Back to Journals » Clinical Pharmacology: Advances and Applications » Volume 17
Predictive Analysis of Non-Cardiac Drug-Induced QTc Interval Prolongation: A Cross-Sectional Study
Authors Albekairy NA, Aldawsari RA, Alanazi S, Almutairi N, AlSayari N, Abu Al-Burak S, Bawazeer MA, Alfehaid L ![]() , Shawaqfeh MS
, Shawaqfeh MS
Received 30 November 2024
Accepted for publication 23 April 2025
Published 13 May 2025 Volume 2025:17 Pages 85—96
DOI https://doi.org/10.2147/CPAA.S509476
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Khaled Deeb
Nataleen A Albekairy,1,2,* Reema Abdullah Aldawsari,1,2,* Sarah Alanazi,1,2,* Nora Almutairi,1,2,* Nora AlSayari,1,2,* Salem Abu Al-Burak,3 Mona Abubakr Bawazeer,1,2 Lama Alfehaid,2,4,5 Mohammad S Shawaqfeh2,4
1College of Medicine, King Saud bin Abdulaziz University for Health Sciences, Riyadh, Saudi Arabia; 2King Abdullah International Medical Research Center (KAIMRC), Ministry of National Guard Health Affairs (MNGHA), Riyadh, Saudi Arabi; 3Schulich School of Medicine and Dentistry, Western University, Ontario, Canada; 4Pharmacy Practice Department, College of Pharmacy, King Saud bin Abdulaziz University for Health Sciences, Riyadh, Saudi Arabia; 5Department of Pharmaceutical Care Services, King Abdulaziz Medical City, Ministry of National Guard-Health Affairs, Riyadh, Saudi Arabia
*These authors contributed equally to this work
Correspondence: Lama Alfehaid, College of Pharmacy, Clinical Pharmacy Practice; King Saud bin Abdulaziz University for Health Sciences – Riyadh KSA, Tel +966114299999; Ext. 95008, Email [email protected]
Purpose: This study aimed to assess the real-world impacts of non-cardiac drug-induced QTc interval prolongation and identify associated risk factors in acute care settings.
Patients and Methods: A cross-sectional study reviewed medical charts of 7,778 patients admitted to tertiary teaching hospitals from January 2016 to December 2022. Patients on CredibleMeds-listed QTc-prolonging non-cardiac drugs were identified, excluding those with congenital long QTc syndrome or on QTc-prolonging cardiac medications. Data collection involved reviewing medication charts and recording demographic and clinical data, including comorbidities and laboratory values. A logistic regression analysis was performed to address confounders, and known risk factors, calculating Odds Ratios (OR) and 95% confidence intervals (CI). Statistical analysis used SPSS Version 21.0, with p < 0.05 indicating significance.
Results: Out of 7,778 screened patients, 151 met the inclusion criteria. Among these, 75.5% demonstrated prolonged QTc values. The study identified 42 distinct medications associated with QT interval prolongation, categorized into six therapeutic groups. Proton pump inhibitors (PPIs) were the most common cause of non-cardiac drug-induced QTc interval prolongation, with esomeprazole representing 46.5% of the cases. Antimicrobial medications followed, with azithromycin at 9.6% and piperacillin-tazobactam at 6.1%. The multivariate analysis revealed that heart failure was significantly associated with QTc prolongation odd ratio (OR) 4.98 with 95% confidence interval CI [1.58 to 17.35], while other factors such as age, BMI, and certain comorbidities did not show a statistically significant impact.
Conclusion: The findings highlight the significant risk associated with the in-hospital administration of QTc-prolonging non-cardiac medications, particularly among patients with heart failure. Future research should aim to include a larger patient population and employ comprehensive data collection methods across multiple centers to enhance the robustness and generalizability of the findings.
Keywords: QTc prolongation, drug-induced, torsade de pointes, arrhythmia, non-cardiac medications
Introduction
QT interval prolongation refers to an abnormal lengthening of the QT interval on an electrocardiogram (ECG), indicating a disruption in the ventricular repolarization process of the heart. This condition is particularly concerning as it is associated with severe ventricular tachyarrhythmias, including torsades de pointes (TdP) and sudden cardiac death (SCD).1 According to current diagnostic standards, a corrected QT interval (QTc) exceeding 450 milliseconds (msec) is classified as prolonged for males, while for females, the threshold is established at over 470 msec. The risk of experiencing TdP and SCD increases significantly when the QTc exceeds 500 msec.2–5
Prolonged QTc can result from dysfunction in cardiac sodium or potassium channels, which may arise from either congenital genetic mutations or acquired external factors. Acquired QTc prolongation is more prevalent, often due to various pharmacological agents that influence cardiac ion channels. Notable examples include certain antiarrhythmic drugs, macrolide antibiotics, and various psychotropic medications.6 Additional contributing risk factors encompass cardiovascular diseases, thyroid disorders, electrolyte imbalances (such as hypokalemia or hyponatremia), and advanced age, particularly in individuals over 65 years.4,5
The unpredictable and potentially dangerous effects of drug-induced QTc interval prolongation have raised significant concerns regarding medication safety. Over the past two decades, this has prompted the withdrawal or restriction of certain drugs from the market. In response to these concerns,7,8 the Arizona Center for Education and Research on Therapeutics (AzCERT) has developed a standardized system for drug identification, categorizing medications based on their risk of inducing TdP and QT prolongation.9 Their platform, CredibleMeds®, classifies drugs into four categories: those known to induce TdP in clinical use, those with conditional risks that may induce TdP at high doses or under specific conditions (such as long QT syndrome, bradycardia, or hypokalemia), and those that prolong the QT interval without sufficient evidence of causing TdP.10
Despite the established associations between numerous drugs and QT prolongation, the actual risk remains ambiguous in many instances, highlighting the necessity for continuous monitoring during treatment to effectively manage these risks. A pharmacovigilance observational study has investigated drug-induced QT interval prolongation by analyzing data from the FDA Adverse Event Reporting System database. This study identified 1,579 drugs associated with 28,581 cases of QT prolongation, with a particular focus on the top 40 drugs involved. The findings indicated that QT prolongation was more prevalent among females and individuals aged 18–65, with antidepressants and antipsychotics being the primary drug classes implicated.11
Nevertheless, reports on drug-induced QTc prolongation in Saudi Arabia are limited. This study aimed to explore the actual effects of QTc-prolonging non-cardiac medications, as listed in CredibleMeds, and to identify the determinants and risk factors associated with QT interval prolongation among hospitalized patients receiving these medications.
Materials And Methods
Study Design and Settings
The study was a cross-sectional study that reviewed medical charts of patients admitted to King Abdulaziz Medical City (KAMC) at National Guard Health Affairs in Riyadh between January 2016 and December 2022. This tertiary care facility, which has a capacity exceeding 1500 beds, accommodates approximately 20,000 patient admissions annually.
Study Subjects
The study included adult patients (aged 18 years and older) admitted to general wards, including medical, psychiatric, and critical care units, who were receiving QTc-prolonging non-cardiac drugs recognized and listed by CredibleMeds (List of CredibleMeds® Medications That were Screened for) and had available ECG records. Patients with congenital Long QT Syndrome or those on antiarrhythmic medications known to prolong the QTc interval were excluded. Accurately assessing non-cardiac drug-induced QTc interval prolongation requires excluding patients with congenital Long QT Syndrome, structural heart disease, and those on antiarrhythmic drugs. This exclusion helps focus on acquired QTc prolongation and enhances study homogeneity, ensuring results specifically relate to the non-cardiac medications and facilitating a clearer interpretation of their effects on QTc interval prolongation.
Data Collection
The data collection involved a thorough review of medication charts for the enrolled patients. Demographic and clinical data were systematically gathered and recorded in an Excel spreadsheet. The data collection sheet encompassed demographic data such as gender, age, and BMI. Relevant comorbidities were recorded, including heart failure, myocardial infarction, sepsis, hypothyroidism, and bradycardia. Pertinent laboratory values such as potassium (K), magnesium (Mg), and calcium (Ca) levels were also collected. The CredibleMeds-listed QTc-prolonging non-cardiac drugs that were available in our hospital formulary available in (supplementary materials) were recorded and grouped into (antimicrobials, proton pump inhibitors (PPIs), anti-emetics, antidepressants, antipsychotics, and antihistamines); data on dosage, frequency, and number of medications were collected. QTc information and heart rate measurements were included as well.
QTc and Heart Rate Measurements
The QT interval was measured automatically, and the heart rate was determined by averaging the RR interval from an automated twelve-lead ECG. The QT interval was plotted against heart rate on the Isbister Nomogram to assess the risk of QTc prolongation. The Isbister nomogram was utilized for the graphical representation of the QT interval in relation to the heart rate. This method helped determine whether a specific QT interval is abnormal for a given heart rate, obviating the need for intricate calculations. When the plotted point exceeds a predefined risk threshold on the nomogram, it signifies an elevated risk for TdP arrhythmias.12 A QT interval was classified as prolonged if the QT-heart rate pair was ≥ 450 msec for men and ≥ 470 msec for women.
Data Analysis
Statistical analysis was performed using commercially available software (SPSS Version 21.0). The baseline characteristics of normally distributed data were described using mean and standard deviation (SD), while median and interquartile range [IQR] were used for skewed data. Categorical variables, including the baseline characteristics and the known QTc prolonging risk factors, were expressed using percentages and frequencies. A multiple logistic regression analysis was conducted to address potential confounders, including the known risk factors, and the Odds Ratio (OR) along with the 95% confidence interval (CI) was calculated.
Ethical Considerations
The study protocol received approval from the Institutional Review Board (IRB) of King Abdullah International Medical Research Center (KAIMRC) at the Ministry of National Guard Health Affairs (IRB Approval No.: IRB/2813/22). KIMARC IRB waived patient consent due to the retrospective nature of the study. There was no direct interaction with patients or collection of biological samples. Instead, the study relied on the review of existing patient records. Data was extracted only after obtaining ethical approval from the institutional review board of KAIMRC. Patients’ privacy and confidentiality were maintained throughout the entire data collection process, such that no patients’ identifiers or personal data were collected or disclosed. All collected data, whether hard or soft copies, were securely stored within the premises of KAMC hospital and were only accessed by the investigators involved in this project. All procedures adhered to KIMARC guidelines and regulations, ensuring compliance with the Declaration of Helsinki.
Results
Study Population
One hundred and fifty-one patients out of 7,778 screened patients met the predefined inclusion (Figure 1), illustrates the flowchart of the study. Among these, 90 (59.6%) were female, and 61 (40.4%) were male. The median age of the study population was 67, with IQR [77–44] years; age distribution indicates that 77 patients (59.9%) were over 65, while 74 (49.0%) were under 65 years old. In terms of body mass index (BMI), five patients (3.3%) were underweight, 23 (15.2%) had normal weight, 50 (33.1%) were overweight, and 57 (37.7%) were classified as obese. The most common comorbidity was heart failure with a reduced ejection fraction, affecting 85 patients (56.3%). Other notable conditions included sepsis in 31 patients (20.5%) and myocardial infarction in 24 patients (15.9%). The prevalence of other known risk factors associated with QTc prolongation within this cohort is illustrated in (Table 1).
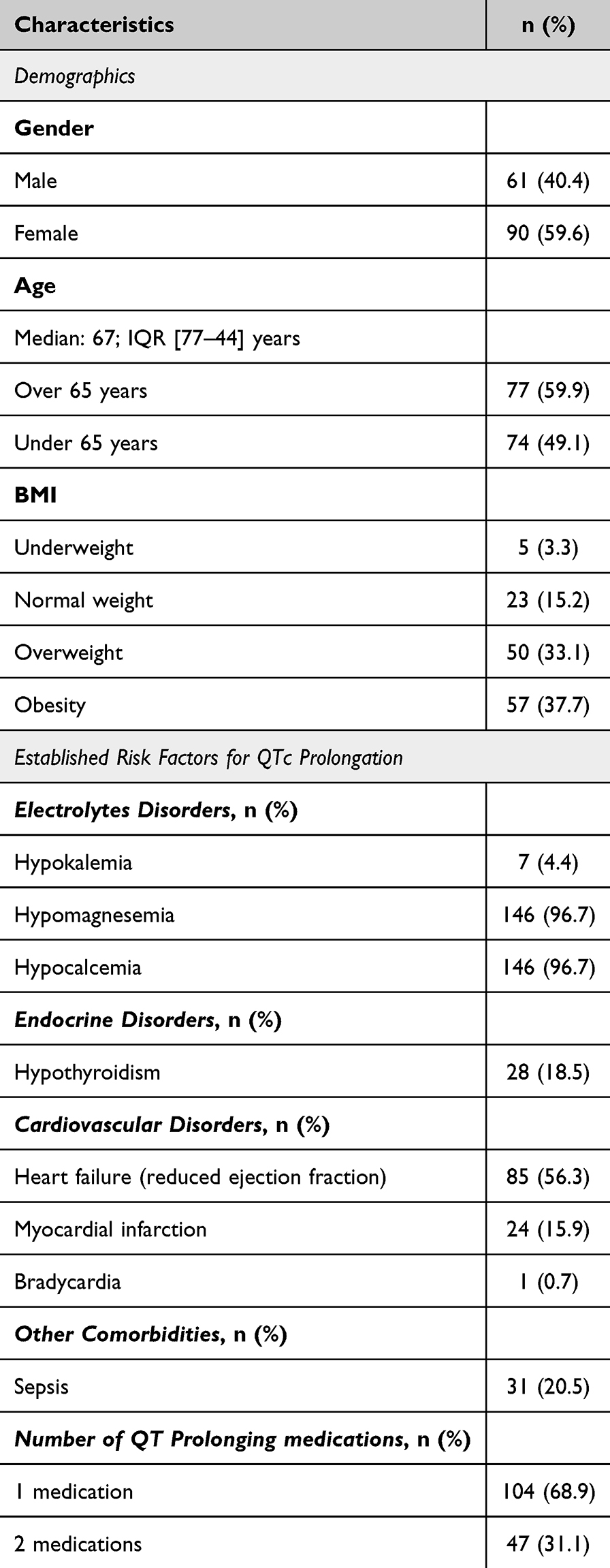 |
Table 1 Clinical Characteristics of Included Patients (n=151) |
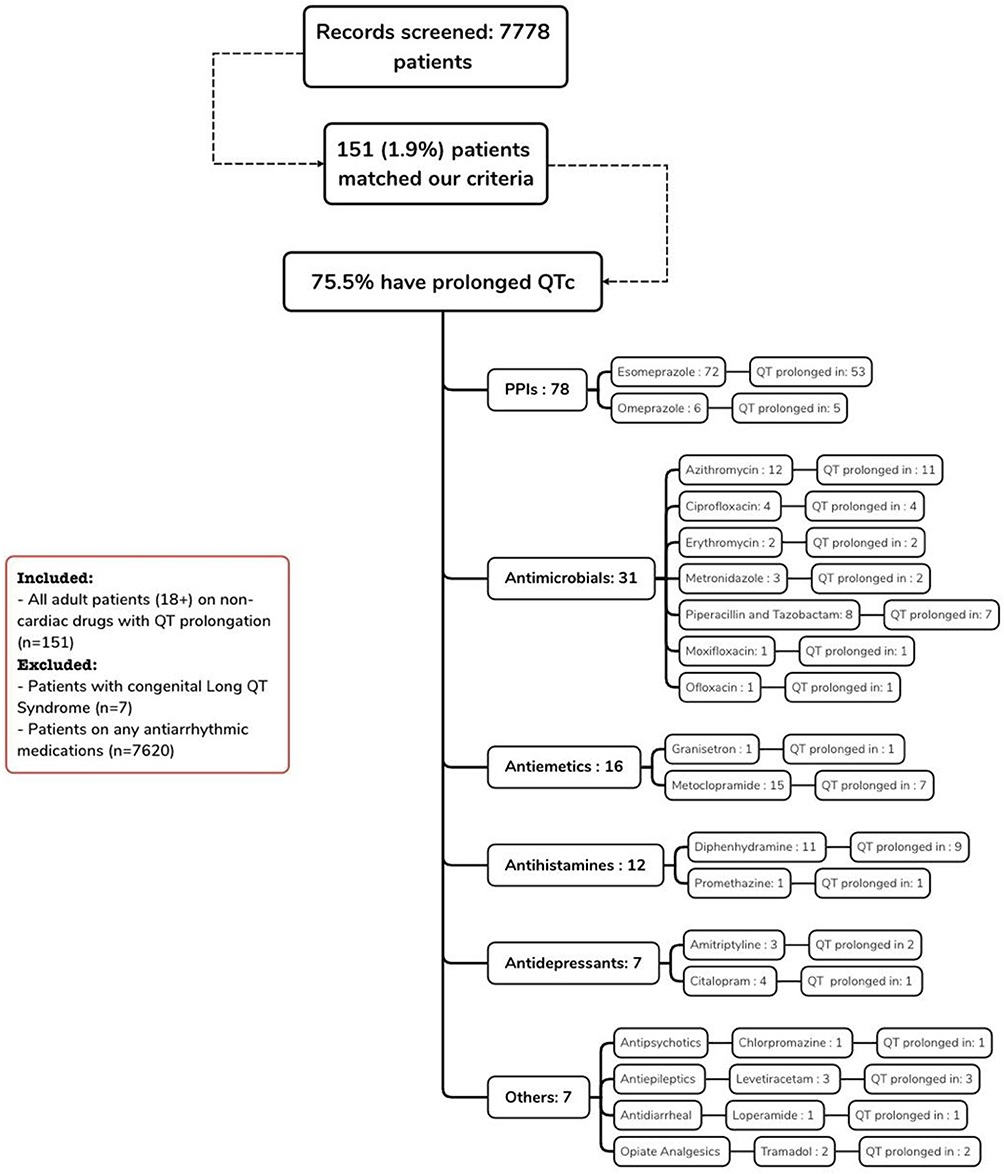 |
Figure 1 Flowchart of the Research Project. Abbreviations: PPIs, Proton Pump Inhibitors. |
Non-Cardiac Drug-Induced QTc Interval Prolongation
Upon assessing the included patients’ QTc intervals, 114 (75.5%) patients demonstrated prolonged QTc values. Further analysis revealed 42 different medications linked to QT interval prolongation, divided into six therapeutic categories. PPIs posed the greatest risk (51% of cases), particularly esomeprazole; among the patients, 53 were identified with QTc interval prolongation. This was followed by antimicrobial drugs, with 28 patients (24.6%) experiencing QTc interval prolongation, primarily those receiving azithromycin (39.3%) or piperacillin and tazobactam (25%). Lastly, antiemetics was a concern, mainly due to metoclopramide, which accounted for 43.8% (see Figure 1).
In the Isbister Nomogram, medication groups were plotted, with each medication color-coded (Figures 2–5), showing the relationship between the median QTc interval and heart rate for each respective group. Figure 2 reveals that the antimicrobials group, encompassing medications such as azithromycin, ciprofloxacin, erythromycin, moxifloxacin, piperacillin, and ofloxacin, was associated with most cases deemed at high risk of developing TdP. Figure 3 indicates the PPI users exhibited higher risk plots in most cases, with esomeprazole showing a particularly significant association. Figure 4 illustrates the antiemetic medications group, which displayed variable scatters around the risk line with no discernible trend. Notably, one case involving granisetron fell within the high-risk domain, while ondansetron and metoclopramide were situated around the risk line. Lastly, in Figure 5, the group plot of the remaining medications shows a discernible high-risk trend attributed particularly to the antihistamine diphenhydramine. Other medication categories, comprising antipsychotics, immunosuppressants, antidepressants, and anti-epileptics, demonstrated a tendency to cluster around the risk line.
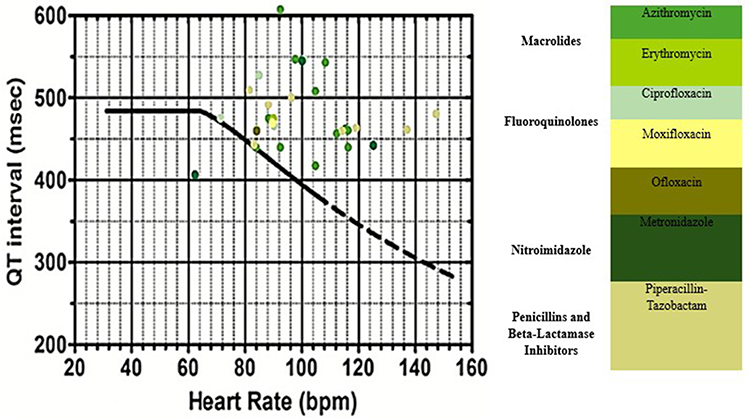 |
Figure 2 This nomogram shows patients who were on antimicrobials. It includes macrolides (Azithromycin and Erythromycin), fluoroquinolones (Ciprofloxacin, Moxifloxacin and Ofloxacin), nitroimidazole (Metronidazole), penicillins and beta-lactamase inhibitors (Piperacillin-tazobactam). Each QT interval is plotted against heart rate, and when the QT-heart rate pair is above the cut-off line, the QT is considered prolonged. |
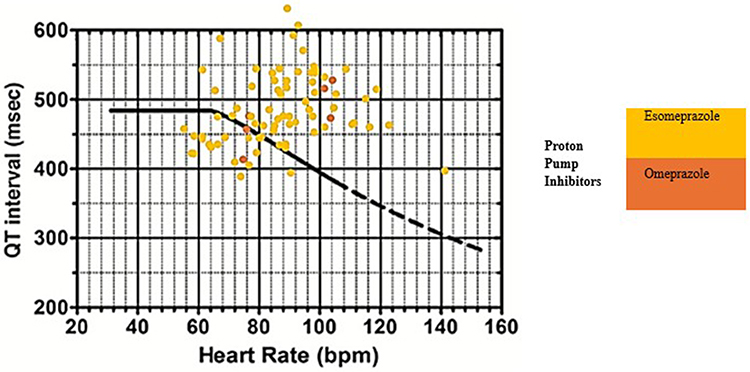 |
Figure 3 This nomogram shows patients who were on proton pump inhibitors. It includes Esomeprazole and Omeprazole. Each QT interval is plotted against the heart rate, and when the QT-heart rate pair is above the cut-off line, the QT is considered prolonged. |
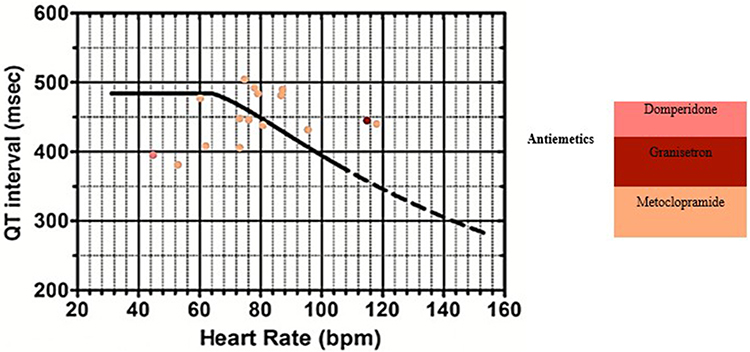 |
Figure 4 This nomogram shows patients who were on antiemetics. It includes Domperidone, Granisetron and Metoclopramide. Each QT interval is plotted against the heart rate, and when the QT-heart rate pair is above the cut-off line, the QT is considered prolonged. |
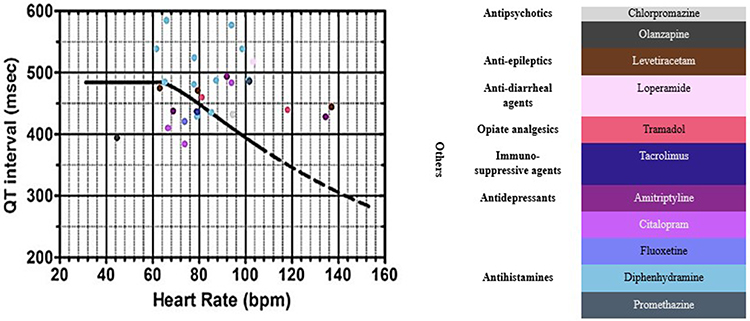 |
Figure 5 This nomogram shows patients who were broadly grouped as being on other medications. It includes antipsychotics (Chlorpromazine and Olanzapine), anti-epileptics (Levetiracetam), anti-diarrheal agents (Loperamide), opiate analgesics (Tramadol), immuno-suppressive agents (Tacrolimus), antidepressants (Amitriptyline, Citalopram, and Fluoxetine, and antihistamines (Diphenhydramine and Promethazine). Each QT interval is plotted against the heart rate, and when the QT-heart rate pair is above the cut-off line, the QT is considered prolonged. |
Impact of Known QTc Prolongation Risk Factors on Non-Cardiac Drug-Induced QTc Interval Prolongation
Findings from a multiple logistic regression analysis revealed that among those who experienced QTc interval prolongation, 54% were older than 65 years, with a non-statistically significant effect in the odds of QTc interval prolongation, OR 0.79; 95% CI [0.23 to 2.49]. Females comprised 47% of the identified patients, presenting statistically significant lower odds of QTc prolongations OR: 0.27;95% CI of [0.09 to 0.75]. Patients with a BMI of 25 or higher were prevalent, with no statistically significant effect on the odds of QTc prolongation, OR:1.84, 95% CI [0.56 to 6.34]. Hypokalemia was noted in only 3 out of 63 individuals (4.8%) with a prolonged QTc interval. Conversely, heart failure was more common in this cohort, affecting 69.8%, and was associated with a statistically significant increase in the odds of QTc prolongation, OR: 4.98; 95% CI of [1.58 to 17.35]. Myocardial infarction and hypothyroidism were reported in the past medical history of 12.7% and 15.9% of these patients, with no statistically significant odds of QTc prolongation, OR: 0.29, 95% CI [0.07 to 1.03], and OR: 0.76, 95% CI [0.20 to 2.89], respectively. Sepsis was diagnosed in 22.2% of identified patients with a non-statistically significant increase in the odds of Qtc prolongation, OR: 1.48, 95% CI [0.36 to 5.99], tachycardia as well existed in 20.6% of patients with no statistically significant effect on the odds of Qtc prolongation 0.52 [0.17 to 1.51]. Similarly, patients who were on more than two drugs had no significant increase in the odds of Qtc prolongation OR: 1.47, 95% CI [0.59 to 3.78] (Table 2).
 |
Table 2 Analysis of Baseline Characteristics and Established Risk Factors of QTc Interval Prolongation Using a Multivariate Approach |
Discussion
The present study provides a comprehensive analysis of QT interval prolongation associated with non-cardiac medications in real-world settings, including diverse populations encompassing various age groups and comorbidities. The findings indicate a high prevalence of QT interval prolongation among hospitalized patients receiving CredibleMeds-listed non-cardiac drugs. Antimicrobials, PPIs, and antiemetics were identified as key contributors to QTc interval prolongation. Moreover, our study provides valuable insights into the risk factors associated with non-cardiac drug-induced QTc interval prolongation in a real-world hospital setting. The multivariate analysis revealed that heart failure was significantly associated with QTc prolongation, while other factors such as age, BMI, and certain comorbidities did not show a statistically significant impact. These findings emphasize the importance of vigilant monitoring and tailored approaches in different clinical settings to mitigate potential risks.
Previous research has shown that females typically have a higher risk of QTc prolongation, with longer QTc intervals observed in females compared to males. This difference is attributed to variations in ion channel activity, tissue conductivity, and heart dimensions between sexes, leading to longer QT intervals in women.13 However, our multiple logistic regression analysis results reveal that females with non-cardiac drug-induced QTc interval prolongation actually had lower odds compared to their male counterparts. This may partially be explained by a study that revealed a significant increase in the QTc in the elderly male population, associated with a decline in testosterone levels,14 who comprise almost 60% of our study subjects. On the other hand, multivariate logistic regression analysis revealed that advanced age (> 65 years old) overall was not associated with a statistically significant increase in the odds of drug-induced QTc interval prolongation compared to the younger cohort.
It is widely acknowledged that obesity significantly impacts the structural integrity of the heart, potentially leading to abnormalities in the repolarization of the ventricles and atria.15,16 While certain studies have established a correlation between BMI and prolonged QTc interval,17 others have reported no difference in QTc interval values between individuals with uncomplicated obesity and control subjects.18 Consistent with these findings, our study did not identify a statistically significant increase in the odds of QTc interval prolongation among overweight and obese cohorts; this can be attributed to the small sample size of this group, evident in the broad confidence interval [0.56 to 6.34].
Moreover, the current study highlights heart failure with reduced ejection fraction as the most prevalent comorbidity observed in patients with prolonged QT intervals. This comorbidity exhibited high odds of drug-induced QTc interval prolongation in the multivariate analysis. This correlation is consistent with existing data, which indicate that patients with heart failure demonstrate altered regulation of potassium and calcium channels, as well as reduced levels of the gap-junction protein connexin 43.19 These alterations result in prolonged repolarization duration, rendering patients more susceptible to TdP when exposed to noncardiac QT-prolonging drugs, which incidentally block myocardial potassium channels and further delay repolarization.20
Sepsis was identified as the second most common comorbidity among those with prolonged Qtc, present in 22% of cases. Although the odds of prolonged QTc interval in our study were not statistically significant, it holds clinical importance due to the potential for sepsis-induced cardiomyopathy to impair myocardial contractility and lead to atrial and ventricular arrhythmias. It is important to note that various metabolic factors can influence QTc duration and may fluctuate during sepsis, resulting in either shortened or prolonged QTc interval, which could explain our observations.21 Additionally, the limited size of this cohort may affect this result.
Myocardial infarction was observed in 12.7% of the cases, yet no statistically significant prolongation of the QTc interval was detected. This may be attributed to changes in QT behavior during the immediate period following acute ST-elevation myocardial infarction. According to a study, the QTc interval begins to prolong at the time of the acute event, peaks three days later, and then starts to shorten.22 Further research indicated that while ventricular repolarization is prolonged during the acute phase of myocardial infarction, the QTc intervals return to baseline levels once the myocardial ischemia resolves, thus preventing permanent prolongation.23
Electrolyte disturbances are recognized as clinical risk factors that increase the risk of QTc interval prolongation. These disturbances can cause or exacerbate clinical arrhythmia, even in the presence of normal cardiac tissue.24 In our study, hypomagnesemia and hypocalcemia were prevalent in most cases (96.7%). Hypomagnesemia, associated with various disorders, can disrupt energy metabolism, alter action potentials, and destabilize myocardial cells, primarily resulting in ventricular arrhythmia.25 Hypocalcemia, although rarely occurring in isolation, is a known but uncommon cause of QTc interval prolongation.26 Despite limited available data, a recent meta-analysis found a positive correlation between QTc interval and corrected total serum calcium levels.27 Among all electrolyte disturbances, hypokalemia had the strongest association with QTc prolongation.28 However, as potassium levels often reflect the results of blood tests performed immediately after resuscitation efforts, hypokalemia was only evident in a small percentage of our findings (4.8%).
Hypothyroidism was present in a significant portion of the affected patients (15.9%). Our findings revealed that patients with hypothyroidism, although not statistically proven, had lower odds of QT prolongation than those without this condition. This aligns with existing literature, which indicates an inverse relationship between thyroid hormone levels and the QT interval.29
This study also examined the effect of combined QT-prolonging medications; approximately one-third (31.1%) of cases were exposed to two QT-prolonging medications simultaneously. However, these patients did not show significant clinical differences compared to those on a single QT-prolonging medication. This finding aligns with previous research that found no significant increase in QTc prolongation for patients taking multiple QT-relevant medications or those on conditional or risk medications.30
It is important to clarify that the risk factors discussed in this study were primarily derived from existing literature and not directly identified through multivariable analysis within our study population. We determined the frequency of these previously described risk factors among our patients and made interpretations based on their prevalence. This approach limits our ability to assert with certainty that these risk factors behave similarly in our study beyond their frequency of occurrence. Consequently, this represents a limitation of our study, as it may lead to biased interpretations and does not account for other unanalyzed factors that could be associated with QT prolongation, potentially leading to confounding bias.
Upon examining the most common medication associated with QTc prolongation. PPIs accounted for seventy-eight cases (51.66%). The PPI nomogram frequently showed higher risk plots, particularly with esomeprazole. Among the patients using esomeprazole, 53 (35.1%) experienced QT prolongation. Although rare, PPI-induced hypomagnesemia can be associated with Torsades de Pointes (TdP) due to PPIs’ class effect of reducing intestinal magnesium absorption.31 Despite increasing evidence, PPIs are not recognized as contributing factors to QTc interval prolongation in clinical practice.32
Additionally, in this study, the antimicrobial group, including medications such as azithromycin, ciprofloxacin, erythromycin, moxifloxacin, piperacillin-tazobactam, and ofloxacin, was associated with most cases considered at high risk for developing TdP. The use of antimicrobials can lead to acquired QT prolongation.33 Various case reports and studies have documented several cardiac effects related to quinolone-induced arrhythmia, including QT interval prolongation, TdP, ventricular tachycardia, ventricular fibrillation, and sudden cardiac death.34 Recently, a case report described a 40-year-old man with no history of cardiac disease who died from recurrent cardiac arrest secondary to ciprofloxacin-induced TdP.35 Additionally, macrolides are known to prolong the QTc interval and cause dispersion of repolarization across the ventricular wall, potentially inducing TdP.36
Among antiemetics, cardiac effects related to QTc prolongation were frequently reported with domperidone and setrons (granisetron, ondansetron).37 A case report highlighted granisetron’s significant impact on the QTc interval, describing acute bradycardia that led to asystole and cardiac arrest shortly after an intravenous granisetron injection in a female patient.38 When assessing the risk of QTc prolongation, antiemetic medications showed variable scatter around the risk line, with no clear trend. Notably, one case involving granisetron fell within the high-risk domain, while ondansetron and metoclopramide were near the risk line.
Plotting the remaining drugs revealed a distinct high-risk pattern primarily associated with the antihistamine diphenhydramine. Several studies have confirmed that an overdose of diphenhydramine is linked to a significant increase in the QTc interval.39 Furthermore, diphenhydramine use was associated with two incidences of Torsades de Pointes in an observational cohort evaluation.40 Conversely, other classes of medications, such as immunosuppressants, antidepressants, antipsychotics, and antiepileptics, appeared to cluster around the risk line.Our study provides valuable insights, and although it has certain limitations, these offer opportunities for future research improvements. Like other retrospective cross-sectional studies, there is a risk of uncontrolled confounding variables, which can enhance our understanding of complexities in real-world settings. The selection bias stemming from the inclusion of diverse clinical scenarios—such as psychiatric wards, internal medicine wards, and intensive care units—reflects the varied exposure to QT-prolonging drugs and underscores the need for tailored approaches in different settings. This diversity, while challenging, highlights the importance of context-specific findings. Attrition bias, another potential limitation, points to the dynamic nature of clinical data collection and highlights the importance of robust data management strategies. Although reliance on data from a single center limits generalizability, it allows for a focused and detailed analysis that can lay the groundwork for multi-center studies. We acknowledge that we missed collecting some variables that contribute to QTc prolongation, such as infections, which could act as confounding factors. Future research should aim to include a larger patient population and employ comprehensive data collection methods across multiple centers to enhance the robustness of the findings. Additionally, implementing specific strategies to control selection and attrition bias will further strengthen the validity of future results, paving the way for more reliable and applicable conclusions.
Conclusion
Our study provides valuable insights into the risk factors associated with non-cardiac drug-induced QTc interval prolongation in a real-world hospital setting. While our findings highlight the significant risk associated with the in-hospital administration of QTc-prolonging non-cardiac medications, particularly among patients with heart failure, we acknowledge the limitations of our study, including potential selection and attrition biases. The multivariate analysis revealed that heart failure was significantly associated with QTc prolongation, while other factors such as age, BMI, and certain comorbidities did not show a statistically significant impact. These results underscore the importance of vigilant monitoring and tailored approaches in different clinical settings to mitigate potential risks. Future research should aim to include a larger patient population and employ comprehensive data collection methods across multiple centers to enhance the robustness and generalizability of the findings.
Acknowledgment
The authors would like to thank the data management department at King Abdullah International Medical Research Center for facilitating data collection for this project.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Sarazan RD. The QT interval of the electrocardiogram. Encyclopedia of Toxicology: Third Edition. 2014;10–15. doi:10.1016/B978-0-12-386454-3.00917-9
2. Davies RA, Ladouceur VB, Green MS, et al. The 2023 Canadian Cardiovascular Society clinical practice update on management of the patient with a prolonged QT interval. Canadian Journal of Cardiology. 2023;39(10):1285–1301. doi:10.1016/J.CJCA.2023.06.011/ASSET/11BF2C21-B48A-4FBA-846E-71F212DAFA4F/MAIN.ASSETS/GR9.JPG
3. Shah RR. Drugs, QT interval prolongation and ICH E14: the need to get it right. Drug Safety. 2005;28(2):115–125. doi:10.2165/00002018-200528020-00003/METRICS
4. Beinart R, Zhang Y, Lima JAC, et al. The QT interval is associated with incident cardiovascular events: the mesa study. Journal of the American College of Cardiology. 2014;64(20):2111–2119. doi:10.1016/J.JACC.2014.08.039
5. Vink AS, Neumann B, Lieve KVV, et al. Determination and Interpretation of the QT interval: comprehensive analysis of a large cohort of long QT Syndrome patients and controls. Circulation. 2018;138(21):2345–2358. doi:10.1161/CIRCULATIONAHA.118.033943/SUPPL_FILE/CIRC_CIRCULATIONAHA-2018-033943_SUPP1.PDF
6. Nachimuthu S, Assar MD, Schussler JM. Drug-induced QT interval prolongation: mechanisms and clinical management. Therapeutic Advances in Drug Safety. 2012;3(5):241–253. doi:10.1177/2042098612454283/ASSET/IMAGES/LARGE/10.1177_2042098612454283-FIG4.JPEG
7. Alomar M, Palaian S, Al-tabakha MM. 2019 Pharmacovigilance in perspective: drug withdrawals, data mining and policy implications. F1000Research. 2019;8(2109):2109. doi:10.12688/f1000research.21402.1
8. van Noord C, Eijgelsheim M, Stricker BHC. Drug- and non-drug-associated QT interval prolongation. British Journal of Clinical Pharmacology. 2010;70(1):16–23. doi:10.1111/J.1365-2125.2010.03660.X
9. Woosley RL, Heise CW, Romero KA. QTdrugs List: AZCERT, Inc. 1822 Innovation Park Dr. Oro Valley, AZ; 2008 Available from: www.crediblemeds.org.
10. For healthcare providers: crediblemeds. Available from: https://crediblemeds.org/healthcare-providers.
11. Tan H, Yan X, Chen Y, et al. A real-world pharmacovigilance study of drug-induced QT interval prolongation: analysis of spontaneous reports submitted to FAERS. Frontiers in Cardiovascular Medicine. 2024;11:1363382. doi:10.3389/FCVM.2024.1363382/BIBTEX
12. Isbister GK. Risk assessment of drug-induced QT prolongation. Australian Prescriber. 2015;38(1):20–24. doi:10.18773/AUSTPRESCR.2015.003
13. Peirlinck M, Sahli Costabal F, Kuhl E. Sex differences in drug-induced arrhythmogenesis. Frontiers in Physiology. 2021;12:708435. doi:10.3389/FPHYS.2021.708435/BIBTEX
14. Rabkin SW, Cheng XBJ, Thompson DJS. Detailed analysis of the impact of age on the QT interval. Journal of Geriatric Cardiology: JGC. 2016;13(9):740. doi:10.11909/J.ISSN.1671-5411.2016.09.013
15. Iacobellis G, Ribaudo MC, Leto G, et al. Influence of excess fat on cardiac morphology and function: study in uncomplicated obesity. Obesity Research. 2002;10(8):767–773. doi:10.1038/OBY.2002.104
16. Iacobellis G, Ribaudo MC, Zappaterreno A, Iannucci CV, Di Mario U, Leonetti F. Adapted changes in left ventricular structure and function in severe uncomplicated obesity. Obesity Research. 2004;12(10):1616–1621. doi:10.1038/OBY.2004.201
17. Ravikumar V, Vajravelu HR, Ayyavoo S, Ramraj B. Correlation of adiposity indices with electrocardiographic ventricular variables and vascular stiffness in young adults. Journal of Clinical and Diagnostic Research: JCDR. 2017;11(6). doi:10.7860/JCDR/2017/27641.10062
18. Girola A, Enrini R, Garbetta F, Tufano A, Caviezel F. QT dispersion in uncomplicated human obesity. Obesity Research. 2001;9(2):71–77. doi:10.1038/OBY.2001.9
19. Näbauer M. Potassium channel down-regulation in heart failure. Cardiovascular Research. 1998;37(2):324–334. doi:10.1016/S0008-6363(97)00274-5/2/37-2-324-FIG2.GIF
20. Woosley RL, Schwartz PJ, Elavathil LJ, Tomlinson CW. Drug-induced long QT syndrome and torsade de pointes. The Canadian Journal of Cardiology. 2005;21(10):185–200. doi:10.1007/978-3-030-22672-5_10
21. Wasserstrum Y, Lotan D, Itelman E, et al. Corrected QT interval anomalies are associated with worse prognosis among patients suffering from sepsis. Internal Medicine Journal. 2016;46(10):1204–1211. doi:10.1111/IMJ.13170
22. Mann T, Moses A, Yesaulov A, et al. QT interval dynamics in patients with ST-elevation MI. Frontiers in Cardiovascular Medicine. 2023;9. doi:10.3389/FCVM.2022.1056456.
23. Taylor GJ, Crampton RS, Gibson RS, Stebbins PT, Waldman MTG, Beller GA. Prolonged QT interval at onset of acute myocardial infarction in predicting early phase ventricular tachycardia. American Heart Journal. 1981;102(1):16–24. doi:10.1016/0002-8703(81)90407-5
24. El-Sherif N, Turitto G. Electrolyte disorders and arrhythmogenesis. Cardiology Journal. 2011;18(3):233–245.
25. Negru AG, Pastorcici A, Crisan S, Cismaru G, Popescu FG, Luca CT. The role of hypomagnesemia in cardiac arrhythmias: a clinical perspective. Biomedicines. 2022;10(10):2356. doi:10.3390/BIOMEDICINES10102356
26. Tang JKK, Rabkin SW. Hypocalcemia-induced QT interval prolongation. Cardiology. 2022;147(2):191–195. doi:10.1159/000515985
27. Newman DB, Fidahussein SS, Kashiwagi DT, et al. Reversible cardiac dysfunction associated with hypocalcemia: a systematic review and meta-analysis of individual patient data. Heart Failure Reviews. 2014;19(2):199–205. doi:10.1007/S10741-013-9371-1
28. Vandael E, Vandenberk B, Vandenberghe J, Willems R, Foulon V. Risk factors for QTc-prolongation: systematic review of the evidence. International Journal of Clinical Pharmacy. 2017;39(1):16–25. doi:10.1007/S11096-016-0414-2
29. Tayal B, Graff C, Selmer C, et al. Thyroid dysfunction and electrocardiographic changes in subjects without arrhythmias: a cross-sectional study of primary healthcare subjects from Copenhagen. BMJ Open. 2019;9(6):e023854. doi:10.1136/BMJOPEN-2018-023854
30. Riad FS, Davis AM, Moranville MP, Beshai JF. Drug-Induced QTc Prolongation. American Journal of Cardiology. 2017;119(2):280–283. doi:10.1016/j.amjcard.2016.09.041
31. Chrysant SG. Proton pump inhibitor-induced hypomagnesemia complicated with serious cardiac arrhythmias. Expert Review of Cardiovascular Therapy. 2019;17(5):345–351. doi:10.1080/14779072.2019.1615446
32. Danielsson B, Collin J, Nyman A, et al. Drug use and torsades de pointes cardiac arrhythmias in Sweden: a nationwide register-based cohort study. BMJ Open. 2020;10(3):e034560. doi:10.1136/BMJOPEN-2019-034560
33. Roden DM. Drug-Induced Prolongation of the QT Interval. New England Journal of Medicine. 2004;350(10):1013–1022. doi:10.1056/NEJMRA032426
34. Frothingham R. Rates of torsades de pointes associated with ciprofloxacin, ofloxacin, levofloxacin, gatifloxacin, and moxifloxacin. Pharmacotherapy: The Journal of Human Pharmacology and Drug Therapy. 2001;21(12):1468–1472. doi:10.1592/PHCO.21.20.1468.34482
35. Usmael S, Seyoum T. Sudden cardiac death due to ciprofloxacin induced torsade de pointes. Available from: https://d197for5662m48.cloudfront.net/documents/publicationstatus/202787/preprint_pdf/15c091c12116d05dc56b628d0daf2fcb.pdf.
36. Gitler B, Berger LS, Buffa SD. Torsades de pointes induced by erythromycin. Chest. 1994;105(2):368–372. doi:10.1378/CHEST.105.2.368
37. Rochoy M, Auffret M, Béné J, Gautier S. Antiemetics and cardiac effects potentially linked to prolongation of the QT interval: case/non-case analysis in the national pharmacovigilance database. Revue d’epidemiologie et de Sante Publique. 2017;65(1):1–8. doi:10.1016/J.RESPE.2016.06.335
38. Al Harbi M, Al Rifai D, Al Habeeb H, Wambi F, Geldhof G, Dimitriou V. A case of granisetron-associated intraoperative cardiac arrest. Middle East Journal of Anaesthesiology. 2016;23(4):475–478.
39. Zareba W, Moss AJ, Rosero SZ, Hajj-Ali R, Konecki J, Andrews M. Electrocardiographic findings in patients with diphenhydramine overdose. The American Journal of Cardiology. 1997;80(9):1168–1173. doi:10.1016/S0002-9149(97)00634-6
40. Pratt CM, hertz RP, Ellis BE, Crowell SP, Louv W, Moyé L. Risk of developing life-threatening ventricular arrhythmia associated with terfenadine in comparison with over-the-counter antihistamines, ibuprofen and clemastine. The American Journal of Cardiology. 1994;73(5):346–352. doi:10.1016/0002-9149(94)90006-X
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.