Back to Journals » International Journal of Nanomedicine » Volume 21
Precision Pediatric Cancer Nanomedicine: Advancing Personalized Nano Therapies to Reduce Non-Communicable Diseases Through AI-Driven 3D-Printed Drugs
Authors Choudhary N, Kumar D ![]() , Jyoti TP, Prajapati BG, Kchaou M
, Jyoti TP, Prajapati BG, Kchaou M ![]() , Webster TJ
, Webster TJ ![]() , Faiyazuddin M
, Faiyazuddin M ![]()
Received 18 October 2025
Accepted for publication 26 January 2026
Published 13 February 2026 Volume 2026:21 575214
DOI https://doi.org/10.2147/IJN.S575214
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. RDK Misra
Neeraj Choudhary,1 Dinesh Kumar,1 Thakur Prava Jyoti,2 Bhupendra G Prajapati,3 Mohamed Kchaou,4 Thomas J Webster,5– 7 Md Faiyazuddin8
1GNA School of Pharmacy, GNA University, Phagwara, Punjab, 144401, India; 2University College of Pharmaceutical Sciences, Guru Kashi University, Talwandi Sabo, Bathinda, Punjab, 151302, India; 3Department of Pharmaceutics, Parul Institute of Pharmacy, Faculty of Pharmacy, Parul University, Waghodia, Vadodara, Gujarat, 391760, India; 4Department of Industrial Engineering, College of Engineering, University of Bisha, Bisha, Saudi Arabia; 5Division of Pre-College and Undergraduate Studies, Brown University, Providence, RI, 02917, USA; 6School of Health Sciences and Biomedical Engineering, Hebei University of Technology, Tianjin, 300131, People’s Republic of China; 7School of Engineering, Saveetha University, Chennai, 600077, India; 8Center for Global Health Research, Saveetha Institute of Medical and Technical Sciences, Chennai, Tamil Nadu, India
Correspondence: Md Faiyazuddin, Email [email protected] Thomas J Webster, Email [email protected]
Abstract: Pediatric cancers (PC) require treatments that maintain cure rates while minimizing long-term toxicity and non-communicable diseases. Yet, conventional dosing, adult-oriented formulations, and high treatment burden remain major limitations in childhood cancer care. This review synthesizes the current evidence using artificial intelligence (AI) and 3D nano printing as emerging tools to support personalized pediatric oncology. A structured literature search of PubMed, Scopus, Web of Science, and Google Scholar (2005– 2024) identified English-language studies related to pediatric cancer, nanomedicine (NM), 3D printing, precision dosing, and pharmacogenomics, and relevant findings were organized by cancer type, clinical application, and potential impact on toxicity, adherence, and survivorship. Across leukemia, neuroblastoma, brain tumors, bone sarcoma, and lymphoma, AI-supported platforms were found to improve individualized chemotherapy exposure, anticipate toxicity based on clinical or pharmacogenomic markers, and assist clinicians towards modifying early treatment. At the same time, 3D nano printing enabled child-friendly medicines, multi-drug polypills, and controlled-release formulations that reduced dosing errors and improved treatment adherence. Early hospital-based experience with Bayesian therapeutic drug monitoring and on-demand pediatric drug printing suggested high feasibility for real clinical settings. Overall, AI-guided dosing and nano-printed formulations enhanced precision, lowering acute and late toxicities that support healthier long-term outcomes in children with cancer, particularly when linked to disease-specific needs. Further multicenter pediatric studies, regulatory development, and expansion of hospital 3D printing capacity are recommended to enable safe and equitable translation of these technologies into routine clinical care.
Keywords: pediatric oncology, artificial intelligence, 3D printing, personalized medicine, non-communicable diseases
Introduction
Every year, more than 400,000 children are diagnosed with cancer, making it one of the leading causes of childhood illness and death worldwide.1 While survival rates for acute lymphoblastic leukemia are above 90% in high-income countries, they remain below 40% in many low and middle-income countries. Even for children who survive, current treatments often bring serious challenges. Most medicines are designed for adults and then adapted for children, which can lead to dosing errors, poor adherence, and harmful side effects. Long-term survivors also face risks of non-communicable diseases such as heart disease from anthracyclines, hearing loss from cisplatin, and learning difficulties after cranial irradiation.2,3 This highlights the urgent need for safer, personalized treatments tailored specifically to children.
New technologies such as artificial intelligence (AI) and 3D nano printing are creating opportunities to meet this need. AI driven molecular profiling can analyze genetic, clinical, and treatment data to predict how a child will respond to therapy, adjust doses, reduce the risk of side effects and improve adherence (Figure 1A and B).4 At the same time, 3D nano printing enables the production of personalized medicines on demand, such as flavored chewable tablets, mini-tablets, and polypills tailored to a child’s age, weight, genetic profile, and treatment plan.4,5 These approaches also allow for controlled-release formulations, which help maintain stable drug levels and reduce toxic peaks.6 Together, AI and 3D nano printing promise not only to improve survival but also to protect children from long-term cancer complications under a new term “Precision Pediatric Cancer Nanomedicine”. Despite rapid innovations, several challenges regarding translation into pediatric oncology remain persistence. These include a lack of dedicated attention to the development of pediatric-specific nanocarriers; an absence of AI-informed molecular profiling in how treatments are selected; scant utilization of organoid or ex vivo tumor models for dosing customization; limited strides toward personalized pediatric drug printing; and scattered literature that fails to bring these cutting-edge technologies together into a single, cohesive framework.
 |
Figure 1 Integration of AI-driven approaches into precision pediatric cancer nanomedicine. This figure illustrates how ML algorithms integrate multidimensional, genomic, clinical, and environmental data to optimize pediatric cancer management. AI models analyze complex datasets to guide personalized nano treatment strategies, including optimized dosing and formulation design. The solid arrows reflect how patient data feed into the AI/ML model to yield optimized dosing and personalized treatment plans. Horizontal arrows from AI toward the patient indicate model-driven therapeutic recommendations. The dotted line reflects the indirect route through which the AI-assisted choices translate into better outcomes that aim to: (A) reduce drug toxicity, (B) enhance treatment adherence, (C) minimize the risk of non-communicable diseases, and (D) ultimately improve survival outcomes in pediatric oncology patients. |
Earlier published reviews have discussed AI in oncology7 and/or 3D printing in pharmaceuticals.5 However, none have brought these fields together in the context of precision pediatric cancer nanomedicine (NM). This current review focuses on the combined use of AI and 3D nano printing in pediatric cancer care, with a special emphasis on reducing treatment-related non-communicable diseases (NCDs) (Figure 1C and D). It brings together AI-driven drug formulation strategies, pharmacogenomics, personalized 3D-printed medicines, and real-world clinical evidence into a single integrated framework. By addressing both technological innovations and clinical challenges, this manuscript presents a fresh perspective from past findings on how these tools centered on NM can transform pediatric oncology.8 Despite progress in chemotherapy, radiotherapy, and supportive care, most existing studies continue to rely on adult-derived dose strategies, fragmented formulations, and retrospective toxicity management. Previous reviews have examined AI in oncology or 3D printing in pharmaceuticals, but they do not address these technologies in a pediatric-specific context or evaluate their combined role in improving treatment adherence, pharmacogenomics-based dosing, and prevention of long-term non-communicable diseases.9 This gap limits understanding of how precision manufacturing and computational tools may reshape survivorship. Therefore, this review aims to synthesize the current evidence of AI-assisted dosing and 3D nano-printed pediatric drug formulations, summarizing their disease-specific applications, and assessing their potential to reduce toxicity, enhance adherence, and support long-term pediatric cancer outcomes.
Methodology of Literature Search
This work is a review based on a structured search of PubMed, Scopus, Web of Science, and Google Scholar for English-language articles published from 2005–2024. Search terms covered pediatric cancer, NM, 3D printing, artificial intelligence, precision dosing, and pharmacogenomics. Relevant clinical studies and reviews were screened, and non-oncology or non-clinical engineering papers were excluded. Due to heterogeneity in study designs, a meta-analysis was not performed; instead, findings were summarized narratively and organized by cancer type, clinical application, and implications for toxicity reduction, adherence, and survivorship. The synthesized evidence was used to outline current progress and future recommendations.
Pediatric Cancer Challenges and the Need for Personalized Nano Therapies
PC care presents unique challenges distinct from those in adult oncology. Treatments often do not consider children’s specific genetic backgrounds, leading to long-term side effects like heart disease and secondary cancers.10 Genetic variability within tumors causes parts of the same tumor to respond differently, increasing the risk.11 Difficulties with medication forms and treatment adherence further limit success. These challenges highlight the urgent need for personalized, child-friendly therapies (Table 1). A detailed discussion is provided in the subsections below.
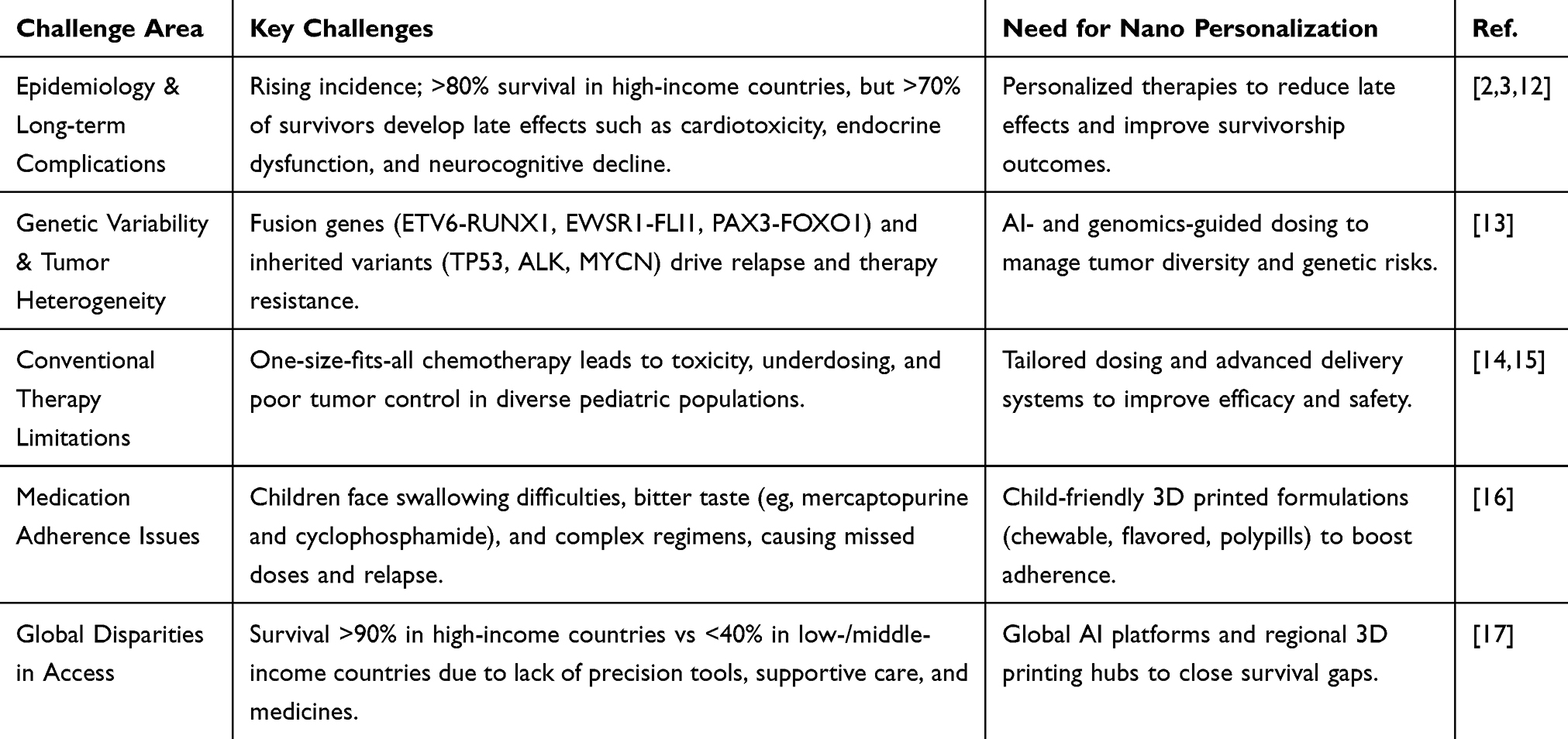 |
Table 1 Key Challenges and Treatment Gaps in Pediatric Oncology |
Epidemiology and Long-Term Treatment Complications
PC remains a leading cause of disease-related mortality in children and adolescents, with global incidence rates showing a gradual but steady increase in recent decades. Leukemia, central nervous system tumors, and lymphomas remain the most common childhood cancers, reflecting a significant burden on healthcare systems worldwide.18 While survival rates have improved substantially due to advancements in chemotherapy, radiotherapy, and supportive care, the long-term health consequences of these treatments present critical challenges.
Evidence from survivorship cohorts highlights that a large majority of children treated for cancer develop late complications. For instance, a Polish multicenter study of survivors diagnosed before the age of three reported that only 17% retained normal function across all organ systems, while over 80% experienced dysfunction in at least one system, commonly affecting the cardiovascular, urinary, auditory, immune, and visual domains.19,20 Further, data from the British Childhood Cancer Survivor Study demonstrated that the risk of mortality extends far beyond the initial five-year survival mark. Second primary cancers, circulatory disease, and pulmonary disease accounted for 77% of the excess deaths observed 45 years after the initial cancer diagnosis.21 Such findings emphasize that pediatric cancer survivors are at a heightened risk of developing chronic non-communicable diseases, including cardiac dysfunction and secondary malignancies, which substantially reduce life expectancy and quality of life. Importantly, while improvements in frontline therapy have reduced cancer recurrence, they have simultaneously increased the prevalence of treatment-related complications.
As highlighted in recent reviews, the toxicities of chemotherapy and radiotherapy, ranging from cardiotoxicity to endocrine dysfunction, pose lifelong risks, underscoring the urgent need for precision strategies that minimize exposure while maintaining therapeutic efficacy.22 These epidemiological patterns and survivorship outcomes underscore the necessity for personalized, low-toxicity treatment strategies. Emerging technologies such as AI-driven 3D nano printed drugs offer opportunities to tailor formulations to reduce cumulative toxicity, thereby potentially preventing long-term organ dysfunction and reducing the burden of chronic non-communicable diseases in childhood cancer survivors.23
Genetic Variability and Tumor Heterogeneity
PCs are quite different from adult cancers, especially when it comes to their genetics. While adult cancers tend to have numerous small genetic mutations, known as point mutations, pediatric cancers usually have fewer of these. Instead, child tumors exhibit more significant changes in the structure of their DNA, such as large rearrangements, gene fusions (where parts of two different genes join together), and alterations in the number of copies of certain genes. These genetic changes happen not only by chance but are often inherited from parents, which means some children are born with genetic variants that increase their risk of developing cancer.24,25 Important genes in pediatric cancers include MYCN and ALK in neuroblastoma, WT1 and TP53 in a Wilms’ tumor, and a range of fusion genes, such as ETV6-RUNX1, in childhood leukemia. These inherited and acquired changes together shape how these cancers grow and behave26,27 (Figure 2A).
 |
Figure 2 AI-driven analysis of tumor heterogeneity to personalize nano cancer therapy. This figure illustrates the progression of tumor complexity to targeted therapy exploiting AI. (A) Patient-specific genetic variability, such as gene fusion, further leads to tumor heterogeneity. (B) Intertumor heterogeneity across patients (interpatient), between metastatic locations (inter-metastatic), and in multi-focal disease. (C) Intratumor heterogeneity is cellular, genomic, and epigenetic heterogeneity of a single primary tumor. (D) Personalized nano therapies facilitated by precise AI examination ultimately lead to lower worldwide disease burden and improved patient survival. Solid arrows indicate information flow from genetic alterations and heterogeneity patterns toward detailed tumor analysis and AI-assisted treatment planning. The solid return arrow shows the additional contribution of intratumor heterogeneity to further shaping therapeutic decisions. The dotted arrow reflects the indirect pathway by which individualized therapies should achieve better overall outcomes, resulting in a reduction of global disease burden and improved survival. |
One of the complex aspects of pediatric cancers is their genetic heterogeneity, which means the tumor is composed of different groups of cells with distinct genetic profiles. This can occur between different child tumors (inter-tumor heterogeneity) and even within a single tumor (intra-tumor heterogeneity).28 For example, a Wilms’ tumor may have regions with different genetic mutations like WT1 or varying numbers of copies of chromosomal parts. In contrast, neuroblastoma tumors may contain subpopulations where some cells exhibit MYCN amplification, while others do not.29 This diversity within the tumor can cause some cancer cells to respond differently to treatment, making it hard to eradicate the disease. Importantly, this variation can exist from the early stages of tumor development and change over time, especially after treatment.30 These gene fusions play a big role in pediatric tumor diversity and development. Fusions like ETV6-RUNX1 are common in childhood leukemia, while other fusion genes, such as EWSR1-FLI1, drive Ewing sarcoma, and PAX3-FOXO1 is seen in rhabdomyosarcoma. These genetic rearrangements not only initiate tumors but also contribute to the complexity of genetic changes across different tumor cells. Because these fusion genes often vary in their presence and activity across different parts of the tumor, they add another layer of complexity to tumor heterogeneity, influencing how the tumor grows and its potential resistance to treatment31 (Figure 2B and C).
Understanding the genetic diversity and hereditary factors associated with pediatric cancers is crucial for improving diagnosis, treatment, and monitoring. Different groups of tumor cells may respond differently to therapies, which can lead to treatment resistance and relapse if not all subpopulations are targeted. Taking a biopsy from only one tumor area might miss some genetic differences important for choosing the right treatment. Furthermore, inherited mutations not only increase cancer risk but also affect how a child metabolizes drugs and their chances of side effects or second cancers.32,33 Therefore, combining information about inherited genetics with detailed tumor analysis is crucial to create more effective and personalized treatments for children with cancer (Figure 2D).
Current Gaps in Conventional Therapies and Adherence Issues
The burden of epidemiology and long-term treatment complications, as well as the influence of genetic and tumor heterogeneity, highlights that conventional treatments in pediatric oncology often fail to strike a balance between efficacy and safety. Standard chemotherapy and radiotherapy protocols are typically adapted from adult cancers and do not fully address the unique biology of childhood tumors. This one-size-fits-all approach can result in over-treatment, which increases late toxicities such as cardiomyopathy, infertility, and secondary cancers, or under-treatment, which allows for a relapse in high-risk cases.15 In acute lymphoblastic leukemia, which represents the most common childhood malignancy, poor adherence to oral maintenance therapy with 6-mercaptopurine has been directly linked to relapse, even in well-resourced settings.34 In pediatric Hodgkin lymphoma, intensifying chemotherapy and radiotherapy reduces recurrence but exposes survivors to late effects, such as cardiovascular disease and secondary solid tumors, particularly breast and thyroid cancers.35 Similarly, in brain tumors, especially medulloblastoma, craniospinal irradiation improves survival but is associated with neurocognitive decline, growth hormone deficiency, and reduced quality of life for long-term survivors.36
Treatment adherence is also a major concern in low- and middle-income countries, where 20–30% of children discontinue therapy due to high costs, lack of transportation, or drug unavailability.37 Even when drugs are available, formulation barriers cause additional problems. Many medicines are not designed for children, large tablets are difficult to swallow, liquid preparations may be bitter, and some drugs require refrigeration that families cannot maintain. Medicines are often crushed or diluted before given to children, which can change their stability and reduce how well they work.38
These examples demonstrate that conventional pediatric cancer treatments do not adequately account for biological diversity, toxicity, or the realities of medication use in children. AI-guided 3D printing can create personalized, child-friendly medicines, such as flavored chewable tablets, mini-printlets, or combined pills that enhance the way children take their medication, ensure accurate doses, and reduce potential harmful side effects. By addressing these issues, 3D nano printing helps make pediatric cancer treatments safer and more effective worldwide.
As shown in Table 2, conventional approaches to pediatric oncology remain constrained by empirical dosing, adult-oriented formulations, and reactive toxicity management. These limitations often translate into under- or over-dosing, poor adherence, and preventable treatment-related complications.39 In contrast, AI-driven dosing and 3D-printed personalized nano formulations provide proactive, patient-specific solutions that directly address these gaps. By integrating pharmacogenomic, clinical, and environmental data, AI enables precision dosing that conventional trial-and-error methods cannot achieve.40 Similarly, 3D printing produces age-appropriate, palatable, and simplified dosage forms that overcome barriers of taste, pill burden, and complexity inherent to standard regimens.41,42 Importantly, predictive AI models shift toxicity management from a reactive to a preventive paradigm, reducing the risk of long-term non-communicable diseases such as cardiotoxicity and endocrine dysfunction.43 Together, these approaches not only enhance survival but also ensure healthier survivorship, an outcome that conventional strategies have struggled to secure.
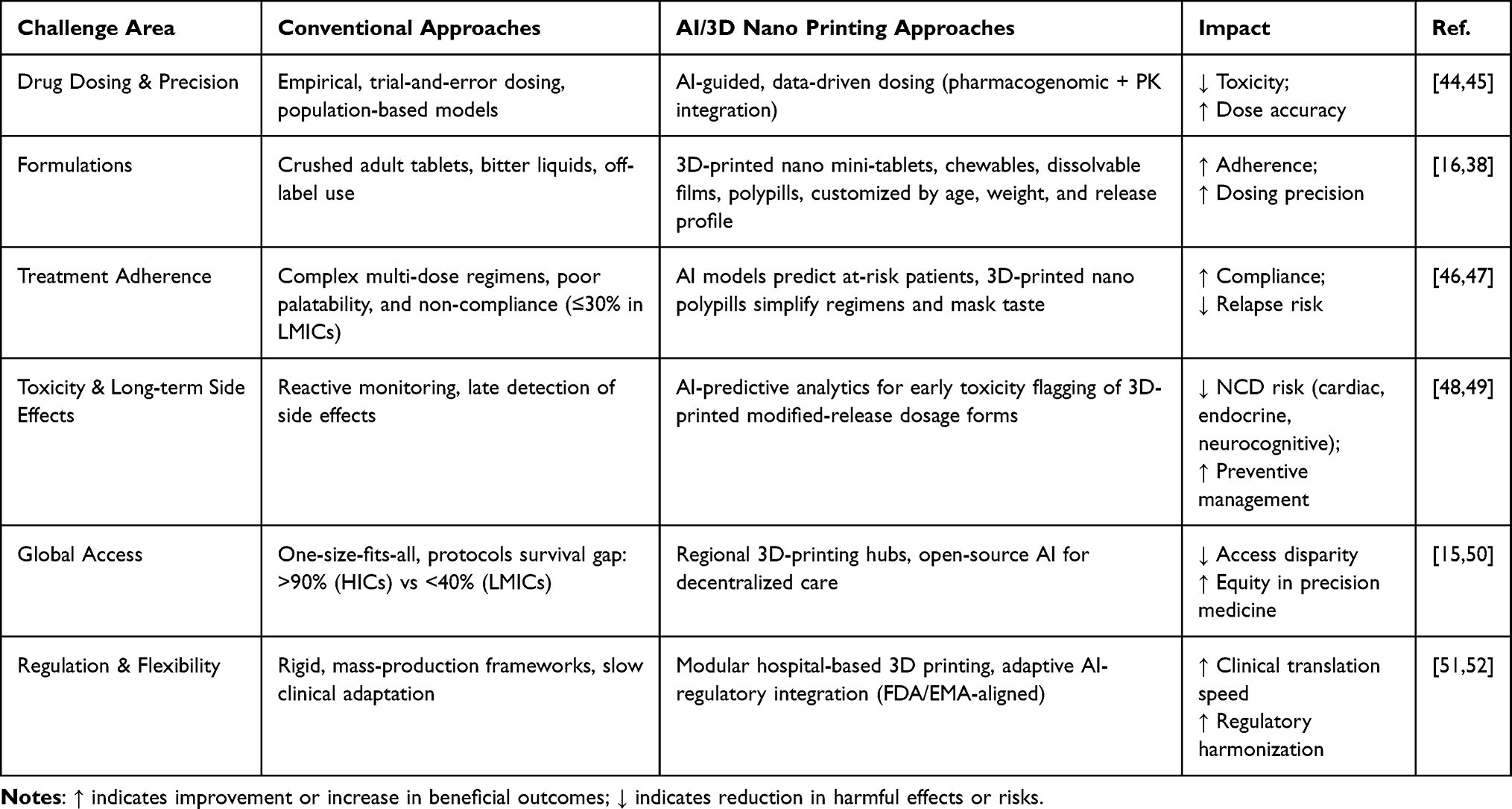 |
Table 2 Conventional Approaches vs AI/3D Nano Printing in Pediatric Oncology |
3D Nano Printed Drugs: Custom Formulations for Individual Needs
Conventional pediatric oncology still relies heavily on adult-sized tablets that must often be crushed or diluted, leading to dosing errors, instability, and reduced therapeutic accuracy. These formulations are frequently bitter and unpalatable, resulting in poor adherence and, in many cases, treatment discontinuation.53 In contrast, 3D nano printing enables the production of mini-tablets, flavored chewables, and dissolvable films that are tailored to a child’s age, weight, and swallowing ability. Such personalized dosage forms directly improve tolerability and compliance, addressing one of the major barriers of conventional therapy.54,55 By combining AI with 3D nano printing, pediatric oncology is entering a new era where medicines can be customized to a child’s genetic profile and lifestyle requirements, through innovations in fabrication techniques.56 AI models further optimize these designs by predicting the right dose, drug ratios, and release profiles based on genetic and clinical data, ensuring both precision and safety.57 In parallel, controlled-release and targeted delivery systems developed through 3D nano printing allow for spatial and temporal control of chemotherapy delivery, helping to minimize toxic peaks and improving therapeutic consistency.58 These advances directly support the long-term goal of reducing treatment-related non-communicable diseases, including cardiotoxicity, metabolic syndromes, and neurocognitive decline, by lowering drug toxicity while maintaining efficacy.49 Together, the integration of AI-guided drug design, nano fabrication techniques, and controlled-release drug platforms creates a connected framework for truly personalized pediatric cancer care that enhances survival while protecting quality of life, as represented in Figure 3.
 |
Figure 3 3D nano printing methods for personalized pharmaceutical products in pediatric cancer treatment. (A) Customized formulations are produced by 3D nano printing techniques based on individual patient requirements. (B) Personalized therapy products are facilitated through 3D printing, producing different dosage forms such as chewable tablets, mini-tablets, controlled-release devices, and polypills. (C) 3D printing technologies used to print these patient-specific dosage forms are depicted as: (i) Fused Deposition Modeling, (ii) Inkjet Printing, (iii) Extrusion Methods, (iv) Modular Printlets, and (v) Selective Laser Sintering. |
Techniques for Fabricating Patient-Specific Nano Drug Forms
Treating cancer in children presents unique challenges because their bodies are still growing, and they often respond differently to medicines compared to adults. Conventional drug formulations are rarely tailored to meet pediatric needs, making it challenging to deliver the correct dose, minimize side effects, and ensure that young patients adhere to their treatment plans. 3D nano printing technologies offer promising solutions by enabling healthcare providers to create medicines tailored to each child’s specific condition, body weight, genetic profile, and individual treatment requirements (Figure 3A and B). Several techniques, including Fused Deposition Modeling (FDM), Inkjet Printing, Selective Laser Sintering (SLS), Semi-Solid Extrusion (SSE), and Modular Printlets (Table 3 and Figure 3C), have been successfully applied in pediatric cancer care and NM, thereby improving safety, efficacy, and adherence as further described below.
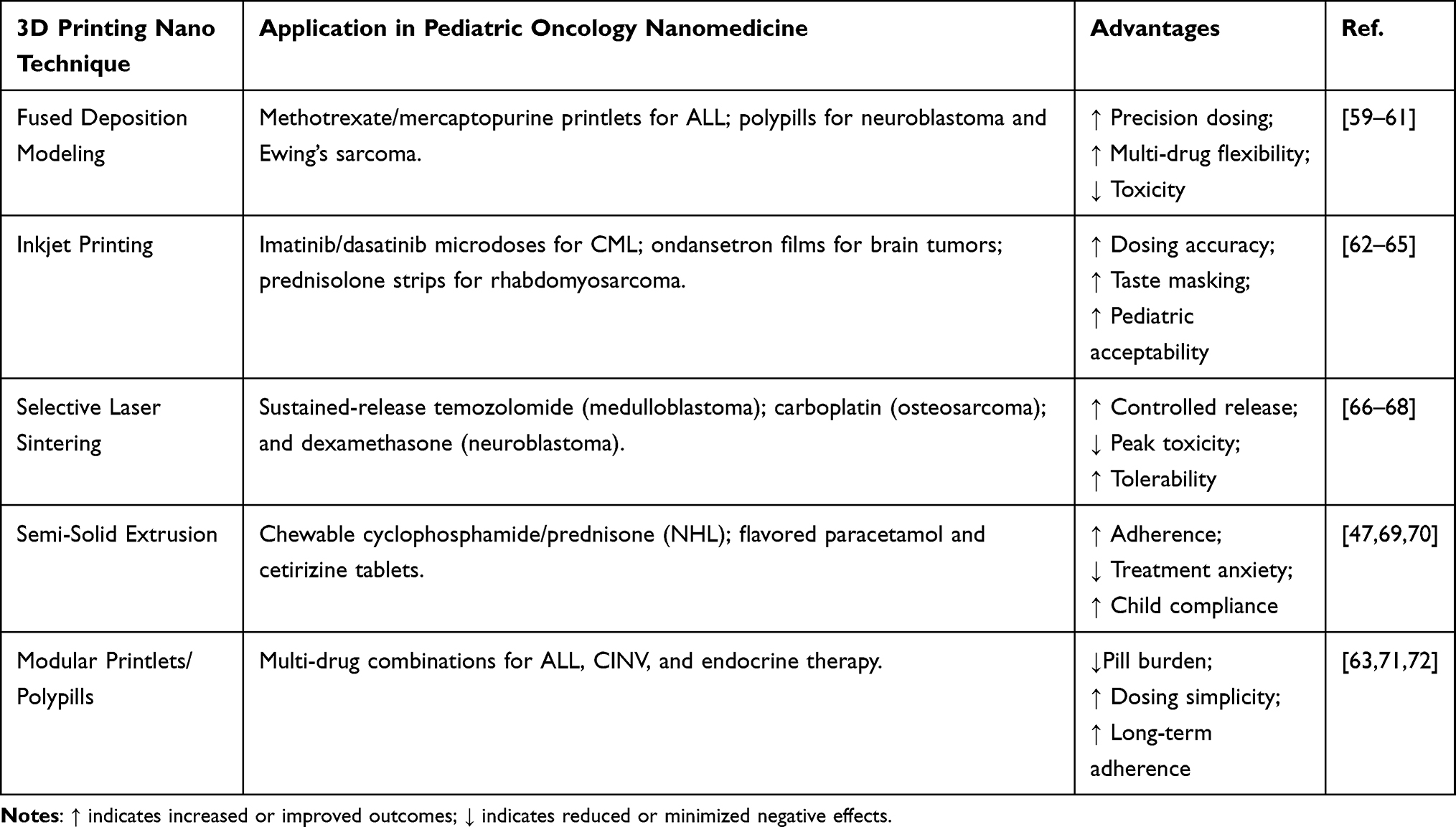 |
Table 3 3D Printing Techniques and Their Applications in Pediatric Oncology Nanomedicine |
Fused Deposition Modeling (FDM)
FDM is widely used to create tablets with precise shapes, doses, and drug-release profiles, making it particularly useful in pediatric oncology. In children with acute lymphoblastic leukemia, the most common childhood cancer, chemotherapy drugs like methotrexate and mercaptopurine must be given in exact doses. FDM allows tablets to be customized according to the child’s body surface area, reducing the risk of toxicity or treatment failure.59 Similarly, children with neuroblastoma often require complex multi-drug regimens including cyclophosphamide and doxorubicin. Using FDM, tablets can be printed to match each patient’s unique treatment schedule while avoiding harmful drug interactions.60 For example, in Ewing’s sarcoma, where vincristine, actinomycin D, and cyclophosphamide are used in combination, FDM helps design tablets with staggered release patterns, allowing for precise dosing that minimizes cumulative side effects.61 For children with medulloblastoma, a common brain tumor, temozolomide tablets printed by FDM offer sustained release, preventing sudden spikes in drug concentration that could worsen neurological symptoms.73 FDM has also been frequently used with 3D nanoparticles which aid in immune system avoidance, prolonged drug release at very small concentrations, and even controllable on-demand release necessary for children (Figure 3C(i)).
Inkjet Printing
Inkjet printing is another advanced technique that sprays tiny droplets (even nanometer dimensions) of a drug solution onto substrates, enabling highly accurate dosing and improved taste features essential for pediatric cancer treatment.74 Targeted therapies like dasatinib and imatinib, used in pediatric chronic myeloid leukemia, require precise dosing to avoid toxicity while ensuring therapeutic effectiveness. Inkjet printing ensures that each dose is personalized to the patient’s metabolism and health status.75 Children with gliomas and other brain tumors often suffer from chemotherapy-induced nausea; dissolvable ondansetron films printed with flavors help manage these symptoms, making treatment more tolerable.76 Similarly, prednisolone used in rhabdomyosarcoma can be printed in microdosages and nanodosages to reduce side effects while maintaining efficacy. Antibiotics like amoxicillin, required to treat infections in immunocompromised pediatric cancer patients, have been printed as flavored strips, improving compliance and reducing discomfort64,65 (Figure 3C(ii)).
Semi-Solid Extrusion (SSE)
SSE is especially suited for making soft, chewable formulations that are easier for children to take. Flavors and sweeteners can be added to mask the bitterness of chemotherapy drugs, enhancing adherence and reducing treatment-related anxiety. For example, cyclophosphamide and prednisone, used in non-Hodgkin lymphoma, have been printed as flavored chewable tablets, making long-term treatment regimens more acceptable to children.47 Similarly, paracetamol printed with flavors has helped manage pain and fever in children undergoing treatment for leukemia.69 Cetirizine, used to address allergies and side effects in brain tumor patients, has been printed into chewable tablets to encourage regular use. Iron supplements needed to treat anemia during cancer treatment have also been printed into palatable chewable forms for children with blood cancers, improving treatment adherence and nutritional support.70 Nanomaterials and nanoparticles have been used in conjunction with SSE to further improve efficacy (Figure 3C(iii)).
Modular Printlets and Polypills
Modular printlets and polypills combine multiple drugs into one tablet, reducing the complexity of treatment schedules and improving treatment adherence. Maintenance therapy often includes 6-mercaptopurine, methotrexate, and folinic acid; these drugs can be combined into a single polypill, ensuring that children receive all necessary medicines while reducing the chances of missed doses.71 Ondansetron and dexamethasone, used together to manage nausea and inflammation during chemotherapy for brain tumors, have been combined into single tablets to streamline treatment.63 Levothyroxine and calcium supplements, required for children who develop endocrine dysfunction after cancer treatment, have been printed into combination tablets that ensure consistent dosing over long periods.72 Similarly, vitamin D and zinc supplements, often recommended to support immune function during chemotherapy, have been combined into chewable polypills that encourage regular intake and improve overall treatment outcomes.77 Nanomaterials and nanoparticles have been used for modular printlets and polypills to control the nanometer spatial and temporal release of such drugs (Figure 3C(iv)).
Selective Laser Sintering (SLS)
SLS is particularly beneficial for creating tablets with controlled-release properties, allowing medications to act steadily over time, a crucial consideration in pediatric cancer care. For example, temozolomide tablets for children with medulloblastoma and gliomas have been printed using SLS to ensure that the drug is released slowly, helping reduce nausea and neurological side effects while maintaining therapeutic levels.66 Similarly, carboplatin tablets printed for osteosarcoma patients allow for sustained drug release, preventing the fatigue and nausea that often accompany chemotherapy.67 Children with neuroblastoma benefit from controlled-release dexamethasone tablets that manage inflammation during treatment, while reducing systemic side effects.68 SLS has also been used to print ibuprofen tablets for leukemia patients, providing extended pain relief during chemotherapy with fewer daily doses.78 In SLS, the laser power can be easily changed to maintain nanoparticle size and nanotexture to avoid immune system clearance and embed very small quantities of drugs needed for children (Figure 3C(v)).
Controlled-Release Nano Systems and Targeted Delivery
In pediatric cancer care, controlling the release and distribution of a drug in the body is crucial for achieving optimal therapeutic outcomes while minimizing adverse side effects. Children’s bodies are more sensitive to fluctuations in drug concentration, and their developing organs can be easily affected by aggressive treatments. Conventional dosing methods often result in drug peaks that cause toxicity or troughs that reduce effectiveness, which is especially dangerous in cancers like leukemia, brain tumors, and bone cancers.79 Controlled-release nano systems and targeted delivery platforms help overcome these challenges by ensuring that medicines are delivered at the correct dose, over the appropriate period, and to the specific site of the disease. These approaches are particularly beneficial in cancers such as acute lymphoblastic leukemia, brain tumors, neuroblastoma, and bone cancer, where nano precision in treatment can greatly affect outcomes and long-term health.
Controlled-release nano systems are designed to release a drug gradually over time rather than all at once. For example, in children with medulloblastoma, a common brain tumor, the chemotherapy agent temozolomide can be formulated into porous tablets with or without nanoparticles that steadily release the drug, maintaining therapeutic levels for longer time periods while reducing neurological side effects such as seizures and fatigue.80 Similarly, dexamethasone, used to reduce inflammation during cancer treatment, can be embedded in slow-release tablets with or without nanoparticles for children with neuroblastoma, helping control edema without causing sudden spikes in drug concentration that may lead to mood swings or metabolic disturbances.81 For children undergoing treatment for osteosarcoma, controlled-release formulations of carboplatin ensure that the drug is absorbed over time, lowering the risks of nausea and fatigue that are common with bolus chemotherapy administration.82
Targeted delivery systems further refine treatment by directing the drug specifically to cancer cells, a cancer cell receptor, cancer cell internal organelle, etc., thereby sparing healthy tissues. This is particularly important in pediatric cancers, where growing organs are vulnerable to damage from toxic chemotherapy. Lipid-based nanoparticles, polymeric carriers, and implantable matrices are among the technologies being used to achieve this precision.83 In acute lymphoblastic leukemia, for instance, targeted nano liposomal formulations of methotrexate and other drugs are being investigated to deliver the chemotherapy directly to bone marrow, improving the drug’s effectiveness while reducing systemic toxicity.84 Similarly, gliomas in the brain have been treated with drug-loaded nanoparticles that cross the blood-brain barrier and release medication locally, reducing nausea and cognitive side effects often associated with systemic administration.85 For neuroblastoma, implantable hydrogel matrices embedded with cyclophosphamide have shown promise in releasing drugs at the tumor site over extended time periods, minimizing the need for frequent injections and improving patient comfort.86 In addition to improved dosing and site-specific delivery, these systems enhance patient treatment adherence and quality of life. Children are spared from repeated invasive procedures, and families benefit from simpler treatment regimens. Targeted nano delivery also opens new possibilities for combining therapies, such as immunotherapy with chemotherapy, without increasing toxicity. Recent studies have demonstrated that polymeric nano carriers delivering combinations of vincristine and other agents to bone tumors achieve better tumor shrinkage with fewer side effects.87 As research continues and more nano formulations enter clinical practice, these systems are expected to play a pivotal role in personalizing care for children battling cancer, improving therapeutic outcomes while reducing the burden of treatment-related complications.
Advances in Chewable, Flavored, and Multi-Dose Nano Printlets for Improved Adherence
Ensuring medication adherence is a major challenge in pediatric cancer care, as children often face difficulties swallowing large pills, dealing with unpleasant tastes, and managing complex dosing schedules. Advances in 3D nano printing have led to the development of chewable, flavored, and multi-dose printlets that improve treatment experiences and outcomes (Figure 3). For instance, in non-Hodgkin lymphoma, bitter drugs (such as cyclophosphamide and prednisone) have been formulated into chewable tablets flavored with sweeteners and fruit extracts, making it easier for children to complete long chemotherapy regimens.88 Many of these flavors are added in nanoformulations during manufacturing leveraging the increasing surface area needed for enhanced taste at lower concentrations. Similarly, flavored methotrexate printlets have been used in acute lymphoblastic leukemia to enhance compliance during maintenance therapy.89 Flavored formulations have also been applied to supportive care drugs widely used in pediatric oncology. In children receiving chemotherapy for brain tumors, dissolvable ondansetron films with added flavors mask bitterness, helping reduce nausea-related treatment discontinuation and improving adherence.90 Paracetamol chewable tablets with fruity flavors have been successfully used to control pain and fever in children with leukemia.91 Multi-dose nano printlets, for children with neuroblastoma, release multiple agents at predetermined intervals, helping reduce pill burden and dosing errors.92 In maintenance therapy for acute lymphoblastic leukemia, polypills combining 6-mercaptopurine, methotrexate, and folinic acid have led to better compliance and fewer missed doses compared to traditional multi-tablet regimens.93
Clinical studies confirm the benefits of these formulations. A trial with leukemia patients found that flavored chewable tablets significantly improved adherence and reduced side effects,94 while a study in brain tumors showed that dissolvable films helped children tolerate treatment better, improving the quality of life.80 Using AI to customize printlets based on a child’s age, weight, and metabolism is making treatments safer and more effective, while helping families manage care at home.56 These improvements represent a significant step toward providing more accessible and personalized care for children with cancer.
AI-Driven Design: Enhancing Drug Development and Treatment Precision
Traditional chemotherapy dosing remains largely empirical, with adjustments often made only after toxicities have already occurred. This trial-and-error approach increases the risk of relapse from underdosing or late organ damage from overdosing, and is especially harmful in children, whose developing organs make them more vulnerable to dosing errors.95 In contrast, AI-driven pharmacogenomic platforms, such as MTXPK.org for methotrexate dosing, enable proactive and model-informed dose adjustments by integrating genetic, clinical, and pharmacokinetic data. This approach reduces toxic peaks, enhances treatment precision, and improves overall safety in pediatric oncology.96 AI-driven design is changing the way drugs are developed and used in pediatric cancer care by making treatments faster, safer, and more personal. With machine learning models for formulation optimization, AI can virtually test thousands of possibilities, predicting the optimal drug combinations, doses, and release patterns without the need for lengthy trial-and-error experiments93 (Table 4).
 |
Table 4 AI and ML Applications in Pediatric Oncology Nano Formulations |
These tools are especially useful for children, who often need flexible, age-appropriate medicines. Equally important, AI can integrate clinical, genetic, and environmental data to inform treatment decisions. For example, pharmacogenomic insights, such as TPMT or CYP3A5 variants that alter how chemotherapy is processed, can be combined with lifestyle or exposure factors to design safer and more effective dosing plans.102 This enables each therapy to be more precisely tailored to the child’s biology and living conditions. Finally, predictive analytics for treatment response and safety utilize data from biomarkers, imaging, and past treatments to forecast how a child will respond to a drug and whether side effects, such as heart damage or other long-term non-communicable diseases, may occur. Such models are already helping clinicians adjust treatment early to protect children from harm.103 Together, these AI-driven approaches create a powerful framework where every step from drug design to delivery is personalized, giving children with cancer a better chance of a cure and healthier lives after treatment.
Machine Learning Models for Nano Formulation Optimization
Machine learning (ML) can help scientists predict how various ingredients, tablet shapes, nanomaterial design, and release systems impact the efficacy of a medicine within the body. This saves time and reduces the need for trial-and-error experiments. For example, recent research has shown that ML models can predict the dissolution and release of a drug with more than 97% accuracy, which could be applied to important cancer drugs such as methotrexate or vincristine.48,97 Most children with cancer take several medicines at once, which can be hard to manage. ML can guide the design of 3D-printed multi-drug tablets, also called “oncology polypills”. These tablets can combine several drugs in one printlet, reducing pill burden and improving treatment compliance. Studies using Bayesian optimization have already shown success in designing safe and stable drug combinations, and these ideas can be extended to pediatric cancer care.98,99 Another challenge is taste. Many cancer drugs for children are very bitter, such as cyclophosphamide and mercaptopurine, which makes them difficult to take every day. ML models trained on taste data have been used to predict which nano ingredients or coatings can make medicines taste better. Applying these models to 3D-printed nano formulations can create flavored, chewable tablets that are more palatable for children, allowing them to adhere to long-term treatment plans.60,100 Finally, ML can also help predict side effects and toxicities before they happen. By combining formulation details with genetic information, such as TPMT variants for thiopurines or CYP3A5 for vincristine, ML can identify children who might have stronger reactions to standard doses (Table 4). This allows doctors to adjust treatment safely and reduce harmful effects.101 Compared to conventional materials, nanomaterials can more easily adjust properties (drug dissolution, drug release, taste, etc) important for pediatric cancer NM. Together, these tools point toward a future where ML and 3D nano printing work hand in hand to deliver safe, effective, and child-friendly cancer treatments.
Integrating Clinical, Genetic, and Environmental Data
Personalizing treatment for children with cancer requires more than just adjusting drug doses. Clinical data, such as age, weight, organ function, growth stage, and past treatment history, play a crucial role in determining how medicines interact with the body. For example, younger children often have immature liver or kidney function, which can change how they metabolize chemotherapy agents. ML models can combine these clinical features to design optimized nano formulations, ensuring that 3D-printed nano tablets release drugs at the right rate for each developmental stage. Recent studies in precision oncology have shown that integrating clinical records with AI models can improve the prediction of therapeutic outcomes and survival for pediatric cancers (Figure 4A, D and E).99
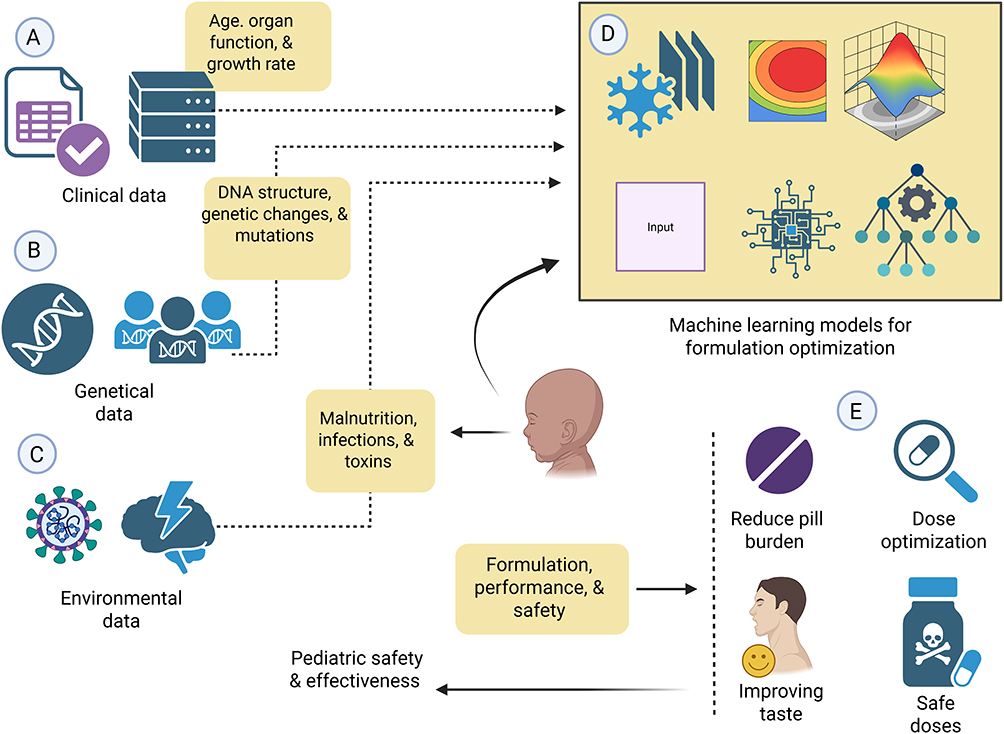 |
Figure 4 ML models and the efficiency in reproducing data to maximize drug nano formulation safety and efficacy in children. (A) Information regarding clinical patient factors such as age, organ function, and growth rate. (B) Genetical information related to DNA structure, genetic alterations, and mutations is provided. (C) Information regarding environmental factors such as malnutrition, infections, and toxins are addressed. (D) ML models for data collection and drug optimization to enhance drug safety and performance. Dotted arrows mark the input of patient-specific data into the ML system, while solid arrows represent the resulting formulation decisions grounded in predicted safety and performance. (E) The resulting improvements in pediatric effectiveness and safety aim at optimal outcomes such as decreased pill burden, optimizing doses, better taste, and securing doses. |
Genetic data are critical for personalizing pediatric cancer therapy, as many anticancer drugs are influenced by pharmacogenomics. Genetic variation is a powerful driver of differences in how children respond to cancer therapy, making pharmacogenomics crucial for personalized treatment. In acute lymphoblastic leukemia, TPMT and NUDT15 variants strongly influence thiopurine metabolism, whereas standard doses can cause severe myelosuppression in carriers unless adjusted.104 Similarly, CYP3A5 polymorphisms affect vincristine metabolism, with poor metabolizers experiencing higher rates of neurotoxicity due to slower clearance.105 Beyond ALL, other pharmacogenomic markers play a major role: DPYD variants predisposed to fluoropyrimidine toxicity,106 GSTM1 and GSTT1 deletions increased the risk of methotrexate-related hepatotoxicity,107 and UGT1A1*28 polymorphisms altered irinotecan clearance and toxicity in neuroblastoma and other pediatric solid tumors.108 Using genetic information in ML models helps predict which children may need smaller doses, slower-release medicines, or different drug combinations. When combined with 3D nano printing, this technology becomes capable of creating personalized tablets on demand, tailored to each child’s unique DNA profile. For example, children with TPMT or NUDT15 variants could receive thiopurine nano tablets designed to release very small, safe doses,109 while those with CYP3A5 variants could be given vincristine nano tablets that release the drug more slowly to lower the risk of neurotoxicity.110 By bringing together pharmacogenomics, ML, and 3D printing, doctors can provide treatments that are more precise, safer, and better suited to each child with cancer (Figure 4B, D and E).
Environmental and lifestyle factors often determine how children with cancer tolerate therapy. Malnutrition, common in low- and middle-income countries, reduces hepatic enzyme activity and protein binding, altering the pharmacokinetics of chemotherapy. For example, malnourished children with acute lymphoblastic leukemia have been shown to experience higher treatment-related toxicity and poorer survival.111 Infectious disease burden is another factor: chronic infections, such as malaria or helminths, can activate immune and metabolic pathways that interfere with drug metabolism, potentially leading to under- or overexposure to anticancer agents.112 Exposure to environmental toxins, such as arsenic-contaminated water, indoor air pollution, or pesticides, can also impact drug safety. For instance, arsenic exposure in children has been linked to impaired liver function, which may alter the metabolism of hepatically cleared chemotherapeutics.113 Similarly, nutritional supplements and herbal medicines, often used by families during cancer care, can interact with standard chemotherapy, for example St. John’s wort and green tea extracts, which affect cytochrome P450 enzymes and alter the clearance of vincristine and cyclophosphamide114,115 (Figure 4C).
Predictive Analytics for Treatment Response and Safety on Drug Delivery
Predictive analytics is becoming increasingly essential in pediatric oncology to anticipate how children will respond to treatment and minimize harmful side effects.116 In medulloblastoma, the most common malignant brain tumor in children, models that combine clinical data with molecular subtypes (WNT, SHH, Group 3, and Group 4) help predict survival and long-term neurocognitive outcomes, guiding more personalized therapy.117 In diffuse intrinsic pontine glioma (DIPG), which has very poor survival rates, predictive models using imaging and genomic data are being developed to identify children unlikely to respond to radiotherapy, enabling the earlier consideration of alternative strategies.118 In solid pediatric tumors, predictive tools also play an important role. In neuroblastoma, variants such as UGT1A1*28 are linked to severe toxicity from irinotecan-based regimens, while in Ewing sarcoma, ML applied to imaging and biomarkers can identify children with poor chemotherapy response, allowing timely treatment modification.108,119 In hepatoblastoma, predictive models that use gene expression can help identify which children are likely to respond well to cisplatin. This makes it possible to give the drug only to those who will benefit, while avoiding unnecessary side effects in resistant children.120 Predictive analytics is also improving long-term care for childhood cancers. In rhabdomyosarcoma, heart damage from anthracyclines can be predicted early using biomarkers and heart scans, allowing doctors to protect children at the highest risk.121 In children with neuroblastoma or hepatoblastoma treated with cisplatin, genetic variants such as SLC16A5 and ACYP2 have been linked to permanent hearing loss122 (Figure 5A). By connecting these predictive tools with 3D nano printing, doctors can adjust drug doses and release patterns in real-time, making treatments safer, more effective, and tailored to each child.123
 |
Figure 5 The figure justifies the comparison of the effects of traditional and 3D-printed nano drugs on paediatric oncology. (A) Conventional oncology has hazards of non-communicable disorders in children. (B) Advanced oncology that uses 3D-printed pharmaceuticals delivers better survival, less toxicity, and safer, more tailored treatment. Solid arrows illustrate the directional progression from treatment type to associated outcomes, including risks such as nephropathy, cardiomyopathy, hearing loss, and secondary cancers. (C) Examples of various non-communicable diseases caused by conventional methods of treatment. (D) Personalized pharmaceuticals use pharmacokinetic modelling to ensure quality control, target-specific drug release, and dose adjustments. The dotted dividing line separates harmful long-term effects from modern precision-based improvements. |
Improving Outcomes: Reducing Side Effects and Non-Communicable Diseases
Conventional oncology typically relies on the late detection of toxicities, such as anthracycline-induced cardiotoxicity or cisplatin-related hearing loss, which are often evident years after therapy and significantly compromise survivorship.124,125 This reactive model leaves limited scope for preventive intervention. In contrast, AI-driven predictive analytics enable early identification of children at high risk, allowing clinicians to adapt therapies before irreversible damage occurs. At the same time, 3D-printed modified-release formulations minimize harmful drug peaks, shifting toxicity management from a reactive to a preventive paradigm and improving both safety and long-term health outcomes.126 Improving outcomes in pediatric oncology requires not only curing cancer but also reducing side effects and long-term health risks. AI and 3D printing help in minimizing toxicity and treatment-related complications by enabling controlled-release formulations that prevent harmful drug peaks.127 At the same time, child-friendly formulations such as chewable or flavored nano printlets, supported by AI-driven monitoring, improve medication adherence and survivorship care.128 Precision dosing and predictive models also help in reducing secondary non-communicable diseases, such as cardiotoxicity from anthracyclines, hearing loss from cisplatin, and metabolic disorders after cranial irradiation.129,130 Importantly, these advances are supported by real-world evidence, as hospital-based trials demonstrate that AI-guided dosing platforms and on-demand 3D-printed drugs enhance both adherence and safety in children.51 The integration of these approaches provides children with both improved survival and protection against lifelong health complications, as illustrated in Figure 5B.
Minimizing Toxicity and Treatment-Related Complications
Children with cancer are highly sensitive to side effects, which can lead to lifelong health problems such as heart disease, lung damage, kidney failure, and metabolic disorders.131 AI-based predictive models can help identify which patients are at the highest risk before treatment begins. In acute lymphoblastic leukemia, ML has been utilized to predict relapse and toxicities more accurately, supporting safer treatment adjustments.132 Similar approaches are emerging in osteosarcoma, where AI tools analyzing imaging and clinical data can predict poor response to high-dose methotrexate and guide safer alternatives.48 When combined with 3D printing, these predictive insights can be transformed into safer and more personalized medicines. In acute lymphoblastic leukemia, children at risk of asparaginase hypersensitivity can be switched to safer Erwinia-derived formulations, which can be manufactured on demand.133 In Wilms tumor, nephrotoxicity from ifosfamide or carboplatin can be predicted using renal biomarkers, and AI can guide the design of modified-release 3D-printed nano tablets to reduce kidney injury.134 In Hodgkin lymphoma, pulmonary toxicity from bleomycin is a major concern, and predictive analytics using lung function tests may support safer dosing or even nano printing of drug combinations that omit bleomycin when risks are high.135 Preventing long-term complications is equally important for survivorship. Anthracyclines, used in leukemia and sarcomas, are highly effective but increase the risk of chronic heart failure; predictive models using cardiac imaging and biomarkers help identify children most at risk.136 In pediatric brain tumors, cranial irradiation can cause growth hormone deficiency and metabolic syndrome, but predictive analytics linked with personalized nano dosing may help reduce these risks.137 Similarly, in hepatoblastoma, gene-expression-based models can predict which children will benefit from cisplatin, avoiding unnecessary toxicity in resistant cases.138 By combining AI prediction with 3D-printed drug nano formulations, pediatric oncology can move towards safer, child-specific therapies that lower both acute toxicity and long-term non-communicable disease risks.
Strategies for Improving Medication Adherence and Enhancing Survivorship Care
Medication adherence is essential in childhood cancer, yet many children struggle to follow long and complex regimens. In acute lymphoblastic leukemia, children who miss even a small number of daily mercaptopurine doses face a nearly fourfold higher risk of relapse compared to those with good adherence.139 Challenges include the large number of medicines, unpleasant taste, swallowing difficulties, and social or family pressures, all of which can be solved through pediatric cancer NM. AI prediction models use clinical and prescription data to identify patients at risk of poor adherence, allowing for proactive treatment adjustments.140
Making medicines more suitable for children is also a proven way to improve adherence. Studies show that poor taste leads to refusal in nearly one-third of pediatric patients. In leukemia, a flavored liquid formulation of imatinib improved tolerability and facilitated regular use in children who were unable to swallow tablets.62 3D nano printing technologies take this further by enabling the creation of chewable, mini-tablet, or dissolvable film versions of essential medicines, tailored to a child’s age, size, and taste preferences. These child-friendly dosage forms directly reduce refusal and improve day-to-day treatment completion.141
Another key strategy is reducing the pill burden children face during therapy. Pediatric cancer nano treatment often requires a mix of chemotherapy, antibiotics, and supportive care, which can overwhelm families. 3D-printed nano polypills and modular nano printlets can combine several drugs into a single daily dose, simplifying regimens and making adherence more manageable.142 With AI integration, these nano polypills can be customized for each child, adjusting drug combinations and release timing to ensure safety and maximum benefit. This not only makes treatment easier but also reduces caregiver stress, improving the overall quality of care. Better adherence also leads to improved long-term outcomes and enhanced survivorship. Many childhood cancer survivors face long-term effects such as heart damage from anthracyclines or hormonal problems after cranial irradiation.143 Predictive models using biomarkers and imaging can identify children most at risk of cardiotoxicity or endocrine dysfunction, allowing doctors to adapt therapy earlier.144,145 By linking these insights with 3D-printed personalized drug nano formulations, such as extended-release or low-peak tablets, it becomes possible to reduce toxicity, prevent non-communicable diseases, and ensure that survivors enjoy a healthier quality of life.
Reducing Risk of Secondary Non-Communicable Diseases (Cardio, Metabolic, Neurocognitive, etc)
Children who survive cancer often face long-term health problems caused by the treatments that saved their lives. These are called secondary non-communicable diseases and include heart disease, diabetes, obesity, and learning or memory problems (Figure 5C). With survival rates now exceeding 80% in many pediatric cancers, preventing these late effects has become a major priority. AI and 3D nano printing, when combined, provide new tools to predict which children are most at risk and to design safer, personalized therapies that reduce long-term complications.4 Cardiotoxicity is one of the most serious late effects, especially from anthracyclines like doxorubicin, used in leukemia, sarcomas, and lymphomas.146 Even moderate cumulative doses can cause permanent heart damage and lead to heart failure years later. Large cohort studies confirm that childhood cancer survivors exposed to anthracyclines have a much higher risk of early cardiac disease.147 AI-driven prediction models that combine biomarkers and heart imaging can identify more vulnerable children. At the same time, 3D-printed extended-release nano formulations of cardiotoxic drugs could reduce sharp peaks in drug levels, lowering stress on the heart. Metabolic disorders such as obesity, insulin resistance, and growth hormone deficiency are also common in survivors. These often occur in children treated with cranial irradiation or corticosteroids, which damage the hypothalamic–pituitary axis. In survivors of medulloblastoma, nearly 50% develop an endocrine or metabolic complication within 10 years of therapy.148 AI can integrate radiation dose maps and endocrine biomarkers to predict which children are most at risk. With this information, 3D nano printing can produce tailored hormone replacement or optimized steroid formulations, reducing the severity of these long-term complications.
Late neurocognitive effects are another major challenge. Treatments such as cranial irradiation and high-dose methotrexate can cause long-term difficulties with memory, attention, and school performance. Research shows that more than 40% of survivors of childhood acute lymphoblastic leukemia experience measurable neurocognitive problems that affect daily life.149 AI models utilizing MRI scans and treatment history are being developed to predict which children are at risk of developing these impairments. In parallel, 3D-printed precision dosing of methotrexate and other neurotoxic drugs can help avoid overexposure, reducing the risk of cognitive decline.
By combining AI prediction tools with personalized 3D nano printing, pediatric cancer care can go beyond survival to focus on healthy survivorship. This approach makes it possible to tailor therapy in a way that reduces side effects, prevents secondary non-communicable diseases and ensures that children not only beat cancer but also live healthier lives after treatment (Figure 5D).
Real-World Evidence and Clinical Outcomes: Case Studies from Pediatric Trials and Hospital Implementations
Real-world studies in pediatric oncology demonstrate that AI-driven decision support and precision drug manufacturing are already being integrated into clinical use. A major advance has been the development of MTXPK.org, a web-based tool that utilizes population pharmacokinetic models constructed from over 31,000 methotrexate levels in 772 children with acute lymphoblastic leukemia. This tool forecasts drug clearance and supports personalized adjustments in leucovorin rescue and glucarpidase use, improving safety during high-dose methotrexate therapy.44 Updated versions have extended their applicability to broader pediatric populations, showing how model-informed precision dosing can be embedded into hospital workflows.150 Another important case study comes from busulfan dosing in pediatric hematopoietic stem cell transplantation. Busulfan is highly effective but carries a risk of life-threatening sinusoidal obstructive syndrome. In a study of 172 children, hospitals using Bayesian therapeutic drug monitoring (TDM) reduced the rate of SOS nearly in half, from 29% to 15%, while maintaining the same survival rates.45 This real-world evidence proves that AI-enabled or Bayesian-informed dosing is not only feasible but also improves hard clinical outcomes in pediatric cancer care.
Hospitals have also started using pharmacogenomic testing to guide therapy. At St. Jude, the PG4KDS program integrated genetic testing into the medical record, utilizing automated alerts. About 78% of children tested had at least one important genetic change, such as TPMT or SLCO1B1 variants, which helped doctors adjust drug doses and reduce side effects.151 This is one of the largest examples of real-world precision medicine in pediatric oncology. On the drug manufacturing side, 3D nano printing has been utilized in hospitals to produce child-friendly medications. One study reported the use of chewable sulfamethoxazole/trimethoprim tablets, printed at the hospital pharmacy, for children requiring infection prevention during chemotherapy. The tablets were easy for children to take and accurately dosed.152 This shows how point-of-care 3D nano printing can support personalized drug delivery in pediatric cancer. Finally, AI tools are improving cancer diagnosis. A DNA methylation-based ML classifier used in children’s hospitals changed the diagnosis in about 12% of brain tumor cases, leading to more accurate treatment decisions.153 This real-world application of AI in diagnostics demonstrates how new technologies can directly enhance care and outcomes for children with cancer. The connection between AI/3D nano printing and side effect reduction with survivorship is highlighted in Table 5.
 |
Table 5 Improving Outcomes: Linking AI/3D Nano Printing with Side Effect Reduction and Survivorship |
Ethical, Regulatory, and Safety Considerations in Pediatric Cancer Nanomedicine Applications
Conventional “one-size-fits-all” treatments worsen global inequalities in childhood cancer care. While survival rates are above 90% in high-income countries, they remain below 40% in many low- and middle-income countries.154 These gaps exist because current systems depend on centralized drug production and limited access to precision tools. In contrast, regional 3D-printing hubs and open-source AI platforms offer low-cost, scalable solutions. By making personalized medicine availability closer to patients, these approaches can help close survival gaps and improve access to advanced care worldwide.155 The use of AI and 3D nano printing in pediatric cancer care raises important ethical questions regarding data protection and informed consent. These technologies rely on sensitive information, such as genetic profiles and treatment records, which must be handled with the highest level of confidentiality and privacy (Figure 6A). Since children cannot legally consent, parents or guardians provide permission, while older children should also be asked for assent to respect their role in decision-making.156,157 Strong safeguards are necessary to ensure compliance with international data protection laws, such as the GDPR in Europe and HIPAA in the US. Experts also emphasize that AI systems must be explainable and transparent, as “black-box” algorithms could erode trust in pediatric cancer care.158 Regulation of AI-assisted, 3D-printed medicines is still evolving, and children face unique challenges. The US FDA has issued early guidance on 3D printing of drugs, while the European Medicines Agency (EMA) has also recognized its potential. However, there are still no clear pediatric-specific rules. Similarly, the FDA’s framework for Software as a Medical Device provides a pathway for AI decision tools, but very few have been tested in children. To move forward safely, regulatory agencies must design flexible systems that incorporate real-world evidence and genetic data, enabling the rapid adoption of new technologies while safeguarding children’s health52 (Figure 6B).
 |
Figure 6 This figure emphasizes: (A) The data protection framework for intensive privacy measures, parental consent, and approval by a legal guardian. (B) Regulatory framework for pediatric guidelines, defined rules of AI and 3D nano printing, along with the application of real-world evidence. (C) Equity and Access is centered on minimizing global inequalities and promoting open models of AI. (D) Globalization stresses the necessity of global cooperation and ensuring safe, global use of such sophisticated technologies. |
Equity and access are also major concerns. Today, a child with leukemia has a 90% chance of survival in high-income countries, but less than 40% in many low- and middle-income countries.46 If AI systems are primarily built on data from wealthy countries, they may not perform as well for children in other regions. Likewise, advanced 3D nano printing may remain limited to elite hospitals unless global initiatives expand access to this technology. To reduce disparities, international programs should focus on open AI models, regional 3D printing hubs, and training for local healthcare teams, ensuring every child has a chance to benefit from these innovations (Figure 6C). Finally, the future of these technologies depends on international collaboration and harmonization. Without shared standards, fragmented rules could hinder the clinical adoption of new technologies. Global groups, such as the International Council for Harmonization (ICH) and the WHO, can help create unified pediatric guidelines. A promising approach is the use of modular manufacturing, where certified hospital-based 3D printers operate under a central license, and producing safe personalized drugs on demand. The proposed Pharma3DPI initiative represents this vision, bringing together hospitals, regulators, and industry partners to test and approve AI-driven 3D-printed medicines across countries, ensuring safety, trust, and rapid adoption4,159 (Figure 6D). The ethical, regulatory, and access considerations for AI and 3D nano printing in pediatric oncology NM are outlined in Table 6 and illustrated in Figure 6.
 |
Table 6 Ethical, Regulatory, and Access Considerations for AI and 3D Printing in Pediatric Oncology Nanomedicine |
Case Studies
As mentioned, due to the prescribed anti-cancer medication, pediatric cancer patients often suffer from additional health problems often ignored. This section highlights the combined role that 3D printing of nanomaterials can play to reduce heart and skin problems in such patients, while treating the underlying cancer. This section also covers case studies with select cancers and specifically how the above-mentioned 3D printings of nanomaterials have aided such cancer treatment.
3D-Printed Hydrogels and Bioinks for Precision Drug Delivery and Regenerative Tissue Engineering
This case study demonstrates the potential of 3D printing and bioprinting technologies to be used in the real world for personalized drug delivery and regenerative medicine through the incorporation of rational material design and engineering, geometry-controlled drug delivery, cell–material interactions and functional testing in vivo (Figure 7). Drug release kinetics can be engineered solely through the digital design of the microarchitecture of the hydrogel tablets. In the study, tablets of hydrogels constructed to various geometries of solid, coaxial annulus and porous honeycomb architectures were constructed using stereolithography-based 3D fabrication.60 Porous tablets were shown to release a drug at faster and greater cumulative amounts when compared to the other geometries, a phenomenon attributable to higher surface-area-to-volume ratios which can be engineered to cause significant and higher release under simulated conditions of the human gastrointestinal system. Furthermore, bioprinting is effective in the fabrication of dual-layer hydrogel scaffolds incorporating cartilage and bone specific bioactive compounds that resulted in spatially controlled chondrogenesis and osteogenesis. This was demonstrated in an osteochondral defect model through the scaffolds improving macroanatomical repair, higher ICRS scores, additional mineral accretion, and favorable trabecular microarchitecture on micro-CT. The study highlights the importance of bioink composition in dECM-based systems for cardiovascular applications as they provided the bioactive compounds that promoted vascularization and improved myocardial repair through maturation of the regenerative vascular structures which reduced remodeling of the ventricle, lowered tissue fibrosis, and improved function of the heart post myocardial infarction.160
Figure 7 Continued. Figure 7 Case study demonstrating the integration of 3D printing and bioprinting for personalized drug delivery and regenerative medicine. (1) Stereolithography-based fabrication of hydrogel tablets with distinct geometries (solid, coaxial annulus, multi-pore, and honeycomb designs) and their corresponding cumulative drug-release profiles under simulated gastric (pH 1.2) and intestinal (pH 6.8) conditions, highlighting geometry-dependent modulation of release kinetics161 (Copyright 2020, Elsevier). (2) Bioprinted dual-layer hydrogel scaffold for osteochondral repair, showing macroscopic regeneration, improved ICRS scores, and enhanced bone microarchitecture, including increased bone volume fraction and mineral density, as confirmed by micro-computed tomography162 (scale bars = 2 mm; *p<0.05 and **p<0.01; ns = not statistically different; Copyright 2024, Elsevier). (3) Schematic representation of bioink design principles, illustrating the interdependence of printability, cell behavior, and mechanical properties, along with classification of bioinks into hydrogel-based, synthetic polymer-based, decellularized extracellular matrix (dECM)-based, composite, and cell-aggregate systems.163 (4) Functional evaluations of dECM-based bioinks in cardiac regeneration, demonstrating enhanced stem cell maturation, neovascularization, reduced ventricular remodeling, and improved cardiac function following myocardial infarction164 (A and B scale bar = 50 mm; E scale bar = 10 mm; F scale bar = 2 mm; *p<0.05; **p<0.005; Copyright 2017, Elsevier). (5) In vivo wound-healing assessment using 3D-bioprinted skin substitutes, showing accelerated wound closure and superior regenerative outcomes compared with full-thickness skin grafts, microskin grafts, and untreated controls165 (*p<0.05; **p<0.01; Copyright 2023, ACCSCEINCE, Creative Commons Attribution 4.0). (6) Histological and immunofluorescence analyses of regenerated skin tissues, confirming enhanced epithelialization, collagen deposition, angiogenesis, and expression of key regenerative biomarkers166 (Copyright 2024, Elsevier). (7) Evaluation of cell viability during bioprinting at varying cell densities using live/dead staining, demonstrating an optimal cell-loading range that balances uniform cell distribution with high post-printing survival. Collectively, these panels illustrate how digitally controlled 3D printing and bioactive material design enable precision drug delivery and tissue regeneration with strong translational relevance167 (Copyright 2022, Elsevier).
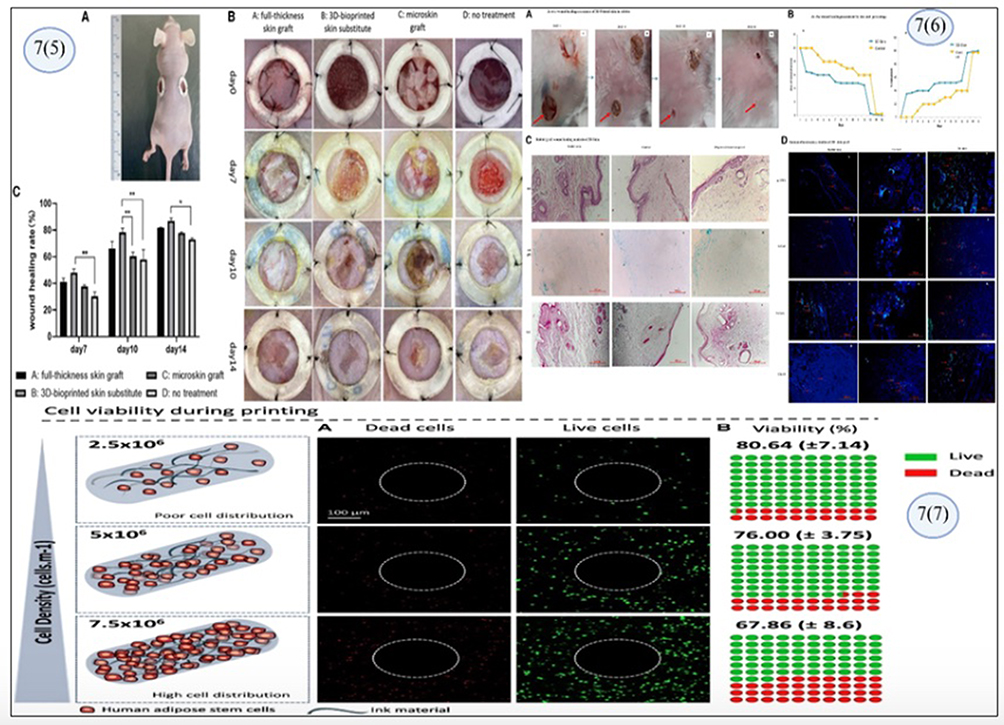
Regarding the healing of wounds, synthetic skin substitutes that incorporate human adipose-derived stem cells outperformed traditional skin grafts. They achieved quicker wound healing, greater epithelialization, more extensive neovascularization, and improved cellular and protein organization. Although positive outcomes were achieved, the study reproduced one major limitation of bioprinting: that cell density impacts viability. The intermediate densities of cells in the study achieved a balance of uniform cell distribution and survival. Overall, the example highlights the importance of 3D printing in controlling the rate of drug release and the subsequent biological effects. This example illustrates the growing intersection of biotechnology with performing on-demand patient therapy.168
Multifunctional 3D-Printed Nanocomposite Scaffolds for Synergistic Cancer Therapy and Tissue Regeneration
This case study demonstrates the purposeful design and multifunctional capabilities of cutting-edge 3D-printed nanocomposite scaffolds designed to simultaneously tackle the challenges of post-tumor resection cancer recurrence and tissue regeneration.169 The scaffolds are designed to integrate cross-printed macroporous scaffolds with bioactive photothermal, photodynamic, and chemodynamic therapeutic systems and maintain mechanical and regenerative functioning.170 The scaffolds also serve as theranostic platforms with the ability to controllably deform and release therapeutics due to the presence of engineered stimuli-responsive nanoparticles embedded within print-ready matrix systems.
At the architectural level, extrusion-based 3D printing allows the fabrication of highly ordered scaffolds with designed anisotropies. These scaffolds are exceptionally robust with designed pore sizes and are interconnected to sustain uniform flow and physiological nutrient diffusion to their interior. Critically, the printed scaffolds retain mechanical properties and interconnected porous architectures when immersed in simulated body fluid, which confirms the scaffolds would permit cell infiltration and mechanical interlocking for enhanced bioactivity in vivo. The scaffolds at this scale have incorporated copper-based protein-stabilized additional structures (CuS@BSA) that serve as multifunctional therapeutic agents. These nanoparticles thermally ablate (PTT) and produce localized heat. They also amplify the generation of reactive oxygen species (ROS) through photodynamic (PDT) and chemodynamic (CDT) processes. These rapid and multi-pronged responses to NIR (or near-infrared) ablate the tumor microenvironment through the generation of oxidative intracellular stress and subsequent mitochondrial destabilization along with the modulation of hypoxic cell death (Figure 8). The anticancer cell death that follows occurs with significantly reduced collateral damage to support healthy tissues.
 |
Figure 8 Case study demonstrating nanoparticle-integrated 3D-printed shape-memory scaffolds for multimodal cancer therapeutics. (1) Fabrication and therapeutic mechanism of nanoparticle-integrated 3D-printed scaffolds: illustration of the synthesis of CuS@BSA nanoparticles and their incorporation into alginate-based bioinks for extrusion-based 3D printing. The resulting scaffolds enable multimodal cancer therapy through synergistic photothermal (PTT), photodynamic (PDT), and chemodynamic (CDT) effects under near-infrared irradiation, leading to localized tumor cell destruction after implantation (*p<0.05).169 (2) Structural and microstructural characterization of printed scaffolds: Scanning electron microscopy images showing well-defined macroporous architectures, interconnected pore networks, and homogeneous nanoparticle distribution within the printed scaffolds. High-resolution micrographs confirm the preserved structural integrity across multiple length scales, supporting both mechanical stability and biological functionality170 (Copyright 2024, Elsevier). (3) Mechanical performance and stability of the nanocomposite scaffolds: Quantitative evaluation of compressive strength and modulus of 3D-printed scaffolds before and after immersion in simulated body fluid. The nanocomposite constructs exhibit enhanced mechanical properties compared with nanoparticle-free controls, demonstrating resistance to physiological degradation and suitability for load-bearing regenerative applications171 (scale bars = 100 nm; Copyright © 2024 American Chemical Society). (4) Shape-memory behavior and minimally invasive implantation: Demonstration of shape deformation, fixation, and rapid recovery of the 3D-printed scaffolds under thermal or NIR stimulation. The shape-memory effect enables temporary compression for implantation into irregular defects, followed by fast recovery to the original geometry, ensuring precise defect filling and stable in situ therapeutic performance172 (Copyright IOP Publishing). |
In addition to the ablation of the tumor, the scaffolds have displayed remarkable shape-memory self-adaptive behavior. Their remarkable macroscopic and microscopic (porous) shape adaptive behavior and bioactivity support the regeneration of the defective tissue and also permits self-contained modular distribution of the therapeutic nanoparticles as the scaffolds form intimate contact with surrounding tissues. When pre-stressed, the shape memory behavior permits rapid recovery to the original shape, allowing for controlled defect closure.172 This dual-functioning modular system demonstrates the ongoing advancements in the unilateral integration of 3D printing, nanotechnology, and responsive-stimuli materials, shifting the paradigm of tissue scaffolds. These systems, in their core functionality, also respond actively to the surgical and oncological challenges of tissue bio-regeneration.
Discussion
PCs differ widely in their biology, treatment responses, and long-term complications, and therefore, a single generalized approach is not appropriate for all children.173 The purpose of this review was to highlight how artificial intelligence and 3D nano printing may support safer, more personalized cancer therapy in children. The evidence suggests that these technologies have the greatest value when they are connected to the specific needs of individual malignancies rather than being applied broadly to pediatric cancer as a whole.174
In acute lymphoblastic leukemia (ALL), a long-term cure depends on the correct dosing of oral maintenance therapy and daily adherence. The pharmacogenomic variation in TPMT or NUDT15 can lead to excessive toxicity when standard doses are used. AI-supported dosing platforms, such as methotrexate prediction tools, help clinicians adjust doses before severe toxicity occurs.104 When these dosing decisions are combined with child-friendly 3D-printed formulations, such as flavored or mini-tablet mercaptopurine, the risk of relapse linked to poor adherence may be reduced.175
Neuroblastoma demonstrates a different clinical need. High-risk tumors may carry MYCN amplification and large chromosomal rearrangements, which are associated with aggressive behavior and chemoresistance.176 In such cases, conventional systemic delivery exposes young children to significant toxicity. Localized or controlled-release nano-delivery systems, supported by AI models that estimate toxicity risk, may allow chemotherapy to be given in smaller, sustained amounts directly to the tumor region, minimizing systemic exposure.177
For medulloblastoma, survival rates have improved, but radiotherapy and chemotherapy can cause long-term neurocognitive and endocrine deficits.178 AI-based molecular classifiers help distinguish tumor subgroups with different risks, which may allow for future treatment de-escalation for low-risk patients. At the same time, modified-release formulations of temozolomide or supportive medicines, produced through 3D printing, may help limit peak drug levels and reduce neurological side effects.117
In osteosarcoma and Ewing sarcoma, treatment involves intensive multi-drug chemotherapy. Children can accumulate serious cardiac, renal, or pulmonary injury from this approach.179 Machine-learning models that integrate imaging and laboratory markers can help identify patients who may not respond well to standard dosing, allowing for earlier treatment modifications. In parallel, 3D-printed polypills or controlled-release tablets may simplify complex drug schedules and reduce treatment burden for families.180
Late morbidity is also a major concern in Hodgkin lymphoma, where anthracycline-induced cardiomyopathy and bleomycin-related lung injury can appear years after treatment. Predictive models based on cardiac or pulmonary biomarkers may help clinicians modify dose intensity before irreversible injury develops. In the future, extended-release nano-formulations could lower peak exposure and support long-term cardiovascular health.181
Across these disease examples, a common theme emerges. Conventional pediatric oncology often identifies toxicity only after injury has already occurred, and many children struggle with medication adherence due to taste, swallowing difficulties, and/or pill burden. AI-supported dosing tools and 3D-printed pediatric formulations shift this paradigm toward prevention by anticipating toxicity, adjusting treatment earlier, and producing medicines that children are more willing to take.182 Early clinical evidence, for example, Bayesian dosing of methotrexate and busulfan, or hospital-based production of chewable formulations, suggests that these innovations are already workable in real clinical settings.65
However, important challenges remain. Regulatory pathways for 3D-printed pediatric medicines are still evolving, clinical studies involving children are limited, and global access to AI technologies is uneven. There is also a need for more diverse data from low- and middle-income countries, where survival rates remain low, and treatment abandonment is common.23 These factors must be addressed before precision pediatric NM can be used widely. Overall, the current evidence indicates that AI and 3D nano printing can improve dosing accuracy, reduce toxicity, increase adherence, and potentially prevent long-term non-communicable diseases in survivors. Their value is highest when matched to the biological and clinical features of specific childhood cancers.183 Continued collaboration between clinicians, pharmacists, engineers, and regulatory bodies will be essential to translate these early advances into routine pediatric cancer care. A key limitation is the heterogeneity and scarcity of pediatric-specific trials, which restricts direct comparison of outcomes and delay regulatory approval of 3D-printed formulations.
Future Directions: Integrating Technology for Better Long-Term Care
The future of pediatric oncology NM is being transformed by the combination of AI-driven precision tools and point-of-care (PoC) 3D printing, which together enable safer, more effective and child-specific therapies. Advances in modular manufacturing and hospital-based PoC systems now make it possible to produce personalized medicines, such as chewable, flavored, mini-tablets, or multi-drug polypills, directly at the bedside, with strict quality controls to ensure safety and dosing accuracy.51,56 At the same time, AI applications in pediatric oncology are expanding rapidly, from pharmacogenomic-guided dosing and therapeutic drug monitoring to risk prediction and the integration of imaging and genomics. Tools like the MTXPK platform, built from thousands of methotrexate dosing records, already support real-time decision-making in hospitals and highlight how AI can be embedded into routine pediatric cancer care.96 Together, these advances form a digital manufacturing ecosystem capable of delivering real-time personalized therapies that improve adherence, reduce toxicity, and strengthen treatment outcomes.
For these innovations to have a global impact, they must be delivered through strong collaboration and harmonized regulation. Today, the survival rate for childhood ALL exceeds 90% in high-income countries. Still, it remains below 40% in many low- and middle-income countries, underscoring the urgent need for shared AI platforms, regional 3D printing hubs, and specialized training.46 Global programs such as the WHO Global Initiative for Childhood Cancer (GICC) are working to close these survival gaps. At the same time, proposed collaborations like the Pharma3DPI consortium aim to establish international networks of hospitals, regulators, and industry to validate AI-driven, 3D-printed medicines under unified standards.4,184 Regulatory agencies are also adapting: the US FDA has issued guidance on 3D-printed drugs, and the Software as a Medical Device framework offers a pathway for AI-based tools. However, pediatric-specific rules are still limited.185 Looking toward 2030, a clear roadmap is emerging where AI-enabled dosing, modular manufacturing, and international cooperation converge to improve survival, reduce late complications, and secure healthier long-term outcomes for children with cancer worldwide.
Conclusion
PC care requires approaches that are safe, individualized, and designed for the unique biological and developmental needs of children. The literature reviewed in this manuscript shows that artificial intelligence and 3D nano printing have emerging potential to support such personalization. AI can guide clinicians in predicting drug clearance, adjusting doses based on genetic variation, and anticipating toxicity before clinical injury occurs. At the same time, 3D nano printing enables the creation of age-appropriate formulations, including mini-tablets, chewables, controlled-release printlets, and multi-drug combinations that may improve adherence and reduce treatment burden for families.
These combined strategies are especially relevant in settings where long-term survivors face risks of cardiotoxicity, neurocognitive decline, endocrine dysfunction, and other non-communicable diseases related to intensive chemotherapy and radiotherapy. Early clinical examples, such as model-informed methotrexate dosing, Bayesian-guided busulfan monitoring, and hospital-printed pediatric dosage forms, indicate that translation into practice is feasible.
Based on published pediatric dosing studies, Bayesian methotrexate and busulfan monitoring has demonstrated reductions in acute toxicities and safer exposure control, while survivorship cohorts show elevated risks of cardiomyopathy and metabolic dysfunction after anthracycline-based therapy, supporting efforts to lower long-term NCD burden. These interpretations arise from a narrative synthesis of clinical studies and hospital implementation reports rather than original interventional trials. In line with the concept of precision pediatric cancer NM, we recommend clinical adoption of validated AI-guided dose-adjustment tools, expansion of hospital-based 3D printing for pediatric-friendly medications, and prioritization of multicenter pediatric research. Key limitations include heterogeneous study designs, limited pediatric trials, and regulatory and access challenges, particularly in low-resource regions.
However, broader implementation will require regulatory clarity, equitable access to data and technology, and more pediatric-specific clinical studies. If these barriers are addressed, AI-enabled dosing and on-demand pediatric drug printing may help shift the focus of childhood cancer care from reactive toxicity management to proactive prevention, supporting not only survival but healthier long-term outcomes.
Abbreviations
AI, Artificial Intelligence; ALL, Acute Lymphoblastic Leukemia; AML, Acute Myeloid Leukemia; CINV, Chemotherapy-Induced Nausea and Vomiting; CML, Chronic Myeloid Leukemia; CYP3A5, Cytochrome P450 Family 3 Subfamily A Member 5; CYP450, Cytochrome P450 Enzyme Family; DPYD, Dihydropyrimidine Dehydrogenase; EMA, European Medicines Agency; FDA, Food and Drug Administration; FDM, Fused Deposition Modeling; GDPR, General Data Protection Regulation; GICC, Global Initiative for Childhood Cancer; GSTM1, Glutathione S-Transferase Mu 1; GSTT1, Glutathione S-Transferase Theta 1; HIPAA, Health Insurance Portability and Accountability Act; HICs, High-Income Countries; HPC, Hospital-Based Printing Centers; HSCT, Hematopoietic Stem Cell Transplantation; ICH, International Council for Harmonisation; LMICs, Low- and Middle-Income Countries; ML, Machine Learning; MTXPK.org, Methotrexate Pharmacokinetic Dosing Platform; NCD, Non-Communicable Disease; NCDs, Non-Communicable Diseases; NHL, Non-Hodgkin Lymphoma; NM, Nanomedicine; NUDT15, Nudix Hydrolase 15; PC, Pediatric Cancer; PK, Pharmacokinetics; PoC, Point-of-Care; PoC 3DP, Point-of-Care 3D Printing; Pharma3DPI, Pharmaceutical 3D Printing Initiative; SHH, Sonic Hedgehog Pathway; SLS, Selective Laser Sintering; SOS, Sinusoidal Obstructive Syndrome; SSE, Semi-Solid Extrusion; TDM, Therapeutic Drug Monitoring; TPMT, Thiopurine Methyltransferase; UGT1A1, Uridine Diphosphate Glucuronosyltransferase 1A1; WHO, World Health Organization; WNT, Wingless-related Integration Site.
Data Sharing Statement
All data will be provided in the manuscript file.
Consent for Publication
We hereby give consent for the publication of the entitled “Precision Pediatric Cancer Nanomedicine: Advancing Personalized Nano Therapies to Reduce Non-Communicable Diseases Through AI-Driven 3D-Printed Drugs”.
Acknowledgment
The authors gratefully acknowledges the support provided by the respective institutions involved in this work. Generative AI-assisted tools were not used in the preparation of the text, scientific interpretations, analyses, or conclusions. Figures were created using BioRender.com under a valid license.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
No funding agency is acknowledged.
Disclosure
The authors declare that they have no known competing financial interests or personal relationships.
References
1. Geel J, Howard SC. Barriers to achieving childhood cancer cure. In: Pediatric Surgical Oncology. Springer; 2025:63–32.
2. Zhang N, Wen D, Wang T, Deng J. Disparities in incidence and mortality of pediatric acute lymphoblastic leukemia across countries with different incomes. Leukemia. 2024;38(12):2731–2734. doi:10.1038/s41375-024-02433-1
3. Scott E. Investigating and Identifying Genetic Predictors for Cisplatin-Induced Hearing Loss and Anthracycline-Induced Cardiotoxicity. Vancouver: University Of British Columbia; 2023.
4. Bernatoniene J, Stabrauskiene J, Kazlauskaite JA, Bernatonyte U, Kopustinskiene DM. The future of medicine: how 3D printing is transforming pharmaceuticals. Pharmaceutics. 2025;17(3):390. doi:10.3390/pharmaceutics17030390
5. Huanbutta K, Burapapadh K, Sriamornsak P, Sangnim T. Practical application of 3D printing for pharmaceuticals in hospitals and pharmacies. Pharmaceutics. 2023;15(7):1877. doi:10.3390/pharmaceutics15071877
6. Wen H, He B, Wang H, et al. Structure-based gastro-retentive and controlled-release drug delivery with novel 3D printing. AAPS Pharm Sci Tech. 2019;20(2):68. doi:10.1208/s12249-018-1237-3
7. Dlamini Z, Francies FZ, Hull R, Marima R. Artificial intelligence (AI) and big data in cancer and precision oncology. Comput Struct Biotechnol J. 2020;18:2300–2311. doi:10.1016/j.csbj.2020.08.019
8. Singh D, Dhiman VK, Pandey M, et al. Personalized medicine: an alternative for cancer treatment. Cancer Treat Res Commun. 2024;42:100860. doi:10.1016/j.ctarc.2024.100860
9. Redekop WK, Mladsi D. The faces of personalized medicine: a framework for understanding its meaning and scope. Value in Health. 2013;16(6, Supplement):S4–S9. doi:10.1016/j.jval.2013.06.005
10. Sweet-Cordero EA, Biegel JA. The genomic landscape of pediatric cancers: implications for diagnosis and treatment. Science. 2019;363(6432):1170–1175. doi:10.1126/science.aaw3535
11. López-Carrasco A, Berbegall AP, Martín-Vañó S, et al. Intra-tumour genetic heterogeneity and prognosis in high-risk neuroblastoma. Cancers. 2021;13(20):5173. doi:10.3390/cancers13205173
12. Lustberg MB, Kuderer NM, Desai A, Bergerot C, Lyman GH. Mitigating long-term and delayed adverse events associated with cancer treatment: implications for survivorship. Nat Rev Clin Oncol. 2023;20(8):527–542.
13. Vadapalli S, Abdelhalim H, Zeeshan S, Ahmed Z. Artificial intelligence and machine learning approaches using gene expression and variant data for personalized medicine. Brief Bioinform. 2022;23(5):bbac191.
14. Hamdy NM, Basalious EB, El-Sisi MG, et al. Advancements in current one-size-fits-all therapies compared to future treatment innovations for better improved chemotherapeutic outcomes: a step-toward personalized medicine. Curr Med Res Opin. 2024;40(11):1943–1961. doi:10.1080/03007995.2024.2416985
15. Zahnreich S, Schmidberger H. Childhood cancer: occurrence, treatment and risk of second primary malignancies. Cancers. 2021;13(11):2607. doi:10.3390/cancers13112607
16. Chandramouli M, Basavanna V, Ningaiah S. A comprehensive review of paediatric drug development: an extensive analysis of present difficulties and prospects for the future. Biointerface Res Appl Chem. 2024;14:145.
17. Anaya J-M, Herrán M, Pino LE. Challenges and opportunities for precision medicine in developing nations. Expert Rev Precis Med Drug Dev. 2025;10(1):1–15. doi:10.1080/23808993.2025.2505796
18. Stiller C. Epidemiology of pediatric cancer. In: Pediatric Surgical Oncology. CRC Press; 2022:3–9.
19. Latoch E, Zubowska M, Młynarski W, et al. Late effects of childhood cancer treatment in long-term survivors diagnosed before the age of 3 years–A multicenter, nationwide study. Cancer Epidemiol. 2022;80:102209. doi:10.1016/j.canep.2022.102209
20. Pawłowski P, Ziętara KJ, Zaj N, Samardakiewicz-Kirol E, Samardakiewicz M. Adolescent survivors of childhood cancer: biopsychosocial challenges and the transition from survival to quality of life. Children. 2025;12(8):980. doi:10.3390/children12080980
21. Byrne J, Schmidtmann I, Rashid H, et al. Impact of era of diagnosis on cause‐specific late mortality among 77 423 five‐year European survivors of childhood and adolescent cancer: the PanCareSurFup consortium. Int J Cancer. 2022;150(3):406–419. doi:10.1002/ijc.33817
22. Crocco M, d’Annunzio G, La Valle A, et al. Endothelial dysfunction in childhood cancer survivors: a narrative review. Life. 2021;12(1):45. doi:10.3390/life12010045
23. Philip AK, Faiyazuddin M. Chapter 1 - An overview of artificial intelligence in drug development. In: Philip A, Shahiwala A, Rashid M, Faiyazuddin M, editors. A Handbook of Artificial Intelligence in Drug Delivery. Academic Press; 2023:1–8.
24. Suspitsin EN, Imyanitov EN. Hereditary conditions associated with elevated cancer risk in childhood. Biochemistry. 2023;88(7):880–891. doi:10.1134/S0006297923070039
25. Smith SC, Zhang L. Germline and Somatic changes associated with the development of inherited and De Novo Pediatric Acute Myeloid Leukemia. Genes. 2025;16(7):798.
26. Angione SD, Akalu AY, Gartrell J, et al. Fusion oncoproteins in childhood cancers: potential role in targeted therapy. J Pediatr Pharmacol Ther. 2021;26(6):541–555. doi:10.5863/1551-6776-26.6.541
27. Mroczek A, Zawitkowska J, Kowalczyk J, Lejman M. Comprehensive overview of gene rearrangements in childhood T-cell acute lymphoblastic leukaemia. Int J Mol Sci. 2021;22(2):808. doi:10.3390/ijms22020808
28. Reccia I, Pai M, Kumar J, Spalding D, Frilling A. Tumour heterogeneity and the consequent practical challenges in the management of gastroenteropancreatic neuroendocrine neoplasms. Cancers. 2023;15(6):1861. doi:10.3390/cancers15061861
29. Faiyazuddin M, Rahman SJQ, Anand G, et al. The impact of artificial intelligence on healthcare: a comprehensive review of advancements in diagnostics, treatment, and operational efficiency. Health Sci Rep. 2025;8(1):e70312. doi:10.1002/hsr2.70312
30. Andersson N, Ferro M, Jansson C, Chattopadhyay S, Karlsson J, Gisselsson D. Tracing metastatic spread in pediatric solid tumors using copy number and targeted deep sequencing. J Pathol. 2025;267:347–365. doi:10.1002/path.6472
31. Lei S, Jia S, Takalkar S, et al. Genomic profiling of circulating tumor DNA for childhood cancers. Leukemia. 2025;39(2):420–430. doi:10.1038/s41375-024-02461-x
32. Linga BG, Mohammed SG, Farrell T, Rifai HA, Al-Dewik N, Qoronfleh MW. Genomic newborn screening for pediatric cancer predisposition syndromes: a holistic approach. Cancers. 2024;16(11):2017. doi:10.3390/cancers16112017
33. Nafchi HM, Solatzadeh H, Hajimaghsoudi E, Babakhanzadeh E. Personalizing cancer therapy: the role of pharmacogenetics in overcoming drug resistance and toxicity. Mol Biol Rep. 2025;52(1):785. doi:10.1007/s11033-025-10887-4
34. Zeng XL, Heneghan MB, Badawy SM. Adherence to oral chemotherapy in acute lymphoblastic leukemia during maintenance therapy in children, adolescents, and young adults: a systematic review. Current Oncol. 2023;30(1):720–748. doi:10.3390/curroncol30010056
35. Ali N, Selim M, Salah Z, El Nabarawy NM, Hussein H, Sidhom I. Cardiovascular and thyroid late effects in pediatric patients with Hodgkin lymphoma treated with ABVD protocol. J Pediatr Hematol Oncol. 2023;45(4):e455–e463. doi:10.1097/MPH.0000000000002638
36. Major N, Patel NA, Bennett J, et al. The current state of radiotherapy for pediatric brain tumors: an overview of post-radiotherapy neurocognitive decline and outcomes. J Pers Med. 2022;12(7):1050. doi:10.3390/jpm12071050
37. Farrag A, Mohammed K, Ghazaly M, Berthold F. Noncompliance of pediatric cancer patients with chemotherapy: a single-center experience in a lower-middle income country. Pediatric Hematol Oncol. 2024;41(1):41–53. doi:10.1080/08880018.2023.2256780
38. Cohen J, Lee C, Markham R, Szerwo J, Roska M, Bubalo J. Medication use process and assessment of extemporaneous compounding and alternative routes of administration of oral oncology drugs: guidance for clinical and oncology pharmacists. J Am Coll Clin Pharm. 2022;5(11):1176–1228. doi:10.1002/jac5.1698
39. Hudson MM, Bhatia S, Casillas J, et al. Long-term follow-up care for childhood, adolescent, and young adult cancer survivors. Pediatrics. 2021;148(3):e2021053127. doi:10.1542/peds.2021-053127
40. Parvin N, Joo SW, Jung JH, Mandal TK. Multimodal AI in biomedicine: pioneering the future of biomaterials, diagnostics, and personalized healthcare. Nanomaterials. 2025;15(12):895. doi:10.3390/nano15120895
41. Page S, Da Costa SB, Stillhart C, Timpe C, Wagner L. The design of patient-centric dosage forms for older adults. In: Pharmaceutical Formulations for Older Patients. Springer; 2023:63–95.
42. Racaniello GF, Silvestri T, Pistone M, et al. Innovative pharmaceutical techniques for Paediatric dosage forms: a systematic review on 3D printing, prilling/vibration and microfluidic platform. J Pharmaceut Sci. 2024;113(7):1726–1748. doi:10.1016/j.xphs.2024.04.001
43. Al-Dekah AM, Sweileh W. Role of artificial intelligence in early identification and risk evaluation of non-communicable diseases: a bibliometric analysis of global research trends. BMJ open. 2025;15(5):e101169. doi:10.1136/bmjopen-2025-101169
44. Zhan M, Sun Y, Zhou F, et al. Population pharmacokinetics of methotrexate in paediatric patients with acute lymphoblastic leukaemia and malignant lymphoma. Xenobiotica. 2022;52(3):265–273. doi:10.1080/00498254.2022.2069060
45. Gurlek Gokcebay D, Arman Bilir O, Şahin S, Ok Bozkaya İ, Ozbek NY. Role of therapeutic drug monitoring of intravenous Busulfan for prevention of sinusoidal obstructive syndrome in children. Pediatr Transplant. 2022;26(5):e14266. doi:10.1111/petr.14266
46. Liu W, Fang J, Zhu M, Zhou J, Yuan C. Global, regional, and National burden of childhood leukemia from 1990 to 2021. BMC Pediatrics. 2025;25(1):571. doi:10.1186/s12887-025-05847-7
47. Rodríguez-Pombo L, Awad A, Basit AW, Alvarez-Lorenzo C, Goyanes A. Innovations in chewable formulations: the novelty and applications of 3D printing in drug product design. Pharmaceutics. 2022;14(8):1732. doi:10.3390/pharmaceutics14081732
48. Zhao J, Dai S, He J, Liu N, Zhang B, Li S. Prediction of high-dose methotrexate blood concentration in osteosarcoma patients using machine learning. Drug Des Devel Ther. 2025;Volume 19:3631–3643. doi:10.2147/DDDT.S515535
49. Clarós A, Ciudin A, Muria J, et al. A model based on artificial intelligence for the prediction, prevention and patient-centred approach for non-communicable diseases related to metabolic syndrome. Eur J Public Health. 2025:ckaf098.
50. Akpe V, Cock I. Decentralising cancer diagnostics: advances in point-of-care biosensor technologies and digital health integration. 2025.
51. Parramon-Teixido CJ, Rodríguez-Pombo L, Basit AW, et al. A framework for conducting clinical trials involving 3D printing of medicines at the point-of-care. Drug Delivery Transl Res. 2025:1–20.
52. Reis ME, Bettencourt A, Ribeiro HM. The regulatory challenges of innovative customized combination products. Front Med. 2022;9:821094. doi:10.3389/fmed.2022.821094
53. Litalien C, Bérubé S, Tuleu C, et al. From paediatric formulations development to access: advances made and remaining challenges. Br J Clin Pharmacol. 2022;88(10):4349–4383. doi:10.1111/bcp.15293
54. Bracken L, Habashy R, McDonough E, et al. Creating acceptable tablets 3D (CAT 3D): a feasibility study to evaluate the acceptability of 3D printed tablets in children and young people. Pharmaceutics. 2022;14(3):516. doi:10.3390/pharmaceutics14030516
55. Lafeber I, Ruijgrok EJ, Guchelaar H-J, Schimmel KJ. 3D printing of pediatric medication: the end of bad tasting oral liquids?—a scoping review. Pharmaceutics. 2022;14(2):416. doi:10.3390/pharmaceutics14020416
56. Carou-Senra P, Rodríguez-Pombo L, Monteagudo-Vilavedra E, et al. 3D printing of dietary products for the management of inborn errors of intermediary metabolism in pediatric populations. Nutrients. 2023;16(1):61. doi:10.3390/nu16010061
57. Kumar D, Tanwar R, Bahmani K, Kumar S, Pal R, Vinchurkar K. Case studies and success stories in FDM 3D printing for pharmaceuticals. In: Innovations in Drug Manufacturing: FDM 3D Printing for Pharmaceuticals. Springer; 2025:253–269.
58. Mazumdar H, Khondakar KR, Das S, Halder A, Kaushik A. Artificial intelligence for personalized nanomedicine; from material selection to patient outcomes. Expert Opin Drug Deliv. 2025;22(1):85–108. doi:10.1080/17425247.2024.2440618
59. Alzahrani A, Narala S, Youssef AAA, et al. Fabrication of a shell-core fixed-dose combination tablet using fused deposition modeling 3D printing. Eur J Pharm Biopharm. 2022;177:211–223. doi:10.1016/j.ejpb.2022.07.003
60. Kapoor DU, Pareek A, Uniyal P, Prajapati BG, Thanawuth K, Sriamornsak P. Innovative applications of 3D printing in personalized medicine and complex drug delivery systems. iScience. 2025;28:113505. doi:10.1016/j.isci.2025.113505
61. Castillo Écija H. Development and application of xenograft models to predict the prognosis and study the treatment-driven evolution of pediatric sarcomas. 2022.
62. Nikolova Z, Peng B, Hubert M, et al. Bioequivalence, safety, and tolerability of imatinib tablets compared with capsules. Cancer Chemother Pharmacol. 2004;53(5):433–438. doi:10.1007/s00280-003-0756-z
63. Bergese SD, Puente EG, Antor MA, et al. A prospective, randomized, double-blinded, double-dummy pilot study to assess the preemptive effect of triple therapy with aprepitant, dexamethasone, and promethazine versus ondansetron, dexamethasone and promethazine on reducing the incidence of postoperative nausea and vomiting experienced by patients undergoing craniotomy under general anesthesia. Front Med. 2016;3:29. doi:10.3389/fmed.2016.00029
64. Tejo-Otero A, Lustig-Gainza P, Fenollosa-Artés F, Valls A, Krauel L, Buj-Corral I. 3D printed soft surgical planning prototype for a biliary tract rhabdomyosarcoma. J Mech Behav Biomed Mater. 2020;109:103844. doi:10.1016/j.jmbbm.2020.103844
65. Rampedi PN, Ogunrombi MO, Adeleke OA. Leading paediatric infectious diseases—current trends, gaps, and future prospects in oral pharmacotherapeutic interventions. Pharmaceutics. 2024;16(6):712. doi:10.3390/pharmaceutics16060712
66. Katamesh AA, Subaiea GM, Mostafa M, et al. Revolutionizing cancer care: the role of 3D printing in personalized oncology. ACS omega. 2025;10:39350–39370. doi:10.1021/acsomega.5c01642
67. Tabriz AG, Kuofie H, Scoble J, Boulton S, Douroumis D. Selective Laser Sintering for printing pharmaceutical dosage forms. J Drug Delivery Sci Technol. 2023;86:104699. doi:10.1016/j.jddst.2023.104699
68. Majrashi M, Kotowska A, Scurr D, Hicks JM, Ghaemmaghami A, Yang J. Sustained release of dexamethasone from 3D-printed scaffolds modulates macrophage activation and enhances osteogenic differentiation. ACS Appl Mater Interfaces. 2023;15(49):56623–56638.
69. Santos MLD. 3D printing of personalized medicines for paediatric use. 2019.
70. Kaushik P, Mittal V, Kaushik D. Unleashing the potential of β–cyclodextrin inclusion complexes in bitter taste abatement: development, optimization and evaluation of taste masked anti-emetic chewing gum of promethazine hydrochloride. AAPS Pharm Sci Tech. 2024;25(6):169. doi:10.1208/s12249-024-02888-6
71. Schrøder H, Clausen N, Øtergård E, Pressler T. Folic acid supplements in vitamin tablets: a determinant of hematological drug tolerance in maintenance therapy of childhood acute lymphoblastic leukemia. Pediatric Hematol Oncol. 1986;3(3):241–247. doi:10.3109/08880018609031223
72. Tao D. The effectiveness of combined treatment with vitamin D and sodium levothyroxine in children with hypothyroidism. Int J Clin Exp Med Res. 2025;9(3):310–313. doi:10.26855/ijcemr.2025.05.010
73. Orcheston-Findlay L, Bax S, Utama R, Engel M, Govender D, O’Neill G. Advanced spheroid, tumouroid and 3D bioprinted in-vitro models of adult and paediatric glioblastoma. Int J Mol Sci. 2021;22(6):2962. doi:10.3390/ijms22062962
74. Carou‐Senra P, Rodríguez‐Pombo L, Awad A, Basit AW, Alvarez‐Lorenzo C, Goyanes A. Inkjet printing of pharmaceuticals. Adv Mater. 2024;36(11):2309164. doi:10.1002/adma.202309164
75. Bernsen EC, Hogenes VJ, Nuijen B, Hanff LM, Huitema ADR, Diekstra MHM. Practical recommendations for the manipulation of kinase inhibitor formulations to age-appropriate dosage forms. Pharmaceutics. 2022;14(12):2834. doi:10.3390/pharmaceutics14122834
76. Wargantiwar S, Bhattacharya S. Biocompatible natural polymers and cutting-edge fabrication techniques in the development of next-generation oral thin films for enhanced drug delivery systems. Curr Pharm Des. 2024.
77. Schmitt AK, Puppa M-A, Wessels I, Rink L. Vitamin D3 and zinc synergistically induce regulatory T cells and suppress interferon-γ production in mixed lymphocyte culture. J Nutr Biochem. 2022;102:108942. doi:10.1016/j.jnutbio.2022.108942
78. Zhelezniakov M. Assessment of selective laser sintering (SLS) 3D printing as a manufacturing technique for pediatric dosage forms. 2022.
79. Basak D, Arrighi S, Darwiche Y, Deb S. Comparison of anticancer drug toxicities: paradigm shift in adverse effect profile. Life. 2021;12(1):48. doi:10.3390/life12010048
80. Rahman R, Janowski M, Killick-Cole CL, et al. Childhood brain tumors: a review of strategies to translate CNS drug delivery to clinical trials. Cancers. 2023;15(3):857. doi:10.3390/cancers15030857
81. Pourmadadi M, Maleki M, Rahdar A, Aboudzadeh MA. Innovative polymeric and non-polymeric nanocarrier systems for dexamethasone: enhancing precision and reducing side effects. J Nanopart Res. 2025;27(6):167. doi:10.1007/s11051-025-06363-6
82. Bakhrushina EO, Mikhel IB, Buraya LM, et al. Implantation of in situ gelling systems for the delivery of chemotherapeutic agents. Gels. 2024;10(1):44. doi:10.3390/gels10010044
83. Mishra R, Pal R, Khan Z, Sahoo S, Chawra HS, Kumar D. Solid Lipid Nanoparticles (SLNPs): a state-of-the-art formulation strategy and their applications against Tuberculosis (TB) and analgesic effects. Nanosci Nanotechnol Asia. 2025;15(3):E22106812379362. doi:10.2174/0122106812379362250602075954
84. Yohan A, Jacques C, Fletcher T, Suk-In T, Campbell RB. An overview of conventional drugs and nanotherapeutic options for the treatment and management of pediatric acute lymphoblastic leukemia. Anticancer Agents Med Chem. 2022;22(18):3050–3061. doi:10.2174/1871520622666220426105922
85. Gharbavi M, Parvanian S, Leilan MP, Tavangar S, Parchianlou M, Sharafi A. Niosomes-based drug delivery in targeting the brain tumors via nasal delivery. Nasal Drug Deliv. 2023:279–324.
86. Pandey A, Malviya R, Sharma PK, Rahate K. Biomaterial based stem cells therapy for cancer. Curr Stem Cell Res Ther. 2023;18(8):1041–1055. doi:10.2174/1574888X18666230110154333
87. Deng Q, Yue S, You F, et al. Vincristine/Volasertib polymersome injection enables high-efficiency synergistic treatment of acute lymphoblastic leukemia. Acta Biomater. 2025;200:641–652. doi:10.1016/j.actbio.2025.05.041
88. Witchmichen C, Schmidt P. Pediatric oncologic pharmacy.
89. Conroy S, Newman C, Gudka S. Unlicensed and off label drug use in acute lymphoblastic leukaemia and other malignancies in children. Ann Oncol. 2003;14(1):42–47. doi:10.1093/annonc/mdg031
90. Dahmash EZ, Patel AN, Faizi E, et al. Fabrication and characterisation of taste-masked orally dissolving films containing ondansetron hydrochloride using Novel Poly (Amide-Thioester) nanocapsules based on L-cysteine amino-acid. J Pharm Innovation. 2025;20(1):28. doi:10.1007/s12247-024-09902-1
91. Ranmal SR, Walsh J, Tuleu C. Poor-tasting pediatric medicines: part 1. A scoping review of their impact on patient acceptability, medication adherence, and treatment outcomes. Front Drug Deliv. 2025;5:1553286. doi:10.3389/fddev.2025.1553286
92. Tambe S, Jain D, Meruva SK, et al. Recent advances in amorphous solid dispersions: preformulation, formulation strategies, technological advancements and characterization. Pharmaceutics. 2022;14(10):2203. doi:10.3390/pharmaceutics14102203
93. Hooijberg J, De Vries N, Kaspers G, Pieters R, Jansen G, Peters G. Multidrug resistance proteins and folate supplementation: therapeutic implications for antifolates and other classes of drugs in cancer treatment. Cancer Chemother Pharmacol. 2006;58(1):1–12. doi:10.1007/s00280-005-0141-1
94. Tang N, Kovacevic A, Zupanec S, et al. Perceptions of parents of pediatric patients with acute lymphoblastic leukemia on oral chemotherapy administration: a qualitative analysis. Pediatr Blood Cancer. 2022;69(1):e29329. doi:10.1002/pbc.29329
95. Menz BD, Stocker SL, Verougstraete N, et al. Barriers and opportunities for the clinical implementation of therapeutic drug monitoring in oncology. Br J Clin Pharmacol. 2021;87(2):227–236. doi:10.1111/bcp.14372
96. Taylor ZL, Miller TP, Poweleit EA, et al. Clinical covariates that improve the description of high dose methotrexate pharmacokinetics in a diverse population to inform MTXPK. org. Clin Transl Sci. 2023;16(11):2130–2143. doi:10.1111/cts.13600
97. Gharehnazifam Z, Dolatabadi R, Baniassadi M, et al. Computational analysis of vincristine loaded silk fibroin hydrogel for sustained drug delivery applications: multiphysics modeling and experiments. Int J Pharm. 2021;609:121184. doi:10.1016/j.ijpharm.2021.121184
98. Tallorin L, Wang J, Kim WE, et al. Discovering de novo peptide substrates for enzymes using machine learning. Nat Commun. 2018;9(1):5253. doi:10.1038/s41467-018-07717-6
99. Elbadawi M, McCoubrey LE, Gavins FK, et al. Disrupting 3D printing of medicines with machine learning. Trends Pharmacol Sci. 2021;42(9):745–757. doi:10.1016/j.tips.2021.06.002
100. Tabriz AG, Fullbrook DHG, Vilain L, et al. Personalised tasted masked chewable 3D printed fruit-chews for paediatric patients. Pharmaceutics. 2021;13(8):1301. doi:10.3390/pharmaceutics13081301
101. Toksvang LN, Brigitha LJ, van der Sluis IM, et al. Therapeutic drug monitoring in acute lymphoblastic leukemia–a deep dive into pharmacokinetics,-dynamics, and-genetics of antileukemic drugs. Expert Rev Clin Pharmacol. 2025;18(3):131–149. doi:10.1080/17512433.2025.2465426
102. Srivastav AK, Mishra MK, Lillard JW, Singh R. Transforming pharmacogenomics and CRISPR gene editing with the power of artificial intelligence for precision medicine. Pharmaceutics. 2025;17(5):555. doi:10.3390/pharmaceutics17050555
103. Marques L, Costa B, Pereira M, et al. Advancing precision medicine: a review of innovative in silico approaches for drug development, clinical pharmacology and personalized healthcare. Pharmaceutics. 2024;16(3):332. doi:10.3390/pharmaceutics16030332
104. Lubis IS, Anggadiredja K, Artarini AA, Sari NM, Suryawan N, Zazuli Z. NUDT15 pharmacogenetics in acute lymphoblastic leukemia: synthesizing progress for personalized thiopurine therapy. Med Sci. 2025;13(3):112. doi:10.3390/medsci13030112
105. Pozzi E, Fumagalli G, Chiorazzi A, Canta A, Cavaletti G. Genetic factors influencing the development of vincristine-induced neurotoxicity. Expert Opin Drug Metab Toxicol. 2021;17(2):215–226. doi:10.1080/17425255.2021.1855141
106. De Mattia E, Polesel J, Silvestri M, et al. The burden of rare variants in DPYS gene is a novel predictor of the risk of developing severe fluoropyrimidine-related toxicity. Human Genomics. 2023;17(1):99. doi:10.1186/s40246-023-00546-9
107. Lopez-Lopez E, Gutierrez-Camino A, Bilbao-Aldaiturriaga N, Pombar-Gomez M, Martin-Guerrero I, Garcia-Orad A. Pharmacogenetics of childhood acute lymphoblastic leukemia. Pharmacogenomics. 2014;15(10):1383–1398. doi:10.2217/pgs.14.106
108. Zhu X, Zhu J, Sun F, et al. Influence of UGT1A1* 6/* 28 polymorphisms on irinotecan-related toxicity and survival in pediatric patients with relapsed/refractory solid tumors treated with the VIT regimen. Pharmacogenomics Pers Med. 2021;Volume 14:369–377. doi:10.2147/PGPM.S292556
109. Franca R, Braidotti S, Stocco G, Decorti G. Understanding thiopurine methyltransferase polymorphisms for the targeted treatment of hematologic malignancies. Expert Opin Drug Metab Toxicol. 2021;17(10):1187–1198. doi:10.1080/17425255.2021.1974398
110. Wu C-Y, Li G-T, Chu -C-C, et al. Proactive therapeutic drug monitoring of vincristine in pediatric and adult cancer patients: current supporting evidence and future efforts. Arch Toxicol. 2023;97(2):377–392. doi:10.1007/s00204-022-03418-8
111. Rujkijyanont P, Inaba H. Diagnostic and treatment strategies for pediatric acute lymphoblastic leukemia in low-and middle-income countries. Leukemia. 2024;38(8):1649–1662. doi:10.1038/s41375-024-02277-9
112. Chen J-Y, Zhou J-K, Pan W. Immunometabolism: towards a better understanding the mechanism of parasitic infection and immunity. Front Immunol. 2021;12:661241. doi:10.3389/fimmu.2021.661241
113. Islam K, Haque A, Karim R, et al. Dose-response relationship between arsenic exposure and the serum enzymes for liver function tests in the individuals exposed to arsenic: a cross sectional study in Bangladesh. Environ Health. 2011;10(1):64. doi:10.1186/1476-069X-10-64
114. Chan W-J-J, Adiwidjaja J, McLachlan AJ, Boddy AV, Harnett JE. Interactions between natural products and cancer treatments: underlying mechanisms and clinical importance. Cancer Chemother Pharmacol. 2023;91(2):103–119. doi:10.1007/s00280-023-04504-z
115. Pochet S, Lechon A-S, Lescrainier C, et al. Herb-anticancer drug interactions in real life based on VigiBase, the WHO global database. Sci Rep. 2022;12(1):14178. doi:10.1038/s41598-022-17704-z
116. Kumar D, Rajni RS, Rani S, Kumari R. Formulation and evaluation of emulgel of an antifungal drug for topical drug delivery. J Pharm Negat Results. 2023:4087–4100.
117. Kim DT, Uloho-Okundaye M, Frederico SC, Guru S, Kim MJ, Chang SD. Advancing medulloblastoma therapy in pediatrics: integrative molecular classification and emerging treatments. Brain Sci. 2025;15(8):896. doi:10.3390/brainsci15080896
118. Yu X, Li S, Mai W, et al. Pediatric diffuse intrinsic pontine glioma radiotherapy response prediction: MRI morphology and T2 intensity-based quantitative analyses. Eur Radiol. 2024;34(12):7962–7972. doi:10.1007/s00330-024-10855-9
119. Zhou C, Li H, Zeng H, Wang P. Incidence trends, overall survival, and metastasis prediction using multiple machine learning and deep learning techniques in pediatric and adolescent population with osteosarcoma and Ewing’s sarcoma: nomogram and webpage. Clin Transl Oncol. 2025;27(5):2327–2338. doi:10.1007/s12094-024-03717-9
120. Somers KM, Tabbouche RB, Bondoc A, et al. Retreatment with cisplatin may provide a survival advantage for children with relapsed/refractory hepatoblastoma: an institutional experience. Cancers. 2023;15(15):3921. doi:10.3390/cancers15153921
121. Curren V, Dham N, Spurney C. Diagnosis, prevention, treatment and surveillance of anthracycline-induced cardiovascular toxicity in pediatric cancer survivors. Hearts. 2021;2(1):45–60. doi:10.3390/hearts2010005
122. Iațentiuc A, Iațentiuc IM, Frăsinariu OE, et al. The role of genetic and non-genetic factors in the occurrence of cisplatin-associated ototoxicity. Int J Mol Sci. 2025;26(10):4787. doi:10.3390/ijms26104787
123. Gholap AD, Uddin MJ, Faiyazuddin M, Omri A, Gowri S, Khalid M. Advances in artificial intelligence for drug delivery and development: a comprehensive review. Comput Biol Med. 2024;178:108702. doi:10.1016/j.compbiomed.2024.108702
124. Kallenberger EM, Briggs EE, Nguyen SA, et al. Preventing hearing loss in children receiving cisplatin: a systematic review and meta‐analysis. Laryngoscope. 2025;135:2662–2669. doi:10.1002/lary.32158
125. Wu M, Yang Y, Cao M, et al. Drug-induced cardiotoxicity in children during the past 30 years: a bibliometric study and visualization analysis. Med Sci Monit. 2023;29:e938673–1. doi:10.12659/MSM.938673
126. Poudel I, Mita N, Babu RJ. 3D printed dosage forms, where are we headed? Expert Opin Drug Deliv. 2024;21(11):1595–1614. doi:10.1080/17425247.2024.2379943
127. Bhuskute H, Shende P, Prabhakar B. 3D printed personalized medicine for cancer: applications for betterment of diagnosis, prognosis and treatment. AAPS Pharm Sci Tech. 2021;23(1):8. doi:10.1208/s12249-021-02153-0
128. Kukade A, Kawade S, Lokare S, Kharage A. Artificial intelligence in medication adherence and personalized treatment plans. Int J Sci Res Technol. 2025.
129. Chang W-T, Liu C-F, Feng Y-H, et al. An artificial intelligence approach for predicting cardiotoxicity in breast cancer patients receiving anthracycline. Arch Toxicol. 2022;96(10):2731–2737. doi:10.1007/s00204-022-03341-y
130. Deutsch BC, Collopy C, Kallogjeri D, Piccirillo JF. Validation of hearing loss prediction tool for cisplatin chemotherapy and radiation in head and neck cancer treatment. JAMA Otolaryngol Head Neck Surg. 2021;147(2):182–189. doi:10.1001/jamaoto.2020.4620
131. Uddin MJ, Gholap AD, Khan T, et al. The Integration of Nanotechnology, Artificial Intelligence (AI), Machine Learning (ML) and 3D-Bioprinting Approaches for Personalized COVID-19 Treatment. J Biomed Nanotechnol. 2024;20(12):1759–1790. doi:10.1166/jbn.2024.3933
132. Mehrbakhsh Z, Hassanzadeh R, Behnampour N, et al. Machine learning-based evaluation of prognostic factors for mortality and relapse in patients with acute lymphoblastic leukemia: a comparative simulation study. BMC Med Inf Decis Making. 2024;24(1):261. doi:10.1186/s12911-024-02645-6
133. Anderson S. Pharmacogenomic and Machine Learning Insights for the Prediction of l-Asparaginase-Induced Hypersensitivity in Pediatric Cancer. University of British Columbia; 2025.
134. Daw NC, Gregornik D, Rodman J, et al. Renal function after ifosfamide, carboplatin and etoposide (ICE) chemotherapy, nephrectomy and radiotherapy in children with Wilms tumour. Eur J Cancer. 2009;45(1):99–106. doi:10.1016/j.ejca.2008.09.017
135. Jennane S, Ababou M, El Haddad M, et al. Bleomycin-induced lung toxicity in Hodgkin’s lymphoma: risk factors in the positron emission tomography era. Cureus. 2022;14(4):e23993. doi:10.7759/cureus.23993
136. Stolojanu C, Steflea R, Micsescu-Olah AM, Alexandra I, Popoiu A, Doros G. Combined utility of speckle tracking echocardiography and cardiac biomarkers for early detection of anthracycline-induced cardiotoxicity in pediatric oncology patients. Biomedicines. 2024;12(12):2849. doi:10.3390/biomedicines12122849
137. Harary PM, Rajaram S, Chen MS, Hori YS, Park DJ, Chang SD. Genomic predictors of radiation response: recent progress towards personalized radiotherapy for brain metastases. Cell Death Discov. 2024;10(1):501. doi:10.1038/s41420-024-02270-2
138. Hirsch TZ, Pilet J, Morcrette G, et al. Integrated genomic analysis identifies driver genes and cisplatin-resistant progenitor phenotype in pediatric liver cancer. Cancer Discov. 2021;11(10):2524–2543. doi:10.1158/2159-8290.CD-20-1809
139. Sharma SK. Drugs used post stem cell transplant. In: Basics of Hematopoietic Stem Cell Transplant. Springer; 2023:661–685.
140. Babel A, Taneja R, Mondello Malvestiti F, Monaco A, Donde S. Artificial intelligence solutions to increase medication adherence in patients with non-communicable diseases. Front Digit Health. 2021;3:669869. doi:10.3389/fdgth.2021.669869
141. Peng X, Liu Z, Luo C, et al. PSMD12 promotes hepatocellular carcinoma progression by stabilizing CDK1. Front Immunol. 2025;16:1581398. doi:10.3389/fimmu.2025.1581398
142. Karavasili C, Babaee S, Kutty S, et al. Modular titratable polypills for personalized medicine and simplification of complex medication regimens. Adv Healthc Mater. 2023;12(27):e2301101. doi:10.1002/adhm.202301101
143. Ning Q, Yang T, Guo X, et al. CHB patients with rtA181T‐mutated HBV infection are associated with higher risk hepatocellular carcinoma due to increases in mutation rates of tumour suppressor genes. J Viral Hepat. 2023;30(12):951–958. doi:10.1111/jvh.13886
144. Novikova A, Poltavskaya M, Pavlova M, et al. Cardiac dysfunction and exercise tolerance in patients after complex treatment for cranial and craniospinal tumors in childhood. J Clin Med. 2024;13(11):3045. doi:10.3390/jcm13113045
145. Perry TR, Roberts ML, Sunkara B, et al. Modeling precision cardio-oncology: using human-induced pluripotent stem cells for risk stratification and prevention. Curr Oncol Rep. 2021;23(7):77. doi:10.1007/s11912-021-01066-2
146. Wang Y, Wang Q, Yang TW, et al. Analysis of immune and inflammatory microenvironment characteristics of noncancer end-stage liver disease. J Interferon Cytokine Res. 2023;43(2):86–97. doi:10.1089/jir.2022.0172
147. Lipshultz ER, Chow EJ, Doody DR, et al. Cardiometabolic risk in childhood cancer survivors: a report from the Children’s Oncology Group. Cancer Epidemiol Biomarkers Prev. 2022;31(3):536–542. doi:10.1158/1055-9965.EPI-21-0360
148. Claude F, Ubertini G, Szinnai G. Endocrine disorders in children with brain tumors: at diagnosis, after surgery, radiotherapy and chemotherapy. Children. 2022;9(11):1617. doi:10.3390/children9111617
149. Nigro S, Hall L, Harman J, et al. The association of environmental factors with neurocognitive outcomes in survivors of childhood acute lymphoblastic leukemia (ALL). Support Care Cancer. 2024;32(1):1. doi:10.1007/s00520-023-08212-5
150. Tu Q, Cotta M, Raman S, Graham N, Schlapbach L, Roberts JA. Individualized precision dosing approaches to optimize antimicrobial therapy in pediatric populations. Expert Rev Clin Pharmacol. 2021;14(11):1383–1399. doi:10.1080/17512433.2021.1961578
151. Carr DF, Turner RM, Pirmohamed M. Pharmacogenomics of anticancer drugs: personalising the choice and dose to manage drug response. Br J Clin Pharmacol. 2021;87(2):237–255. doi:10.1111/bcp.14407
152. Stoops M, Do B, Ramos S, et al. Clinical implementation of a paediatric 3D-printed combination of Sulfamethoxazole and Trimethoprim. Int J Pharm. 2025;676:125581. doi:10.1016/j.ijpharm.2025.125581
153. Benfatto S, Sill M, Jones DT, et al. Explainable artificial intelligence of DNA methylation-based brain tumor diagnostics. Nat Commun. 2025;16(1):1787. doi:10.1038/s41467-025-57078-0
154. Horgan D, Mia R, Erhabor T, et al. Fighting cancer around the world: a framework for action. Healthcare. 2022:2125.
155. Alotaibi BS, Shema AI, Ibrahim AU, et al. Assimilation of 3D printing, Artificial Intelligence (AI) and Internet of Things (IoT) for the construction of eco-friendly intelligent homes: an explorative review. Heliyon. 2024;10(17). doi:10.1016/j.heliyon.2024.e23999
156. Wen S, Theobald S, Gangas P, et al. A practical guide to apply AI in childhood cancer: data collection and AI model implementation. EJC Paediatr Oncol. 2024;4:100197. doi:10.1016/j.ejcped.2024.100197
157. Kováč P, Jackuliak P, Bražinová A, et al. Artificial intelligence-driven facial image analysis for the early detection of rare diseases: legal, ethical, forensic, and cybersecurity considerations. AI. 2024;5(3):990–1010. doi:10.3390/ai5030049
158. Mohammed S, Malhotra N. Ethical and regulatory challenges in machine learning-based healthcare systems: a review of implementation barriers and future directions. BenchCouncil Trans Benchmarks Stand Eval. 2025;5:100215. doi:10.1016/j.tbench.2025.100215
159. Yang S, Hu X, Zhu J, et al. Aspects and implementation of pharmaceutical quality by design from conceptual frameworks to industrial applications. Pharmaceutics. 2025;17(5):623. doi:10.3390/pharmaceutics17050623
160. Jang J, Park HJ, Kim SW, et al. 3D printed complex tissue construct using stem cell-laden decellularized extracellular matrix bioinks for cardiac repair. Biomaterials. 2017;112:264–274. doi:10.1016/j.biomaterials.2016.10.026
161. Karakurt I, Aydoğdu A, Çıkrıkcı S, Orozco J, Lin L. Stereolithography (SLA) 3D printing of ascorbic acid loaded hydrogels: a controlled release study. Int J Pharm. 2020;584:119428. doi:10.1016/j.ijpharm.2020.119428
162. Wu Z, Sun H, Hu X, et al. Muti-interactions based 3D-printed osteochondral biomimetic scaffold for BMP-2 sustained release. European Polymer Journal. 2024;218:113343. doi:10.1016/j.eurpolymj.2024.113343
163. Gungor-Ozkerim PS, Inci I, Zhang YS, Khademhosseini A, Dokmeci MR. Bioinks for 3D bioprinting: an overview. Biomater Sci. 2018;6(5):915–946. doi:10.1039/C7BM00765E
164. Jang J, Park H-J, Kim S-W, et al. 3D printed complex tissue construct using stem cell-laden decellularized extracellular matrix bioinks for cardiac repair. Biomaterials. 2017;112:264–274. doi:10.1016/j.biomaterials.2016.10.026
165. Fu H, Zhang D, Zeng J, et al. Application of 3D-printed tissue-engineered skin substitute using innovative biomaterial loaded with human adipose-derived stem cells in wound healing. Int J Bioprinting. 2023;9(2):674. doi:10.18063/ijb.v9i2.674
166. Damle MN, Chaudhari L, Tardalkar K, et al. A biologically functional bioink based on extracellular matrix derived collagen for 3D printing of skin. Int J Biol Macromol. 2024;258:128851. doi:10.1016/j.ijbiomac.2023.128851
167. Diogo GS, Marques CF, Freitas-Ribeiro S, et al. Mineralized collagen as a bioactive ink to support encapsulation of human adipose stem cells: a step towards the future of bone regeneration. Biomater Adv. 2022;133:112600. doi:10.1016/j.msec.2021.112600
168. Yang Y, Qiao X, Huang R, et al. E-jet 3D printed drug delivery implants to inhibit growth and metastasis of orthotopic breast cancer. Biomaterials. 2020;230:119618. doi:10.1016/j.biomaterials.2019.119618
169. Zhang J, Zhao S, Zhu M, et al. 3D-printed magnetic Fe(3)O(4)/MBG/PCL composite scaffolds with multifunctionality of bone regeneration, local anticancer drug delivery and hyperthermia. J Mater Chem B. 2014;2(43):7583–7595. doi:10.1039/c4tb01063a
170. Liu C, Wang Z, Wei X, Chen B, Luo Y. 3D printed hydrogel/PCL core/shell fiber scaffolds with NIR-triggered drug release for cancer therapy and wound healing. Acta Biomater. 2021;131:314–325. doi:10.1016/j.actbio.2021.07.011
171. Colak B, Cihan MC, Ertas YN. 3D-printed, implantable alginate/cus nanoparticle scaffolds for local tumor treatment via synergistic photothermal, photodynamic, and chemodynamic therapy. ACS Appl Nano Mater. 2023;6(17):16076–16085. doi:10.1021/acsanm.3c03433
172. Zhuang H, Lin R, Liu Y, et al. Three-dimensional-printed bioceramic scaffolds with osteogenic activity for simultaneous photo/magnetothermal therapy of bone tumors. ACS Biomater Sci Eng. 2019;5(12):6725–6734. doi:10.1021/acsbiomaterials.9b01095
173. Hassan M, Shahzadi S, Kloczkowski A. Harnessing artificial intelligence in pediatric oncology diagnosis and treatment: a review. Cancers. 2025;17(11):1828. doi:10.3390/cancers17111828
174. Dalboni da Rocha JL, Lai J, Pandey P, et al. Artificial intelligence for neuroimaging in pediatric cancer. Cancers. 2025;17(4):622. doi:10.3390/cancers17040622
175. Maillard M, Nishii R, Yang W, et al. Additive effects of TPMT and NUDT15 on thiopurine toxicity in children with acute lymphoblastic leukemia across multiethnic populations. J Natl Cancer Inst. 2024;116(5):702–710. doi:10.1093/jnci/djae004
176. Bartolucci D, Montemurro L, Raieli S, et al. MYCN impact on high-risk neuroblastoma: from diagnosis and prognosis to targeted treatment. Cancers. 2022;14(18):4421. doi:10.3390/cancers14184421
177. AlKhazal A, Chohan S, Ross DJ, Kim J, Brown EG. Emerging clinical and research approaches in targeted therapies for high-risk neuroblastoma. Front Oncol. 2025;15. doi:10.3389/fonc.2025.1553511
178. Govender D, de Monaco BA, Dhall G, Thompson EM. Chapter Five - Medulloblastoma chapter - past perspectives and future directions. In: Abdelbaki MS, Fisher PB, Limbrick DD, editors. Advances in Cancer Research. Academic Press; 2025:141–184.
179. Zhra M, Akhund SA, Mohammad KS. Advancements in osteosarcoma therapy: overcoming chemotherapy resistance and exploring novel pharmacological strategies. Pharmaceuticals. 2025;18(4):520. doi:10.3390/ph18040520
180. Morya VK, Magar AG, Park S-H, Noh K-C. Systemic strategies for osteosarcoma: advances and future directions. Discov Oncol. 2025;16(1):1367. doi:10.1007/s12672-025-02208-9
181. Nygård L, Vogelius IR, Kofoed KF, Bentzen S, Specht L. Late cardiac toxicity after anthracyclines and radiotherapy for lymphoma-a regression analysis of dose-response. Hematol Oncol. 2025;43(5):e70134. doi:10.1002/hon.70134
182. Thornton CP, Daniali M, Wang L, Makeneni S, Barz Leahy A. Using natural language processing to identify symptomatic adverse events in pediatric oncology: tutorial for clinician researchers. JMIR Bioinform Biotechnol. 2025;6:e70751. doi:10.2196/70751
183. Milliken RL, Quinten T, Andersen SK, Lamprou DA. Application of 3D printing in early phase development of pharmaceutical solid dosage forms. Int J Pharm. 2024;653:123902. doi:10.1016/j.ijpharm.2024.123902
184. Kumar Gupta D, Ali MH, Ali A, et al. 3D printing technology in healthcare: applications, regulatory understanding, IP repository and clinical trial status. J Drug Target. 2022;30(2):131–150. doi:10.1080/1061186X.2021.1935973
185. Tettey-Engmann F, Parupelli SK, Bauer SR, Bhattarai N, Desai S. Advances in artificial intelligence-based medical devices for healthcare applications. Biomed Mater Devices. 2025:1–21.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Artificial Intelligence in the Management of Asthma: A Review of a New Frontier in Patient Care
Tan LD, Nguyen N, Lopez E, Peverini D, Shedd M, Alismail A, Nguyen HB
Journal of Asthma and Allergy 2025, 18:1179-1191
Published Date: 16 August 2025
Nanomedicine for Acute Kidney Injury: Precision Delivery Strategies, Therapeutic Breakthroughs, Challenges, and Future Perspectives
Wang Y, Wang N, Qu L, Jiao Y, Xiao Z
International Journal of Nanomedicine 2025, 20:14015-14031
Published Date: 22 November 2025
Intelligent Nanomedicine Systems Utilizing Diverse Nanoparticles for Osteosarcoma Therapy: A Review
Cai J, Yang H, He Z, Wu C
International Journal of Nanomedicine 2025, 20:14115-14130
Published Date: 25 November 2025
Formulation Progress, Challenges, and Perspectives of Anti-Inflammatory Natural Products
Fang H, Wu A, Zhao M, Nan X, Yang L, Liu H
Drug Design, Development and Therapy 2026, 20:606531
Published Date: 7 May 2026