")
Back to Journals » Clinical Interventions in Aging » Volume 17
Prediction of Postoperative Delirium After Cardiac Surgery with A Quick Test of Cognitive Speed, Mini-Mental State Examination and Hospital Anxiety and Depression Scale
Authors Segernäs A, Skoog J , Ahlgren Andersson E , Almerud Österberg S , Thulesius H , Zachrisson H
Received 19 November 2021
Accepted for publication 2 March 2022
Published 2 April 2022 Volume 2022:17 Pages 359—368
DOI https://doi.org/10.2147/CIA.S350195
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Nandu Goswami
Anna Segernäs,1,* Johan Skoog,2,* Eva Ahlgren Andersson,3 Sofia Almerud Österberg,4,5 Hans Thulesius,6,7,* Helene Zachrisson2,*
1Primary Health Care Center Ekholmen in Linköping and Department of Health, Medicine and Caring Sciences, Linköping University, Linköping, Sweden; 2Department of Clinical Physiology and Department of Health, Medicine and Caring Sciences, Linköping University, Linköping, Sweden; 3Department of Thoracic Surgery and Department of Health, Medicine and Caring Sciences, Linköping University, Linköping, Sweden; 4Department of Health and Caring Sciences, Faculty of Health and Life Sciences, Linnaeus University, Växjö, Sweden; 5Department of Research and Development, Region Kronoberg, Växjö, Sweden; 6Department of Clinical Sciences, Malmö, Faculty of Medicine, Lunds University, Lund, Sweden; 7Department of Medicine and Optometry, Faculty of Health and Life Sciences, Linnaeus University, Kalmar, Sweden
*These authors contributed equally to this work
Correspondence: Johan Skoog, Department of Clinical Physiology and Department of Health, Medicine and Caring Sciences, Linköping University, Linköping, Sweden, Tel +46 10 103 00 00, Email [email protected]
Purpose: To evaluate if preoperative assessment with A Quick Test of Cognitive Speed (AQT) could increase the accuracy of predicting delirium after cardiac surgery compared to Mini-Mental State Examination (MMSE), and examine if a composite of variables, including cognitive function and depressive symptoms, could be useful to predict delirium.
Patients and Methods: Cardiac surgery was performed in 218 patients (mean age 72 years). Preoperative evaluation involved AQT, MMSE and Hospital Anxiety And Depression Scale (HADS). Postoperative delirium was assessed using Nursing Delirium Screening Scale (Nu-DESC) and Confusion Assessment Method-ICU (CAM-ICU). Logistic regression was performed to detect predictors of postoperative delirium and receiver operator characteristic curves (ROC) with area under the curve (AUC) to determine the accuracy.
Results: Postoperative delirium occurred in 47 patients (22%) who had lower MMSE scores (median (range), 27 (19– 30) vs 28 (20– 30), p=0.009) and slower AQT (median (range), 76 (48– 181) vs 70 (40– 182) seconds, p=0.030) than patients without delirium. Predictive power measured as AUC (95% CI) was 0.605 (0.51– 0.70) for AQT and 0.623 (0.53– 0.72) for MMSE. Logistic regression (OR, 95% CI) showed MMSE < 27 points (2.72, 1.27– 5.86), AQT > 70 sec (2.26, 1.03– 4.95), HADS-D > 4 points (2.60, 1.21– 5.58) and longer cardiopulmonary bypass-time (1.007, 1.002– 1.013) to be associated with postoperative delirium. Combining these parameters yielded an AUC of 0.736 (0.65– 0.82).
Conclusion: The ability of predicting delirium using AQT was similar to MMSE, and only slightly higher by combining AQT and MMSE. Adding HADS-D and cardiopulmonary bypass-time to MMSE and AQT increased the predictive power to a borderline acceptable discriminatory value. Preoperative cognitive tests and screening for depressive symptoms may help identify patients at risk of postoperative delirium. Yet, there is still a need to establish useful preoperative tests.
Keywords: postoperative delirium, cardiopulmonary bypass, Mini Mental State Examination, A Quick Test of Cognitive Speed, The Hospital Anxiety and Depression Scale
Introduction
Postoperative delirium is common after cardiac surgery with a prevalence ranging between 11%–52% depending on patient selection and evaluation method.1 Postoperative delirium is associated with increased length of hospital stay as well as increased morbidity and mortality.2,3 Thus, preoperative identification of individuals at higher risk of developing postoperative delirium is important to facilitate preventive efforts already in the preoperative period.4 Although the pathophysiological mechanisms of delirium are multifactorial, cognitive impairment prior to surgery is a well-documented risk factor.1 Several studies have used the Mini-Mental State Examination (MMSE) to evaluate cognitive status and lower MMSE scores have frequently been associated with a higher risk of developing delirium.5–7 However, MMSE scores can be affected by education, age, language, ethnicity,8,9 and the ability to identify patients with mild cognitive impairment have been reported to be limited with MMSE.10 This may be partly due to under-represented testing of executive function, cognitive speed and attention, which could represent early signs of mild cognitive impairment,10,11 and could thus lead to an underestimation of individuals at risk of postoperative delirium during the preoperative assessment. Based on this, other cognitive test may be beneficial in evaluating the risk of postoperative delirium. A Quick Test of Cognitive Speed (AQT) is a user-friendly and quickly administered test of processing speed, attention and executive function.12 AQT is not affected by education and minimally affected by age,13 and could thus serve as a complement to MMSE during the preoperative evaluation. In addition, depression has recently been suggested to be associated with delirium after cardiac surgery,14 and screening for preoperative depressive symptoms can be done by The Hospital Anxiety and Depression Scale (HADS).15 Thus, the primary aim of the present study was to evaluate if preoperative assessment with AQT could increase the accuracy of predicting delirium after cardiac surgery. The secondary aim was to test if a composite of preoperative assessment variables, including depression and quality of life measures, could be useful to predict postoperative delirium. We hypothesized that a slower performance during the cognitive speed test AQT during preoperative evaluation was associated with a higher risk of developing delirium after cardiac surgery. Further, we hypothesized that including evaluations of the patients’ mental status regarding anxiety and depression symptoms would improve the prediction of postoperative delirium as compared to cognitive tests alone.
Materials and Methods
Participants
In this dual center study, we recruited 218 patients who were scheduled for cardiac surgery at the Departments of Cardiothoracic surgery, Blekinge Hospital Karlskrona, during a period of four years, and Linköping University Hospital, Sweden, during a period of three years. Recruitment of patients was contingent on the availability of specially trained research nurses during the data collection period, and patients were recruited consecutively on days when research nurses were working. In accordance with our inclusion criteria, all patients needed to be at least 50 years old and have no prior history of dementia or severe psychiatric disease. Exclusion criteria were emergency procedures, inability to complete the neuropsychological tests (deafness, blindness, language difficulties). All patients were scheduled for coronary artery bypass graft (CABG) surgery, aortic valve replacement (AVR) surgery, mitral valve replacement (MVR) surgery or mitral plastic surgery, or combined surgery (CABG and AVR). One patient was excluded due to lack of delirium assessment in the postoperative period. Medical, Health and functional data were collected by interviewing the patients in connection to their neuropsychological tests.
Demographic variables and data regarding the operative procedures, risk factors and laboratory values were collected from the patients’ medical records and in a local database at the cardiothoracic Departments. The study was approved by the regional ethical review board in Linköping, Sweden, 2010/166-31 and 2010/426-32, and all participants signed a written informed consent in accordance with the Declaration of Helsinki.
Screening Instruments
Postoperative delirium was evaluated using the Nursing Delirium Screening Scale (Nu-DESC) at Linköping University Hospital and the Confusion Assessment Method-ICU (CAM-ICU) at Blekinge Hospital Karlskrona. All patients were daily evaluated, with screening for delirium at least once a day, during the first post-operative week and the staff who made the registrations were well acquainted with the instruments in clinical routine. The Nu-DESC detects delirium by evaluating disorientation, inappropriate behavior, inappropriate communication, illusions/hallucinations, psychomotor retardation, each graded between 0 and 2 (0=absent, 1=mild, 2=severe), with a maximum score of 10. A score of ≥2 was considered as postoperative delirium in this study.16 The CAM-ICU diagnoses delirium by assessing fluctuating mental status, inattention, disorganized thinking and an altered state of consciousness.17 Delirium was defined as present if the patient presented with an acute change in mental status with difficulty focusing attention in combination with altered level of consciousness or disorganized thinking.18 The sensitivity and specificity of detecting delirium have been reported to be similar between Nu-DESC and CAM-ICU,19 and both methods have been validated as appropriate screening tool for diagnosing delirium.16,20,21
The neuropsychological tests MMSE and AQT were used to assess the patients’ cognitive function. The MMSE assesses orientation in time and place, working memory and delayed memory, attention, language, and visuospatial ability. The maximum score is 30 points (range 0–30), with lower scores denoting more impaired cognition. Preoperative MMSE scores <27 points were used to indicate an abnormal test result.22 AQT consists of 40 visual stimuli as geometric figures – circles, squares, rectangles, or triangles, colored red, black, yellow, or blue. In this study, we used the patients’ readings of AQT form-naming and color and form-naming. The AQT assesses perceptual function and cognitive speed. Cut-off reading times for abnormal performance for AQT form has been suggested to be >35 seconds and AQT color and form >70 seconds.23
We used the Hospital Anxiety and Depression Scale (HADS) to evaluate anxiety and depression. HADS consists of 14 items with seven statements for each sub scale: HADS Anxiety (HADS-A) and HADS Depression (HADS-D). Every statement has four possible choices (on the Likert scale ranging from zero to three), and the maximum score per sub scale is 21 points.24 Preoperative HADS-D scores >4 points were used to indicate an abnormal test result.25
We assessed Health‐related quality of life with EQ‐5D, which evaluates individuals in five domains (mobility, self‐care, usual activities, pain/discomfort and anxiety/depression).26 Each domain is divided into three levels of graded severity. A global health index was generated for each individual by aggregating and weighting the five domains, using the Danish EQ‐5D time-trade-off tariff.27 The EQ-5D also contains a health state visual analogue scale (EQ-VAS) ranging from 0 to 100 millimeters, representing the worst imaginable to the best imaginable health state.
Anesthesia and Operative Procedure
Anesthetic and surgical procedures were standardized for all patients. Drugs were withheld after an overnight’s fast with the exception of betablockers and calcium antagonists. Patients were premedicated with paracetamol and oxazepam, and anaesthesia was induced with thiopentone 1 mg/kg body weight and fentanyl 30 μg/kg body weight. For neuromuscular blockade, 50 mg Rocuronium was used at induction and 30 mg at sternal closure. Fentanyl and isoflurane were used to maintain anesthesia. Antibiotic prophylaxis was given 30 minutes before skin incision, and heparin was administrated according to recommendations by HepCon with activated clotting time held over ≥ 480 sec. If arterial pressure (MAP) fell < 50 mmHg, phenylephrine was added. The surgical procedures involved the following phases. 1) surgery start with skin incision; 2) graft harvesting in CABG procedures; 3) administration of Heparin; 4) establishment of the ECC circuit with insertion of the aortic and venous cannula when blood pressure (BT) was <100 mmHg, and after epiaortic ultrasound scan of the ascending aorta; 5) start of CPB, with the time noted in the anesthesia record; 6) aortic cross clamping and administration of cardioplegic solution, which was repeated every 20 minutes for myocardial protection; 7) cardiac surgery procedure was performed; 8) aortic cross clamp removal; 9) termination of CPB, with the time noted in the anesthesia record, and administration of phenylephrine, adrenaline, noradrenaline when needed; 9) aortic decannulation, when BT <100 mmHg and administration of protamine. The procedure was performed with non-pulsatile flow during CPB, and moderate hemodilution (hematocrit 20–25%) and mild hypothermia (33–36 C°) were usually employed. Perioperative parameters were not assessed in the present study although during the standardized CBP procedure, cerebral oximetry was used to detected changes in cerebral blood flow and the minute ventilation was corrected to maintain normocapnia in order to keep cerebral blood flow stable.
Statistical Analysis
Statistical analyses were performed using SPSS statistics 27 for Windows (IBM, Armonk, NY, USA). Continuous normally distributed data were compared by unpaired Student’s t-test and Mann–Whitney U-test was used when data were ordinal or not normally distributed. Categorical variables were analyzed using Chi‐square test. A stepwise backward logistic regression analyses was performed to identify risk factors for postoperative delirium. Variables with p values <0.15 in the univariable analysis were entered into the multivariable analysis. Odds ratios (ORs) and 95% CIs were calculated and the Hosmer-Lemeshow test was used to assess the fit of the model. Receiver operating characteristic (ROC) curves were constructed using univariate parameters and the predicted probability from logistic regression. The area under the curve (AUC) with 95% CI was calculated and interpreted as acceptable discrimination for values 0.7≤ AUC <0.8; as excellent discrimination for values 0.8≤ AUC <0.9 and outstanding discrimination for values AUC ≥0.9.28 Statistical significance was defined at p <0.05.
Results
Patient’s Characteristics
Of 218 patients undergoing cardiac surgery, 159 men (73%) and 59 women (27%), 47 patients developed postoperative delirium (22%) assessed by Nu-DESC and CAM-ICU. No differences in frequency of postoperative delirium were seen between men (n = 34, 21%) and women (n = 13, 22%) p = 0.92. Further, no difference in frequency of diagnosing delirium was seen with Nu-DESC (n = 22, 22%) compared to CAM-ICU (n = 25, 22%), p = 0.99.
Univariable Predictors of Postoperative Delirium
Univariable comparisons between patients developing delirium and those who did not are presented in Table 1. Median age (range) was higher in the delirium group (76 (61–85) years) compared to the non-delirium group (71 (50–85) years, p = 0.01). Patients with delirium displayed lower MMSE score (p = 0.009), slower performance during the cognitive speed test AQT color and form (p = 0.03) and lower EQ5D score (p = 0.04) during preoperative assessments. Patients who developed delirium more frequently displayed HADS-D score >4 (p = 0.012) and EQ-VAS <61 mm (p = 0.015). Combined CABG and valve surgery were more common in patients with delirium (p = 0.006) as well as longer cardiopulmonary bypass time (p =0.01).
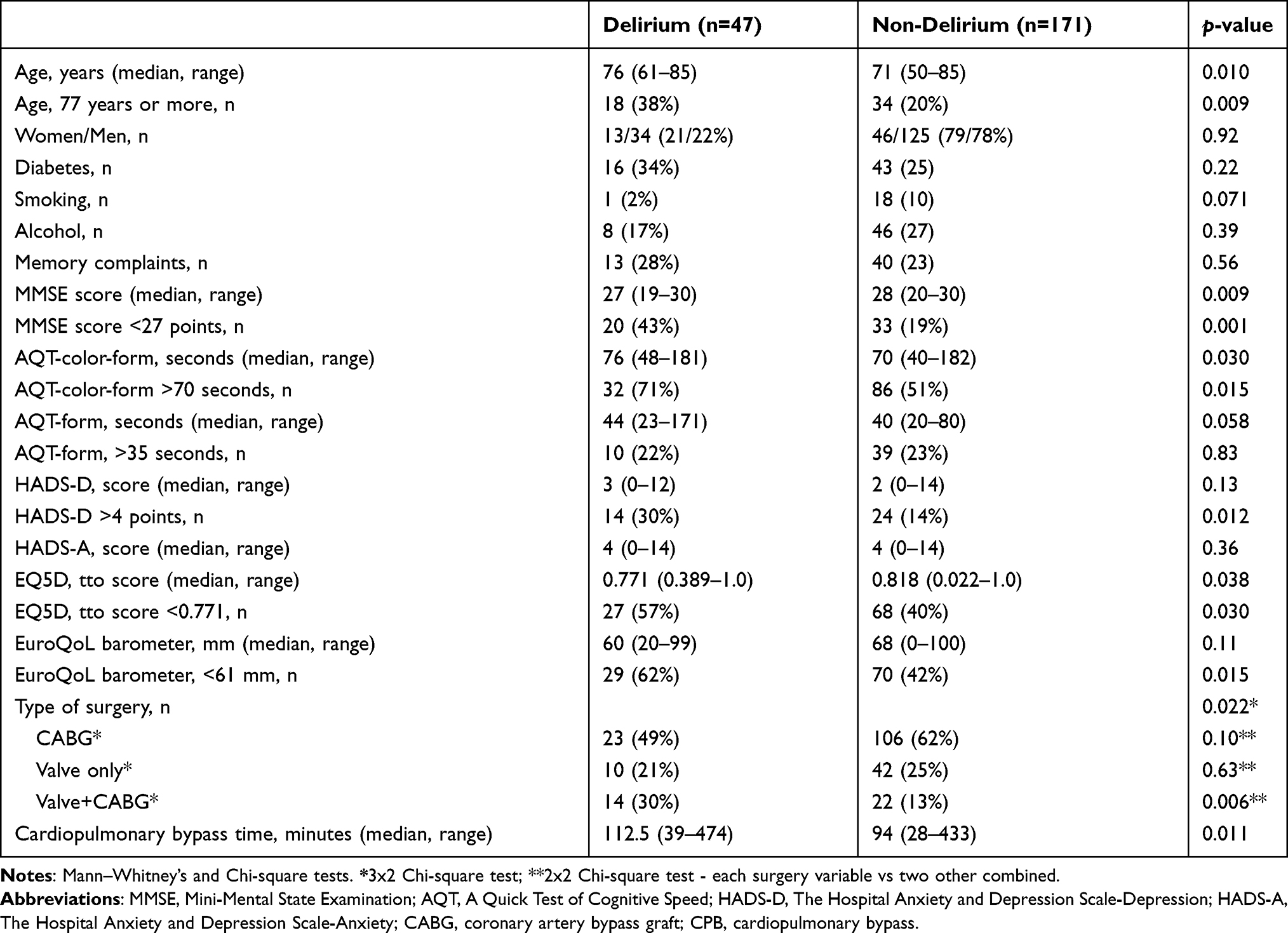 |
Table 1 Comparing Preoperative and Perioperative Characteristics of Patients Who Developed Postoperative Delirium and Those Who Did Not Among 218 Patients Undergoing Cardiac Surgery at Two Participating Thoracic Surgery Centers in South Sweden |
Multivariable Predictors of Postoperative Delirium
In the multivariable analysis, backward logistic regression models were performed based on parameters with p <0.15 from the univariable comparison. The included parameters were age, sex, smoking, MMSE <27 points, AQT color and form >70 seconds, HADS-D >4, EQ5D, EQ-VAS, type of operation and cardiopulmonary bypass-time. Table 2 shows the results of the final model where preoperative MMSE score <27 points, AQT color and form >70 seconds, HADS-D score >4 points and longer cardiopulmonary bypass-time were associated with higher risk of developing postoperative delirium.
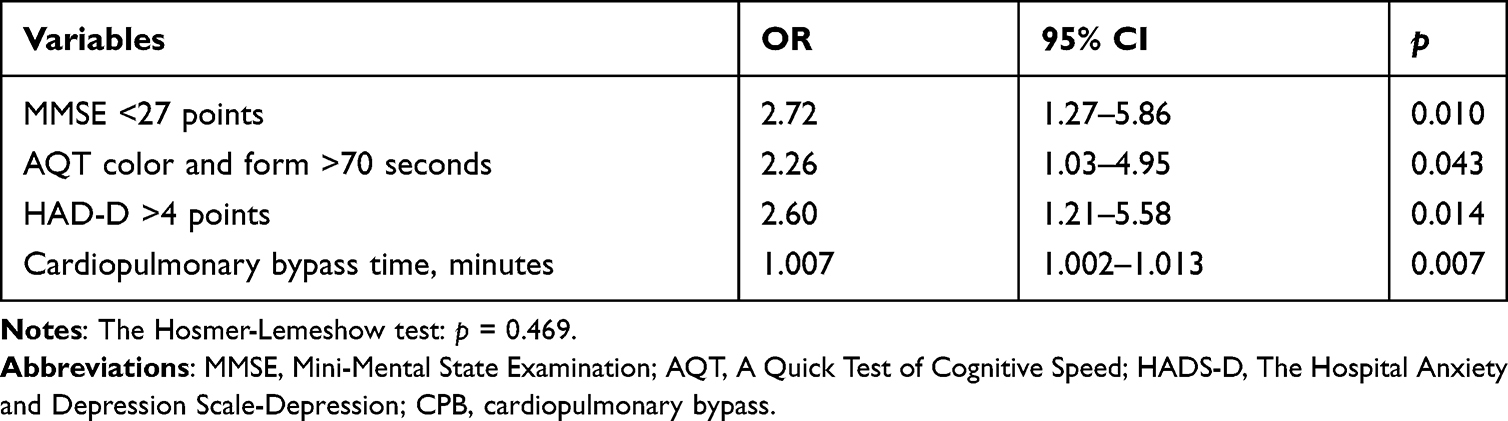 |
Table 2 Multivariable Analysis of Risk Factors Associated with Postoperative Delirium |
ROC Curves for Assessing Accuracy of Predictors of Postoperative Delirium
Receiver operating curves (ROC) curves were used to assess the accuracy of MMSE, AQT color and form and HADS-D as single predictors for postoperative delirium. The AUC (95% CI) was 0.623 (0.53–0.72) for MMSE, 0.605 (0.51–0.70) for AQT color and form and 0.571 (0.47–0.67) for HADS-D. The ROC curve of the predicted probability from logistic modelling with preoperative MMSE <27 points) and AQT color and form >70 seconds demonstrated an AUC (95% CI) of 0.664 (0.57–0.76). Figure 1 shows the ROC curve of the predicted probability from the logistic regression composite variable model comprising of MMSE <27 points, AQT color and form >70 seconds, HADS-D >4 and cardiopulmonary bypass-time, with an AUC (95% CI) of 0.736 (0.65–0.82).
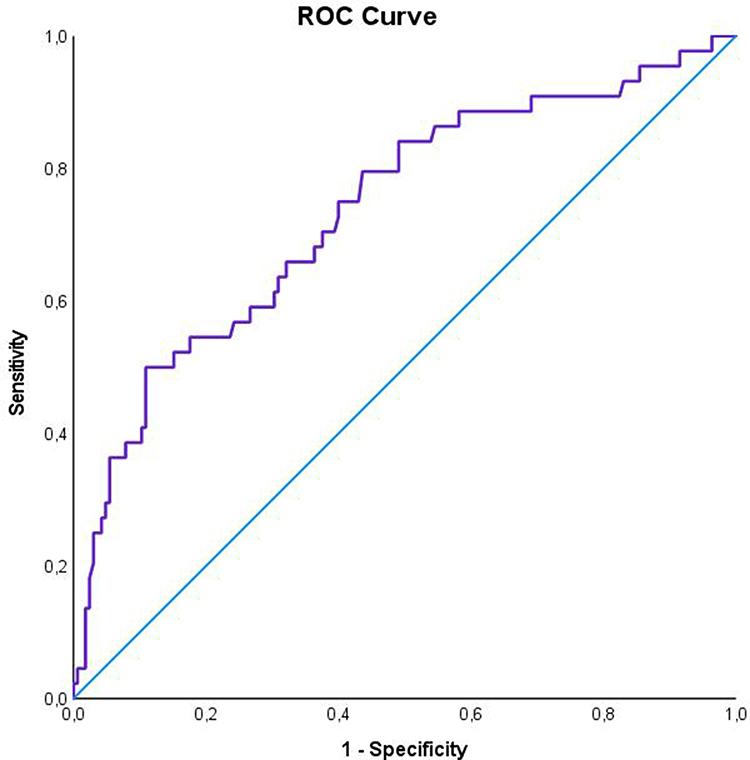 |
Figure 1 ROC curve for the probabilities from logistic modeling using MMSE (>27 points), AQT color and form (>70 seconds), HADS-D (>4 points) and cardiopulmonary by-pass-time. The AUC (95% CI) was 0.736 (0.65–0.82). |
Discussion
The present study confirmed the hypothesis that a slower preoperative performance of the cognitive speed test AQT color and form was associated with a higher risk of developing delirium after cardiac surgery. However, adding AQT color and form to a preoperative cognitive evaluation with MMSE did not significantly increase the ability to predict postoperative delirium compared to using MMSE alone. Nonetheless, ROC analysis showed that a composite of MMSE, AQT, HADS-D and cardiopulmonary bypass-time had an improved and borderline acceptable discriminatory value in predicting postoperative delirium.
Preoperative interventions with focus on improvement of orientation, mobilization, nutritional status, senses, and sleep, as well as decreasing medication use, pain, and anxiety, has been suggested to reduce postoperative delirium according to a systematic review.29 Models that could identify patients at a higher risk of postoperative delirium thus seems important since it may help health care professionals to implement preventive interventions.29,30
Preoperative cognitive impairment defined as low preoperative MMSE scores are common in patients with postoperative delirium.5–7 We also did find that patients with postoperative delirium had a lower preoperative MMSE score than patients without delirium and preoperative MMSE scores <27 points were independently associated with a higher risk of postoperative delirium. However, the ROC analysis showed an AUC of 0.623, which is not an acceptable discrimination for postoperative delirium prediction. One possible explanation is that MMSE was affected by individual characteristics such as age, ethnicity and education,8,11 which could give a ceiling effect, ie, that the test performance was favorably affected by education, or other parameters, independent of cognitive functioning.31 This has previously been linked to a limited ability of MMSE to detect mild cognitive impairment,32 and a poorer sensitivity in finding individuals susceptible to postoperative delirium after cardiac surgery.33 One possible reason for a ceiling effect has been attributed to the lack of assessment of executive functions in MMSE.10,11,32 Thus, AQT, a user-friendly and easily administered test that measures processing speed, attention and executive functions, that could be suited for preoperative evaluation, was used in the present study to complement MMSE.12 AQT’s age effects are limited and AQT is not affected by education level.13 Our results showed that patients with postoperative delirium indeed had a slower preoperative test performance and that AQT color and form >70 seconds was independently associated with a higher risk of postoperative delirium. However, the ROC curve showed an AUC of 0.605, meaning that AQT did not provide a greater accuracy in predicting postoperative delirium compared to MMSE. By combining MMSE <27 points and AQT color and form >70 seconds the AUC increased to 0.664. Alas, the combination did not provide a preoperative acceptable prediction of postoperative delirium (AUC >0.7).
Preoperative symptoms of depression has been a significant predictor of postoperative delirium in cardiac surgery patients.14 However, the definition of depression varies across studies depending on different questionnaires,14 and the pathophysiological link between depression and postoperative delirium is unknown although disturbances in glucocorticoid levels has been suggested as a possible mechanism.34 For example, increased levels of glucocorticoids as well as dysregulation of the hypothalamus-pituitary- adrenal axis may result in structural changes in hippocampus and prefrontal cortex, which could increase the risk of delirium in affected patients.35,36
In our study, we used HADS-D to screen for depression, and a cut-off value of >4 was used in accordance with other studies.25 Significantly more patients with delirium had HADS-D above the cut-off, and HADS-D was independently associated with a higher risk of postoperative delirium in the multivariable analysis. Yet, ROC analysis for HADS-D alone showed an AUC that was lower than MMSE and AQT and too low to be of Clinical value. Preoperative anxiety evaluated with HADS-A has also been associated with postoperative delirium.37 However, the present study found no differences in HADS-A between patients who developed delirium and those who did not.
Longer cardiopulmonary bypass-time was also associated with an increased risk of developing postoperative delirium and it is a known delirium risk factor related to more complex surgery, larger doses of anesthetic drugs and greater volumes of blood transfusion, with increased risk of cerebral hypoperfusion and/or hyperperfusion and systemic inflammatory response.38 Cardiopulmonary bypass-time is correlated to the type of operation,6 where combined valve and CABG surgery often demands longer cardiopulmonary bypass-times. This is also illustrated by the fact that patients undergoing combined surgery in our study more frequently developed postoperative delirium compared to those operated with CABG or valve alone. Our secondary aim was to evaluate a composite of risk factors, involving both cognitive tests and the patients’ mental status, based on previous studies and the idea that both cognitive and psychological factors appear to affect the risk of developing postoperative delirium. By combining MMSE <27 points, AQT color and form >70 seconds, HADS-D >4 points and cardiopulmonary bypass-time, the AUC increased to 0.736, which is a borderline acceptable discriminatory value in clinical practice. Preoperative screening of cognitive function and depression as well as knowledge of the type of operation may thus help identify patients at risk of developing postoperative delirium. Nonetheless, to make preoperative screening more clinically applicable there is a need for further studies to find other tests or test combinations that increase the preoperative predictive accuracy for postoperative delirium.39 It is possible that tests with higher sensitivity for mild cognitive impairment are needed. For example, Montreal Cognitive Assessment (MoCA) in combination with Trial Making Test B may be more suitable for detection of mild cognitive impairment.40,41 Further, frailty is a recognized concept in cardiac surgery, which has been associated with postoperative complications,42,43 and other physiological parameters, such as impaired cerebral autoregulation or cerebrovascular reserve capacity have also been related to an increased risk of postoperative delirium.44,45 Thus, a combination of tests capable of complementing each other may be the best way forward given the multifactorial nature of delirium.
Limitations
Our study had several limitations. There was a potential selection bias regarding the recruitment of patients based on availability of research nurses. Our study was an observational study where patients were recruited consecutively on days when research nurses were working. The Diagnostic and Statistical Manual of Mental Disorders 5th edition (DSM-5) is the gold standard for diagnosing delirium.46 However, in clinical settings delirium is often evaluated with the support of observation and symptom estimation instruments. In this study, preoperative and postoperative performances were compared at two different thoracic surgery centers and patients were assessed for delirium by two different instruments, Nu-DESC or CAM-ICU depending on the participating center. Assessment of interrater reliability was not conducted, and although the sensitivity and specificity of detecting delirium have been reported to be similar between Nu-DESC and CAM-ICU,19 differences in detecting postoperative delirium cannot be excluded. However, in our study the prevalence of postoperative delirium was the same at both participating centers. We did not evaluate the possible contribution of present medications or anesthetics on the risk of developing postoperative delirium, but preoperative and perioperative procedures were standardized according to clinical routine. Our study was conducted in patients undergoing cardiac surgery and our findings may not be generalizable to other types of surgery.
Conclusions
A slower preoperative performance of AQT color and form was associated with a higher risk of developing delirium after cardiac surgery. However, the accuracy of predicting postoperative delirium using AQT was similar to MMSE, and the combination of AQT and MMSE marginally increased the predictive power measured by AUC. A composite of MMSE, AQT, HADS-D and cardiopulmonary bypass time further increased the predictive accuracy to an AUC of 0.736, which is a borderline acceptable discriminatory value in clinical practice. Our results confirm the association of impaired preoperative cognitive function as well as depressive symptoms with postoperative delirium. Yet, further studies are needed to evaluate which tests are most useful in preoperative clinical evaluations to predict postoperative delirium.
Author Contributions
All authors met the following conditions:
1. Made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas.
2. Drafted or wrote, or substantially revised or critically reviewed, the article.
3. Agreed on the journal to which the article was submitted.
4. Reviewed and agreed on all versions of the article before submission, during revision, the final version accepted for publication, and any significant changes introduced at the proofing stage.
5. Agreed to take responsibility and be accountable for the contents of the article.
Funding
This work was supported by grants from the Medical Research Council of Southeast Sweden (FORSS start grant 389071 and grant FORSS 660611) and the Region Kronoberg Research Council (grant 4967). The funders did not have any impact in the design of the study and collection, analysis and interpretation of the data or in writing the manuscript.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Lin Y, Chen J, Wang Z. Meta-analysis of factors which influence delirium following cardiac surgery. J Card Surg. 2012;27(4):481–492.
2. Mangusan RF, Hooper V, Denslow SA, Travis L. Outcomes Associated With Postoperative Delirium After Cardiac Surgery. Am J Critical Care. 2015;24(2):156–163.
3. Kirfel A, Menzenbach J, Guttenthaler V, et al. Postoperative delirium after cardiac surgery of elderly patients as an independent risk factor for prolonged length of stay in intensive care unit and in hospital. Aging Clin Exp Res. 2021;1:43.
4. Burton JK, Craig L, Yong SQ, et al. Non-pharmacological interventions for preventing delirium in hospitalised non-ICU patients. Cochrane Database Syst Rev. 2021;11(11):Cd013307.
5. Cao S-J, Chen D, Yang L, Zhu T. Effects of an abnormal mini-mental state examination score on postoperative outcomes in geriatric surgical patients: a meta-analysis. BMC Anesthesiol. 2019;19(1):74.
6. Veliz-Reissmüller G, Torres HA, van der Linden J, Lindblom D, Jönhagen ME. Pre-operative mild cognitive dysfunction predicts risk for post-operative delirium after elective cardiac surgery. Aging Clin Exp Res. 2007;19(3):172–177.
7. Wu Y, Shi Z, Wang M, et al. Different MMSE Score Is Associated with Postoperative Delirium in Young-Old and Old-Old Adults. PLoS One. 2015;10(10):e0139879.
8. Crum RM, Anthony JC, Bassett SS, Folstein MF. Population-based norms for the Mini-Mental State Examination by age and educational level. JAMA. 1993;269(18):2386–2391.
9. Scazufca M, Almeida OP, Vallada HP, Tasse WA, Menezes PR. Limitations of the Mini-Mental State Examination for screening dementia in a community with low socioeconomic status: results from the Sao Paulo Ageing & Health Study. Eur Arch Psychiatry Clin Neurosci. 2009;259(1):8–15.
10. Pendlebury ST, Cuthbertson FC, Welch SJ, Mehta Z, Rothwell PM. Underestimation of cognitive impairment by Mini-Mental State Examination versus the Montreal Cognitive Assessment in patients with transient ischemic attack and stroke: a population-based study. Stroke. 2010;41(6):1290–1293.
11. Mitchell AJ. A meta-analysis of the accuracy of the mini-mental state examination in the detection of dementia and mild cognitive impairment. J Psychiatr Res. 2009;43(4):411–431.
12. Wiig EH, Nielsen NP, Jacobson JM, Quick A. Test of Cognitive Speed: patterns of age groups 15 to 95 years. Percept Mot Skills. 2007;104(3 Pt 2):1067–1075.
13. Nielsen NP, Wiig EH. Alzheimer’s Quick Test cognitive screening criteria for West African speakers of Krio. Age Ageing. 2006;35(5):503–507.
14. Falk A, Kåhlin J, Nymark C, Hultgren R, Stenman M. Depression as a predictor of postoperative delirium after cardiac surgery: a systematic review and meta-analysis. Interact Cardiovasc Thorac Surg. 2020.
15. Lisspers J, Nygren A. SOderman E; Hospital Anxiety and Depression Scale (HAD): some psychometric data for a Swedish sample. Acta Psychiatr Scand. 1997;96(4):281–286.
16. Gaudreau J-D, Gagnon P, Harel F, Tremblay A, Roy M-A. Fast, Systematic, and Continuous Delirium Assessment in Hospitalized Patients: the Nursing Delirium Screening Scale. J Pain Symptom Manage. 2005;29(4):368–375.
17. Ely EW, Shintani A, Truman B, et al. Delirium as a predictor of mortality in mechanically ventilated patients in the intensive care unit. JAMA. 2004;291(14):1753–1762.
18. Ely EW, Inouye SK, Bernard GR, et al. Delirium in mechanically ventilated patients: validity and reliability of the confusion assessment method for the intensive care unit (CAM-ICU). JAMA. 2001;286(21):2703–2710.
19. Neufeld KJ, Leoutsakos JS, Sieber FE, et al. Evaluation of two delirium screening tools for detecting post-operative delirium in the elderly. Br J Anaesth. 2013;111(4):612–618.
20. Luetz A, Heymann A, Radtke FM, et al. Different assessment tools for intensive care unit delirium: which score to use? Crit Care Med. 2010;38(2):409–418.
21. Gusmao-Flores D, Salluh JI, Chalhub R, Quarantini LC. The confusion assessment method for the intensive care unit (CAM-ICU) and intensive care delirium screening checklist (ICDSC) for the diagnosis of delirium: a systematic review and meta-analysis of clinical studies. Critical Care. 2012;16(4):R115.
22. Kvitting AS, Fällman K, Wressle E, Age-Normative MJ. MMSE Data for Older Persons Aged 85 to 93 in a Longitudinal Swedish Cohort. J Am Geriatr Soc. 2019;67(3):534–538.
23. Nielsen NP, Wiig EH, Warkentin S, Minthon L. Clinical utility of color-form naming in Alzheimer’s disease: preliminary evidence. Percept Mot Skills. 2004;99(3 Pt 2):1201–1204.
24. Zigmond AS, Snaith RP. The Hospital Anxiety and Depression Scale. Acta Psychiatr Scand. 1983;67(6):361–370.
25. Kjærgaard M, Arfwedson Wang CE, Waterloo K, Jorde R. A study of the psychometric properties of the Beck Depression Inventory-II, the Montgomery and Åsberg Depression Rating Scale, and the Hospital Anxiety and Depression Scale in a sample from a healthy population. Scand J Psychol. 2014;55(1):83–89.
26. Xu C. EuroQol - a new facility for the measurement of health-related quality of life. Health Policy (New York). 1990;16(3):199–208.
27. Wittrup-Jensen KU, Lauridsen J, Gudex C, Pedersen KM. Generation of a Danish TTO value set for EQ-5D health states. Scand J Public Health. 2009;37(5):459–466.
28. Mandrekar JN. Receiver operating characteristic curve in diagnostic test assessment. J Thoracic Oncol. 2010;5(9):1315–1316.
29. Janssen TL, Alberts AR, Hooft L, Mattace-Raso F, Mosk CA, van der Laan L. Prevention of postoperative delirium in elderly patients planned for elective surgery: systematic review and meta-analysis. Clin Interv Aging. 2019;14:1095–1117.
30. Wang S, Hanneman P, Xu C, et al. Critical Care Recovery Center: a model of agile implementation in intensive care unit (ICU) survivors. Int Psychogeriatrics. 2019;32(12):1409–1418.
31. Franco-Marina F, García-González JJ, Wagner-Echeagaray F, et al. The Mini-mental State Examination revisited: ceiling and floor effects after score adjustment for educational level in an aging Mexican population. Int Psychogeriatrics. 2010;22(1):72–81.
32. Trzepacz PT, Hochstetler H, Wang S, Walker B, Saykin AJ. Alzheimer’s Disease Neuroimaging I. Relationship between the Montreal Cognitive Assessment and Mini-mental State Examination for assessment of mild cognitive impairment in older adults. BMC Geriatr. 2015;15:107.
33. Itagaki A, Sakurada K, Matsuhama M, Yajima J, Yamashita T, Kohzuki M. Impact of frailty and mild cognitive impairment on delirium after cardiac surgery in older patients. J Cardiol. 2020;76(2):147–153.
34. Elsamadicy AA, Adogwa O, Lydon E, et al. Depression as an independent predictor of postoperative delirium in spine deformity patients undergoing elective spine surgery. J Neurosurgery. 2017;27(2):209.
35. Ekstrand J, Hellsten J, Tingström A. Environmental enrichment, exercise and corticosterone affect endothelial cell proliferation in adult rat hippocampus and prefrontal cortex. Neurosci Lett. 2008;442(3):203–207.
36. Murray F, Smith DW, Hutson PH. Chronic low dose corticosterone exposure decreased hippocampal cell proliferation, volume and induced anxiety and depression like behaviours in mice. Eur J Pharmacol. 2008;583(1):115–127.
37. Ren A, Zhang N, Zhu H, Zhou K, Cao Y, Liu J. Effects of Preoperative Anxiety on Postoperative Delirium in Elderly Patients Undergoing Elective Orthopedic Surgery: a Prospective Observational Cohort Study. Clin Interv Aging. 2021;16:549–557.
38. Zhang WY, Wu WI, Gu JJ, et al. Risk factors for postoperative delirium in patients after coronary artery bypass grafting: a prospective cohort study. J Crit Care. 2015;30(3):606–612.
39. Rao A, Shi SM, Afilalo J, et al. Physical Performance and Risk of Postoperative Delirium in Older Adults Undergoing Aortic Valve Replacement. Clin Interv Aging. 2020;15:1471–1479.
40. Ciesielska N, Sokołowski R, Mazur E, Podhorecka M, Polak-Szabela A, Kędziora-Kornatowska K. Is the Montreal Cognitive Assessment (MoCA) test better suited than the Mini-Mental State Examination (MMSE) in mild cognitive impairment (MCI) detection among people aged over 60? Meta-analysis. Psychiatr Pol. 2016;50(5):1039–1052.
41. McAlister C, Schmitter-Edgecombe M, Lamb R. Examination of Variables That May Affect the Relationship Between Cognition and Functional Status in Individuals with Mild Cognitive Impairment: a Meta-Analysis. Arch clin neuropsychol. 2016;31(2):123–147.
42. Gracie TJ, Caufield-Noll C, Wang NY, Sieber FE. The Association of Preoperative Frailty and Postoperative Delirium: a Meta-analysis. Anesth Analg. 2021;133(2):314–323.
43. Afilalo J, Mottillo S, Eisenberg MJ, et al. Addition of Frailty and Disability to Cardiac Surgery Risk Scores Identifies Elderly Patients at High Risk of Mortality or Major Morbidity. Circ Cardiovasc Qual Outcomes. 2012;5(2):222–228.
44. Caldas JR, Panerai RB, Bor-Seng-Shu E, et al. Dynamic cerebral autoregulation: a marker of post-operative delirium? Clin Neurophysiol. 2019;130(1):101–108.
45. Bydén M, Segernäs A, Thulesius H, et al. Cerebrovascular Reserve Capacity as a Predictor of Postoperative Delirium: a Pilot Study. Front Surg. 2021;8:658849.
46. European Delirium A, American Delirium S. The DSM-5 criteria, level of arousal and delirium diagnosis: inclusiveness is safer. BMC Med. 2014;12(1):141.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.