Back to Journals » Journal of Asthma and Allergy » Volume 19
Precision Prediction of Pediatric Subcutaneous Immunotherapy Outcomes Using a Clinical Nomogram for House Dust Mite Allergy
Authors Zhuang SJ, Fan TT, Lai RL, Ruan XY, Huang SM, Gao ZH, Liu CY, Lu ZW, Huang MF, Liu XL, Yang FH, Shen KL, Zhang Y, Bao YM
Received 6 March 2026
Accepted for publication 8 May 2026
Published 22 May 2026 Volume 2026:19 605382
DOI https://doi.org/10.2147/JAA.S605382
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Luis Garcia-Marcos
Shi-Jie Zhuang,1 Ting-Ting Fan,1 Rong-Li Lai,1 Xin-Yu Ruan,1 Shi-Min Huang,1 Zi-Hong Gao,1 Chun-Yan Liu,1 Zhi-Wei Lu,1 Miao-Feng Huang,1 Xiao-Lan Liu,1 Fang-Hua Yang,1 Kun-Ling Shen,1 Yan Zhang,2 Yan-Min Bao1
1Department of Respiratory Medicine, Shenzhen Children’s Hospital, Shenzhen, Guangdong, 518026, People’s Republic of China; 2School of Statistics and Data Science, Nanjing Audit University, Nanjing, Jiangsu, 211815, People’s Republic of China
Correspondence: Yan-Min Bao, Department of Respiratory Medicine, Shenzhen Children’s Hospital, Shenzhen, Guangdong, 518026, People’s Republic of China, Email [email protected] Yan Zhang, School of Statistics and Data Science, Nanjing Audit University, Nanjing, Jiangsu, 211815, People’s Republic of China, Email [email protected]
Background: The identification of predictive biomarkers for subcutaneous immunotherapy (SCIT) is of great importance for improving its clinical efficacy. This study aims to construct a nomogram predicting the efficacy of SCIT and to evaluate the predictive value of Der p 1 and Der p 2 for SCIT response.
Methods: This study included children with allergic rhinitis (AR) and/or asthma (AS) who received house dust mite (HDM) SCIT at Shenzhen Children’s Hospital between 2021 and 2024. Baseline characteristics and laboratory data were retrospectively collected before SCIT. The sIgE to HDM components were measured in children’s serum before SCIT. The efficacy of SCIT was assessed with VAS scores. Potential predictors for the efficacy of HDM SCIT were identified with logistic regression analysis. A nomogram predicting the efficacy of HDM SCIT was constructed and internally validated.
Results: Among the 209 children who were successfully followed up after one year of treatment, 166 (79%) responded to HDM SCIT, while 43 (21%) were non-responders. Logistic regression analysis identified that Der p (1+2) sIgE, the Der p (1+2) sIgE/tIgE ratio and asthma as predictors of HDM SCIT efficacy. A nomogram predicting the efficacy of HDM SCIT was developed by incorporating the three predictors. The nomogram achieved an AUC of 0.80 (95% CI=0.72– 0.87) and a C-index of 0.80 (95% CI=0.72– 0.87). At a cutoff value of 43.87kUA/L, Der p (1+2) sIgE achieved an AUC of 0.75, superior to tIgE and the Der p (1+2) sIgE/tIgE ratio.
Conclusion: The Der p 1 and Der p 2 were predictors of HDM SCIT. Der p (1+2) sIgE outperformed both the Der p (1+2) sIgE/tIgE ratio and tIgE in predicting the efficacy of HDM SCIT. A nomogram incorporating Der p (1+2) sIgE, the Der p (1+2) sIgE/tIgE ratio and asthma was developed for the visual and quantitative prediction of HDM SCIT efficacy.
Keywords: house dust mite, HDM, Der p 1, Der p 2, subcutaneous immunotherapy, SCIT, nomogram
Introduction
House dust mites (HDM), including Dermatophagoides pteronyssinus (Der p) and Dermatophagoides farinae (Der f), are a primary source of inhalant allergens causing allergic rhinitis (AR) and asthma (AS).1,2 Allergen immunotherapy (AIT) is a disease-modifying treatment that induces long-term immunologic tolerance by administering gradually increasing doses of the causative allergen. Among AIT modalities, subcutaneous immunotherapy (SCIT) has the longest history and most extensive evidence base, demonstrating its capacity to not only alleviate symptoms but also to potentially prevent the progression of allergic disease and the development of new sensitizations.3,4 This foundational role has established SCIT as a cornerstone in the management of moderate-to-severe allergic conditions inadequately controlled by conventional medications. However, SCIT has a slow onset of action, incurs relatively high costs, and demonstrates suboptimal efficacy in some patients. It is important to identify effective biomarkers for early distinction of patients likely to respond to SCIT.
With the rapid advancement of component-resolved diagnosis (CRD) technology, studies have revealed that HDM is actually composed of various distinct mite allergen components.5 The World health organization and international union of immunological societies (WHO/IUIS, https://www.allergen.org) have identified more than 40 types of mite allergen components. The heterogeneity of HDM sensitization patterns across regions, which is driven by factors such as local climate, disease profiles, and allergen exposure levels-these factors influence both mite species prevalence and dominant allergenic component–may have implications for the efficacy of SCIT and the underlying pathogenic mechanisms.6 The majority (>50%) patients are sensitized to major HDM allergen components, including Der p 1, Der p 2, Der f 1, Der f 2, and Der p 23. In contrast, a subset (10–50%) of patients is sensitized to minor components, such as Der p 5, Der p 7, and Der p 10.7,8 Since standardized vaccines of HDM are typically rich in Der p 1, Der p 2, Der f 1, and Der f 2, other HDM components are relatively low or absent.9 Given the variability in HDM component sensitization profiles among individuals, evidences suggest that patients sensitized to Der p 1, Der p 2, Der f 1, and Der f 2 derive the greatest clinical benefit from SCIT.10,11
The Immunotherapy Group of the European Academy of Allergy and Clinical Immunology (EAACI) has identified seven key biomarkers for monitoring and forecasting the efficacy of SCIT. Among these biomarkers, the IgE family, which includes total IgE (tIgE), specific IgE (sIgE), and the sIgE/tIgE ratio, is widely acknowledged as a reliable indicator for predicting the efficacy of SCIT.12 Serum sIgE is an immunoglobulin produced by the immune system in response to specific allergens, primarily synthesized by B cells with the assistance of T cells. Upon re-exposure to the corresponding allergen, sIgE binds to the allergen to form immune complexes, which subsequently activate downstream effector cells. This activation triggers the release of inflammatory mediators, leading to the onset of allergic reactions.13,14 Di et al found that the sIgE/tIgE ratio measured before SCIT in patients sensitized to grass, pollen, or HDM was closely correlated with its clinical efficacy (r=0.72, P<0.001).12 Moreover, the area under the curve (AUC) was 0.97 (P<0.05), indicating that as predictive biomarkers, the serum sIgE/tIgE ratio could effectively predict the clinical efficacy of SCIT, with performance superior to that of serum tIgE and sIgE.15 Li et al reported that in children undergoing SCIT, serum tIgE and the sIgE/tIgE ratio were significantly associated with treatment efficacy. In predicting clinical outcomes of SCIT, the area under the ROC curve (AUC) for tIgE was 0.77 (95% CI, 0.70–0.83), demonstrating better predictive performance compared to the sIgE/tIgE ratio and sIgE levels alone.16
Currently, there is a lack of nomograms to predict immunotherapy response using HDM components in the children population studied. Therefore, this study intends to investigate the relationship between major HDM components and the efficacy of HDM SCIT. By collecting relevant clinical data from patients during SCIT, we seek to identify independent factors that can effectively predict the therapeutic outcome of HDM SCIT. Furthermore, a nomogram prediction will be constructed to provide a visual and quantitative tool for forecasting the efficacy of SCIT in HDM sensitized children, thereby offering valuable reference and guidance for predicting treatment response in this population.
Materials and Methods
Patients
This was a retrospective study. We included children with AR and/or AS who were received HDM SCIT at Shenzhen Children’s Hospital between August 2021 and January 2024. Inclusion criteria were as follows: (i) the diagnoses of AR and AS was defined according to the Allergic Rhinitis and its Impact on Asthma (ARIA) guideline,17 (ii) patient’s allergic symptoms were consistent with HDM monosensitization, (iii) allergic status was confirmed by the skin prick test (SPT) and measurement of serum sIgE for Der p or Der f, (iv) age 5 to 15 years old, with normal development, (v) met the SCIT enrollment criteria: patients with moderate-to-severe allergic asthma or allergic rhinitis who had inadequate symptom control despite optimal pharmacotherapy and allergen avoidance,18 (vi) signed the informed consent form. Exclusion criteria were as follows: (i) previous and/or current use of biologics (eg, omalizumab, dupilumab), (ii) previous use of allergen-specific immunotherapy (ASIT) for HDM, (iii) acute-phase symptoms of AR or AS, (iv) sensitization to allergens other than Der p and Der f, including pollens and fungi, (v) moderate-to-severe specific dermatitis, (vi) other chronic diseases.
HDM Standardized Allergen Vaccines
SCIT was administered using HDM standardized allergen vaccines produced by either ALK-Abelló (Denmark) or Allergopharma (Germany). The vaccine of ALK-Abelló (Denmark) consists of full allergens with 100% Der p. The vaccine of ALK-Abelló is available in four concentrations: No.1 (100 SQ-U/mL), No.2 (1000 SQ-U/mL), No.3 (10000 SQ-U/mL) and No.4 (100000 SQ-U/mL). The treatment process comprised two distinct phases: the dose escalation phase and the maintenance phase. According to the ALK-Abelló product manual, the dose escalation phase lasted 15 weeks with weekly subcutaneous injections. Preparations No.1, No.2, and No.3 were administered sequentially, each injected three times at gradually increasing doses. Preparation No. 4 required six injections, with the dose escalating to 1.0 mL (100,000 SQ-U) or the maximum tolerated dose. During maintenance, a 1.0mL dose of injection of Preparation No.4 was administered every 4 to 6 weeks. The vaccine of Allergopharma (Germany) consisted of a combination of full allergens with 50% Der p and 50% Der f. The vaccine of Allergopharma was available in three concentrations: No.1 (50 TU/mL), No.2 (500 TU/mL) and No.3 (5000 TU/mL). The treatment process comprised two distinct phases: the dose escalation phase and the maintenance phase. According to the Allergopharma product manual, the dose escalation phase lasted 15 weeks with weekly subcutaneous injections. Preparations No.1 and No.2 were administered sequentially, each injected four times at gradually increasing doses. Preparation No.3 required seven injections, with the dose escalating to 1.0 mL (5000 TU/mL) or the maximum tolerated dose. During maintenance, a 1.0 mL dose of injection of preparation No.3 was administered every 4 to 6 weeks.
During SCIT, if a patient exhibited symptoms or signs of vaccine intolerance, the physician could reduce the dose and reschedule the next injection per the product manual. To prevent adverse reactions, anti-allergic medications were administered before each SCIT injection.
Subjective Efficacy Evaluation of HDM SCIT
Patient’s subjective symptoms were assessed using the visual analogue scale (VAS).19 The scale employs a 10cm straight line with opposite ends labeled “Comfort” and “Discomfort” respectively. Respondents marked their current symptom intensity perception on the VAS scale. VAS scores were calculated by measuring the distance (in cm/mm) from the “Comfort” starting point to the participant’s mark. The higher the VAS score, the more severe the symptoms. The VAS was assessed at baseline and 12 months after SCIT. Responders to SCIT were defined as individuals who demonstrated at least a 30% improvement in their VAS scores from the baseline after 12 months of undergoing SCIT.15
Objective Efficacy Evaluation of AR and AS
According to the EAACI, combined symptom and medication score (CSMS) was used to evaluate the objective efficacy of patients with AR, basing on a weight equal to the total daily symptom score (dSS) and the total daily medication score (dMS).20 The dSS was the sum of all individual symptoms divided by the number of symptoms, the dSS range being 0 to 3 (the maximum score is 3). The dMS ranged from 0 to 3, increasing with the intensity of the drug. The CSMS is the sum of dSS (range 0–3) and dMS (range 0–3). CSMS values were in the range of 0–6. In patients who, in addition to AR, had AS, a childhood asthma control test (C-ACT) that consisted of 7 questions (4 child-reported and 3 caregiver-reported) in relationship to asthma control in the previous 4 weeks was conducted.21 The scores could range from 0 (worst control) to 27 (total control). The CSMS and the C-ACT score were assessed at baseline and 12 months after SCIT.
Collection of Clinical Indicators
Peripheral blood samples were collected retrospectively. Baseline information collected included age, sex, height, weight, diagnosis, family history of allergies, passive smoking history, and asthma diagnosis. Laboratory indicators collected included eosinophils (Eos), basophils (Baso), fractional exhaled nitric oxide (FeNO), forced vital capacity (FVC), forced expiratory volume in one second (FEV1), FEV1/FVC, maximum midexpiratory flow (MMEF), maximal expiratory flow at 75%, 50%, and 25% of vital capacity (MEF75%, MEF50%, MEF25%). These indicators were collected before SCIT initiation.
Detection of Serum tIgE and sIgE
Serum tIgE and sIgE to Der p and Der f were measured with ImmunoCAP (Thermo Fisher Scientific Inc, Sweden) according to the manufacturer’s instructions. Serum sIgE to Der p 1, Der p 2, Der p 10, and Der p 23 was measured by NOVEOS IgE test (HYCOR Biomedical, America) according to the manufacturer’s instructions. Serum tIgE and sIgE levels were quantified for all samples by certified technicians. Serum levels of tIgE and sIgE were expressed in kUA/L. The measurable range for tIgE was 2.00 to 5000.00kUA/L, and values exceeding 5000.00kUA/L were assigned a value of 5000.00kUA/L. The measurable range for sIgE to Der p, Der f, Der p 1, Der p 2, Der p 10, and Der p 23 was 0.10 to 100.00kUA/L, and values exceeding 100.00kUA/L were assigned a value of 100.00kUA/L. The level of sIgE≧0.35kUA/L was considered positive. sIgE concentrations were quantified and classified into grades 0–6 based on the criteria of China Consensus Document on Allergy Diagnostics: Grade 0 (<0.35kUA/L), Grade 1 (0.35kUA/L≦sIgE<0.70kUA/L), Grade 2 (0.70kUA/L≦sIgE<3.50kUA/L), Grade 3 (3.50kUA/L≦sIgE<17.50kUA/L), Grade 4 (17.50kUA/L≦sIgE<50.00kUA/L), Grade 5 (50.00kUA/L≦sIgE<100.00kUA/L) and Grade 6 (sIgE≧100.00kUA/L).1
Technology Roadmap
In this study, patients receiving HDM SCIT were followed up via the questionnaire survey. Baseline information, laboratory indicators and serum samples of eligible patients were collected, and the efficacy of HDM SCIT was evaluated using the VAS score. The distribution of serum HDM components in patients was analyzed, and a nomogram was constructed via logistic regression analysis. The model was validated using ROC curve, DCA and HL test (Figure 1).
 |
Figure 1 Flowchart for constructing a nomogram. Abbreviations: SCIT, Subcutaneous immunotherapy; VAS, Visual analogue scale; CSMS, Combined symptom and medication score; HDM, House dust mite; ROC, Receiver operating characteristic curve; DCA, Decision curve analysis; HL test, Hosmer–Lemeshow test. Notes: VAS↓≥30%, responders to SCIT were defined as individuals who demonstrated at least a 30% improvement in their VAS scores from the baseline after 12 months of undergoing SCIT. |
Statistical Analysis
All data were processed via SPSS 27.0 (IBM, Armonk, NY, USA) and R software. Most data were not normally distributed (Shapiro-Wilks test: most P values are less than 0.05), therefore continuous variables were presented as median with interquartile range (IQR). Categorical variables were presented as percentages. The Author Proof Photograph χ2 test or the Mann–Whitney test was used to compare differences between groups. To assess the variables associated with the efficacy of SCIT, we employed univariate logistic regression analysis. Variables with P<0.05 in univariate analysis were entered into a multivariable logistic regression model. The predictive model was then assessed using a forward conditional selection procedure, eliminated variables with an exit threshold set at P=0.05. Odds ratios (ORs) with 95% confidence intervals (CI) and P values were calculated. A nomogram was constructed to predict the efficacy of HDM SCIT. Bootstrap method was used to verify the model. The discriminatory ability of the nomogram was assessed by the area under the receiver operating characteristic curve (AUC). An AUC value closer to 1.0 than to 0.5 indicated better model performance. Model calibration was evaluated by calibration curves and the Hosmer–Lemeshow (HL) test. The clinical utility of the prediction model was assessed through decision curve analysis (DCA). Statistical significance for all analyses was defined as a two-sided p-value<0.05.
Results
Patients’ Baseline Information, Laboratory Indicators and Serum IgE Levels
Among the 314 children who received HDM SCIT, efficacy was successfully evaluated in 209 patients (67%) after one year of treatment. Among the evaluated children, 166 (79%) responded to HDM SCIT, while 43 (21%) were non-responders. Detailed reasons for follow-up failure were provided (Figure 1). In the 209 successfully followed-up children, the age range was 5 to 15 years and the body mass index (BMI) range was 13.89 to 31.76 kg/m2. The prevalence of asthma was higher in responders than in non-responders. After 1 year of SCIT, the CSMS and VAS scores of the responders decreased significantly compared to the non-responders (P<0.05). There was no statistically significant difference in the C-ACT scores (P>0.05). Children who were responsive to HDM SCIT demonstrated significantly higher serum IgE levels of Der p 1 sIgE, Der p 2 sIgE, Der p (1+2) sIgE, tIgE, Der p sIgE, and Der f sIgE than non-responsive children did (P<0.05). These responsive children also showed significantly higher ratios of Der p 1 sIgE/tIgE, Der p 2 sIgE/tIgE, Der p sIgE/tIgE, and Der p (1+2) sIgE/tIgE than non-responsive children (P<0.05). No statistically significant differences were detected in laboratory indicators, Der p 10 sIgE, Der p 23 sIgE, or the Der f sIgE/tIgE ratio (Table 1).
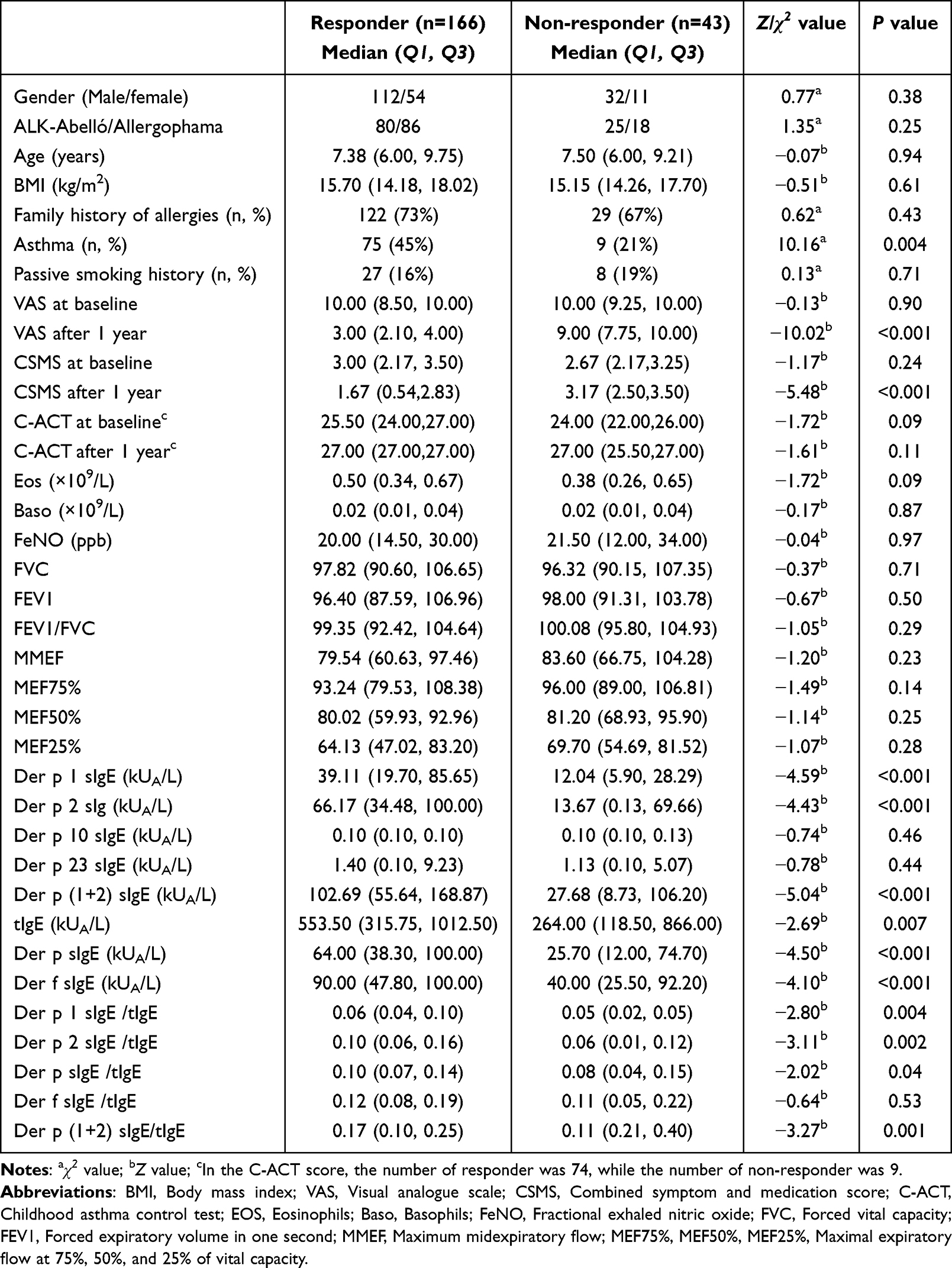 |
Table 1 Comparison of Baseline Information, Laboratory Indicators and Serum IgE Levels Between Responders and Non-Responders |
Sensitization Prevalence and Distribution Characteristics of HDM Components
Among the 209 patients, all (100%) showed IgE reactivity to HDM extracts (Der p and Der f). Sensitization to specific Der p components was distributed as follows: Der p 1 (96%), Der p 2 (88%), Der p 23 (56%), and Der p 10 (9%). There were significant differences in sensitization prevalence among Der p components (χ2=416.62, P<0.001). The sIgE levels to Der p (98%), Der f (98%), Der p 1 (94%), and Der p 2 (86%) were predominantly in grades 3, 4, 5, and 6 [Supplementary Table 1].
Comparison of Serum IgE in Children with AR and/or AS
In children with AR, the sIgE levels to Der p, Der f, Der p 1, and Der p (1+2), as well as tIgE, were significantly lower than those in children with AR and AS (P<0.05). However, the sIgE levels to Der p 2, Der p 10, and Der p 23 in children with AR were lower than those in children with AR and AS, but the difference was not significant (P>0.05) [Supplementary Table 2].
Logistic Regression Analysis of Predictors Associated with SCIT Responders
To identify the predictors of SCIT efficacy, the variables that showed statistically significant differences (P<0.05) in Tables 1 were included in univariate and subsequent multivariate logistic regression analyses (Forward conditional method). Three predictors were identified, namely asthma (OR=3.11, P=0.007), Der p (1+2) sIgE (OR=1.02, P<0.001), and the Der p (1+2) sIgE/tIgE ratio (OR=1070.48, P=0.001) (Table 2).
 |
Table 2 Candidate Predictors for SCIT Efficacy on Logistic Regression Analyses |
Nomogram Prediction
Based on logistic regression results, three variables were selected to construct a nomogram for predicting the efficacy of HDM SCIT, including Der p (1+2) sIgE, the Der p (1+2) sIgE/tIgE ratio, and asthma (Figure 2). A higher total nomogram score indicated a greater likelihood that HDM SCIT would be effective. For example, for a patient with serum Der p (1+2) sIgE level of 200 kUA/L, a Der p (1+2) sIgE/tIgE ratio of 0.04, and no asthma, the nomogram score for SCIT efficacy was 63.2 points, which corresponded to a predicted probability of effective SCIT of 83.70%.
 |
Figure 2 A nomogram model for predicting the efficacy of HDM SCIT. |
Bootstrap method (B=1000) was used to verify the model [Supplementary Table 3]. DCA indicated that the nomogram offered significant net benefit. This net benefit was occurred across at threshold probabilities between 24% and 91% (Figure 3A). For the nomogram, the calibration curve showed no significant difference between the predicted and actual probabilities of effective SCIT (χ2=15.48, df=8, P=0.051>0.05) (Figure 3B). The nomogram achieved an AUC of 0.80 (95% CI=0.72–0.87) and a C-index of 0.80 (95% CI=0.72–0.87) (Figure 4A).
 |
Figure 3 (A) Calibration curves assessing the efficacy of HDM SCIT. (B) Decision curve analysis of the SCIT nomogram. |
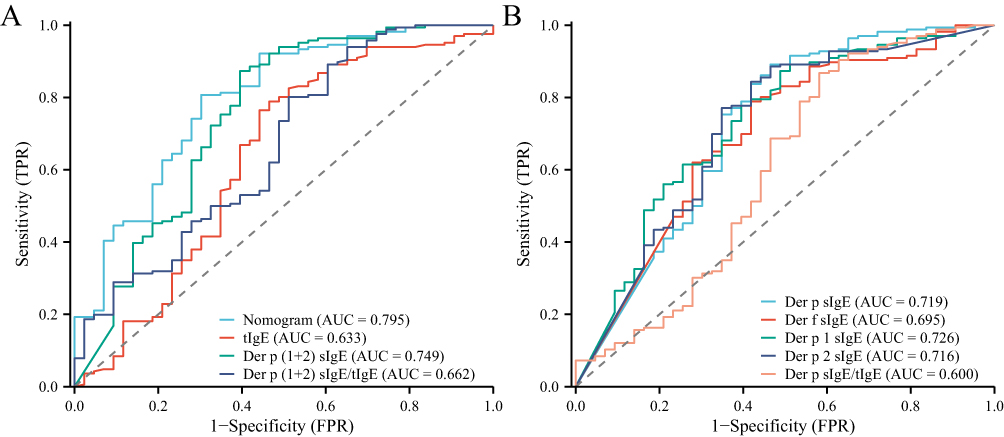 |
Figure 4 (A) ROC of the nomogram and of predictors. (B) ROC of serum HDM sIgE. |
Predictive Capacity of the Nomogram and of Serum IgE for SCIT Efficacy
We compared the predictive capacity of the nomogram, serum tIgE, serum HDM sIgE for SCIT efficacy using ROC curves (Figure 4A and B). At a cutoff value of 0.75, the nomogram demonstrated a sensitivity of 80% and a specificity of 65% (AUC=0.80). At a cutoff value of 43.87kUA/L, Der p (1+2) sIgE demonstrated a sensitivity of 78% and a specificity of 63% (AUC=0.75). At a cutoff value of 10%, the Der p (1+2) sIgE/tIgE ratio demonstrated a sensitivity of 84% and a specificity of 56% (AUC=0.66) (Table 3).
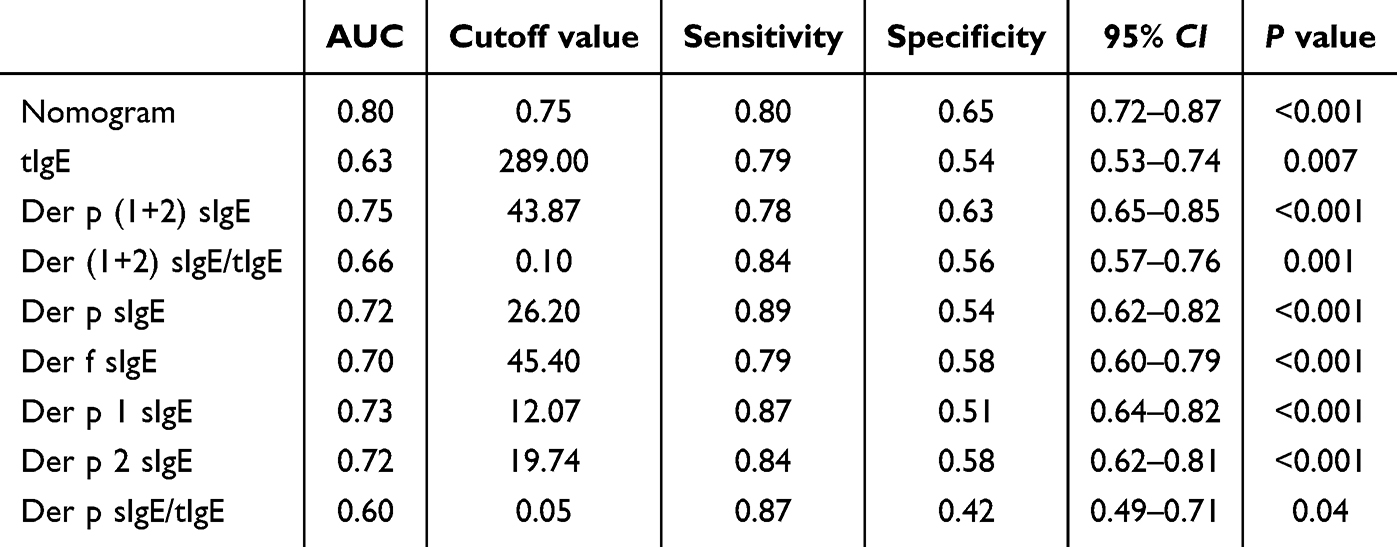 |
Table 3 Predictive Capacity of the Nomogram and of Serum IgE |
Discussion
Although SCIT was currently the only disease-modifying treatment for allergic diseases, its clinical application remained limited due to suboptimal efficacy in some patients, high costs, and a prolonged treatment duration.22–24 Therefore, the identification of biomarkers to accurately predict the efficacy of HDM SCIT held significant clinical importance. This study analyzed the relationship between serum sIgE to HDM components and the efficacy of HDM SCIT in patients. We explored the predictive value of Der p 1 and Der p 2 for SCIT efficacy and developed a nomogram to predict it visually and quantitatively.
Consistent with some studies, Der p 1, Der p 2, and Der p 23 were identified as the major sensitizing HDM components in patients with AR and/or AS, demonstrating sensitization rates exceeding 50%.2,25,26 In this study, over 90% of the patients were sensitized to Der p 1 and Der p 2, indicating that the current HDM SCIT targeting these components may be appropriate for most children. However, some patients exhibited sensitization only to Der p 10 and Der p 23, suggesting a potentially reduced therapeutic response to HDM SCIT. This indicated that variations in sensitization profiles to HDM components among patients highlighted the clinical significance of component-resolved diagnostics for predicting SCIT efficacy. Additionally, the SCIT response rate was 79% in our study, below the 90% threshold. This observation indicates that while HDM component profiles contribute to outcomes, the efficacy of HDM SCIT is also modulated by other factors independent of allergen sensitization patterns.27–29
To explore potential clinical predictors as comprehensively as possible, we conducted a thorough and detailed investigation of 209 pediatric patients’ baseline information, laboratory indicators and serum IgE levels. This study encompassed involves multiple combinations of major HDM components (Der p 1 and Der p 2) to investigate the relationship between HDM components and the efficacy of SCIT. Furthermore, we employed various analysis approaches to identify the key predictors and develop the prediction model. Through between-group comparison and logistic regression analysis, we successfully identified asthma, Der p (1+2) sIgE, and the Der p (1+2) sIgE/tIgE ratio as the top-ranked variables. Furthermore, we constructed the nomogram for the efficacy of HDM SCIT. By incorporating these three markers into a prediction model, we achieved a higher predictive value for responders compared to using single parameters alone. The model demonstrated good predictive capability, with a C-index of 0.80, AUC of 0.80, sensitivity of 80%, and specificity of 65%. The calibration curve indicated good accuracy, with observed probabilities in good agreement with the predicted probabilities (HL test, P>0.05). Decision curve analysis suggested that the nomogram had clinical utility for predicting the efficacy of HDM SCIT.
Importantly, compared with the existing models,30–32 the predictive indicators used in our nomogram were easily accessible in clinical practice and had high accuracy, which was helpful for rapid prediction of SCIT effects. For example, Wang et al used a random forest algorithm to identify the sIgE/tIgE ratio, TFR/TFH2 cell ratio, and CD23+BSM frequency as key biomarkers for predicting the efficacy of SCIT. Furthermore, they developed a prediction model for SCIT efficacy using these biomarkers, and this model showed excellent predictive performance with an AUC of 0.90.30 However, the study employed flow cytometry to detect the relevant biomarkers, limiting its current widespread application in clinical settings. Liu et al proposed combining therapeutic effect within 8 weeks with the sIgE/tIgE ratio to predict long-term HDM SCIT efficacy. However, this model achieved only moderate predictive performance (AUC=0.69) and required post-treatment data, preventing pre-treatment efficacy prediction.31
In clinical practice, when sIgE levels of HDM exceed 0.70kUA/L with associated allergic symptoms, HDM SCIT may be considered.1,33 However, the specific efficacy of SCIT requires further evaluation. Currently, studies predicting the efficacy of HDM SCIT are mostly focused on Der p sIgE and tIgE. Liu et al demonstrated that a Der p sIgE/tIgE ratio≧12.6% effectively predicted the efficacy of sublingual immunotherapy (SLIT), with its predictive performance superior to that of Der p sIgE.34 Tu et al proposed that the efficacy of HDM SCIT was primarily associated with sIgE. When the sIgE levels of Der p reached or exceeded 53.86 kUA/L, this level could effectively predict the efficacy of HDM SCIT.35 These findings suggested that the higher the sIgE levels were, the greater the likelihood of response to HDM immunotherapy. However, Der p 1 sIgE and Der p 2 sIgE in relation to the efficacy of HDM SCIT are rarely studied. Whether Der p 1 sIgE and Der p 2 sIgE can serve as biomarkers for predicting the efficacy of HDM SCIT remains inconclusive.36–38 Some studies found that Der p 1 sIgE and Der p 2 sIgE decreased in children with AR undergoing HDM SCIT.37 Furthermore, changes in Der p 1 sIgE and Der p 2 sIgE showed a significant positive correlation with clinical symptom improvement (P<0.05).38 These findings suggest that Der p 1 sIgE and Der p 2 sIgE may serve as effective biomarkers for the efficacy of HDM SCIT. Our study discovered that the baseline levels of Der p 1 sIgE and Der p 2 sIgE were significantly higher in responders than in non-responders (P<0.05). This implied that patients with elevated levels of Der p 1 sIgE and Der p 2 sIgE exhibited better responses to HDM SCIT. Thresholds of 43.87 kUA/L for Der p (1 + 2) sIgE effectively predicted the efficacy of HDM SCIT. Moreover, their predictive performance was superior to tIgE, Der p sIgE and the Der p sIgE/tIgE ratio. Therefore, Der p 1 sIgE and Der p 2 sIgE could serve as biomarkers.
In this study, asthma (AS) was significantly associated with the efficacy of HDM SCIT, suggesting that HDM allergic children with AS were more likely to respond to the therapy. To date, no prior studies had supported this conclusion. Previous studies had found that the immune mechanisms of SCIT for AR with and without AS were different.39 Patients with AS might exhibit a more robust Th2-type immune response,40 which was more responsive to SCIT. Besides, patients with AS often had higher levels of sIgE to major HDM components (Der p 1 and Der p 2),41,42 which correlated with greater clinical benefit from SCIT. This aligned with our previous finding that HDM SCIT demonstrated better efficacy if the Der p (1+2) sIgE levels reached or exceeded 43.87 kUA/L. We also noted that asthma-related airway inflammation might enhance dendritic cell activation and antigen presentation, leading to improved immunological tolerance induction.43
There were several limitations in our current nomogram. Firstly, the target population of the nomogram was children aged 5 to 15 years with AR and/or AS who were monosensitization to HDM only. Therefore, this model should not be extrapolated to adults, patients with polysensitization, or those who did not have AR and/or AS. Secondly, the nomogram was only internally validated in a single-center cohort, which might introduce a selection bias. The nomogram required external validation in randomized, double-blind, placebo-controlled trials with larger sample size to confirm its clinical utility and generalization. Thirdly, this study used two different immunoassay platforms. Serum tIgE and sIgE to HDM extracts (Der p and Der f) were measured using the ImmunoCAP system, while sIgE to HDM components (Der p 1, 2, 10, and 23) was assayed using the NOVEOS platform. While both systems were validated and widely used, inherent differences in assay principles, calibration, and dynamic ranges might affect the comparability of absolute IgE values. Therefore, our results should be interpreted with caution, and future studies should consider using a single platform or perform cross-platform validation for direct comparisons.
Conclusion
In our study, we developed a nomogram to predict the efficacy of HDM SCIT using asthma, Der p (1+2) sIgE, and the Der p (1+2) sIgE/tIgE ratio in children with AR and/or AS. With clinically accessible predictors, the model demonstrated robust predictive performance in the validation cohort, and the conclusions drawn from the study were directly supported by the nomogram’s calibration and discrimination metrics.
Data Sharing Statement
The datasets generated and/or analyzed during the current study are not publicly available due to patient privacy and ethical restrictions but are available from the corresponding author Yan-Min Bao on reasonable request and with approval from the Ethics Committee of Shenzhen Children’s Hospital, Guangdong, China.
Ethics Approval
The study was approved by the Ethics Committee of Shenzhen Children’ s Hospital, Guangdong, China (No. 202307402). Written informed consent was obtained from the legal guardian/parent of the minors prior to study commencement. This study adhered to the ethical standards of the Declaration of Helsinki and its amendments.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Yan-Min Bao’s research was supported by the Precision Diagnosis and Treatment Breakthrough Project for Difficult and Complicated Diseases of Shenzhen Children’s Hospital (No. LCYJ2022070). Yan Zhang’s research was supported by the National Social Science Fund of China (No.23BTJ054), and open project of Nanjing Audit University Joint Lab for Statistics and Finance (No.2025JLSF309).
Disclosure
The authors declared that they had no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
References
1. Chen H, Li J, Cheng L, et al. China consensus document on allergy diagnostics. Allergy Asthma Immunol Res. 2021;13(2):177–12. doi:10.4168/aair.2021.13.2.177
2. Zou X, Hu H, Huang Z, et al. Serum levels of specific immunoglobulin E to Dermatophagoides pteronyssinus allergen components in patients with allergic rhinitis or/and asthma. Allergy Asthma Proc. 2021;42(1):e40–e46. doi:10.2500/aap.2021.42.200105
3. Hesse L, Oude Elberink JNG, van Oosterhout AJM, et al. Allergen immunotherapy for allergic airway diseases: use lessons from the past to design a brighter future. Pharmacol Ther. 2022;237:108115. doi:10.1016/j.pharmthera.2022.108115
4. Zhi L, Bai Y, Liao W, et al. The safety and tolerability of a one strength dose-escalation scheme for subcutaneous immunotherapy with a native house dust mite extract in Chinese children: a multicenter, randomized, open label clinical trial. Heliyon. 2024;10(8):e29450. doi:10.1016/j.heliyon.2024.e29450
5. Spiric J, Reuter A, Rabin RL. Mass spectrometry to complement standardization of house dust mite and other complex allergenic extracts. Clin Exp Allergy. 2017;47(5):604–617. doi:10.1111/cea.12931
6. Muddaluru V, Valenta R, Vrtala S, et al. Comparison of house dust mite sensitization profiles in allergic adults from Canada, Europe, South Africa and USA. Allergy. 2021;76(7):2177–2188. doi:10.1111/all.14749
7. Posa D, Hofmaier S, Arasi S, et al. Natural evolution of IgE responses to mite allergens and relationship to progression of allergic disease: a review. Curr Allergy Asthma Rep. 2017;17(5):28. doi:10.1007/s11882-017-0697-y
8. Batard T, Baron-Bodo V, Martelet A, et al. Patterns of IgE sensitization in house dust mite-allergic patients: implications for allergen immunotherapy. Allergy. 2016;71(2):220–229. doi:10.1111/all.12796
9. Casset A, Mari A, Purohit A, et al. Varying allergen composition and content affects the in vivo allergenic activity of commercial Dermatophagoides pteronyssinus extracts. Int Arch Allergy Immunol. 2012;159(3):253–262. doi:10.1159/000337654
10. Rodríguez-Domínguez A, Berings M, Rohrbach A, et al. Molecular profiling of allergen-specific antibody responses may enhance success of specific immunotherapy. J Allergy Clin Immunol. 2020;146(5):1097–1108. doi:10.1016/j.jaci.2020.03.029
11. Caraballo L, Valenta R, Acevedo N, et al. Are the terms major and minor allergens useful for precision allergology? Front Immunol. 2021;12:651500. doi:10.3389/fimmu.2021.651500
12. Shamji MH, Kappen JH, Akdis M, et al. Biomarkers for monitoring clinical efficacy of allergen immunotherapy for allergic rhinoconjunctivitis and allergic asthma: an EAACI Position Paper. Allergy. 2017;72(8):1156–1173. doi:10.1111/all.13138
13. Tan TJ, Layhadi JA, Shamji MH. Mechanisms and biomarkers of subcutaneous immunotherapy and sublingual immunotherapy in allergen immunotherapy. Allergy Asthma Proc. 2022;43(4):254–259. doi:10.2500/aap.2022.43.220030
14. Şahin E, Bafaqeeh SA, Güven SG, et al. Mechanism of action of allergen immunotherapy. Am J Rhinol Allergy. 2016;30(5):1–3. doi:10.2500/ajra.2016.30.4367
15. Di Lorenzo G, Mansueto P, Pacor ML, et al. Evaluation of serum s-IgE/total IgE ratio in predicting clinical response to allergen-specific immunotherapy. J Allergy Clin Immunol. 2009;123(5):1103–1110, 1110.e1–e4. doi:10.1016/j.jaci.2009.02.012
16. Li Q, Li M, Yue W, et al. Predictive factors for clinical response to allergy immunotherapy in children with asthma and rhinitis. Int Arch Allergy Immunol. 2014;164(3):210–217. doi:10.1159/000365630
17. Brożek JL, Bousquet J, Agache I, et al. Allergic Rhinitis and its Impact on Asthma (ARIA) guidelines-2016 revision. J Allergy Clin Immunol. 2017;140(4):950–958. doi:10.1016/j.jaci.2017.03.050
18. Bousquet J, Pfaar O, Togias A, et al. 2019 ARIA Care pathways for allergen immunotherapy. Allergy. 2019;74(11):2087–2102. doi:10.1111/all.13805
19. Bousquet PJ, Combescure C, Neukirch F, et al. Visual analog scales can assess the severity of rhinitis graded according to ARIA guidelines. Allergy. 2007;62(4):367–372. doi:10.1111/j.1398-9995.2006.01276.x
20. Pfaar O, Demoly P, Gerth van Wijk R, et al. Recommendations for the standardization of clinical outcomes used in allergen immunotherapy trials for allergic rhinoconjunctivitis: an EAACI Position Paper. Allergy. 2014;69(7):854–867. doi:10.1111/all.12383
21. Liu AH, Zeiger R, Sorkness C, et al. Development and cross-sectional validation of the childhood asthma control test. J Allergy Clin Immunol. 2007;119(4):817–825. doi:10.1016/j.jaci.2006.12.662
22. Roberts G, Pfaar O, Akdis CA, et al. EAACI Guidelines on Allergen Immunotherapy: allergic rhinoconjunctivitis. Allergy. 2018;73(4):765–798. doi:10.1111/all.13317
23. Agache I, Lau S, Akdis CA, et al. EAACI guidelines on allergen immunotherapy: house dust mite-driven allergic asthma. Allergy. 2019;74(5):855–873. doi:10.1111/all.13749
24. Alvaro-Lozano M, Akdis CA, Akdis M, et al. EAACI allergen immunotherapy user’s guide. Pediatr Allergy Immunol. 2020;31(Suppl 25):1–101. doi:10.1111/pai.13189
25. Posa D, Perna S, Resch Y, et al. Evolution and predictive value of IgE responses toward a comprehensive panel of house dust mite allergens during the first 2 decades of life. J Allergy Clin Immunol. 2017;139(2):541–549. doi:10.1016/j.jaci.2016.08.014
26. Liu Y, Zhao L, Wang J, et al. Serological analysis of allergic components of house dust mite provides more insight in epidemiological characteristics and clinical symptom development in North China. Front Immunol. 2023;14:1083755. doi:10.3389/fimmu.2023.1083755
27. Shin YS, Jung JW, Park JW, et al. Clinical Efficacy of Allergen-Specific Immunotherapy from Patient and Physician Perspectives. Yonsei Med J. 2019;60(5):446–453. doi:10.3349/ymj.2019.60.5.446
28. Huang Y, Wang C, Cao F, et al. Comparison of long-term efficacy of subcutaneous immunotherapy in pediatric and adult patients with allergic rhinitis. Allergy Asthma Immunol Res. 2019;11(1):68–78. doi:10.4168/aair.2019.11.1.68
29. Lin Y, Liu J, He J, et al. Effects of subcutaneous immunotherapy in allergic rhinitis children sensitive to dust mites. Allergol Immunopathol. 2023;51(1):84–91. doi:10.15586/aei.v51i1.666
30. Wang N, Song J, Sun SR, et al. Immune signatures predict response to house dust mite subcutaneous immunotherapy in patients with allergic rhinitis. Allergy. 2024;79(5):1230–1241. doi:10.1111/all.16068
31. Liu D, Li J, Gao Y, et al. Clinical response to subcutaneous immunotherapy at 3 years in allergic rhinitis patients is predicted by short-term treatment effectiveness. Clin Transl Allergy. 2023;13(2):e12223. doi:10.1002/clt2.12223
32. Wang M, Gong L, Luo Y, et al. Transcriptomic analysis of asthma and allergic rhinitis reveals CST1 as a biomarker of unified airways. Front Immunol. 2023;14:1048195. doi:10.3389/fimmu.2023.1048195
33. Namysłowski A, Lipiec A, Zieliński W, et al. The importance of specific IgE antibodies in the epidemiology of allergic rhinitis and asthma (ECAP survey): part five. The relationship between the concentration of specific IgE antibodies in serum and types of rhinitis. Postepy Dermatol Alergol. 2023;40(5):617–624. doi:10.5114/ada.2023.130314
34. Liu W, Zeng Q, Luo R. Predictors for short-term efficacy of allergen-specific sublingual immunotherapy in children with allergic rhinitis. Mediators Inflamm. 2020;2020:1847061. doi:10.1155/2020/1847061
35. Tu YY, Yuan GM, Shi FP, et al. [Predictor of clinical response to subcutaneous immunotherapy with dust mites in polysensitized allergic rhinitis patients]. Zhonghua Er Bi Yan Hou Tou Jing Wai Ke Za Zhi. 2023;58(10):992–997. Chinese. doi:10.3760/cma.j.cn115330-20230329-00139
36. Wang J, Xu B, Jia X, et al. Predictive value of Der p 2-specific IgE for subcutaneous immunotherapy in children with allergic rhinitis. Sci Rep. 2024;14(1):25467. doi:10.1038/s41598-024-73575-6
37. Huang J, Xiang R, Tan L, et al. Dust mite component analysis: identifying key allergens components for effective immunotherapy in allergic rhinitis. Int Immunopharmacol. 2023;125(Pt A):111111. doi:10.1016/j.intimp.2023.111111
38. Arroabarren E, Echechipía S, Galbete A, et al. Association between component-resolved diagnosis of house dust mite allergy and efficacy and safety of specific immunotherapy. J Investig Allergol Clin Immunol. 2019;29(2):164–167. doi:10.18176/jiaci.0359
39. Shamji MH, Sharif H, Layhadi JA, et al. Diverse immune mechanisms of allergen immunotherapy for allergic rhinitis with and without asthma. J Allergy Clin Immunol. 2022;149(3):791–801. doi:10.1016/j.jaci.2022.01.016
40. Bousquet J, Melén E, Haahtela T, et al. Rhinitis associated with asthma is distinct from rhinitis alone: the ARIA-MeDALL hypothesis. Allergy. 2023;78(5):1169–1203. doi:10.1111/all.15679
41. Yang Y, Zhu R, Huang N, et al. The Dermatophagoides pteronyssinus Molecular Sensitization Profile of Allergic Rhinitis Patients in Central China. Am J Rhinol Allergy. 2018;32(5):397–403. doi:10.1177/1945892418787116
42. Flashner BM, Rifas-Shiman SL, Oken E, et al. Contributions of asthma, rhinitis and IgE to exhaled nitric oxide in adolescents. ERJ Open Res. 2021;7(2):00945–2020. doi:10.1183/23120541.00945-2020
43. Fiala S, Fleit HB. Clinical and experimental treatment of allergic asthma with an emphasis on allergen immunotherapy and its mechanisms. Clin Exp Immunol. 2023;212(1):14–28. doi:10.1093/cei/uxad031
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.