Back to Journals » Clinical Ophthalmology » Volume 17
Predicting Prognosis Based on Regional Prevalence, Ulcer Morphology and Treatment Strategy in Vision-Threatening Pythium insidiosum Keratitis
Received 13 March 2023
Accepted for publication 24 April 2023
Published 5 May 2023 Volume 2023:17 Pages 1307—1314
DOI https://doi.org/10.2147/OPTH.S412274
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Bharat Gurnani,1 Kirandeep Kaur2
1Department of Cornea and Refractive Surgery, Sadguru Netra Chikitsalya, Shri Sadguru Seva Sangh Trust, Chitrakoot, Madhya Pradesh, 485334, India; 2Department of Pediatric Ophthalmology, Sadguru Netra Chikitsalya, Shri Sadguru Seva Sangh Trust, Chitrakoot, Madhya Pradesh, 485334, India
Correspondence: Bharat Gurnani, Department of Cornea and Refractive Surgery, Sadguru Netra Chikitsalya, Shri Sadguru Seva Sangh Trust, Janaki-kund, Chitrakoot, Madhya Pradesh, 485334, India, Tel +91 9080523059, Email [email protected]
Abstract: Pythium insidiosum is an oomycete belonging to the phylum Straminipila and family Pythiaceae. It causes rapidly progressive vision-threatening keratitis. Clinically, microbiologically and morphologically, it closely resembles fungal keratitis; hence it is also labelled as a “parafungus”. The clinical features mimicking fungus are subepithelial and stromal infiltrate, endo-exudates, corneal melt and hypopyon. The hallmark features of Pythium are tentacular projections, reticular dot-like infiltrate, peripheral furrowing and thinning, and rapid limbal spread. Microbiological corneal smearing on KOH and Gram stain reveal septate or aseptate, obtuse to perpendicular hyphae which mimic fungal hyphae. Culture on any nutritional agar reveals cream, cottonwool-like, fluffy colonies, and diagnosis is confirmed by zoospore formation by the leaf incarnation method. Medical management with antifungals and antibacterials still presents a dilemma. Early therapeutic keratoplasty has been the proposed treatment in most cases. We hypothesize that the prognosis of Pythium keratitis is governed by regional geographical variations, ulcer size and density on presentation, and initial treatment strategy. The available literature supporting the proposed hypothesis is also discussed, along with the hallmark features of Pythium and how it masquerades as other microorganisms causing keratitis. We also aim to propose a novel diagnostic and treatment algorithm for managing this vision-threatening keratitis.
Keywords: Pythium insidiosum, keratitis, parafungus, hyphae, zoospore parafungus
Introduction
Pythium insidiosum is an oomycete residing in aquatic bodies, with a higher prevalence in tropical and subtropical regions of the world.1 It belongs to the kingdom Straminipila, class Oomycete, phylum Oomycota and family Pythiaceae.2 It causes sight-threatening keratitis and the clinical picture closely mimics fungal keratitis. Hence, it is also called a “parafungus”.3 Morphologically, it mimics fungus owing to its zygomycetous branching, but lacks ergosterol in the cell wall.4 Hasika et al reported a prevalence of 5.9% in their retrospective analysis.5 The first case of systemic pythiosis was reported in Thailand in 1884 and the first case of keratitis was reported in 1988; since then, there have been numerous reports from all over the world.6 More recently, Pythium keratitis has gained widespread importance because of the high virulence of the microorganism, lack of standard diagnostic modalities, delay in diagnosis and treatment, and high recurrence rate.7 The common clinical features mimicking fungal keratitis are epithelial breach, subepithelial infiltrate, cottonwool-like stromal infiltrate, endothelial exudates, satellite lesions, descemetocele, ring infiltrates, anterior chamber hypopyon, corneal thinning, melt and perforation.8 The classical hallmark features of Pythium are reticular dots, tentacles, hyphated edges, peripheral furrowing and early limbal spread (Figures 1a, 1b, 2a, and b).9 The laboratory diagnosis is made by microbiological smearing and culture on nutritional agar and zoospore identification by the leaf incarnation method.10 The time-tested recommended treatment modalities are antifungals (5% natamycin, 1% itraconazole and 1% voriconazole),5 antibacterials (0.2% linezolid, 1% azithromycin, 4% minocycline and 1% tigecycline)11 and therapeutic keratoplasty.5 However, the treatment protocols vary from centre to centre, and specific antimicrobial therapy remains undetermined. Today, P. insidiosum diagnosis and treatment still pose challenges to the clinician since the clinical, morphological and microbiological characteristics of Pythium closely resemble those of fungal keratitis. To safeguard the patients from this vision-threatening entity, we hypothesize that the prognosis of P. insidiosum keratitis is dependent upon the regional prevalence of the species, the corneal infiltrate size, location and density at presentation, and initial treatment strategy. We also discuss the hallmark slit-lamp clinical features of Pythium and list the clinical features masquerading as other species causing keratitis. Moreover, we propose a novel diagnostic and treatment algorithm for managing this vision-threatening keratitis.
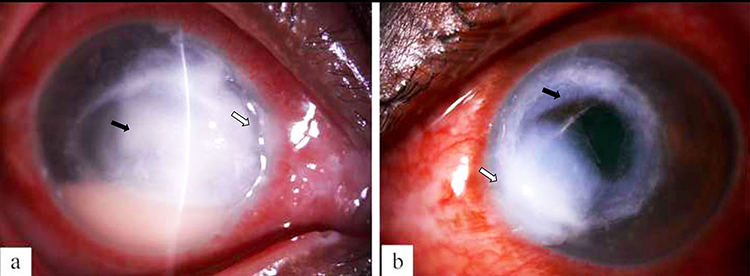 |
Figure 1 (a) Digital slit-lamp image of the right eye of the patient depicting diffuse conjunctival congestion, 8×8 mm creamy white full-thickness infiltrate (black arrowhead), stromal melt and nasal peripheral furrowing (white arrowhead) with guttering along with 3 mm anterior chamber hypopyon (severe ulcer). (b) Digital slit-lamp image of the right eye of the patient depicting diffuse conjunctival congestion, crescentic eccentric 7×7 mm mid to posterior stromal infiltrate (black arrowhead), inferonasal full-thickness infiltrate, nasal limbal spread (white arrowhead), and central corneal thinning with impending perforation (severe ulcer). |
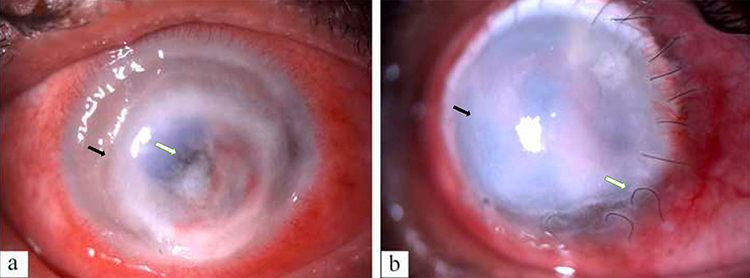 |
Figure 2 (a) Digital slit-lamp image of the patient depicting diffuse conjunctival congestion, superficial vascularization, total full-thickness corneal infiltrate with 360-degree limbal infiltrate and paralimbal thinning (black arrowhead) with central impending perforation (white arrowhead) (severe ulcer). (b) Digital slit-lamp image of the patient depicting diffuse conjunctival congestion, total graft infiltrate (black arrowhead), graft host junction melt from 1 to 7 o’clock (white arrowhead) and loose sutures along with superficial vascularization. |
Hypothesis
The first report of systemic pythiosis came in 1884, when it was described in British horses.1 The first reports of ocular pythiosis came from Thailand in 1988, in a thalassaemic patient with cutaneous blisters,12 then, in 1989, five cases of Thai thalassaemia with cutaneous blisters were reported.13 Human pythiosis has been classified as vascular, ocular, dermatological and disseminated.14 In Thailand, the most common form is vascular, followed by ocular pythiosis. However, in India and other parts of the world, isolated ocular involvement is the most common. The majority of case reports and studies from Thailand had poor prognosis, probably because of systemic involvement along with ocular involvement, and the high regional virulence of the species due to geographical variations.15 However, in India and other countries, the prognosis is better, probably as a result of better systemic immunity and targeted ocular treatment. After Thailand, most cases have been reported from India16,17 and China.18 There have been case reports of Pythium keratitis from Australia,19 New Zealand,20 Canada,21 Israel22 and Japan,23 but the reported numbers are lower, probably because of the lower regional prevalence and the majority of cases being misdiagnosed as fungal keratitis.
Based on our day-to-day clinical experience, we hypothesize that Pythium keratitis prognosis is also governed by the infiltrate size, density and location. We believe that, clinically, the Jones criteria for microbial keratitis are also valid for Pythium keratitis. Ulcer size greater than 4×4 mm, mid to posterior stromal involvement and ulcers involving the visual axis have poor outcome and prognosis.24 Apart from these criteria, the presence of hallmark clinical features, such as early limbal spread, peripheral guttering, furrowing and tentacular projections, provides an indicator of the severity and virulence of microorganisms and usually has poorer visual outcome. We hypothesize modified Jones criteria for Pythium in Table 1.1,3,5,11 The various proposed treatment strategies for Pythium are antifungals,5 antibacterials,11 therapeutic keratoplasty,5 cryotherapy with ethanol to the host bed,25 cyanoacrylate glue with bandage contact lens,17 enucleation and evisceration.9 Before 2010, less was known about the morphology, pathophysiology and virulence of Pythium, and it was labelled as a fungus.26 Hence, the targeted treatment was antifungals (5% natamycin, 1% itraconazole and 1% voriconazole) and in non-resolving cases therapeutic keratoplasty and enucleation. Most studies quoted enucleation as the sole treatment for Pythium.27 In a landmark clinical trial, Bagga et al,11 based on their disc diffusion assay results, proved that antibiotics such as linezolid and azithromycin have higher efficacy and more favourable outcomes in Pythium cases compared to antifungals. The literature review revealed better visual outcomes and lower enucleation rates for Pythium cases after 20158, as a result of the growing use of antibacterials over antifungals.17,28 Adjunctive treatments, such as cyanoacrylate glue with bandage contact lens17 for stromal melt cases and cryotherapy with ethanol,25 have shown benefits but are still experimental. We propose that antibacterials should be the first line drugs in culture-proven Pythium cases and that antifungals still have a role to play if the diagnosis is delayed.
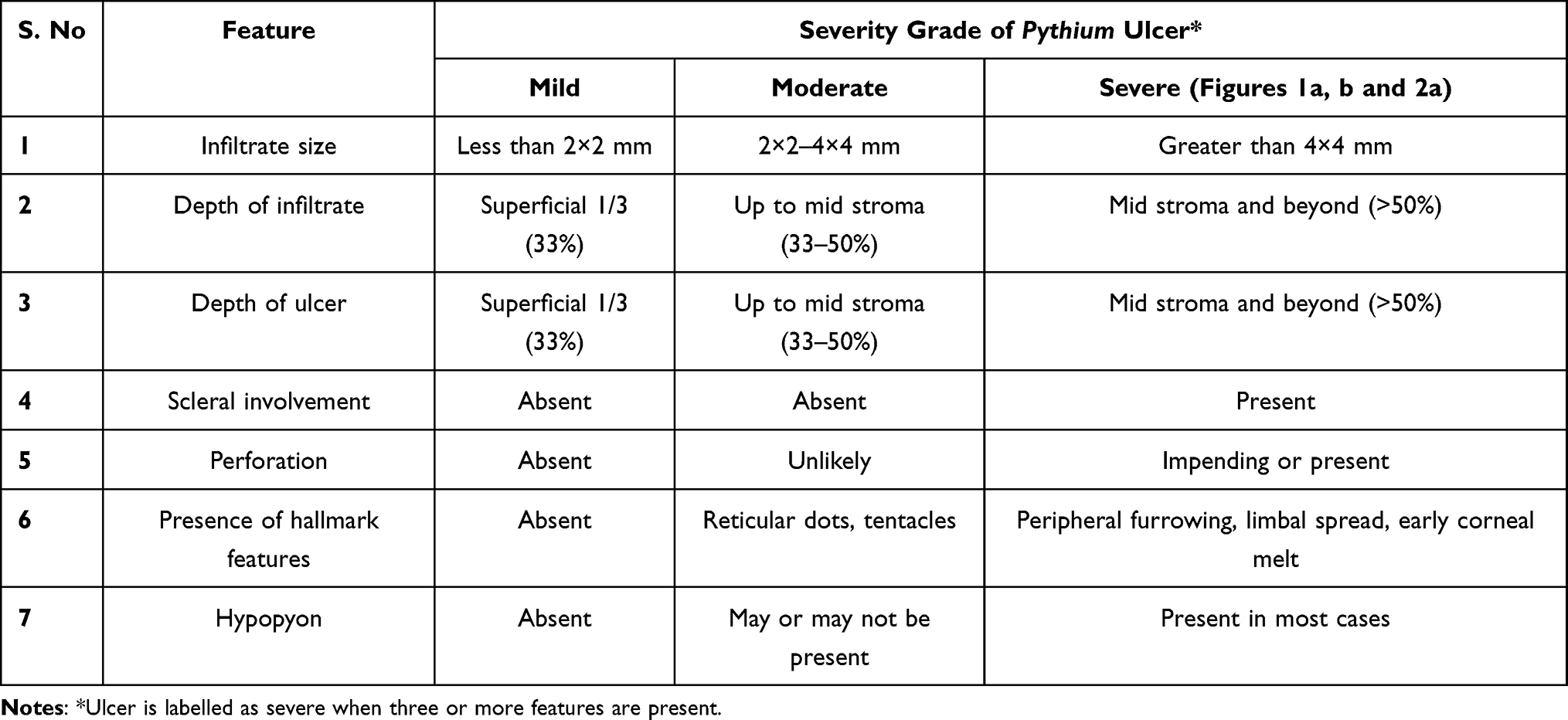 |
Table 1 Proposed Modified Jones Criteria for Pythium insidiosum Keratitis (Gurnani and Kaur Severity Grading of Pythium insidiosum Keratitis)3,5,11 |
From the detailed literature review and our day-to-day clinical experience, we hypothesize that the prognosis of this vision-threatening keratitis is governed by regional prevalence, the infiltrate size, density and location at presentation, and initial medical management. Although many clinical studies have been published on this entity, none has embarked on determining the factors governing the prognosis of these cases. We have detailed the supportive literature while evaluating the hypothesis. We have also added the hallmark clinical features of Pythium to facilitate diagnosis, and compared it with its masquerading counterparts. Moreover, we propose a novel management protocol for managing these cases, which is a potential addition to the existing literature.
Evaluation of the Hypothesis
We need to determine whether prognosis is governed by regional prevalence, ulcer morphology and treatment strategy. Kunavisarut et al,27 in their retrospective analysis of 10 patients from Ramathibodi Hospital, Thailand, in 1988–1998, showed that seven out of eight patients underwent enucleation or evisceration and two were lost to follow-up. They highlighted that neither antibiotics nor antifungals were able to curb the infection. Thanathanee et al,29 in their case series of four patients from Thailand, showed that antifungals were ineffective; all patients underwent therapeutic keratoplasty and one patient needed evisceration. All of the eyes had a poor outcome. An analysis by Puangsricharern et al in 2021,9 of 26 eyes from Thailand, reported a 57.5% enucleation rate, and the majority of eyes had poor anatomical and functional outcome. He et al30 reported a case of Pythium in a 7-year-old from China. The child was managed with therapeutic keratoplasty with recurrent graft infection. The globe was salvaged but the patient had a poor visual outcome. Gurnani et al,3 in their retrospective analysis of 30 patients from India, showed that 23.3% improved with conservative management and achieved a globe salvage rate of 90%. There were no cases of enucleation or evisceration. Maeno et al23 successfully managed a 20-year-old man from Japan with triple drug therapy of minocycline, linezolid and chloramphenicol. His visual acuity improved from 20/2000 to 20/25. Similarly, Ramappa et al31 reported successful management of presumptive Pythium keratitis with antibacterials alone in a 42-year-old woman after 3 weeks of intensive therapy. Thus, it can inferred that the prognosis of Pythium keratitis cases from Thailand,32 China,18 Israel22 and Australia19 is worse than that of those from India,3 probably due to differences in the regional prevalence and virulence of the species. Ahirwar et al assessed the safety and efficacy of three antibiotics – 0.2% linezolid, 1% azithromycin and 1% tigecycline – in their in vitro rabbit model. Corneal infection was induced by injecting Pythium zoospore in rabbit eyes, and the response to all three drugs was assessed. The success rate was 16.7% with azithromycin, 25% with tigecycline and 50% with linezolid. Hence, linezolid showed superior efficacy and safety, and the authors proposed that this should be considered as the first line drug for vision-threatening Pythium keratitis.28 In another report, Thanathanee et al assessed the role of immunotherapy in Pythium keratitis. They injected three doses of Pythium insidiosum antigen immunotherapy (PIAI) at 3-week intervals in 10 eyes of 10 patients. Out of the 10 eyes, one eye underwent enucleation and only three eyes could be saved after therapeutic keratoplasty. Hence, they concluded that PIAI did not show any efficacy in the treatment of Pythium keratitis.33
Based on the Jones criteria,34 it has been well proven that large ulcer size, visual axis involvement, mid to posterior stromal infiltrate, endo-exudates, corneal perforation, early limbal spread, scleritis and endophthalmitis are poor prognostic factors. Agarwal et al,35 in their retrospective analysis of 10 patients, noted recurrence in seven patients, and all of the eyes had a failed graft. Two eyes underwent evisceration. All of the eyes had a central full-thickness infiltrate involving the visual axis. The two eyes that did not show any recurrence had smaller ulcers, measuring less than 3×3 mm. Hasika et al,5 in their retrospective analysis of 71 patients, demonstrated that patients with larger ulcer size and classical features of Pythium required surgical treatment and the prognosis was guarded in most of the cases. Tentacle-like infiltrates were seen in 36, dot infiltrates in 15, peripheral furrowing in nine, perforation in five and total corneal ulcer in six. Only three patients showed improvement with medical management. Puangsricharern et al,9 in their analysis of 26 patients, showed that 57.7% underwent globe removal. They concluded that the globe removal group patients were older, with a maximum infiltrate area of ≥6 mm, and showed satellite lesions, multifocal infiltrates and hypopyon. Pythium hyphae were denser on histopathological analysis. Hence, ulcer morphology has a key role to play in determining the final visual outcome and prognosis (Figure 1a and b).
Analysing the treatment strategy, Hou et al,18 in their case series of three patients, showed that after initial treatment with antifungals the ulcers worsened and all patients underwent therapeutic keratoplasty. Later, enucleation was performed, the patients were treated antibacterials and the infection resolved. Gurnani et al,3 in their analysis of 30 patients, emphasized that antifungals should be initiated before the culture results are known, and antibacterials should be initiated once culture positivity of Pythium has been confirmed. A total of 23.3% improved with medical treatment and 63.3% improved with surgical treatment. They had a globe salvage rate of 90%. Vishwakarma et al24 also emphasized antibacterial treatment for Pythium keratitis, and out of their 18 patients only three underwent evisceration. Hasika et al5 managed all of their 71 patients with antifungals and therapeutic keratoplasty, and none of the patients had a clear graft 1 month postoperatively. The prognosis was guarded in the majority of cases. Bagga et al,11 in their landmark randomized trial, showed that antibacterials have a higher efficacy than antifungals. Gurnani et al17 successfully managed a 9-year-old paediatric patient with cyanoacrylate glue, topical linezolid and azithromycin, thus, again, emphasizing the role of antibacterials in the treatment of Pythium keratitis. They also highlighted that cyanoacrylate glue has antibacterial properties, which can have an additive synergistic effect with linezolid and azithromycin. Hence, this detailed and comprehensive literature review reveals that Pythium keratitis prognosis is governed by the above-mentioned factors. Prompt diagnosis and targeted treatment can salvage these eyes. Taking a leap forward, we have enlisted various hallmark clinical features of Pythium keratitis along with its masqueraders, and we have also proposed a diagnostic and management protocol which all ophthalmologists, at a global level, can follow to safeguard the anatomical and functional outcomes in these cases.
Hallmark Clinical Features and Masqueraders
The diagnosis of Pythium keratitis requires a high index of clinical suspicion, and the treating ophthalmologists and cornea specialists must be aware of the hallmark features of Pythium as well the clinical features that masquerade as other microorganisms. Table 2 gives a comprehensive overview of the clinical features of P. insidiosum keratitis.3,5,11,24,31,36,37
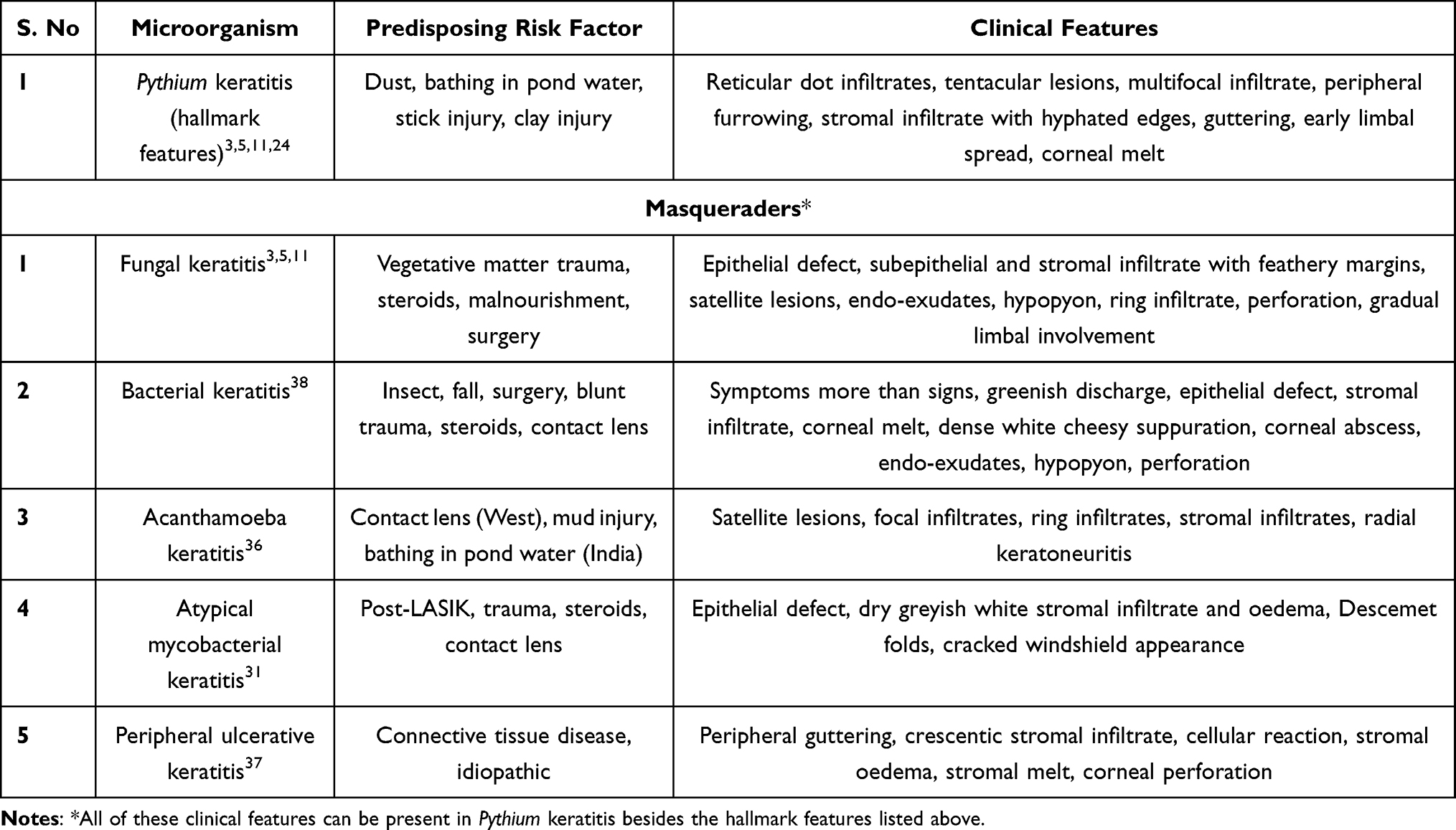 |
Table 2 Hallmark Clinical Features of Pythium insidiosum Keratitis and Its Masqueraders |
Management Protocol for Pythium insidiosum Keratitis
The diagnosis and treatment strategy for P. insidiosum keratitis has always been a challenge for treating ophthalmologists. Today, there is still a lack of clarity and consensus on the diagnosis and treatment strategy and there are no defined guidelines for this. On corneal scraping, Pythium mimics fungal filaments; hence, whether to initiate antifungals or antibacterials remains a question. Antibacterials have shown better outcomes in culture-proven cases. Non-resolving cases (Figure 2a) require a therapeutic keratoplasty with 1 mm margin clearance, in contrast to usual fungal keratitis cases with 0.5 mm margin clearance. Recurrent graft infection will require repeat therapeutic keratoplasty (Figure 2b) and tarsorrhaphy, early stromal melt cases with require cyanoacrylate glue and bandage contact lens, and endophthalmitis and pan-ophthalmitis will require enucleation. Here, we propose a diagnostic and treatment algorithm for the diagnosis and treatment of P. insidiosum keratitis, which is an add-on to the existing literature and which, to the best of our knowledge, has not been described previously (Figure 3).3,5,8,11,24,25,35
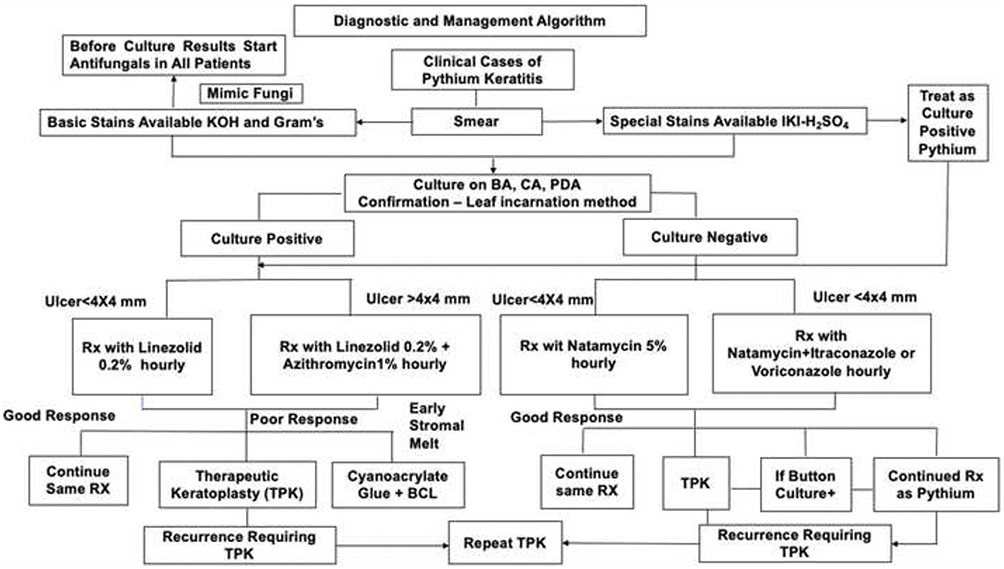 |
Figure 3 The novel diagnostic and management protocol of Pythium insidiosum keratitis. Abbreviations: KOH, potassium hydroxide; IKI-H2SO4, iodine potassium iodide–sulfuric acid; BA, blood agar; CA, chocolate agar; PDA, potato dextrose agar; RX, treatment; TPK, therapeutic keratoplasty. |
Consequences of the Hypothesis and Discussion
Pythium insidiosum keratitis has always presented a diagnostic and treatment dilemma for clinicians.37 The presence of hallmark features should alert the treating ophthalmologist to the possibility of Pythium keratitis.3 Masqueraders should be kept in mind while managing this devastating corneal infection. Antibacterials have shown more promise than antifungals.11 Early therapeutic keratoplasty with a margin clearance of 1 mm is the gold-standard treatment in rapidly proliferating cases.5 The proposed algorithm will assist in the management of these cases, with good anatomical and functional outcomes.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Gaastra W, Lipman LJ, De Cock AW, et al. Pythium insidiosum: an overview. Vet Microbiol. 2010;146(1–2):1–16. doi:10.1016/j.vetmic.2010.07.019
2. Nam B, Choi YJ. Phytopythium and Pythium species (Oomycota) isolated from freshwater environments of Korea. Mycobiology. 2019;47(3):261–272. doi:10.1080/12298093.2019.1625174
3. Gurnani B, Christy J, Narayana S, Rajkumar P, Kaur K, Gubert J. Retrospective multifactorial analysis of Pythium keratitis and review of literature. Indian J Ophthalmol. 2021;69(5):1095–1101. doi:10.4103/ijo.IJO_1808_20
4. Gurnani B, Kaur K. Pythium Keratitis. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2022.
5. Hasika R, Lalitha P, Radhakrishnan N, Rameshkumar G, Prajna NV, Srinivasan M. Pythium keratitis in South India: incidence, clinical profile, management, and treatment recommendation. Indian J Ophthalmol. 2019;67(1):42–47. doi:10.4103/ijo.IJO_445_18
6. Thianprasit M, Chaiprasert A, Imwidthaya P. Human pythiosis. Curr Top Med Mycol. 1996;7(1):43–54.
7. Chitasombat MN, Jongkhajornpong P, Lekhanont K, Krajaejun T. Recent update in diagnosis and treatment of human pythiosis. Peer J. 2020;8:e8555. doi:10.7717/peerj.8555
8. Agarwal S, Iyer G, Srinivasan B, et al. Clinical profile, risk factors and outcome of medical, surgical and adjunct interventions in patients with Pythiuminsidiosum keratitis. Br J Ophthalmol. 2019;103(3):296–300. doi:10.1136/bjophthalmol-2017-311804
9. Puangsricharern V, Chotikkakamthorn P, Tulvatana W, et al. Clinical characteristics, histopathology, and treatment outcomes of pythium keratitis: a retrospective cohort study. Clin Ophthalmol. 2021;15:1691–1701. doi:10.2147/OPTH.S303721
10. Mittal R, Jena SK, Desai A, Agarwal S. Pythium insidiosum keratitis: histopathology and rapid novel diagnostic staining technique. Cornea. 2017;36(9):1124–1132. doi:10.1097/ICO.0000000000001244
11. Bagga B, Sharma S, Madhuri Guda SJ, et al. Leap forward in the treatment of Pythium insidiosum keratitis. Br J Ophthalmol. 2018;102(12):1629–1633. doi:10.1136/bjophthalmol-2017-311360
12. Permpalung N, Worasilchai N, Chindamporn A. Human pythiosis: emergence of fungal-like organism. Mycopathologia. 2020;185(5):801–812. doi:10.1007/s11046-019-00412-0
13. Sathapatayavongs B, Leelachaikul P, Prachaktam R, et al. Human pythiosis associated with thalassemia hemoglobinopathy syndrome. J Infect Dis. 1989;159(2):274–280. doi:10.1093/infdis/159.2.274
14. Krajaejun T, Sathapatayavongs B, Pracharktam R, et al. Clinical and epidemiological analyses of human pythiosis in Thailand. Clin Infect Dis. 2006;43(5):569–576. doi:10.1086/506353
15. Permpalung N, Worasilchai N, Plongla R, et al. Treatment outcomes of surgery, antifungal therapy and immunotherapy in ocular and vascular human pythiosis: a retrospective study of 18 patients. J Antimicrob Chemother. 2015;70(6):1885–1892. doi:10.1093/jac/dkv008
16. Sane SS, Madduri B, Mohan N, Mittal R, Raghava JV, Fernandes M. Improved outcome of pythium keratitis with a combined triple drug regimen of linezolid and azithromycin. Cornea. 2021;40(7):888–893. doi:10.1097/ICO.0000000000002503
17. Gurnani B, Narayana S, Christy J, Rajkumar P, Kaur K, Gubert J. Successful management of pediatric pythium insidiosum keratitis with cyanoacrylate glue, linezolid, and azithromycin: rare case report. Eur J Ophthalmol. 2022;32(5):NP87–NP91. doi:10.1177/11206721211006564
18. Hou H, Wang Y, Tian L, Wang F, Sun Z, Chen Z. Pythium insidiosum keratitis reported in China, raising the alertness to this fungus-like infection: a case series. J Med Case Rep. 2021;15(1):619. doi:10.1186/s13256-021-03189-3
19. Badenoch PR, Mills RA, Chang JH, Sadlon TA, Klebe S, Coster DJ. Pythium insidiosum keratitis in an Australian child. Clin Exp Ophthalmol. 2009;37(8):806–809. doi:10.1111/j.1442-9071.2009.02135.x
20. Murdoch D, Parr D. Pythium insidiosum keratitis. Aust NZ J Ophthalmol. 1997;25(2):177–179. doi:10.1111/j.1442-9071.1997.tb01304.x
21. Gurnani B, Kaur K, Agarwal S, et al. Pythium insidiosum Keratitis: past, Present, and Future. Ophthalmol Ther. 2022;11(5):1629–1653. doi:10.1007/s40123-022-00542-7
22. Tanhehco TY, Stacy RC, Mendoza L, Durand ML, Jakobiec FA, Colby KA. Pythium insidiosum keratitis in Israel. Eye Contact Lens. 2011;37(2):96–98. doi:10.1097/ICL.0b013e3182043114
23. Maeno S, Oie Y, Sunada A, et al. Successful medical management of Pythium insidiosum keratitis using a combination of minocycline, linezolid, and chloramphenicol. Am J Ophthalmol Case Rep. 2019;15:100498. doi:10.1016/j.ajoc.2019.100498
24. Vishwakarma P, Mohanty A, Kaur A, et al. Pythium keratitis: clinical profile, laboratory diagnosis, treatment, and histopathology features post-treatment at a tertiary eye care center in Eastern India. Indian J Ophthalmol. 2021;69(6):1544–1552. doi:10.4103/ijo.IJO_2356_20
25. Agarwal S, Srinivasan B, Janakiraman N, et al. Role of topical ethanol in the treatment of pythium insidiosum keratitis-A proof of concept. Cornea. 2020;39(9):1102–1107. doi:10.1097/ICO.0000000000002370
26. Kwon-Chung KJ. Phylogenetic spectrum of fungi that are pathogenic to humans. Clin Infect Dis. 1994;19(Suppl 1):S1–S7. doi:10.1093/clinids/19.supplement_1.s1
27. Kunavisarut S, Nimvorapan T, Methasiri S. Pythium corneal ulcer in Ramathibodi Hospital. J Med Assoc Thai. 2003;86(4):338–342.
28. Ahirwar LK, Kalra P, Sharma S, et al. Linezolid shows high safety and efficacy in the treatment of Pythium insidiosum keratitis in a rabbit model. Exp Eye Res. 2021;202:108345. doi:10.1016/j.exer.2020.108345
29. Thanathanee O, Enkvetchakul O, Rangsin R, Waraasawapati S, Samerpitak K, Suwan-apichon O. Outbreak of Pythium keratitis during rainy season: a case series. Cornea. 2013;32(2):199–204. doi:10.1097/ICO.0b013e3182535841
30. He H, Liu H, Chen X, Wu J, He M, Zhong X. Diagnosis and treatment of pythium insidiosum corneal ulcer in a Chinese child: a case report and literature review. Am J Case Rep. 2016;17:982–988. doi:10.12659/ajcr.901158
31. Ramappa M, Nagpal R, Sharma S, Chaurasia S. Successful medical management of presumptive pythium insidiosum keratitis. Cornea. 2017;36(4):511–514. doi:10.1097/ICO.0000000000001162
32. Nonpassopon M, Jongkhajornpong P, Aroonroch R, Koovisitsopit A, Lekhanont K. Predisposing factors, clinical presentations, and outcomes of contact lens-related pythium keratitis. Cornea. 2021;40(11):1413–1419. doi:10.1097/ICO.0000000000002651
33. Thanathanee O, Bhoomibunchoo C, Anutarapongpan O, Suwan-Apichon O, Charoensuk K, Chindamporn A. Role of Immunotherapy in Pythium insidiosum Keratitis. Am J Trop Med Hyg. 2022;107(1):110–112. doi:10.4269/ajtmh.22-0015
34. Jones DB. Decision-making in the management of microbial keratitis. Ophthalmology. 1981;88(8):814–820. doi:10.1016/s0161-6420(81)34943-4
35. Agarwal S, Iyer G, Srinivasan B, Agarwal M, Panchalam Sampath Kumar S, Therese LK. Clinical profile of pythium keratitis: perioperative measures to reduce risk of recurrence. Br J Ophthalmol. 2018;102(2):153–157. doi:10.1136/bjophthalmol-2017-310604
36. Raghavan A, Bellamkonda P, Mendoza L, Rammohan R. Pythium insidiosum and Acanthamoeba keratitis in a contact lens user. BMJ Case Rep. 2018;11(1):bcr2018226386. doi:10.1136/bcr-2018-226386
37. Kate A, Bagga B, Ahirwar LK, Mishra DK, Sharma S. Unusual presentation of Pythium keratitis as peripheral ulcerative keratitis: clinical dilemma. Ocul Immunol Inflamm. 2022;30(7–8):2023–2026. doi:10.1080/09273948.2021.1952276
38. Lelievre L, Borderie V, Garcia-Hermoso D, et al. Imported Pythium insidiosum keratitis after a swim in Thailand by a contact lens-wearing traveler. Am J Trop Med Hyg. 2015;92(2):270–273. doi:10.4269/ajtmh.14-0380
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Breaking-Down Barriers: Proposal of Using Cellulose Biosynthesis Inhibitors and Cellulase Enzyme as a Novel Treatment Modality for Vision Threatening Pythium Insidiosum Keratitis
Gurnani B, Natarajan R, Mohan M, Kaur K
Clinical Ophthalmology 2024, 18:765-776
Published Date: 11 March 2024
Immune Camouflage in Pythium insidiosum Keratitis: A Hypothesis on Molecular Mimicry and Host Pattern Recognition Receptor Evasion
Gurnani B, Kaur K
Clinical Ophthalmology 2025, 19:4855-4873
Published Date: 19 December 2025