Back to Journals » Cancer Management and Research » Volume 13
Predicting Malignancy of Biliary Stricture with a Nomogram in Patients with a Non-Malignant Endoscopic Tissue Diagnosis: A Retrospective Study
Authors Zhang Y ![]() , Jiang Q, Wang Q, Feng Y, Wu D, Guo T, Zhang S, Chen X
, Jiang Q, Wang Q, Feng Y, Wu D, Guo T, Zhang S, Chen X ![]() , Yang Y, Shi W, Wu X, Yang A
, Yang Y, Shi W, Wu X, Yang A
Received 12 August 2021
Accepted for publication 20 September 2021
Published 11 October 2021 Volume 2021:13 Pages 7735—7745
DOI https://doi.org/10.2147/CMAR.S333333
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Chien-Feng Li
Yizhen Zhang,1 Qingwei Jiang,1 Qiang Wang,1 Yunlu Feng,1 Dongsheng Wu,1 Tao Guo,1 Shengyu Zhang,1 Xi Chen,2 Yingyun Yang,1 Wen Shi,1 Xi Wu,1 Aiming Yang1
1Department of Gastroenterology, Peking Union Medical College Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, People’s Republic of China; 2Department of Gastroenterology, Yihe Hospital, Zhengzhou, Henan Province, People’s Republic of China
Correspondence: Xi Wu; Aiming Yang
Department of Gastroenterology, Peking Union Medical College Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, No. 1 Shuaifuyuan, Dongcheng District, Beijing, 100730, People’s Republic of China
Email [email protected]; [email protected]
Purpose: The accurate differentiation between benign and malignant biliary stricture is significant but challenging. Tissue diagnosis of biliary stricture by endoscopy sampling can provide excellent specificity but insufficient sensitivity. For patients with suspected malignant biliary stricture (MBS) but non-malignant was reported in endoscopy tissue samples, we constructed a nomogram to predict malignancy and improve the overall diagnostic performance.
Patients and Methods: 232 patients with suspected MBS and underwent endoscopy tissue sampling from January 2017 to December 2019 were included, among which 123 patients’ endoscopy tissue samples were classified as non-malignant (including atypical, negative for malignancy, and nondiagnostic). Demographics, serum markers, radiological and sampling results of these 123 patients were collected to construct a nomogram using multivariate analysis.
Results: The nomogram was developed based on bilirubin, CA19-9, radiological result, and atypical sampling results and provided an AUC of 0.863 (95% CI 0.795– 0.930) for predicting MBS. The specificity, sensitivity, and accuracy of endoscopy tissue diagnosis were 100.00%, 59.90%, and 68.53%, respectively. With the nomogram added, the overall diagnosis specificity, sensitivity, and accuracy were 95.24%, 89.20%, and 90.23%, respectively.
Conclusion: The nomogram can predict malignancy in patients whose endoscopy tissue diagnoses were non-malignant. The overall diagnostic performance was improved with the nomogram added.
Keywords: malignant biliary stricture, endoscopic tissue sampling, bilirubin, CA19-9, radiology
Introduction
Biliary stricture, a critical clinical condition, is frequently presented as a diagnostic dilemma and can cause serious severe symptoms and complications.1–3 A biliary stricture can be caused by either benign or malignant etiologies, with malignant biliary stricture (MBS) accounting for approximately 70% of instances. The accurate distinguishing between benign and malignant biliary stricture is critical to guide appropriate treatment.
Tissue sampling is critical for differentiating the cause of biliary stricture adequately, which can be accomplished by endoscopic retrograde cholangiopancreatography (ERCP)-based tissue sampling and endoscopic ultrasound-guided fine needle aspiration (EUS-FNA). Endoscopy tissue samples are commonly classified as positive for malignancy, suspicious for malignancy, atypical, negative for malignancy, or nondiagnostic. Strictures with tissue samples classified as positive or suspicious for malignancy are usually considered as MBS. The specificity of endoscopy tissue sampling can be approximately 100% under this criterion, but the sensitivity is insufficient.4–6 Among the non-malignant results, atypical results are complicated to interpret since they can be caused by heterogeneous causes, including paracancerous or low cellularity specimens from MBS cases, or reactive alterations due to inflammatory conditions or procedural artifacts.7 Previous studies have found that 36.5–70.7% of patients with atypical results turned out to have malignancy later.8–11 Therefore, the significance of an atypical result in the prediction of malignancy warrants further exploration.
Furthermore, diagnosing MBS often requires a combination of different diagnostic modalities. The elderly had a higher incidence of malignancy in suspected MBS patients. The levels of serum total bilirubin, alkaline phosphatase (ALP), and gamma-glutamyltransferase (γ-GT) are higher in malignant biliary stricture than in benign biliary stricture, with bilirubin being the most important discriminator for malignancy.12,13 A markedly elevated bilirubin level has a high positive predictive value for the existence of malignancy.14 Serum tumor markers carbohydrate antigen 19–9 (CA19-9) and carcinoma embryonic antigen (CEA) are elevated in several gastrointestinal cancers, and CA19-9 is the most significant and widely utilized biomarker in pancreaticobiliary cancer.15 Various cross-sectional radiological images have been reported to be useful in identifying biliary stricture, such as computed tomography (CT) and magnetic resonance imaging (MRI)/magnetic resonance cholangiopancreatography (MRCP).16,17
In a previous study, Lindberg et al18 discussed the limitations of four separate methods (brush cytology, DNA analysis, serum CA19-9, and serum CEA) used at the time of ERCP to diagnose MBS and reported a higher sensitivity when the four methods were combined. Hence, a prediction model that integrates endoscopy non-malignant tissue sampling results and these noninvasive parameters may assist in predicting malignancy in biliary stricture. In this study, we analyzed the correlations between demographics, serum markers, radiological imaging, and endoscopy sampling results with MBS for patients whose endoscopic tissue samples were categorized as non-malignant, and developed a prediction model in the form of a nomogram. The improvement in diagnostic performance when the nomogram prediction data were included was evaluated.
Methods
Patients
A total of 246 patients with suspected MBS underwent ERCP-based tissue sampling and/or EUS-FNA at Peking Union Medical College Hospital between January 2017 and December 2019.
Inclusion Criteria
- the presence of biliary stricture identified by cross-sectional radiological imaging;
- obstructive jaundice, and/or elevated levels of liver tests in a cholestatic pattern, and/or cholangitis;
- assessment of bilirubin, CA19-9, and CEA before biliary drainage and/or tissue sampling;
- a final malignant/benign diagnosis based on endoscopic/surgical histology or a follow-up longer than 12 months.
Exclusion Criteria
- received tumor-related chemoradiotherapy or targeted therapy within 1 month before tissue acquisition;
- known history of primary pancreato-biliary carcinoma;
- altered gastrointestinal anatomy or duodenal obstruction.
Finally, a total of 232 patients were recruited in this study. The study was conducted in accordance with the Declaration of Helsinki, and was approved by the ethical committee of Peking Union Medical College Hospital (Ethical Number: S-K1706).
Data Collection and Definitions
The medical records of selected patients were reviewed, including clinical, laboratory, radiological, endoscopic, and pathological data and follow-up results.
Laboratory tests, such as bilirubin, CA19-9 and CEA, were assessed before biliary drainage. Two specialist radiologists assessed cross-sectional radiological images, including MRCP and contrast-enhanced CT/MRI. Irregular strictures, a simultaneous pancreatic duct stricture (“double duct sign”), an abnormally enhanced mass lesion, and secondary signs of malignancy (such as vascular infiltration and evidence of metastases) were all used to identify malignant from benign strictures.
Endoscopic tissue samples were classified into the following categories: (1) positive for malignancy, (2) suspicious for malignancy, (3) atypical, (4) negative for malignancy, and (5) nondiagnostic. Samples classified as positive or suspicious for malignancy were categorized as malignant, whereas samples classified as atypical, negative for malignancy, and nondiagnostic were categorized as non-malignant.
The final diagnosis was based on the following criteria in decreasing priority: (1) surgical pathology, (2) endoscopic cytology or histology, and (3) clinical diagnosis by long-term follow-up of more than 12 months.
Endoscopic Procedures
Endoscopic procedures were achieved using standardized protocols by five senior endoscopists. All endoscopists were highly experienced and currently perform 400 ERCP/EUS cases per year. Written informed consent was obtained from each patient before the procedure.
ERCP was performed with JF or TJF-260V (Olympus, Tokyo, Japan). Initial cannulation and cholangiography were performed to observe the morphology and location of the stricture. Brush cytology was performed by passing a brush into the biliary tree over a guidewire under fluoroscopy. The brush was moved to and fro across the stricture more than 10 times. Biliary forceps biopsies were performed in cases evaluated to be safe and feasible, yielding 1 to 6 specimens.
EUS-FNA was performed using the linear-array echoendoscope GF-UCT240 (Olympus, Tokyo, Japan). Doppler examination was performed before FNA to ensure the absence of intervening vascular structures along the anticipated needle path. EUS-FNA was attempted with a standard 19-, 22-, or 25-gauge needle or a 20-gauge biopsy needle as directed by the endoscopist’s preference, characteristics, and location of the lesion. After puncturing each lesion, the stroke was carefully performed 10–20 times. Rapid on-site evaluation (ROSE) was not routinely available. The puncture procedure was repeated until the whitish material became visible macroscopically. Often 1–4 passes were performed.
Biliary brush and FNA samples were expressed onto glass slides, then fixed with 95% ethanol for subsequent Papanicolaou staining. Additional material was submitted for the ThinPrep cytologic test. Biliary biopsy and visible core specimens were placed in formalin for histological analysis. All samples were sent to the pathology department for interpretation by expert pathologists and cytopathologists dedicated to biliopancreatic diseases.
Model Construction and Validation
The prediction model was built based on multivariate logistic regression analysis. Before construction, multicollinearity analysis was performed by calculating the variance inflation factor (VIF) among the features; a VIF value > 10 was considered to indicate multicollinearity. The corresponding variables were excluded from the model. A backward stepwise variable selection procedure was used in multivariate models for model selection based on the Akaike information criterion (AIC). The final model was tested for predictive power using internal validation, which was performed using the bootstrap resampling method by randomly drawing 1000 samples from the primary dataset to avoid overoptimism.
Statistical Analysis
Statistical analysis was performed using R (http://www.R-project.org) and EmpowerStats software (X&Y Solutions). Continuous variables are expressed as medians with interquartile ranges (IQRs), and are compared using the Mann–Whitney U-test. Categorical variables are expressed as frequencies and percentages, and are compared using the Pearson chi-squared test. A P value < 0.05 was considered statistically significant. The Hmisc package was used to plot the nomogram. The pROC package was used to plot the ROC curves and measure the AUCs. The diagnostic performance was evaluated by calculating sensitivity, specificity, positive likelihood ratio, negative likelihood ratio, positive predictive value, and negative predictive value. Receiver operating curves (ROC) and the corresponding area under the curve (AUC) values were used to assess the discrimination ability of the model.
Results
Clinicopathological Characteristics of the Study Patients
Among the study cohort, 182 patients were diagnosed as malignant biliary stricture, and 50 patients were diagnosed as benign biliary stricture. Table 1 shows the baseline characteristics and endoscopy tissue sampling results of the study patients. The final diagnoses are presented in Table 2. Patients with MBS were older and had a higher level of bilirubin, CA19-9, and CEA. A total of 109 MBS patients were diagnosed after endoscopy tissue sampling with a positive or suspicious for malignancy sampling result. The remaining 123 patients were brought into the next step of model construction. In the MBS, cholangiocarcinoma and pancreatic cancer are the two most common etiologies.
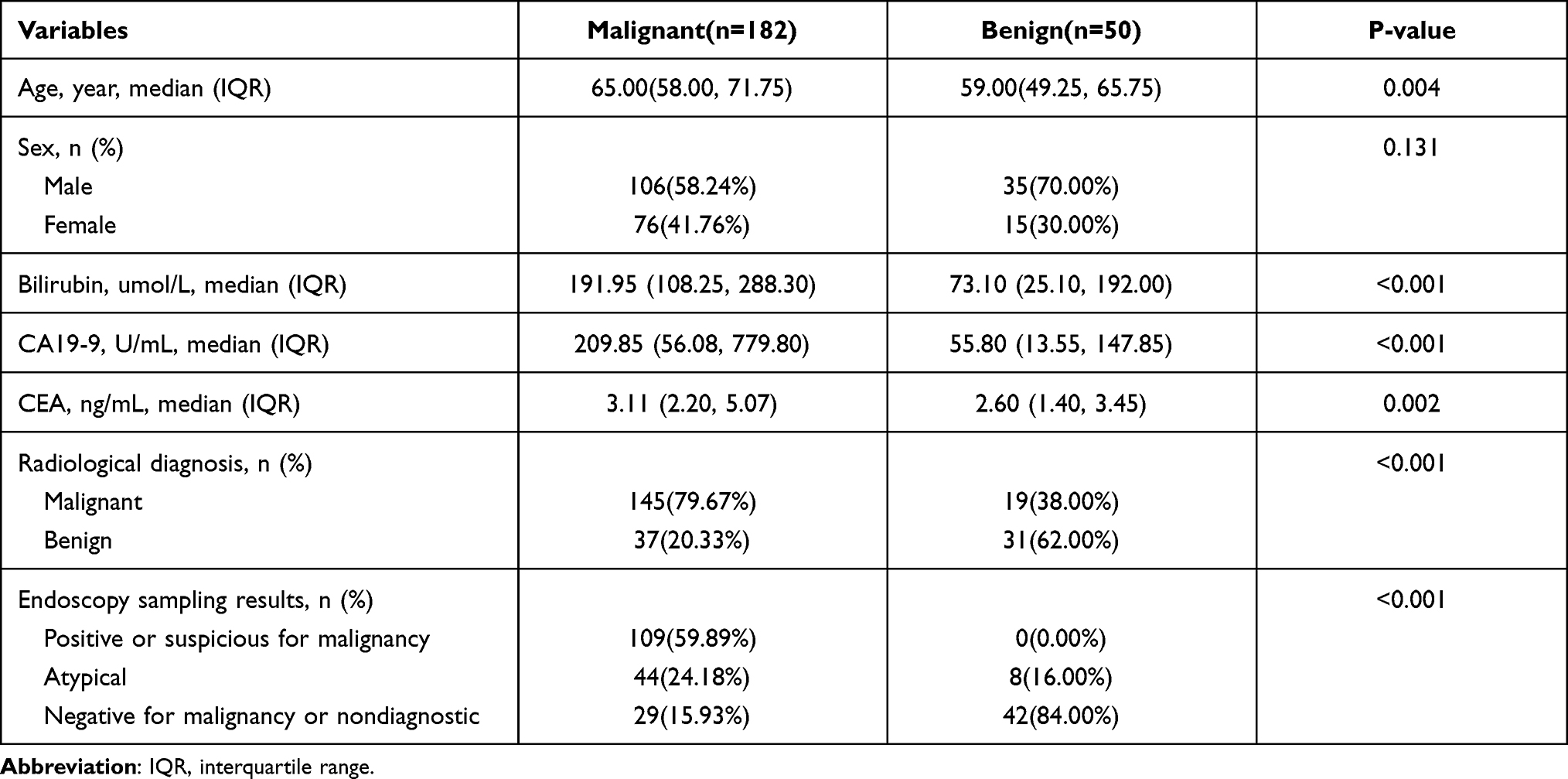 |
Table 1 Baseline Characteristics and Endoscopy Sampling Results of the Study Patients |
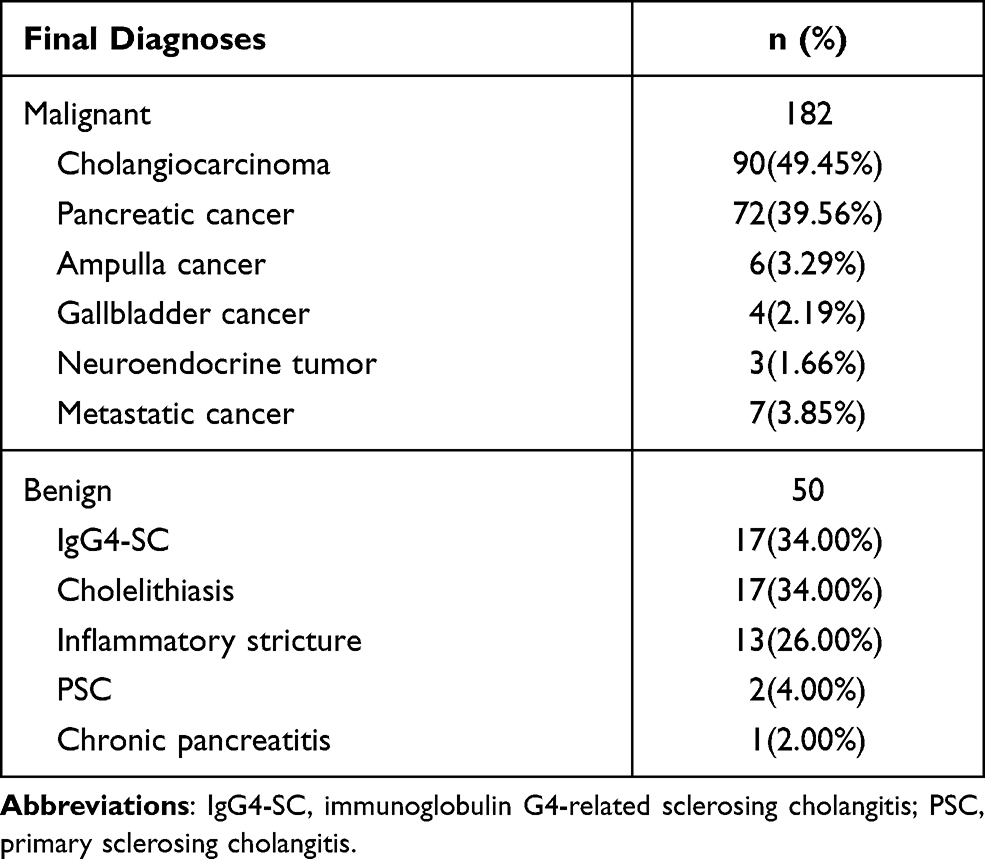 |
Table 2 Final Diagnoses of the Study Patients |
Logistic Regression Analysis and the Nomogram Construction
After the initial endoscopy tissue sampling, 109 patients were diagnosed with MBS. A logistic regression analysis was carried out on the remaining 123 patients. As shown in Table 3, age, bilirubin, CA 19–9, CEA, radiological diagnosis, and atypical endoscopy sampling are related to MBS in univariate logistic regression analysis. After the stepwise variable selection procedure, bilirubin, CA19-9, radiological diagnosis, and atypical endoscopy sampling showed independent correlation with MBS. The best diagnostic performance of bilirubin was reached when the cut-off value was 100umol/L with a specificity of 57.14% and a sensitivity of 76.06%. When bilirubin>400umol/L, the specificity was 98.00%. The best diagnostic performance of CA19-9 was reached when the cut-off value was 217U/mL, with a specificity of 86.05% and a sensitivity of 48.48%. When CA19-9>500U/mL, the specificity was 95.35%. Therefore, bilirubin, CA19-9, radiological diagnosis, and atypical sampling result were incorporated into the final nomogram, and the upper threshold of bilirubin and CA19-9 were 400umol/L and 500U/mL, respectively. The nomogram is presented in Figure 1.
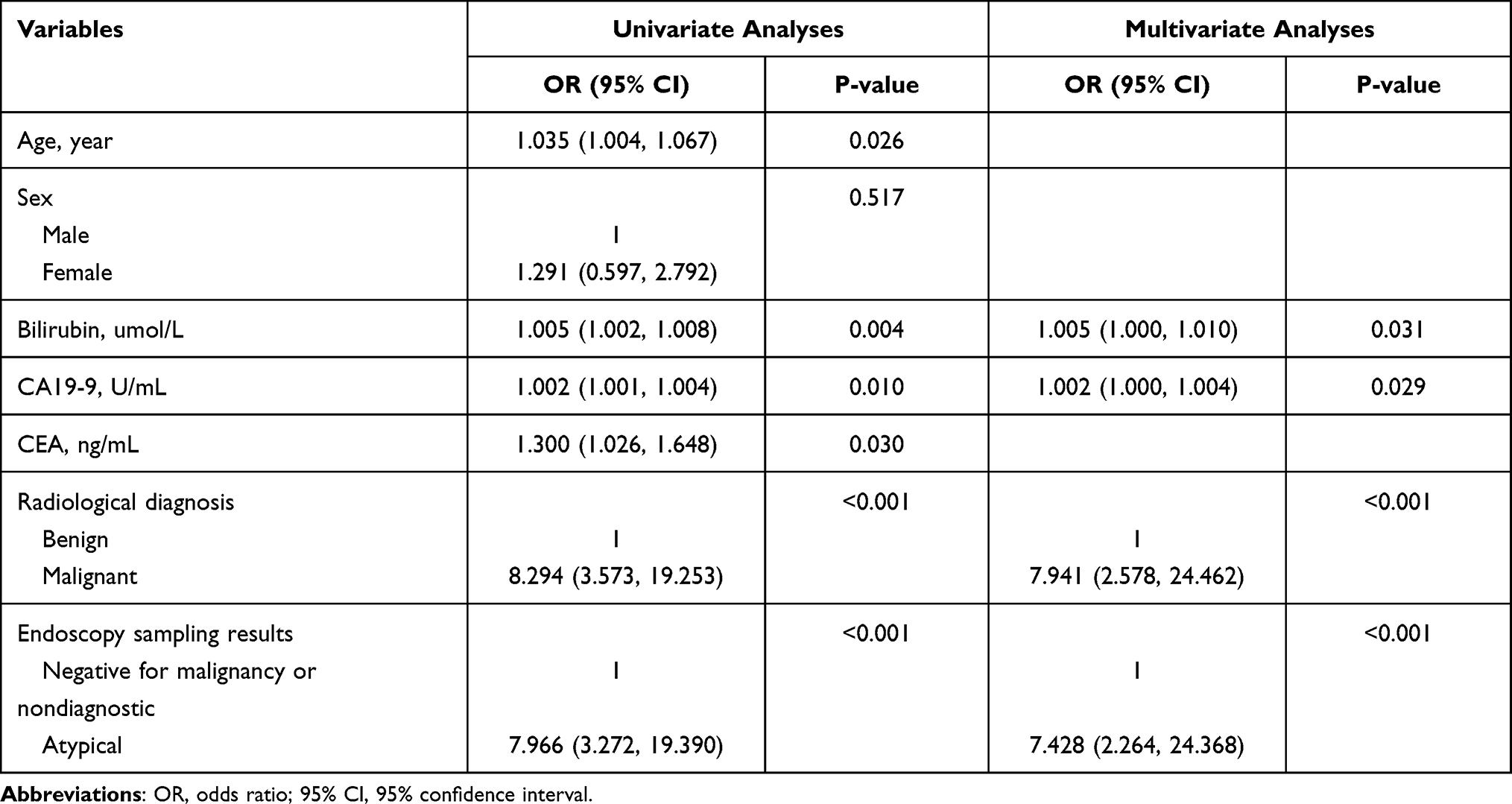 |
Table 3 Univariate and Multivariate Logistic Regression Analysis in Patients with a Non-Malignant Endoscopy Sampling Result |
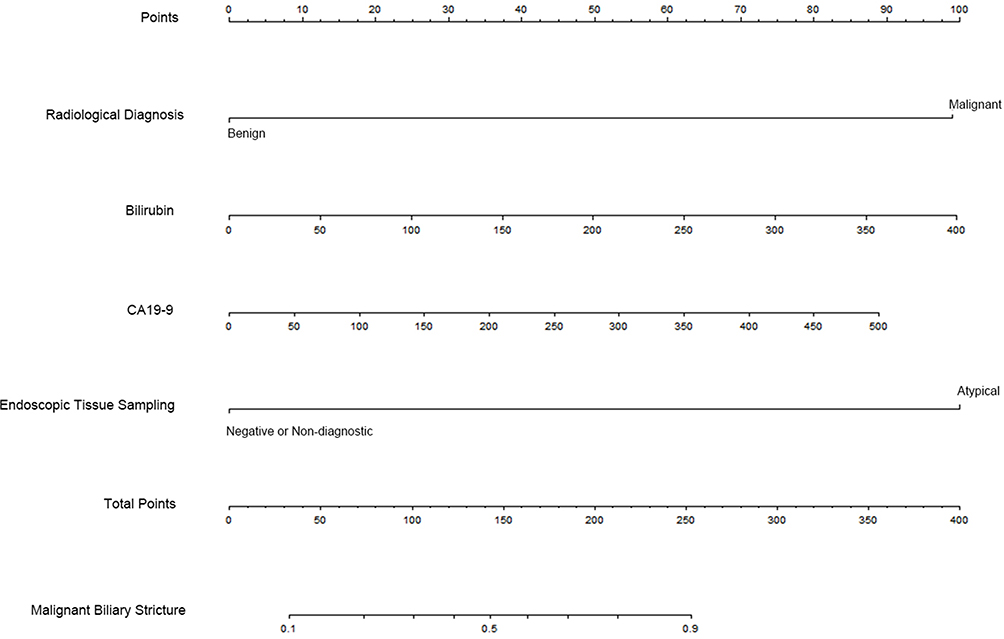 |
Figure 1 The nomogram to predict malignancy in biliary stricture patients with a non-malignant endoscopy sampling result. |
Diagnostic Performance of the Nomogram
As shown in Figure 2, the AUC of the nomogram was 0.863 (95% CI 0.795–0.930), which was higher than bilirubin (AUC=0.707 (95% CI 0.604–0.809, P-value=0.001), CA19-9 (AUC=0.684 (95% CI 0.584–0.784), P-value<0.001), radiological diagnosis (AUC=0.715 (95% CI 0.611–0.818, P-value<0.001), atypical sampling result (AUC=0.706 (95% CI 0.608–0.805), P-value<0.001) as a separate method. The diagnostic performance of the nomogram was presented in Table 4, with a specificity and a sensitivity of 95.24% and 70.31%, respectively.
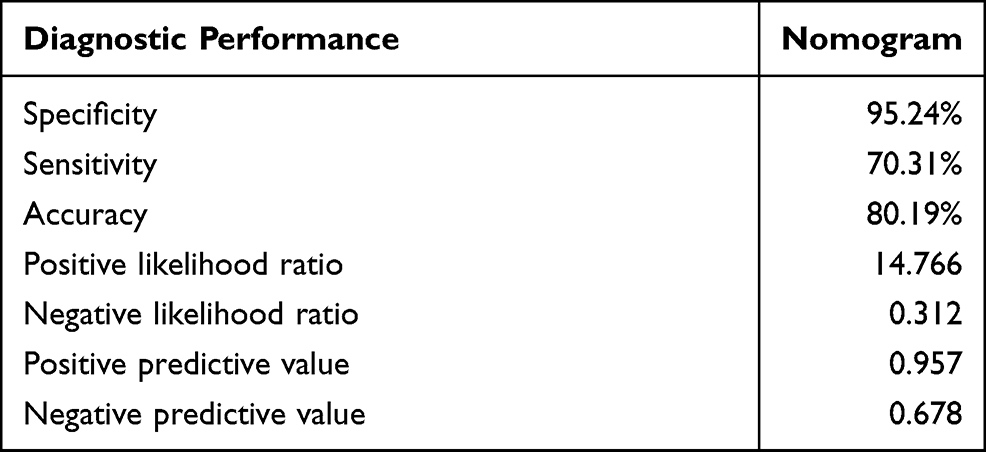 |
Table 4 Diagnostic Performance of the Nomogram |
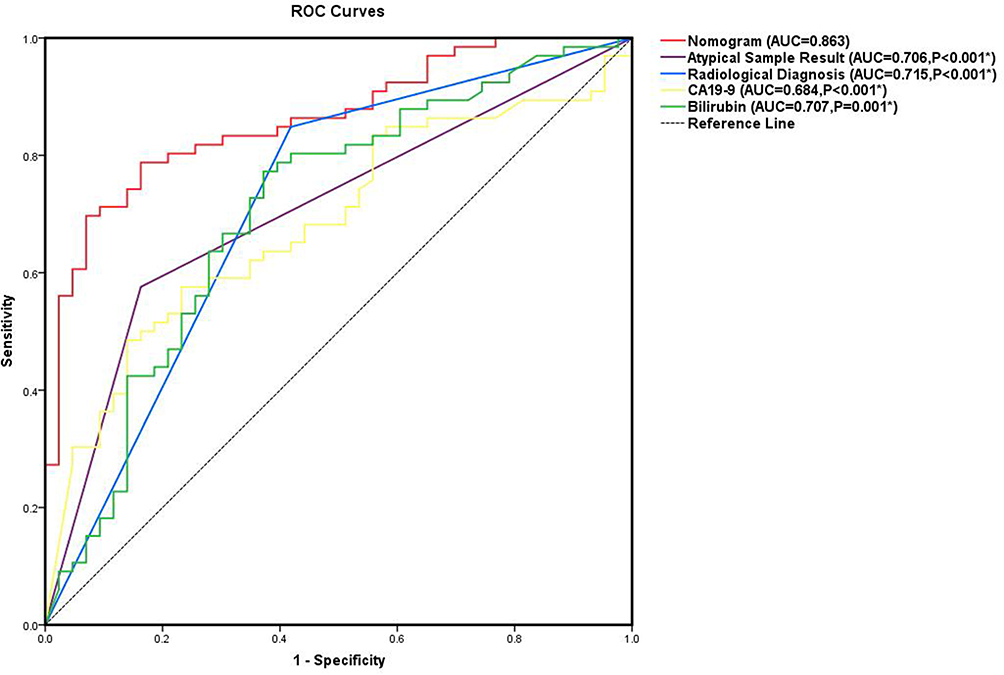 |
Figure 2 Receiver Operating Characteristic (ROC) curves of the nomogram, bilirubin, CA19-9, radiological diagnosis, and atypical sample result. *Compared with the AUC of nomogram. |
Improvement of Diagnostic Performance with the Combination of Nomogram
As presented in Table 5, The specificity, sensitivity and accuracy of initial endoscopy tissue diagnosis were 100.00%, 59.90% and 68.53% respectively. After the nomogram was added for the patients whose initial endoscopy tissue sampling was non-malignant, the overall diagnostic performance was improved with a specificity of 95.24%, a sensitivity of 89.02%, and an accuracy of 90.23%.
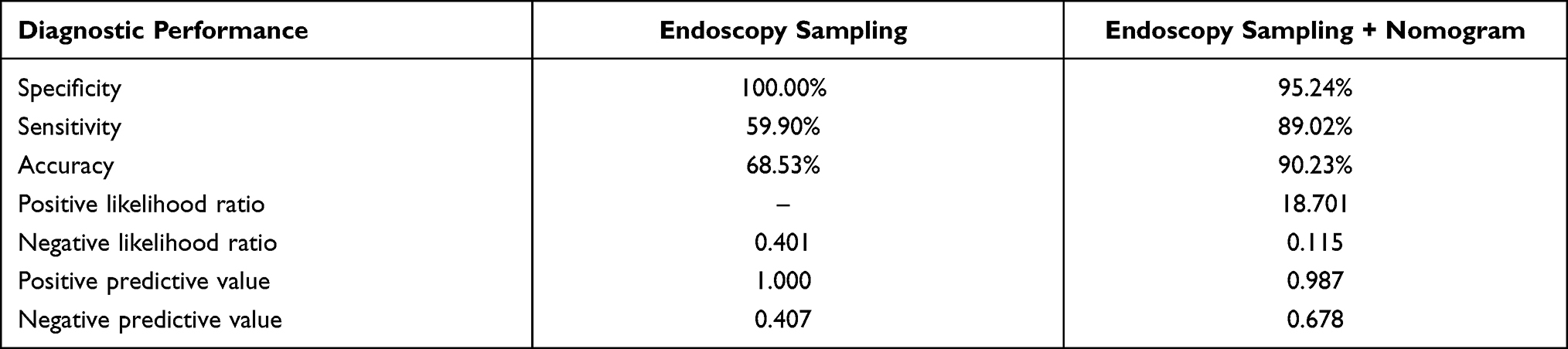 |
Table 5 Diagnostic Performance of the Initial Endoscopy Sampling and the Combination of Endoscopy Sampling with the Nomogram |
Discussion
We enrolled 232 patients with suspected MBS in this study, with 109 of them being diagnosed as MBS via endoscopic tissue sampling. A multivariate logistic regression analysis was performed on the remaining 123 patients, and bilirubin, CA19-9, radiological diagnosis, and atypical sampling result showed independent correlations with MBS. A prediction model was constructed using these parameters in the form of a nomogram. The nomogram can distinguish between malignant and benign biliary strictures with an AUC of 0.863 (95% CI 0.795–0.930). When the endoscopic tissue diagnosis is combined with the nomogram, the overall diagnostic performance improves.
The differentiation between benign and malignant biliary strictures can be difficult, but is of great significance regarding prognosis and planning optimal therapy. ERCP-based tissue sampling and EUS-FNA are two commonly utilized endoscopic methods for obtaining tissue samples.
ERCP-based tissue sampling, including brush cytology and intraductal forceps biopsy, is widely considered to be the first-line sampling method for suspected MBS.19 Brush cytology is routinely done to diagnose malignant biliary strictures because it is simple to perform, associated with fewer adverse events, but is restricted by its low sensitivity ranging from 30% to 81%.4–6,20 If adequate samples were acquired, intraductal forceps biopsy can provide information about the tissue structure and tissue invasion. However, it is associated with increased worries regarding perforation and bleeding. A meta-analysis21 reported that the sensitivity of intraductal forceps biopsy for the detection of malignancy did not differ much from that of brush cytology. The suboptimal sensitivity of ERCP-based tissue sampling was attributed to the difficulty of obtaining sufficient tissue samples in the obstructed bile duct, the desmoplastic nature of tumors, the submucosal spread of neoplasia and extrinsic compression leading to the stricture. In our institution, brush cytology is routinely conducted, and intraductal forceps biopsy was decided to perform after the evaluation of safety and feasibility based on pre-procedure cross-sectional radiological imaging and cholangiography.
EUS-FNA of ductal lesions shows moderate to high sensitivity and fewer complications, and is recommended as an alternative after a negative ERCP-based sampling,19 or as a first-line sampling method.6,22 ROSE has been shown to boost EUS-FNA diagnostic yield in various investigations.23,24 However, ROSE requires considerable expertise and its availability is limited due to additional time and cost. Also, randomized controlled trials25,26 and meta-analysis27 present a noninferiority to forgoing it. Recent data suggests EUS-guided fine needle biopsy (EUS-FNB), which can preserve tissue and sample integrity, is as effective as EUS-FNA with ROSE.28,29 EUS-FNA of small lesions presenting as biliary wall thickening is technically difficult, so it is generally limited to cases in which a well-defined mass is present.30
ERCP-based sampling and EUS-FNA have different characteristics. Initial sampling methods can be decided depending on the level of obstructive jaundice, the combination of cholangitis, as well as the location and nature of the stricture.
Apart from endoscopic methods, tissue samples can be obtained through percutaneous transhepatic cholangiography(PTC), which was reported to have relative higher risk of adverse event31 and tumor seeding.32 Besides, external drains need more additional post-operative medical care. Nevertheless, Fohlen et al reported transhepatic forceps biopsy has higher sensitivity for lesions located at the upper part of the biliary tree (hilum or intrahepatic bile duct).33 Therefore, PTC-based tissue sampling is an alternative in patients not suitable for endoscopic strategies. Advanced endoscopic tissue sampling, such as peroral cholangioscopy (POC)-guided sampling, is another option,2,19 but with an increased risk of complications and costs.
It was reported that an ERCP procedure with brush cytology, a DNA analysis, combined with serum analysis of CA 19–9 and CEA, can increase the possibility of distinguishing between malignant and benign biliary strictures.18 Therefore, combining different methods can help MBS diagnosis in a less invasive and economical way. Our prediction model, which was based on bilirubin, CA19-9, radiological diagnosis, and atypical sampling results, showed an AUC of 0.863 (95% CI 0.795–0.930) to distinguish MBS in patients whose endoscopic sampling was non-malignant, providing additional information for assessment and clinical decision making. For those patients with positive results provided by the prediction model, more intensive strategies might be taken into consideration by clinicians, including additional surgery, or advanced tissue sampling. For patients with negative results, a close follow-up is an option after explaining the possible risk to the patients. In this way, the prediction model can benefit from better tailoring of disease management for the patients, thus improving the prognosis and life quality of the patients.
It is difficult to interpret pancreaticobiliary cytologic and histologic specimens, especially if stenting or surgical procedures have been undertaken recently. When cells exhibit cytoplasmic, nuclear, or architectural traits that are inconsistent with normal or reactive cellular changes, but are insufficient to designate the cells as a neoplasm or suspicious for a high-grade malignancy, they are classified as atypical. This is a diverse category. This category includes individuals with reactive alterations, low cellularity specimens, premalignant changes (dysplasia), and patients who were assigned to this category due to pathologist caution in diagnosis.7 Malignancy, pronounced inflammation, and a history of recent surgical intervention, including stenting, can all lead to an atypical diagnosis.34 As a result, the management of atypical results is dilemmatic and complicated. The prevalence of an atypical sampling result in different series ranged from 10% to 31%,6,8,10,20,34 and malignancy was identified in 37–71% of patients with an atypical result.8–11,34,35 In our study, MBS was identified in 85% of patients with an atypical result. It is slightly higher than in other research, which may result from pathologists’ caution.
Cytologic preparation can influence the specimen interpretation. The ThinPrep method has advantages over the direct smear in the elimination of air-drying artifacts and blood-clotting artifacts, and decreased overlap of epithelial cells.36 The combination of ThinPrep and direct smears, which are routinely performed in our institution, was reported to have better diagnostic performance.8 The inter-observer variability and experience of cytopathological diagnoses is a concern, and cytopathologists dedicated to biliopancreatic diseases are significant for accurate interpretation of specimens.37 In this study, expert cytopathologists made diagnosis of these samples who are highly experienced in pathology and cytopathology, which helped minimize the impact from inter-observer variability of cytologic results.
Bilirubin levels can help predict malignancy in biliary obstruction patients, with cut-off values ranging from 75–145umol/L.12–14,38 Among 1026 obstructive jaundice patients, Garcea et al found that a bilirubin level > 100µmol/l had the best sensitivity and specificity of 72% and 87% for predicting malignancy, respectively, and that the specificity increased to 100% when the cut-off value was > 400umol/L.14 The level of bilirubin was generally higher in MBS due to the inexorable progression of the malignancy, and a markedly elevated bilirubin level has an important positive predictive value for malignancy. In our study, the best diagnostic performance of bilirubin was also obtained at a cut-off value of 100umol/L, and when > 400umol/L, the specificity was 98.0%. Considering bilirubin higher than 400umol/L will make little difference in diagnostic performance, the upper threshold of bilirubin brought into the nomogram was set as 400umol/L to reduce the adverse effect of extreme values of continuous variables.
CA19-9 is a carbohydrate antigen expressed by several epithelial cancers as well as in normal pancreatic and biliary ductal epithelial cells, and can be used to diagnose pancreatic cancer and cholangiocarcinoma.15 The utility of CA19-9 has several confounding limitations, and the specificity for diagnosing MBS was suboptimal, ranging from 39–70% using the regular cut-off value.39,40 In MBS, the elevated CA19-9 was from the additional synthesis by proliferating malignant cells. But patients with genotypically negative Lewis blood group antigen do not synthesize CA19-9. More importantly, biliary obstruction and inflammation, which can lead to an increase in secretion, accumulation, and subsequent leak into the bloodstream of CA19-9, often cause a false positive result of CA19-9. As a result, 100U/mL and 129U/mL were recommended as cut-off values in two different clinical approaches for MBS diagnosis.2,3 Although, extremely high levels of CA19-9 were reported in benign cases occasionally,41 CA19-9>500U/mL was more often used to evaluate stage and resectability.15 When CA19-9>500U/mL, the specificity was 95.35%, so, the upper threshold of CA19-9 brought into the nomogram was set as 500U/mL based on the same considerations as before. There is often a fall of CA19-9 in benign diseases after biliary drainage, so the CA19-9 after biliary drainage is significant for MBS diagnosis.42 To minimize the disturbance of biliary obstruction, Liu et al evaluated the diagnostic performance of the ratio of CA19-9 to bilirubin, and found it was better than CA19-9.43 C-reactive protein (CRP), one of the acute-phase proteins, could increase under an inflammatory response to tumor invasion. Greca et al reported that it was a more appropriate adjusting factor for CA19-9 compared with bilirubin.44
Cross-sectional radiological imaging has been widely used as a noninvasive technique to evaluate biliary strictures, and can offer a relatively detailed view of the biliary system to identify the presence and location of the stricture.1 Irregular strictures, a concomitant pancreatic duct stricture (“double duct sign”), a mass lesion with delayed enhancement, secondary signs of malignancy (such as vascular infiltration and evidence of metastases) are signs of MBS.16,45,46 The presence of a mass and delayed enhancement were reported to differentiate the MBS independently.45,46 The sensitivity and specificity of cross-sectional radiological imaging for diagnosing MBS were reported to be 67–85% and 63–82%, respectively.16,17 18F-FDG PET-CT, combining functional and anatomic imaging, plays an important role in malignancy diagnosis. Wang et al reported that 18F-FDG PET-CT is of great value in differentiating malignant from benign origins of obstructive jaundice, with the sensitivity and specificity of 86% and 74%, respectively, and is a useful adjuvant to conventional imaging.47 Malignant cases with low FDG uptake48 and the concealed tumor image by diffuse FDG uptake due to secondary pancreatitis may lead to false-negative results. Benign inflammatory diseases, such as autoimmune pancreatitis, may also accumulate FDG and result in false-positive results.49
There were several limitations in our research. First, this was a retrospective, single-center study, selection bias was inevitable Because the lack of prospective design, laboratory test and radiological imaging examinations varied in different patients, more specific research about diagnostic performance of different radiological images, PET-CT, CA19-9 after drainage, and the CRP-adjusted CA19-9 could not be evaluated. Second, the sample size is relatively modest. Adding data from other medical centers could help improve the model’s clinical efficacy even more.
Conclusion
In this study, we constructed a nomogram based on bilirubin, CA19-9, radiological diagnosis, and the atypical sample result for suspected MBS patients whose endoscopic tissue diagnoses were non-malignant. The combination of the endoscopic tissue diagnosis and the nomogram improved overall diagnostic performance.
Abbreviations
MBS, malignant biliary stricture; ERCP, endoscopic retrograde cholangiopancreatography; EUS-FNA, endoscopic ultrasound-guided fine needle aspiration; EUS-FNB, endoscopic ultrasound-guided fine needle biopsy; CT, computed tomography; MRI, magnetic resonance imaging; MRCP, magnetic resonance cholangiopancreatography; CA19-9, carbohydrate antigen 19-9; CEA, carcinoma embryonic antigen; ROSE, Rapid on-site evaluation; IQR, interquartile ranges; ROC, receiver operating curves; AUC, area under the curve. CI, confidence interval.
Acknowledgments
We thank Ruinan Liu for assistance in data collection.
Funding
This work was supported by the National Key Research and Development Program of China [grant number 2016YFC1302802] and Beijing Municipal Science and Technology Project [grant number Z181100001618013].
Disclosure
The authors report no conflicts of interest in this work.
References
1. Dorrell R, Pawa S, Zhou Y, Lalwani N, Pawa R. The diagnostic dilemma of malignant biliary strictures. Diagnostics. 2020;10(5):337. doi:10.3390/diagnostics10050337
2. Dumonceau JM, Delhaye M, Charette N, Farina A. Challenging biliary strictures: pathophysiological features, differential diagnosis, diagnostic algorithms, and new clinically relevant biomarkers - part 1. Therap Adv Gastroenterol. 2020;13:1756284820927292. doi:10.1177/1756284820927292
3. Bowlus CL, Olson KA, Gershwin ME. Evaluation of indeterminate biliary strictures. Nat Rev Gastroenterol Hepatol. 2016;13(1):28–37. doi:10.1038/nrgastro.2015.182
4. de Bellis M, Sherman S, Fogel EL, et al. Tissue sampling at ERCP in suspected malignant biliary strictures (Part 2). Gastrointest Endosc. 2002;56(5):720–730. doi:10.1016/S0016-5107(02)70123-5
5. Lee YN, Moon JH, Choi HJ, et al. Tissue acquisition for diagnosis of biliary strictures using peroral cholangioscopy or endoscopic ultrasound-guided fine-needle aspiration. Endoscopy. 2019;51(1):50–59. doi:10.1055/a-0645-1395
6. Weilert F, Bhat YM, Binmoeller KF, et al. EUS-FNA is superior to ERCP-based tissue sampling in suspected malignant biliary obstruction: results of a prospective, single-blind, comparative study. Gastrointest Endosc. 2014;80(1):97–104. doi:10.1016/j.gie.2013.12.031
7. Pitman MB, Layfield LJ. Guidelines for pancreaticobiliary cytology from the Papanicolaou society of cytopathology: a review. Cancer Cytopathol. 2014;122(6):399–411. doi:10.1002/cncy.21427
8. Volmar KE, Vollmer RT, Routbort MJ, Creager AJ. Pancreatic and bile duct brushing cytology in 1000 cases: review of findings and comparison of preparation methods. Cancer. 2006;108(4):231–238. doi:10.1002/cncr.21842
9. Witt BL, Kristen Hilden RN, Scaife C, et al. Identification of factors predictive of malignancy in patients with atypical biliary brushing results obtained via ERCP. Diagn Cytopathol. 2013;41(8):682–688. doi:10.1002/dc.22924
10. Park JY, Jeon TJ. Factors associated with malignant biliary strictures in patients with atypical or suspicious cells on brush cytology. Clin Endosc. 2019;52(2):168–174. doi:10.5946/ce.2018.105
11. Navaneethan U, Singh T, Gutierrez NG, et al. Predictors for detection of cancer in patients with indeterminate biliary stricture and atypical cells on endoscopic retrograde brush cytology. J Dig Dis. 2014;15(5):268–275. doi:10.1111/1751-2980.12134
12. Saluja SS, Sharma R, Pal S, Sahni P, Tk C. Differentiation between benign and malignant hilar obstructions using laboratory and radiological investigations: a prospective study. HPB (Oxford). 2007;9(5):373–382. doi:10.1080/13651820701504207
13. Meister T, Uphoff MA, Heinecke A, et al. Novel score for prediction of malignant bile duct obstruction based on biochemical and clinical markers. Aliment Pharmacol Ther. 2015;41(9):877–887. doi:10.1111/apt.13152
14. Garcea G, Ngu W, Neal CP, Dennison AR, Berry DP. Bilirubin levels predict malignancy in patients with obstructive jaundice. HPB. 2011;13(6):426–430. doi:10.1111/j.1477-2574.2011.00312.x
15. Lee T, Teng TZJ, Shelat VG. Carbohydrate antigen 19-9 - tumor marker: past, present, and future. World J Gastrointest Surg. 2020;12(12):468–490. doi:10.4240/wjgs.v12.i12.468
16. Heinzow HS, Kammerer S, Rammes C, Wessling J, Domagk D, Meister T. Comparative analysis of ERCP, IDUS, EUS and CT in predicting malignant bile duct strictures. World J Gastroenterol. 2014;20(30):10495–10503. doi:10.3748/wjg.v20.i30.10495
17. Rösch T, Meining A, Frühmorgen S, et al. A prospective comparison of the diagnostic accuracy of ERCP, MRCP, CT, and EUS in biliary strictures. Gastrointest Endosc. 2002;55(7):870–876. doi:10.1067/mge.2002.124206
18. Lindberg B, Arnelo U, Bergquist A, et al. Diagnosis of biliary strictures in conjunction with endoscopic retrograde cholangiopancreaticography, with special reference to patients with primary sclerosing cholangitis. Endoscopy. 2002;34(11):909–916. doi:10.1055/s-2002-35298
19. Sun B, Moon JH, Cai Q, et al. Review article: Asia-Pacific consensus recommendations on endoscopic tissue acquisition for biliary strictures. Aliment Pharmacol Ther. 2018;48(2):138–151. doi:10.1111/apt.14811
20. Jo JH, Cho CM, Jun JH, et al. Same-session endoscopic ultrasound-guided fine needle aspiration and endoscopic retrograde cholangiopancreatography-based tissue sampling in suspected malignant biliary obstruction: a multicenter experience. J Gastroenterol Hepatol. 2019;34(4):799–805. doi:10.1111/jgh.14528
21. Navaneethan U, Njei B, Lourdusamy V, Konjeti R, Vargo JJ, Parsi MA. Comparative effectiveness of biliary brush cytology and intraductal biopsy for detection of malignant biliary strictures: a systematic review and meta-analysis. Gastrointest Endosc. 2015;81(1):168–176. doi:10.1016/j.gie.2014.09.017
22. Onda S, Ogura T, Kurisu Y, et al. EUS-guided FNA for biliary disease as first-line modality to obtain histological evidence. Therap Adv Gastroenterol. 2016;9(3):302–312. doi:10.1177/1756283X15625584
23. Klapman JB, Logrono R, Dye CE, Waxman I. Clinical impact of on-site cytopathology interpretation on endoscopic ultrasound-guided fine needle aspiration. Am J Gastroenterol. 2003;98(6):1289–1294. doi:10.1111/j.1572-0241.2003.07472.x
24. Iglesias-Garcia J, Dominguez-Munoz JE, Abdulkader I, et al. Influence of on-site cytopathology evaluation on the diagnostic accuracy of endoscopic ultrasound-guided fine needle aspiration (EUS-FNA) of solid pancreatic masses. Am J Gastroenterol. 2011;106(9):1705–1710. doi:10.1038/ajg.2011.119
25. Wani S, Mullady D, Early DS, et al. The clinical impact of immediate on-site cytopathology evaluation during endoscopic ultrasound-guided fine needle aspiration of pancreatic masses: a prospective multicenter randomized controlled trial. Am J Gastroenterol. 2015;110(10):1429–1439. doi:10.1038/ajg.2015.262
26. Kappelle WFW, Van Leerdam ME, Schwartz MP, et al. Rapid on-site evaluation during endoscopic ultrasound-guided fine-needle aspiration of lymph nodes does not increase diagnostic yield: a randomized, multicenter trial. Am J Gastroenterol. 2018;113(5):677–685. doi:10.1038/s41395-018-0025-8
27. Kong F, Zhu J, Kong X, et al. Rapid on-site evaluation does not improve endoscopic ultrasound-guided fine needle aspiration adequacy in pancreatic masses: a meta-analysis and systematic review. PLoS One. 2016;11(9):e0163056. doi:10.1371/journal.pone.0163056
28. Bang JY, Kirtane S, Krall K, et al. In memoriam: fine-needle aspiration, birth: fine-needle biopsy: the changing trend in endoscopic ultrasound-guided tissue acquisition. Dig Endosc. 2019;31(2):197–202. doi:10.1111/den.13280
29. Chen YA-O, Chatterjee A, Berger R, et al. Endoscopic ultrasound (EUS)-guided fine needle biopsy alone vs. EUS-guided fine needle aspiration with rapid onsite evaluation in pancreatic lesions: a multicenter randomized trial. Endoscopy. 2021;12:1438–8812.
30. Ohshima Y, Yasuda I, Kawakami H, et al. EUS-FNA for suspected malignant biliary strictures after negative endoscopic transpapillary brush cytology and forceps biopsy. J Gastroenterol. 2011;46(7):921–928. doi:10.1007/s00535-011-0404-z
31. Inamdar S, Slattery E, Bhalla R, Sejpal DV, Trindade AJ. Comparison of adverse events for endoscopic vs percutaneous biliary drainage in the treatment of malignant biliary tract obstruction in an inpatient national cohort. JAMA Oncol. 2016;2(1):112–117. doi:10.1001/jamaoncol.2015.3670
32. Kim KM, Park JW, Lee JK, Lee KH, Lee KT, Shim SG. A comparison of preoperative biliary drainage methods for perihilar cholangiocarcinoma: endoscopic versus percutaneous transhepatic biliary drainage. Gut Liver. 2015;9(6):791–799. doi:10.5009/gnl14243
33. Fohlen AA-O, Bazille C, Menahem B, et al. Transhepatic forceps biopsy combined with biliary drainage in obstructive jaundice: safety and accuracy. Eur Radiol. 2019;29(5):2426–2435. doi:10.1007/s00330-018-5852-x
34. Stewart CJ, Mills PR, Carter R, et al. Brush cytology in the assessment of pancreatico-biliary strictures: a review of 406 cases. J Clin Pathol. 2001;54(6):449–455. doi:10.1136/jcp.54.6.449
35. Lal A, Okonkwo A, Schindler S, De Frias D, Nayar R. Role of biliary brush cytology in primary sclerosing cholangitis. Acta Cytol. 2004;48(1):9–12. doi:10.1159/000326276
36. Ylagan LR, Fau LL, Maluf HM. Endoscopic bile duct brushing of malignant pancreatic biliary strictures: retrospective study with comparison of conventional smear and ThinPrep techniques. Diagn Cytopathol. 2003;28(4):196–204. doi:10.1002/dc.10267
37. Wight CO, Zaitoun AM, Boulton-Jones JR, Dunkley C, Beckingham IJ, Ryder SD. Improving diagnostic yield of biliary brushings cytology for pancreatic cancer and cholangiocarcinoma. Cytopathology. 2004;15(2):87–92. doi:10.1046/j.0956-5507.2003.00097.x
38. Al-Mofleh IA, Aljebreen AM, Al-Amri SM, et al. Biochemical and radiological predictors of malignant biliary strictures. World J Gastroenterol. 2004;10(10):1504–1507. doi:10.3748/wjg.v10.i10.1504
39. Marrelli D, Caruso S, Pedrazzani C, et al. CA19-9 serum levels in obstructive jaundice: clinical value in benign and malignant conditions. Am J Surg. 2009;198(3):333–339. doi:10.1016/j.amjsurg.2008.12.031
40. Kim HJ, Kim MH, Myung SJ, et al. A new strategy for the application of CA19-9 in the differentiation of pancreaticobiliary cancer analysis using a receiver operating characteristic curve. Am J Gastroenterol. 1999;94(7):1941–1946. doi:10.1111/j.1572-0241.1999.01234.x
41. Sheen-Chen SM, Sun CK, Liu YW, Eng HL, Ko SF, Ch K. Extremely elevated CA19-9 in acute cholangitis. Dig Dis Sci. 2007;52(11):3140–3142. doi:10.1007/s10620-006-9164-7
42. Ong SL, Sachdeva A, Garcea G, et al. Elevation of carbohydrate antigen 19.9 in benign hepatobiliary conditions and its correlation with serum bilirubin concentration. Dig Dis Sci. 2008;53(12):3213–3217.
43. Liu W, Liu Q, Wang W, et al. Differential diagnostic roles of the serum CA19-9, total bilirubin (TBIL) and the ratio of CA19-9 to TBIL for benign and malignant. J Cancer. 2018;9(10):1804–1812. doi:10.7150/jca.25093
44. La Greca G, Sofia M, Lombardo R, et al. Adjusting CA19-9 values to predict malignancy in obstructive jaundice: influence of bilirubin and C-reactive protein. World J Gastroenterol. 2012;18(31):4150–4155. doi:10.3748/wjg.v18.i31.4150
45. Tirotta F, Giovinazzo F, Hodson J, et al. Risk factors to differentiate between benign proximal biliary strictures and perihilar cholangiocarcinoma. HPB. 2020;22(12):1753–1758. doi:10.1016/j.hpb.2020.03.023
46. Choi SH, Han JK, Lee JM, et al. Differentiating malignant from benign common bile duct stricture with multiphasic helical CT. Radiology. 2005;236(1):178–183. doi:10.1148/radiol.2361040792
47. Wang S-B, Wu H-B, Wang Q-S, et al. 18F-FDG PET/CT in differentiating malignant from benign origins of obstructive jaundice. Hepatobiliary Pancreat Dis Int. 2015;14(5):516–522. doi:10.1016/S1499-3872(15)60392-7
48. Sabaté-Llobera AA-O, Gràcia-Sánchez L, Reynés-Llompart G, et al. Differences on metabolic behavior between intra and extrahepatic cholangiocarcinomas at (18) F-FDG-PET/CT:prognostic implication of metabolic parameters and tumor markers. Clin Transl Oncol. 2019;21(3):324–333. doi:10.1007/s12094-018-1926-0
49. Tang CYL, Chua WM, Cheng LTJ, Fong W, Zaheer S, Lam WW-C. 18 F-FDG PET/CT manifestations of IgG4-related disease. Br J Radiol. 2021;94:1124. doi:10.1259/bjr.20210105
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.