Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 18
Predicting HbA1c Target Achievement in Type 2 Diabetes: A Retrospective Single-Centre Nomogram Derived From National MMC-Standardised Management
Authors Lu M, Zhou H, Liu Y, Song J, Lu X, Liu Y
Received 12 May 2025
Accepted for publication 6 September 2025
Published 22 September 2025 Volume 2025:18 Pages 3589—3600
DOI https://doi.org/10.2147/DMSO.S535766
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Ernesto Maddaloni
Ming Lu,* Hua Zhou,* Yanxing Liu, Juanjuan Song, Xiaolin Lu, Yan Liu
Department of Endocrinology, The Third People’s Hospital of Datong, Datong, Shanxi, 037000, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yan Liu, Department of Endocrinology, The Third People’s Hospital of Datong, No. 1 Wenchang Street, Datong, Shanxi, 037000, People’s Republic of China, Tel +86-13994393959, Email [email protected]
Background: This study assessed the effectiveness of standardized management implemented by the National Metabolic Management Center (MMC) for patients with type 2 diabetes. The goal was to develop a nomogram for predicting HbA1c target achievement.
Methods: A retrospective single-centre study was conducted, including 853 type 2 diabetes patients enrolled in the National Standardized Metabolic Disease Management Center at the Third People’s Hospital of Datong City from June 2019 to June 2020. After one year of MMC’s standardized management, factors influencing HbA1c achievement were identified through univariate and multivariate analyses to establish a predictive model. Missing data were handled using appropriate imputation methods. Model accuracy and performance were assessed using internal validation and ROC curve analysis.
Results: Significant improvements were observed following MMC’s standardized management, including reductions in SBP, FBG, Hb, HCT, MPV, γ-GT, ALB, TG, TC, HbA1c, and LDL-c levels (P< 0.05), and increases in AST, BUN, Cr, UA, and HDL-c levels (P< 0.05). The absolute HbA1c level decreased, and the rate of achieving the HbA1c target (< 7%) was significantly enhanced (P< 0.05). Multivariate analysis identified FBG and HCT as independent protective factors for HbA1c achievement, while ALB was a risk factor. The developed predictive model exhibited favorable discriminative ability (c-index: 0.747, 95% CI: 0.703– 0.790), confirmed by decision curve analysis.
Conclusion: Standardized MMC management may guide care for type 2 diabetes patients. The predictive model established in this study may assist in improving HbA1c achievement rates, although external validation is needed.
Keywords: type 2 diabetes, HbA1c, national metabolic management center, personalized predictive model, internal validation
Introduction
The global prevalence of diabetes is on the rise, driven by factors such as population aging, sedentary lifestyles, and high-calorie diets.1,2 According to the International Diabetes Federation (IDF), the number of adults living with diabetes worldwide is projected to surpass 642 million by 2040.3 Research indicates that the prevalence of diabetes among Chinese adults stands at a staggering 10.9%, yet less than one-third of individuals are aware of their condition and receive appropriate glucose-lowering therapy. Furthermore, among those undergoing treatment, fewer than 50% achieve the target glycated hemoglobin level of ≤7%.4 Inadequate blood glucose control in diabetes patients can lead to the excessive generation of reactive oxygen species, triggering apoptosis of pancreatic β cells and the onset of complications in the cardiovascular, renal, retinal, and nervous systems. These complications significantly impact quality of life and reduce life expectancy.5,6 Hence, early detection and standardized management of diabetes and its associated complications are crucial for improving patient outcomes.
As a pivotal platform driving the management of chronic metabolic diseases, the National Standardized Metabolic Disease Management Center (MMC) has pioneered a “one-stop treatment, comprehensive management” approach. Established in 2016, MMC centers have revolutionized the management of diabetes, with digital medical information systems extending care beyond hospital walls through apps, WeChat, and phone communication. Currently, numerous hospitals nationwide have adopted MMC protocols, improving diabetes management and reducing complications.7,8 Despite these advancements, achieving HbA1c targets in MMC-managed patients remains sub-optimal, with fewer than half reaching the target level of ≤7%.9
Several HbA1c-prediction tools, such as the UKPDS risk engine and electronic health-record models, have been developed for other populations, but they are not suitable for MMC-managed Chinese cohorts due to differences in healthcare delivery models and patient characteristics. The use of fasting glucose (FBG), hematocrit (HCT), and albumin (ALB) as potential predictors of HbA1c achievement is warranted based on their strong associations with glucose metabolism and vascular health.10,11 These biomarkers have been shown to impact blood glucose control, yet their role in predicting HbA1c attainment in the context of MMC management is not well understood.12
The MMC model differs from conventional care through more frequent contacts, digital monitoring, and multidisciplinary input. This model’s widespread adoption across China has demonstrated national impact, significantly improving diabetes management outcomes.13,14 To better understand and predict HbA1c attainment, we aim to develop an individualized predictive model that integrates baseline clinical variables.
The primary hypothesis of this study is that a nomogram incorporating baseline clinical variables will accurately predict 1-year HbA1c control in MMC-managed adults, providing insights for personalized care and management.
Methods
Patients
From June 2019 to June 2020, a total of 853 patients with type 2 diabetes who received standardized management at the Third People’s Hospital of Datong City MMC were included in the study. Inclusion criteria:15 (1) meeting the 1999 World Health Organization (WHO) diagnostic and classification criteria for type 2 diabetes; (2) aged between 18 and 75 years, regardless of gender; (3) willing to undergo standardized metabolic disease management, having good compliance with follow-up, and able to adhere to regular follow-up for at least 5 years; (4) possessing a certain level of learning ability, with patients and their family members able to accept follow-up via phone or WeChat, without cognitive or communication impairments, and capable of normal communication; (5) local residents with a residency of at least 5 years in the Datong area; (6) patients who are informed and have signed an informed consent form. Exclusion criteria:15 (1) expected survival time less than 5 years; (2) history of drug abuse or substance abuse; (3) active viral hepatitis, HIV/AIDS, syphilis, and other sexually transmitted diseases, as well as active tuberculosis and other infectious diseases; (4) type 1 diabetes; (5) type 2 diabetes with acute complications; (6) other special types of diabetes; (7) pregnancy status. The study was approved by The Third People’s Hospital of Datong review board, and written informed consent was obtained before participation. This study was conducted in accordance with the Declaration of Helsinki.
Management Approach
The MMC management model9 was adopted in this study: patients entering the standardized metabolic disease management center were uniformly followed up at the Endocrinology Department’s MMC clinic in our hospital, where they underwent diagnosis, treatment, and follow-up according to the MMC standard operating procedures (SOP), including screening and treatment of diabetes-related complications. Utilizing the MMC App platform facilitated communication and interaction between doctors and patients, as well as seamless information exchange between within and outside the hospital, enabling standardized management and intervention through the metabolic disease management center platform. All 853 patients in this study received standardized MMC management for one year.
Data Collection
Patient history was collected, and baseline measurements of blood pressure (SBP, DBP), body mass index (BMI) were recorded. Visceral fat and subcutaneous fat were measured using a bioelectrical impedance analysis instrument. Fasting venous blood samples were collected for the measurement of HbA1c, red blood cell indices (Hb, MCV, MCH, HCT), liver function indices (ALT, AST, ALP, γ-GT), renal function indices (BUN, Cr, UA), lipid profile (TG, TC, HDL-c, LDL-c), blood glucose level (FBG), albumin (ALB), and mean platelet volume (MPV).
Statistical Analysis
We calculated the median, mean, and interquartile range for all continuous outcomes, and determined the frequency count and percentage for categorical outcomes. Continuous outcomes were assessed using the Mann–Whitney U-test, while categorical variables were analyzed using χ2 or appropriate Fisher exact tests. The final results of the multivariable logistic regression were utilized to develop nomograms with the rms package in R software. The discriminatory performance of the nomograms was quantitatively evaluated using the c-index. Calibration plots were generated to visually compare predicted and actual risks. Internal validation and calibration validation of the models were conducted through 1000 bootstrapped resamples. DCA was performed to assess the clinical utility of the nomograms in predicting risks.
Results
Comparison of Treatment Efficacy in Patients Following One Year of Standardized Management
A cohort of 853 individuals diagnosed with type 2 diabetes, who were admitted to the National Standardized Metabolic Disease Management Center (MMC) at the Third People’s Hospital in Datong City between June 2019 and June 2020, were included in this study. The study aimed to evaluate the effectiveness of standardized management provided by MMC over a one-year period. No statistically significant differences (P>0.05) were observed in DBP, BMI, visceral fat, subcutaneous fat, MCV, MCH, ALT, and ALP levels before and after the treatment period. However, SBP, FBG, Hb, HCT, MPV, γ-GT, ALB, TG, TC, HbA1c, and LDL-c exhibited a significant decreasing trend following standardized management by MMC (P<0.05). Conversely, AST, BUN, Cr, UA, and HDL-c showed a significant increasing trend post standardized management by MMC (P<0.05) (Table 1).
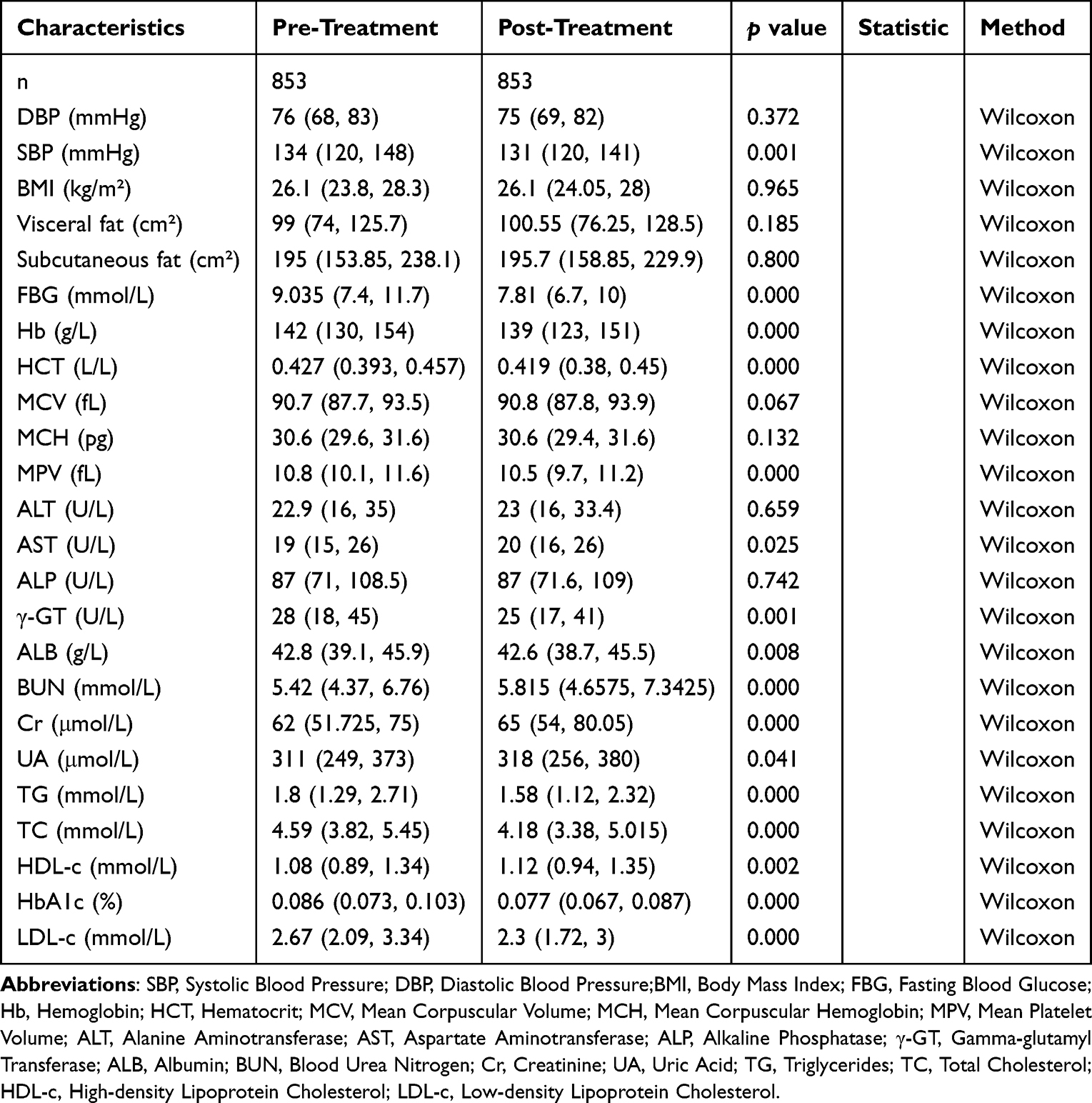 |
Table 1 Comparison of Various Indicators in Type 2 Diabetes Patients After One year of Standardized Management |
Comparison of HbA1c and Blood Lipid Control Rates in Type 2 Diabetes Patients After 1 Year of Standardized Management
Following 1 year of adherence to the guidelines outlined in the Medical Management of Diabetes Care (MMC), a cohort of 853 individuals with type 2 diabetes exhibited notable improvements in HbA1c control, with a rate of 30.5%. Additionally, the control rates for TG and TC were reported at 56.3% and 59.9%, respectively. These rates demonstrated a significant increase compared to the pre-implementation period of MMC standardized management (P<0.05) (Table 2).
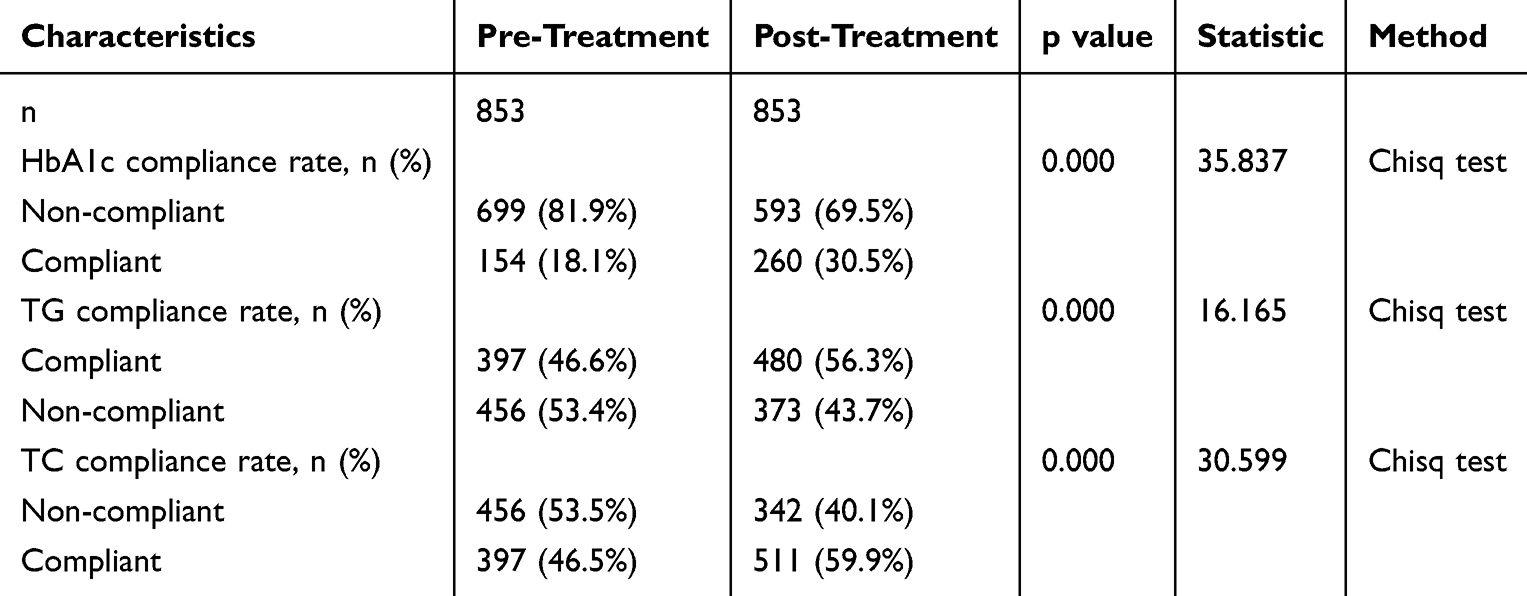 |
Table 2 Rate of Achieving Target Indicators in Type 2 Diabetes Patients After One year of Standardized Management |
Single-Factor Analysis of HbA1c Reaching Standard After One year of Standardized Management
A total of 853 patients with type 2 diabetes were categorized into two groups based on their attainment of the HbA1c target: compliant group and non-compliant group. The study found no statistically significant differences (P>0.05) in DBP, SBP, BMI, visceral fat, subcutaneous fat, Hb, MCV, MPV, ALT, AST, ALP, γ-GT, BUN, TC, HDL-c, and LDL-c between the two groups. However, statistically significant differences (P<0.05) were observed in FBG, HCT, MCH, ALB, Cr, UA, TG, and region between compliant group and Non-compliant group. The compliant group exhibited a significant decrease in FBG, HCT, and TG levels, while showing an increase in MCH, ALB, Cr, and UA levels. Additionally, the study revealed that the rate of achieving the target HbA1c level was higher in urban areas compared to rural areas (Table 3).
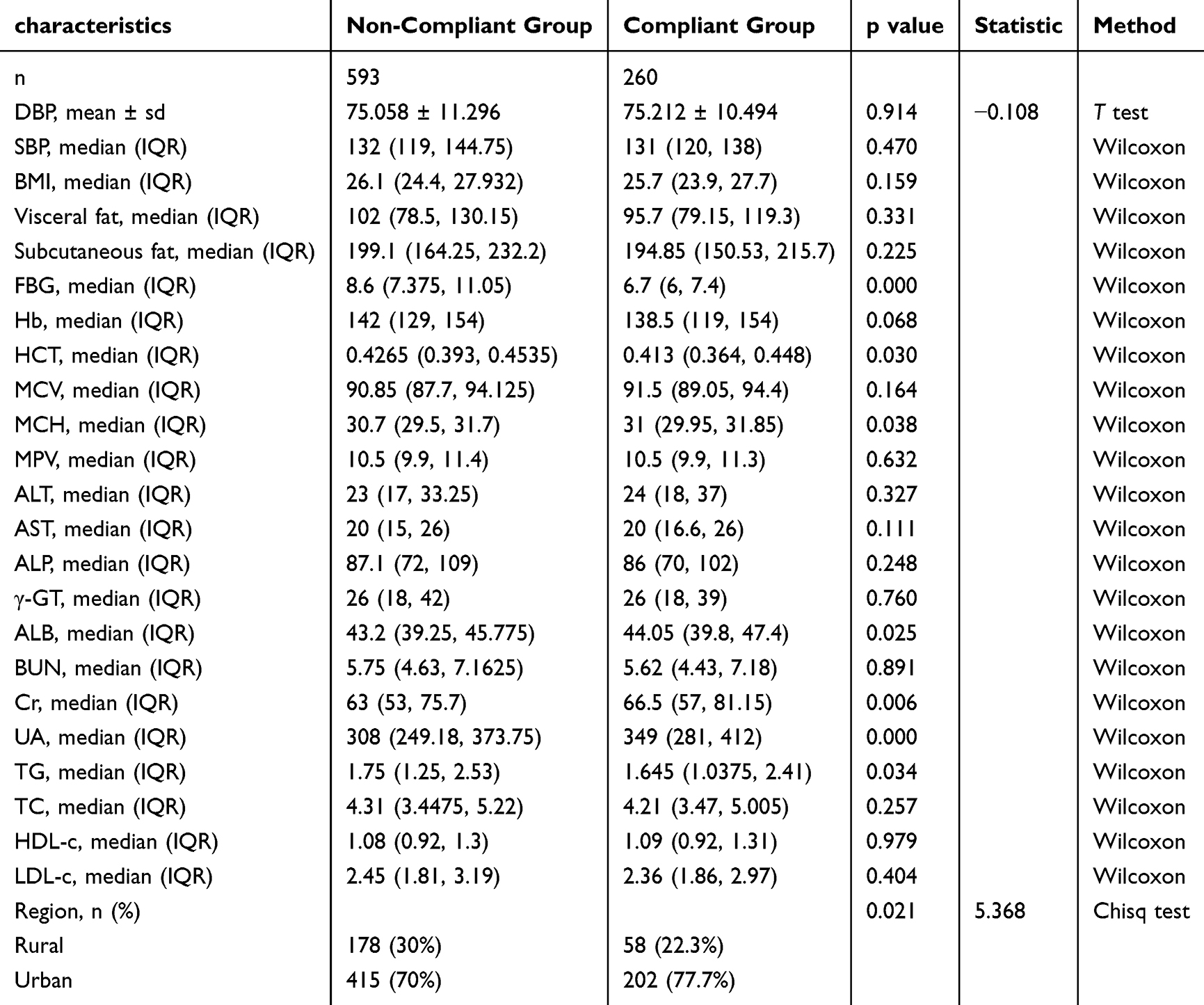 |
Table 3 Correlation Between Baseline Characteristics of Type 2 Diabetes Patients and Probability of Achieving HbA1c Target After One year of Standardized Management |
Development of an Individualized Prediction Model
The achievement of standard HbA1c levels was considered as the dependent variable, while the differential factors (FBG, HCT, MCH, ALB, Cr, UA, TG, Region) identified through single-factor analysis were treated as independent variables in a multiple logistic regression analysis. The results, as shown in Table 4, indicated that FBG and HCT were independent protective factors for reaching standard HbA1c levels (P<0.05), while ALB was an independent risk factor for standard HbA1c levels (P<0.05). A model incorporating these independent predictive factors was established and represented using a line graph (Figure 1).
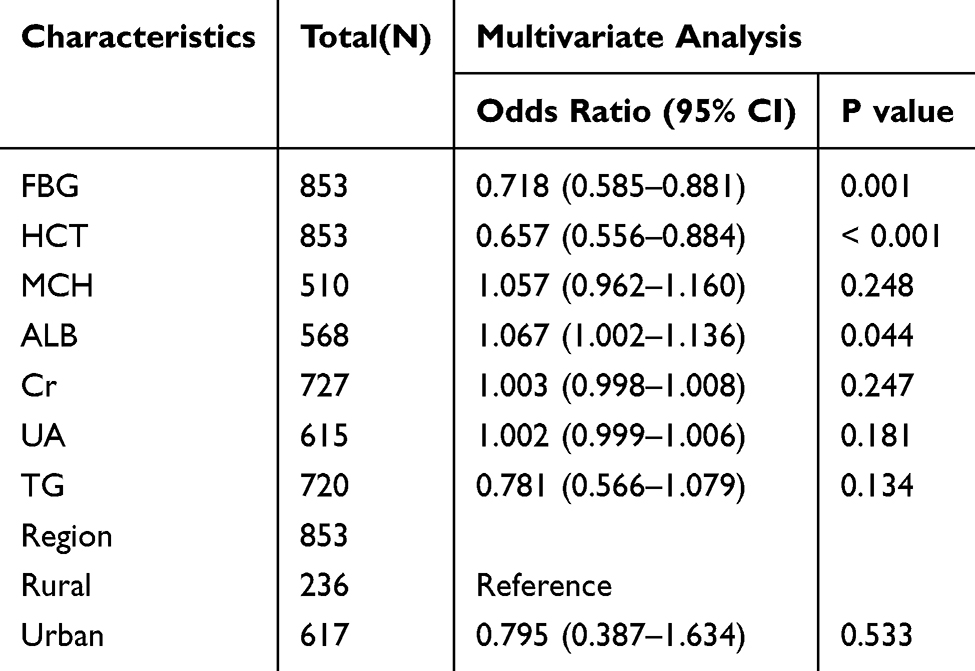 |
Table 4 Multifactor Logistic Regression Analysis of Factors Influencing HbA1c Target Achievement |
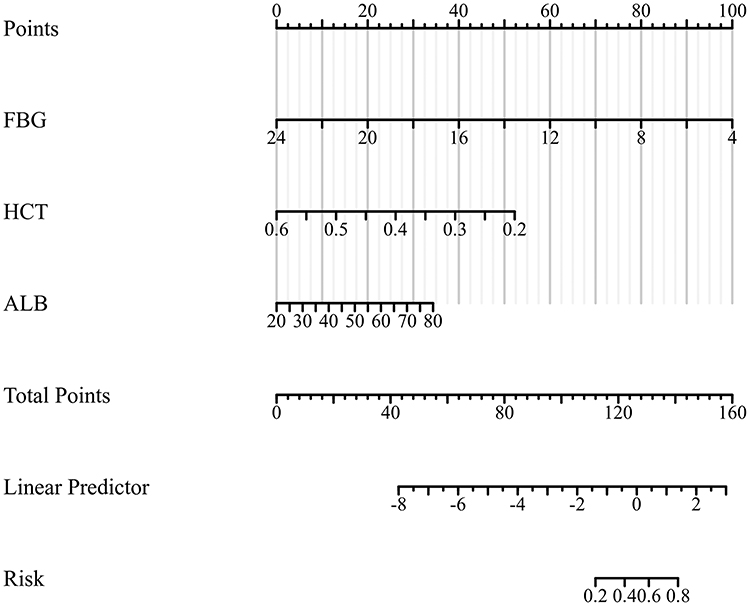 |
Figure 1 Predictive nomogram model for HbA1c target achievement based on multivariable logistic regression analysis. |
Validation of Nomogram
Using bootstrapping technique with 1000 samples for internal validation, the results, as shown in Figure 2, revealed a Harrell C-Index of 0.747 (0.703–0.791). The derived model demonstrated good calibration, with a Hosmer-Lemeshow test chi-square value of 10.852 and P=0.210, indicating good predictive accuracy. As depicted in Figure 3, the ROC of the prediction column plot was 0.747 (95% CI 0.703–0.790), suggesting good discrimination. Based on the results in Figure 4, the model exhibited good clinical predictive performance.
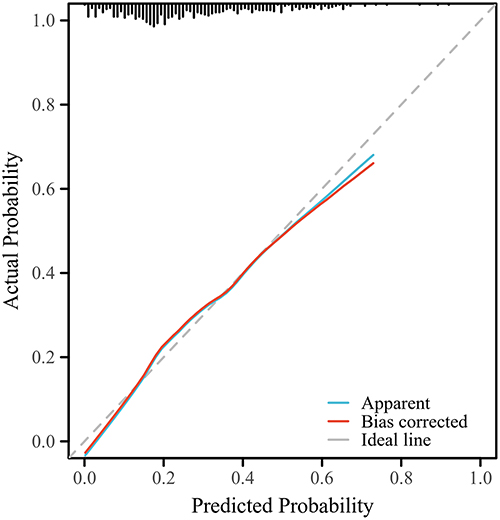 |
Figure 2 Calibration curve for the nomogram model. |
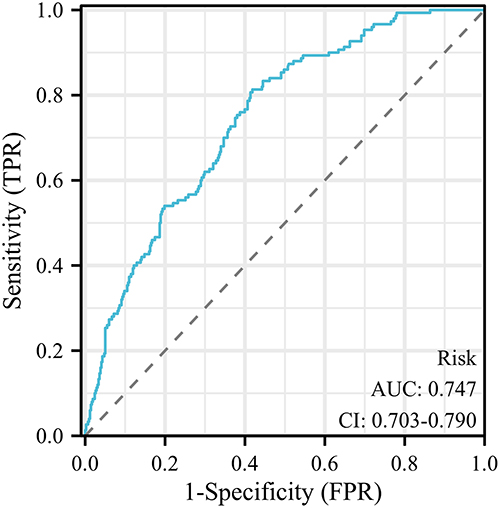 |
Figure 3 ROC curve for the nomogram model. |
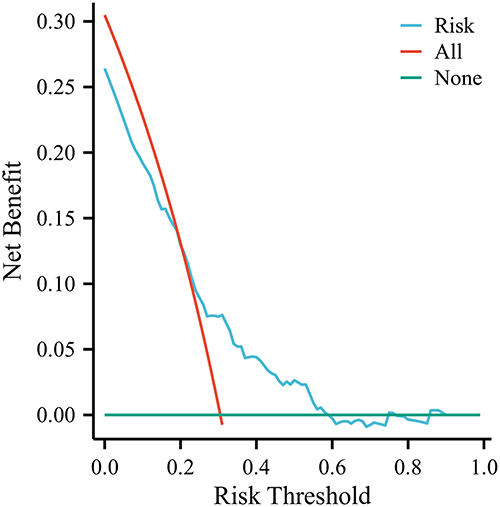 |
Figure 4 Decision curve analysis for the nomogram model. |
Discussion
Diabetes is a widespread disease that has garnered significant investments from governments and families, yet the management of the disease remains suboptimal. Even in developed nations, the rate of diabetes control meeting established standards has not surpassed 50%.16 Inadequate blood glucose control in diabetic patients can result in various acute and chronic complications.17 Research has demonstrated that the implementation of standardized management protocols based on Multidisciplinary Medical Care (MMC) can effectively regulate metabolic parameters in individuals with pancreatic dysfunction.7 The objective of this investigation is to develop and validate a personalized predictive model for attaining HbA1c targets in individuals with type 2 diabetes. By conducting a comparative analysis of the efficacy and changes in indicators among 853 patients following one year of MMC standardized management, our goal is to investigate the influence of MMC management on patients’ physiological parameters, blood glucose levels, and lipid profiles, as well as the alterations in HbA1c target attainment rates and associated factors.
Diabetes is a common risk factor for cardiovascular diseases. According to data from the China Cardiovascular Metabolic Disease Registry (CCMR) - 3B,18 the incidence of ischemic heart disease and cerebrovascular disease in Chinese patients with type 2 diabetes combined with dyslipidemia significantly increased to 14.6%. Furthermore, studies have shown19 that long-term intensive treatment of diabetes patients significantly reduces blood pressure and lipid metabolism levels, thereby reducing the risk of cardiovascular and microvascular events. According to the latest “Chinese Type 2 Diabetes Prevention and Treatment Guidelines” (2020 edition), a rational treatment strategy for type 2 diabetes should involve comprehensive management, including control of blood glucose, blood pressure, blood lipids, and weight, with lifestyle management guidance being long-term and individualized. However, the current diabetes management models in China have certain limitations, whether they are hospital-centered, community-centered, or mobile medical management models. In this context, Mobile Medical Care (MMC) as a simplified and cost-effective diabetes management model has attracted attention. In multiple regions such as Dalian, Zhengzhou, Shanghai, Ningbo, etc., after undergoing MMC management, patients have shown significant improvements in blood glucose, blood lipid levels, and self-management capabilities. In our hospital, under the MMC management model, tailored educational approaches have been adopted based on the characteristics of Datong area, particularly targeting rural residents. Through methods such as pictures, short videos, distributing small gifts, and face-to-face communication, we work with patients to develop exercise and dietary plans, and teach insulin injection methods. By following the MMC Housekeeper WeChat public account, family members can join the diabetes management platform to better understand the patient’s blood pressure, blood glucose, and other conditions. Doctors can promptly access the patient’s various indicators through the MMC platform, make adjustment plans as needed, thereby enhancing patient compliance with proper diet, blood glucose monitoring, and regular exercise.
In this study, we conducted a one-year efficacy comparison of standardized management of 853 type 2 diabetes patients with MMC. The results demonstrated a significant impact of MMC standardized management on the efficacy of type 2 diabetes patients. Specifically, lowered indicators such as SBP, FBG, and HbA1c were closely associated with the control and management of diabetes. Hypertension is a common complication in diabetes patients,20 and MMC standardized management effectively improved patients’ blood pressure and blood glucose levels through comprehensive intervention measures including medication, dietary control, and exercise guidance, thereby reducing the risk of cardiovascular events and diabetes complications. HbA1c is a key indicator for evaluating long-term blood glucose control in diabetes.21 Following MMC standardized management, a significant decrease in HbA1c levels in patients indicated that MMC could effectively improve patients’ blood glucose control levels. This result is closely related to factors such as rigorous blood glucose monitoring, personalized treatment plans, and patient education provided by MMC. The study suggests that in type 2 diabetes patients, the occurrence of diabetes complications is significantly associated with hyperglycemia, and a decrease in HbA1c levels can significantly reduce the risk of complications (such as retinopathy, nephropathy, and cardiovascular diseases).22,23
The UK Prospective Diabetes Study (UKPDS) has shown that a 1% reduction in HbA1c can decrease the probability of diabetes-related endpoints by 21%, reduce the risk of diabetes-related mortality by 21%, and lower the risk of microvascular complications by 37%.22 Therefore, early glycemic control through inclusion in a Multidisciplinary Management Clinic (MMC) can significantly reduce the occurrence of both macrovascular and microvascular complications in diabetes patients. Following MMC management, levels of TG, TC, and LDL-c have significantly decreased, while HDL-c has shown an increasing trend. These changes indicate that MMC effectively improves patients’ lipid metabolism, reducing the risk of atherosclerosis and cardiovascular events. Lipid abnormalities are common metabolic disorders in diabetic patients, posing a serious threat to cardiovascular health.24 Furthermore, our study found that after standardized MMC management for one year, there was a significant improvement in the achievement rates of HbA1c, TG, and TC targets in type 2 diabetes patients, demonstrating that MMC management effectively enhances patients’ glycemic and lipid control levels, reducing disease risk and improving quality of life, consistent with previous research findings.9 Therefore, by controlling lipid levels, MMC helps reduce the cardiovascular disease risk in diabetes patients. Additionally, elevated markers such as AST, BUN, and Cr reflect the impact of standardized MMC management on liver and kidney function. Diabetes patients often have liver and kidney function abnormalities,25,26 and the comprehensive interventions of standardized MMC management may stimulate liver and kidney function, leading to the elevation of these markers. However, these changes may be temporary and require long-term follow-up and monitoring.
Type 2 diabetes mellitus (T2DM) is a common chronic metabolic disease, and one of the key goals in its management is to reduce HbA1c levels to decrease the risk of complications.27 In this study, we analyzed the results of 853 T2DM patients who underwent one year of standardized management at the National Metabolic Management Center (MMC), and found differences in several baseline characteristics and biochemical markers between the group that achieved target HbA1c levels and the group that did not. These differences may have influenced the rate of achieving target HbA1c levels. The study results showed a significant decrease in FBG levels in the group that achieved target HbA1c levels. Good glycemic control is one of the key factors for T2DM patients to achieve target levels. FBG, as a representative of fasting blood glucose levels, has a significant impact on achieving target HbA1c levels. The study suggests that controlling FBG levels can effectively lower HbA1c levels, thereby improving the management of diabetes in patients.28 Low FBG levels may reflect effective medication therapy and dietary control in MMC standardized management, promoting glucose stability. The group that achieved target HbA1c levels also showed a significant decrease in HCT. HCT is a measure of the proportion of red blood cells in the blood, and its decrease may reflect the impact of MMC management on patient blood circulation. Some studies29–31 suggest that T2DM patients are at risk of anemia, and the decrease in HCT may be related to blood glucose control and medication therapy in MMC management. High HCT levels may indicate dehydration or blood concentration in patients, which could affect the stability of glucose metabolism.32
Meanwhile, ALB levels exhibited a significant increase in the group achieving the target HbA1c levels. Albumin, a vital protein in the body, may reflect an enhancement in the nutritional status of patients undergoing comprehensive metabolic control (CMC) management. Optimal nutritional status plays a pivotal role in maintaining metabolic equilibrium and averting complications in individuals with T2DM. The levels of albumin in diabetic individuals are frequently influenced by renal function and nutritional status.33 Decreased albumin levels could signify malnutrition or renal dysfunction, potentially leading to instability in blood glucose metabolism and impacting the attainment of HbA1c targets.34 Conversely, there was a notable decreasing trend in TG levels among individuals meeting the HbA1c targets. TG serves as an independent factor contributing to the risk of cardiovascular disease in patients with T2DM, and its reduction may be linked to therapeutic interventions targeting lipid abnormalities in CMC management. This underscores that standardized CMC management not only aids in glycemic control but also enhances the lipid metabolism profile of patients. Recent investigations35,36 have highlighted that the geographical location (urban versus rural) independently influences blood glucose regulation, with urban dwellers exhibiting higher rates of achieving glycemic targets compared to their rural counterparts. Studies have indicated a higher prevalence and awareness of diabetes in urban settings than in rural areas.35 Our research unveiled a higher rate of HbA1c target attainment in urban regions compared to rural locales, potentially attributed to the differential healthcare resources accessible to urban and rural populations.
Conclusions
In this study, we have developed a personalized predictive model aimed at forecasting the achievement of HbA1c targets one year after standardized management at the National Metabolic Management Center (MMC) in individuals diagnosed with type 2 diabetes mellitus. Using univariate analysis, we identified several factors, including FBG, HCT, MCH, ALB, Cr, UA, TG, and Region, and selected FBG and HCT as independent protective factors for achieving HbA1c targets, while ALB emerged as an independent risk factor. We constructed a predictive model based on these variables and validated it using internal validation and bootstrapping techniques, demonstrating strong calibration and predictive accuracy.
Despite these promising results, the study has several limitations. Firstly, it is a single-center, retrospective study with a relatively small sample size, which may introduce selection bias. Additionally, other potential influencing factors were not considered in the model, and the HCT variable was initially coded incorrectly, which may have impacted the results. Further external validation and comparison with simpler benchmarks, such as baseline HbA1c, are required to confirm the clinical utility of this model. Moreover, future research should focus on expanding the sample size, adopting a multicenter design, and evaluating additional variables to enhance predictive accuracy. Given the observed post-MMC rises in renal and liver markers, further investigation is necessary to understand their implications for long-term clinical outcomes. Therefore, while our model demonstrates potential, its practical utility and clinical application remain pending external validation.
Abbreviations
IDF, International Diabetes Federation; National Standardized Metabolic Disease MMC, Management Center; HbA1c, glycated hemoglobin; WHO, World Health Organization; SOP, standard operating procedures; BMI, body mass index; TC, total cholesterol; TG, triglycerides; DCA, decision curve analysis; CCMR, China Cardiovascular Metabolic Disease Registry; MMC, Mobile Medical Care; UKPDS, UK Prospective Diabetes Study; MMC, Multidisciplinary Management Clinic; T2DM, type 2 diabetes mellitus; CMC, comprehensive metabolic control.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Informed Consent
The study was approved by The Third People Hospital of Datong review board, and written informed consent was obtained before participation. This study was conducted in accordance with the Declaration of Helsinki.
Author Contributions
YL, HZ and ML performed experiments, analyzed data, and wrote the manuscript. YXL, JJS, XLL, HZ and ML interpreted results. YL designed study, and approved the final manuscript. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors have no conflicts of interest to declare for this work.
References
1. Glovaci D, Fan W, Wong ND. Epidemiology of diabetes mellitus and cardiovascular disease. Curr Cardiol Rep. 2019;21(4):21. doi:10.1007/s11886-019-1107-y
2. Amiel SA, Aschner P, Childs B. International Hypoglycaemia Study Group. Hypoglycaemia, cardiovascular disease, and mortality in diabetes: epidemiology, pathogenesis, and management. Lancet Diabetes Endocrinol. 2019;7(5):385–396. doi:10.1016/S2213-8587(18)30315-2
3. Zheng Y, Ley SH, Hu FB. Global aetiology and epidemiology of type 2 diabetes mellitus and its complications. Nat Rev Endocrinol. 2018;14(2):88–98. doi:10.1038/nrendo.2017.151
4. Wang L, Gao P, Zhang M, et al. Prevalence and ethnic pattern of diabetes and prediabetes in China in 2013. JAMA. 2017;317(24):2515–2523. doi:10.1001/jama.2017.7596
5. Volpe CMO, Villar-Delfino PH, Dos Anjos PMF, Nogueira-Machado JA. Cellular death, reactive oxygen species (ROS) and diabetic complications. Cell Death Dis. 2018;9(2):119. doi:10.1038/s41419-017-0135-z
6. Panigrahy SK, Bhatt R, Kumar A. Reactive oxygen species: sources, consequences and targeted therapy in type 2 diabetes. J Drug Target. 2017;25(2):93–101. doi:10.1080/1061186X.2016.1207650
7. Zhang Y, Wang W, Ning G. Metabolic management center: an innovation project for the management of metabolic diseases and complications in China. J Diabetes. 2019;11(1):11–13. doi:10.1111/1753-0407.12847
8. Gu L, Ma Y, Zheng Q, et al. The effects of economic status on metabolic control in type 2 diabetes mellitus at 10 metabolic management centers in China. J Diabetes. 2024;16(1):e13466. doi:10.1111/1753-0407.13466
9. Wang X, Zhao W, Ke J, Zhao D. Comparison and analyses of therapeutic effects between metabolic management center (MMC) and conventional management modes. Acta Diabetol. 2020;57(9):1049–1056. doi:10.1007/s00592-020-01518-4
10. Jia W. Standardising HbA1c-based diabetes diagnosis: opportunities and challenges. Expert Rev Mol Diagn. 2016;16(3):343–355. doi:10.1586/14737159.2016.1133299
11. Yazdanpanah S, Rabiee M, Tahriri M, et al. Evaluation of glycated albumin (GA) and GA/HbA1c ratio for diagnosis of diabetes and glycemic control: a comprehensive review. Crit Rev Clin Lab Sci. 2017;54(4):219–232. doi:10.1080/10408363.2017.1299684
12. Echouffo-Tcheugui JB, Perreault L, Ji L, Dagogo-Jack S. Diagnosis and management of prediabetes: a review. JAMA. 2023;329(14):1206–1216. doi:10.1001/jama.2023.4063
13. Ceriello A, Monnier L, Owens D. Glycaemic variability in diabetes: clinical and therapeutic implications. Lancet Diabetes Endocrinol. 2019;7(3):221–230. doi:10.1016/S2213-8587(18)30136-0
14. Giugliano D, Maiorino M, Bellastella G, Chiodini P, Esposito K. Relationship of baseline HbA1c, HbA1c change and HbA1c target of < 7% with insulin analogues in type 2 diabetes: a meta-analysis of randomised controlled trials. Int J Clin Pract. 2011;65(5):602–612. doi:10.1111/j.1742-1241.2010.02619.x
15. Chatterjee S, Khunti K, Davies MJ. Type 2 diabetes. Lancet. 2017;389(10085):2239–2251. doi:10.1016/S0140-6736(17)30058-2
16. Gandhi GY, Kovalaske M, Kudva Y, et al. Efficacy of continuous glucose monitoring in improving glycemic control and reducing hypoglycemia: a systematic review and meta-analysis of randomized trials. J Diabetes Sci Technol. 2011;5(4):952–965. doi:10.1177/193229681100500419
17. Ali MK, Pearson-Stuttard J, Selvin E, Gregg EW. Interpreting global trends in type 2 diabetes complications and mortality. Diabetologia. 2022;65(1):3–13. doi:10.1007/s00125-021-05585-2
18. Ji L, Hu D, Pan C, et al. Primacy of the 3B approach to control risk factors for cardiovascular disease in type 2 diabetes patients. Am J Med. 2013;126(10):
19. Nathan DM, Lachin JM, Bebu I, et al. Glycemia reduction in type 2 diabetes - microvascular and cardiovascular outcomes. N Engl J Med. 2022;387(12):1075–1088.
20. Kim HJ, Kim KI. Blood pressure target in type 2 diabetes mellitus. Diabetes Metab J. 2022;46(5):667–674. doi:10.4093/dmj.2022.0215
21. Wang M, Hng TM. HbA1c: more than just a number. Aust J Gen Pract. 2021;50(9):628–632. doi:10.31128/AJGP-03-21-5866
22. Stratton IM, Adler AI, Neil HA, et al. Association of glycaemia with macrovascular and microvascular complications of type 2 diabetes (UKPDS 35): prospective observational study. BMJ. 2000;321(7258):405–412. doi:10.1136/bmj.321.7258.405
23. Nathan DM, McGee P, Steffes MW, Lachin JM. Relationship of glycated albumin to blood glucose and HbA1c values and to retinopathy, nephropathy, and cardiovascular outcomes in the DCCT/EDIC study. Diabetes. 2014;63(1):282–290. doi:10.2337/db13-0782
24. Nelson AJ, Nicholls SJ. Treating dyslipidemia in type 2 diabetes. Cardiol Clin. 2018;36(2):233–239. doi:10.1016/j.ccl.2017.12.005
25. Moh MC, Pek SLT, Sze KCP, et al. Associations of non-invasive indices of liver steatosis and fibrosis with progressive kidney impairment in adults with type 2 diabetes. Acta Diabetol. 2023;60(6):827–835. doi:10.1007/s00592-023-02058-3
26. Chung GE, Han K, Lee KN, et al. Association between fatty liver index and risk of end-stage renal disease stratified by kidney function in patients with type 2 diabetes: a nationwide population-based study. Diabetes Metab. 2023;49(4):101454. doi:10.1016/j.diabet.2023.101454
27. Sarnowski C, Hivert MF. Impact of genetic determinants of HbA1c on type 2 diabetes risk and diagnosis. Curr Diab Rep. 2018;18(8):52. doi:10.1007/s11892-018-1022-4
28. Kurukulasuriya LR, Sowers JR. Therapies for type 2 diabetes: lowering HbA1c and associated cardiovascular risk factors. Cardiovasc Diabetol. 2010;9:45. doi:10.1186/1475-2840-9-45
29. Stefánsson BV, Heerspink HJL, Wheeler DC, et al. Correction of anemia by dapagliflozin in patients with type 2 diabetes. J Diabetes Complications. 2020;34(12):107729. doi:10.1016/j.jdiacomp.2020.107729
30. Gauci R, Hunter M, Bruce DG, Davis WA, Davis TME. Anemia complicating type 2 diabetes: prevalence, risk factors and prognosis. J Diabetes Complications. 2017;31(7):1169–1174. doi:10.1016/j.jdiacomp.2017.04.002
31. Xie L, Shao X, Yu Y, et al. Anemia is a risk factor for rapid eGFR decline in type 2 diabetes. Front Endocrinol. 2023;14:1052227. doi:10.3389/fendo.2023.1052227
32. Kanbay M, Tapoi L, Ureche C, et al. Effect of sodium-glucose cotransporter 2 inhibitors on hemoglobin and hematocrit levels in type 2 diabetes: a systematic review and meta-analysis. Int Urol Nephrol. 2022;54(4):827–841. doi:10.1007/s11255-021-02943-2
33. Xu S, Ren R, Li W, et al. The association between obesity indicators and metabolic risk factors in type-2 diabetic patients. Heliyon. 2023;9(9):e20013. doi:10.1016/j.heliyon.2023.e20013
34. Suo M, Wen D, Wang W, Zhang T. Comparative study on hemoglobin A1c, glycated albumin and glycosylated serum protein in aplastic anemia patients with Type 2 diabetes mellitus. Biosci Rep. 2020;40(5). doi:10.1042/BSR20192300
35. Boadu WIO, Anto EO, Frimpong J, et al. Prevalence, knowledge, and lifestyle-associated risk factors of dyslipidemia among Ghanaian type-2 diabetes mellitus patients in rural and urban areas: a multicenter cross-sectional study. Health Sci Rep. 2023;6(8):e1475. doi:10.1002/hsr2.1475
36. Wan Q, Harris MF, Powell-Davies G, et al. Cardiovascular risk levels in general practice patients with type 2 diabetes in rural and urban areas. Aust J Rural Health. 2007;15(5):327–333. doi:10.1111/j.1440-1584.2007.00916.x
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.