Back to Journals » Therapeutics and Clinical Risk Management » Volume 20
Predictive Factors for Iliac Limb Occlusions After Endovascular Abdominal Aneurysm Repair: Determined from Aortoiliac Anatomy, Endovascular Procedures, and Aneurysmal Remodeling
Authors Yuan Z ![]() , Du C, You Y, Wang J
, Du C, You Y, Wang J
Received 22 February 2024
Accepted for publication 16 May 2024
Published 20 May 2024 Volume 2024:20 Pages 297—311
DOI https://doi.org/10.2147/TCRM.S459594
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor De Yun Wang
Zihui Yuan,* Chao Du,* Yun You,* Jian Wang
Department of Vascular Surgery, Union Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jian Wang, Department of Vascular Surgery, Union Hospital, Tongji Medical College, Huazhong University of Science and Technology, 1277 Jiefang Avenue, Wuhan, 430022, People’s Republic of China, Tel +11-86-15902735929, Email [email protected]
Purpose: Iliac limb occlusion (ILO) is a serious complication of endovascular abdominal aneurysm repair (EVAR). This study aimed to identify predictive factors for ILO derived from aortoiliac morphology, endovascular procedure-related parameters, and aneurysmal remodeling characteristics.
Patients and Methods: Patient demographics, pre-EVAR anatomical characteristics of the aneurysm, endovascular procedure details, and post-EVAR aneurysmal remodeling outcomes were analyzed and compared using univariate analysis. Statistically significant factors were subsequently subjected to Cox regression and Kaplan–Meier analyses.
Results: Between January 2013 and April 2022, 66 patients were included in this study. Fourteen patients presented with ILO and were compared with 52 control patients with patent endograft limb over at least 1-year of follow-up. The tortuosity indices of the common iliac artery (CIA) and endograft iliac limb to vessel oversizing were significantly larger in the ILO group than in the patent endograft limb group. The CIA index of tortuosity ≥ 1.08, and endograft iliac limb to vessel oversizing ≥ 18.8% were independent predictors for ILO. During the follow-up of all patients, the proximal aortic neck and CIA diameters increased, aneurysm sac diameter decreased, and aortic neck and aortic length increased. The aortoiliac length increased over time in patients with patent endograft limb but not in patients with ILO. A change in the lowest renal artery-left iliac bifurcation distance ≦0.07 mm increased the risk of ILO.
Conclusion: ILO is predisposed to occur when the CIA index of tortuosity ≥ 1.08 and endograft iliac limb to vessel oversizing ≥ 18.8% are present. Significant aortoiliac remodeling, including proximal aortic neck dilatation, neck straightening, aneurysmal sac regression, iliac artery enlargement, and aortic lengthening, occurs after EVAR. Aortoiliac elongation was observed in patients with patent endograft limb, but not in patients with ILO. ILO was associated with a change in the lowest renal artery–left iliac bifurcation from the postoperative measurements ≦ 0.07 mm.
Keywords: abdominal aortic aneurysm, endovascular abdominal aneurysm repair, iliac limb occlusion, aortoiliac anatomy, aneurysmal remodeling, oversizing, aortoiliac tortuosity
Introduction
Endovascular abdominal aneurysm repair (EVAR) is widely used to treat infrarenal abdominal aortic aneurysms. EVAR is a minimally invasive procedure, with shorter hospital stays and fewer short-term complications than open surgery.1,2 Iliac limb occlusion (ILO) is a well-known early or late complication of endovascular abdominal aneurysm repair (EVAR) and requires re-intervention by surgical, endovascular, or hybrid techniques in most cases.3–5 The short- and long-term ILO rates are still considerable, with an incidence of 5.6–5.9% in patients undergoing EVAR.3–5
There are many reasons for ILO, which can be categorized as aortoiliac anatomy, graft-related causes, and aneurysmal remodeling over time. Aortoiliac anatomical factors that potentially correlate with ILO include maximum aneurysmal diameter, proximal neck measurements, distal abdominal aortic anatomy,6,7 common iliac artery (CIA) diameter,8 external iliac artery (EIA) diameter,3,8,9 and iliac artery tortuosity.10–12 Graft-related technical factors that predispose to ILO include distal loading zone in the EIA,3,8,9,13–15 endograft limb diameters,15 and excessive oversizing of the endograft limb.16,17 Aneurysmal remodeling outcomes over time are defined as dilatation of the proximal neck dilatation,18–23 shrinkage of the aneurysmal sac,18,20 aortoiliac elongation,18,24 and enlargement of the iliac artery.18,20,22,23 Endovascular graft fixation depends on the integrity and long-term structural stability of the aorta near the site of graft deployment. Aortoiliac remodeling can challenge endograft fixation and sealing. The stent graft migrates toward the aortic bifurcation, and ILO may occur if the native aorta becomes dilated or lengthened. In addition, aortoiliac conformational changes may cause limb kinking or occlusion over time. However, no study has investigated whether the remodeling outcomes of abdominal aortic aneurysms predispose to ILO after EVAR.
The aims of this study were as follows: 1) to compare patient demographics, aortoiliac anatomy, graft-related factors, and aneurysmal remodeling post-EVAR between patients with and without ILO. 2) To identify potential risk factors derived from anatomy, techniques, and aneurysmal remodeling for ILO after EVAR.
Materials and Methods
Patient Selection
A total of 593 patients underwent EVAR for infrarenal abdominal aortic aneurysm (AAA) and/or CIA aneurysm in our department between January 2013 and April 2022. The inclusion criteria for this study were elective TEVAR for asymptomatic AAA or symptomatic AAA using an infrarenal bifurcated stent graft, with iliac stent graft limbs being deployed in the CIAs or EIAs. Patients with abdominal aortic dissection, mycotic aneurysms, and traumatic pseudoaneurysms as well as those for whom postoperative computed tomography angiography (CTA) images could not be obtained were excluded. All post-EVAR and follow-up CTA were checked by two investigators to identify the ILO. Occlusion was defined as complete blockage of the lumen diameter of the stent graft, as evidenced by CT angiography, regardless of symptoms. ILO was observed in 14 patients (15 limbs). Fifty-two patients were available for CTA scans preoperatively, postoperatively before discharge, and with a minimum 1-year follow-up, and no ILO occurred until the latest CT scans. Overall, 66 patients were included in this analysis. This study was conducted in accordance with the ethical guidelines of the 1975 Declaration of Helsinki and its amendments, and the protocol was approved by the Ethics Committee of Wuhan Union Hospital (2022IEC392). Because this was a retrospective review, the requirement for written informed consent was waived, and the patient information was anonymized before analysis.
EVAR Procedures
All the procedures, including EVAR and iliac limb extension, were performed by experienced vascular surgeon. Systemic heparinization was achieved using 5000 IU of heparin. Simultaneous bilateral access to the common femoral arteries was obtained via bilateral femoral artery preparation after systemic heparinization. All endovascular stent grafts were deployed below the renal arteries, whereas the endograft limbs were deployed with a distal sealing zone in the CIAs or EIAs depending on the extent of the aneurysm. The distal landing zone of endovascular stent grafts was located in EIAs following internal iliac artery (IIA) coil embolization. Four different types of devices were used: 49 (74.2%) Talent and Endurant (Medtronic Vascular, Santa Rosa, CA, USA), two (3.0%) Cordis, six (9.1%) Microport, and nine (13.6%) Lifetech. Completion angiography to assess graft position and function was performed routinely without stiff wires in place in order to detect limb kinking that might predispose to thrombosis.
Image Analysis and Measurements
Preoperative anatomy, procedure-related data, and postoperative and long-term follow-up data were prospectively obtained from the patient records and CTA scans at different time-points. All measurements (diameter, length, and angle) were performed with semi-automatically generated center-lumen line reconstructions on a workstation using dedicated vascular reconstruction software (AW 4.4–4.5, Advantage WorkStation, GE Healthcare). Two vascular surgeons blinded to the patient history and outcomes separately reviewed the cross-sectional and axial reconstruction of the CTA scans. These two vascular surgeons had extensive experience with workstation and centerline measurements.25 If an agreement could not be reached after discrepancies were discussed, an independent investigator was consulted to reach a final consensus.
Anatomical Measurements
Preoperative AAA anatomical measurements focused mainly on aneurysmal sac diameters, infrarenal proximal aortic neck, distal abdominal aorta, and iliac artery ipsilateral to limb occlusion. Diameter measurements were determined from outer-to-outer circumferential wall perpendicular to the long axis of the vessel. Proximal aortic neck length was defined as the distance from the lowest renal artery level to the onset of the aneurysm. The proximal aortic neck diameter was defined as the maximum diameter of the aorta 15 mm below the lowest renal artery. The proximal aortic neck angle is the most acute angle calculated between the lowest renal artery along the midline of the lumen to the origin of the aneurysm and the aortic bifurcation. The presence of mural thrombus and calcification was defined when more than half of the vascular circumference was covered with thrombi or calcification by gross measurement. The CIA index of tortuosity was calculated as the length of the CIA based on the center-lumen line from the aortic bifurcation to the origin of the internal iliac artery divided by the straight-line distance between the two landmarks. A double iliac sign was defined as the observation that the iliac arteries were visually doubled or more on an axial CTA slice. The double iliac sign was recorded as present or absent; however, no other quantitative measurements were performed.
EVAR Procedure-Related Factors
The ratio between the sum of the endograft limb diameter and the distal aorta diameter was calculated. Endograft iliac limb parameters included diameter, oversizing, and distal landing zone in the EIA. Iliac limb parameters were measured at the end of the landing zone. The degree of oversizing of the endograft iliac limb was calculated as the ratio of the iliac limb diameter to the preoperative landing zone diameter of the CIA or the EIA. The diameter of each endograft limb was measured at the level of the terminal abdominal aorta. Endograft iliac limbs with smaller diameters in the terminal abdominal aorta were defined as the smaller limb (SL) and those with larger diameters in the terminal aorta were defined as the larger limb (LL). Endograft limb extension was defined as a procedure in which the distal landing zone of the endovascular stent grafts was extended to the EIA for various reasons.
Aneurysmal Remodeling Outcomes
Baseline reference CTA images were obtained postoperatively after EVAR and before discharge. Serial follow-up CTA scans were reviewed to evaluate aneurysmal remodeling. CTA analysis consisted of measuring the proximal aortic neck angulation, the following diameters: proximal aortic neck, aneurysm sac, and CIA, and the following distances: superior mesenteric artery (SMA) to the lowest renal artery, SMA to iliac bifurcation, SMA to left iliac bifurcation, SMA to right iliac bifurcation, lowest renal to left iliac bifurcation, and lowest renal-right iliac bifurcation. The aortic diameters were measured at planes perpendicular to the central line from the adventitia to the adventitia. Standardized centerline aortic lengths were also measured. All measurements were obtained postoperative and during all follow-up CTA scans, and the changes in these measurements from the postoperative baseline to follow-up were recorded.
Statistical Analysis
Categorical variables are reported as counts and percentages. Chi-square or Fisher’s exact test was used to compare categorical variables. Continuous variables are reported as mean ± standard deviation and median (first quartile, third quartile) according to the normality of distribution. Univariate analysis between groups was performed using Student’s t-test for variables with normal distribution and the Mann–Whitney U-test for independent nonparametric data. Differences among groups were analyzed using analysis of variance (ANOVA) for variables with normal distribution and the Kruskal–Wallis test for independent nonparametric data. All analyses were performed using SPSS, version 9.4 software. Cox regression analysis was performed to determine the influence of variables on ILO at follow-up. Variables with statistical significance in univariate analysis were entered into a Cox multivariate model. The results of the regression analysis are presented as hazard ratios (HR) and 95% confidence intervals (CI). Kaplan–Meier time to event analysis was used to evaluate the cumulative proportion of patients with patent endograft limb at the follow-up. Differences in ILO free survival were evaluated with a Log rank test. Statistical significance was assumed when the p-value was <0.05.
Results
Baseline Characteristics of Patients Enrolled in This Study
This study included 66 patients who underwent standard EVAR and regular follow-up CTA between January 2013 and April 2022. During follow-up, 52 patients presented with the bilateral patent endograft limb preoperatively, within 1 week before discharge, and during a minimum follow-up of 1 year, and 14 patients unfortunately suffered from ILO until the latest imaging examination. The patient demographics and concomitant diseases are shown in Table 1. Male patients accounted for 71.4% and 94.2% of the cases with ILO and patent endograft limbs, respectively (p = 0.032). Coronary artery disease was more frequently observed in patients with ILO (64.3%) than in those with patent endograft limb (26.9%) (p = 0.009). For the remaining factors, statistical analysis failed to show a significant difference between the ILO and patent endograft limb groups, including age, hypertension, diabetes mellitus, smoking, chronic kidney disease, cerebrovascular accident, cancer, and chronic obstructive pulmonary disease.
 |
Table 1 Baseline Demographics and Concomitant Diseases of Patients Included in the Study |
Clinical Pattern, Time to Occlusion, and Treatment Option of ILO
Table 2 lists the presenting symptom, time to event, the left/right or both of ILO, and treatment modalities in patients with ILO. Fourteen patients with ILO were observed until the latest follow-up CTA, including 1 patient who had ILO in both limbs. Their ages ranged from 58 to 75 years, and 10 patients (71.4%) were male. Of the 14 patients with ILO, two (14.3%) had ILO within 30 days following EVAR, and the majority of patients (12/14, 85.7%) were diagnosed with ILO within the first year of follow-up. However, two patients (14.3%) were identified as having ILO after one year of follow-up. The presenting symptoms of ILO were acute ischemia with rest pain in five patients (35.7%) and mild-to-moderate claudication in six patients (42.9%). In three patients (21.4%), the ILOs were asymptomatic and were found on follow-up CTA. ILO was located on the right side (11/14, 78.6%), left side (14.3%), or both sides (7.1%).
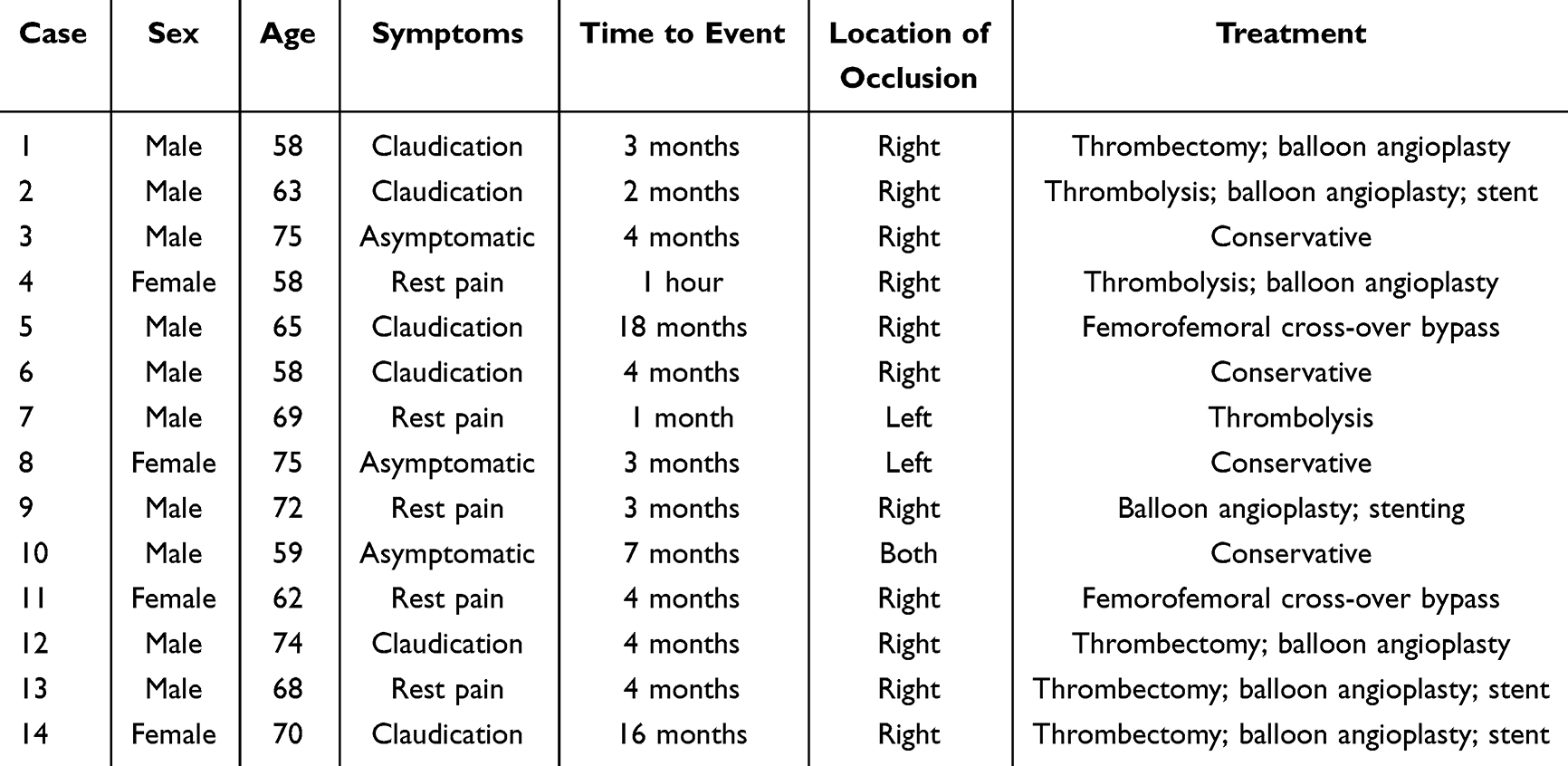 |
Table 2 Symptoms, Time and Treatment of Iliac Limb Occlusion |
Three patients (21.4%) were treated with catheter-directed thrombolysis, followed by percutaneous transluminal balloon angioplasty in two patients and adjunctive stenting in one patient. Four patients (28.6%) were treated with surgical thrombectomy, followed by transluminal balloon angioplasty in four patients and adjunctive stenting in three patients. Two patients (14.3%) were treated with femorofemoral crossover bypass. One patient (7.1%) underwent transluminal balloon angioplasty, followed by adjunctive stenting. The remaining four patients (28.6%) received conservative treatment. None of the reported patients underwent major amputation.
Morphologic Characteristics of Aortoiliac Anatomy
Table 3 presents the differences between the ILO and patent endograft limb groups with respect to the aortoiliac morphology variables. The maximum aneurysm sac diameters were significantly smaller in patients with ILO (35.4 [9.6; 49.9] mm) than in those with patent endograft limb (52.6 [38.9; 66.3] mm) (p = 0.008). The CIA index of tortuosity was significantly higher in patients with ILO (1.09 [1.04; 1.18]) than in those with patent endograft limb (1.04 [1.03; 1.07]) (p = 0.016). One patient had ILO three months after EVAR with a tortuosity index of 1.38 (Figure 1). The double iliac sign was observed significantly more often in six patients (42.9%) with ILO than in six patients (11.5%) with patent endograft limbs (p = 0.007). One patient showed a double iliac sign (DIS) on preoperative CTA and developed a right ILO five months after EVAR (Figure 2).
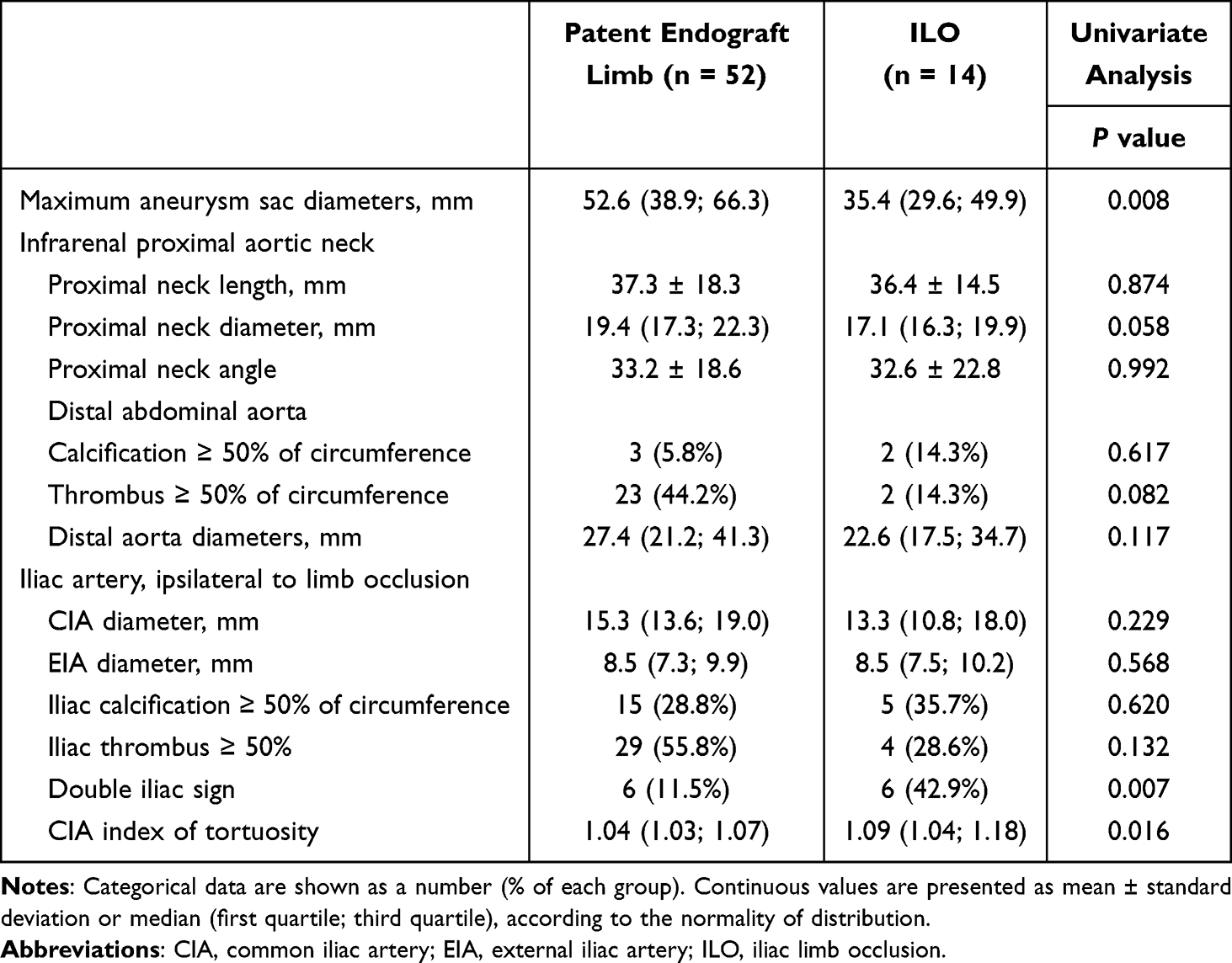 |
Table 3 Potential Predictors from Preoperative Aorto-Iliac Anatomy for Predicting Iliac Limb Occlusion |
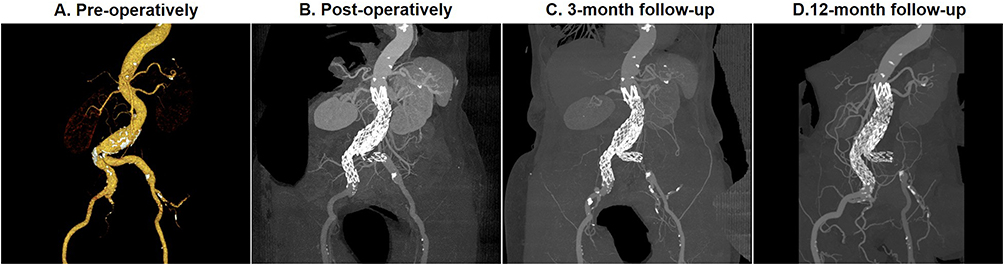 |
Figure 1 ILO due to tortuous CIA. (A) The preoperative CTA indicated the severe tortuosity of left CIA and tortuosity index of left CIA was calculated as 1.38. (B) Tortuous CIA resulted in limb stent-graft kinking after EVAR. (C) ILO was found at 3-month follow-up. (D) Conservative treatment was performed with significant symptom relief at 12-month follow-up. Abbreviations: ILO, iliac limb occlusion; CIA, common iliac artery; CTA, computed tomography angiography; EVAR, endovascular abdominal aneurysm repair. |
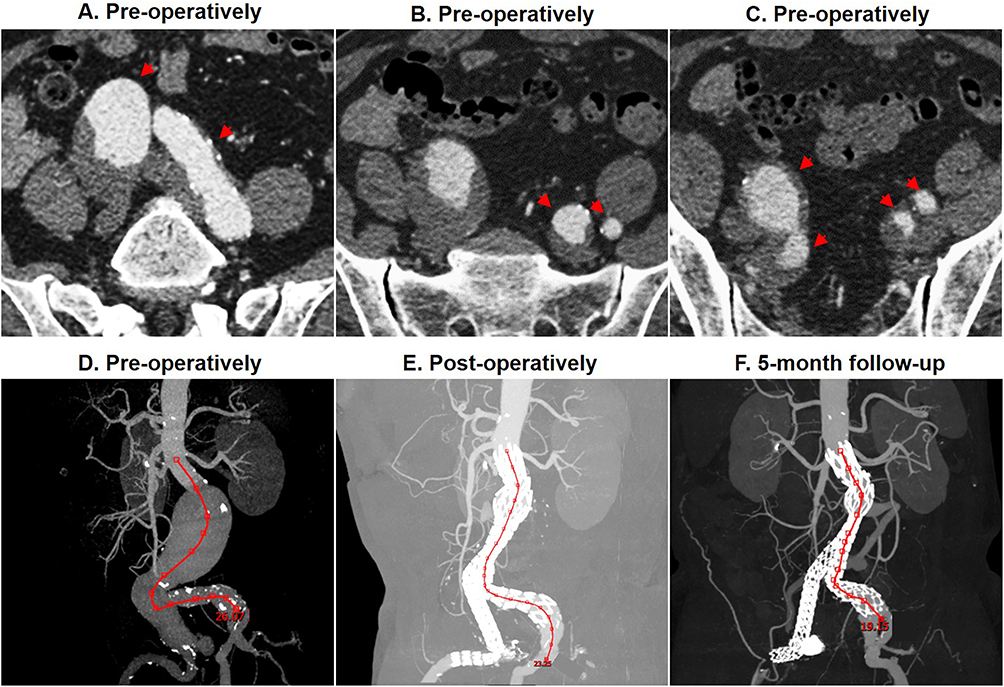 |
Figure 2 ILO and double iliac sign. (A–C) Double iliac sign was defined as the observation that a part of the iliac vessel within the landing zone of the graft limb was visually doubled or more on the axial CTA slice (red arrows). Double iliac sign was present on the preoperative CTA (red arrows). (D–F) Lowest renal artery–left iliac bifurcation distances were 26.1 mm, 23.3 mm, and 19.2 mm preoperatively, postoperatively, and at 5-month follow-up, respectively. Right ILO occurred at 5 months after EVAR and was associated with the significant decrease in lowest renal artery-left iliac bifurcation distance. Abbreviations: ILO, iliac limb occlusion; CTA, computed tomography angiography; EVAR, endovascular abdominal aneurysm repair. |
For the remaining factors measured in iliac artery ipsilateral to ILO, there were no significant differences between the ILO group and patent endograft limb group, on CIA diameters, EIA diameters, iliac calcification ≥50%, and iliac thrombus ≥50% of circumference. Infrarenal proximal aortic neck measurements included diameter, length, and angle and did not differ significantly between the ILO and patent endograft limb groups. Distal abdominal aorta parameters including calcification ≥50% of circumference, thrombus ≥50% of circumference, and distal aorta diameter were also not significantly different between the ILO and patent endograft limb groups.
EVAR Procedure-Related Factors
Table 4 presents the EVAR procedure-related parameters of the ILO and patent endograft limb groups. The difference in diameter between the LL and SL (LL-SL) was statistically larger in patients with ILO (1.9 [0.9; 5.4] mm) than in those with patent endograft limb (1.3 [0.5; 2.5] mm) (p = 0.048). The SL was occluded due to compression of the LL within the distal narrow aorta 19 months after EVAR (Figure 3). Endograft-to-vessel oversizing was significantly larger in patients with ILO (20.2% ± 6.7%) than in those with patent endograft limb (12.7% ± 4.7%) (p < 0.001).
 |
Table 4 Potential Predictors from Procedure-Related Technical Factors for Predicting Iliac Limb Occlusion |
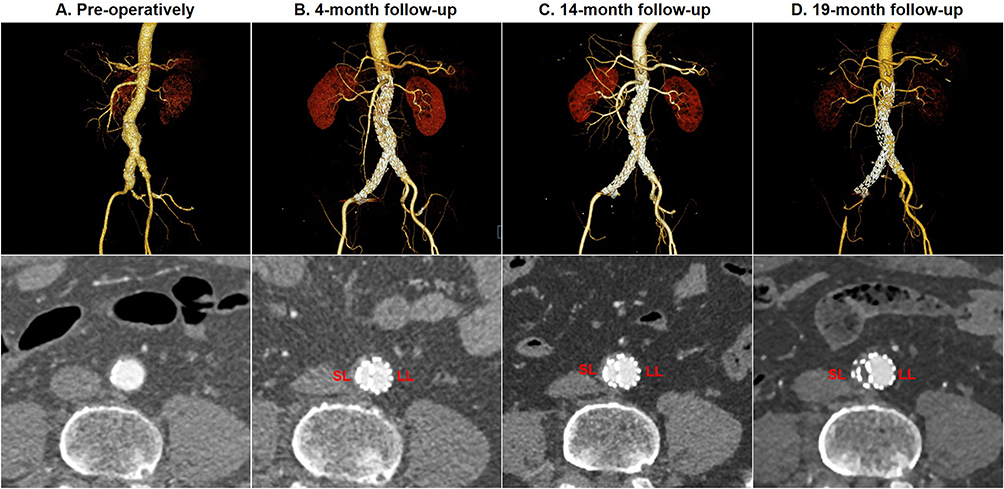 |
Figure 3 ILO due to the interaction between LL and SL within the distal narrow aorta. (A) The preoperative CTA showed the terminal narrow aorta diameter of 16.5 mm. (B and C) LL interacted with SL within the narrow terminal aorta, and a large difference in diameter between LL and SL was created at 4-month and 14-month follow-up. (D) SL was subsequently occluded at 19-month follow-up. Abbreviations: ILO, iliac limb occlusion; CTA, computed tomography angiography; LL, large limb; SL, small limb. |
No significant difference was observed in the sum of the endograft limb diameters/distal aorta diameters and endograft iliac limb diameters between the ILO and patent endograft limb groups. Extension of the graft into the EIA was not more frequently observed in patients with ILO (42.9%) than in those with patent endograft limb (36.5%).
Aortoiliac Remodeling from Postoperative Measurement After EVAR
Table 5 presents EVAR-induced aortoiliac remodeling in patients with patent endograft limb and with ILO. Proximal aortic neck diameter increased by an average of 2.4 [0.8; 4.7] mm and 0.8 [0.5; 1.5] mm in patients with patent endograft limb and ILO, respectively (Figure 4). This change was more significant in patients with patent endograft limb than in those with ILO (p = 0.030). Proximal aortic neck straightened over time with angulation decreased by a mean of 0.4 ± 9.0 degrees in patients with patent endograft limb and 0.3 ± 11.7 degrees in patients with ILO. Aneurysm sac regression was also significant (Figure 5): decreased by a mean of 0.9 [−5.2; 1.0] mm in patients with patent endograft limb and 0.5 [−2.7; 1.0] mm in patients with ILO. CIA diameters significantly increased over time with the mean increases of 1.2 [0.2; 2.4] mm in patients with patent endograft limb and 1.5 [−0.7; 3.2] mm in patients with ILO (Figure 6).
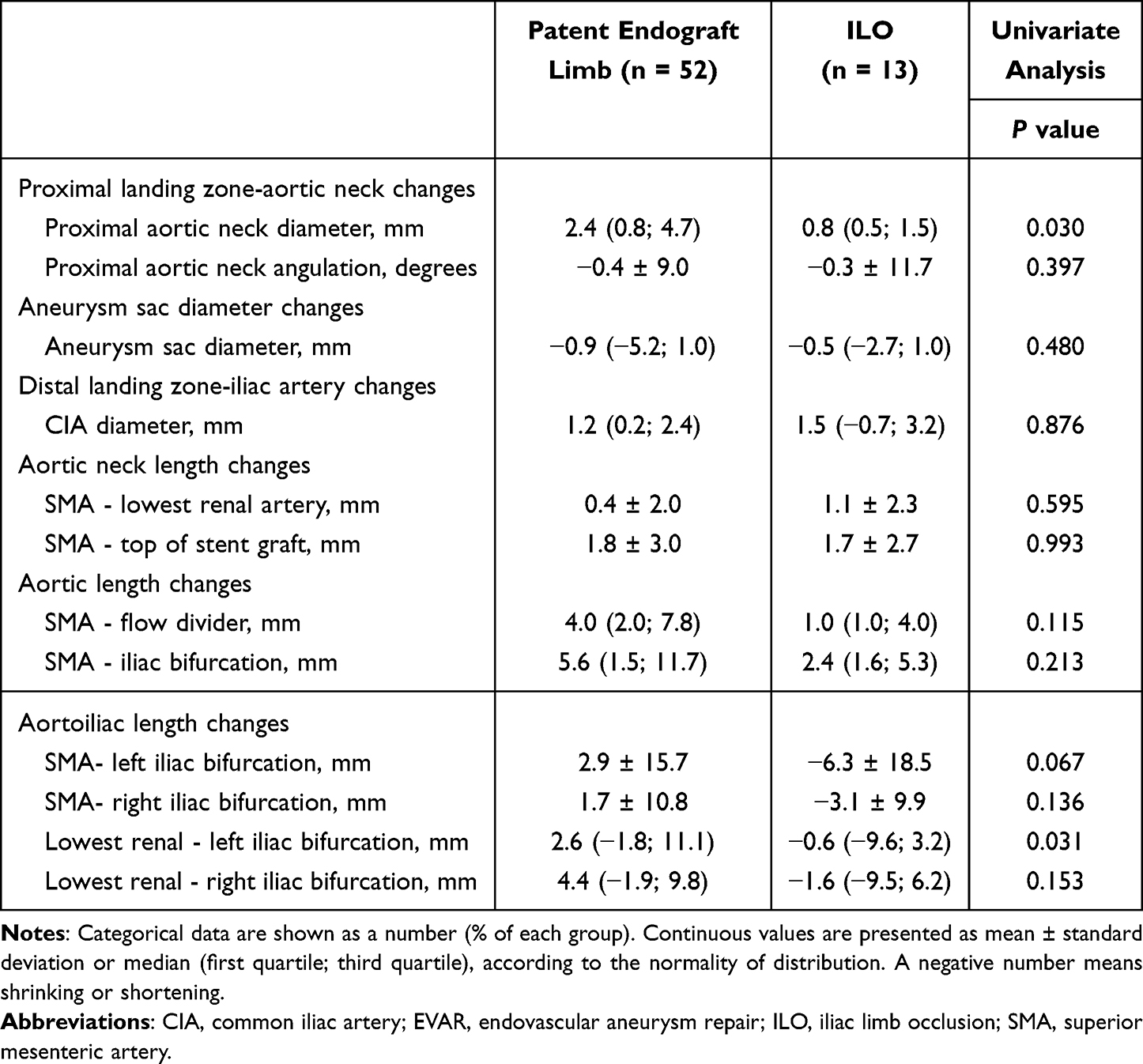 |
Table 5 Potential Factors from Aortic Aneurysm Remodeling After EVAR for Inducing Iliac Limb Occlusion |
 |
Figure 4 Proximal aortic neck dilatation over time following EVAR. (A, B) Proximal aortic neck diameters were 20.5 mm and 23.0 mm on preoperative and postoperative CTA, respectively. (C and D) The sagittal CTA scans obtained at 13 month and 3 years after EVAR showed aortic neck dilatation of 26.5 mm and 26.3 mm. Abbreviations: EVAR, endovascular abdominal aneurysm repair; CTA, computed tomography angiography. |
 |
Figure 5 Aneurysmal sac regression over time following EVAR. (A and B) The axial CTA scans obtained preoperatively and postoperatively before discharge showed the maximum aneurysmal sac diameter of 70.8 mm and 69.4 mm. (C) The 4-month axial CTA scans indicated the aneurysmal sac regression of 54.9 mm. (D) The 5-year axial CTA scans demonstrated a total regression of the aneurysmal sac due to the remodeling of aneurysmal mural thrombus. Abbreviations: EVAR, endovascular abdominal aneurysm repair; CTA, computed tomography angiography. |
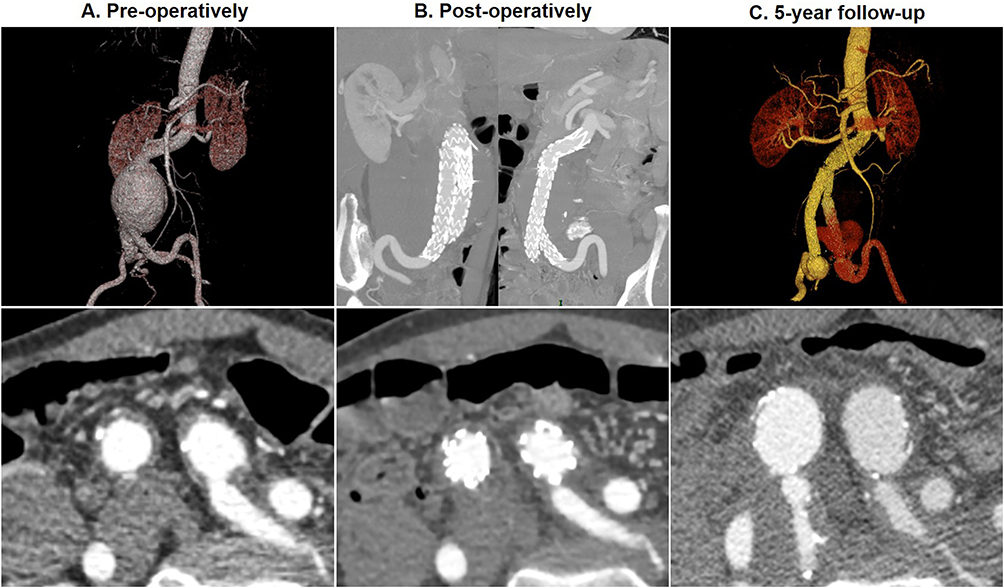 |
Figure 6 Common iliac artery enlargement over time following EVAR. (A) The axial and reconstructed CTA scans obtained preoperatively showed the right and left CIA diameter of 15.9 mm and 20.7 mm at the iliac bifurcation. (B) The axial and reconstructed CTA scans obtained postoperatively before discharge indicated the right and left CIA diameter of 16.1 mm and 20.8 mm at the iliac bifurcation. (C) The 5-year axial and reconstructed CTA scans demonstrated the aneurysmal dilatation of bilateral CIA nearby the iliac bifurcation and the right and left CIA diameters of 31.41 mm and 33.94 mm. Abbreviations: EVAR, endovascular abdominal aneurysm repair; CTA, computed tomography angiography; CIA, common iliac artery. |
SMA–lowest renal artery increased significantly with a lengthening of 0.4 ± 2.0 mm in patients with patent endograft limb and 1.1 ± 2.3 mm in patients with ILO. SMA–the top of stent graft also increased significantly with a lengthening of 1.8 ± 3.0 mm in patients with patent endo-graft limb and 1.7 ± 2.7 mm in patients with ILO. SMA–flow divider lengthened by an average of 4.0 [2.0; 7.8] mm in patients with patent endograft limb and 1.0 [1.0; 4.0] mm in patients with ILO. The SMA iliac bifurcation also lengthened by an average of 5.6 [1.5; 11.7] mm in patients with patent endograft limb and 2.4 (1.6; 5.3) cm in patients with ILO (Figure 7).
 |
Figure 7 Aortoiliac elongation over time following EVAR. (A and B) The axial and reconstructed CTA scans obtained preoperatively and postoperatively before discharge showed the SMA–iliac bifurcation distance of 14.1 mm and 14.9 mm. (C) The 19-month CTA scans showed the SMA–iliac bifurcation lengthening of 17.3 mm. Abbreviations: EVAR, endovascular abdominal aneurysm repair; CTA, computed tomography angiography; SMA, superior mesenteric artery; EVAR, endovascular abdominal aneurysm repair. |
Aortoiliac lengthening was obvious in patent endograft limb group with an average increase of 2.9 ± 15.7 mm in SMA–left iliac bifurcation, 1.7 ± 10.8 mm in SMA–right iliac bifurcation, 2.6 [−1.8; 11.1] mm in lowest renal artery–left iliac bifurcation, and 4.4 [−1.9; 9.8] mm in lowest renal artery–right iliac bifurcation. Conversely, the average length of aortoiliac segments was shortened in the ILO group with an average decrease of 6.3 ± 18.5 mm in SMA–left iliac bifurcation, 3.1 ± 9.9 mm in SMA–right iliac bifurcation, 0.6 [−9.6; 3.2] mm in lowest renal artery–left iliac bifurcation, and 1.6 [−9.5; 6.2] mm in lowest renal artery–right iliac bifurcation. The lowest renal artery-left iliac bifurcation showed a statistically significant difference between the patent endograft limb and the ILO groups (p = 0.031).
Risk Factors for Iliac Limb Occlusion After EVAR
The results of Cox regression analysis for ILO are presented in Table 6. CIA index of tortuosity ≥1.08 (HR = 1.584, 95% CI = 1.073–2.339; p = 0.021) and endograft to vessel oversizing ≥18.8% (HR = 1.347, 95% CI = 1.150–1.577; p < 0.001) were identified as independent risk factors for ILO. Kaplan–Meier analysis confirmed a significantly lower ILO-free survival when the CIA index of tortuosity was ≥1.08 (47.6% vs 87.1%; Figure 8A) or when the endograft-to-vessel oversizing was ≥18.8% (31.1% vs 94.0%; Figure 8B). Moreover, the presence of one risk factor was associated with a relatively lower ILO-free survival rate compared with none of the two predictors (75.0% vs 96.3%; Figure 8C). Change of lowest renal artery–left iliac bifurcation from postoperative measurement ≤0.07 mm (HR = 0.543, 95% CI = 0.333–0.886; p = 0.015) increased the risk for ILO after EVAR. Kaplan–Meier analysis indicated a significantly lower ILO-free survival when changes in lowest renal–left iliac bifurcation from postoperative measurements ≤0.07 mm (66.8% vs 86.8%; Figure 8D).
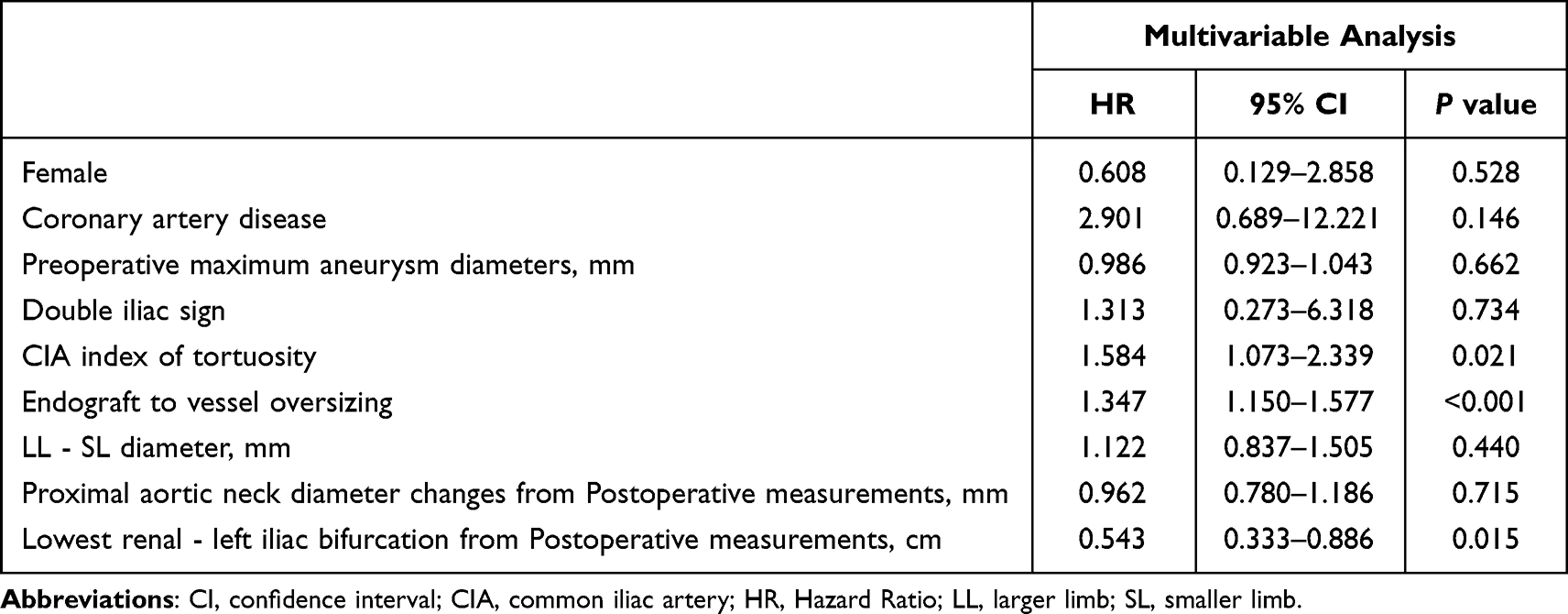 |
Table 6 Multivariable Proportional Hazards Analysis of Variables Affecting the Risk for Iliac Limb Occlusion |
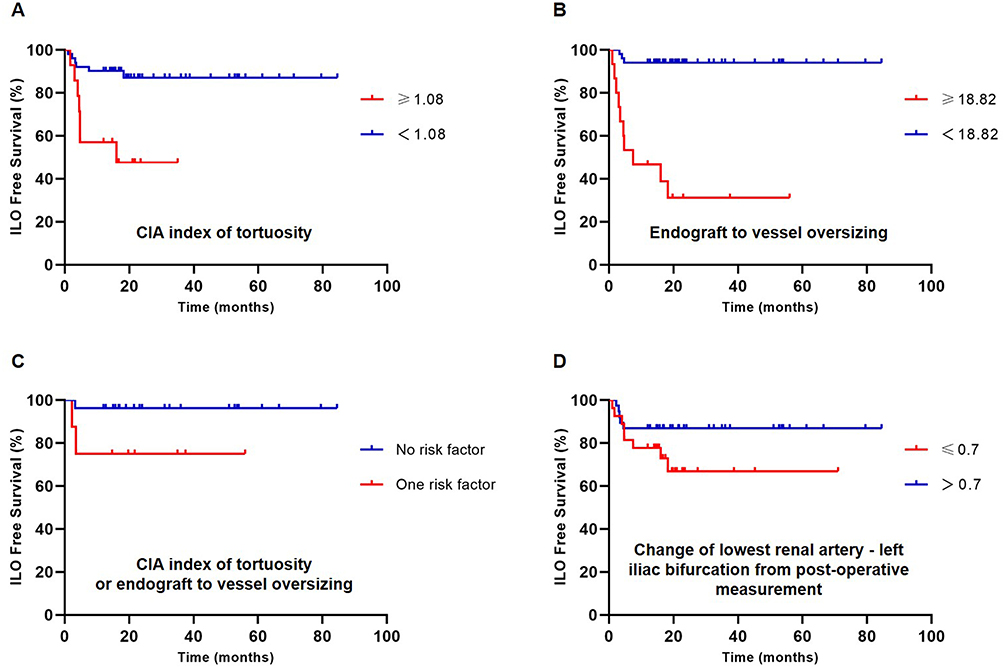 |
Figure 8 Kaplan–Meier analysis of ILO-free survival. (A) tortuosity index of CIA ≥1.08 or <1.08, (B) endograft iliac limb to vessel oversizing ≥18.8% or <18.8%, (C) neither tortuosity index of CIA ≥1.08 nor endograft iliac limb to vessel oversizing ≥18.8% or one risk factor, (D) change of lowest renal artery-left iliac bifurcation from postoperative measurement ≤0.07 mm. Abbreviations: ILO, iliac limb occlusion; CIA, common iliac artery. |
Discussion
We previously reported that ILO following EVAR contributes to tortuous iliac arteries. A CIA index of tortuosity ≥1.08 was identified as an independent risk factor for ILO. This is consistent with two previous studies,10–12 which indicated that the angulation and tortuosity of the CIA were indicators of ILO after EVAR. Long and tortuous iliac arteries were more likely to be associated with endograft limb compression and/or kinking and thrombosis after deployment. When we reviewed the reconstructed CT images in 14 cases with demonstrated ILO following EVAR, endograft kinking occurred in the most angulated CIA in two patients. When tortuosity is located at the CIA close to the iliac bifurcation or distal EIA, it is helpful to avoid endograft limb deployment into the iliac arterial segment of the abrupt transition. When aortoiliac angulation resulted in kinking of the endograft iliac limb, the adjunctive iliac stent in the endograft limb increased resistance against kinking and significantly reduced the risk of postoperative ILO.26,27
Endograft limb oversizing ≥18.82% was recognized as a predisposing factor for ILO in this study. This is in line with two previous studies, which reported that a >15% oversized endograft in the iliac arteries appeared to be an independent predictor of ILO after EVAR.16,17 Excessive oversizing of the endograft may lead to bunching of the endograft limb into relatively small-sized vessels. Radial force of the distal iliac endograft limb in the vessel lumen can result in stenosis and obstruction. In contrast, the extension of the endograft limb into the EIA did not prove to be a significant risk factor for ILO. This is consistent with a study by Mantas et al,16 which indicated that an endograft into the EIA did not impact the ILO. However, previous studies have identified endograft extensions to the EIA as a risk factor for ILO.3,8,9
Significant aortoiliac remodeling, including proximal aortic neck dilation, neck straightening, aneurysm sac regression, aortoiliac elongation, and iliac artery enlargement, occurs after EVAR. Proximal aortic neck dilation may relate to the oversizing and radial force of the stent graft, especially during the early months.18 Dilation in the long term may be due to the natural progression of an aneurysmal wall degeneration.18 The probability of aortic neck dilation rates was reported to be 59% ± 6.1% at 4 years after EVAR.19 Proximal aortic neck dilatation was more rapid at the first postoperative month and at the third postoperative year (24–36 months).20 In the study of Vukovic et al,21 proximal aortic neck diameter expanded by 2 to 4 mm within 1 year. Proximal aortic neck diameter 15 mm below the lowest main renal artery increased from 23.5 ± 2.5 mm at 1 month to 27.3 ± 2.8 mm at 5 years.22 Proximal aortic neck dilatation appeared to be more marked at the level closest to the aneurysm than at the level of the renal arteries.23 Neck angulation changes after EVAR are well documented in the literature.18,22 Proximal aortic neck angulation straightening occurred after EVAR, with a decrease of 0.6 ± 7 degrees from 1 month to 5 years.22 A reduction of aneurysm sac diameter was reported after EVAR with a greater regression rate during the first six postoperative months and at 2 years postoperative interval.20 Significant aortoiliac elongation was observed up to 5 years after EVAR, and aortic measurements included SMA–top of stent graft, SMA–flow divider, SMA–iliac bifurcation, and top of stent graft–iliac bifurcation.24 An expansion of CIA at the distal landing zone was more prominent in the first six postoperative months.18,20 Between 1 month and 5 years, iliac artery diameter at the attachment zone increased from 13.0 ± 3.1 mm to 14.6 ± 3.4 mm and from 13.4 ± 3.4 mm to 16.3 ± 3.8 mm on the right and left sides, respectively.22 The increase at the level of the iliac arteries was distally more marked than at its origin.23
Significant aortic lengthening was observed in the aortoiliac segments over the study period but not in the iliofemoral segments.24 This is in agreement with the results of our study. A recent study demonstrated that aortic elongation occurred after EVAR and did not differ between the patent endograft limb and ILO groups. Aortic elongation was determined by measuring the SMA–lowest renal artery, SMA–top of the stent graft, SMA–flow divider, SMA–and the iliac bifurcation. Aortoiliac measurements were obtained with a focus on the iliofemoral arterial length, including the SMA–left iliac bifurcation, SMA–right iliac bifurcation, lowest renal–left iliac bifurcation, and lowest renal–right iliac bifurcation. This study found an average increase in aortoiliac measurements in patients with patent endograft limb; nevertheless, an average decrease in aortoiliac midline distances was observed in patients with ILO. The change in the distance between the lowest renal artery and the left iliac bifurcation was statistically lower in patients with ILO than in patients with patent endograft limb, and this change ≤0.07 was identified as an independent predictor of ILO after EVAR. It is presumed that aortoiliac tortuosity might result in a decrease in the distance between the lowest renal artery and left iliac bifurcation after EVAR.
This study has several limitations. First, retrospective studies exhibit inherent drawbacks in terms of missing data and selection bias owing to a lack of randomization. Patients with ILO may have been missed, particularly those who developed only mild or no symptoms. The study showed an imbalance in the number of cases treated with each endograft type as well as the total follow-up duration. Second, the number of patients enrolled in the study was sixty-six and relatively small, with a low ILO event rate; 14 patients were diagnosed with ILO after EVAR. Their experience was also limited to only four types of endografts, with no data on ILO with other types of devices. Third, the total number of 527 patients excluded owing to incomplete or inadequate follow-up CT image quality was relatively high and may have biased the reported results.
Conclusion
The tortuosity index of CIA ≥1.08 on preoperative CTA serves as a reliable predictor of ILO after EVAR. Endograft iliac limb-to-vessel oversizing ≥18.8% increased the risk of ILO after EVAR. Aortoiliac remodeling after EVAR involves the expansion of the proximal aortic neck, reduction of the aortic neck angulation, regression of the aneurysm sac diameter, expansion of the iliac arteries, and aortic elongation. Aortoiliac shortening is present in patients with ILO, but not in patients with patent endograft limb. The change in the lowest renal artery to the left iliac bifurcation ≦0.07 between the postoperative and follow-up CT images was independently related to the occurrence of ILO.
Abbreviations
AAA, abdominal aortic aneurysm; CTA, computed tomography angiography; CI, confidence interval; CIA, common iliac artery; EIA, external iliac artery; EVAR, endovascular abdominal aneurysm repair; HR, hazard ratio; IIA, internal iliac artery; ILO, Iliac limb occlusion; LL, larger limb; SL, smaller limb; SMA, superior mesenteric artery.
Funding
This work was funded by the National Natural Science Foundation of China [grant numbers 82370469], Natural Science Foundation of Hubei Province of China [grant number 2022CFB075], Key Laboratory of Biological Targeted Therapy of Hubei Province [grant number 2021swbx020], and Science Foundation of Wuhan Union Hospital [grant number 2021xhyn109].
Disclosure
The authors report no conflicts of interest in this work.
References
1. EVAR trial participants. Endovascular aneurysm repair versus open repair in patients with abdominal aortic aneurysm (EVAR trial 1): randomised controlled trial. Lancet. 2005;365:2179–2186. doi:10.1016/S0140-6736(05)66627-5
2. Patel R, Sweeting MJ, Powell JT, et al. Endovascular versus open repair of abdominal aortic aneurysm in 15-years’ follow-up of the UK endovascular aneurysm repair trial 1 (EVAR trial 1): a randomised controlled trial. Lancet. 2016;388:2366–2374. doi:10.1016/S0140-6736(16)31135-7
3. Bogdanovic M, Stackelberg O, Lindström D, et al. Limb graft occlusion following endovascular aneurysm repair for infrarenal abdominal aortic aneurysm with the zenith alpha, excluder, and endurant devices: a multicentre cohort study. Eur J Vasc Endovasc Surg. 2021;62:532–539. doi:10.1016/j.ejvs.2021.05.015
4. Hammond A, Hansrani V, Lowe C, et al. Meta-analysis and meta-regression analysis of iliac limb occlusion after endovascular aneurysm repair. J Vasc Surg. 2018;68:1916–1924.e7. doi:10.1016/j.jvs.2018.08.153
5. Spath P, Pasqui E, Angiletta D, et al. Penumbra indigo percutaneous aspiration thrombectomy system in the treatment of aortic endograft iliac limb occlusion: results from an Italian multicentre registry. Eur J Vasc Endovasc Surg. 2023;66:77–84. doi:10.1016/j.ejvs.2023.04.008
6. Bianchini Massoni C, Gargiulo M, Freyrie A, et al. Abdominal aortic bifurcation anatomy and endograft limb size affect the use of adjunctive iliac stenting after bifurcated endograft deployment for abdominal aortic aneurysm. J Cardiovasc Surg. 2018;59:237–242. doi:10.23736/S0021-9509.16.08871-6
7. Inaba Y, Yoshitake A, Hayashi K, et al. Effect of the terminal aortic diameter on the patency rate of iliac limbs after endovascular aortic repair. Ann Vasc Dis. 2019;12:519–523. doi:10.3400/avd.oa.19-00080
8. Choi E, Lee SA, Ko GY, et al. Risk factors for early and late iliac limb occlusions of stent grafts extending to the external iliac artery after endovascular abdominal aneurysm repair. Ann Vasc Surg. 2021;70:401–410. doi:10.1016/j.avsg.2020.06.028
9. Faure EM, Becquemin JP, Cochennec F; ENGAGE collaborators. Predictive factors for limb occlusions after endovascular aneurysm repair. J Vasc Surg. 2015;61:1138–45.e2. doi:10.1016/j.jvs.2014.11.084
10. Taudorf M, Jensen LP, Vogt KC, et al. Endograft limb occlusion in EVAR: iliac tortuosity quantified by three different indices on the basis of preoperative CTA. Eur J Vasc Endovasc Surg. 2014;48:527–533. doi:10.1016/j.ejvs.2014.04.018
11. Coulston J, Baigent A, Selvachandran H, et al. The impact of endovascular aneurysm repair on aortoiliac tortuosity and its use as a predictor of iliac limb complications. J Vasc Surg. 2014;60:585–589. doi:10.1016/j.jvs.2014.03.279
12. de Donato G, Pasqui E, Nano G, et al. Long-term results of treatment of infrarenal aortic aneurysms with low-profile stent grafts in a multicenter registry. J Vasc Surg. 2022;75:1242–1252.e2. doi:10.1016/j.jvs.2021.09.036
13. Conway AM, Modarai B, Taylor PR, et al. Stent-graft limb deployment in the external iliac artery increases the risk of limb occlusion following endovascular AAA repair. J Endovasc Ther. 2012;19:79–85. doi:10.1583/11-3550.1
14. Maleux G, Koolen M, Heye S, et al. Limb occlusion after endovascular repair of abdominal aortic aneurysms with supported endografts. J Vasc Interv Radiol. 2008;19:1409–1412. doi:10.1016/j.jvir.2008.07.005
15. Carroccio A, Faries PL, Morrissey NJ, et al. Predicting iliac limb occlusions after bifurcated aortic stent grafting: anatomic and device-related causes. J Vasc Surg. 2002;36:679–684. doi:10.1016/S0741-5214(02)00117-9
16. Mantas GK, Antonopoulos CN, Sfyroeras GS, et al. Factors predisposing to endograft limb occlusion after endovascular aortic repair. Eur J Vasc Endovasc Surg. 2015;49:39–44. doi:10.1016/j.ejvs.2014.09.012
17. Moulakakis KG, Antonopoulos CN, Klonaris C, et al. Bilateral endograft limb occlusion after endovascular aortic repair: predictive factors of occurrence. Ann Vasc Surg. 2018;46:299–306. doi:10.1016/j.avsg.2017.07.019
18. Kapetanios D, Banafsche R, Jerkku T, et al. Current evidence on aortic remodeling after endovascular repair. J Cardiovasc Surg. 2019;60:186–190. doi:10.23736/S0021-9509.19.10878-6
19. Cao P, Verzini F, Parlani G, et al. Predictive factors and clinical consequences of proximal aortic neck dilatation in 230 patients undergoing abdominal aorta aneurysm repair with self-expandable stent-grafts. J Vasc Surg. 2003;37:1200–1205. doi:10.1016/S0741-5214(02)75340-8
20. Tsilimparis N, Dayama A, Ricotta JJ. Remodeling of aortic aneurysm and aortic neck on follow-up after endovascular repair with suprarenal fixation. J Vasc Surg. 2015;61:28–34. doi:10.1016/j.jvs.2014.06.104
21. Vukovic E, Czerny M, Beyersdorf F, et al. Abdominal aortic aneurysm neck remodeling after Anaconda stent graft implantation. J Vasc Surg. 2018;68:1354–1359. doi:10.1016/j.jvs.2018.02.041
22. Torsello G, Pratesi G, van der Meulen S, et al. Aortoiliac remodeling and 5-year outcome of an ultralow-profile endograft. J Vasc Surg. 2019;69:1747–1757. doi:10.1016/j.jvs.2018.09.059
23. Kaladji A, Cardon A, Laviolle B, et al. Evolution of the upper and lower landing site after endovascular aortic aneurysm repair. J Vasc Surg. 2012;55:24–32. doi:10.1016/j.jvs.2011.07.067
24. Chandra V, Rouer M, Garg T, et al. Aortoiliac elongation after endovascular aortic aneurysm repair. Ann Vasc Surg. 2015;29:891–897. doi:10.1016/j.avsg.2014.12.041
25. Yuan Z, Li Y, Jin B, et al. Remodeling of aortic configuration and abdominal aortic branch perfusion after endovascular repair of acute type B aortic dissection: a computed tomographic angiography follow-Up. Front Cardiovasc Med. 2021;8:752849. doi:10.3389/fcvm.2021.752849
26. Oshin OA, Fisher RK, Williams LA, et al. Adjunctive iliac stents reduce the risk of stent-graft limb occlusion following endovascular aneurysm repair with the Zenith stent-graft. J Endovasc Ther. 2010;17:108–114. doi:10.1583/09-2854.1
27. Bianchini Massoni C, Gargiulo M, Giovanetti F, et al. Adjunctive stenting of endograft limbs during endovascular treatment of infrarenal aortic and iliac aneurysms according to 3-projection completion angiography. J Endovasc Ther. 2011;18:585–590. doi:10.1583/11-3467.1
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.