Back to Journals » Journal of Inflammation Research » Volume 19
Predictive Factors And Treatments Associated with Clinical Remission in Severe Eosinophilic Asthma
Authors Lupia C, Marchi G ![]() , Chiarella E, Piazzetta GL, Lobello N
, Chiarella E, Piazzetta GL, Lobello N ![]() , Crimi C, Poto R
, Crimi C, Poto R ![]() , Maglio A, Vatrella A
, Maglio A, Vatrella A ![]() , Pelaia G
, Pelaia G ![]() , Pelaia C
, Pelaia C ![]()
Received 7 January 2026
Accepted for publication 6 March 2026
Published 11 March 2026 Volume 2026:19 552265
DOI https://doi.org/10.2147/JIR.S552265
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Tara Strutt
Chiara Lupia,1 Guido Marchi,2 Emanuela Chiarella,3 Giovanna Lucia Piazzetta,3 Nadia Lobello,3 Claudia Crimi,4 Remo Poto,5 Angelantonio Maglio,6 Alessandro Vatrella,6 Girolamo Pelaia,1 Corrado Pelaia3
1Department of Health Sciences, University “Magna Graecia” of Catanzaro, Catanzaro, Italy; 2Pulmonology Unit, Cardiothoracic and Vascular Department, University Hospital of Pisa, Pisa, Italy; 3Department of Medical and Surgical Sciences, University “Magna Graecia” of Catanzaro, Catanzaro, Italy; 4Department of Clinical and Experimental Medicine, University of Catania, Catania, Italy; 5Department of Translational Medical Sciences, University of Naples Federico II, Naples, Italy; 6Department of Medicine, Surgery, and Dentistry, University of Salerno, Salerno, Italy
Correspondence: Corrado Pelaia, University “Magna Graecia” of Catanzaro, Department of Medical and Surgical Sciences, Viale Europa – Località Germaneto, Catanzaro, 88100, Italy, Tel + 39 0961 3647007, Fax + 39 0961 3647193, Email [email protected]
Abstract: Severe eosinophilic asthma represents a relatively small proportion of the overall asthma population but accounts for a disproportionate burden of exacerbations, oral corticosteroid (OCS) exposure and healthcare use. The advent of biologic therapies targeting type 2 (T2) inflammation has made clinical remission a realistic goal and raised new questions about how and when to de-escalate inhaled corticosteroids (ICS) and biologics in patients achieving stable disease. This narrative review summarizes current evidence and expert recommendations on: definitions and levels of clinical remission in severe eosinophilic asthma; the role of different biologics in inducing remission; safety and feasibility of ICS and biologic de-escalation after remission; and clinical and biological predictors of sustained remission and successful step-down. Biologics such as anti-IgE, anti-IL-5/5Rα, anti-IL-4Rα and anti-thymic stromal lymphopoietin (TSLP) markedly reduce exacerbations, OCS use and, in a substantial minority of patients, induce clinical or “deep” remission on-treatment. Prospective randomized controlled trials and real-world data (e.g. SHAMAL and registry studies) indicate that structured, physician-guided ICS reduction is feasible for many patients without loss of control, whereas abrupt or unsupervised reduction is associated with worse outcomes. Evidence on biologic withdrawal is more heterogeneous: discontinuation of mepolizumab, tezepelumab or omalizumab frequently leads to loss of control, although a subset maintains remission off-treatment. Favorable predictors of remission and tolerability of de-escalation include fewer prior exacerbations, lower chronic OCS exposure, shorter disease duration, better preserved FEV1 and effective suppression of T2 biomarkers. Within the context of severe eosinophilic asthma remission, de-escalation of therapy may follow a cautious, hierarchical, clinician-led strategy prioritizing OCS, then ICS, and only subsequently biologics, with predefined failure criteria and shared decision-making. This proposed pathway is presented as a pragmatic synthesis of the available evidence and should be interpreted as expert opinion rather than formal guideline recommendations. Robust, standardized definitions and validated predictors are still needed to safely expand off-treatment remission to a larger proportion of patients.
Keywords: severe asthma, clinical remission, predictive factors, biologic therapies, de-escalation
Introduction
Asthma is a chronic inflammatory disease of the airways characterized by variable respiratory symptoms, such as dyspnea, cough, wheeze and chest tightness, and by usually reversible airflow limitation that fluctuates over time.1 It affects millions of individuals worldwide and is associated with substantial impairment in quality of life, work and school absenteeism, and considerable direct and indirect healthcare costs.1 Within this heterogeneous spectrum, severe asthma accounts for a minority of patients but is responsible for a disproportionate share of the overall disease burden: it remains uncontrolled despite optimized high-dose inhaled corticosteroids (ICS) in combination with long-acting β2-agonists (LABA) and appropriate management of comorbidities, or requires such intensive treatment to maintain acceptable control.2,3 In these patients, severe exacerbations, emergency department visits, hospitalizations and recurrent or chronic use of oral corticosteroids (OCS) are more frequent, with important consequences for long-term prognosis. Over the past few years, the international scientific community has shown growing interest in the concept of clinical remission in asthma, and particularly in severe asthma.4 The traditional therapeutic approach has been centered on ICS, used alone or in combination with other controllers and adjusted in a stepwise fashion according to symptom control, with the aim of achieving what is perceived as an acceptable clinical equilibrium.5 This strategy, however, carries the risk of overexposure to corticosteroids, both inhaled and systemic, with potentially relevant short- and long-term adverse effects.6 In parallel with what has occurred in other chronic inflammatory diseases, such as rheumatoid arthritis and inflammatory bowel disease, the notion of remission has emerged in asthma as a more ambitious treatment goal, encompassing not only symptom control but also preserved lung function, improved health-related quality of life and the absence of a need for systemic corticosteroids over a prolonged period, often defined as at least twelve months.4,7 The advent of biologic therapies has markedly transformed the management landscape of severe asthma. These long-acting agents, often described as Disease Modifying Anti-Asthmatic Drugs (DMAADs), target key pathways of type 2 inflammation in a selective manner and may, at least in theory, influence airway remodeling processes.4,8 Their use has revolutionized the impact of severe asthma on patients’ lives in recent years, primarily by reducing the need for long-term OCS and the frequency of severe exacerbations.6,9 Against this background, an important clinical question has emerged: once clinical remission or a stable, well-controlled disease state has been achieved, is it possible to safely taper, and potentially reduce to a minimum, maintenance ICS therapy?10 It is now well documented that biologics can enable a substantial reduction in the dose of systemic corticosteroids required to maintain asthma control.11
Whether a similar de-escalation strategy can be extended to more stable patients with severe asthma who are well controlled on biologic therapies remains a matter of debate.12 In patients with severe eosinophilic asthma in stable good control, decisions about tapering or discontinuing biologics must balance the potential benefits of reducing treatment burden and adverse effects against the risk of relapse, loss of disease control and permanent deterioration of lung function, particularly in the presence of relevant comorbidities such as eosinophilic granulomatosis with polyangiitis or chronic rhinosinusitis with nasal polyps (CRSwNP).13 In this narrative review, we first summarize current evidence on predictive clinical, functional and biological factors associated with achieving clinical remission in severe eosinophilic asthma, with a particular focus on patients treated with biologic agents. We then discuss how different biologic and background therapies can be used and optimized to induce and maintain remission, and under which circumstances inhaled corticosteroids and biologic treatments may be safely de-escalated once clinical remission, whether spontaneous or treatment-induced, has been established. Our review provides a pragmatic synthesis of operational definitions of on-treatment, off-treatment and deep remission, summarizes the available evidence on step-down of ICS and on biologic de-escalation/withdrawal after remission, and proposes a clinician-facing, stepwise de-escalation algorithm; this framework should be interpreted as expert opinion given the current evidence gaps.
We conducted a targeted literature search in PubMed/MEDLINE and Embase up to September 2025 using combinations of keywords related to severe asthma, eosinophilic phenotype, clinical remission, biologic therapy, withdrawal/discontinuation, de-escalation, and inhaled corticosteroid (ICS) step-down. We prioritized randomized controlled trials and extension studies, complemented by real-world observational cohorts and consensus/Delphi statements; reference lists of relevant papers were hand-searched to identify additional studies.
Severe Eosinophilic Asthma: Definition, Epidemiology and Clinical Burden
Severe asthma is now recognized as a distinct and heterogeneous subset within the broader asthma population.2 Current international guidelines define severe asthma as a disease that remains uncontrolled despite adherence to high-dose ICS plus a second controller, usually a LABA, and optimal management of contributory factors and comorbidities, or that worsens when this treatment is reduced.2,3 Before labelling asthma as “severe”, physicians are expected to reassess the diagnosis, inhaler technique, adherence, and the presence of modifiable risk factors such as active smoking, environmental exposures or untreated upper airway disease.14
Subjects with severe asthma represent a small proportion of all people with asthma, commonly estimated at around 3–10% of the total asthmatic population, yet they account for a disproportionately high share of the overall disease burden.15 Patients with severe asthma are more likely to experience frequent and sometimes life-threatening exacerbations, repeated emergency department visits and hospitalizations, and they are often exposed to recurrent or continuous OCS courses.16 These patterns of disease activity and treatment use are associated with increased mortality, substantial healthcare utilization and considerable direct and indirect costs.17 Beyond the economic impact, severe asthma imposes a heavy toll on daily functioning, participation in work or education, and psychological well-being, with many patients reporting persistent fear of exacerbations and a sense of unpredictability about their disease.18 Clinically and biologically, severe asthma is not a single entity but a heterogeneous spectrum of phenotypes and endotypes.19 A sizeable proportion of patients exhibit a type-2 (T2)-high inflammatory pattern, often characterized by eosinophilia, elevated fractional exhaled nitric oxide (FeNO), and comorbid conditions such as CRSwNP or atopic dermatitis.20 Others express non-T2 or mixed inflammatory profiles, in which neutrophilic or pauci-granulocytic patterns predominate and for whom targeted therapies are less well established.21 Additional layers of complexity arise from age of onset, obesity, smoking status and the presence of overlapping conditions such as bronchiectasis or chronic obstructive pulmonary disease.21 Taken together, these features explain why severe asthma continues to be a major unmet clinical need. Despite advances in pharmacological options and in the understanding of underlying mechanisms, many patients remain at risk of exacerbations, lung function decline and treatment-related adverse effects, particularly from long-term OCS exposure. It is within this context that the concept of clinical remission and the possibility of safely de-escalating therapy, first ICS and, potentially, biologics, have gained prominence as emerging treatment goals in severe asthma.
Definition of Clinical Remission
For many years, the primary therapeutic goal in asthma has been to achieve and maintain good disease control. In practice, this has meant minimizing day- and night-time symptoms, reducing the need for reliever medication, preventing exacerbations and preserving lung function as far as possible. These domains are commonly assessed through validated symptom questionnaires and spirometry, and have provided a pragmatic background for tailoring treatment intensity.22–25 Within this paradigm, step-up or step-down decisions are driven by the degree of control achieved under a given regimen, rather than by a clearly defined endpoint beyond “well-controlled” disease.26
More recently, the concept of clinical remission has emerged as a potential extension of this traditional notion of control.4 While there is no universally accepted definition, most proposed frameworks converge on a set of core elements: absence or near-absence of asthma symptoms, no exacerbations requiring systemic corticosteroids or urgent healthcare utilization over a sustained period, stable or improved lung function, and no need for maintenance oral corticosteroids.27 These criteria are typically required to be met for at least 12 consecutive months to distinguish remission from transient periods of good control.28 Because lung-function “stability” is defined heterogeneously across remission frameworks, we adopted a pragmatic operationalization aimed at avoiding misclassification due to spirometric test variability: absence of a sustained, clinically meaningful decline in FEV1, ie. changes within the usual measurement variability (approximately 100 mL) and without a persistent ≥10% relative reduction over the observation period. This approach is clinically relevant in severe asthma, where complete normalization of FEV1 may be unattainable due to fixed airflow limitation. In some definitions, improvements in patient-reported quality of life and minimal rescue medication use are also explicitly included.29
It is useful to distinguish among different levels of remission. Clinical remission on-treatment refers to a state in which the patient fulfils the above criteria while continuing maintenance therapy, which may include inhaled corticosteroids and/or biologic agents.30 Complete remission is sometimes used to describe a more stringent condition in which clinical remission is accompanied by normalization of lung function and, in some proposals, evidence of quiescent airway inflammation.31 A further, more ambitious concept is that of clinical remission off-treatment, where the same criteria are maintained after withdrawal of controller medications. In routine clinical setting, however, most discussion currently focuses on clinical remission on-treatment as a realistic and measurable target. Indeed, in everyday practice, many patients with severe eosinophilic asthma experience substantial but incomplete improvement under biologic therapy. For these individuals, we propose the term partial remission as a pragmatic intermediate construct between symptom control and full clinical remission. Partial remission can be recognized as a sustained, clinically meaningful reduction in disease burden (eg., no hospitalizations, ≤1 OCS-treated exacerbation, reduced maintenance OCS exposure, and improved symptoms and quality of life) while at least one domain remains below strict remission thresholds, most commonly lung function and/or T2 biomarkers. This concept may help to guide treatment optimization and shared decision-making in real-world practice, but it requires prospective validation and harmonization across studies. Typical examples include patients who have discontinued maintenance OCS and no longer require emergency care, yet retain residual symptoms, impaired lung function or persistently elevated type 2 (T2) biomarkers. Recognizing partial remission is relevant for both patient communication and therapeutic decision-making: it acknowledges the magnitude of response while emphasizing that the disease remains active and that aggressive de-escalation, particularly of biologic therapy, may be premature. In the present framework, partial remission is therefore considered as a desirable but still transitional state, which may justify cautious reduction of OCS and, in selected cases, inhaled corticosteroids (ICS), but generally not complete withdrawal of anti-inflammatory maintenance therapy.30–32 Proposed definitions of clinical remission are summarized in Table 1.
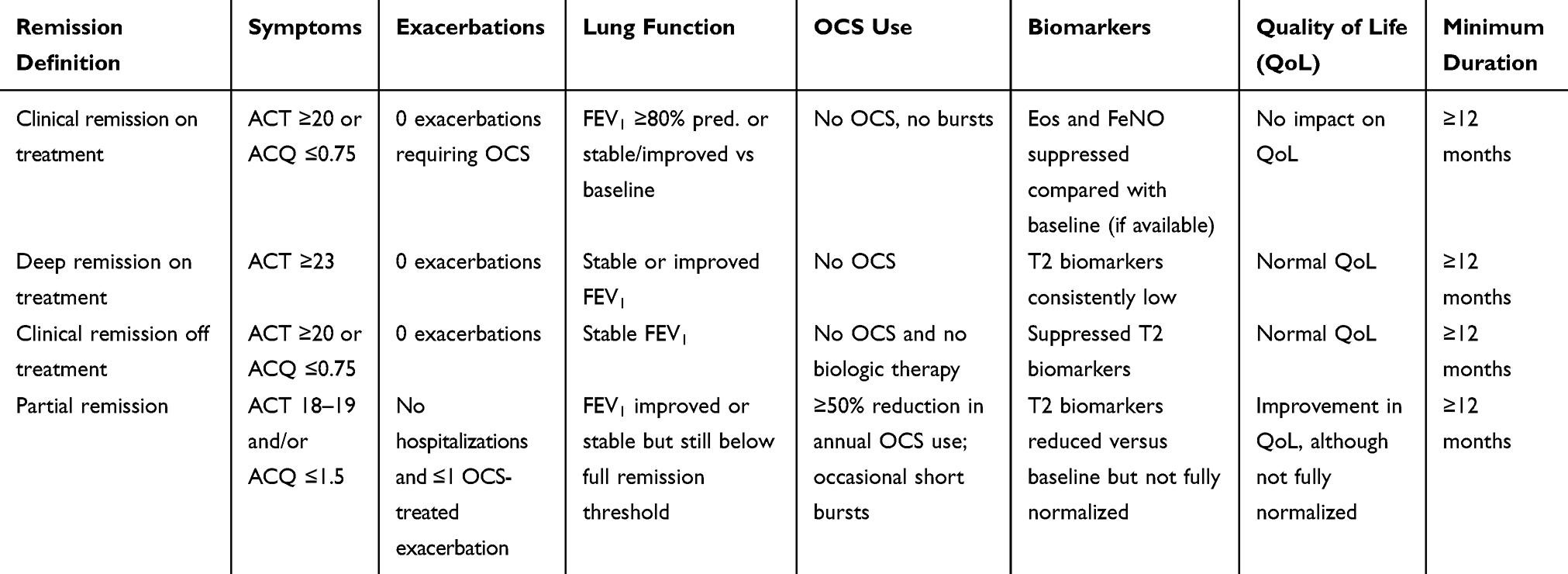 |
Table 1 Proposed Operational Definitions of Remission in Severe Asthma |
It is also important to acknowledge that remission components can be observed in patients not receiving biologic therapy, including placebo arms of randomized trials and real-world cohorts managed in structured specialist settings. In biologic trials, a small but non-negligible proportion of placebo-treated participants fulfil multi-component remission definitions over 12 months, likely reflecting optimized background therapy, improved adherence, structured follow-up and regression to the mean rather than a true disease-modifying effect.10 These effects should be considered when interpreting remission rates and when attributing remission exclusively to biologic treatment.
Moving from control to remission as a treatment goal carries several conceptual and practical implications. First, remission implies not only the absence of troublesome symptoms and exacerbations, but also a degree of stability and robustness of this favorable state over time. Second, it raises the question of how intensively patients should be treated to achieve and maintain such a condition, and, conversely, whether treatment can be safely reduced once remission has been established. Third, it highlights the need for reliable, operational definitions that can be applied consistently across studies and in clinical practice, allowing meaningful comparison of outcomes and clear communication with patients.33
At present, several challenges remain. Definitions of remission vary across studies in terms of the required duration, the stringency of symptom and lung function thresholds, and the role assigned to biomarkers of airway inflammation. The heterogeneity of severe asthma, with its diverse phenotypes and endotypes, further complicates this scenario, as the likelihood of achieving remission and the stability of that state may differ markedly among patients. In addition, the instruments used to assess symptoms, quality of life and exacerbations are not always harmonized, thus limiting comparability between cohorts.
Despite these uncertainties, the shift towards remission reflects a broader change in perspective: from simply preventing worsening to aiming for the best possible long-term outcome for each individual patient. In severe asthma, where the burden of disease and treatment remains substantial, this evolving concept has direct implications for how clinicians think about initiating, maintaining and eventually de-escalating high-intensity therapies, including inhaled corticosteroids and biologic agents.
Biologic Treatments to Achieve Clinical Remission in Severe Eosinophilic Asthma
The therapeutic landscape of severe asthma has changed markedly with the availability of several biologic agents targeting distinct pathways of type 2 inflammation.8,34 These drugs are added to high-dose inhaled corticosteroids and long-acting bronchodilators in patients with persistent symptoms and/or frequent exacerbations, and are selected on the basis of clinical phenotype, biomarkers and comorbidities.9 Although biologic therapies share the extensive goals of reducing exacerbations, improving control and sparing OCS, their specific targets and ideal candidate profiles differ, which is highly relevant when considering their potential to induce or maintain clinical remission.35 Omalizumab, the first biologic approved for asthma, is an anti-IgE monoclonal antibody for allergic severe asthma with sensitization to perennial allergens.36 It inhibits IgE-mediated responses and has consistently been shown to lower exacerbation rates and improve control.37 Anti-IL-5 and anti-IL-5 receptor agents (mepolizumab, reslizumab, benralizumab) are indicated in eosinophilic severe asthma and act by neutralizing IL-5 or depleting eosinophils, thereby producing marked reductions in disease exacerbations and OCS use, with benralizumab achieving near-complete eosinophil depletion.38,39 Dupilumab, targeting the IL-4 receptor α and thereby blocking IL-4/IL-13-driven signaling, addresses a broader type 2-high population characterized by eosinophilia or elevated FeNO, and is particularly attractive in the presence of CRSwNP or atopic dermatitis.40 Tezepelumab, an anti-TSLP monoclonal antibody, neutralizes an upstream epithelial alarmin and has demonstrated efficacy across a wider biomarker spectrum, including some patients with lower eosinophil counts, thus extending biologic options beyond the “classic” type 2-high profile.41
Collectively, these modern therapeutic agents support the view of biologics as potential disease-modifying anti-asthmatic drugs rather than simple add-on controllers. By targeting key inflammatory drivers, they can decrease or eliminate maintenance OCS, stabilize lung function and markedly lower the exacerbation burden.42 In a subset of appropriately selected patients, the resulting long-lasting stability may satisfy the proposed criteria for clinical remission on-treatment.43 At the same time, heterogeneous responses, the influence of comorbidities and differences in mechanism of action mean that the choice of a given biologic—and its long-term role in any de-escalation strategy—must be carefully individualized. Key clinical trials and real-world studies on clinical remission with T2 biologics in severe eosinophilic asthma are summarized in Table 2.
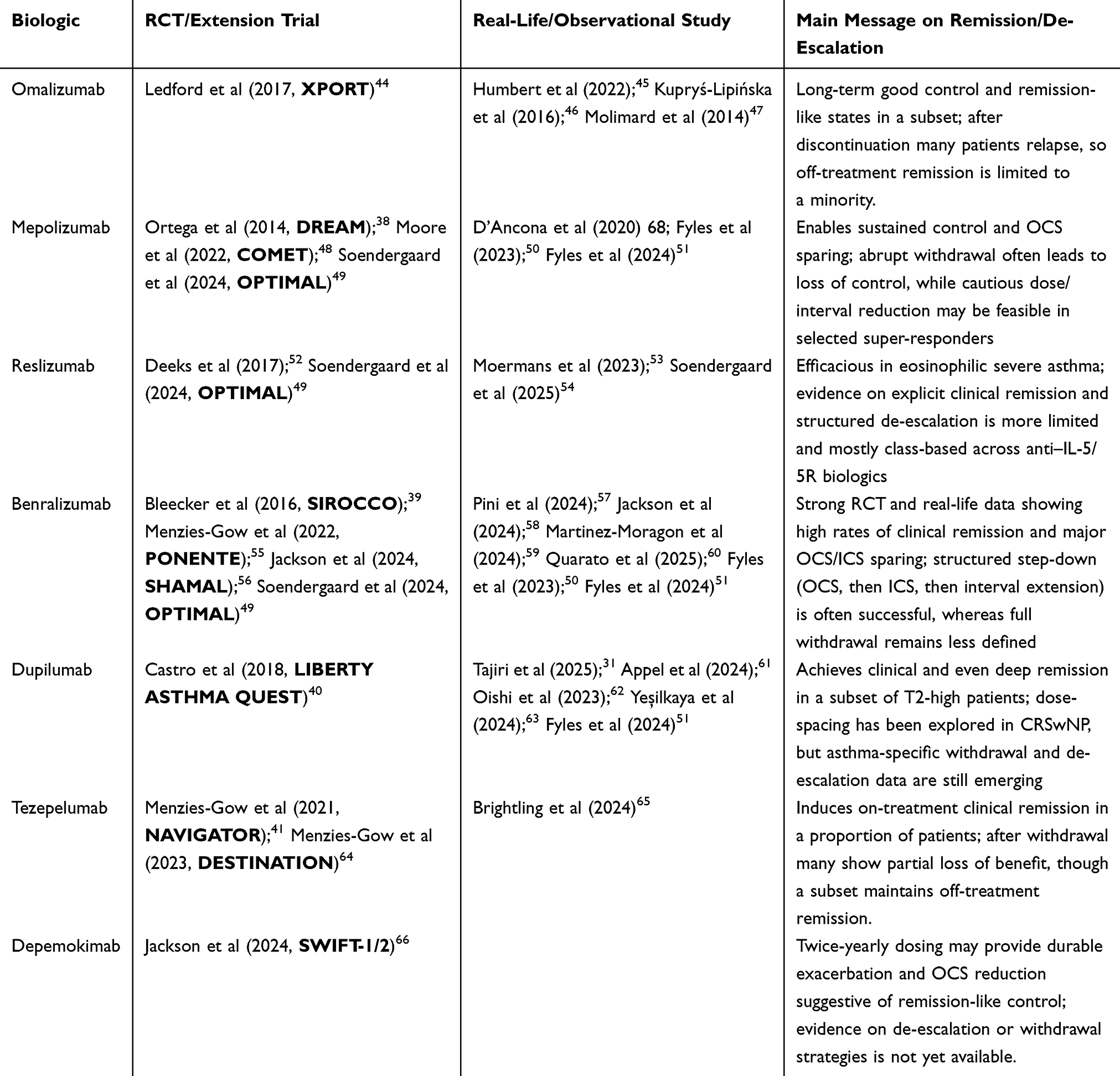 |
Table 2 Summary of Key Clinical Trials and Real-World Studies on Clinical Remission with T2 Biologics in Severe Eosinophilic Asthma |
Predictive Factors for Achieving Clinical Remission in Severe Eosinophilic Asthma
Not all patients with severe asthma appear equally likely to achieve a stable remission or to tolerate de-escalation of treatment without loss of control. Identifying clinical and biological predictors of sustained remission is therefore central to a more rational and personalized approach. Real-world cohorts and post-hoc analyses of clinical trials suggest that remission and “deep” remission occur in a substantial minority of biologic-treated patients, but with considerable heterogeneity between individuals and across drugs.62,67
Clinical Predictors
From a clinical standpoint, several features repeatedly emerge as favorable. Patients who achieve clinical or deep remission tend to have fewer exacerbations and lower OCS requirements before biologic initiation, better preserved lung function and shorter asthma duration than non-remitters.
Importantly, predictors of relative treatment response may differ from predictors of achieving remission. For example, GINA highlights that a higher number of severe exacerbations in the previous year, baseline maintenance OCS use and lower baseline lung function (eg., FEV1 <65% predicted) are associated with a higher likelihood of clinical benefit from anti–IL-5/IL-5Rα therapy.1 These markers identify patients with more active T2-driven disease and higher baseline risk who may show large relative improvements on treatment; however, they also denote greater baseline severity and/or fixed obstruction, which can make it harder to meet stringent remission thresholds. Where “shorter asthma duration” has been associated with remission, emerging data suggest that the duration of severe asthma/high-intensity treatment may be more informative than total asthma duration, and longer overall disease duration does not uniformly imply a lower remission probability.63 In a real-world cohort of severe asthma patients treated with different biologics, higher baseline FEV1% predicted was the only independent predictor of 12- and 36-month remission.58 Similarly, Oishi et al showed that “deep remission” – defined as clinical remission plus normalized lung function and suppressed type 2 (T2) inflammation – was associated with shorter disease duration and FEV1 around 90% predicted at baseline.62 Other long-term benralizumab and mepolizumab series report higher remission rates in patients with adult-onset asthma, absence of fixed airflow limitation and lower chronic OCS exposure at baseline. In contrast, long-standing disease, persistent fixed obstruction, current or former smoking, obesity and multiple comorbidities consistently appear as barriers to remission.50,59,60
Biomarkers and Differentiation Between Biologic Classes
Biologically, markers of type 2 inflammation, such as blood eosinophil counts and FeNO levels, remain the most widely studied candidates. However, across biologic classes, response signals show some consistent patterns. For anti–IL-5/IL-5Rα therapies, better outcomes are most often seen in patients with higher baseline blood eosinophil counts and a prior history of exacerbations and/or OCS use; reaching more stringent remission criteria tends to be linked with better preserved FEV1 and with a shorter duration of severe asthma, while baseline FeNO is a less reliable predictor for this class. With anti–IL-4Rα treatment, elevated FeNO and/or blood eosinophils, together with T2 comorbidities such as CRSwNP or atopic dermatitis, are commonly associated with greater clinical benefit and may increase the chance of achieving remission. Anti-TSLP therapy shows efficacy across a wide range of biomarker levels, although higher eosinophils and/or FeNO generally correspond to larger treatment effects; predictors of remission and the durability of control after stopping treatment are still being defined. For anti-IgE therapy, selection is primarily driven by evidence of allergic sensitization and meeting dosing eligibility based on IgE level and body weight; remission evidence is comparatively limited, and discontinuation studies indicate that relapse is frequent in a substantial proportion of patients. Moreover, biomarkers should not be used in isolation to define disease control or remission. In most proposed remission definitions, biomarker suppression is at most a supportive domain (more often associated with “deep remission”) rather than a mandatory criterion for clinical remission. Elevated blood eosinophil counts and FeNO levels prior to biologic initiation are well-established predictors of response to anti-IL-5/5Rα, anti-IL-4Rα and anti-TSLP therapies. A recent systematic review found moderate-to-high quality evidence that blood eosinophils ≥300 cells/µL, FeNO >40 ppb, lower OCS dose (<10 mg/day) and better baseline control predict favorable treatment outcomes.68 However, their role as predictors of sustained remission or safe de-escalation is less clearly defined. Some studies suggest that patients who ultimately enter remission have higher baseline airway T2 activity (eg., increased sputum eosinophils, eotaxin-1, IL-5, eosinophil peroxidase) but show profound suppression of these markers under therapy, particularly with anti-IL-5/5Rα agents.53 In routine practice, persistently low blood eosinophil counts under treatment, together with stable or decreasing FeNO, may indicate effective suppression of T2 inflammation and therefore support attempts to reduce ICS or biologic dosing, whereas rising eosinophils or FeNO during tapering often precede or accompany functional decline and may serve as early warning signs requiring re-intensification of therapy.54,69–71
Airway-based biomarkers may further refine risk stratification. Sputum eosinophil counts and related T2 markers (eg., IL-5, TSLP, EPX) have been proposed as predictors of on-biologic remission after anti-IL-5 or anti-IL-5Rα therapy, although their use is limited by availability and standardization outside specialized centres.72,73 Emerging data also suggest that lower sputum IL-6 and IL-8 – reflecting less neutrophilic inflammation – may be associated with a higher likelihood of remission under anti-IL-5Rα treatment.74
Comorbidities and Patient-Reported Outcome Measures
Comorbidity burden is another key determinant of remission. Uncontrolled treatable traits such as upper-airway disease, obesity, gastro-oesophageal reflux, obstructive sleep apnoea, bronchiectasis/COPD overlap and anxiety or dysfunctional breathing can perpetuate symptoms and risk, thereby lowering the likelihood of meeting stringent remission criteria. Conversely, parallel improvement of T2-driven comorbidities (eg., CRSwNP, atopic dermatitis) may signal a broader “multimorbid” response and support a higher probability of sustained clinical remission when these conditions are proactively managed.10 More specifically, CRSwNP is a prototypical T2 comorbidity and its presence—and improvement with optimal comorbidity management or targeted biologic therapy—may reflect a “united airways” response associated with a higher probability of sustained clinical remission.13
Patient-reported outcome measures (PROMs) also have a role in this context. Tools such as the ACQ and the Asthma Control Test (ACT), alongside health-related quality-of-life instruments, provide a structured way to track the subjective dimension of disease control over time.22,23 In studies searching for “super-responders”, stringent symptom and exacerbation criteria (eg., elimination of exacerbations, ACQ improvement ≥2× MCID, withdrawal of maintenance OCS) are combined with stable or improved lung function to define highly responsive phenotypes.75,76 These composite profiles are intuitively attractive as predictors of successful de-escalation and have been incorporated into real-world definitions of clinical and deep remission, but they have not yet been formally validated across different populations and biologic agents.
Key-Point Summary
Finally, the relationship between symptom perception, lung function and biomarker trajectories is not always linear. Some patients report excellent symptom control despite residual airflow limitation or biochemical evidence of ongoing type 2 inflammation, while others have prominent symptoms driven by comorbidities or dysfunctional breathing despite apparently “quiet” airways. This underscores the importance of integrating multiple domains—clinical history (including exacerbation and OCS burden), spirometry, biomarkers and PROMs—when estimating an individual patient’s likelihood of sustained remission and their suitability for treatment de-escalation, rather than relying on any single isolated parameter. In summary, key determinants of clinical remission in severe asthma can be condensed as follows: (i) remission is achieved by only a subset of biologic-treated patients and long-term durability is still being defined; (ii) the most consistent predictors are preserved lung function, low chronic OCS exposure, fewer prior exacerbations, and shorter duration of severe asthma/high-intensity treatment; (iii) response predictors may differ from remission predictors, since high baseline severity can produce larger gains yet still hinder stringent remission (eg., due to fixed obstruction); (iv) eosinophils and FeNO guide response and monitoring—stable suppression supports control, while increases during tapering may anticipate relapse; and (v) comorbidities strongly modulate remission likelihood, so assessment should integrate history, spirometry, biomarkers and PROMs.
Predictive factors for clinical remission in severe eosinophilic asthma are summarized in Figure 1.
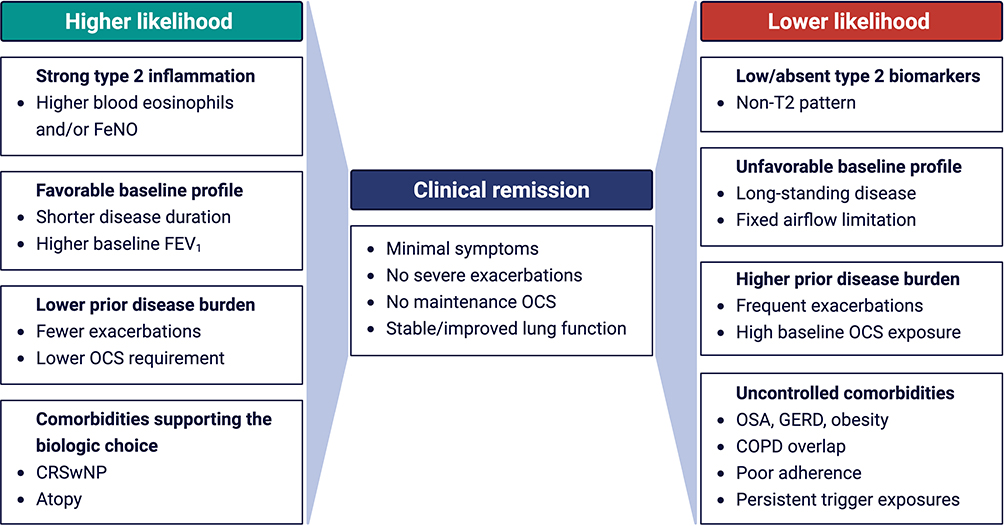 |
Figure 1 Predictive factors for clinical remission in severe eosinophilic asthma. |
Evidence for ICS De-Escalation After Clinical Remission
One of the most relevant questions arising when clinical remission on-treatment is achieved under biologic therapy is whether the maintenance dose of ICS can be safely and effectively reduced. Although ICS are generally believed to be safer than systemic corticosteroids, prolonged exposure to high doses is associated with an increased risk of adverse events, ranging from mild local effects (hoarseness, pharyngitis, oropharyngeal candidiasis) to more serious systemic complications (adrenal suppression, cataract, osteoporotic fractures and diabetes), in a dose-dependent manner.77 Considering these concerns, current Global Initiative for Asthma (GINA) recommendations advise clinicians to consider ICS dose reduction in patients with severe asthma who respond well to biologic agents.1 In the inhaled step-down sequence, GINA further suggests withdrawing add-on inhaled therapies (eg., long-acting muscarinic antagonists, LAMA) before reducing the ICS–LABA dose.1 In practice, this sequence is intended to preserve the protective effect of ICS on exacerbation risk while simplifying therapy: thus, in patients with sustained control, the first step is usually discontinuation of LAMA, with subsequent cautious reduction of ICS dose only after stability is confirmed (no exacerbations, stable lung function and symptoms) over follow-up. Exceptions may be considered when LAMA provides clear ongoing bronchodilator benefit (eg., persistent airflow limitation) or when ICS-related adverse effects mandate earlier dose reduction, but even in these cases step-down should be individualized and closely monitored. Further studies are needed to define the safest and most effective de-escalation algorithms across different phenotypes and risk profiles.
The SHAMAL trial provided important prospective evidence in this regard.56 In patients with severe eosinophilic asthma well controlled on benralizumab, stepwise reduction of maintenance ICS–formoterol to the lowest effective dose was shown to be both safe and feasible.56 In approximately 92% of participants, ICS doses could be reduced without loss of asthma control, and more than 60% were able to switch to an as-needed ICS regimen. Within the reduction arm, however, a mild but statistically significant association was observed between rising FeNO levels and FEV1 decline, with the greatest deterioration in lung function seen in patients who had shifted to ICS on demand only.56 The authors hypothesized that the FeNO increase following ICS reduction reflected residual, non-eosinophilic airway inflammation that remained ICS-responsive, leading to a modest impairment in lung function without a corresponding increase in exacerbations. Whether similar step-down strategies are equally safe with other biologics remains to be established, although encouraging data are emerging from the tezepelumab extension trial DESTINATION and the Phase 3 SWIFT-1 and SWIFT-2 studies assessing the long-acting anti-IL-5 depemokimab.64,66
Real-life data from the Severe Asthma Network in Italy (SANI) registry further support the possibility of ICS de-escalation in patients on benralizumab.57 Pini et al retrospectively evaluated 92 patients treated with benralizumab for at least 36 months. Most remained on their baseline ICS dose (66.3%), but in about 30% a reduction in inhaled therapy was achieved, most documented at the 36-month follow-up visit. When comparing patients with stable versus reduced ICS doses, no statistically significant differences were found in blood eosinophil counts, lung function, patient-reported outcomes or exacerbation rates. ICS de-escalation did not lead to increased OCS use, instead maintaining a sustained OCS-sparing effect. Baseline characteristics such as sex, age, body mass index (BMI), smoking history, age at diagnosis and concomitant CRSwNP were similar between groups, suggesting that a gradual ICS reduction can be successfully attempted irrespective of demographic profile or traditional risk factors for loss of control. Notably, patients in whom ICS tapering was successful had a lower frequency of OCS use at baseline, indicating that limited prior OCS exposure may be a predictor of successful ICS de-escalation.57 Although FeNO data were not reported, the persistent suppression of blood eosinophils in both groups not only supports the presence of an effective biologic response, but also points to blood eosinophil counts as a potentially useful biomarker to guide de-escalation strategies.
Different findings were reported in a study by D’Ancona et al, which included 91 patients with severe eosinophilic asthma treated with mepolizumab for 12 months.78 In this cohort, 68% maintained good adherence to ICS, whereas 18% had poor adherence. Patients with good ICS adherence experienced a greater reduction of OCS dose(p = 0.031), higher rates of OCS discontinuation (p = 0.045) and a lower tendency to exacerbations (p = 0.011) compared with poorly adherent patients, suggesting that suboptimal ICS use predisposes to poorer disease control despite biologic therapy.78 These results should not be interpreted as evidence that mepolizumab is less effective than benralizumab in enabling ICS reduction; rather, they highlight that decisions regarding ICS de-escalation should be led by the clinician, based on objective measures of control and risk, rather than by the patient’s subjective sense of well-being or non-adherence.
Further insight comes from a retrospective study by Fyles et al, who examined 70 patients with severe asthma classified as “super-responders” to biologic therapy (omalizumab n = 8, mepolizumab n = 14, benralizumab n = 48).51 Super-responders were defined by the absence of OCS use and exacerbations. The authors reported treatment outcomes at 12 and 24 months after standard inhaled therapy had been stepped down, either following a clinician’s decision or because of poor adherence. Neither physician-guided de-escalation nor poor adherence were associated with a significant overall deterioration in asthma control; however, clinician-driven tapering appeared safer and preferable, as reflected by significantly better scores on Asthma Control Questionnaire (ACQ). Taken together, these data suggest that ICS reduction is feasible in a substantial proportion of patients achieving clinical remission on biologics, but that it should be pursued in a structured, physician-supervised manner, ideally supported by objective markers of disease activity and careful longitudinal monitoring.
Evidence for Biologic De-Escalation and Discontinuation After Clinical Remission
The question of whether, and at what point, biologic therapy can be discontinued after achieving clinical remission in severe asthma—while still maintaining disease control—remains largely unresolved and requires more robust evidence. Studies examining withdrawal or dose reduction of biologics have yielded heterogeneous results, influenced by the specific agent, the tapering strategy employed and the characteristics of the study population. At present, there is no clear consensus on the optimal duration of treatment or on the safest approach to stop biologic therapy; available data are molecule-specific and often limited in follow-up.
For mepolizumab, the COMET (Cessation Versus Continuation of Long-term Mepolizumab Treatment) trial provides the most informative evidence.48 In patients with severe eosinophilic asthma treated for at least three years, discontinuation of mepolizumab led to loss of disease control and an increased risk of exacerbations, accompanied by a rise in blood eosinophil counts back towards pre-treatment levels.68 Within the first year after withdrawal, 59% of patients experienced at least one clinically significant exacerbation. Worsening of morning peak expiratory flow was observed from week 4, together with deterioration in daily symptom scores, increased need for rescue medication and more frequent unscheduled healthcare use, underscoring the clinical consequences of abrupt cessation.48 For benralizumab, specific studies focusing on withdrawal in patients in remission are not yet available, so evidence is limited to extrapolations from general extension studies and clinical experience.
More detailed post-withdrawal data exist for tezepelumab. In a 40-week follow-up phase after two years of active treatment, patients showed a gradual loss of clinical benefit, with progressive increases in blood eosinophil counts and FeNO levels, and a decline in FEV1; however, none of these parameters fully returned to pre-treatment baselines, while IgE levels remained low throughout follow-up.65 Among the 33% of patients (127/379) who had achieved clinical remission on-treatment with tezepelumab, 22% maintained remission off-treatment at the end of the 40-week observation period.65 These findings suggest that a subset of patients may sustain disease control and even remission after withdrawal, though the majority exhibit at least some degree of relapse.
The evidence regarding omalizumab discontinuation is particularly variable, reflecting differences in treatment duration and patient selection. Overall, long-term continuation appears to confer greater benefit in symptom control and exacerbation prevention than stopping therapy. In one study, 67% of patients who continued omalizumab remained exacerbation-free, compared with 47.7% of those who discontinued; time to first exacerbation was also significantly longer in the continuation group.44 The multicentre randomized XPORT trial reported that 33% of patients who stopped omalizumab experienced exacerbations within one year, versus 19% of those who maintained therapy.44 Real-world data from the French national health database showed that only 24% of adults who discontinued omalizumab with stable asthma remained controlled at three years; in children, this proportion was 33%.45 Smaller observational cohorts have reported even higher relapse rates: in a Polish monocentric study of 14 patients treated for at least 36 months, 79% of those who stopped omalizumab experienced deterioration in asthma control and severe exacerbations, especially among those on high-dose OCS, while another study found loss of control in 55.7% of patients after discontinuation, with a mean time to relapse of 13 months.46,47
Data on dupilumab withdrawal in severe asthma are not yet available. However, in patients with CRSwNP, dose spacing after six months of treatment—extending the dosing interval to every four weeks—was reported to be feasible without loss of control, suggesting that similar strategies might eventually be explored in asthma, although this remains speculative at present.61
Rather than complete discontinuation, some studies have examined dose reduction or interval prolongation of anti–IL-5 biologics. The OPTIMAL trial, a randomized controlled study, evaluated an algorithm for tapering mepolizumab, benralizumab and reslizumab in patients with severe asthma who had achieved clinical control.49 The protocol involved progressively extending dosing intervals by 50% and then a further 50% (up to 125% of the standard interval), with the option of full discontinuation if well tolerated. Loss of control, defined by a ≥15% fall in FEV1 from baseline, blood eosinophils ≥0.3 × 109/L or an exacerbation requiring OCS, prompted shortening of the interval. Most patients (78%) in the titration arm tolerated interval extension, but there was a trend towards a higher exacerbation rate compared with standard dosing (32% vs 17%; p = 0.13), particularly towards the end of the study during attempted complete withdrawal. Patients without prior maintenance OCS use were more likely to successfully discontinue biologics. No permanent loss of lung function or serious adverse events related to tapering were observed, and declines in FEV1 during titration were reversible when dosing frequency was increased. Consistent with the higher exacerbation rate, a significant late rise in blood eosinophils was seen in the titration arm (p < 0.001).49
On the basis of current knowledge, general recommendations remain cautious. GINA guidelines for severe asthma suggest that biologic discontinuation should not be considered before at least 12 months of continuous therapy and only in patients with well-controlled asthma on moderate doses of ICS.1 Mohan et al have proposed criteria for withdrawal that include clinical remission, absence of significant type 2 inflammation, no OCS use and a low prior exacerbation burden.79 Ideal candidates may be the so-called “super-responders”, characterized by absence of symptoms and exacerbations, stable lung function and low inflammatory biomarkers; for these patients, an algorithm combining gradual tapering and potential discontinuation based on clinical outcomes and Th2-related markers has been proposed, although it has not yet been validated across different severe asthma populations.79 Yilmaz et al have suggested a minimum biologic treatment duration of five years before considering withdrawal, in order to reduce the risk of early relapse.80
Overall, strategies involving gradual dose reduction or interval prolongation appear more promising and better tolerated than abrupt discontinuation, but even these approaches carry a non-negligible risk of loss of control in a subset of patients.81 Decisions about tapering or stopping biologics should therefore be individualized, integrating clinical course, biomarker trends and patient-specific risk factors.82 In summary, while biologics clearly have the potential to induce on-treatment remission in severe asthma, the evidence base for complete withdrawal is still limited and points to a substantial risk of disease worsening in many cases. Dose reduction and dosing interval extension are emerging as plausible intermediate strategies, but long-term prospective studies are needed to define durable off-treatment remission, identify robust predictors of safe withdrawal and develop internationally accepted, evidence-based tapering algorithms.
A Pragmatic Approach to De-Escalation in Severe Eosinophilic Asthma Remission
Given the current uncertainties, de-escalation in patients with severe asthma who have achieved clinical remission should be approached in a structured and cautious way. As a first step, the diagnosis of severe asthma should be reconfirmed and potential confounders—such as poor inhaler technique, uncontrolled comorbidities or ongoing exposure to triggers—should be revisited. Remission itself should be defined using explicit criteria, including absence of exacerbations, minimal or no symptoms, stable or improved lung function and no need for maintenance OCS over a predefined period, typically at least 12 months.83 Only once this stability has been documented, should step-down be considered. In practical terms, most experts advocate a hierarchical strategy. Long-term OCS, when present, should be prioritized for reduction and discontinuation, given their well-known systemic toxicity. Once OCS have been safely withdrawn and stability maintained, attention can shift to ICS de-escalation.55 This may involve gradual dose reductions at intervals of several months, with careful monitoring of symptoms, lung function and biomarkers such as blood eosinophils and, where available, FeNO. Relatively small downward steps are preferable to abrupt dose halving or discontinuation, and each step should be consolidated before further reductions are attempted. Only after successful OCS and ICS tapering should modification of biologic therapy be contemplated.84 Initial strategies may focus on extending dosing intervals rather than stopping treatment outright, particularly with agents for which pharmacokinetic and pharmacodynamic profiles support such an approach. A stepwise sequence of de-escalation, together with suggested monitoring and failure criteria, is summarized in Figure 2.
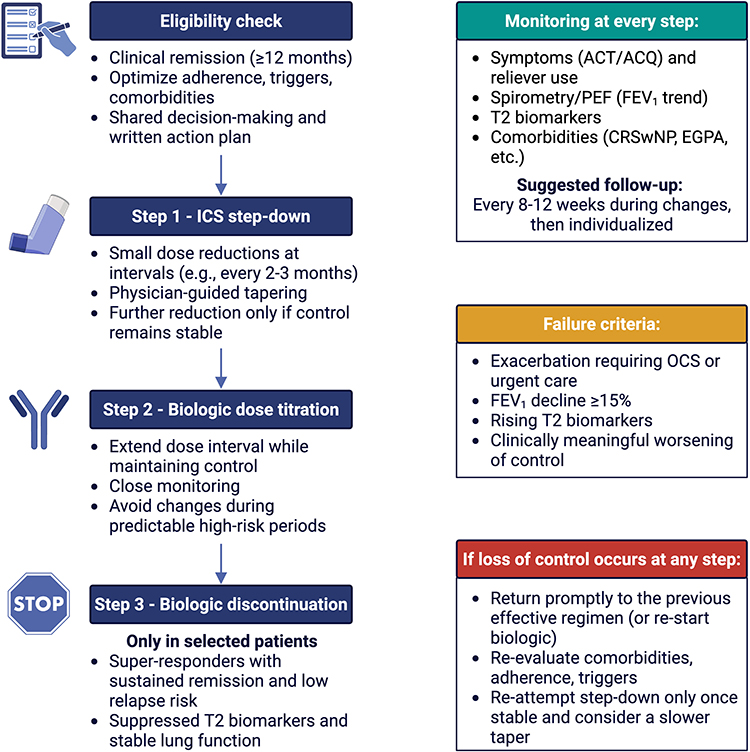 |
Figure 2 Stepwise de-escalation following clinical remission in severe eosinophilic asthma: a proposed pragmatic algorithm. |
Throughout this process, predefined criteria for “failure” of de-escalation—such as a clinically meaningful FEV1 decline, a rise in biomarkers above agreed thresholds, or the occurrence of exacerbations—should be agreed in advance and communicated clearly to the patient. Meeting these criteria should trigger prompt re-escalation to the previous effective regimen, with the understanding that step-down is inherently reversible. In particular, not all exacerbations reflect failure of biologic therapy: episodes driven predominantly by viral/bacterial infection, non-adherence, comorbidity flares (eg., rhinosinusitis) or non–type 2 mechanisms may occur despite adequate control of T2 inflammation. Accordingly, any deterioration during tapering should trigger a structured reassessment (including trigger review, exacerbation phenotyping and, when feasible, biomarker measurement) before concluding that the biologic is ineffective.
Shared decision-making is essential at every stage. Patients should be informed about the potential benefits of reducing treatment burden and side effects, as well as the possibility of relapse and the need for closer follow-up during tapering. Involving patients in setting goals, choosing the pace of de-escalation and recognizing early warning signs can improve adherence to the plan and reduce anxiety around treatment changes. Whenever possible, structured follow-up schedules, use of validated questionnaires and, in some cases, home monitoring tools (such as peak flow and/or app-based symptom diaries) can support a more responsive and individualized implementation of de-escalation strategies in clinical practice.
Conclusions
The emergence of biologic therapies has made clinical remission a realistic goal for a subset of patients with severe asthma, significantly changing expectations for long-term disease control. At the same time, remission on-treatment raises new and complex questions about how intensively patients need to be treated once stability is achieved, and whether maintenance OCS, high-dose ICS and biologics can be safely reduced or even discontinued in selected individuals.
Current evidence suggests that de-escalation is feasible for many patients, particularly with respect to OCS and, in a substantial proportion, ICS. However, the evidence supporting biologic dose reduction, interval extension, or withdrawal is still limited, heterogeneous, and largely derived from selected populations and relatively small prospective datasets. Strategies involving gradual dose reduction or interval extension of biologics appear promising but are associated with a non-negligible risk of relapse, especially when complete withdrawal is attempted. Clinical history, lung function and biomarkers of type 2 inflammation, together with patient-reported outcomes, can help to guide decision-making, although no single parameter has yet emerged as a definitive predictor of success.
In this context, a cautious, stepwise and clinician-led approach, grounded on shared decision-making and supported by close monitoring, seems the most appropriate strategy. Until stronger evidence becomes available, treatment de-escalation in severe asthma remission should be viewed as an individualized therapeutic trial rather than a routine practice, with clear criteria for success and for prompt re-escalation. Future research aimed at standardizing definitions, validating predictors and testing structured tapering algorithms will be crucial to translate the concept of remission from an aspirational goal into a practical, safely achievable outcome for a larger proportion of patients with severe asthma.
Abbreviations
ACQ, Asthma Control Questionnaire; ACT, Asthma Control Test; BMI, body mass index; COMET, Cessation Versus Continuation of Long-term Mepolizumab Treatment; CRSwNP, chronic rhinosinusitis with nasal polyps; DMAADs, Disease Modifying Anti-Asthmatic Drugs; EPX, eosinophil peroxidase; FEV1, forced expiratory volume in one second; FeNO, fractional exhaled nitric oxide; GINA, Global Initiative for Asthma; ICS, inhaled corticosteroids; IL, interleukin; LABA, long-acting β2-agonist; LAMA, long-acting muscarinic antagonist; MCID, minimal clinically important difference; OCS, oral corticosteroids; PROMs, patient-reported outcome measures; SANI, Severe Asthma Network in Italy; T2, type 2 (eosinophilic) inflammation; TSLP, thymic stromal lymphopoietin; XPORT, Xolair Persistence Of Response Trial.
Data Sharing Statement
Data sharing not applicable to this article as no datasets were generated or analyzed during the current study.
Author Contributions
CL – Conceptualization, Writing–original draft, Visualization, Writing–review and editing; GM – Conceptualization, Visualization, Writing–review and editing; EC – Conceptualization, Visualization, Writing–review and editing; GLP – Conceptualization, Visualization, Writing–review and editing; NL – Conceptualization, Visualization, Writing–review and editing; CC – Conceptualization, Visualization, Writing–review and editing; RP – Conceptualization, Visualization, Writing–review and editing; AM – Conceptualization, Visualization, Writing–review and editing; AV – Supervision, Visualization, Writing–review and editing; GP – Supervision, Visualization, Writing–review and editing; CP – Conceptualization, Visualization, Supervision, Writing–review and editing. All authors gave final approval of the version to be published; approved on the journal to which this article was submitted; and agree to be accountable to the content of this article.
Funding
This research received no external funding.
Disclosure
Prof. Dr. Claudia Crimi reports personal fees from GSK, Astra Zeneca, Sanofi, F&P, Philips, Airliquid, outside the submitted work. All authors declare that the research was conducted in the absence of any commercial or financial relationships that could be considered potential conflicts of interest.
References
1. Ginasthma. Global Strategy for Asthma Management and Prevention. Available from: www.ginasthma.org.
2. Porsbjerg C, Melén E, Lehtimäki L, Shaw D. Asthma. Lancet. 2023;401(10379):858–16. doi:10.1016/S0140-6736(22)02125-0
3. Moore WC, Bleecker ER, Curran-Everett D, et al. Characterization of the severe asthma phenotype by the National Heart, Lung, and Blood Institute’s Severe Asthma Research Program. J Allergy Clin Immunol. 2007;119(2):405–413. doi:10.1016/j.jaci.2006.11.639
4. Thomas D, McDonald VM, Pavord ID, Gibson PG. Asthma remission: what is it and how can it be achieved? Eur Respir J. 2022;60(5):2102583. doi:10.1183/13993003.02583-2021
5. Krings JG, Beasley R. The Role of ICS-Containing Rescue Therapy Versus SABA Alone in Asthma Management Today. J Allergy Clin Immunol Pract. 2024;12(4):870–879. doi:10.1016/j.jaip.2024.01.011
6. Von Bülow A, Hansen S, Sandin P, et al. Use of High-Dose Inhaled Corticosteroids and Risk of Corticosteroid-Related Adverse Events in Asthma Findings From the NORDSTAR Cohort. J Allergy Clin Immunol Pract. 2025;13(7):1609–1619.e5. doi:10.1016/j.jaip.2025.01.023
7. Lommatzsch M. Remission in asthma. Curr Opin Pulm Med. 2024;30(3):325–329. doi:10.1097/MCP.0000000000001068
8. Pastore D, Lupia C, D’Amato M, et al. Emerging biological treatments for asthma. Expert Opin Emerg Drugs. 2025;30(2):87–97. doi:10.1080/14728214.2025.2460529
9. D’Amato M, Pastore D, Lupia C, et al. Biologic Therapy in Severe Asthma: a Phenotype-Driven and Targeted Approach. J Clin Med. 2025;14(13):4749. doi:10.3390/jcm14134749
10. Farinha I, Heaney LG. Barriers to clinical remission in severe asthma. Respir Res. 2024;25(1):178. doi:10.1186/s12931-024-02812-3
11. Perez-de-Llano L, Scelo G, Tran TN, et al. Exploring Definitions and Predictors of Severe Asthma Clinical Remission after Biologic Treatment in Adults. Am J Respir Crit Care Med. 2024;210(7):869–880. doi:10.1164/rccm.202311-2192OC
12. Hansen S, Baastrup Søndergaard M, von Bülow A, et al. Clinical Response and Remission in Patients With Severe Asthma Treated With Biologic Therapies. Chest. 2024;165(2):253–266. doi:10.1016/j.chest.2023.10.046
13. Pelaia C, Zannoni E, Paoletti G, Marzio V, Heffler E, Carrón-Herrero A. Clinical remission in severe asthma: lights and shadows on an ambitious goal. Curr Opin Allergy Clin Immunol. 2024;24(4):230–236. doi:10.1097/ACI.0000000000000991
14. Chung KF, Dixey P, Abubakar-Waziri H, et al. Characteristics, phenotypes, mechanisms and management of severe asthma. Chin Med J. 2022;135(10):1141–1155. doi:10.1097/CM9.0000000000001990
15. Manti S, Magri P, De Silvestri A, et al. Epidemiology of severe asthma in children: a systematic review and meta-analysis. Eur Respir Rev. 2024;33(174):240095. doi:10.1183/16000617.0095-2024
16. Busse WW. Consequences of severe asthma exacerbations. Curr Opin Allergy Clin Immunol. 2023;23(1):44–50. doi:10.1097/ACI.0000000000000870
17. Seshadri N, Faig W, Young LR, Hill DA. Risk factors for hospitalization in subspecialty patients with severe persistent asthma. Respir Med. 2024;235:107867. doi:10.1016/j.rmed.2024.107867
18. Castillo JR, Peters SP, Busse WW. Asthma Exacerbations: pathogenesis, Prevention, and Treatment. J Allergy Clin Immunol Pract. 2017;5(4):918–927. doi:10.1016/j.jaip.2017.05.001
19. Ricciardolo FL, Bertolini F, Carriero V, Sprio AE. Asthma phenotypes and endotypes. Minerva Med. 2021;112(5):547–563. doi:10.23736/S0026-4806.21.07498-X
20. Maison N, Omony J, Illi S, et al. T2-high asthma phenotypes across lifespan. Eur Respir J. 2022;60(3):2102288. doi:10.1183/13993003.02288-2021
21. Peri F, Amaddeo A, Badina L, Maschio M, Barbi E, Ghirardo S. T2-Low Asthma: a Discussed but Still Orphan Disease. Biomedicines. 2023;11(4):1226. doi:10.3390/biomedicines11041226
22. Nathan RA, Sorkness CA, Kosinski M, et al. Development of the asthma control test: a survey for assessing asthma control. J Allergy Clin Immunol. 2004;113(1):59–65. doi:10.1016/j.jaci.2003.09.008
23. Juniper EF, O’Byrne PM, Guyatt GH, Ferrie PJ, King DR. Development and validation of a questionnaire to measure asthma control. Eur Respir J. 1999;14(4):902–907. doi:10.1034/j.1399-3003.1999.14d29.x
24. Louis R, Satia I, Ojanguren I, et al. European Respiratory Society guidelines for the diagnosis of asthma in adults. Eur Respir J. 2022;60(3):2101585. doi:10.1183/13993003.01585-2021
25. Miller MR, Hankinson J, Brusasco V, et al. Standardisation of spirometry. Eur Respir J. 2005;26(2):319–338. doi:10.1183/09031936.05.00034805
26. Cazzola M, Matera MG, Rogliani P, Calzetta L, Ora J. Step-up and step-down approaches in the treatment of asthma. Expert Rev Respir Med. 2021;15(9):1159–1168. doi:10.1080/17476348.2021.1935245
27. Canonica GW, Blasi F, Carpagnano GE, et al. Severe Asthma Network Italy Definition of Clinical Remission in Severe Asthma: a Delphi Consensus. J Allergy Clin Immunol Pract. 2023;11(12):3629–3637. doi:10.1016/j.jaip.2023.07.041
28. Canonica GW, Bagnasco D, Bondi B, et al. SANI clinical remission definition: a useful tool in severe asthma management. J Asthma. 2024;61(12):1593–1600. doi:10.1080/02770903.2024.2376919
29. UK Severe Asthma Registry. McDowell PJ, McDowell R, et al. Clinical remission with biologic therapies in severe asthma: a matter of definition. Eur Respir J. 2024;63(6):2400160. doi:10.1183/13993003.00160-2024.
30. Menzies-Gow A, Bafadhel M, Busse WW, et al. An expert consensus framework for asthma remission as a treatment goal. J Allergy Clin Immunol. 2020;145(3):757–765. doi:10.1016/j.jaci.2019.12.006
31. Tajiri T, Suzuki M, Nishiyama H, et al. Clinical and complete remission in patients with severe asthma with 24-month dupilumab treatment. Respir Investig. 2025;63(5):711–717. doi:10.1016/j.resinv.2025.06.002
32. Menzies-Gow A, Szefler SJ, Busse WW, et al. Clinical remission in severe asthma: a new goal? J Allergy Clin Immunol. 2020;145(6):1671–1678. doi:10.1016/j.jaci.2020.03.012
33. Busse WW, Chupp G, Corbridge T, Stach-Klysh A, Oppenheimer J. Targeting Asthma Remission as the Next Therapeutic Step Toward Improving Disease Control. J Allergy Clin Immunol Pract. 2024;12(4):894–903. doi:10.1016/j.jaip.2024.01.044
34. Gyawali B, Georas SN, Khurana S. Biologics in severe asthma: a state-of-the-art review. Eur Respir Rev. 2025;34(175):240088. doi:10.1183/16000617.0088-2024
35. Seluk L, Davis AE, Rhoads S, Wechsler ME. Novel asthma treatments: advancing beyond approved novel step-up therapies for asthma. Ann Allergy Asthma Immunol. 2025;134(1):9–18. doi:10.1016/j.anai.2024.09.016
36. Loureiro CC, Amaral L, Ferreira JA, et al. Omalizumab for Severe Asthma: beyond Allergic Asthma. Biomed Res Int. 2018;2018:3254094. doi:10.1155/2018/3254094
37. Humbert M, Bousquet J, Bachert C, et al. IgE-Mediated Multimorbidities in Allergic Asthma and the Potential for Omalizumab Therapy. J Allergy Clin Immunol Pract. 2019;7(5):1418–1429. doi:10.1016/j.jaip.2019.02.030
38. Ortega HG, Liu MC, Pavord ID, et al. Mepolizumab treatment in patients with severe eosinophilic asthma. N Engl J Med. 2014;371(13):1198–1207. doi:10.1056/NEJMoa1403290
39. Bleecker ER, FitzGerald JM, Chanez P, et al. Efficacy and safety of benralizumab for patients with severe asthma uncontrolled with high-dosage inhaled corticosteroids and long-acting β2-agonists (SIROCCO): a randomised, multicentre, placebo-controlled phase 3 trial. Lancet. 2016;388(10056):2115–2127. doi:10.1016/S0140-6736(16)31324-1
40. Castro M, Corren J, Pavord ID, et al. Dupilumab Efficacy and Safety in Moderate-to-Severe Uncontrolled Asthma. N Engl J Med. 2018;378(26):2486–2496. doi:10.1056/NEJMoa1804092
41. Menzies-Gow A, Corren J, Bourdin A, et al. Tezepelumab in Adults and Adolescents with Severe, Uncontrolled Asthma. N Engl J Med. 2021;384(19):1800–1809. doi:10.1056/NEJMoa2034975
42. Agache I, Beltran J, Akdis C, et al. Efficacy and safety of treatment with biologicals (benralizumab, dupilumab, mepolizumab, omalizumab and reslizumab) for severe eosinophilic asthma. A systematic review for the EAACI Guidelines - recommendations on the use of biologicals in severe asthma. Allergy. 2020;75(5):1023–1042. doi:10.1111/all.14221
43. Couillard S, Lachapelle P. De-Escalation of Severe Asthma Therapy: do We Wean the Biologic or the Inhaler First? Can Resp Today. 2025;1(1):31–38. doi:10.58931/cret.2025.116
44. Ledford D, Busse W, Trzaskoma B, et al. A randomized, multicenter study evaluating Xolair® (omalizumab) persistence of response after long-term therapy (XPORT). J Allergy Clin Immunol. 2017;140(1):162–169.e2. doi:10.1016/j.jaci.2016.08.054
45. Humbert M, Bourdin A, Taillé C, et al. Real-life omalizumab exposure and discontinuation in a large nationwide population-based study of paediatric and adult asthma patients. Eur Respir J. 2022;60(5):2103130. doi:10.1183/13993003.03130-2021
46. Kupryś-Lipińska I, Majak P, Molinska J, Kuna P. Effectiveness of the Polish program for the treatment of severe allergic asthma with omalizumab: a single-center experience. BMC Pulm Med. 2016;16(1):61. doi:10.1186/s12890-016-0224-2
47. Molimard M, Mala L, Bourdeix I, Le Gros V. Observational study in severe asthmatic patients after discontinuation of omalizumab for good asthma control. Respir Med. 2014;108(4):571–576. doi:10.1016/j.rmed.2014.02.003
48. Moore WC, Kornmann O, Humbert M, et al. Stopping versus continuing long-term mepolizumab treatment in severe eosinophilic asthma (COMET study). Eur Respir J. 2022;59(1):2100396. doi:10.1183/13993003.00396-2021
49. Soendergaard MB, Bjerrum AS, Rasmussen LM, et al. Titration of anti-IL-5 biologics in severe asthma: an open-label randomised controlled trial (the OPTIMAL study). Eur Respir J. 2024;64(2):2400404. doi:10.1183/13993003.00404-2024
50. Fyles F, Nuttall A, Joplin H, Burhan H. Long-Term Real-World Outcomes of Mepolizumab and Benralizumab Among Biologic-Naive Patients With Severe Eosinophilic Asthma: experience of 3 Years’ Therapy. J Allergy Clin Immunol Pract. 2023;11(9):2715–2723. doi:10.1016/j.jaip.2023.05.025
51. Fyles F, Burton R, Nuttall A, Joplin H, Watkins L, Burhan H. Clinical remission among severe asthmatics on monoclonal antibody therapy: real-world outcomes at 2 years. ERJ Open Res. 2024;10(6):00261–2024. doi:10.1183/23120541.00261-2024
52. Deeks ED, Brusselle G. Reslizumab in Eosinophilic Asthma: a Review. Drugs. 2017;77(7):777–784. doi:10.1007/s40265-017-0740-2
53. Moermans C, Brion C, Bock G, et al. Sputum Type 2 Markers Could Predict Remission in Severe Asthma Treated With Anti-IL-5. Chest. 2023;163(6):1368–1379. doi:10.1016/j.chest.2023.01.037
54. Soendergaard MB, Hansen S, Håkansson KEJ, et al. Early Reduction of FeNO on Anti-IL5 Biologics Is Associated With Clinical Remission of Severe Asthma. Allergy. 2025;80(4):986–995. doi:10.1111/all.16425
55. Menzies-Gow A, Gurnell M, Heaney LG, et al. Oral corticosteroid elimination via a personalised reduction algorithm in adults with severe, eosinophilic asthma treated with benralizumab (PONENTE): a multicentre, open-label, single-arm study. Lancet Respir Med. 2022;10(1):47–58. doi:10.1016/S2213-2600(21)00352-0
56. Jackson DJ, Heaney LG, Humbert M, et al. Reduction of daily maintenance inhaled corticosteroids in patients with severe eosinophilic asthma treated with benralizumab (SHAMAL): a randomised, multicentre, open-label, Phase 4 study. Lancet. 2024;403(10423):271–281. doi:10.1016/S0140-6736(23)02284-5
57. Pini L, Bagnasco D, Beghè B, et al. Unlocking the Long-Term Effectiveness of Benralizumab in Severe Eosinophilic Asthma: a Three-Year Real-Life Study. J Clin Med. 2024;13(10):3013. doi:10.3390/jcm13103013
58. Yeşilkaya S, Aksu K, Tuğçe Vural Solak G, et al. Variables predicting clinical remission among adults with severe asthma treated with biologic agents. Eur Ann Allergy Clin Immunol. 2024;56(5):219–226. doi:10.23822/EurAnnACI.1764-1489.318
59. Martinez-Moragon E, Chiner E, Suliana Mogrovejo A, et al. Real-world clinical remission of severe asthma with benralizumab in Spanish adults with severe asthma. J Asthma. 2024;61(10):1190–1204. doi:10.1080/02770903.2024.2332351
60. Quarato CMI, Tondo P, Lacedonia D, et al. Long-Term Clinical Remission on Benralizumab Treatment in Severe Eosinophilic Asthma: a Four-Year Real-Life Study. J Clin Med. 2025;14(6):2075. doi:10.3390/jcm14062075
61. Appel HM, Lochbaum R, Hoffmann TK, Hahn J. Chronische Rhinosinusitis mit nasalen Polypen – verlängerung der Dupilumab-Therapieintervalle [Chronic rhinosinusitis with nasal polyps-extension of dupilumab treatment intervals]. HNO. 2024;72(7):499–503. doi:10.1007/s00106-024-01487-y
62. Oishi K, Hamada K, Murata Y, et al. A Real-World Study of Achievement Rate and Predictive Factors of Clinical and Deep Remission to Biologics in Patients with Severe Asthma. J Clin Med. 2023;12(8):2900. doi:10.3390/jcm12082900
63. Damiański P, Białas AJ, Kołacińska-Flont M, et al. Pathway to Remission in Severe Asthma: clinical Effectiveness and Key Predictors of Success with Benralizumab Therapy: a Real-Life Study. Biomedicines. 2025;13(4):887. doi:10.3390/biomedicines13040887
64. Menzies-Gow A, Wechsler ME, Brightling CE, et al. Long-term safety and efficacy of tezepelumab in people with severe, uncontrolled asthma (DESTINATION): a randomised, placebo-controlled extension study. Lancet Respir Med. 2023;11(5):425–438. doi:10.1016/S2213-2600(22)00492-1
65. Brightling CE, Caminati M, Llanos JP, et al. Biomarkers and clinical outcomes after tezepelumab cessation: extended follow-up from the 2-year DESTINATION study. Ann Allergy Asthma Immunol. 2024;133(3):310–317.e4. doi:10.1016/j.anai.2024.04.031
66. Jackson DJ, Wechsler ME, et al. Twice-Yearly Depemokimab in Severe Asthma with an Eosinophilic Phenotype. N Engl J Med. 2024;391(24):2337–2349. doi:10.1056/NEJMoa2406673
67. Menzies-Gow A, Hoyte FL, Price DB, et al. Clinical Remission in Severe Asthma: a Pooled Post Hoc Analysis of the Patient Journey with Benralizumab. Adv Ther. 2022;39(5):2065–2084. doi:10.1007/s12325-022-02098-1
68. Rattu A, Dixey P, Charles D, et al. Predictors of Response to Biologics for Severe Asthma: a Systematic Review and Meta-Analysis. Allergy. 2025. doi:10.1111/all.70031
69. Heffler E, Carpagnano GE, Favero E, et al. Fractional Exhaled Nitric Oxide (FENO) in the management of asthma: a position paper of the Italian Respiratory Society (SIP/IRS) and Italian Society of Allergy, Asthma and Clinical Immunology (SIAAIC). Multidiscip Respir Med. 2020;15(1):36. doi:10.4081/mrm.2020.36
70. Al Ghobain MO, Alsubaie AS, Aljumah WA, et al. The Correlation Between Fractional Exhaled Nitric Oxide (FeNO), Blood Eosinophil Count, Immunoglobulin E Levels, and Spirometric Values in Patients With Asthma. Cureus. 2023;15(2):e35289. doi:10.7759/cureus.35289
71. Hoshino Y, Soma T, Uchida Y, Shiko Y, Nakagome K, Nagata M. Treatment Resistance in Severe Asthma Patients With a Combination of High Fraction of Exhaled Nitric Oxide and Low Blood Eosinophil Counts. Front Pharmacol. 2022;13:836635. doi:10.3389/fphar.2022.836635
72. Principe S, Jarjour NN. Pro: clinical remission in asthma - implications for asthma management. Eur Respir Rev. 2025;34(176):240181. doi:10.1183/16000617.0181-2024
73. Mailhot-Larouche S, Celis-Preciado C, Heaney LG, Couillard S. Identifying super-responders: a review of the road to asthma remission. Ann Allergy Asthma Immunol. 2025;134(1):31–45. doi:10.1016/j.anai.2024.09.023
74. Moermans C, Decerf N, Javaux N, et al. High local type-2 inflammation is linked to response in severe asthma treated with anti-Interleukin-5 receptor. Respir Med. 2025;243:108151. doi:10.1016/j.rmed.2025.108151
75. Upham JW, Le Lievre C, Jackson DJ, et al. Defining a Severe Asthma Super-Responder: findings from a Delphi Process. J Allergy Clin Immunol Pract. 2021;9(11):3997–4004. doi:10.1016/j.jaip.2021.06.041
76. Harrison OK, Marlow L, Finnegan SL, Ainsworth B, Pattinson KTS. Dissociating breathlessness symptoms from mood in asthma. Biol Psychol. 2021;165:108193. doi:10.1016/j.biopsycho.2021.108193
77. Dahl R. Systemic side effects of inhaled corticosteroids in patients with asthma. Respir Med. 2006;100(8):1307–1317. doi:10.1016/j.rmed.2005.11.020
78. D’Ancona G, Kavanagh J, Roxas C, et al. Adherence to corticosteroids and clinical outcomes in mepolizumab therapy for severe asthma. Eur Respir J. 2020;55(5):1902259. doi:10.1183/13993003.02259-2019
79. Mohan A, Qiu AY, Lugogo N. Long-term safety, durability of response, cessation and switching of biologics. Curr Opin Pulm Med. 2024;30(3):303–312. doi:10.1097/MCP.0000000000001067
80. Yılmaz İ, Paçacı Çetin G, Arslan B, et al. Biological therapy management from the initial selection of biologics to switching between biologics in severe asthma. Ağır astımda biyolojik ajanların ilk seçiminden biyolojikler arasında geçişe kadar biyolojik tedavi yönetimi. Tuberk Toraks. 2023;71(1):75–93. doi:10.5578/tt.20239910
81. Ramirez-Villamizar J, Ibarra-Enríquez CD, Galindo-Sánchez JS, Serrano-Reyes C, Fernández-Trujillo L. Discontinuation of biologic therapy in severe asthma: evidence and strategies for safe withdrawal: a scoping review. World Allergy Organ J. 2025;18(9):101107. doi:10.1016/j.waojou.2025.101107
82. Hamada K, Oishi K, Murata Y, Hirano T, Matsunaga K. Feasibility of Discontinuing Biologics in Severe Asthma: an Algorithmic Approach. J Asthma Allergy. 2021;14:1463–1471. doi:10.2147/JAA.S340684
83. Merrell E, Khurana S. Recent evidence for stepping down severe asthma therapies. Curr Opin Pulm Med. 2025;31(3):294–301. doi:10.1097/MCP.0000000000001156
84. Bleecker ER, Al-Ahmad M, Bjermer L, et al. Systemic corticosteroids in asthma: a call to action from World Allergy Organization and Respiratory Effectiveness Group. World Allergy Organ J. 2022;15(12):100726. doi:10.1016/j.waojou.2022.100726
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Long-Term Efficacy and Clinical Remission After Benralizumab Treatment in Patients with Severe Eosinophilic Asthma: A Retrospective Study
Numata T, Araya J, Okuda K, Miyagawa H, Minagawa S, Ishikawa T, Hara H, Kuwano K
Journal of Asthma and Allergy 2022, 15:1731-1741
Published Date: 29 November 2022