MRI or CT to evaluate resorption through imaging and/or clearly define the criteria used to determine resorption. The interval between the first and the last imaging follow-up should be more than 3 months.
Exclusion Criteria
The exclusion criteria were articles unrelated to resorption in LDH, articles of no value for resorption prediction, review-based articles, and case reports. Studies lacking follow-up imaging, studies without extractable predictor information, or studies that did not provide a definition of imaging resorption were also excluded.
Data Extraction
Two independent reviewers extracted relevant information from the literature regarding diagnosis, predictive factors, follow-up time, number of cases, imaging examination (CT/ MRI) used, and results (whether resorption occurred). Disagreements were resolved by consensus.
Quality Assessment
Articles that met the selection criteria were independently assessed by the authors for quality using the ROBINS-I tool.10 In accordance with the ROBINS-I guidelines, articles were assessed for each item according to the following rating scale: low risk of bias, moderate risk of bias, critical risk of bias and no information. Articles with critical risk of bias or serious risk of bias were be excluded from the review. The relevant results are presented in the form of a risk bias plot.
Results
Study Design and Characteristics
In total, 1115 publications were retrieved. After removing duplicates, 635 studies remained for screening. Irrelevant literature was eliminated by browsing the titles and abstracts of the included studies. Finally, the quality of 24 publications was assessed. Quality assessment revealed 2 articles are of critical risk of bias and have been excluded. The outcomes are summarized in Figure 2. Finally, 22 studies were included in this review (Figure 3).
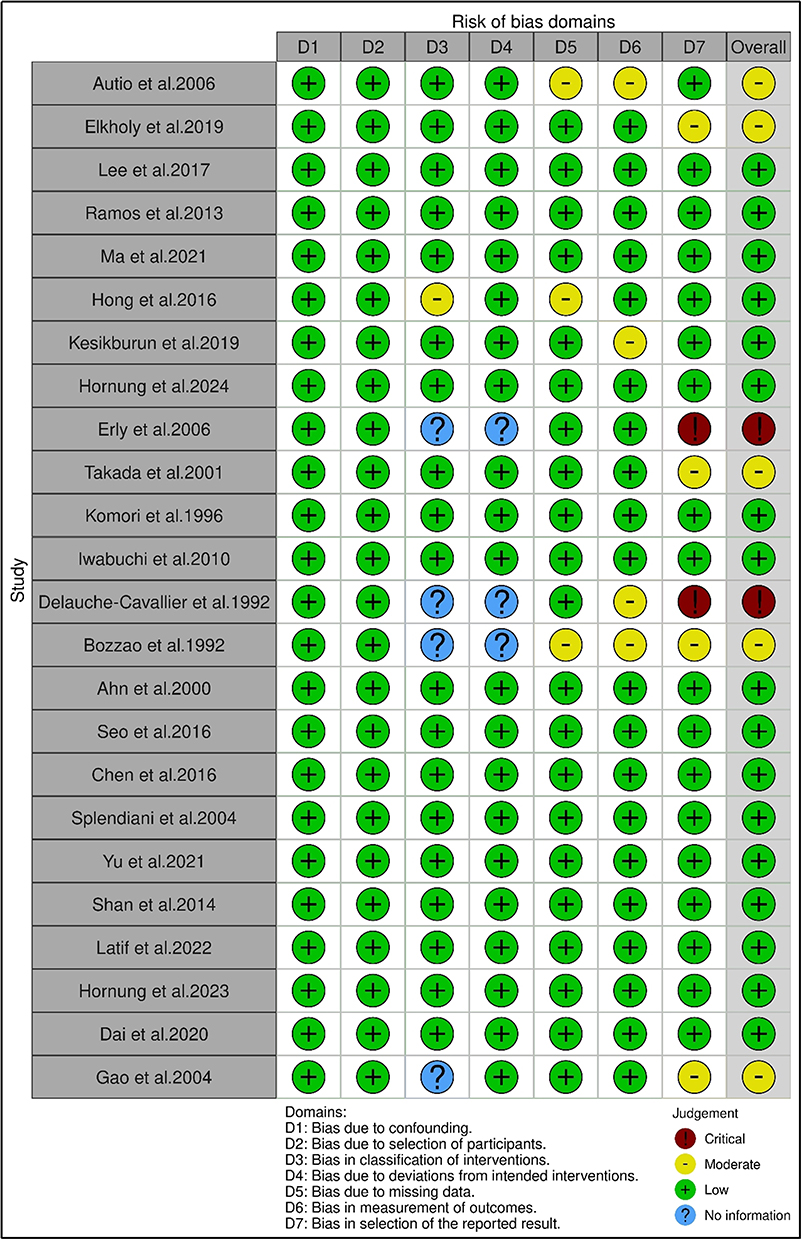 |
Figure 2 Risk assessment of bias of the included studies. |
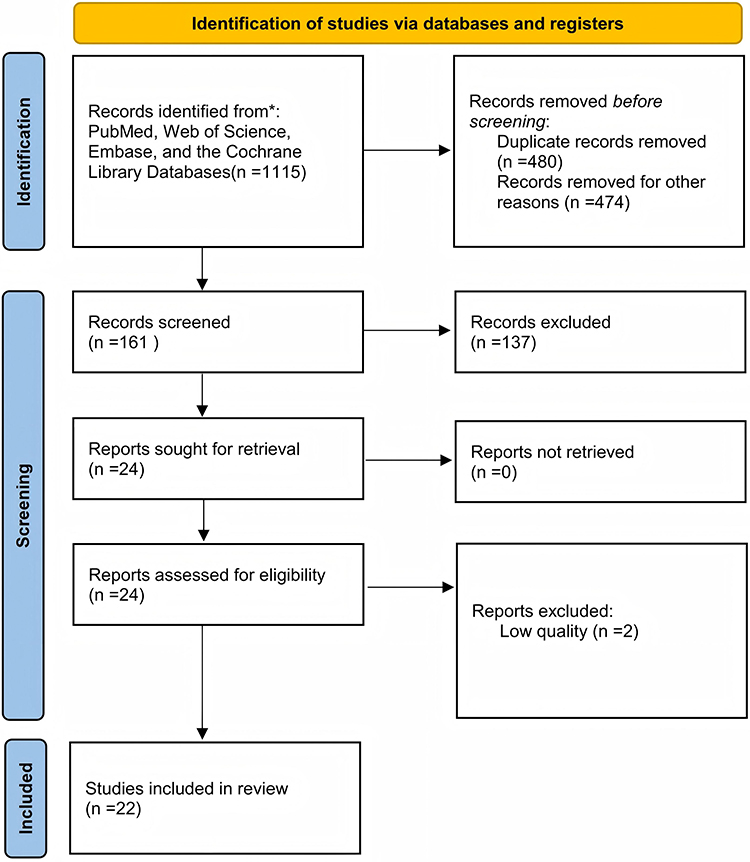 |
Figure 3 PRISMA flowchart of the articles selection process. Notes: Adapted from Page MJ, McKenzie JE, Bossuyt PM et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 2021;372:n71. doi: 10.1136/bmj.n71.9 |
All of the included studies were observational study design, with 9 prospective studies included. Comparative Tables 1–5 lists the relevant data and describes the results of these studies. The purpose of all included studies was to investigate the predictive factors associated with LDH resorption.
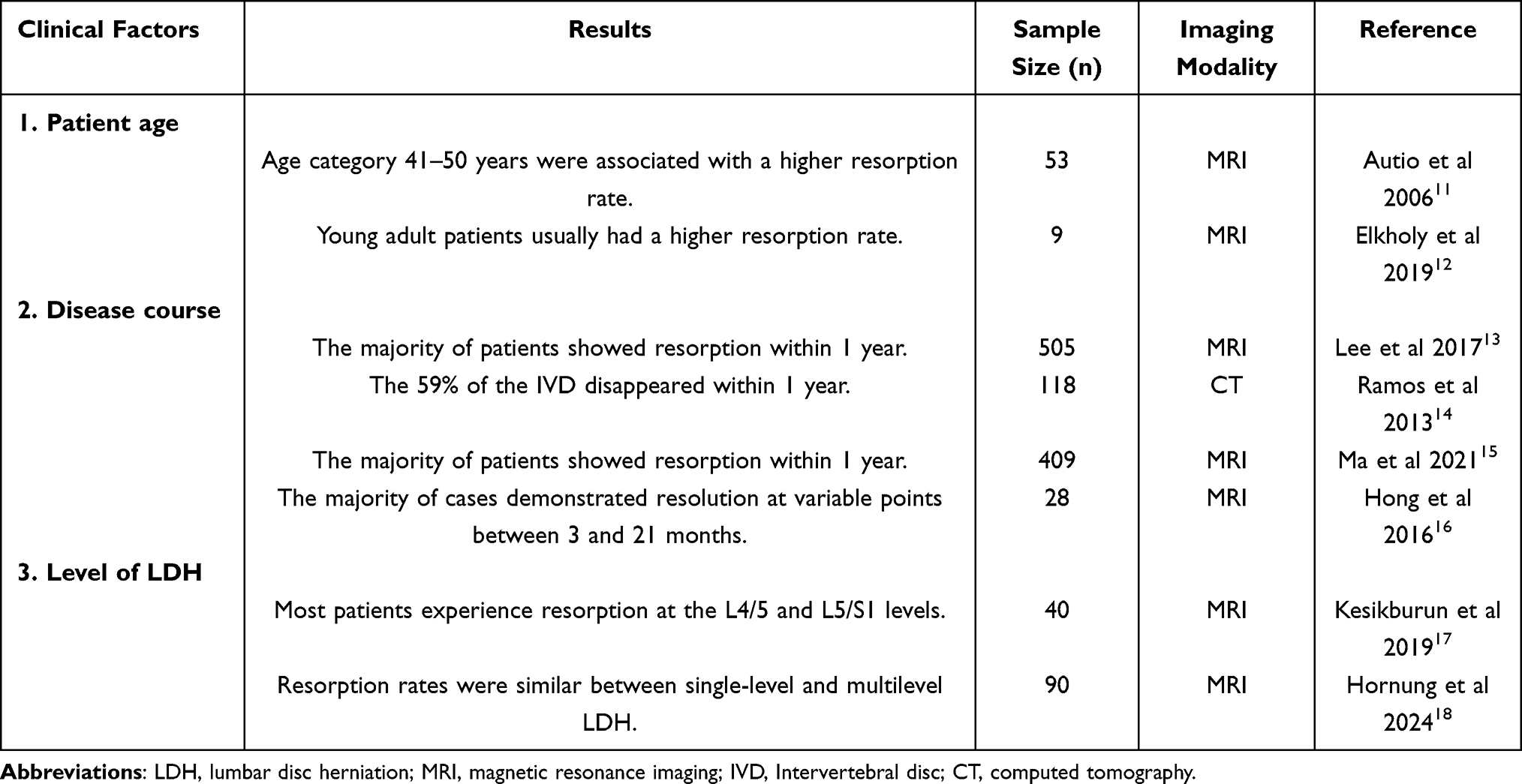 |
Table 1 Prediction of Resorption by Clinical Factors |
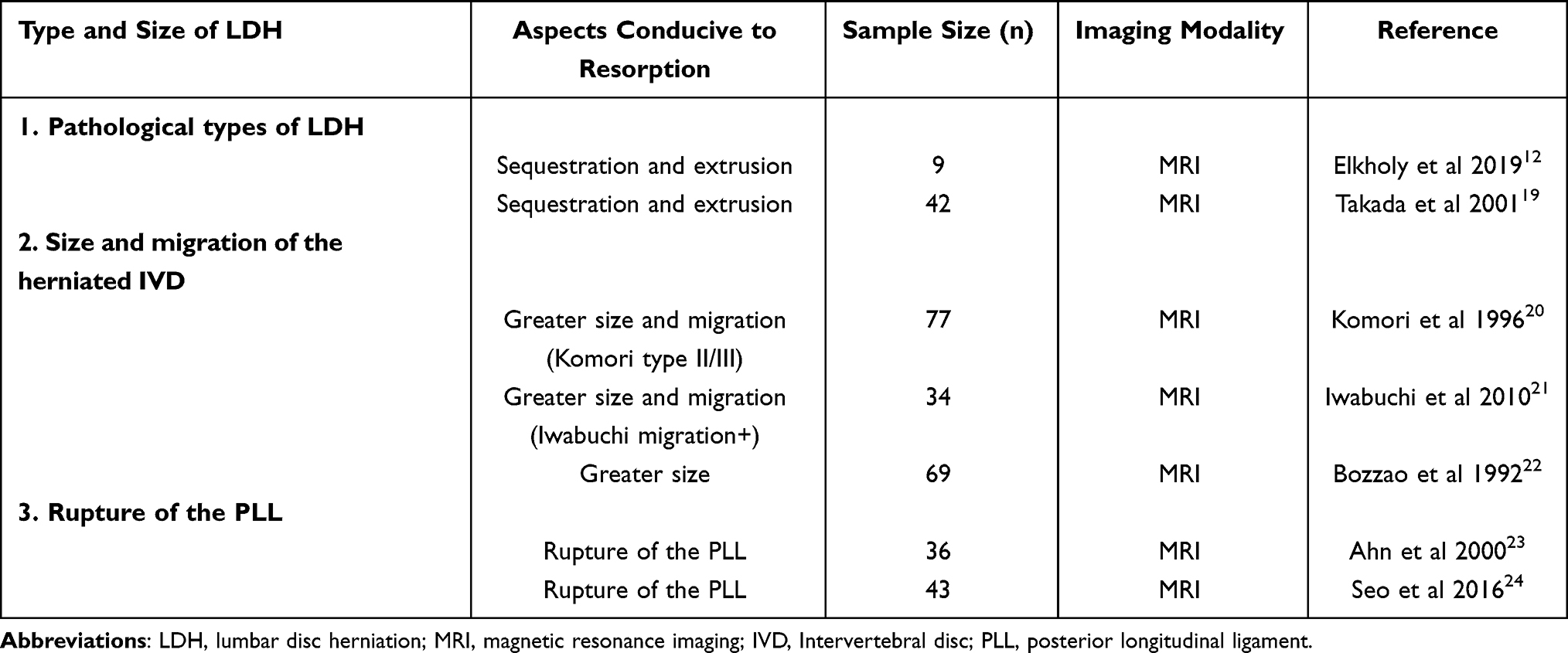 |
Table 2 Prediction of Resorption by Type and Size of LDH |
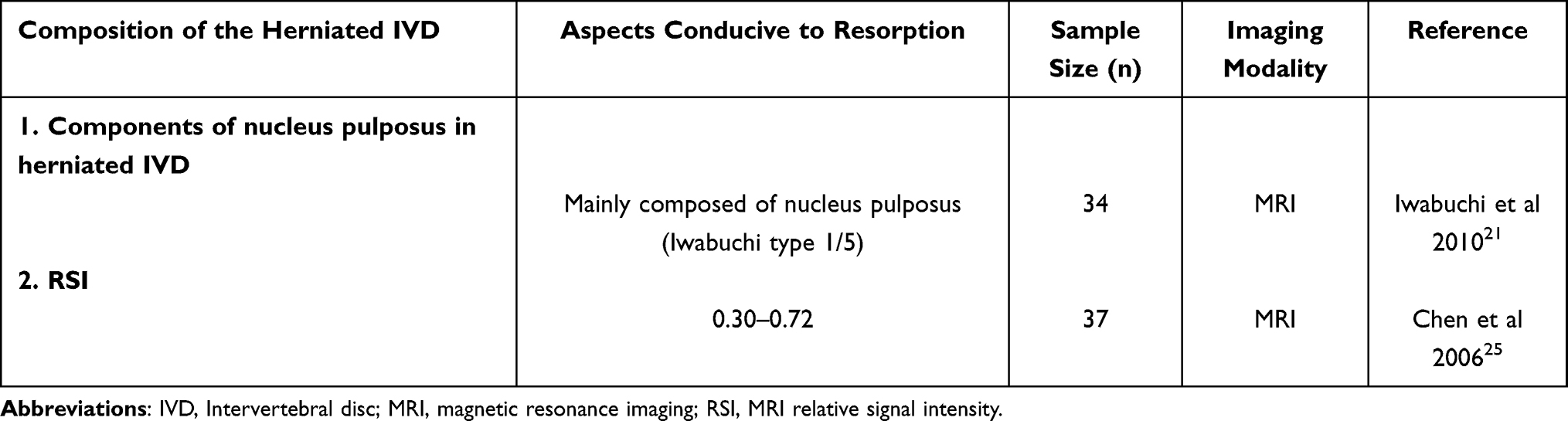 |
Table 3 Prediction of Resorption by Composition of the Herniated IVD |
 |
Table 4 Prediction of Resorption by Imaging Features of LDH |
 |
Table 5 Prediction of Resorption by Spinal Physiology |
Clinical Factors
The available literature suggested that patient age, disease course, and level of disc herniation were correlated with the occurrence of resorption (Table 1). It was generally accepted that resorption was more likely to occur in young and middle-aged patients than in older patients, and the active period for resorption was within 1 year of onset.11,15
Patient Age
Autio et al showed that patients with LDH in the 41- to 50-year age group had a high rate of resorption, and a recent retrospective study reported a similar finding.11,12 It is generally accepted that the probability of resorption is higher in young and middle-aged patients than in older patients, which may be related to the degree of degeneration of the intervertebral disc. In mildly to moderately degenerated discs, there are changes in the extracellular matrix along with senescence and apoptosis of the nucleus pulposus cells. These changes are often accompanied by an inflammatory immune response or the growth of microvessels,33–35 which are conditions conducive to resorption.
Disease Course
In the early stages of LDH, the nucleus pulposus breaks through the fibrous ring of the disc and contacts the bloodstream. This induces high expression of various inflammatory factors and immunoproteins, making the early stage of LDH a critical period for resorption. Previous case reports have shown that the longest LDH resorption occurred 4 years after the onset of the disease.36 Follow-up MRI has confirmed that the active period of resorption occurs within 1 year after onset,13,14,37 during which time patients may experience remission of clinical symptoms, and some may experience significant resorption or even disappearance of the herniated IVD. Ma et al performed non-surgical treatment in 409 patients with giant LDH, and 189 patients experienced resorption. Among these patients, 128 (67.72%) experienced resorption within 1 year of onset.15 Macki et al reported 53 cases of ruptured LDH resorption. Follow-up MRI showed that the time to resorption after LDH was 9.27 ± 13.32 months.38 Hong et al conducted a retrospective review of 28 patients who underwent at least two MRI examinations and found that most cases of massive LDH demonstrated resolution at variable time points between 3 and 21 months.16
Level of Disc Herniation
The most common levels of LDH are L4/5 and L5/S1,39 with approximately 95% of herniations occurring in these two levels.40 Because of the high pressure and stress concentration on these two levels and the relative weakness of the posterior longitudinal ligament (PLL), the degenerated fibrous ring is prone to rupture under external forces and is therefore prone to protrusion.41 L4/5 and L5/S1 are also the levels at which LDH resorption is most likely to occur. Kesikburun et al analysed 40 patients with LDH resorption and found that the levels at which resorption occurred were L4/5 and L5/S1 in 70% of the patients.17 Macki et al found that the highest rate of resorption occurred at L4/5 (58.3%), followed by L5/S1 (25.0%), L1/2 (4.2%), and L2/3 (0.0%).38 Resorption rates were similar between single-level and multilevel LDH at various time points throughout a prospective assessment, providing insights that disc healing may have unique programmed signatures.18
Effect of Body Weight on Resorption
Obesity and a high body mass index (BMI) are thought to increase the risk of lumbar spine degeneration,42,43 which can further contribute to the LDH. Tokmak et al reported a case of LDH resorption in a 42-year-old woman following weight loss and suggested that dehydration and increased endothelial cell proliferation were possible mechanisms for the resorption.44 However, other case studies have come to the opposite conclusion. Hornung et al analysed the BMI of 90 patients with LDH resorption and found no difference between patients with resorption within 3 months and after 3 months.30 Kesikburun et al prospectively analysed 40 patients with LDH, among whom 4 patients showed no resorption, 6 patients developed partial resorption, and 30 patients developed complete resorption, with no difference in BMI among the three groups.17 Therefore, the effect of body weight on resorption is currently unclear, and further evidence is needed.
Type and Size of LDH
Pathological Types of LDH
The pathological types of LDH can be broadly classified into four types: bulging, protrusion, extrusion, and sequestration.45,46 The literature suggests that the extrusion and sequestration forms of LDH are prone to resorption.47,48 In a study by Elkholy et al, resorption occurred in 9 of 289 patients with LDH, 5 of whom had the sequestration type and 4 of whom had the extrusion type.12 Chiu et al examined the probability of resorption in different types of LDH and reported resorption rates of 96%, 70%, 41%, and 13% for the sequestration, extrusion, protrusion, and bulging types, respectively.49 Takada et al performed MRI follow-up of 42 patients with LDH who received conservative treatment and showed that of the protrusion (n=7), extrusion (n=17), and sequestration (n=18) types, the sequestration type was most likely to undergo resorption, followed by the extrusion type.19 Some published case reports have shown that LDH resorption occurs mostly in the extrusion and sequestration forms.50,51
Size and Migration of the Herniated IVD
Many cases of large LDH resorption have been reported52–54 Regarding the size and migration of the LDH, a large herniated IVD with a greater degree of migration is more likely to undergo resorption than is a small herniated IVD with less extensive migration.46 Komori et al proposed a typology based on the size and migration of the herniated IVD (Figure 4).20 The authors classified LDH into three types (I–III) based on the degree of migration of the herniated IVD on MRI. The distinction between types I and II lay in whether the black line behind the herniated disc tissue was interrupted; interruption or disappearance of this line indicated that the herniated tissue had crossed the PLL. The distinction between type II and type III lay in whether the herniated disc exceeded the height of the parent disc. Type III was further divided into three levels based on the herniated disc height as a proportion of the vertebral body height (Figure 5). Clinical observations have shown that the probability of resorption in LDH increases with the degree of migration. Similar to the Komori classification, Iwabuchi et al classified LDH migration into two categories, namely with or without migration of the herniated IVD, using one-quarter of the vertebral body height as the boundary. MRI follow-up of 34 patients with LDH revealed 21 cases of resorption, there were more patients with migration in the resorption group.21 Bozzao et al also confirmed that resorption is related to the initial size of the herniated IVD and that a large initial size is more prone to resorption.22
 |
Figure 4 Komori classification. Type I: The blackline behind the herniated disc tissue is intact. Type II: The blackline behind the herniated disc tissue is ruptured. Type III: The herniated disc exceeds the height of the parent disc. |
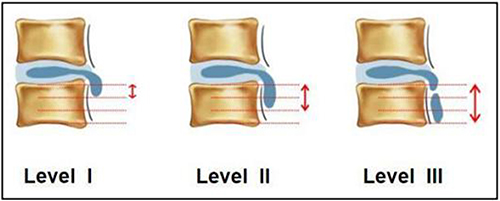 |
Figure 5 Levels of type I to III LDH in the Komori classification. Level I: Migration of the herniated disc by one-third of the vertebral body height. Level II: Migration of the herniated disc by two-thirds of the vertebral body height. Level III: Migration of the herniated disc by the full vertebral body height. |
Rupture of the PLL
LDH can be classified as ruptured or non-ruptured depending on whether the PLL is ruptured. Ahn et al used MRI to follow up 36 patients with different types of LDH and divided the patients into 3 groups: those with subligamentous, transligamentous, and sequestered herniations. The authors reported 56%, 79%, and 100% shrinkage, respectively, for each type and concluded that herniated disc material protruding from the PLL was beneficial for resorption.23 Seo et al followed up 56 levels of herniated IVDs by MRI in 43 patients with LDH, finding eventual resorption in 35 levels and significantly more patients with (56/22) than without (56/13) PLL rupture.24 Therefore, the authors concluded that larger migrating herniations tend to regress more readily than smaller herniations because penetration of the annulus fibrosus or PLL exposes disc material to the systemic circulation in the epidural space, thereby enhancing cellular inflammatory reactions. Only when the PLL ruptures does the herniated IVD have access to the blood flow, triggering the various mechanisms that promote resorption. The extrusion and sequestration types of LDH, Komori types II and III LDH, and LDH with Iwabuchi migration are pathologically classified as ruptured LDH, which favours resorption (Table 2).
Composition of the Herniated IVD
Components of Nucleus Pulposus in Herniated IVD
The lumbar IVD consists of the nucleus pulposus, fibrous ring, and cartilaginous endplate. Iwabuchi et al studied the predictive value of the protruding tissue components for resorption and classified the herniated IVD components into five types based on the different signal characteristics of herniated disc tissue on T1- and T2-weighted MRI: type 1, mostly nucleus pulposus; type 2, mostly fibrous ring; type 3, mucinous-like changes; type 4, granulation tissue hyperplasia; and type 5, partially fibrous ring. Of these five types, type 1 (T1-weighted isointense signal, T2-weighted high signal intensity) and type 5 (T1-weighted low signal intensity, T2-weighted isointense signal) are susceptible to resorption, whereas types 2 to 4 undergo almost no resorption.21 In a herniated IVD in which the nucleus pulposus is the main component, the water content is high and the degree of denaturation is low; therefore, an immune response and tissue dehydration are likely to occur, leading to resorption. The immune response, and dehydration and contraction of the herniated nucleus pulposus are two important hypotheses for the mechanism underlying resorption in LDH.4,38,55
MRI Relative Signal Intensity
The MRI relative signal intensity (RSI) of the herniated IVD allows a more objective analysis of the composition and degree of degeneration of the LDH. On MRI, RSI is defined as the ratio of the signal intensity of the herniated IVD to the signal intensity of the cerebrospinal fluid at the same level.25 As mentioned, the nucleus pulposus has a high water content and, therefore, appears with relatively high signal intensity on MRI. Another factor affecting the RSI of the herniated IVD is the degree of degeneration of the LDH, with MRI signal intensity decreasing with increasing degeneration of the disc within a certain range. Studies have shown that mild to moderate degenerated LDH is associated with a stronger inflammatory response compared with severe degenerated LDH, which facilitates resorption.56 Chen et al analysed the RSI and resorption rates of 39 intervertebral disc MRIs from 37 patients and found that macrophage infiltration as well as the degree of neovascularisation in herniated tissue specimens peaked when the RSI was 0.30–0.72.25
Prediction of resorption based on composition of the herniated IVD is shown in Table 3.
Imaging Features of LDH
MRI Signal Enhancement Around the Herniated IVD
Once herniation has occurred, the extruded material is recognized by the immune system, and the resultant inflammatory response begins the degradation process.57 This results in granulation tissue formation around the herniated tissue and new blood vessel in-growth. These changes manifest as the “bull’s eye sign” on enhanced MRI (ie, increased circumferential signal strength with no strengthening of the signal in the central IVD).14 Autio et al used MRI to predict resorption in patients with LDH and found that resorption was more likely with greater thickness and stronger signals at the edge of the annular enhancement than with thin and weaker signals.11 In accordance with ongoing research, some scholars have further classified the “bull’s eye sign” to better predict resorption. Yu et al selected the level of the herniated IVD with the greatest extent of herniation on T1-weighted images in the horizontal view on contrast-enhanced MRI, then divided the LDH into three types (A to C) according to the size of the marginal annular enhancement around the herniated IVD (Figure 6). The authors evaluated 64 patients with LDH: 26 patients with type A, 23 with type B, and 15 with Type C. The patients were followed up for 12 to 34 months, and 42 patients completed non-surgical treatment. The success rates of non-surgical treatment for types A, B, and C were 88.46%, 69.57%, and 20.00%, respectively. Resorption occurred in 32 patients with types A and B, whereas no resorption occurred in patients with type C.27
 |
Figure 6 Classification of the “bull’s eye sign” on enhanced MRI. (A), (D), and (G) Level at which the herniated IVD was most prominent on plain MRI T2WI in the horizontal view. (B), (E), and (H) Level at which the herniated IVD was most prominent on enhanced MRI T1WI in the horizontal view. (C), (F), and (I) Schematic diagram of the enhanced area of the herniated IVD ring. Type A shows a complete bull’s eye sign, and the annular enhanced area surrounds the entire herniated nucleus pulposus. Type B shows the annular enhanced area partially surrounding the herniated nucleus pulposus. In Type C, there is no obvious annular enhancement around the herniated disc. |
Modic Changes
Modic changes are an influential factor in LDH resorption, and resorption is more likely to occur in the absence of adjacent vertebral Modic changes. Modic changes in the vertebral body indicate a high degree of disc degeneration. Highly degenerated disc tissue is not conducive to resorption because of the loss of water and increased cartilage composition.11,58 Similarly, histological studies have shown that some IVD tissue with Modic changes contains more cartilaginous endplate components and exhibits less neovascularisation and macrophage infiltration, characteristics that are not conducive to resorption.28,29 This phenomenon may be related to the difficulty of proteoglycan reduction and inflammatory cell invasion in hyaline cartilage.59 Prediction of resorption based on imaging features of LDH is shown in Table 4.
Spinal Physiology
Sacral Slope
Hornung et al designed a prospective study to predict the factors associated with LDH resorption. This study included 93 patients with acute symptomatic LDH, and all patients experienced resorption within 1 year. Multivariate modelling showed that a greater L4 posterior vertebral height, greater sacral slope, and larger herniated volume at baseline were most predictive of early resorption.30 A small sacral slope has been suggested as a contributing factor in the development of LDH.60,61 A greater sacral slope reduces the pressure on the disc, potentially stimulating self-ablation mechanisms in a low-pressure environment. Notably, a recent retrospective study came to the opposite conclusion. In a retrospective analysis of 67 patients with LDH, Dai et al found no statistically significant difference in the sacral slope between patients with and without resorption. Therefore, further research is needed to demonstrate the relationship between the sacral slope and resorption.31
Spinal Canal Morphology
Based on its cross-sectional morphology, the spinal canal can be divided into three categories: elliptical, triangular, and trilobar.32 Elliptical canals have the largest area, followed by triangular and trilobar canals; therefore, herniated material in elliptical canals is prone to resorption in LDH because of the relatively rich blood supply. Another possible factor contributing to resorption is that the large space within elliptical spinal canals accommodates the nucleus pulposus tissue well. Even if the herniated material is substantial, nerve compression is less pronounced, leading to milder clinical symptoms.62 Furthermore, patients with mild clinical symptoms are more likely to be treated non-surgically, which involves a lower risk of nerve injury and facilitates the possibility of resorption.
Prediction of resorption based on spinal physiology is shown in Table 5.
Discussion
The Mechanisms of LDH Resorption
The mechanisms of LDH resorption is recognized to be related to the following factors: immune privilege and inflammation, neovascularization, extracellular matrix metabolic imbalance, dehydration, and mechanical shrink of the herniated IVD.46,57 Of these mechanisms, immune privilege and inflammation is the most widely studied, and most of the aspects of predicting resorption mentioned earlier are related to it. For example, younger patients, rupture of the PLL, bull’s eye sign and large size of IVD all indicate a higher degree of inflammatory response.
There is no blood supply in the intervertebral disc tissue, isolating the nucleus pulposus tissue from the host immune system, and is considered an immune-privileged tissue.63 When the immune privilege barrier is damaged, such as when the herniated IVD breaks through the annulus fibrosus and PLL and is exposed to the immune environment, an autoimmune reaction is triggered.46,64–66 This leads to a variety of pathological processes such as neovascularisation and immune cell infiltration. Ratsep et al examined the surgically excised lumbar disc specimens of 29 patients with non-contained (PLL ruptures) disc herniations and 21 patients with contained disc herniations. The authors concluded that severe histodegeneration is associated with enhanced neovascularisation and potentially spontaneous regression of the herniated IVD.67 Macrophages play an important role in the process of LDH resorption. When disc herniation occurs, factors such as tumour necrosis factor-α, monocyte chemoattractant protein-1, and interleukin (IL)-8 promote macrophage recruitment, creating conditions favourable for neovascularisation and inflammatory responses.68,69 Factors that participate in macrophage-associated inflammatory cascades include IL-6, IL-8, prostaglandin E2, and cyclooxygenase-2.46 Arai et al observed the histological changes in the extruded and sequestrated IVD. Immunohistological staining of the area with inflammatory cell infiltration revealed the presence of T cells and macrophages. Therefore, the authors concluded that LDH resorption may have resulted from the phagocytic activities of these cells.70 In addition, MMPs are an important mediator in the process of LDH resorption and are thought to contribute to IVD degradation (Figure 7).
 |
Figure 7 Immune mechanism of resorption in LDH. When disc herniation occurs and the PLL ruptures, the body recruits macrophages into the herniated disc, causing secretion of immune factors such as IL-6, IL-8, PGE2, COX-2, MMPs, and VEGF. The herniated IVD is eventually resorbed under the effects of inflammation, neovascularisation, and enzymatic degradation. Abbreviations: LDH, lumbar disc herniation; PLL, posterior longitudinal ligament; IL, interleukin; PGE2, prostaglandin E2; COX-2, cyclooxygenase-2; MMPs, matrix metalloproteinases; VEGF, vascular endothelial growth factor; IVD, Intervertebral disc. |
“Inflammation-Preserving” Treatment
Non-steroidal anti-inflammatory drugs are considered effective in the treatment of LDH, providing relief of low back pain and improving function.71,72 Other recommended drugs include glucocorticoids and steroids.73,74 The use of these drugs benefits patients by blocking the inflammatory reaction and thus improving symptoms. However, disruption of the inflammatory reaction can also have an impact on resorption. In an animal study, Minamide et al performed histological observations of intervertebral discs in 36 rabbits and found that lipopolysaccharide accelerated the replacement of grafted intervertebral disc by fibrous tissue.75 This finding suggests that resorption of the disc occurred in the epidural space of the rabbit, whereas high-dose steroids suppressed the replacement. In addition, Aydin et al observed disc specimens from 50 patients who had been treated with cyclooxygenase-2 inhibitors and found that most of the specimens showed no significant inflammatory reaction.76 By contrast, Buttermann et al concluded that epidural steroid injections relieved clinical symptoms and had no effect on LDH resorption.77 Therefore, for patients whose symptoms are not serious or who can tolerate their symptoms, “inflammation-preserving” treatment can be administered under close observation. Such treatment may be conducive to resorption.
The Value of Contrast-Enhanced MRI for Predicting LDH Resorption
The value of contrast-enhanced MRI for prediction of LDH resorption has been suggested. Splendiani et al evaluated 64 patients, affected by 72 lumbar disk herniations. At MRI follow-up exams regression of disk herniation was observed in 34.72% of cases. Among these, herniations with peripheral contrast-enhancement in 83% of cases.26 Sakai et al reported a case of resorption in a patient with recurrent intradural LDH and reviewed the MRI findings. Gadolinium-enhanced MRI showed rim enhancement not only at the initial presentation but also at recurrence.4, A recently published prospective follow-up study, which included a total of 82 patients, also confirmed the value of contrast-enhanced MRI in predicting LDH resorption.78 Notably, although contrast-enhanced MRI has shown value in predicting resorption, the clinical use of this technique is limited by the risks associated with the use of contrast agents, including allergic reactions and impaired renal function.79,80
In addition, since the occurrence of resorption requires a process, there is a possibility that some patients may experience resorption during the process of waiting for symptom relief. Therefore, we need to attach importance to the value of “waiting”. For patients with a high probability of resorption, conservative treatment can be chosen in the absence of progressive neurological impairment, cauda equina syndrome, urgent impacts on daily life, and standardized non-surgical treatment shows no efficacy.
Limitations of the Current Evidence
However, the current understanding of LDH resorption and its predictive factors is constrained by several methodological limitations. Primarily, there is a notable scarcity of high-quality prospective clinical studies specifically designed to investigate this phenomenon. The natural history of resorption requires long-term and regular imaging follow-up to accurately document its progression. This presents significant practical challenges, including poor patient compliance due to the asymptomatic nature of resorption in many cases and the substantial financial burden associated with repeated MRI scans. These factors inevitably lead to missing data and attrition bias in cohorts, ultimately compromising the robustness and generalizability of the findings. Future research should prioritize well-designed, multi-center prospective cohort studies with standardized imaging protocols and follow-up schedules.
Conclusion
Resorption is an objective phenomenon in patients with LDH. Patients’ clinical factors, type and size of the LDH, composition of the herniated IVD, imaging features of the LDH, and spinal physiology may predict the probability of natural resorption of the herniated disc. Thus, clinicians should fully consider the possibility of resorption before making therapeutic strategy for patients with LDH. In addition, the development of various disease prediction models has become increasingly sophisticated today. Future research could integrate imaging biomarkers with clinical and biological predictive factors to further refine this study.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
This study is a review that synthesizes data from previously published literature. Ethics approval was not required as no original human participants or experimental procedures were involved.
Acknowledgments
The authors would like to appreciate all the staff of the participating scientific research.
Author Contributions
Xueqiang Shen: Conceptualization, Methodology, Formal analysis, Writing - original draft.
Feng Dai: Data curation, Formal analysis, Validation, Writing - review & editing.
Zihang Li: Data curation, Visualization, Software, Writing - review & editing.
Hong Jiang: Investigation, Validation, Writing - review & editing.
Jintao Liu: Investigation, Validation, Writing - review & editing.
Jianwei Wang: Supervision, Project administration, Resources, Writing - review & editing.
Pengfei Yu: Supervision, Conceptualization, Funding acquisition, Writing - review & editing.
All authors agreed to the final version submitted for publication; agreed to submitting this paper to Journal of Inflammation Research; and agree to be accountable for the content of this paper.
Funding
This work was supported by Suzhou Municipal Health Commission (NO. KJXW2023047; NO. GSWS2022084), Suzhou Wumen Medical School Research Special Research Fund (NO. SYWD2024298), National Natural Science Foundation of China (NO. 82374220; NO. 82474529), Jiangsu Provincial Science and Technology Development Program of Traditional Chinese Medicine (NO. MS2025067). The funding body had no participation in the study’s design, data collection, analyses, and writing the paper.
Disclosure
The authors declare that they have no competing interests.
References
1. Penchev P, Ilyov IG, Todorov T, Petrov P, Traykov P. Comprehensive analysis of treatment approaches for lumbar disc herniation: a systematic review. Cureus. 2024;16(8):e67899. doi:10.7759/cureus.67899
2. GBD 2019 Diseases and Injuries Collaborators. Global burden of 369 diseases and injuries in 204 countries and territories, 1990-2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet. 2020;396(10258):1204–16. doi:10.1016/s0140-6736(20)30925-9
3. Rashed S, Vassiliou A, Starup-Hansen J, Tsang K. Systematic review and meta-analysis of predictive factors for spontaneous regression in lumbar disc herniation. J Neurosurg Spine. 2023;39(4):471–478. doi:10.3171/2023.6.SPINE23367
4. Sakai T, Tsuji T, Asazuma T, Yato Y, Matsubara O, Nemoto K. Spontaneous resorption in recurrent intradural lumbar disc herniation. Case report. J Neurosurg Spine. 2007;6(6):574–578. doi:10.3171/spi.2007.6.6.11
5. Çitişli V, Ibrahimoğlu M. Spontaneous remission of a big subligamentous extruded disc herniation: case report and review of the literature. Korean J Spine. 2015;12(1):19–21. doi:10.14245/kjs.2015.12.1.19
6. Chiang JY, Chen DC, Cho DY. Spontaneous resolution of a large lumbar disc herniation. Joint Bone Spine. 2017;84(4):495. doi:10.1016/j.jbspin.2016.09.011
7. Hong J, Ball PA. Images in clinical medicine. resolution of lumbar disk herniation without surgery. N Engl J Med. 2016;374(16):1564. doi:10.1056/NEJMicm1511194
8. Dai F, Dai YX, Jiang H, Yu PF, Liu JT. Non-surgical treatment with XSHHD for ruptured lumbar disc herniation: a 3-year prospective observational study. BMC Musculoskelet Disord. 2020;21(1):690. doi:10.1186/s12891-020-03723-2
9. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021:
10. Morche J, Freitag S, Hoffmann F, et al. GRADE guidelines: 18. How ROBINS-I and other tools to assess risk of bias in nonrandomized studies should be used to rate the certainty of a body of evidence. Z Evidenz Fortbild Q. 2020;150-152:124–133. doi:10.1016/j.zefq.2019.11.003
11. Autio RA, Karppinen J, Niinimäki J, et al. Determinants of spontaneous resorption of intervertebral disc herniations. Spine. 2006;31(11):1247–1252. doi:10.1097/01.brs.0000217681.83524.4a
12. Elkholy AR, Farid AM, Shamhoot EA. Spontaneous resorption of herniated lumbar disk: observational retrospective study in 9 patients. World Neurosurg. 2019;124:e453–e459. doi:10.1016/j.wneu.2018.12.115
13. Lee J, Kim J, Shin JS, et al. Long-term course to lumbar disc resorption patients and predictive factors associated with disc resorption. Evid Based Complement Alternat Med. 2017;2017:2147408. doi:10.1155/2017/2147408
14. Ramos Amador A, Alcaraz Mexía M, González Preciado JL, Fernández Zapardiel S, Salgado R, Páez A. Natural history of lumbar disc hernias: does gadolinium enhancement have any prognostic value? Radiologia-Madrid. 2013;55(5):398–407. doi:10.1016/j.rx.2011.10.011
15. Ma Z, Yu P, Jiang H, et al. Conservative treatment for giant lumbar disc herniation: clinical study in 409 cases. Pain Physician. 2021;24(5):E639–e648.
16. Hong SJ, Kim DY, Kim H, Kim S, Shin KM, Kang SS. Resorption of massive lumbar disc herniation on MRI treated with epidural steroid injection: a retrospective study of 28 cases. Pain Physician. 2016;19(6):381–388.
17. Kesikburun B, Eksioglu E, Turan A, Adiguzel E, Kesikburun S, Cakci A. Spontaneous regression of extruded lumbar disc herniation: correlation with clinical outcome. Pak J Med Sci. 2019;35(4):974–980. doi:10.12669/pjms.35.4.346
18. Hornung AL, Rudisill SS, Barajas JN, et al. How does resorption differ among single-level and multilevel lumbar disc herniations? A prospective multi-imaging and clinical phenotype study. Spine. 2024;49(11):763–771. doi:10.1097/brs.0000000000004955
19. Takada E, Takahashi M, Shimada K. Natural history of lumbar disc hernia with radicular leg pain: spontaneous MRI changes of the herniated mass and correlation with clinical outcome. J Orthop Surg. 2001;9(1):1–7. doi:10.1177/230949900100900102
20. Komori H, Shinomiya K, Nakai O, Yamaura I, Takeda S, Furuya K. The natural history of herniated nucleus pulposus with radiculopathy. Spine. 1996;21(2):225–229. doi:10.1097/00007632-199601150-00013
21. Iwabuchi M, Murakami K, Ara F, Otani K, Kikuchi S. The predictive factors for the resorption of a lumbar disc herniation on plain MRI. Fukushima J Med Sci. 2010;56(2):91–97. doi:10.5387/fms.56.91
22. Bozzao A, Gallucci M, Masciocchi C, et al. Lumbar disk herniation: MR imaging assessment of natural history in patients treated without surgery. Radiology. 1992;185(1):135–141. doi:10.1148/radiology.185.1.1523297
23. Ahn SH, Ahn MW, Byun WM. Effect of the transligamentous extension of lumbar disc herniations on their regression and the clinical outcome of sciatica. Spine. 2000;25(4):475–480. doi:10.1097/00007632-200002150-00014
24. Seo JY, Roh YH, Kim YH, Ha KY. Three-dimensional analysis of volumetric changes in herniated discs of the lumbar spine: does spontaneous resorption of herniated discs always occur? Eur Spine J. 2016;25(5):1393–1402. doi:10.1007/s00586-014-3587-1
25. Chen QX, Liu YS, Li FC. Histopathological changes of sequestration-type lumbar herniated disc. Chin J Orthop. 2006;26(8):539–543. doi:10.3760/j.issn:0253-2352.2006.08.009
26. Splendiani A, Puglielli E, De Amicis R, Barile A, Masciocchi C, Gallucci M. Spontaneous resolution of lumbar disk herniation: predictive signs for prognostic evaluation. Neuroradiology. 2004;46(11):916–922. doi:10.1007/s00234-004-1232-0
27. Yu P, Jiang H, Ma Z, et al. The outcome predicted value of enhanced MRI for prolapsed or sequestrated lumbar disc herniation. Chin J Orthop. 2021;41(18):1350–1360. doi:10.3760/cma.j.cn121113-20200804-00481
28. Shan Z, Fan S, Xie Q, et al. Spontaneous resorption of lumbar disc herniation is less likely when modic changes are present. Spine. 2014;39(9):736–744. doi:10.1097/brs.0000000000000259
29. Latif R, Imran S, Ahmad I, Ilyas MS, Aziz A, Zehra U. Vertebral endplate changes correlate with presence of cartilaginous endplate in the herniated disc tissue: factor predicting failure of conservative treatment. Asian Spine J. 2022;16(2):212–220. doi:10.31616/asj.2021.0106
30. Hornung AL, Barajas JN, Rudisill SS, et al. Prediction of lumbar disc herniation resorption in symptomatic patients: a prospective, multi-imaging and clinical phenotype study. Spine J. 2023;23(2):247–260. doi:10.1016/j.spinee.2022.10.003
31. Dai G, Wang F, Liu L, et al. Sagittal balance parameters correlate with resorption of the lumbar disc extrusion: results of a retrospective study. Sichuan Da Xue Xue Bao Yi Xue Ban. 2020;51(4):533–539. doi:10.12182/20200760205
32. Gao L, Cui H, Tian Z. Research on internal absorption and related factors after protrasion of intervertebral disc in lumbar. Chin J Tradi Med Trauma & Orthop. 2004;12(5):17–19. doi:10.3969/j.issn.1005-0205(2004)05-0017-03
33. Zhang GZ, Deng YJ, Xie QQ, et al. Sirtuins and intervertebral disc degeneration: roles in inflammation, oxidative stress, and mitochondrial function. Clin Chim Acta. 2020;508:33–42. doi:10.1016/j.cca.2020.04.016
34. Chen J, Mei Z, Huang B, et al. IL-6/YAP1/β-catenin signaling is involved in intervertebral disc degeneration. J Cell Physiol. 2019;234(5):5964–5971. doi:10.1002/jcp.27065
35. Lyu FJ, Cui H, Pan H, et al. Painful intervertebral disc degeneration and inflammation: from laboratory evidence to clinical interventions. Bone Res. 2021;9(1):7. doi:10.1038/s41413-020-00125-x
36. Miller S, Casden AM. Spontaneous regression of a herniated disk. A case report with a four year follow-up. Bull Hosp Jt Dis. 1998;57(2):99–101.
37. Zhong M, Liu JT, Jiang H, et al. Incidence of spontaneous resorption of lumbar disc herniation: a meta-analysis. Pain Physician. 2017;20(1):E45–e52.
38. Macki M, Hernandez-Hermann M, Bydon M, Gokaslan A, McGovern K, Bydon A. Spontaneous regression of sequestrated lumbar disc herniations: literature review. Clin Neurol Neurosurg. 2014;120:136–141. doi:10.1016/j.clineuro.2014.02.013
39. Daghighi MH, Pouriesa M, Maleki M, et al. Migration patterns of herniated disc fragments: a study on 1,020 patients with extruded lumbar disc herniation. Spine J. 2014;14(9):1970–1977. doi:10.1016/j.spinee.2013.11.056
40. Deyo RA, Mirza SK. Clinical Practice. Herniated lumbar intervertebral disk. N Engl J Med. 2016;374(18):1763–1772. doi:10.1056/NEJMcp1512658
41. Cunha C, Silva AJ, Pereira P, Vaz R, Gonçalves RM, Barbosa MA. The inflammatory response in the regression of lumbar disc herniation. Arthritis Res Ther. 2018;20(1):251. doi:10.1186/s13075-018-1743-4
42. Lee SY, Kim W, Lee SU, Choi KH. Relationship between obesity and lumbar spine degeneration: a cross-sectional study from the Fifth Korean National Health and Nutrition Examination Survey, 2010–2012. Metab Syndr Relat Disord. 2019;17(1):60–66. doi:10.1089/met.2018.0051
43. Rodriguez-Martinez NG, Perez-Orribo L, Kalb S, et al. The role of obesity in the biomechanics and radiological changes of the spine: an in vitro study. J Neurosurg Spine. 2016;24(4):615–623. doi:10.3171/2015.7.Spine141306
44. Tokmak M, Altiok IB, Guven M, Aras AB, Cosar M. Spontaneous regression of lumbar disc herniation after weight loss: case report. Turk Neurosurg. 2015;25(4):657–661. doi:10.5137/1019-5149.Jtn.9183-13.1
45. Yang JH, Kim HJ, Chang DG, Suh SW, Nam Y, Song HS. Relationship between degree of separation of endplate cartilage and severity of intervertebral disc herniation. Clin Anat. 2022;35(2):204–210. doi:10.1002/ca.23816
46. Yu P, Mao F, Chen J, et al. Characteristics and mechanisms of resorption in lumbar disc herniation. Arthritis Res Ther. 2022;24(1):205. doi:10.1186/s13075-022-02894-8
47. Erly WK, Munoz D, Beaton R. Can MRI signal characteristics of lumbar disk herniations predict disk regression? J Comput Assist Tomogr. 2006;30(3):486–489. doi:10.1097/00004728-200605000-00022
48. Oktay K, Ozsoy KM, Dere UA, et al. Spontaneous regression of lumbar disc herniations: a retrospective analysis of 5 patients. Niger J Clin Pract. 2019;22(12):1785–1789. doi:10.4103/njcp.njcp_437_18
49. Chiu CC, Chuang TY, Chang KH, Wu CH, Lin PW, Hsu WY. The probability of spontaneous regression of lumbar herniated disc: a systematic review. Clin Rehabil. 2015;29(2):184–195. doi:10.1177/0269215514540919
50. Tarukado K, Ikuta K, Fukutoku Y, Tono O, Doi T. Spontaneous regression of posterior epidural migrated lumbar disc fragments: case series. Spine J. 2015;15(6):e57–62. doi:10.1016/j.spinee.2013.07.430
51. Kaliya-Perumal AK, Oh JY. Spontaneous total resolution of severe lumbar disc herniation. Chonnam Med J. 2020;56(1):77–78. doi:10.4068/cmj.2020.56.1.77
52. Gezici AR, Ergün R. Spontaneous regression of a huge subligamentous extruded disc herniation: short report of an illustrative case. Acta Neurochir. 2009;151(10):1299–1300. doi:10.1007/s00701-009-0370-x
53. Benson RT, Tavares SP, Robertson SC, Sharp R, Marshall RW. Conservatively treated massive prolapsed discs: a 7-year follow-up. Ann R Coll Surg Engl. 2010;92(2):147–153. doi:10.1308/003588410x12518836438840
54. Ryu SJ, Kim IS. Spontaneous regression of a large lumbar disc extrusion. J Korean Neurosurg Soc. 2010;48(3):285–287. doi:10.3340/jkns.2010.48.3.285
55. Tsarouhas A, Soufla G, Katonis P, Pasku D, Vakis A, Spandidos DA. Transcript levels of major MMPs and ADAMTS-4 in relation to the clinicopathological profile of patients with lumbar disc herniation. Eur Spine J. 2011;20(5):781–790. doi:10.1007/s00586-010-1573-9
56. Lee JM, Song JY, Baek M, et al. Interleukin-1β induces angiogenesis and innervation in human intervertebral disc degeneration. J Orthop Res. 2011;29(2):265–269. doi:10.1002/jor.21210
57. Hornung AL, Baker JD, Mallow GM, et al. Resorption of lumbar disk herniation: mechanisms, clinical predictors, and future directions. JBJS Rev. 2023;11(1):e22. doi:10.2106/JBJS.RVW.22.00148
58. Kawaguchi K, Harimaya K, Matsumoto Y, et al. Effect of cartilaginous endplates on extruded disc resorption in lumbar disc herniation. PLoS One. 2018;13(4):e0195946. doi:10.1371/journal.pone.0195946
59. Lama P, Zehra U, Balkovec C, et al. Significance of cartilage endplate within herniated disc tissue. Eur Spine J. 2014;23(9):1869–1877. doi:10.1007/s00586-014-3399-3
60. Fei H, Li WS, Sun ZR, Ma QW, Chen ZQ. Analysis of spino-pelvic sagittal alignment in young Chinese patients with lumbar disc herniation. Orthop Surg. 2017;9(3):271–276. doi:10.1111/os.12340
61. Mardare M, Oprea M, Popa I, Zazgyva A, Niculescu M, Poenaru DV. Sagittal balance parameters correlate with spinal conformational type and MRI changes in lumbar degenerative disc disease: results of a retrospective study. Eur J Orthop Surg Traumatol. 2016;26(7):735–743. doi:10.1007/s00590-016-1842-3
62. Dora C, Wälchli B, Elfering A, Gal I, Weishaupt D, Boos N. The significance of spinal canal dimensions in discriminating symptomatic from asymptomatic disc herniations. Eur Spine J. 2002;11(6):575–581. doi:10.1007/s00586-002-0448-0
63. Sun Z, Zhang M, Zhao XH, et al. Immune cascades in human intervertebral disc: the pros and cons. Int J Clin Exp Pathol. 2013;6(6):1009–1014.
64. Yu PF, Jiang H, Liu JT, et al. Traditional Chinese medicine treatment for ruptured lumbar disc herniation: clinical observations in 102 cases. Orthop Surg. 2014;6(3):229–235. doi:10.1111/os.12120
65. Kobayashi S, Meir A, Kokubo Y, et al. Ultrastructural analysis on lumbar disc herniation using surgical specimens: role of neovascularization and macrophages in hernias. Spine. 2009;34(7):655–662. doi:10.1097/BRS.0b013e31819c9d5b
66. Haro H, Kato T, Komori H, Osada M, Shinomiya K. Vascular endothelial growth factor (VEGF)-induced angiogenesis in herniated disc resorption. J Orthop Res. 2002;20(3):409–415. doi:10.1016/s0736-0266(01)00150-4
67. Rätsep T, Minajeva A, Asser T. Relationship between neovascularization and degenerative changes in herniated lumbar intervertebral discs. Eur Spine J. 2013;22(11):2474–2480. doi:10.1007/s00586-013-2842-1
68. Burke JG, Watson RW, McCormack D, Dowling FE, Walsh MG, Fitzpatrick JM. Spontaneous production of monocyte chemoattractant protein-1 and interleukin-8 by the human lumbar intervertebral disc. Spine. 2002;27(13):1402–1407. doi:10.1097/00007632-200207010-00006
69. Wang J, Tian Y, Phillips KL, et al. Tumor necrosis factor α- and interleukin-1β-dependent induction of CCL3 expression by nucleus pulposus cells promotes macrophage migration through CCR1. Arthritis Rheum. 2013;65(3):832–842. doi:10.1002/art.37819
70. Arai Y, Yasuma T, Shitoto K, Yamauchi Y, Suzuki F. Immunohistological study of intervertebral disc herniation of lumbar spine. J Orthop Sci. 2000;5(3):229–231. doi:10.1007/s007760050156
71. Enthoven WT, Roelofs PD, Deyo RA, van Tulder MW, Koes BW. Non-steroidal anti-inflammatory drugs for chronic low back pain. Cochrane Database Syst Rev. 2016;2(2):Cd012087. doi:10.1002/14651858.Cd012087
72. Qaseem A, Wilt TJ, McLean RM, et al. Noninvasive treatments for acute, subacute, and chronic low back pain: a clinical practice guideline from the American College of Physicians. Ann Intern Med. 2017;166(7):514–530. doi:10.7326/m16-2367
73. Balakrishnamoorthy R, Horgan I, Perez S, Steele MC, Keijzers GB. Does a single dose of intravenous dexamethasone reduce Symptoms in Emergency department patients with low Back pain and RAdiculopathy (SEBRA)? A double-blind randomised controlled trial. Emerg Med J. 2015;32(7):525–530. doi:10.1136/emermed-2013-203490
74. Chou R, Hashimoto R, Friedly J. Epidural corticosteroid injections for radiculopathy and spinal stenosis. Ann Intern Med. 2016;164(9):635–636. doi:10.7326/l15-0563
75. Minamide A, Tamaki T, Hashizume H, Yoshida M, Kawakami M, Hayashi N. Effects of steroid and lipopolysaccharide on spontaneous resorption of herniated intervertebral discs. An experimental study in the rabbit. Spine. 1998;23(8):870–876. doi:10.1097/00007632-199804150-00007
76. Aydin MV, Sen O, Kayaselcuk F, et al. Analysis and prevalence of inflammatory cells in subtypes of lumbar disc herniations under cyclooxygenase-2 inhibitor therapy. Neurol Res. 2005;27(6):609–612. doi:10.1179/016164105x49210
77. Buttermann GR. Lumbar disc herniation regression after successful epidural steroid injection. J Spinal Disord Tech. 2002;15(6):469–476. doi:10.1097/00024720-200212000-00007
78. Shen X, Yu P, Shao Y, Liu J, Jiang H, Wang J. Value of contrast-enhanced MRI for predicting resorption of ruptured lumbar disc herniation: a prospective study of 82 cases. J Orthop Surg Res. 2025;20(1):1006. doi:10.1186/s13018-025-06411-w
79. Starekova J, Pirasteh A, Reeder SB. Update on gadolinium-based contrast agent safety, from the AJR special series on contrast media. Am J Roentgenol. 2024;223(3):e2330036. doi:10.2214/AJR.23.30036
80. Endrikat J, Gutberlet M, Hoffmann K, et al. Clinical safety of gadobutrol: review of over 25 years of use exceeding 100 million administrations. Invest Radiol. 2024;59(9):605–613. doi:10.1097/RLI.0000000000001072
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.