Back to Journals » Open Access Emergency Medicine » Volume 13
Practice Patterns and Assessment of Needs for Pediatric Pain Management in Alberta Emergency Departments
Authors Bar Am N, Thull-Freedman J ![]() , Ali S
, Ali S ![]()
Received 6 September 2021
Accepted for publication 3 December 2021
Published 24 December 2021 Volume 2021:13 Pages 587—594
DOI https://doi.org/10.2147/OAEM.S337900
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Hans-Christoph Pape
Neta Bar Am,1 Jennifer Thull-Freedman,1 Samina Ali2
1Departments of Pediatrics and Emergency Medicine, Cumming School of Medicine, University of Calgary, Calgary, Alberta, Canada; 2Department of Pediatrics, Faculty of Medicine & Dentistry, University of Alberta, Edmonton, Alberta, and Women and Children’s Research Institute, University of Alberta, Edmonton, Alberta, Canada
Correspondence: Samina Ali
Department of Pediatrics, 3-582 Edmonton Clinic Health Academy, 11405 – 87 Avenue, Edmonton, Alberta, T6G 1C9, Canada
Tel +1 780 248-5575
Fax +1 888 775-8876
Email [email protected]
Purpose: Many rural and community emergency departments (EDs) experience barriers to providing optimal pain care to children. In preparation for a quality improvement initiative, our team conducted a provincial pediatric pain management practice and needs assessment.
Methods: An online survey was sent to ED administrators and educators from March to May 2017. Themes included pain assessment, pain and distress management strategies, available resources, education, barriers to care, and opportunities for improvement.
Results: Forty-five respondents, from 31 EDs representing all five geographic health zones in Alberta, completed the survey. Use of a pain assessment tool was reported at 93.5% (29/31 sites) of the sites. Topical anesthesia was employed “most of the time” before suturing at 67% (18/27) of sites, versus 15% (4/27) before blood work or IV insertion. Eighty-one percent (22/27) of sites reported physically restraining children for procedures “often”, while 37% (10/27) reported use of comfort positioning “often”. Digital distraction devices were available at 37% (10/27) of sites. Reported challenges included lack of resources (33.3%, 12/36), staff education/knowledge (33.3%, 12/36), and absent policies/poor policy adherence (25.0%, 9/36). Opportunities for improvement included staff member education (73.5%, 25/34) and more resources (58.8%, 20/34). Respondents rated their site’s overall ability to manage children’s pain as 50/100 [IQR:21,61].
Conclusion: General EDs report providing suboptimal children’s pain care, with use of physical restraint for medical procedures, and under-utilization of evidence-based, inexpensive treatment options. There are many gaps in children’s pain care in rural and community EDs which could be addressed through collaborative quality improvement initiatives.
Keywords: children, rural, procedural pain, pain treatment
Introduction
Effective pain management for children visiting emergency departments (EDs) is an internationally recognized priority and has been identified as a fundamental human right.1–3 Undertreatment of healthcare-associated pain may cause both short and long-term negative consequences.4 In the short-term, there is pain and distress for the child, caregivers, and healthcare providers; prolonged procedure time; and slower healing.1,3,5 In the long-term, children can experience increased sensitivity to pain; increased medical care avoidance; social hyper-vigilance; and higher levels of anxiety before a procedure.1,3,5 Expeditious and effective multi-modal pain care improves procedure success rates, decreases the need for repeated attempts, improves ED flow, and improves satisfaction.6 Research has produced high-quality evidence for effective management of children’s pain and numerous initiatives have been established in an attempt to improve care.7–11 While significant progress has been achieved in the form of age-appropriate assessment tools and evidence-based effective treatments, children’s pain often remains undertreated.4,12–17
The province of Alberta has a population of 4.1 million individuals.18 Approximately 55% of the population lives in two large metropolitan areas (Edmonton and Calgary), while the rest of the population is distributed across a broad geographic area.19 In 2018/19, there were 454,252 visits by children to Alberta’s EDs. Nearly three-quarters of these visits took place outside of the province’s two pediatric hospitals, in rural and community EDs.20,21
A 2009 assessment of pediatric pain practices in Alberta’s EDs concluded that few EDs used policies and protocols to manage pediatric pain and that methods to limit procedural pain were underutilized.17 Because of this recognized need, quality improvement (QI) work was initiated through a joint effort between Alberta’s two pediatric emergency departments, and in 2017, plans were made to reassess needs (given that almost a decade had passed and significant political changes had also occurred in the province) and subsequently implement a province-wide children’s pain improvement strategy through the formation of a QI collaborative.6,22–24 We surveyed administrators and nurse educators across Alberta EDs in order to identify current a) practices, b) needs, and c) barriers in EDs that were planning to participate, in order to tailor a quality improvement collaborative to the specific needs of the community that it was intended to serve.
Materials and Methods
Study Design and Time Period
A descriptive cross-sectional survey was conducted from March to May 2017, as part of a QI collaborative addressing pediatric pain management in EDs across Alberta. The project ethics were reviewed according to local procedures for QI. The project was also assessed by the University of Calgary’s Research Ethics Board and deemed to be exempted from review due to its status as QI work.
Setting and Population
Contact information for ED administrators and nurse educators was obtained via the Alberta Health Services Emergency Strategic Clinical Network. There were 108 EDs in Alberta at the time of study. Ten EDs already participating in a pilot phase of the QI collaborative and 2 EDs that did not treat children were excluded. This left 96 EDs eligible to participate.
Survey Tool and Implementation
The survey tool was created, de novo, for the sole purpose of informing the quality improvement collaborative. As such, no formal psychometric testing was performed on the tool, as it was not expected to be used in a repetitive fashion. Questions were created based on expert opinion and reviewed with local ED staff for face and content validity. The survey consisted of a combination of 22 multiple-choice, short-answer and open-ended questions. (See Appendix 1) Survey questions addressed 1) use of pain scales and pain medications, 2) use of non-medicinal comfort measures, 3) parent/guardian presence for procedures, 4) use of topical anesthetics, 4) pediatric pain education for staff, 5) availability of patient education materials, 6) challenges to pediatric pain management, and 7) overall impression of pain management at the site.
An introductory information letter and link to an electronic survey (via SurveyMonkey.com) was sent by email to all nursing and medical leaders at the eligible EDs. Consent was implied in completion of the survey; further, participants were permitted to skip any questions, at their discretion. Two reminders were sent at 2-week intervals, and responses were collected over a 75-day period. The estimated time to complete the survey was 10–15 minutes. A separate email was sent to the same individuals inviting their ED to participate in the anticipated QI collaborative to improve management of children’s pain.
Outcome Measures
The main outcome measure was the proportions of EDs reporting availability of specific pain and distress management resources and strategies. Secondary outcomes included reported frequency of use of strategies, reported barriers, and overall impression of effectiveness of pediatric pain management at the site, reported using a visual analog scale.
Analysis
Data were collected using the SurveyMonkey™ platform and transferred to an ExcelTM spreadsheet for analysis. More than one response was allowed per site. In cases of disagreement regarding availability of a particular resource, sites were counted as having the resource if either respondent reported availability of the resource at their site. In cases of disagreement for an ordinal response, the median response was chosen. In cases of disagreement in questions concerning care practices, the response of the respondent who provided direct care to patients took precedence. For analysis of open-ended questions, two individuals (NB, JTF) reviewed the responses independently for themes and determined a coding schema through consensus. The coding schema was categorized into emerging themes and subthemes. Both team members reviewed the categorization, and disagreements were resolved by consensus.
Results
Demographic Characteristics and Setting
Forty-five individuals from 31 different sites responded to the survey, representing a 32% response rate, by site (22% individual response rate). The median annual ED census of responding sites was 18,217 (Range 2989–73,904; IQR 12,715–48,510). The median annual pediatric census of responding sites was 3519 (Range 548–13,325; IQR 2326–8269). All five geographic health zones in Alberta were represented. See Table 1 for demographic characteristics.
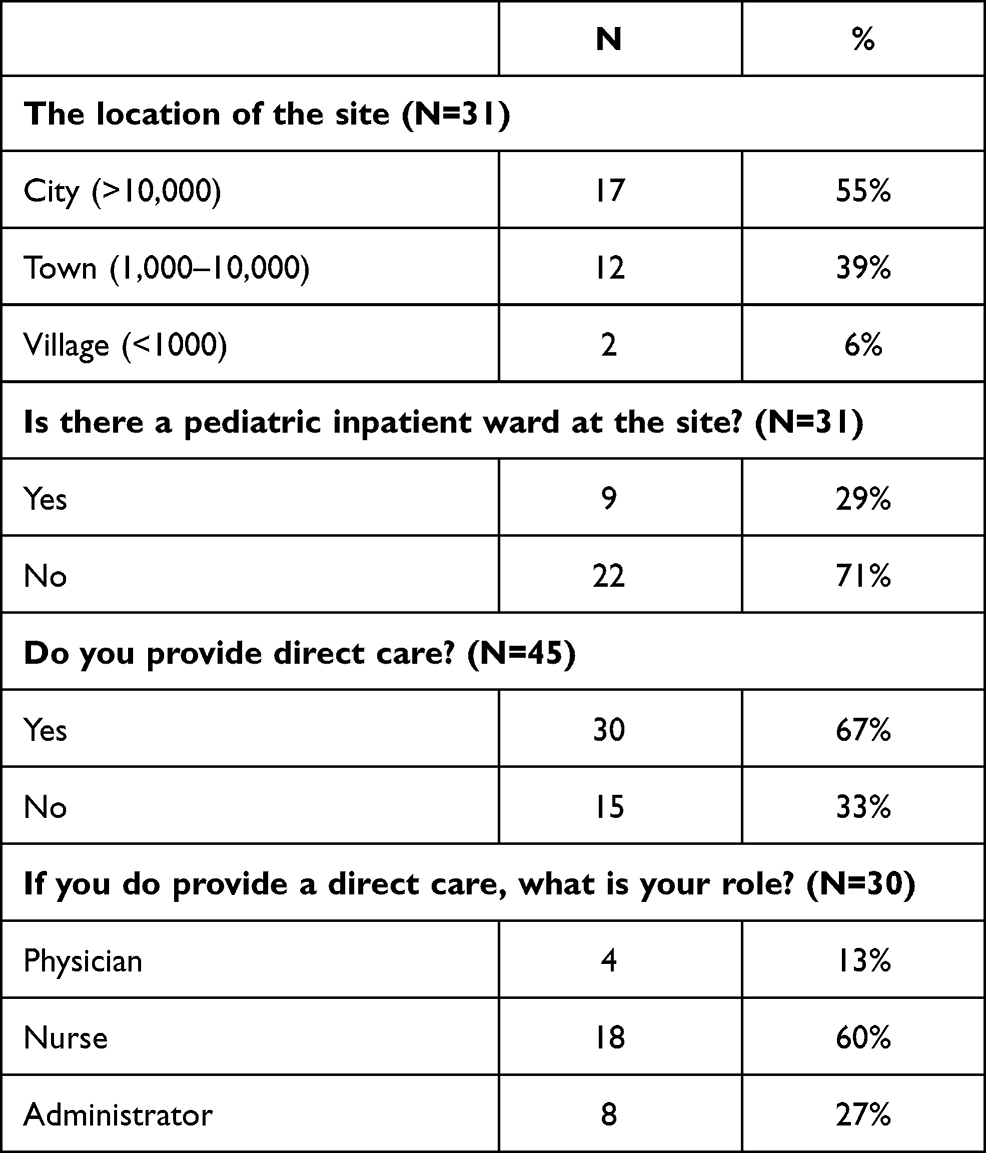 |
Table 1 Demographic Characteristics and Setting |
Pain Assessment
Pain scales were reported to be available at 93.5% of the sites (29/31); these included the Faces Pain Scale-Revised (71%, 22/31), the Verbal Numerical Rating Scale (71%, 22/31), a printed numerical rating scale (26%, 8/31) and the FLACC (Face, Legs, Activity, Cry, Consolability) scale (13%, 4/31). Printed and posted pain scales were most often located at triage (68%, 21/31). At 29% of the sites (9/31), a printed pain scale was in patient treatment rooms.
Pain and Distress Management
Figure 1 presents available non-pharmacological options for pain and distress management at sites. Cold packs (100%), splints (93%), and toys/books (70%) were the most widely available options.
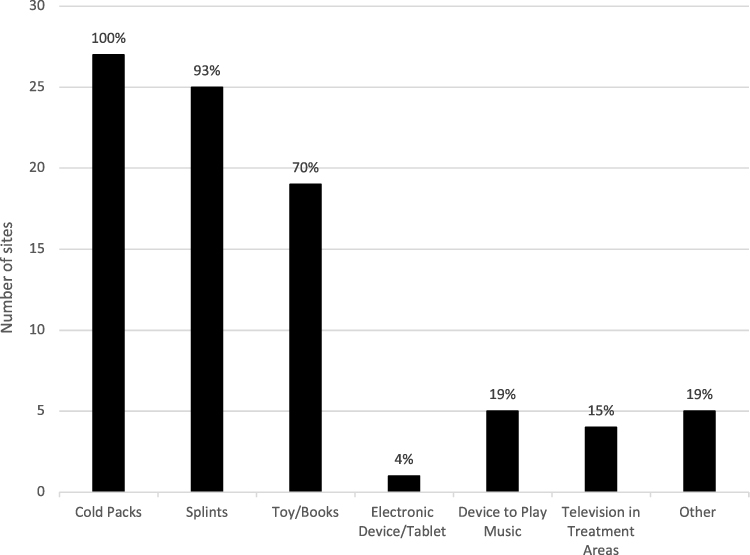 |
Figure 1 Non-pharmacologic options for pain and distress available at ED sites (n=31). |
Figure 2 presents reported availability of medications at sites. Acetaminophen, ibuprofen, ketorolac, and topical anesthetic cream were universally reported as available at all EDs. Less than half of the sites had access to nitrous oxide (48%) and vapocoolant spray (7%).
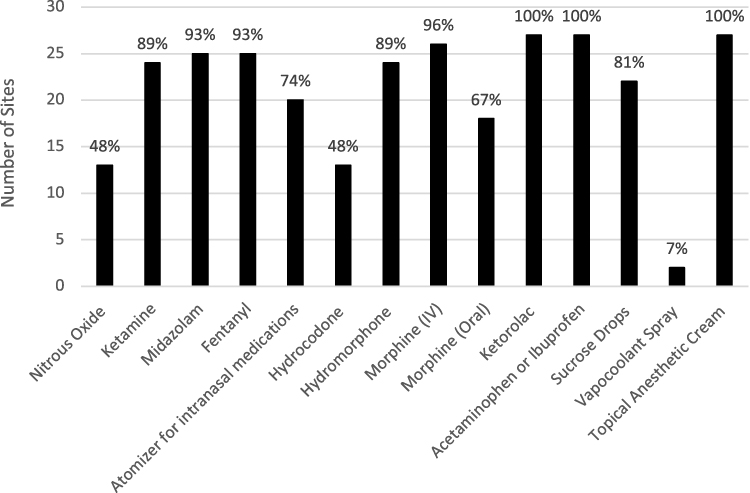 |
Figure 2 Pain medications available across sites (n=27). |
Figure 3 displays available comfort measures that were reported to be used during needle procedures. Only 67% of respondents reported topical anesthetics being used prior to suturing, 15% as using topical anesthetic creams prior to venipuncture, and 37% use of comfort positions for needle procedures “most of the time”. Together with comfort measures, the respondents were asked how often children aged 0–6 years that require a needle procedure are restrained by staff or parents while lying on the bed. 56% (15/27) of them indicated that the restraint is done “most of the time”, while 15% (4/24) answered it is done “not very often”. None said it is “never” being done.
 |
Figure 3 Comfort measures during needle procedures (N=27). |
Pain-Related Education and Training
In 35% of the sites (11/31), new nurses received education in pediatric pain management during orientation, while 39% (12/31) of the sites do not provide such education; 26% (8/31) did not answer/did not know. Annual education in pediatric pain management for nurses was available at 16% (5/31) of the sites; 65% (20/31) of the sites does not provide this content routinely, and 19% of respondents (6/31) did not answer/did not know. Only 6% (2/31) of the sites reported physician education regarding pediatric pain management; 10/31 (32%) of the sites did not provide such education, and 61% (19/31) of responders did not answer the question/did not know. Only one respondent answered that staff received education on how to communicate with a child before, during and after a potentially painful procedure (3.2%, 1/31). 42% of the sites (13/31) reported printed patient education materials regarding children’s pain were available.
Reported Challenges and Opportunities for Improvement
Challenges encountered when treating children’s pain in their ED are summarized in Table 2. The top three reported challenged were staff education/knowledge (33.3%, 12/36), lack of resources (33.3%, 12/36), and lack of policies or poor policy adherence (25.0%, 9/36). The top three reported opportunities for improvement were consistent staff education (73.5%, 25/36), more pain and distress treatment resources (59.8%, 20/36), and staff engagement/ prioritization of pain treatment (14.7%, 5/36). When participants were asked to indicate how well they believed their site managed children’s pain overall, the median response was 50 out of 100 [IQR:21,61].
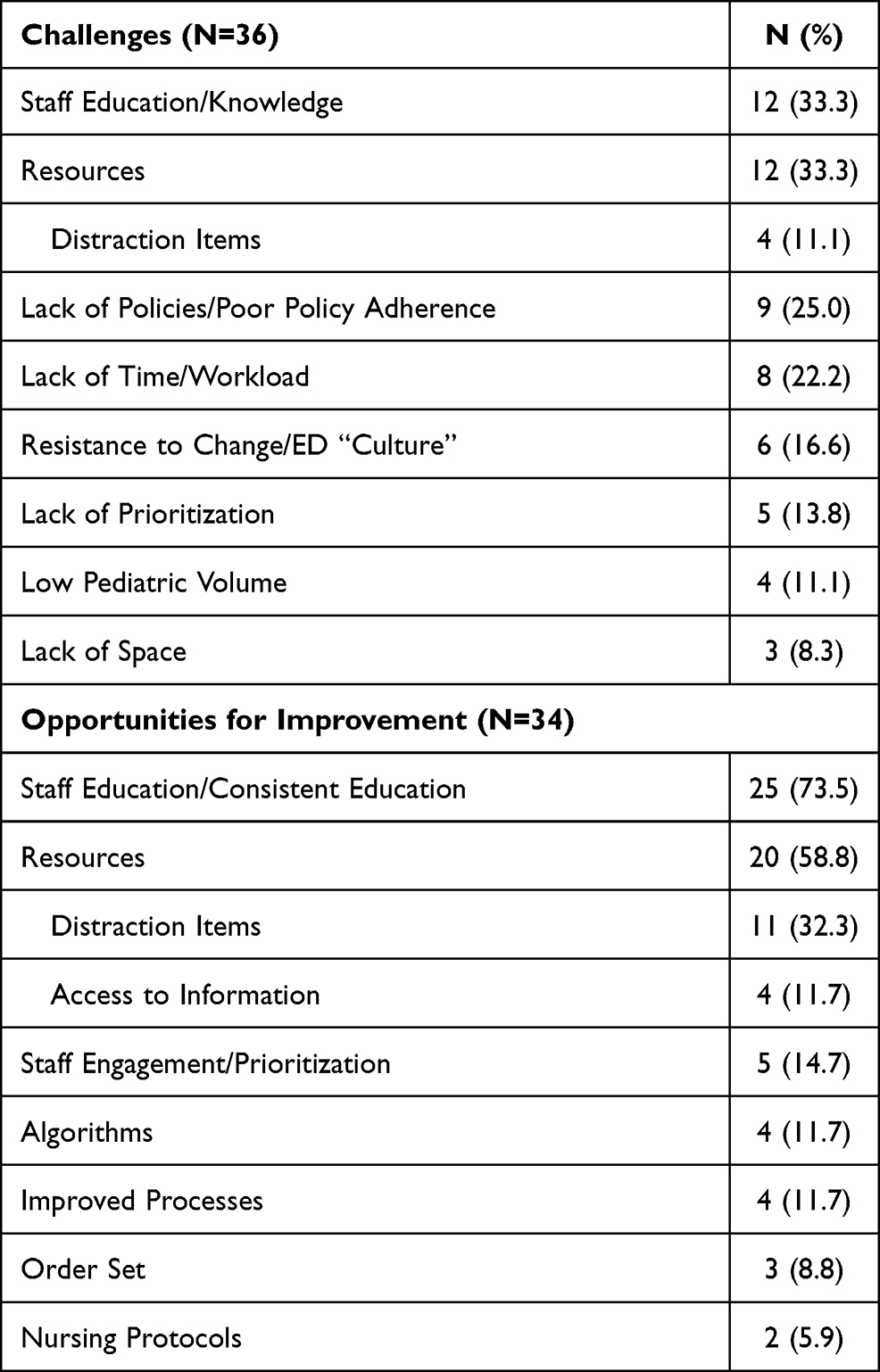 |
Table 2 Challenges and Opportunities for Improvement in Children’s Pain Management |
Discussion
This survey was conducted to inform a province-wide, pain-focused quality improvement collaborative. Pain assessment was reported as occurring at almost all rural and community emergency sites. Despite evidence to support its use, topical anesthesia application before suturing or needle procedures was under-used, physical restraint was employed often at over half the sites, and comfort positioning of a child (with their caregiver) was reported at only a third of sites.2 Staff education about pediatric pain management is very limited. The respondents reported a relatively low (50/100) rating of their ED’s current pediatric pain management. The greatest challenge, but also the greatest opportunity for improvement that the staff members identified was education for the staff members. Another challenge was a lack of resources, especially distraction tool kits.
Pain scales are reported to be in high availability (and presumed resultant use, as per the respondents) at the sites responded to this survey. Compared to a similar survey conducted in 2009 in Alberta EDs,17 the current report of pain scale use is 22.5% higher (71% vs 93.5%). Still, age-appropriate pain scales are not available at all EDs (eg, FLACC). This gap can disproportionately affect the pain measurement and treatment of the most vulnerable, mainly infants and non-verbal children.11,25–27 Working to improve availability and use of pediatric-specific scales could be a low-cost early intervention to improve pain care, at both the individual practitioner level and institutionally.
While some comfort measures are available, there is a shortage of distraction toolkits, and especially electronic devices. In a former study regarding general EDs across Alberta, distraction kits were present in 32% of the EDs, while toys were available in 77%.17 This mirrors the findings of our study, in which 37% (10/27) of the EDs reported having electronic devices for distraction, and 70% (19/27) had toys or books. In contrast, electronic distraction tools’ availability was higher in Canadian pediatric EDs (87%).23 Distraction kits can be inexpensive and can include simple but effective items such as books, pinwheels, light wands, and bubbles.4 Further, relatively inexpensive but versatile digital devices (eg, tablets) can be used and easily sanitized between patients. Integration of these digital and non-digital distraction tools can be accomplished by creating ED-specific toolkits, affixing search-and-find decals in examining rooms, and even simply accessing children’s music and videos via a personal mobile device.
While there seems to be a national readiness in pediatric EDs to encourage family presence during procedures or employ comfort positions,23 it has not been consistently operationalized in general EDs in Alberta. Guiding caregivers’ presence during medical procedures can help improve the experience for all; they can be encouraged to calmly support their child with distraction, gentle touch (if the child wishes), and soothing words (“I’m here for you,” “I love you”). Another identified challenge was that the staff members were not taught what to say to a child before, during and after a procedure. Techniques and interventions, like family presence during the procedure, positioning, cognitive-behavioral interventions or staff communication skills, can be easily taught and adapted to a variety of ED settings, and therefore it may be wise to strengthen these abilities among ED staff.13–15,17
There is a wide range of medications available at the Alberta EDs, including topical anesthetics. Current evidence already indicates the advantages of topical anesthetics at the ED, including higher success rates for procedures, shorter procedure times and less pain.4,28 Alarmingly, the reported use of topical anesthetic creams before IV or bloodwork was lower than previously reported in the same setting, and these lower rates can likely be ascribed to mainly lack of knowledge or staff education, lack of resources, lack of formal strategies for such treatment, poor policy adherence, and high workload that prevent them from providing the treatment.17 Staffing issues were not indicated as a challenge in our study, but a lack of policies or poor adherence to the policies were noted more often than had been reported in the past.17 Lack of time has been mentioned as an obstacle in our study as well as previous studies, and so has inexperience or low pediatric volume. It is worth noting, however, that inexperience with children as an obstacle to pain treatment was mentioned less often than in the previously described Alberta ED study (11 vs 27%). Knowing that the evidence for this simple intervention is so well-established, quality improvement work to improve the uptake of its use would be a logical next steps for institutions where it is still not well-integrated into care.
Similar to the previous Alberta ED survey, lack of knowledge/education is still described as the greatest barrier to pain treatment.17 In this former study, Alberta administrators expressed a desire for more pain management education for staff. Opportunities for education available to nurses and physicians was lower than has been reported in pediatric EDs, in which 53% of sites report education for nurses and 13% of sites report education for physicians.23 A high proportion of respondents in our study named education as an important opportunity for improvement. This can be established best through local, tailored efforts, but could also take advantage of nationally available resources. Globally, many different strategies have been tried to improve children’s pain treatment in EDs, including quality improvement strategies, education interventions and development of guidelines.28–31 All proposed programs were interdisciplinary. The interventions include improvement of processes in order to better communication among staff members, one-day sessions and simulation-based training.9,29,31 Knowledge mobilization efforts such as Translating Emergency Knowledge for Kids (TREKK) and Solutions for Kids in Pain (SKIP) have also attempted to address this issue. TREKK’s collaborative approach has collected the information needs of emergency healthcare professionals and families and used their infrastructure to provide online access to thousands of pediatric emergency resources, including evidence-based clinical and educational resources. They also provide educational sessions and meetings that has built connections between over 165 rural, remote, and urban Canadian EDs.32 Still, further collaborative efforts, working with community practitioners and families, are needed to address these gaps.
There is continued scope for improving children’s pain care in the general ED setting, by implementing low and no-cost, evidence-based interventions. These interventions include comfort positioning, avoiding physical restraint, and utilizing topical anesthetic agents. A gap in education has been identified by ED administrators and educators. Therefore, it is not surprising that many respondents indicated that the opportunity for change lies within education of the staff. It therefore seems likely that a quality improvement initiative that includes pediatric pain management education would be well received by Alberta’s rural and community EDs. It is encouraging that in our study nearly all responding sites reported interest in undertaking quality improvement activities in this area.
Currently, there is limited understanding of how to best improve pediatric pain management practices in general EDs. It would be informative to understand pediatric pain-related institutional needs across wider geographic areas. Research is needed to understand which strategies are most effective in improving children’s pain outcomes in these EDs. There is a need to study and report on which educational and quality improvement initiatives works best for pediatric pain care in the rural and community ED settings, so that pediatric centres may support these facilities in optimizing pain treatment for children.
Limitations
While our study covers approximately one quarter of the Albertan EDs and all geographic zones within the province, selection bias may have led respondents with a greater interest in the subject of pediatric pain to respond. Respondents may not have had a full understanding of all the aspects of pediatric pain treatment they were asked to report, and we did not independently verify the accuracy of their answers. Lastly, this survey is subject to reporting bias, as the results reflect the responses of a small number of administrators, based on their perception of practice rather than observed practice.
Conclusion
We evaluated pediatric pain management practices reported in a cross-section of rural and community EDs across Alberta. Our work shows that although most pharmacological and non-pharmacological treatments are reported as available, their use is sub-optimal. However, there is a high level of interest in participating in quality improvement in this area. Supporting rural and community healthcare facilities and EDs in implementing evidence-based, quality improvement initiatives may facilitate better pain and distress management, and ultimately improve the experience of children and their families.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Brennan F, Carr DB, Cousins M. Pain management: a fundamental human right. Anesth Analg. 2007;105(1):205–221. doi:10.1213/01.ane.0000268145.52345.55
2. Trottier ED, Doré-Bergeron M-J, Chauvin-Kimoff L, Baerg K, Ali S. Managing pain and distress in children undergoing brief diagnostic and therapeutic procedures. Paediatr Child Health. 2019;24(8):509–521. doi:10.1093/pch/pxz026
3. Stinson JN, McGrath P. No pain - all gain: advocating for improved paediatric pain management. Paediatr Child Health. 2007;12(2):93–94.
4. Fein JA, Zempsky WT, Cravero JP. Relief of pain and anxiety in pediatric patients in emergency medical systems. Pediatrics. 2012;130(5):e1391–e1405. doi:10.1542/peds.2012-2536
5. Ali S, McGrath T, Drendel AL. An evidence-based approach to minimizing acute procedural pain in the emergency department and beyond. Pediatr Emerg Care. 2016;32(1):36–42. doi:10.1097/PEC.0000000000000669
6. Drendel AL, Ali S. Ten practical ways to make your ed practice less painful and more child-friendly. Clin Pediatr Emerg Med. 2017;18(4):242–255. doi:10.1016/j.cpem.2017.09.001
7. Ducharme J. Acute pain and pain control: state of the art. Ann Emerg Med. 2000;35(6):592–603. doi:10.1016/S0196-0644(00)70033-3
8. Committee on Psychosocial Aspects of Child and Family H. The Assessment and management of acute pain in infants, children, and adolescents. Pediatrics. 2001;108(3):793–797. doi:10.1542/peds.108.3.793
9. Corwin DJ, Kessler DO, Auerbach M, Liang A, Kristinsson G. An intervention to improve pain management in the pediatric emergency department. Pediatr Emerg Care. 2012;28(6):524–528. doi:10.1097/PEC.0b013e3182587d27
10. Fosnocht DE, Swanson ER, Barton ED. Changing attitudes about pain and pain control in emergency medicine. Emerg Med Clin North Am. 2005;23(2):297–306. doi:10.1016/j.emc.2004.12.003
11. Le May S, Johnston CC, Choinière M, et al. Pain Management Practices in a Pediatric Emergency Room (PAMPER) Study: interventions With Nurses. Pediatr Emerg Care. 2009;25(8):498–503. doi:10.1097/PEC.0b013e3181b0a0af
12. Jacob R, Shavit I. Emergency department pain management of acute abdominal pain and acute appendicitis in children. Isr Med Assoc J. 2016;18(11):689–691.
13. Krauss BSD, Calligaris LMD, Green SMP, Barbi EMD. Current concepts in management of pain in children in the emergency department. Lancet. 2016;387(10013):83–92. doi:10.1016/S0140-6736(14)61686-X
14. Pillai Riddell RR, Racine NM, Gennis HG, et al. Non‐pharmacological management of infant and young child procedural pain. Cochrane Database Syst Rev. 2015;2017(7):CD006275–CD006275. doi:10.1002/14651858.CD006275.pub3
15. Taddio A, Appleton M, Bortolussi R, et al. Reducing the pain of childhood vaccination: an evidence-based clinical practice guideline. CMAJ. 2010;182(18):E843–E855. doi:10.1503/cmaj.101720
16. Scott WA, Golzari SEJ, Soleimanpour H, et al. Procedural Sedation and Analgesia in Children. N Engl J Med. 2014;371(1):90–91. doi:10.1056/NEJMc1405676
17. Ali S, Chambers AL, Johnson DW, et al. Paediatric pain management practice and policies across Alberta emergency departments. Paediatr Child Health. 2014;19(4):190–194. doi:10.1093/pch/19.4.190
18. Statistics Canada. Statistics Canada, Estimates of population (2016 Census and administrative data), by age group and sex for July 1st, Canada, provinces, territories, health regions (2018 boundaries) and peer groups. Available from: https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1710013401.
19. Statistics Canada. Statistics Canada, Population estimates, July 1, by census subdivision, 2016 boundaries Table 17- 10-0142-01: Statistics Canada; 2016. doi:10.25318/1710014201-eng
20. McGillivray D, Nijssen-Jordan C, Kramer MS, Yang H, Platt R. Critical pediatric equipment availability in Canadian hospital emergency departments. Ann Emerg Med. 2001;37(4):371–376. doi:10.1067/mem.2001.112253
21. Grant I. The future of emergency medicine in Canada: submission from CAEP to the Romanow Commission. Part 1. CJEM. 2002;4(5):359–368. doi:10.1017/S1481803500007788
22. Ali S, Weingarten LE, Kircher J, et al. A survey of caregiver perspectives on children’s pain management in the emergency department. CJEM. 2016;18(2):98–105. doi:10.1017/cem.2015.68
23. Trottier ED, Ali S, Le May S, Gravel J. Treating and reducing anxiety and pain in the paediatric emergency department: the TRAPPED survey. Paediatr Child Health. 2015;20(5):239–244. doi:10.1093/pch/20.5.239
24. Shave K, Ali S, Scott SD, Hartling L. Procedural pain in children: a qualitative study of caregiver experiences and information needs. BMC Pediatr. 2018;18(1):324. doi:10.1186/s12887-018-1300-y
25. Ung A, Salamonson Y, Hu W, Gallego G. Assessing knowledge, perceptions and attitudes to pain management among medical and nursing students: a review of the literature. Br J Pain. 2016;10(1):8–21. doi:10.1177/2049463715583142
26. Ramira ML, Instone S, Clark MJ. Pediatric pain management: an evidence-based approach. Pediatr Nurs. 2016;42(1):39–49.
27. Harris J, Ramelet A-S, van Dijk M, et al. Clinical recommendations for pain, sedation, withdrawal and delirium assessment in critically ill infants and children: an ESPNIC position statement for healthcare professionals. Intensive Care Med. 2016;42(6):972–986. doi:10.1007/s00134-016-4344-1
28. Sherman JM, Sheppard P, Hoppa E, Krief W, Avarello J. Let Us Use LET: a Quality Improvement Initiative. Pediatr Emerg Care. 2016;32(7):440–443. doi:10.1097/PEC.0000000000000276
29. Friedman N, Sagi D, Ziv A, Shavit I. Pediatric residents’ simulation-based training in patient safety during sedation. Eur J Pediatr. 2018;177(12):1863–1867. doi:10.1007/s00431-018-3241-8
30. Sauter TC, Hautz WE, Hostettler S, et al. Interprofessional and interdisciplinary simulation-based training leads to safe sedation procedures in the emergency department. Scand J Trauma Resusc Emerg Med. 2016;24(1):97. doi:10.1186/s13049-016-0291-7
31. Iyer SB, Schubert CJ, Schoettker PJ, Reeves SD. Use of quality-improvement methods to improve timeliness of analgesic delivery. Pediatrics. 2011;127(1):e219–e225. doi:10.1542/peds.2010-0632
32. Knisley L, Hartling L, Jabbour M, et al. Translating Emergency Knowledge for Kids (TREKK): using research evidence to improve outcomes for children and families in emergency departments across Canada. CJEM. 2021. doi:10.1007/s43678-021-00205-9
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.