Back to Journals » Clinical Ophthalmology » Volume 19
Practice Patterns and Technology Readiness for Sulcus Tube Placement: A Survey of the American Glaucoma Society Membership
Authors Rahman A, Whitney J, Abdeljabbar N, Webel AD
Received 6 April 2025
Accepted for publication 28 July 2025
Published 20 August 2025 Volume 2025:19 Pages 2871—2877
DOI https://doi.org/10.2147/OPTH.S532710
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Anya Rahman,1,* Jordan Whitney,1,* Nadine Abdeljabbar,1 Aaron D Webel1,2
1University of Missouri - Columbia School of Medicine, Columbia, MO, USA; 2Department of Ophthalmology, University of Missouri - Columbia, Columbia, MO, USA
*These authors contributed equally to this work
Correspondence: Aaron D Webel, Department of Ophthalmology, University of Missouri – Columbia, 3215 Wingate Ct Ste 102, Columbia, MO, 65201, USA, Tel +1 (573) 884-3937, Email [email protected]
Purpose: To evaluate glaucoma surgeons’ practice patterns regarding glaucoma drainage device (GDD) tube shunt placement, assess their opinions on sulcus tube placement, and evaluate their receptiveness to technologies designed to improve sulcus tube placement.
Patients and Methods: A 12-question survey was distributed electronically to American Glaucoma Society (AGS) members between November 6 and December 23, 2024. The survey assessed surgeons’ current tube-shunt placement practice patterns, factors influencing tube placement decisions, and receptiveness to proposed technologies designed for sulcus tube placement. Descriptive analysis was performed on 121 completed responses.
Results: Most respondents (55%) reported a preference for placing tubes in the anterior chamber (AC) for the majority of their pseudophakic patients, with efficiency (62%), safety (62%), and familiarity (57%) reported as primary factors for this decision. Barriers to sulcus placement included concern for intraocular bleeding (67%), technical difficulty of sulcus placement (54%), the risk of vitreous loss and tube occlusion (53%), and iris complications (53%). However, if a sulcus tube insertion technology was available and assuming a randomized controlled trial (RCT) demonstrated the superiority of sulcus over AC placement in minimizing endothelial cell loss (ECL), 85% of respondents indicated they would be likely to routinely place tubes in the sulcus. Features deemed very important for such a technology included tube placement accuracy (87%), ease of use (86%), IOP-lowering effectiveness (73%), time-efficiency (71%), and affordability (67%).
Conclusion: Currently, most glaucoma surgeons favor AC tube placement due to its familiarity, efficiency, and perceived safety, despite associated long-term risk of endothelial cell loss (ECL). Survey findings suggest strong interest in adopting sulcus placement, assuming a proven benefit on ECL and the availability of sulcus placement technologies designed to mitigate technical challenges. Development of robust data and reliable sulcus insertion technologies/techniques may change practice patterns.
Keywords: endothelial cell loss, glaucoma drainage devices, sulcus tube placement, surgical innovation
Introduction
Glaucoma is the leading cause of irreversible blindness globally,1 and is addressed using a wide array of treatment strategies to manage and slow its progression. The only proven therapy to prevent glaucomatous disease progression is lowering the intraocular pressure (IOP). IOP lowering can be accomplished medically, by laser therapy, or surgically, with micro-invasive glaucoma surgery (MIGS) angle-based procedures such as goniotomy and canaloplasty, minimally invasive bleb surgeries (MIBS) such as Preserflo or XEN gel stent implants, or traditional incisional glaucoma procedures such as trabeculectomy and glaucoma drainage device (GDD) tube-shunt surgery. Despite an increase in the use of minimally invasive surgical options, GDDs, utilized both as a primary treatment and as a secondary option when prior surgeries fail, are a mainstay among surgical options to control IOP.2 GDDs are generally comprised of a baseplate and tube, and the tube can be implanted in different ocular locations according to the patient’s particular anatomy and surgeon’s preference – such as the anterior chamber (AC), sulcus, or pars plana following vitrectomy.
In a survey of the AGS membership published in 2022, 90% of respondents indicated routinely placing tubes in the AC.3 However, the placement of tubes in the AC may come with an associated increased risk of corneal damage including endothelial cell loss (ECL). A study illustrated that tube insertion in the AC led to significant ECL over time, posing long-term risks to corneal health.4 Furthermore, studies suggest that insertion of tubes in the sulcus may provide a protective advantage, reducing the rate of ECL while still achieving comparable reductions in IOP as AC tube placement.4–6 Despite these findings, the survey results suggest that most surgeons continue to opt for AC tube placement.3
This survey study also aims to evaluate and assess glaucoma surgeons’ receptiveness to technologies and tools designed for efficient, consistent, and accurate sulcus tube placement. By assessing the receptiveness to innovations that facilitate consistent and accurate sulcus placement, this study seeks to understand the potential for a new technology to change practice patterns. This survey was intended to identify if demand exists for technologies designed to improve sulcus tube placement.
Materials and Methods
An Email with a Qualtrics electronic survey link was sent to the members of the American Glaucoma Society (AGS) subscribed to the AGS forum and responses were collected from November 6, 2024, to December 23, 2024. The AGS membership consists of ophthalmologists in the US and Canada who are actively practicing and have completed a glaucoma fellowship or are current fellows. Participation in the study was voluntary and was not incentivized. Informed consent was not needed for this study because no personal identification information was collected and the data from all participants was pooled together for analysis and publication. The study was approved by the Institutional Review Board at the University of Missouri, Columbia (IRB: 2122230).
The survey consisted of 12 questions (Supplemental Figure 1) wherein surgeons were asked to consider their current practices and preferences for tube shunt placement. Surgeons were asked to rate the level of significance for their reasoning regarding tube placement decisions. Additionally, surgeons evaluated the importance of various features of a potential new technology that would allow for efficient sulcus tube placement. Lastly, they were asked whether the availability of such a technology and an RCT showing the superiority of sulcus over AC placement related to ECL would change their practice patterns. Descriptive analysis was performed. Supplemental information from this survey is included.
Results
Our survey yielded a total of 121 completed survey responses. Most respondents reported practicing in the US (n = 73), one respondent reported practicing in Canada, and 47 respondents declined to list their country of practice. Respondents reported having between 0–5 years (n = 33, 28%), 6–10 years (n = 27, 23%), or 11–20 years (n = 32, 27%) of experience in performing tube shunt surgeries, with 22 respondents (18%) reporting 21–30 years of experience and 6 respondents (5%) reporting 31–50 years of experience. Most respondents (n = 69, 58%) reported performing 0–5 tube shunt surgeries per month, while 37 (31%) reported performing 6–10 tube shunt surgeries per month, 13 (11%) reported performing 11–20 tube shunt surgeries per month, and 1 (1%) reported performing 21–30 tube shunt surgeries per month. A preference for an anterior chamber (AC) approach was observed, with most respondents indicating that between 61–100% of tubes are placed in the anterior chamber for pseudophakic patients (n = 46, 55%) (Supplemental Table 1a).
Using a Likert scale (Not at all important, slightly important, moderately important, very important, extremely important), respondents rated various factors influencing their choice of either AC or sulcus placement. The number of respondents who selected either “very important” or “extremely important” were combined and compared to those who selected either “not at all important” or “slightly important”. Of these, efficiency (n = 75, 62%), safety (n = 75, 62%) and familiarity (n = 69, 57%) were selected as the most important reasons for choosing AC over sulcus tube placement. The lack of a “specifically designed sulcus tube insertion technology” was the only item listed as either “not at all important” or “slightly important” by most respondents (n = 68, 56%) (Supplemental Table 1b).
Respondents were also asked to rate the extent to which various factors would remain barriers to adopting sulcus tube placement, assuming an RCT demonstrated superiority of sulcus over AC tube placement for reducing ECL. When combining the “agree” and “strongly agree” response categories, concern for intraocular bleeding was the most highly reported barrier (n = 80, 67%), with technical difficulty of sulcus placement (n = 65, 54%), risk of vitreous loss and tube occlusion (n = 63, 53%), and concern for iris complications (n = 63, 53%) also being reported as barriers to adoption. Unfamiliarity with sulcus placement (n = 41, 34%) and increased surgical time (n = 39, 33%) were found to be less significant barriers (Table 1 and Figure 1).
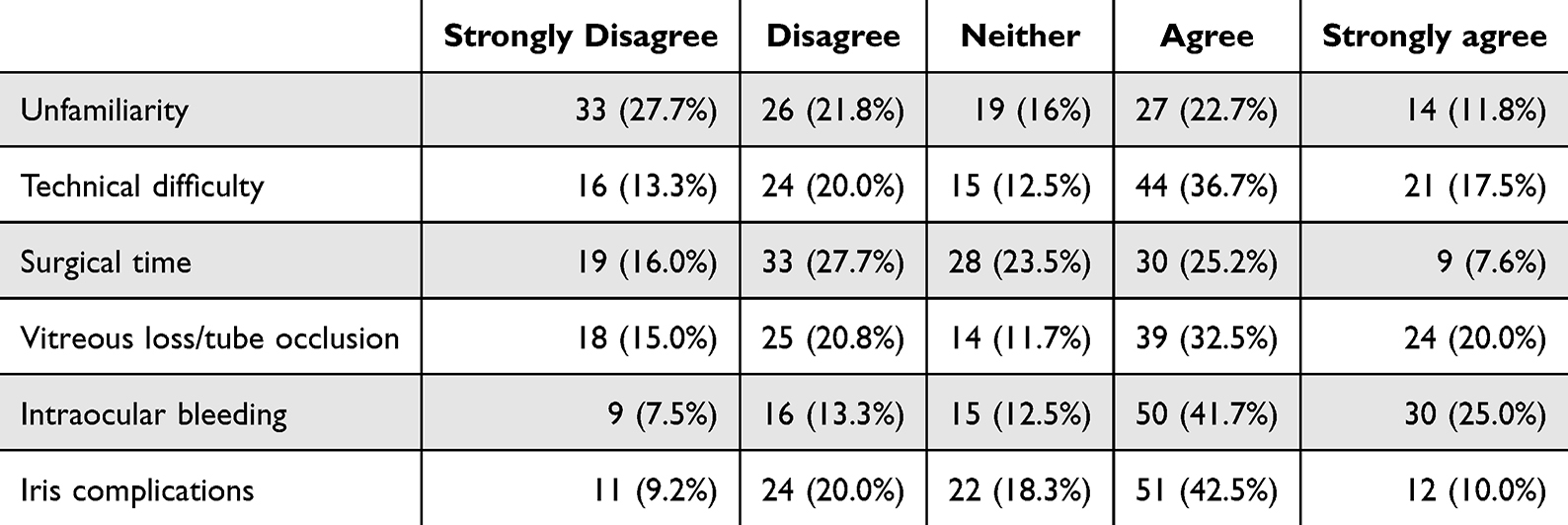 |
Table 1 Continued Barriers to Adoption of Sulcus Tube Placement if a Randomized Controlled Trial Demonstrated the Superiority of Sulcus Over AC Tube Placement for ECL |
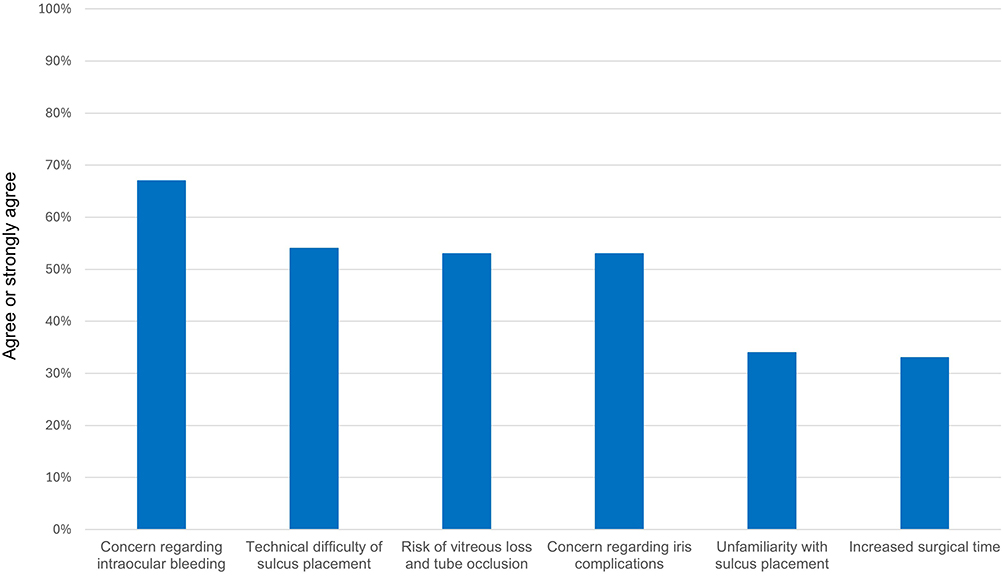 |
Figure 1 Continued barriers to adoption of sulcus tube placement if a randomized controlled trial demonstrated the superiority of sulcus over AC tube placement for endothelial cell loss. |
A large majority (n = 101, 85%) of respondents reported that they would be “likely” or “extremely likely” to routinely place tubes in the sulcus if a sulcus tube insertion technology was available that would allow for more efficient, consistent, and accurate sulcus tube placement, assuming also that a RCT demonstrated the superiority of sulcus over AC tube placement for ECL. (Table 2) Respondents were also asked to rate the importance of specific features in a new sulcus placement technology. Of features assessed, respondents most frequently rated accuracy of tube placement (n = 104, 87%), and ease of use (n 103, 86%) as “very important” or “extremely important” features. Device effectiveness of IOP-lowering (n = 87, 73%), surgical time-efficiency (n = 85, 71%), and affordability (n = 80, 67%) were also found to be “very important” or “extremely important” features (Supplemental Table 1c).
 |
Table 2 Likelihood of Surgeons Changing Tube Placement Practice Patterns Based on RCT Results Showing the Superiority of Sulcus Over AC Tube Placement for ECL and if a Sulcus Tube Technology Was Available |
When asked to indicate the maximum acceptable additional cost for a proposed sulcus tube insertion technology, a majority (81%) of AGS respondents reported a cost of greater than $5 would be acceptable, while approximately a quarter (26%) indicated a cost of more than $50 would be acceptable (Supplemental Table 1d).
Discussion
Although there remains controversy regarding sulcus tube position compared to AC tube position, there is growing evidence of the benefits of placing tubes in the sulcus. In terms of ECL associated with GDDs, several retrospective as well as nonrandomized interventional studies have shown that sulcus positioning results in less ECL compared to AC placement at 2 years.4–6 Evidence also suggests that AC tube placement is associated with increased rates of persistent corneal edema (12–16%),7–9 need for corneal transplantation (2–9%),7–9 and failure of corneal transplant grafts (50% within three years of AC tube placement).10–14 Despite the present survey results indicating a concern among surgeons regarding sulcus placement and possible intraocular bleeding, a retrospective review of GDDs in the sulcus vs the AC demonstrated that in fact the sulcus group had significantly lower rates of hyphema as well as lower rates of severe and late complications compared to the AC group.15 In addition, a retrospective comparison of AC, sulcus, and pars plana techniques found no significant differences in complication or surgical success rates between these three groups.16
With the goal of reducing the technical difficulty associated with sulcus tube placement, various ab interno and ab externo sulcus insertion techniques have been developed and described.15,17–25 In one ab externo technique utilizing a 30-gauge needle for a guiding sclerostomy followed by a larger 23-gauge needle pass, one retrospective review showed a similar reduction in both IOP and glaucoma medication use compared to AC placement.15 One ab interno sulcus tube internal needle guidewire technique (STING) described in a retrospective review resulted in significant IOP and medication reduction compared to baseline at an average follow-up of 11.8 months.25
Our survey findings indicate that most surgeons continue to prefer placing tubes in the anterior chamber (AC) in pseudophakic eyes, though to a lesser degree compared with a previous survey of AGS membership published in 2022.3 This preference persists despite the potential risk of ECL associated with AC placement. This suggests that a RCT demonstrating the superiority of sulcus over AC for ECL may change practice patterns. An ongoing trial called Glaucoma Drainage Device and Endothelial Cell Loss Compare Trial (DECLARE)26 aims to fill the knowledge gap by providing more definitive data regarding the impact of sulcus versus AC placement on long-term corneal health. A significant portion of respondents (85%) indicated they would be likely to adopt sulcus placement if RCT evidence demonstrated its superiority over AC placement on ECL and if a technology was available to mitigate the technical risks of sulcus insertion. This is slightly greater than the 77% of respondents who indicated they would change their practice pattern based on an RCT alone in the previous AGS survey.3 This suggests that advancements addressing the current technical challenges of sulcus placement, such as increased surgical time and the perceived risks of bleeding and other complications, could lead to a potential shift in practice patterns.
Key barriers to sulcus placement adoption included technical difficulty of this approach and the perceived risk of specific procedural complications, such as intraocular bleeding and tube occlusion. These barriers are in line with other data that highlight the challenges of sulcus placement. One retrospective analysis found that sulcus placement requires reinsertion 41% of the time due to malpositioning and is abandoned in 4% of cases.27 This real-world context of sulcus tube placement difficulty is mirrored by our survey results showing that a majority of respondents had concerns about intraocular bleeding (67%), vitreous loss and tube occlusion (53%), iris complications (53%), and technical difficulty of sulcus placement (54%), and that the specific features rated most important for a sulcus placement technology were accuracy of tube placement (87%) and ease of use (86%). This underscores an interest in surgical innovation that could make sulcus placement more accessible and reliable for surgeons.
While most respondents indicated that the lack of a specifically designed sulcus tube insertion technology was either “not at all important” or “slightly important” as their reason for selecting AC tube placement, the majority (81%) of surgeons indicated a willingness to pay greater than $5 for a sulcus tube insertion technology and over a quarter (26%) indicated that a cost of more than $50 would be acceptable This feedback is valuable for developers of glaucoma drainage devices and ophthalmic medical device manufacturers.
Our findings suggest that new technologies aimed at facilitating safe and effective sulcus tube placement may have an impact on clinical practices. Specifically, innovations that address current barriers—such as technical complexity, risk of complications, and increased surgical time—could encourage wider adoption of sulcus placement among glaucoma surgeons. This could lead to a reevaluation of current guidelines and training programs, potentially promoting sulcus placement as a standard option under certain conditions.
Based on these results, we recommend further studies to explore the long-term outcomes of sulcus versus AC placement in glaucoma surgery, particularly focusing on corneal health indicators and complications. Additionally, research into the development and validation of tools that streamline sulcus placement could provide the support needed for a shift in clinical practice. Studies that assess the effectiveness and cost-benefit of new technologies in sulcus placement could provide valuable insights for both practitioners and device manufacturers. Investigating the training requirements for sulcus placement could also help reduce technical barriers and improve the accessibility of this approach.
This study has several limitations. A sample size of 121 may limit the generalizability of the findings. Additionally, as the survey relied on self-reported data, results are subject to recall bias. There is also a possibility of response bias, where surgeons may overstate their openness to new techniques or technologies. Further research, including randomized controlled trials such as the DECLARE trial, is necessary to compare long-term outcomes between AC and sulcus tube placement.
Conclusion
This study highlights the current practice preferences and barriers faced by glaucoma surgeons in the placement of glaucoma drainage devices. Despite potential risks of endothelial cell loss, many surgeons continue to favor AC placement due to perceived safety, efficiency, and familiarity with the approach. However, most respondents expressed that they would be likely to adopt sulcus placement as their primary approach, particularly if robust evidence demonstrated its superiority in reducing endothelial cell loss and if new technologies addressed the technical challenges of this approach. There is a need for randomized controlled trial data to elucidate the long-term safety and effectiveness of sulcus versus AC placement of tube-shunts.
There is also an opportunity for technological innovation to improve the surgical efficiency and reliability of sulcus tube placement. While behavioral modification may trail hypothetical receptiveness to change indicated in survey responses, these results suggest that the introduction of robust data and reliable sulcus technologies/techniques has the potential to change glaucoma specialists’ practice patterns.
Abbreviations
ECL, endothelial cell loss. AC, anterior chamber. RCT, randomized controlled trial. IOP, intraocular pressure. MIGS, minimally invasive glaucoma surgery. MIBS, minimally invasive bleb surgery. GDD, glaucoma drainage device.
Funding
Dr. Aaron D. Webel reports a Mentoring for the Advancement of Physician Scientists (MAPS) grant from the American Glaucoma Society (AGS) to support this study.
Disclosure
Dr. Aaron D. Webel reports a pending patent for “SULCUS TUBE INTERNAL NEEDLE TECHNIQUE (STINT) AND STINT DEVICE”. The authors report no other conflicts of interest in this work.
References
1. Klein R, Klein BE. The prevalence of age-related eye diseases and visual impairment in aging: current estimates. Invest Ophthalmol Vis Sci. 2013;54(14):ORSF5–ORSF13. doi:10.1167/iovs.13-12789
2. Vinod K, Gedde SJ, Feuer WJ, et al. Practice preferences for glaucoma surgery: a survey of the American Glaucoma Society. J Glaucoma. 2017;26(8):687–693. doi:10.1097/IJG.0000000000000720
3. Yonamine S, Ton L, Rose-Nussbaumer J, et al. Survey of the American glaucoma society membership on current glaucoma drainage device placement and postoperative corticosteroid use. Clin Ophthalmol. 2022;16:2305–2310. doi:10.2147/OPTH.S369673
4. Godinho G, Barbosa-Breda J, Oliveira-Ferreira C, et al. Anterior chamber versus ciliary sulcus Ahmed glaucoma valve tube placement: longitudinal evaluation of corneal endothelial cell profiles. J Glaucoma. 2021;30(2):170–174. doi:10.1097/IJG.0000000000001700
5. Zhang Q, Liu Y, Thanapaisal S, et al. The effect of tube location on corneal endothelial cells in patients with Ahmed glaucoma valve. Ophthalmology. 2021;128(2):218–226. doi:10.1016/j.ophtha.2020.06.050
6. Kim JY, Lee JS, Lee T, et al. Corneal endothelial cell changes and surgical results after Ahmed glaucoma valve implantation: ciliary sulcus versus anterior chamber tube placement. Sci Rep. 2021;11(1):12986. doi:10.1038/s41598-021-92420-8
7. Gedde SJ, Herndon LW, Brandt JD, et al. Postoperative complications in the Tube Versus Trabeculectomy (TVT) study during five years of follow-up. Am J Ophthalmol. 2012;153(5):804–814. doi:10.1016/j.ajo.2011.10.024
8. Budenz DL, Feuer WJ, Barton K, et al; Ahmed Baerveldt Comparison Study Group. Postoperative complications in the Ahmed Baerveldt comparison study during five years of follow-up. Am J Ophthalmol. 163;2016:75–82.e3. doi:10.1016/j.ajo.2015.11.023
9. Christakis PG, Kalenak JW, Tsai JC, et al. The Ahmed versus Baerveldt study: five-year treatment outcomes. Ophthalmology. 2016;123(10):2093–2102. doi:10.1016/j.ophtha.2016.06.035
10. Coleman AL, Mondino BJ, Wilson MR, et al. Clinical experience with the Ahmed glaucoma valve implant in eyes with prior or concurrent penetrating keratoplasties. Am J Ophthalmol. 1997;123(1):54–61. doi:10.1016/S0002-9394(14)70992-4
11. Topouzis F, Coleman AL, Choplin N, et al. Follow-up of the original cohort with the Ahmed glaucoma valve implant. Am J Ophthalmol. 1999;128:198–204. doi:10.1016/S0002-9394(99)00080-X
12. Kwon YH, Taylor JM, Hong S, et al. Long-term results of eyes with penetrating keratoplasty and glaucoma drainage tube implant. Ophthalmology. 2001;108:272–278. doi:10.1016/S0161-6420(00)00496-6
13. Al-Torbak A. Graft survival and glaucoma outcome after simultaneous penetrating keratoplasty and Ahmed glaucoma valve implant. Cornea. 2003;22:194–197. doi:10.1097/00003226-200304000-00002
14. Alvarenga LS, Mannis MJ, Brandt JD, et al. The long-term results of keratoplasty in eyes with a glaucoma drainage device. Am J Ophthalmol. 2004;138(2):200–205. doi:10.1016/j.ajo.2004.02.058
15. Alobaida IA, Malik R, Ahmad S. Comparison of surgical outcomes between sulcus and anterior chamber implanted glaucoma drainage devices. Saudi J Ophthalmol. 2020;34(1):1–7. doi:10.4103/1319-4534.301298
16. Samuel S, Chang EK, Gupta S, et al. Outcomes of anterior chamber, sulcus, and pars plana glaucoma drainage device placement in glaucoma patients. J Ophthalmol. 2022;2022:5947992. doi:10.1155/2022/5947992
17. Tello C, Espana EM, Mora R, Dorairaj S, Liebmann JM, Ritch R. Baerveldt glaucoma implant insertion in the posterior chamber sulcus. Br J Ophthalmol. 2007;91(6):739–742. doi:10.1136/bjo.2006.107839
18. Kasuga T, Asaoka S, Asada Y, et al. Proline-assisted tube insertion through sulcus in Ahmed valve. J Glaucoma. 2020;29(9):e106–e107. doi:10.1097/IJG.0000000000001602
19. Nitta K, Akiyama H. A new technique using a 4-0 nylon thread as a guide for easy and precise tube insertion of Ahmed glaucoma valve implant into ciliary sulcus. Cureus. 2023;15(2):e34854. doi:10.7759/cureus.34854
20. Camejo LMD, Noecker R. Ab interno sulcus placement of glaucoma tube implants. Ophthalmic Surg Lasers Imaging. 2008;39(5):434–435. doi:10.3928/15428877-20080901-04
21. Loayza-Gamboa W, Martel-Ramirez V, Inga-Condezo V, Valderrama-Albino V, Alvarado-Villacorta R, Valera-Cornejo D. Needle guided ab interno technique for tube insertion through the ciliary sulcus in uncontrolled glaucoma. Eur J Ophthalmol. 2022;32(1):704–708. doi:10.1177/11206721211007093
22. Maheshwari D, Rao S, Pawar N, Kadar MA, Ramakrishnan R. Early outcomes of 21-gauge needle-guided ab interno tube sulcus placement of a non-valved implant in pseudophakic eyes. Indian J Ophthalmol. 2022;70(3):1051–1053. doi:10.4103/ijo.IJO_2303_21
23. Moreno-Montañés J, Fantes F, García-Gómez P. Polypropylene suture-guided valve tube for posterior chamber implantation in patients with pseudophakic glaucoma. J Cataract Refract Surg. 2008;34(11):1828–1831. doi:10.1016/j.jcrs.2008.05.063
24. Shah A, Kanter JA, Eisengart J, Blieden LS, Qiu M. Three techniques for guidewire-assisted sulcus glaucoma tube shunt placement. Am J Ophthalmol Case Rep. 2024;34:102009. doi:10.1016/j.ajoc.2024.102009
25. Shao CG, Gharabagi AP, King J, Webel AD. Sulcus tube internal needle guidewire technique for glaucoma drainage device placement: improving surgical ease and precision. Ophthalmol Ther. 2024;13(2):635–643. doi:10.1007/s40123-023-00848-0
26. Sulcus versus anterior chamber tube placement for glaucoma drainage devices (DECLARE). ClinicalTrials.gov. Updated May 28, 2024. Available from: https://clinicaltrials.gov/study/NCT05924477. Accessed June 7, 2025.
27. Asaoka S, Kasuga T, Matsunaga T, et al. Operative complications of glaucoma drainage implant tube insertion through the sulcus for pseudophakic eye. J Glaucoma. 2021;30(4):e169–e174. doi:10.1097/IJG.0000000000001783
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.