Back to Journals » International Journal of General Medicine » Volume 18
Predicting Distant Metastasis in Papillary Thyroid Carcinoma: A Postoperative Nomogram Integrating Sex, Histology, Bilaterality, and Extrathyroidal Extension
Received 16 June 2025
Accepted for publication 29 August 2025
Published 12 September 2025 Volume 2025:18 Pages 5409—5419
DOI https://doi.org/10.2147/IJGM.S547317
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Ching-Hsien Chen
Jiaxi Wang, Zhiyu Li, Chuang Chen
Department of Breast and Thyroid Surgery, Renmin Hospital of Wuhan University, Wuhan, People’s Republic of China
Correspondence: Zhiyu Li, Email [email protected] Chuang Chen, Email [email protected]
Background: Papillary thyroid carcinoma (PTC) generally has a good prognosis, but distant metastasis (DM) significantly reduces survival. Existing predictive models for DM have limited accuracy. This study aimed to identify independent risk factors for DM in PTC and develop a clinical prediction model using routine pathological parameters.
Methods: We retrospectively analyzed a cohort of 4127 PTC patients who underwent surgery between 2017 and 2022. Patients were divided into DM (n = 30) and non-DM (n = 4097) groups. Key variables, including sex, age, pathological subtype, tumor size, bilaterality, multifocality, extrathyroidal extension (ETE), and lymph node metastasis (LNM), were collected. We used univariate and multivariate logistic regression to identify independent predictors. A nomogram model was built and its performance was evaluated using ROC curves and other metrics.
Results: Univariate analysis identified male sex (OR = 0.362, p = 0.006), solid variant (OR = 36.509, p < 0.001), Multifocal (OR = 0.247, p < 0.001), bilaterality (OR = 2.847, p = 0.004), and ETE (OR = 4.360, p = 0.016) as significant risk factors. Multivariate analysis confirmed male sex (OR = 0.434, p = 0.029), solid variant (OR = 23.483, p < 0.001), bilaterality (OR = 1.309, p = 0.047), and ETE (OR = 3.094, p = 0.012) as independent predictors. The nomogram model showed a moderate discriminative ability with an AUC of 0.737, a sensitivity of 66.7%, and a specificity of 68.7%.
Conclusion: In this large-scale Chinese cohort study, we identified male sex, solid variant, bilaterality, and ETE as independent risk factors for PTCDM. The resulting model offers a practical tool for postoperative risk assessment, which can help guide customized surveillance and treatment for high-risk patients. Future research should focus on validating this model with external and multicenter cohorts and incorporating molecular biomarkers to further improve its predictive accuracy.
Keywords: papillary thyroid carcinoma, distant metastasis, risk factors, predictive model, nomogram
Introduction
Papillary thyroid carcinoma (PTC) is the most common pathological type of thyroid malignancy, accounting for 80–90% of all thyroid cancers.1,2 In recent years, the global incidence of PTC has shown a significant upward trend.3 Although most PTC patients achieve favorable prognoses (10-year survival rate > 95%) through surgical resection and Radioactive Iodine (RAI) therapy, approximately 5–10% of cases exhibit aggressive biological behavior, developing Distant Metastasis (DM). The most common sites of metastasis are the lungs, bones, and brain, with brain metastasis carrying the worst prognosis.4–6 The 10-year survival rate for patients with DM is less than 20%, and their sensitivity to RAI is significantly reduced, posing significant challenges in clinical management.7,8 Therefore, the early identification of PTC patients at high risk for DM is of great clinical importance for developing individualized surveillance strategies and optimizing adjuvant treatment plans.
PTC exhibits high pathological heterogeneity. According to the 2022 World Health Organization (WHO) classification criteria, PTC can be divided into more than ten subtypes, including the classic variant, follicular variant, solid variant, tall cell variant, and diffuse sclerosing variant.9 The solid variant is more aggressive than the classic variant, with a 3- to 5-fold higher risk of DM. This is likely due to its unique biological behavior, which includes a lack of typical papillary structures and frequent association with BRAF V600E mutations or RET gene fusions.9,10 Conversely, the follicular variant typically presents with larger tumor sizes but lower rates of Extrathyroidal Extension (ETE), lymph node metastasis (LNM), and recurrence, resulting in a relatively better prognosis.11,12 Furthermore, pathological parameters such as tumor multifocality, ETE, and LNM status have been confirmed to correlate with disease progression.12–15 The predictive value of these risk factors is debated; for example it’s unclear whether multifocality, for instance, reflects a tumor’s invasive potential or simply multiple origins.16
Currently, risk prediction models for PTC primarily rely on preoperative clinical parameters (eg, ultrasonographic features, serological markers) and intraoperative frozen section results, with a predominant focus on predicting cervical LNM.17–19 The risk stratification system proposed in the 2015 ATA (American Thyroid Association) guidelines incorporates indicators such as tumor size, LNM, and vascular invasion; however, its predictive efficacy for DM remains limited.20,21 Existing models often fail to adequately assess risk because they do not fully use postoperative pathological data. Additionally, high-risk variants like the solid variant are often underrepresented in study cohorts, leading to an underestimation of their true risk. Recent studies have begun exploring molecular markers (BRAF, TERT mutations), but molecular testing remains costly and clinically inaccessible in many regions, particularly low- and middle-income countries.22 Therefore, there is a critical need for an applicable clinical tool that uses standard pathological data to predict PTCDM and optimize risk-based management.
This study retrospectively analyzed a single-center cohort of 4127 PTC patients from Renmin Hospital of Wuhan University. Our goal was to identify independent risk factors and develop a diagnostic model that incorporates a wide range of clinicopathological features. While PTC generally has a favorable prognosis, DM remains a leading cause of mortality. Existing predictive models often rely on a limited number of pathological parameters, which restricts their clinical utility. To address this, we conducted a rigorous pathological review to comprehensively explore the relationship between postoperative pathological characteristics and metastatic risk. The final model is presented as a user-friendly nomogram for straightforward clinical application. This work not only complements current risk stratification systems but also provides valuable phenotypic anchors for future molecular mechanistic research, ultimately contributing to improved long-term outcomes for PTC patients.
Materials and Methods
Study Design and Ethics
This study was a retrospective study conducted in Renmin Hospital of Wuhan University. Patient data were collected from January 1, 2017, to December 30, 2022 (Figure 1). Inclusion criteria were age ≥ 18 years; preoperative diagnosis by ultrasonography and FNAB; completion of primary tumor surgical resection at our institution; postoperative paraffin-embedded histopathology confirming PTC with complete pathological records. Exclusion criteria: 1) Coexistence of other thyroid malignancies; 2) Preoperative DM; 3) Postoperative follow-up duration < 6 months; 4) Missing critical patient parameters (eg, tumor size, capsular invasion, personal/family history). Grouping: Patients were stratified into two groups based on postoperative follow-up: 1) DM group: Metastasis to distant organs (eg, lung, bone) confirmed by surgical pathology, CT-guided CNB (Core Needle Biopsy), or RAI whole-body scintigraphy; 2) non-DM group: Patients without metastasis or with cervical LNM only. Clinicopathological features were compared between DM and non-DM groups to evaluate whether primary tumors in DM patients exhibited greater aggressiveness. Medical equipment and clinical protocols remained consistent throughout the six-year study period. The study was approved by the Institutional Ethics Committee (Approval No.: WDRY2024-K038; Date: February 6, 2024) and conducted in accordance with the Helsinki Declaration. As a retrospective observational study, informed consent was waived by the Ethics Committee. All patient data were anonymized to protect privacy.
 |
Figure 1 Research flowchart. |
Data Collection
Two researchers collected data using a predefined pathology report form. Data were extracted from the Hospital Information System (HIS), including basic patient information, clinical presentation, pathological data, ultrasonographic and imaging data, laboratory indices, and surgical/postoperative status. Diagnostic criteria for comorbidities were as follows: Hashimoto’s thyroiditis (HT) was diagnosed based on serology (positive TPOAb) and ultrasonographic features; Nodular goiter (NG) was confirmed by postoperative pathology; and FA (Follicular adenoma) was confirmed by postoperative pathology. Lesions were evaluated and graded according to the American College of Radiology Thyroid Imaging, Reporting and Data System (TI-RADS).23 All data underwent dual verification before storage in the hospital database. For samples with missing data, we excluded them from the study.
Statistical Analysis
In the statistical analysis, categorical data were presented as number of patients (percentage), and continuous data were presented as mean ± standard deviation. The Shapiro–Wilk test was used to assess normality. For group comparisons, categorical variables were analyzed using Pearson’s chi-square test or Fisher’s exact test (when expected frequencies were < 5). Continuous variables conforming to a normal distribution with homogeneous variances were analyzed using the t-test or analysis of variance (ANOVA); otherwise, the Mann–Whitney U-test was used. Risk factor analysis employed univariate logistic regression to screen potential risk factors (p < 0.05), followed by multivariate logistic regression to identify independent risk factors (p < 0.05). A diagnostic model was constructed based on the multivariate analysis results, presented as a Nomogram. In order to evaluate the performance of the model more rigorously, we have internally validated the model using the stratified bootstrap. The “validate()” function of the rms package performs stratified sampling by default when processing the categorical endings, ensuring that the sample proportions of the DM group and the non-DM group in each repetition of the sampling are consistent with the original dataset. This effectively solves the bias problem that may be caused by the difference in sample size, thus ensuring the robustness and reliability of the validation results. The R package pROC was used to plot the ROC (Receiver Operating Characteristic) curve and calculate the Area Under the Curve (AUC) to evaluate diagnostic performance. All analyses were performed using R language (version 4.3.2). A two-sided p-value < 0.05 was considered statistically significant.
Results
Patient Baseline Information and Clinical Characteristics
As of December 30, 2022, a total of 4,127 pathologically confirmed PTC patients were included in this study. Based on postoperative follow-up, all patients were categorized into either the DM group or the non-DM group. Females constituted 75.8% of all hospitalized patients. In the non-DM group, females accounted for 75.9% of patients, whereas in the DM group, females accounted for 53.3%, demonstrating a statistically significant difference (p = 0.008). The mean age and standard deviation were 45.471 and 11.902 years, respectively, with no significant difference observed (p = 0.410). Among the enrolled subjects, 11.3% had concomitant HT, 16.3% had concomitant NG, and 1.3% had FA; no significant differences were observed in these three comorbidities. Overall, 12.3% of the study subjects had a family history of malignant tumors or a personal history of non-thyroid malignancies. Within the DM group (n = 30), 2 patients (6.7%) were diagnosed with the solid variant of PTC. In contrast, only 8 patients (0.2%) in the non-DM group (n = 4,097) had this pathological subtype, representing a statistically significant difference. Significant differences were also observed in PTC maximum diameter, unilateral/bilateral involvement at diagnosis, unifocality/multifocality, and the presence of capsular invasion. LNM status was analyzed only in patients who underwent central/lateral compartment lymph node dissection. The presence of central lymph node metastasis (CLNM), the number of CLNM, and the number of lateral lymph node metastasis (LLNM) all showed statistically significant differences between the two groups (Table 1).
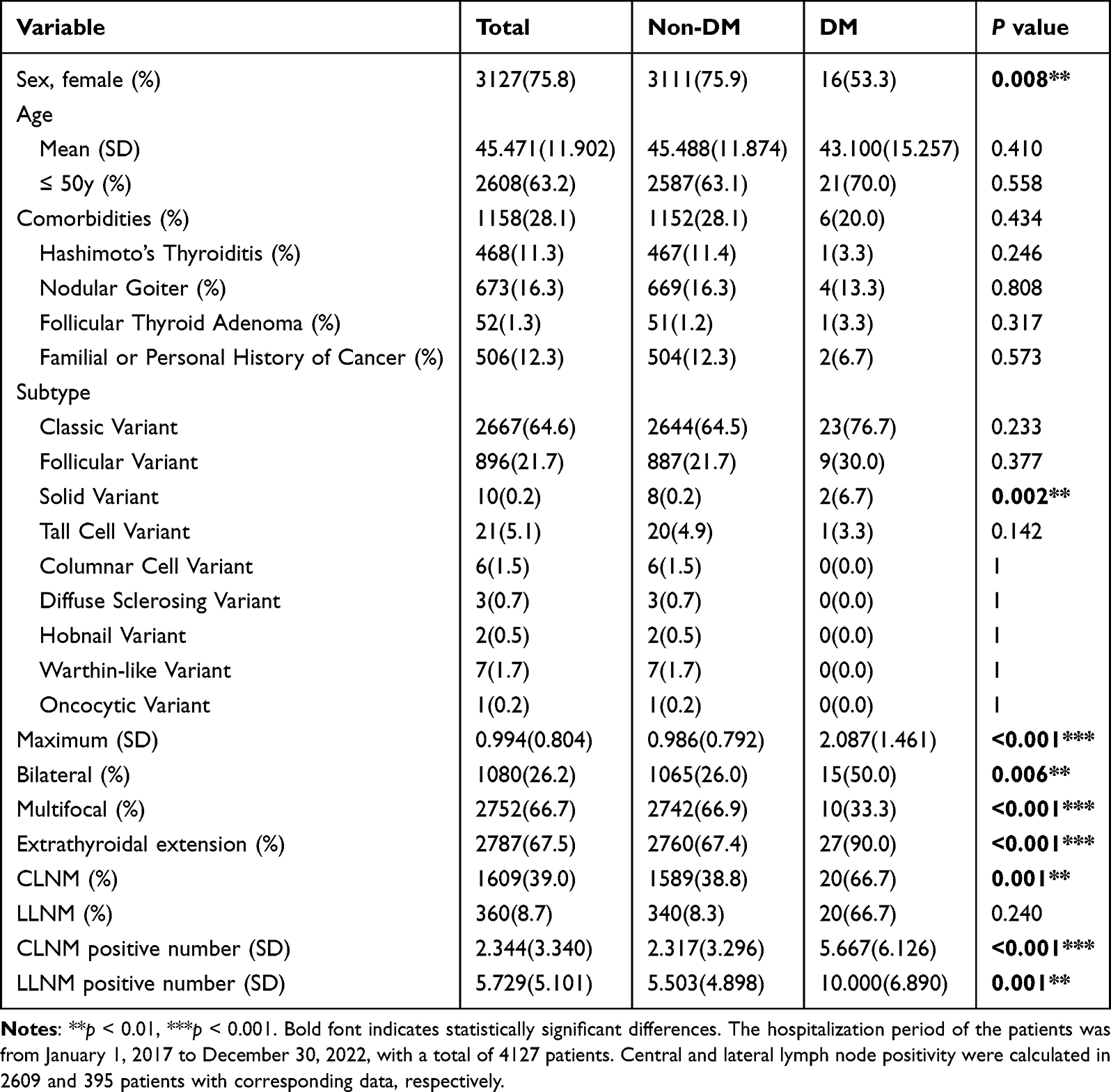 |
Table 1 Basic Information and Pathological Characteristics of Patients with DM/non_DM |
Construction of the Scoring System
Univariate regression analysis was performed to assess correlations between DM and patient baseline characteristics/pathological data. Sex (OR = 0.362, p = 0.006), solid variant of PTC (OR = 36.509, p < 0.001), bilateral involvement (OR = 2.847, p = 0.004), multifocality (OR = 0.247, p < 0.001), and ETE (OR = 4.360, p = 0.016) were significantly associated with DM (Table 2 and Figure 2).
 |
Table 2 Univariable Logistic Regression of Patients with DM/non_DM |
 |
Figure 2 Univariable logistic regression of patients with DM/non_DM. The red dots represent the log2(Odds Ratio), with the dashed lines indicating the 95% CI. A log2(Odds Ratio) less than 0 suggests a protective effect, while a value greater than 0 suggests a risk factor. |
Variables demonstrating statistical significance in univariate analysis were subsequently included in multivariate logistic regression. The analysis revealed that sex, solid variant, bilateral involvement, and ETE were independent risk factors for PTC DM. Female patients exhibited significantly lower risk of DM compared to males (OR = 0.434, p = 0.029). Patients with the solid variant had substantially elevated DM risk (OR = 23.483, p < 0.001). Bilateral involvement (OR = 1.309, p = 0.047) and ETE (OR = 3.094, p = 0.012) were also significantly associated with increased DM risk. Multifocality did not reach statistical significance (p = 0.071) (Table 3 and Figure 3).
 |
Table 3 Multivariable Logistic Regression of Patients with DM/non_DM |
 |
Figure 3 Multivariable logistic regression of patients with DM/non_DM. The red dots represent the log2(Odds Ratio), with the dashed lines indicating the 95% CI. A log2(Odds Ratio) less than 0 suggests a protective effect, while a value greater than 0 suggests a risk factor. |
Development and Validation of the Prediction Model
The four variables—sex, solid variant, bilateral involvement, and ETE—were incorporated into the prediction model. The prediction formula was constructed as follows:
Prediction Score = −6.496691 + Female * (−0.9639) + Solid * 3.2888 + Bilateral * 0.8075 + ETE * 1.2987.
A nomogram was developed to visualize this fitted model. The predictive performance was evaluated using the AUC (0.737) of ROC curve. At the optimal cutoff value of 0.009, the model demonstrated maximum predictive accuracy with sensitivity, specificity, and Youden’s index of 0.667, 0.687, and 0.354, respectively (Figures 4 and 5).
 |
Figure 4 Nomogram based on patient’s basic information and pathological features. To use the nomogram, locate the patient’s value for each variable (Sex, Solid variant, Bilateral, Extrathyroidal extension). Draw a vertical line from the corresponding value to the “Points” scale to get the score for that variable. Sum the points for all variables to get the “Total Points.” The “Total Points” can then be used to predict the “Predicted Probability” of overall survival by drawing a vertical line down to the corresponding scale. The numbers on the lines for Sex, Solid variant, Bilateral, and Extrathyroidal extension represent different categories or levels of the variables. For example, for “Sex”, “0” represent male and “1” might represent female. |
 |
Figure 5 ROC curve of prediction model based on patient’s basic information and pathological features. The red dot on the curve indicates an optimal cut-off point, balancing sensitivity and specificity for the model. The blue line represents the ROC curve, plotting the sensitivity (True Positive Rate) against the 1 - Specificity (False Positive Rate) at various threshold settings. The dashed gray line represents a random classifier (AUC = 0.5). |
Discussion
Despite PTC having the most favorable prognosis among thyroid malignancies, predicting its DM remains crucial. This retrospective cohort study of 4,127 PTC cases identified sex, solid variant, bilateral involvement, and ETE as independent predictors of PTC DM. We developed a prediction model incorporating routine clinical data and postoperative pathological parameters (AUC = 0.737), which holds significant importance for understanding the aggressive behavior of PTC and enabling individualized high-risk stratification.
This study revealed a significant impact of sex on PTC DM. Although females constituted 75.8% of the total cohort, they represented only 53.3% of the DM group. Multivariate analysis further confirmed that female patients had a reduced risk of metastasis compared to males (OR = 0.434). This finding aligns with previous studies,24,25 though the underlying mechanisms are not fully elucidated. Some literature suggests that downregulation of SLC5A5 in male PTC individuals correlates with poorer prognosis.26 Estrogen may inhibit tumor cell migration by activating sex- or reproduction-related pathways, while androgens may promote metastasis by upregulating epithelial-mesenchymal transition (EMT)-related genes (eg, TNNT1). Suppression of the androgen-androgen receptor axis may also be associated with high-risk PTC manifestations.24,27,28 Notably, despite the relatively better prognosis in females, their higher incidence leads to an increased absolute number of DM cases. Future research should investigate the distinct mechanisms of PTC metastasis across sexes to identify sex-specific therapeutic targets.
Regarding pathological subtypes, the solid variant of PTC (SVPTC) exhibited a remarkably high risk of DM (OR = 23.483). Although SVPTC accounted for only 0.2% of the total cohort, it represented 6.7% of the DM group. This result strongly corresponds to the known aggressive nature of the solid variant. Molecular studies indicate that the immunohistochemical expression of common PTC markers CK19 and HBME-1 is reduced within the solid nests of SVPTC.10 Furthermore, SVPTC is frequently associated with RET rearrangements and BRAF V600E mutations.10 These alterations collectively lead to sustained MAPK (Mitogen-Activated Protein Kinase) pathway activation and upregulated telomerase activity, driving genomic instability and metastatic phenotypes. They can also activate nuclear factor kappa-B (NF-κB), increasing inflammatory mediator expression and promoting metastasis.9,10,29 However, limited by the small sample size (n = 10), this study may underestimate the true risk of this variant. In clinical practice, intensified management is recommended for such patients,30 including consideration of prophylactic RAI therapy and shortened imaging surveillance intervals to detect occult metastases early, even with small primary tumors or absence of LNM. Given its extremely high odds ratio, our findings provide strong evidence that identifying the solid variant in pathological reports should immediately flag a patient for heightened clinical attention, regardless of other low-risk features. This knowledge empowers clinicians to consider more aggressive initial treatment strategies or accelerated follow-up schedules to mitigate the high risk of DM.
Bilateral involvement demonstrated independent predictive value (OR = 1.309), suggesting it may not simply be a manifestation of multifocality. While bilateral involvement was significantly associated with metastatic risk in multivariate analysis, multifocality itself did not reach statistical significance (p = 0.071). This phenomenon is common in multifactor analyses, and it usually indicates that Multifocality is strongly associated with other variables in the model, especially those that are significant in the final model. In other words, Multifocality’s independent predictive value is diluted or explained by its effect when it is included in the model at the same time as other, more potent predictors. Specifically, we hypothesized that Multifocality is likely to be confounded or covariate with factors such as Bilateral or Extrathyroidal extension. This paradox may stem from the distinct biology of bilateral tumors: they might represent more aggressive monoclonal subclones rather than the multiclonal origins often seen in multifocal disease.31 In addition, the difference in the distribution of left and right cervical lymph nodes may provide an anatomical pathway for tumor cells to enter the systemic circulation.32 This finding suggests clinicians should reassess the role of bilateral involvement in risk stratification. Enhanced postoperative surveillance is warranted for patients with bilateral PTC, even in the absence of other high-risk features (eg, LNM, aggressive variants).
This study also identified ETE as an independent risk factor for PTC DM (OR = 3.094). Although the AJCC (American Joint Committee on Cancer) staging system classifies ETE as minimal or gross invasion, ETE status alone (without distinguishing extent) effectively predicts PTC DM.33 Current pathology reports often simplify ETE to “present” or “absent”, without reporting minimal or gross invasion. Therefore, a predictive model focusing solely on ETE presence/absence remains clinically relevant and practical for risk assessment. Our model provides a clinically pragmatic tool for risk assessment. This allows for the seamless integration of ETE status into routine clinical risk stratification, guiding decisions on the extent of surgery and the necessity of adjuvant radioactive iodine therapy for DM prevention.
Multifocality was associated with reduced DM risk in univariate analysis (OR = 0.247) but lost significance in multivariate analysis, indicating confounding by other variables. A possible explanation is heterogeneity within multifocal tumors: some arise from multiclonal origins, while others represent intra-thyroidal spread of a single aggressive clone. Thus, multifocality does not guarantee safety. High-risk multifocality should be stratified based on relevant molecular markers (eg, BRAF mutation status) or spatial distribution (bilateral vs unilateral).
Our prediction model integrates four factors: sex, solid variant, bilateral involvement, and ETE, achieving an AUC of 0.737, with sensitivity and specificity of 66.7% and 68.7%, respectively. While this performance demonstrates predictive capability for PTC DM, improvement is possible. LNM burden (presence and number) showed potential predictive value but was excluded from the model as some patients did not undergo lymph node dissection. Previous studies indicate that the number of lymph node metastases correlates positively with tumor angiogenic capacity.34 Tumor cells achieving lymphatic metastasis can promote regulatory T cell (Treg) differentiation, fostering an immune-suppressive microenvironment conducive to distant metastasis.35,36 However, several studies have shown that only extensive LNM or large metastases with extra-lymph node invasion have a stronger correlation with distant metastasis, and the mere presence of LNM is not effective in differentiating high-risk populations.37 The absence of molecular markers (eg, BRAF V600E, TERT promoter mutations) may limit the model’s discriminative power. A two-step strategy could optimize future models: initial screening using routine pathological parameters, followed by supplemental molecular testing for high-risk patients, balancing cost and performance.
Limitation
The limitations of this study warrant acknowledgement. Single-center data limits generalizability. Regional variations in PTC incidence and BRAF V600E mutation rates ultimately lead to differences in metastatic rates.38 Insufficient sample size may also affect risk assessment for rare variants (eg, solid, hobnail). Future multi-center collaboration is needed to enhance model applicability. Some patients may develop metastasis during extended follow-up, potentially leading to underestimated risk. The strengths lie in rigorous data quality control, comprehensive exploration of postoperative pathological parameters, and the provision of a clinically applicable decision-making tool.
Conclusion
In summary, this study established a database for PTC patients at our center and developed a clinical prediction model for PTC DM using basic clinical data and pathological parameters.
This study demonstrated that male sex, solid variant, bilateral involvement, and ETE are independent risk factors for PTC DM. ETE retains significant predictive value for DM even without distinguishing between minimal and gross invasion. Furthermore, LNM is also a risk factor for DM. Although LNM was not incorporated into the model due to the absence of lymph node dissection in some patients, its potential association with DM risk should be considered in clinical practice. The proposed model assists clinicians in assessing the risk of DM in PTC patients following initial surgery. This model will contribute to better management of PTC patients and help mitigate the risk of DM in high-risk individuals. However, there are some limitations of this study, and prospective, multicenter validation is needed in the future; in addition, molecular markers can be incorporated into the model in the future for more accurate prediction.
Abbreviations
PTC, papillary thyroid carcinoma; FNAB, Fine-needle Aspiration Biopsy; RAI, Radioactive Iodine; DM, Distant Metastasis; WHO, World Health Organization; ETE, Extrathyroidal Extension; ATA, American Thyroid Association; CNB, Core Needle Biopsy; HT, Hashimoto’s thyroiditis; NG, Nodular goiter; FA, Follicular adenoma; AUC, the Area Under the Curve; EMT, epithelial-mesenchymal transition; LNM, lymph node metastasis.
Data Sharing Statement
All data generated or analyzed during this study are available from the corresponding author (Chuang Chen, [email protected]) on reasonable request.
Ethics Approval and Consent to Participate
The study has been approved by the Ethics Committee of Renmin Hospital of Wuhan University (NO. WDRY2024-K038). The requirement for obtaining informed consent from the involved patients was waived due to the retrospective nature of the study design.
Acknowledgments
We gratefully acknowledge the helpful suggestion from our team members.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research was supported by Natural Science Foundation of Hubei Province (2023AFB701), and the Open Project of Hubei Key Laboratory (Grant No. 2023KFZZ008) to Z.L.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Prescott JD, Zeiger MA. The RET oncogene in papillary thyroid carcinoma. Cancer. 2015;121(13):2137–2146. doi:10.1002/cncr.29044
2. Xu X, Jing J. Advances on circRNAs contribute to carcinogenesis and progression in papillary thyroid carcinoma. Front Endocrinol. 2020;11:555243. doi:10.3389/fendo.2020.555243
3. Wiltshire JJ, Drake TM, Uttley L, Balasubramanian SP. Systematic review of trends in the incidence rates of thyroid cancer. Thyroid. 2016;26(11):1541–1552. doi:10.1089/thy.2016.0100
4. Lan X, Bao H, Ge X, et al. Genomic landscape of metastatic papillary thyroid carcinoma and novel biomarkers for predicting distant metastasis. Cancer Sci. 2020;111(6):2163–2173. doi:10.1111/cas.14389
5. Toraih EA, Hussein MH, Zerfaoui M, et al. Site-specific metastasis and survival in papillary thyroid cancer: the importance of brain and multi-organ disease. Cancers. 2021;13(7):1625. doi:10.3390/cancers13071625
6. Li C, Wu Q, Sun S. Radioactive iodine therapy in patients with thyroid carcinoma with distant metastases: a SEER-based study. Cancer Control. 2020;27(1):1073274820914661. doi:10.1177/1073274820914661
7. Pacini F. Which patient with thyroid cancer deserves systemic therapy and when? Best Pract Res Clin Endocrinol Metab. 2017;31(3):291–294. doi:10.1016/j.beem.2017.08.001
8. Silaghi H, Lozovanu V, Georgescu CE, et al. State of the art in the current management and future directions of targeted therapy for differentiated thyroid cancer. Int J Mol Sci. 2022;23(7):3470. doi:10.3390/ijms23073470
9. Baloch ZW, Asa SL, Barletta JA, et al. Overview of the 2022 WHO classification of thyroid neoplasms. Endocrine Pathology. 2022;33(1):27–63. doi:10.1007/s12022-022-09707-3
10. Ohashi R. Solid variant of papillary thyroid carcinoma: an under-recognized entity. Endocr J. 2020;67(3):241–248. doi:10.1507/endocrj.EJ19-0414
11. Yang J, Gong Y, Yan S, et al. Comparison of the clinicopathological behavior of the follicular variant of papillary thyroid carcinoma and classical papillary thyroid carcinoma: a systematic review and meta-analysis. Mol Clin Oncol. 2015;3(4):753–764. doi:10.3892/mco.2015.540
12. Yu XM, Schneider DF, Leverson G, Chen H, Sippel RS. Follicular variant of papillary thyroid carcinoma is a unique clinical entity: a population-based study of 10,740 cases. Thyroid. 2013;23(10):1263–1268. doi:10.1089/thy.2012.0453
13. Joseph KR, Edirimanne S, Eslick GD. Multifocality as a prognostic factor in thyroid cancer: a meta-analysis. Int J Surg. 2018;50:121–125. doi:10.1016/j.ijsu.2017.12.035
14. Youngwirth LM, Adam MA, Scheri RP, Roman SA, Sosa JA. Extrathyroidal extension is associated with compromised survival in patients with thyroid cancer. Thyroid. 2017;27(5):626–631. doi:10.1089/thy.2016.0132
15. Ricarte-Filho J, Ganly I, Rivera M, et al. Papillary thyroid carcinomas with cervical lymph node metastases can be stratified into clinically relevant prognostic categories using oncogenic BRAF, the number of nodal metastases, and extra-nodal extension. Thyroid. 2012;22(6):575–584. doi:10.1089/thy.2011.0431
16. Muzza M. The clonal origin of multifocal papillary thyroid cancer: intrathyroidal spread or independent tumors? Minerva Endocrinol. 2021;46(1):35–44. doi:10.23736/S2724-6507.20.03302-7
17. Shen K, Xiao S, Wu X, Zhang G. Preoperative prognostic risk stratification model for papillary thyroid carcinoma based on clinical and ultrasound characteristics. Front Endocrinol. 2022;13:1025739. doi:10.3389/fendo.2022.1025739
18. Liu C, Yang S, Xue T, et al. The application of a clinical-multimodal ultrasound radiomics model for predicting cervical lymph node metastasis of thyroid papillary carcinoma. Front Oncol. 2024;14:1507953. doi:10.3389/fonc.2024.1507953
19. Deng Y, Zhang J, Wang J, et al. Risk factors and prediction models of lymph node metastasis in papillary thyroid carcinoma based on clinical and imaging characteristics. Postgrad Med. 2023;135(2):121–127. doi:10.1080/00325481.2022.2135840
20. Sapuppo G, Grasso S, Di Benedetto G, Belfiore A, Pellegriti G. Prospective study and proposal of an outcome predictive nomogram in a consecutive prospective series of differentiated thyroid cancer based on the new ATA risk categories and TNM. Front Endocrinol. 2023;14:1128963. doi:10.3389/fendo.2023.1128963
21. Haugen BR, Alexander EK, Bible KC, et al. 2015 American thyroid association management guidelines for adult patients with thyroid nodules and differentiated thyroid cancer: the American thyroid association guidelines task force on thyroid nodules and differentiated thyroid cancer. Thyroid. 2016;26(1):1–133. doi:10.1089/thy.2015.0020
22. Cheng X, Zhou Y, Xu S, et al. Risk-stratified distant metastatic thyroid cancer with clinicopathological factors and BRAF/TERT promoter mutations. Exp Clin Endocrinol Diabetes. 2023;131(11):577–582. doi:10.1055/a-2177-1051
23. Zhou J, Yin L, Wei X, et al. Chinese guidelines for ultrasound malignancy risk stratification of thyroid nodules: the C-TIRADS. Endocrine. 2020;70(2):256–279.
24. Jonklaas J, Nogueras-Gonzalez G, Munsell M, et al. The impact of age and gender on papillary thyroid cancer survival. J Clin Endocrinol Metab. 2012;97(6):E878–87.
25. Siraj AK, Parvathareddy SK, Annaiyappanaidu P, et al. Male sex is an independent predictor of recurrence-free survival in middle eastern papillary thyroid carcinoma. Front Endocrinol. 2022;13:777345. doi:10.3389/fendo.2022.777345
26. Yan C, Sun J, He X, Jia L. An age-and sex-matched postoperative therapy should be required in thyroid papillary carcinoma. Front Endocrinol. 2024;15:1339191.
27. Jiang C, Xu F, Yi D, et al. Testosterone promotes the migration, invasion and EMT process of papillary thyroid carcinoma by up-regulating Tnnt1. J Endocrinol Invest. 2024;47(1):149–166. doi:10.1007/s40618-023-02132-1
28. Chou CK, Chi SY, Chou FF, et al. Aberrant expression of androgen receptor associated with high cancer risk and extrathyroidal extension in papillary thyroid carcinoma. Cancers. 2020;12(5):1109. doi:10.3390/cancers12051109
29. Zhou D, Li Z, Bai X. BRAF V600E and RET/PTC promote the activity of nuclear factor-κB, inflammatory mediators, and lymph node metastasis in papillary thyroid carcinoma: a study of 50 patients in inner Mongolia. Med Sci Monit. 2018;24:6795–6808. doi:10.12659/MSM.909205
30. Vuong HG, Odate T, Duong UNP, et al. Prognostic importance of solid variant papillary thyroid carcinoma: a systematic review and meta-analysis. Head Neck. 2018;40(7):1588–1597. doi:10.1002/hed.25123
31. Sun W, Hu Q, Liu Z, Zhang Q, Wang J. Analysis of the clonal origin and differences in the biological behavior of multifocal papillary thyroid carcinoma. Oncol Lett. 2024;28(5):544. doi:10.3892/ol.2024.14677
32. Yoruk O, Yuksel R, Yuksel Y, Dane S. Left-right asymmetry in neck lymph nodes distribution in patients with bilateral laryngeal cancer. Surg Radiol Anat. 2014;36(3):239–242. doi:10.1007/s00276-013-1176-3
33. Turk AT, Asa SL, Baloch ZW, et al. Interobserver variability in the histopathologic assessment of extrathyroidal extension of well differentiated thyroid carcinoma supports the new American joint committee on cancer eighth edition criteria for tumor staging. Thyroid. 2019;29(5):619–624. doi:10.1089/thy.2018.0286
34. Xiangming C, Hokita S, Natsugoe S, et al. Angiogenesis as an unfavorable factor related to lymph node metastasis in early gastric cancer. Ann Surg Oncol. 1998;5(7):585–589. doi:10.1007/BF02303826
35. Weidner N, Semple JP, Welch WR, Folkman J. Tumor angiogenesis and metastasis--correlation in invasive breast carcinoma. N Engl J Med. 1991;324(1):1–8. doi:10.1056/NEJM199101033240101
36. Reticker-Flynn NE, Zhang W, Belk JA, et al. Lymph node colonization induces tumor-immune tolerance to promote distant metastasis. Cell. 2022;185(11):1924–42.e23. doi:10.1016/j.cell.2022.04.019
37. Hong YR, Lee SH, Lim DJ, et al. The stratification of patient risk depending on the size and ratio of metastatic lymph nodes in papillary thyroid carcinoma. World J Surg Oncol. 2017;15(1):74. doi:10.1186/s12957-017-1141-4
38. Rashid FA, Munkhdelger J, Fukuoka J, Bychkov A. Prevalence of BRAF(V600E) mutation in Asian series of papillary thyroid carcinoma-a contemporary systematic review. Gland Surg. 2020;9(5):1878–1900. doi:10.21037/gs-20-430
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.