Back to Journals » International Journal of General Medicine » Volume 14
Practice and Factors Associated with Informed Consenting Process for Major Surgical Procedures Among Health-Care Workers, South Eastern Ethiopia
Authors Negash W ![]() , Assefa N
, Assefa N ![]() , Baraki N, Wilfong T
, Baraki N, Wilfong T ![]()
Received 21 September 2021
Accepted for publication 26 October 2021
Published 8 November 2021 Volume 2021:14 Pages 7807—7817
DOI https://doi.org/10.2147/IJGM.S338243
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Wogene Negash,1 Nega Assefa,2 Negga Baraki,3 Tara Wilfong3
1Nursing Department, School of Health Science, Madda Walabu University Goba Referral Hospital, Goba, Ethiopia; 2School of Nursing and Midwifery, College of Health and Medical Sciences, Haramaya University, Haramaya, Ethiopia; 3School of Public Health, College of Health and Medical Sciences, Haramaya University, Haramaya, Ethiopia
Correspondence: Wogene Negash Tel +251 917796758
Email [email protected]; [email protected]
Background: Medical malpractice, poor patient outcome and medical suits among health-care workers result from improper consenting practices. Therefore, this study aimed to assess practice and factors associated with the informed consenting process for major surgical procedures among health-care workers in public hospitals of Bale Zone, South Eastern Ethiopia.
Methods: An institutional-based cross-sectional study was conducted from March 9 to 24, 2020, among all nurses, midwives, doctors (general physicians, surgeons, gynecologists), emergency surgery officers, anesthetists) who were working at Bale Zone public hospitals during the study period. A self-administered pretested questionnaire was employed. Variables with a p-value of less than 0.25 (age group, sex, educational profession, working unit, work experience, adequate content of consent form, training on informed consent, policy/regulation in institution, administrative support, average number of patient cared per shift, time spent for consent process, knowledge, attitude) at 95% confidence interval in the binary logistic regression analysis were considered for multivariable regression model to control for possible confounding effect.
Results: Of the total sample size (639 health-care workers), 621 (97.2%) were included in this study, of which 311 (50.1%, 95% CI: 46.1– 53.8) practiced proper informed consent during major surgical procedures. Being age above 35 (AOR: 3.032, 95% CI: 1.148– 8.010), male (AOR: 1.607, 95% CI: 1.047– 2.465), above 10 years of working experience (AOR: 2.339, 95% CI: 1.104– 4.955), adequate content of consent form (AOR: 2.785, 95% CI: 1.772– 4.377), having training on informed consent (AOR: 2.305, 95% CI: 1.204– 4.414), spending more time (> 30minutes) for consent process (AOR: 3.014, 95% CI: 1.095– 8.298), having good knowledge (AOR: 1.808, 95% CI: 1.195– 2.737) and favorable attitude (AOR: 2.188, 95% CI: 1.456– 3.287) were significantly associated with good informed consent practice.
Conclusion: Only half of health-care workers practiced good informed consent. Further emphasis needs to be given to improve consent practice.
Keywords: practice, informed consent, health-care workers, public hospitals
Introduction
Informed consent is the process of communication between a patient and health-care provider that results in the patient’s authorization or agreement to undergo a specific medical intervention.1,2 It is fundamental to proper care and treatment of patients. The patient’s signature on the consent form does not by itself constitute informed consent. Rather, it includes providing the patient with adequate information about their health status, treatment options, benefit, the risks and potential problems associated with the medical or surgical treatment, voluntariness, confidentiality, details on the right to refuse or discontinue, and post-surgery plans.2,3 The Canadian Medical Association outlines that informed consent has become the primary paradigm for protecting patients’ legal rights and guiding the ethical practice of medicine. It is legally and ethically required before proceeding with invasive or high-risk clinical procedures.3
A properly informed consent process is at the heart of shared decision-making, legal requirement, and ethical obligations for all surgical procedures.4 Despite this, it is inconsistently practiced and rarely achieves the theoretical ideal.3 Without a basic understanding of the nature of the procedure, risks, benefits, and treatment alternatives, the patient cannot meaningfully participate in decision-making. This emphasizes proper informed consents’ critical importance to providing safe, quality, patient-centered health care is under-question.5
Different studies in Western (Netherland, UK) and Middle East (Pakistan) countries revealed that the practice of proper surgical informed consent (SIC) among health-care providers was suboptimal and did not meet the minimum standards when they conducted informed consent with patients. These studies found the informed consent process contained incomplete information and often did not ensure their patients’ direct involvement in the process.3,6–9
In the Netherlands, one in six surgeons had a SIC-related complaint, illustrating sub-optimal consenting implementation in daily surgical practice.6 In Iran, only 12.6% of the nurses stated that patients were given sufficient information to assure suitable practice of informed consent.10
In Africa, the practice of proper informed consent is poor. In a study conducted in Egypt, only 50% of the physicians reported that they informed their patients about the planned treatment’s possible complications in detail, while 65.7% of the patients mentioned being not informed at all.11 In Uganda and Nigeria, only 50% and 6% of the surgeons reported obtaining consent with sufficient information prior to each surgical procedure.12,13 Seventeen percent of patients were unaware of the specific surgical procedure they had undergone, and only 24% could identify the performing surgeon.14 Surprisingly, in Ethiopia, only 8.1% of the patients received the minimum required information from an informed consent.15
Failing to obtain proper informed consent is an important cause of medical malpractice litigation, including informed consent allegations, battery, patient injury, improper treatment and surgical site operation, poor outcome and prognosis of the procedure, and indemnity payments. The most common informed consent allegations were failure to explain risks and adverse effects of surgery (30.4%).16 The practice of proper informed consenting is affected by excessive workload, language barriers, the difference in educational levels, cultural difference, patient comprehension, use of disclosed information, autonomy, insufficient time allocation, and how well health-care providers meet the minimal standards for disclosure.3,17
In Ethiopia, little attention has been given to the practice of the informed consent process. There is scarce information on the practice and factors affecting the informed consent process among health-care workers in the study area and even in Ethiopia. Therefore, this study aimed to assess the practice and factors associated with informed consent process for major surgical procedures among health-care workers in public hospitals of Bale Zone, Ethiopia.
Conceptual Framework
Conceptual framework of the study developed from reviewing different relevant literatures (Figure 1).9,18–20
 |
Figure 1 Conceptual framework of the study on practice and factors associated with proper informed consenting process for major surgical procedure among health-care workers in public hospitals. |
Methods and Materials
Study Area and Period
The study was conducted in Bale Zone public hospitals from March 9–24, 2020. Bale Zone is found in the Oromia region, and the administrative town is called Bale Robe, which is located 430 km from Addis Ababa, the capital city of Ethiopia. The five public hospitals were Madda Walabu University Goba Referral Hospital, Bale Robe General Hospital, Ginnir General Hospital, Dellomena General Hospital, and Madda Walabu District Hospital. Six hundred thirty-nine health-care workers (nurses, midwives, doctors (including general practitioners (GPs), surgeons and gynecologists), emergency surgery officers (ESOs) and anesthetists) were working at surgical ward, obstetrics and gynecology ward, operating room, labor ward, intensive care unit (ICU) and emergency outpatient department in all hospitals. Annually, on average, about 5760 patients underwent major surgical procedures.
Study Design
An institutional-based cross-sectional study was employed.
Population
All health-care workers (nurses, midwives, doctors (GPs, surgeons, gynecologists), ESOs, anesthetists) who were working at Bale Zone public hospitals were the source population. All health-care workers who were working in Bale Zone public hospitals during the study period were the study population.
Eligibility Criteria
All health-care workers (nurses, midwives, doctors, ESOs and anesthetists) who worked at least 6 months in the hospital were included. Health-care workers who were on annual leave, sick leave or training were excluded from the study. Those who had not been working in surgical, labor, obstetrics and gynecology ward, operating room, ICU and emergency OPD for the last 1 year were excluded as they have less exposure to patients who had undergone surgery.
Sample Size Determination
The sample size was determined by using single population proportion formula considering the proportion of informed consent practice (p=50%), since there were no published studies of similar study population in our country (95% confidence interval and 5% margin of error).
n = (Zα/2)2p (1-p)/d2
n= (1.96)2*0.50(1–0.50)/(0.05)2
n = 384
Where:
n = sample size required
Zα/2 = critical value at 95% level of confidence on normal distribution curve (95%=1.96)
P = estimated proportion of practice of proper informed consenting process
d = margin of error (5%=0.05).
By adding a ten percent nonresponse rate (39), the total sample size for the first objective was 423. Based on the type of hospital (ie, district, general, or referral), there was clustering, and the design effect was considered. Hereafter, by multiplying the calculated sample size by 1.5, the final sample size was 635.
Sampling Procedure
There are five public hospitals in Bale Zone. Hospitals were clustered into referral hospitals, general hospitals, and district hospitals. The total number of health-care workers (nurses, midwives, doctors, ESOs, and anesthetists) was 639, found in the surgical ward, OR, emergency OPD, labor ward, obstetrics and gynecology ward, and ICU. Specifically, 298, 105, 92, 84, and 60 aforementioned professions were found in Madda Walabu University Goba Referral Hospital, Bale Robe General Hospital, Ginnir General Hospital, Dellomena General Hospital, and Madda Walabu District Hospital, respectively. Proportional allocation to sample size was made for each hospital. The study population (639) was almost equal to the calculated sample size (635), which is very small to apply probability randomization methods. Hence, census was conducted on all study population who fullfilled the inclusion criteria and were present at data collection time.
Data Collection Methods
A pretested structured self-administered English version questionnaire was used to collect data on the practice and factors affecting the informed consent process. The questionnaire was adopted and modified from the Professional and Clinical Standards of the Royal College of Surgeons (RCS) of the UK, South Africa, Uganda, FMOH, and EMA.1,12,21–23 The questionnaire was prepared in English and had five parts. Part I: Socio-demographic characteristics of the study participants. Part II: Organizational factors that affect practice of informed consent. Part III: respondents’ knowledge of the informed consent process. Part IV: respondents’ attitude toward the practice of informed consent, which contained questions with responses which ranged from strongly disagree to strongly agree. Part V: assessed the respondents’ practice of the informed consent process, and the questions contained response options of “never”, “sometimes” and “always” (Supplementary Table 1). Data were collected by eight BSc nurses with five supervisors who participated to coordinate, facilitate, and supervise the overall activities during the data collection period. They were recruited out of the study sites. Data collectors were assigned in each hospital to distribute and collect back the questionnaire from study participants.
Variables
Dependent Variable
Informed consent practice.
Independent Variables
Socio-demographic characteristics (age, sex, educational profession, work-experience, language barriers).
Organizational factors (lack of standard consent form, in-service training, time constraint, lack of administrative support (like interpreters available), workload, working unit, and lack of policy or regulation in institution).
Health-care worker–related factors (knowledge, attitude).
Operational Definitions
The practice of informed consent was measured using 13 structured Likert-type questions having options of “never”, “sometimes” and “always” which scored as 1, 2 and 3, respectively. The total score for practice was dichotomized into good and poor practice using the median score as the cut-off point. Good practice: A score greater or equal to the median score for the practice questions. Poor practice: A score below the median score for the practice questions.
Knowledge of informed consent practice was measured using 10 structured knowledge questions with multiple options, totally 13 items having “yes”, “no” and “I don’t know” which was scored as 1 for correct answer and 0 for incorrect answer. The total score for knowledge was dichotomized into good knowledge and poor knowledge using the median score as the cut-off point. Good knowledge: A score greater or equal to the median score for the knowledge questions. Poor knowledge: A score below the median score for the knowledge questions.
Attitude toward the proper informed consent process was measured by using 09 Likert type attitude questions. A score of 1, 2, 3, 4 and 5 was given for strongly disagree, disagree, neutral, agree and strongly agree responses, respectively. The total score for attitude was dichotomized into favorable and unfavorable attitude using the median score as the cut-off point.
Data Quality Control
The questions were adopted and modified from international professional and clinical standard guidelines, and reviewed literature. Pretests were performed on 32 (5%) participants in Dodola Hospital before the actual data collection period to assure the data collection tool’s quality. The collected pre-test data were entered into Epi Data Version 3.1 software to check reliability and internal consistency. Exception to socio-demographic, all variables had Cronbach’s alpha test result greater than 0.72. Data collectors were recruited from out of the study area to minimize bias. The Principal Investigator trained data collectors and supervisors regarding the study’s aim, and clarification of instruments. Regular supervision and immediate feedback were done by the trained supervisors. The collected data were checked for completeness and consistency before data entry into the software. The data were entered into the software for analysis and coding. Double data entry into Epi data version 3.1 was performed by two data clerks.
Method of Data Processing and Analysis
The collected data were checked for completeness and consistency, coded and entered into Epi Data Version 3.1 software and exported into Statistical Package for the Social Sciences (SPSS window version 25) for analysis. Data were explored and cleaned prior to analysis using SPSS. The frequency, percentage, median and standard deviations were employed to describe the study population and the results were presented by text, tables and figures. In binary logistic regression analysis, crude odds ratio with 95% CI was carried out to determine the significant relationship of each independent variable with the practice of informed consent. Variables with a p-value of less than 0.25 at 95% confidence interval in the binary logistic regression analysis were considered for multivariable regression model to control for confounder variables. Multi collinearity was checked. Hosmer–Lemeshow goodness-of-fit was computed to check for model fitness. Omnibus test was significant (p-value <0.0001) and Hosmer–Lemeshow’s test was insignificant (p-value = 0.258). Variables with p-value <0.05 from multivariate analysis were declared as statistically significant. Therefore, variables with p-value <0.05 and 95% CI (which does not include null value) were reported as having a statistically significant association with informed consent practice.
Ethical Consideration
Ethical clearance was obtained/the proposal was approved by Haramaya University, College of Health and Medical Sciences, Institutional Health Research Ethics Review Committee (IHRERC). A formal letter of permission was provided to Bale Zone Health Bureau from Haramaya University. Informed, voluntary, written, and signed consent was obtained from each of the hospital heads and each participating health-care worker. Participants were told their confidentiality would be maintained, and they had the right to refuse to answer the questionnaires and stop or withdraw at any time during data collection. Confidentiality was maintained. The research review and follow-up are in agreement with the principles of the Helsinki declaration.
Results
Socio-Demographic Characteristics of the Respondents
Out of the total sample size (639), 621 study participants successfully participated in this study, with a response rate of 97.2%. This might be due to the aims, benefit, and significance of the study were clearly stated on participants’ consent sheet, and the trained data collectors were assigned in each hospital to distribute the questionnaire to the study participants. Finally, after a while they collect back the questionnaire as soon as they completed. The respondents’ median age was 29 years (+5.69 SD), ranging from 21 to 56 years. More than half, 364 (58.6%) of the respondents were male, and almost half, 301 (48.5%) were married. About half 287 (46.2%) were nurses. More than half, 325 (52.3%) of the respondents had 5 years and less working experience, and almost half, 314 (50.6%), were able to communicate with their patients without challenges (language barrier during communication) (Table 1).
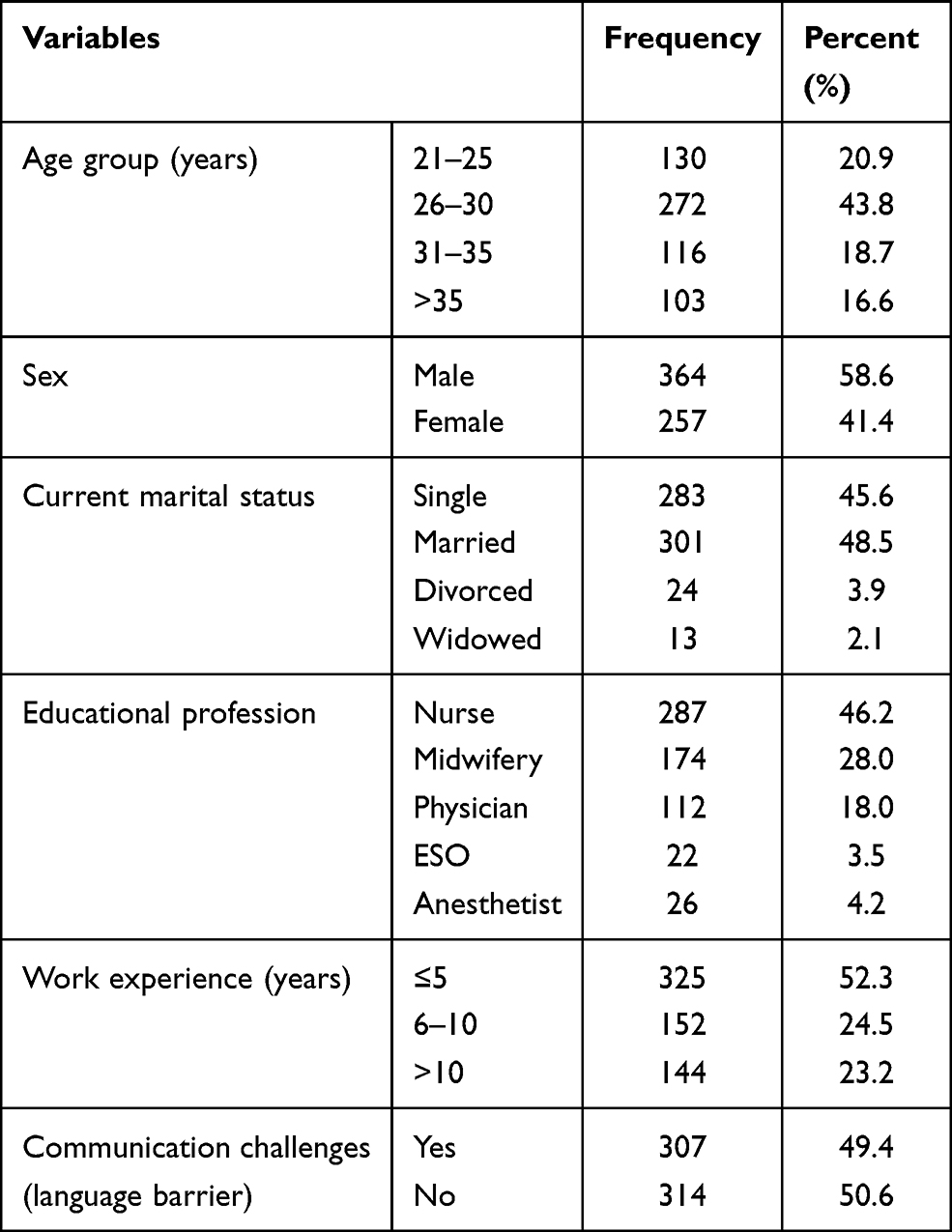 |
Table 1 Socio-Demographic Characteristics of Study Population in Bale Zone Public Hospitals, South Eastern Ethiopia, 2020 (n=621) |
Organizational Factors
One-fifth, 124 (20.0%) of the respondents were working in the surgical ward. Less than half, 266 (42.8%) of the study participants reported that the contents of the informed consent form are adequate to obtain valid consent, and less than one-fourth, 140 (22.5%) had attended in-service training on the surgical informed consent process. Almost half, 310 (49.9%) reported that there is a policy or regulation that supports the practice of informed consent in their institution, and 239 (38.5%) had utilized administrative support (like interpreters available). Two hundred seventy (43.5%) of the participants had provided care for more than ten patients in an average shift, and one-third spent 5–10 minutes to provide information to their patients about the procedure during the professional encounter (Table 2).
 |
Table 2 Organizational Factors on Practice of Informed Consent Process Among Health-Care Workers in Bale Zone Public Hospitals, South Eastern Ethiopia, 2020 (n=621) |
Knowledge and Attitude of Health-Care Workers About the Informed Consent Process
The median score of study participants’ knowledge was nine, and almost half, 323 (52%, 95% CI: 48.3–56.0), had good knowledge about the informed consent process (Figure 2A).
 |
Figure 2 Knowledge, Attitude and Practice of informed consent. (A) Knowledge of informed consent process. (B) Attitude of health-care workers towards informed consent process. Red color represent unfavorable attitude and the green color represent favorable attitude. (C) Practice of informed consent process among health-care workers in Bale Zone Public Hospitals, South Eastern Ethiopia, 2020 (n=621). |
The median score of study participants’ attitude was 33, and more than half, 360 (58%, 95% CI: 53.9–62.0), had a favorable attitude towards the informed consent process (Figure 2B).
Practice of Informed Consent Process
More than half, 343 (55.2%) of the respondents reported that they always obtained informed consent for major surgical procedures, and nearly two-thirds, 371 (59.7%), reported they always informed the reason/indication for surgery. Less than half, 268 (43.2%), always informed the patients about the presence/absence of treatment options. More than one-third, 239 (38.5%), reported they always discussed the risk/potential complications of the procedure. Less than one-third 171 (27.5%) of participants discussed the presence of any favorable environment and the possibility to say no to the proposed surgery (Table 3). The median score of study participants’ informed consent practice was 30, and almost one-half, 311 (50.1%, 95% CI: 46.1–53.8) had good practice towards the informed consent process (Figure 2C).
 |
Table 3 Practice of Informed Consent Process Among Health-Care Workers in Bale Zone Public Hospitals, South Eastern Ethiopia, 2020 (n=621) |
Factors Associated with Informed Consent Process
Bivariate logistic regression analysis revealed that male sex, age above 35 years, above 10 years of working experience, adequate content of consent form (standardized format), presence of policy/regulations in the institution, administrative support, training, time spent more than 30 minutes, good knowledge and favorable attitude had a statistically significant positive association with informed consent practice. In multivariate logistic regression analysis, age above 35, male, more than 10 years of working experience, adequate contents of consent form, training, time spent, knowledge and attitude were statistically, and positively associated with informed consent practice (Table 4).
 |
Table 4 Factors Associated with Informed Consent Practice Among Health-Care Workers in Bale Zone Public Hospitals, South Eastern Ethiopia, 2020 (n=621) |
Discussion
In this study, the practice and factors associated with the informed consent process were assessed, the results showed that only half, 311 (50.1%), of the health-care providers practiced adequate informed consent. Obtaining proper informed consent from patients represents the practical application of patient-health-care provider’s interactive approach, respecting patient autonomy, and indicated that consenting is not just a form to be signed.2 Our study showed that the current informed consent practice in Ethiopia is minimal. In this study, 55.2% of the respondents always obtained informed consent for major surgical procedures. This finding is lower than the 71% found in Italy’s study.19 The possible explanation might be due to the extensive study area coverage; five hospitals in different districts were included in this study, which may vary in nature of patient flow, clinicians’ experience, and standards of hospitals as compared to the study conducted in single institution. Also, the difference in socio-economic status, ie, Italy is not a low- and middle-income country (LMIC). This might be due to demand and supply (health-care workforce particularly, surgeons) were further disproportionate in which one surgeon obligated to treat so many patients, which affected the quality of informed consent. Also, the majority of health-care users were illiterate; rely on clinicians decision that leads to paternalistic approach. It is higher than the study in Uganda, which found 48.8% informed consent practice.12 This discrepancy might be due to the small sample size used in Uganda and the difference in data collection.
In this study, only 27.9% of the respondents always informed the patients about type of anesthesia to be used. This finding was congruent with the study conducted in Hawassa, Ethiopia, where the majority of respondents were not informed about the type of anesthesia to be used.24 The possible explanation might be in our country, where the workforce of physician's, especially surgeon’s, is scarce, the nurses were obtained informed consent even though they were not treating patients with anesthesia. Slightly, more than half (56.2%) of the respondents always informed about the benefits of the surgery in this study. This finding was in line with the study conducted in Addis Ababa, which revealed half (55.6%) of the patients knew the benefits of the surgery.15
In this study, the health-care workers who had good knowledge of informed consent were more likely to practice adequate informed consent than those who had poor knowledge. This finding was supported by the study conducted in Pakistan.7 This might be because knowing the informed consenting process helps integrate each component of consent into practice quickly and thoughtfully. It is a fact that without the basic understanding of the elements of the consenting process, the approach of informed consent will not be optimal.6 Similarly, those with favorable attitudes toward informed consent practice were more likely to practice adequate informed consent than those with unfavorable attitudes. This finding is comparable with the study in Pakistan.7 The possible explanation might be that a favorable attitude towards informed consent practice is fundamental and enhances motivation for practice.
Adequate informed consent practice was higher among health-care workers who had training on consenting than those with no training. This is consistent with another study in the Hawassa,25 and the USA.26 Training can update, boost, clarify and advance existing knowledge and practices as it comprises the components of informed consent, patient autonomy, and patient-centered care. The odds of informed consent practice were higher in institutions with adequate contents of the informed consent form (standardized format) than those without a standardized format. This finding is congruent with the nationally recommended consent form contents.21,22 This might be due to standardized consent form that helps the health-care providers as a guideline to follow and practice each component that should be disclosed to the patient.
Health-care providers who spend more time (>30minutes) on the consenting process were more likely to practice adequate consent than those who spent less than 5 minutes. This finding is in line with South African studies (Aderibigbe & Chima, 2019) and Pakistan.17 The extra time spent for consenting allows more discussion and interaction between patient-health-care providers and adequate time to address patient issues. Work experience was positively associated with adequate practice of informed consent. Respondents who had more than 10 years’ of work experience were more likely to practice adequate informed consent than those who had less than or equal to years’ work experience. This finding is consistent with a study from Italy.19 The experience provides health-care providers with the advantages to recognize and understand the consequences of failure to obtain consent, master their practice, and have training opportunities. Male participants had higher odds of practicing adequate informed consent than females. This finding is congruent with the study in Italy19 and may be due to the large proportion of male health-care providers as compared to females.
In this study, health-care providers above 35 years old were more likely to practice informed consent than those aged 21–25 years. This finding is in line with the study conducted in Italy.19 This may be explained as age increases, their work experience increases, increasing exposure to training and shared experience. As a result, health-care workers increase their knowledge and attitude, leading to improved informed consent practice.
In this study, all study population were included, which is more accurate to get real data as each member is surveyed. Also, it assessed the current overall practice level of informed consenting process since there were no studies investigated before on the title under study in our country. There might be recall bias and inflated informed consent practice level related to social desirability bias since it is self-reported. However, it was minimized by explaining the purpose of the study for the respondents. Although the clinicians were enrolled from five hospitals found in different districts, due to census employed, it might not be generalized nationwide. Also, since the study was cross-sectional, it does not show a cause–effect relationship.
Conclusion and Recommendation
Only half of the health-care workers practiced adequate informed consent. Knowledge, attitude, training, adequate contents of consent form (standardized format), time spent for the consenting process, working experience, sex, and age of the health-care workers had a statistically significant positive association with the informed consent practice. In conclusion, informed consent practice is low and still looks as it is theoretical ideal, which needs more emphasis. Therefore, it is better if emphasis should be given towards standardizing the consent format like the current international and national recommended consent format, provide periodic in-service training for health-care providers on the consent process and each component that should be incorporated, activities to enhance the health-care providers’ attitude, and knowledge. Finally, future studies should include observational studies for improved validity and more robust evidence on informed consent practice.
Abbreviations
ACOG, American College of Obstetrics and Gynecology; AMA, American Medical Association; CI, confidence interval; COR, crude odds ratio; EMA, Ethiopian Medical Association; ESOs, Emergency surgery officers; FMOH, Federal Ministry of Health; ICU, intensive care unit; OPD, outpatient department; SIC, surgical informed consent; USA, United States of America.
Acknowledgments
The author expresses special thanks to Madda Walabu University, Haramaya University, study participants, data collectors, and supervisors. Finally, the author’s heartfelt thanks go to his beloved family for their generous support and all his friends who helped him clarify his doubts during this thesis writing.
Author Contributions
All authors contributed to designing the study, developing the proposal, data analysis, drafting or revising the article, have agreed on the journal to which the article was submitted, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Funding
Madda Walabu University funded the data collection for this research but had no role on the outcome of the study.
Disclosure
The authors declare that they have no conflicts of interest for this work.
References
1. Royal College of Surgeons of England. Consent supported decision making. A guide to good practice; 2018:1–20.
2. Farmer L, Lundy A. Informed-consent: ethical and legal considerations for advanced practice nurses. J Nurse Pract. 2017;13(2):124–126. doi:10.1016/j.nurpra.2016.08.011
3. Hall DE, Prochazka AV, Fink AS. Informed consent for clinical treatment: figure 1. Can Med Assoc J. 2012;184(5):533–540. doi:10.1503/cmaj.112120
4. Murray B. Informed consent: what must a physician disclose to a patient? AMA J Ethics. 2012;14(7):563–566.
5. Schenker Y, Meisel A. Informed consent in clinical care: practical considerations in the effort to achieve ethical goals. JAMA. 2011;305(11):1130–1131. doi:10.1001/jama.2011.333
6. Leclercq WK, Keulers BJ, Houterman S, Veerman M, Legemaate J, Scheltinga MR. A survey of the current practice of the informed consent process in general surgery in the Netherlands. Patient Saf Surg. 2013;7(4):2–7. doi:10.1186/1754-9493-7-4
7. Ashraf B, Tasnim N, Saaiq M, Zaman KU. An audit of the knowledge and attitudes of doctors towards Surgical Informed Consent (SIC). Int J Health Policy Manag. 2014;3(6):315–321. doi:10.15171/ijhpm.2014.109
8. Spatz ES, Krumholz HM, Moulton BW. The new era of informed consent: getting to a reasonable-patient standard through shared decision making. JAMA. 2016;315(19):2063–2064. doi:10.1001/jama.2016.3070
9. Akyuz E, Bulut H, Karadag M. Surgical nurses’ knowledge and practices about informed consent. Nurs Ethics. 2019;12:1–13.
10. Moeini S, Shahriari M, Shamali M. Ethical challenges of obtaining informed consent from surgical patients. Nurs Ethics. 2020;27:527–536.
11. Yasmine GS. Knowledge, practice and perception towards the informed consent process among physicians and patients in General Surgical Departments at Cairo University Hospitals. Egypt J Community Med. 2016;34(2):1–17.
12. Ochieng J, Ibingira C, Buwembo W, et al. Informed consent practices for surgical care at university teaching hospitals: a case in a low resource setting. BMC Med Ethics. 2014;15(40):1–5. doi:10.1186/1472-6939-15-40
13. Ogundiran TO, Adebamowo CA. Surgeons’ opinions and practice of informed consent in Nigeria. J Med Ethics. 2010;36(12):741–745. doi:10.1136/jme.2010.037440
14. Ochieng J, Buwembo W, Munabi I, et al. Informed consent in clinical practice: patients’ experiences and perspectives following surgery. BMC Res Notes. 2015;8(1):765. doi:10.1186/s13104-015-1754-z
15. Chane W, Birhanu B, Suga Y. Quality of informed consent among patients who underwent major surgical procedure in a Tertiary Care Hospital, Addis Ababa, Ethiopia. Open Access Surg. 2020;13:27. doi:10.2147/OAS.S250532
16. Grauberger J, Kerezoudis P, Choudhry AJ, et al. Allegations of failure to obtain informed consent in spinal surgery medical malpractice claims. JAMA Surg. 2017;152(6):e170544. doi:10.1001/jamasurg.2017.0544
17. Jahan F, Roshan R, Nanji K, Sajwani U, Warsani S, Jaffer S. Factors affecting the process of obtaining informed consent to surgery among patients and relatives in a developing country: results from Pakistan. East Mediterr Health J. 2014;20(9):569–577. doi:10.26719/2014.20.9.569
18. Chima S Language as a barrier to informed consent and patient communications in South African hospitals-a working paper.
19. Ingravallo F, Gilmore E, Vignatelli L, et al. Factors associated with nurses’ opinions and practices regarding information and consent. Nurs Ethics. 2014;21(3):299–313. doi:10.1177/0969733013495225
20. Gupta VV, Bhat N, Asawa K, Tak M, Bapat S, Chaturvedi P. Knowledge and attitude toward informed consent among private dental practitioners in Bathinda city, Punjab, India. Osong Public Health Res Perspect. 2015;6(2):73–78. doi:10.1016/j.phrp.2014.12.005
21. Federal Democratic Republic of Ethiopia Minister of Health. National compassionate, respectful and caring training participant manual; 2017:35–37.
22. Ethiopian Medical Association. Medical ethics for doctors in Ethiopia; 2010:7–9.
23. Chima S An investigation of informed consent in clinical practice in South Africa; 2018:659–662.
24. Teshome M, Wolde Z, Gedefaw A, Tariku M, Asefa A. Surgical informed consent in obstetric and gynecologic surgeries: experience from a comprehensive teaching hospital in Southern Ethiopia. BMC Med Ethics. 2018;19(1):38. doi:10.1186/s12910-018-0293-2
25. Teshome M, Wolde Z, Gedefaw A, Asefa A. Improving surgical informed consent in obstetric and gynaecologic surgeries in a teaching hospital in Ethiopia: a before and after study. BMJ Open. 2019;9:e023408.
26. Thompson BM, Sparks RA, Seavey J, et al. Informed consent training improves surgery resident performance in simulated encounters with standardized patients. Am J Surg. 2015;210(3):578–584. doi:10.1016/j.amjsurg.2014.12.044
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.