Back to Journals » International Journal of General Medicine » Volume 18
Predicting Infection Risk in Acute Compartment Syndrome: A Nomogram Model Based on Admission Blood Indicators
Authors Song J, Liu Y, Yang M, Li Y, Hu Y
Received 19 February 2025
Accepted for publication 23 April 2025
Published 26 May 2025 Volume 2025:18 Pages 2741—2748
DOI https://doi.org/10.2147/IJGM.S520844
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
JianJun Song,1 YueJun Liu,2 Meng Yang,3 Yan Li,1 YueYue Hu4
1Emergency ICU, Gynecology Department, Affiliated Hospital of Hebei University of Engineering, Handan, Hebei, People’s Republic of China; 2Department of Gynecology, Gynecology Department, Affiliated Hospital of Hebei University of Engineering, Handan, Hebei, People’s Republic of China; 3Department of Obstetrics and Gynaecology, Mian County People’s Hospital, Handan, Hebei, People’s Republic of China; 4Emergency Department, Gynecology Department, Affiliated Hospital of Hebei University of Engineering, Handan, Hebei, People’s Republic of China
Correspondence: YueYue Hu, Emergency Department, Gynecology Department, Affiliated Hospital of Hebei University of Engineering, Handan, Hebei, People’s Republic of China, Email [email protected]
Purpose: Acute compartment syndrome (ACS) is a serious complication after tibial fracture and it commonly needs fasciotomy, which may affect 20.4% of patients. However, the predictors of infection remain debated. Our purpose aims to explore the role of admission blood indicators in infection in ACS patients.
Methods: We collected clinical data on ACS patients between Jan. 2015 and Jan 2025. According to whether ACS patients suffer from infection or not, they were divided into two groups. We copy with these data by R language software.
Results: Based on univariate analysis, we found that time from injury to admission, time from injury to surgery, and numerous admission blood indicators were relevant to ACS, but logistic regression analysis showed that neutrophil (NEU), white blood cell (WBC), C-reactive protein (CRP) and time from injury to surgery (all p< 0.0001) were predictors for infection in ACS patients. Our nomogram prediction model with 0.995 in AUC with good consistency and good clinical practicality.
Conclusion: We found that the levels of NEU, WBC, CRP and time from injury to surgery were predictors for infection in ACS patients. Our nomogram prediction model can efficiently predict infection in ACS patients.
Keywords: acute compartment syndrome, infection, admission blood indicators, nomogram prediction model, ACS
Introduction
Tibial fracture is one of the most common traumas of lower limbs caused by various injuries.1 Acute compartment syndrome (ACS), as a severe complication after tibial fractures, usually occurs in 2–9% of patients who have suffered high-energy injuries.1 The growing pressure within the compartment can rapidly reduce capillary blood flow, which may cause muscle necrosis or even amputation.2,3 Currently, fasciotomy has been considered to be the most effective therapeutic method for ACS patients because it can quickly reduce intra-compartmental pressure and restore blood flow.4,5 However, fasciotomy can lead to 20.8–36% of patients suffering from surgical site infection (SSI), which brings a huge economic and psychological burden to the families.6–9
Ongoing articles have reported the predictors of SSI in ACS patients receiving fasciotomy. Yang found that open fractures, BMI, and smoking history were closely associated with SSI,9 but Yang did not establish the predictive model of SSI in ACS patients. Moldovan10 found the close relationship between serum biomarkers and Periprosthetic joint infection. To our knowledge, little research has focused on the predictors of SSI in ACS patients, let alone the crucial role of admission blood indicators in the diagnosis of SSI in ACS patients. Therefore, we aim to observe the role of admission blood indicators to predict SSI and then assess its potential biomarkers.
Patients and Methods
Ethics Statement
Our research was obtained by the institutional review boards of Affiliated Hospital of Hebei University of Engineering (2024–020-1) and exemption from informed consent as this is a retrospective study.
Patients
Data on ACS patients after fasciotomy in our hospital from Jan 2015 to Jan 2025. Based on whether ACS patients suffer from infection or not, they were separated into infection group (IG) and non-infection groups (NG). Diagnosis of infection is mainly based on the results of bacterial culture. The inclusion criteria were: 1) tibial fractures patients with ACS (ACS was defined as ∆P< 30 mmHg (∆P = diastolic arterial pressure-intra-compartmental pressure); 2) age ≥18 years; 3) ACS patients received fasciotomy. The exclusion criteria were: 1) patients with vascular injury; 2) patients without tibial fractures; 3) patients with insufficient data.
In our study, the patient characteristics, comorbidities, and admission laboratory results were obtained. The derived inflammatory indicators were included, such as NLR (neutrophils [NEU] count/lymphocytes count), MLR (monocytes count/lymphocytes count), PLR (platelets count/lymphocytes count), SII (platelets count × NEU count)/lymphocytes count), and SIRI (monocyte count × NEU count)/lymphocytes count)
Statistics
We used SPSS (version 27.0 SPSS Inc., Chicago, IL) to analyze the data with significance levels of p<0.05. When the continuous variables met normality criteria, we chose t-test, but if it did not met normality criteria, we used Mann–Whitney U-test. Regarding count data, we used the chi-square test. We used univariate and logistic regression analyses to analyze data. The cut-off values for continuous variables were used by the maximum Youden index (sensitivity+specificity-1) in the ROC curve analysis. Finally, we used R language software to establish the nomogram prediction model for SSI. Calibration curve and decision curve were used to assess the predicted probabilities and clinical application value, respectively.
Results
A total of 219 tibial fracture patients with ACS, including 38 with infection and 181 without infection, were included in this study. After selection based on the inclusion criteria and exclusion criteria, 14 patients with infection and 77 patients without infection were excluded (Figure 1). Finally, 24 patients with infection and 104 patients without infection were included in our study.
 |
Figure 1 Flow diagram of included patients. |
Table 1 showed that there is no difference in age, gender, BMI, mechanism of injury, open injury, blister, and muscle necrosis, as well as a history of smoking, alcohol, heart disease, hypertension, diabetes, and cerebral infarction in two groups (all p >0.05). However, we found that time from injury to admission (p<0.0001) and time from injury to surgery (p<0.0001) were closely related to SSI.
 |
Table 1 Comparison of Characteristics of ACS Patients in Two Groups |
Table 2 showed that there is no difference in the levels of hemoglobin (HGB), lymphocyte (LYM), platelet (PLT), red blood cell (RBC), PLR, and MLR in two groups (all p>0.05). However, we found that monocyte (MON, p<0.0001), NEU (p<0.0001), white blood cell (WBC, p<0.0001), total protein (TP, p<0.0001), C-reactive protein (CRP, p<0.0001), NLR (p<0.0001), SII (p<0.0001) and SIRI (p<0.0001) were closely related to SSI.
 |
Table 2 Admission Laboratory Variables Associated with Infection in ACS Patients |
Furthermore, we performed logistic regression analysis and found that the levels of NEU [p<0.0001, OR = 2.301, 95% CI (1.231, 4.353)], WBC [p<0.0001, OR = 1.669, 95% CI (1.069, 2.214)], CRP [p<0.0001, OR = 1.543, 95% CI (1.181, 2.103)] and time from injury to surgery [p<0.0001, OR = 1.213, 95% CI (1.077, 1.403)] were independent risk factors for ACS (Table 3).
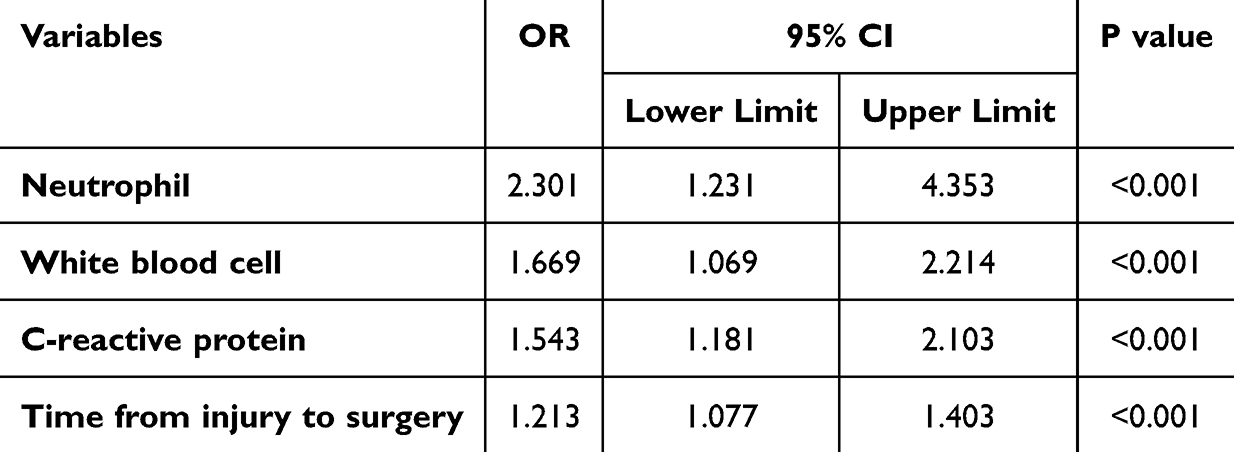 |
Table 3 Logistic Regression Analysis of Laboratory Variables Associated with Infection in ACS Patients |
We establish a nomogram prediction model according the findings of logistic regression analysis (Figure 2). ROC curve implies good discrimination ability [AUC = 0.995, 95% CI (0.990, 1.000), Figure 3] and the calibration curve shows well calibrated (p > 0.05, Figure 4). Decision curve analysis indicates our prediction model with good clinical benefits (Figure 5).
 |
Figure 2 The nomogram prediction model for ACS. |
 |
Figure 3 The receiver operating characteristic curves of the nomogram. |
 |
Figure 4 The calibration curve of the nomogram. |
 |
Figure 5 The decision curve analysis of the nomogram. |
Discussion
ACS, a common complication after tibial fractures, can result in tissue ischemia because of increased intra-compartment pressure, which may cause infection, amputation, or muscle necrosis.1–3 Recently, limited articles reported the incidence and predictors of infection in ACS patients. A previous study has reported that open fractures, BMI, and smoking history were relevant to SSI,9 but it did not use the predictive model to observe the risk factors of SSI in ACS patients. Moldovan10 found the close relationship between serum biomarkers and Periprosthetic joint infection. As far as we know, few research has focused on the predictors of SSI in ACS patients, and ignored the important role of admission blood indicators in the diagnosis of SSI in ACS patients. Thus, the purpose of this article is to investigate whether admission blood indicators can predict SSI or not. In the current study, we found that various laboratory elements were related to SSI in ACS patients by univariate analysis. Furthermore, NEU, WBC, CRP and time from injury to surgery were closely related to SSI by logistic regression analysis. Our prediction model implies good discrimination ability and good clinical benefits.
NEU is the most common type of WBC in our body and plays a crucial role in the innate immune system.11 LYM contributes to the adaptive immune system, including antibody production and cell-mediated immunity.12 MON can release pro-inflammatory and pro-oxidative cytokines against pathogens.13 PLT is mainly responsible for regulating NEU and macrophage recruitment.14 Recently, inflammation ratios have been increasingly studied, including NLR, MLR, and PLR, These indicators have some advantages, such as whole blood count, low-cost, and routine clinical examinations.15 SII, stems from NEU, LYM, and PLT, can accurately reflect the immune and inflammatory levels of the body, which has been studied in the topic on predictors for inflammation diseases.16 SIRI, derived from NUE, LYM, and MON peripheral counts, can also represent inflammation.17 To our knowledge, the relationship between these indexes and SSI in ACS patients has not been studied.
In this study, our findings indicated that the levels of MON, NEU, WBC, TP, CRP, NLR, SII, and SIRI were associated with SSI in univariate analysis. Furthermore, logistic regression analysis indicated that the levels of NEU, WBC, and CRP were independent risk factors for SSI. Yang9 found, a significant correlation between NEU and SSI in univariate analysis, but in multivariate analysis, no significant correlation was found, which is inconsistent with our results and may be due to differences between samples. Therefore, we need large sample data for further research in future studies. As we know, CRP is an important indicator of inflammation levels in the body. Our study found that patients with elevated CRP have a 1.543 times higher risk of SSI after fasciotomy compared to patients with normal CRP levels.
Previous studies have demonstrated that smoking and high BMI were risk factors for SSI. Yang9 also found that these two factors are closely related to SSI, but our study did not find such results. We consider that this may still be related to the differences in the samples. We also investigated the correlation time from injury to admission, time from injury to surgery, and SSI. The results of univariate analysis showed that both were related to SSI, but the results of multivariate analysis only found a significant correlation between injury to surgery time and SSI. As is well known, 6–8 hours after injury is the early stage of treatment. When ACS occurs, high pressure in the compartment leads to tissue ischemia, and delayed treatment can cause muscle necrosis or even amputation. Therefore, the longer the time from injury to surgery, the longer the tissue ischemia time, and the higher the risk of natural tissue necrosis and infection.
Our prediction model to evaluate SSI in ACS patients. The ROC curve suggested good discrimination ability, and the calibration curve showed well calibrated. Decision curve analysis showed our nomogram prediction model with good clinical benefits. Although our study provides some innovative findings, a few limitations should be noted. First, single-center research and limited samples make it difficult to perform a subgroup analysis, which inevitably affects the reliability of the findings. Therefore, a multicenter, randomized controlled study with a larger sample size is required. Second, the inherent boundedness of data collection caused by a retrospective study causes some important inflammatory markers.
In conclusion, We found that the levels of NEU, WBC, CRP and time from injury to surgery were predictors for infection in ACS patients. Our nomogram prediction model can efficiently predict infection in ACS patients.
Data Sharing Statement
The datasets used and/or analysed during the current study available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
Before data collection, this study was approved by the institutional review boards of Affiliated Hospital of Hebei University of Engineering (2024-020-1) in compliance with the Helsinki and an exemption from the informed consent was obtained. All data were anonymized before the analysis to safeguard patient privacy.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors report no competing interests in this work.
References
1. Wang T, Guo J, Long Y, Hou Z. Predictors of acute compartment syndrome in patients with tibial fractures: a meta-analysis. Int Orthop. 2023;47(1):51–65. doi:10.1007/s00264-022-05643-3
2. Wang T, Yang S, Guo J, Long Y, Hou Z. Predictors of muscle necrosis in patients with acute compartment syndrome. Int Orthop. 2023;47(4):905–913. doi:10.1007/s00264-023-05699-9
3. Wang T, Zhang Q, Hou Z. Predictors of amputation in patients with acute compartment syndrome after tibial fracture: a nomogram prediction model. J Orthop Surg Res. 2024;19(1):783. doi:10.1186/s13018-024-05259-w
4. Guo J, Yin Y, Jin L, Zhang R, Hou Z, Zhang Y. Acute compartment syndrome: cause, diagnosis, and new viewpoint. Medicine. 2019;98(27):e16260. doi:10.1097/MD.0000000000016260
5. Mafulli N, Loppini M, Spiezia F, D’Addona A, Mafulli GD. Single minimal incision fasciotomy for chronic exertional compartment syndrome of the lower leg. J Orthop Surg Res. 2016;11(1):61. doi:10.1186/s13018-016-0395-9
6. Wesslen C, Wahlgren CM. Contemporary management and outcome after lower extremity fasciotomy in non-trauma-related vascular surgery. Vasc Endovasc Surg. 2018;52(7):493–497. doi:10.1177/1538574418773503
7. Hake ME, Etscheidt J, Chadayammuri VP, Kirsch JM, Maufrey C. Age and dressing type as independent predictors of postoperative infection in patients with acute compartment syndrome of the lower leg. Int Orthop. 2017;41(12):2591–2596. doi:10.1007/s00264-017-3576-1
8. Whitesides TE, Heckman MM. Acute compartment syndrome: update on diagnosis and treatment. J Am Acad Orthop Surg. 1996;4(4):209–218. doi:10.5435/00124635-199607000-00005
9. Yang S, Long Y, Wang T, Guo J, Hou Z. Predictors for surgical site infection after fasciotomy in patients with acute leg compartment syndrome. J Orthop Surg Res. 2023;18(1):98. doi:10.1186/s13018-023-03589-9
10. Moldovan F. Role of serum biomarkers in differentiating periprosthetic joint infections from aseptic failures after total hip arthroplasties. J Clin Med. 2024;13(19):5716. doi:10.3390/jcm13195716
11. Imran MM, Ahmad U, Usman U, Ali M, Shaukat A, Gul N. Neutrophil/lymphocyte ratio-a marker of COVID-19 pneumonia severity. Int J Clin Pract. 2021;75:e13698. doi:10.1111/ijcp.13698
12. Pfau ML, Menard C, Russo SJ. Inflammatory mediators in mood disorders: therapeutic opportunities. Annu Rev Pharmacol Toxicol. 2018;58:411–428. doi:10.1146/annurev-pharmtox-010617-052823
13. Murphy AJ, Woollard KJ, Suhartoyo A, et al. Neutrophil activation is attenuated by high-density lipoprotein and apolipoprotein A-I in in vitro and in vivo models of inflammation. Arterioscler Thromb Vasc Biol. 2011;31:1333–1341. doi:10.1161/ATVBAHA.111.226258
14. Pogorzelska K, Kretowska A, Krawczuk-Rybak M, Sawicka-Zukowska M. Characteristics of platelet indices and their prognostic significance in selected medical condition-a systematic review. Adv Med Sci. 2020;65:310–315. doi:10.1016/j.advms.2020.05.002
15. Zulfific Z, Weickert CS, Weickert TW, Liu D, Myles N, Galletly C. Neutrophil–lymphocyte ratio–a simple, accessible measure of inflammation, morbidity and prognosis in psychiatric disorders? Australas Psychiatry. 2020;28:454–458. doi:10.1177/1039856220908172
16. Liu X, Guan G, Cui X, Liu Y, Liu Y, Luo F. Systemic immune-inflammation index (SII) can be an early indicator for predicting the severity of acute pancreatitis: a retrospective study. Int J Gen Med. 2021;14:9483–9489. doi:10.2147/IJGM.S343110
17. Cakir N, Koc AN. Gamma-glutamyl transpeptidase-platelet ratio, systemic immune inflammation index, and system inflammation response index in invasive aspergillosis. Rev Assoc Med Bras. 2021;67:1021–1025. doi:10.1590/1806-9282.20210475
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.