Back to Journals » Advances in Medical Education and Practice » Volume 17
Practice and Effectiveness Analysis of Multimodal Integrated Teaching Methods in Neurosurgery Clinical Teaching
Authors Xia D ![]() , Hu Z, Yuan J, Wu D, Lai N, Jin Y
, Hu Z, Yuan J, Wu D, Lai N, Jin Y
Received 19 February 2026
Accepted for publication 15 May 2026
Published 27 May 2026 Volume 2026:17 600232
DOI https://doi.org/10.2147/AMEP.S600232
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Md Anwarul Azim Majumder
Dayong Xia,1 Zhengqing Hu,1 Jinlong Yuan,1 Degang Wu,1 Niansheng Lai,1 Yuelong Jin2
1Department of Neurosurgery, The First Affiliated Hospital of Wannan Medical University (Yijishan Hospital of Wannan Medical University), Wuhu, Anhui, 241001, People’s Republic of China; 2School of Public Health, Wannan Medical College, Wuhu, Anhui, 241002, People’s Republic of China
Correspondence: Yuelong Jin, School of Public Health, Wannan Medical University, Wuhu, Anhui, 241002, People’s Republic of China, Email [email protected]
Objective: To explore the application effectiveness of a multimodal-integrated teaching method combining case-based learning, scenario simulation teaching, and the flipped classroom in neurosurgery education.
Methods: Sixty resident physicians undergoing standardized training in the Department of Neurosurgery at The First Affiliated Hospital of Wannan Medical College from January 2024 to December 2025 were selected as the study subjects. Thirty trainees were taught using the multimodal integrated teaching method (study group), while the other thirty received traditional teaching methods (control group). A diversified evaluation system was used to compare the teaching effectiveness between the two groups.
Results: The study group showed higher satisfaction with the teaching arrangement compared to the control group. Students in the study group also achieved higher scores in surgical skill operation, theoretical knowledge assessment, and had a higher pass rate in case analysis ability than those in the control group. Furthermore, the study group outperformed the control group across all three dimensions of the self-benefit comprehensive questionnaire.
Conclusion: The multimodal integrated teaching method demonstrates significant teaching advantages and effectiveness, warranting further promotion in neurosurgery clinical practice teaching.
Keywords: neurosurgery, case-based learning, scenario simulation, flipped classroom, application effectiveness
Introduction
Neurosurgical diseases are characterized by acute onset, rapid progression, complex anatomical structures, and high surgical risks, placing extremely high demands on the professional competence of practitioners. From foundational knowledge of cranial anatomy and neurophysiology to the diagnosis and treatment of complex cerebrovascular diseases and surgical techniques for brain tumors, and further to emergency management of conditions like cerebral herniation and severe craniocerebral trauma, learners are required to possess solid theoretical foundations, clear clinical reasoning, and proficient operational skills.1 However, traditional teaching models remain prevalent in current neurosurgery education: instructors primarily deliver knowledge points via PowerPoint presentations and blackboard writing in the classroom, supplemented by limited case image displays. The practical component often relies on observation in the operating room or animal experiments, with few opportunities for students to perform hands-on operations themselves. Under this model, students often resort to rote memorization of knowledge points, struggling to effectively bridge theory with clinical practice. They frequently face dilemmas such as “understanding theory but unable to perform operations” or “knowing the diagnosis but finding decision-making difficult” when confronted with real cases.2 With the deepening of medical education reform, the student-centered teaching philosophy is gradually replacing the traditional teacher-centered model, emphasizing the enhancement of student engagement and comprehensive abilities through interactive and immersive learning. Case-based learning guides students in problem analysis using real cases, scenario simulation teaching hones practical skills through simulated environments, and the flipped classroom restructures the teaching process via “pre-class self-learning + in-depth classroom interaction”. The integration of these three approaches provides a novel strategy to address the pain points in neurosurgery teaching.3,4 This study aims to systematically evaluate the application effectiveness of this multimodal integrated teaching method, offering a reference for the reform of neurosurgery education.
Materials and Methods
Research Subjects
Sixty resident physicians undergoing standardized training in the Department of Neurosurgery at The First Affiliated Hospital of Wannan Medical College from January 2024 to December 2025 were selected as the study subjects. Standardized residency training is a mandatory pathway for every medical student to become a clinical physician. According to the Content and Standards for Standardized Residency Training, such training emphasizes the development of core competencies including professionalism, communication skills, and humanistic care, with volunteer service regarded as an important supplement to the “second classroom”. All participating physicians had completed their basic and preclinical medical coursework, possessed a certain foundation of medical knowledge, and had received no specialized teaching or training in neurosurgery prior to this study. They were randomly divided into a study group and a control group using a random number table, with 30 participants in each group. Both the study group and the control group consisted of 27 male and 3 female participants, and all subjects agreed to participate in this study and signed informed consent forms. A pre-course test was administered to both groups before starting the rotation. A comparison of baseline data, including the pre-test results, showed no statistically significant differences between the two groups (P > 0.05), indicating good comparability, as detailed in Table 1.
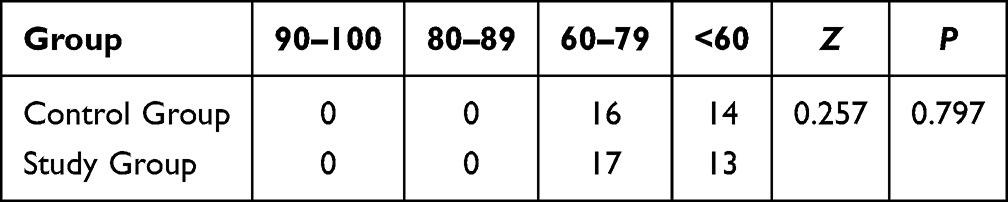 |
Table 1 Comparison of Pre-Test Results Between the Two Groups (n=30) |
Comparison of Pre-Test Results Between the Two Student Groups
The results showed that there was no statistically significant difference in the pre-test comparison between the two groups of students (P > 0.05), as detailed in Table 1.
Teaching Implementation
The same group of instructors, comprising attending neurosurgeons or those with higher professional titles, taught both student groups. The teaching content was unified, covering the diagnosis, differential diagnosis, treatment principles, and related operational skills (eg, lumbar puncture, basic craniotomy procedures) for common neurosurgical diseases such as cerebral hemorrhage, brain tumors, and craniocerebral trauma.
Control Group (Traditional Teaching Method)
This group followed the traditional “theoretical lecture + observational practice” model.
Theoretical Teaching
Instructors systematically explained neurosurgical anatomy, physiological fundamentals, etiology, clinical manifestations, auxiliary examinations, diagnostic criteria, and treatment plans for common diseases using PowerPoint presentations, supplemented by illustrations with typical case images. Textbook exercises were assigned after class for consolidation.
Practical Teaching
Students were arranged to observe relevant skill demonstrations and surgical procedures, watch instructional videos on neurosurgical operations, and practice basic procedures like lumbar puncture in a simulation lab with instructors providing brief guidance.
Study Group (Multimodal Integrated Teaching Method)
Based on the same teaching content and duration, this group utilized a combined model of case-based learning, scenario simulation, and the flipped classroom. The specific implementation process was as follows:
Pre-Class Preparation (Flipped Classroom Foundation)
One week in advance, instructors provided students with learning objectives, key knowledge points, and extended reading materials (eg, latest guidelines, literature on typical cases) for self-study. Preview test questions focusing on foundational theory were also assigned. Students were required to independently watch videos, read materials, complete the test, and record any questions arising during their study. Questions were summarized by study groups (5 students per group) and submitted to the instructor.
In-Class Implementation
Case Discussion (Case-Based Learning)
The instructor selected 1–2 typical cases (eg, “hypertensive intracerebral hemorrhage”, “transtentorial herniation”), presenting patient history, physical examination findings, imaging data, and initial treatment plans. Student groups discussed questions such as “What is the basis for the diagnosis?”, “Which diseases require differential diagnosis?”, and “How should the next treatment plan be formulated?”. Each group selected a representative to present their discussion. The instructor guided the discussion on contentious points, ultimately synthesizing a complete diagnostic and therapeutic reasoning process.
Scenario Simulation (Scenario Simulation Teaching)
Practical teaching was conducted in a simulated ward/operating room, featuring three scenarios: “Emergency Reception of a Craniocerebral Trauma Patient” (Simulated using standardized patients presenting with impaired consciousness and scalp hematoma; students were required to perform history-taking, Glasgow Coma Scale scoring, and request a head CT). “Lumbar Puncture Procedure” (Simulated on a model; students had to perform strict aseptic technique, with instructors providing real-time correction of hand movements). “Emergency Management of Cerebral Herniation” (Simulating monitor readings showing dropping blood pressure and slowed heart rate; students needed to quickly assess the situation and perform interventions like administering dehydrating agents or simulating ventricular puncture). Following each scenario, the instructor provided feedback, using video playback when available, to highlight key procedural points and areas for improvement.
Q&A and Summary
The instructor addressed common questions raised by students before class and those exposed during case discussions and simulations. Finally, the instructor summarized the logical framework of the knowledge points, emphasizing key points (eg, early recognition of cerebral herniation) and difficult aspects (eg, hemostasis techniques in craniotomy).
Post-Class Reinforcement
Each student group was tasked with independently searching for and analyzing one similar case based on the classroom discussion, submitting a written report within one week. The instructor graded and provided feedback on these reports for student review and consolidation.
Evaluation Indicators and Methods
Upon completion of the teaching period, a diversified evaluation system was used to compare the teaching effectiveness between the two groups.
Theoretical Knowledge Assessment
A closed-book exam covering foundational theory, disease diagnosis, and treatment principles was administered (100 points total, 90 minutes duration).
Clinical Skill Operation Assessment
Three practical skills were assessed: ① Lumbar Puncture (30 points); ② Craniotomy Incision Design and Hemostasis Simulation (40 points); ③ Initial Assessment and Management of a Craniocerebral Trauma Patient (30 points).
Case Analysis Ability
Students were provided with one complex case and required to complete diagnosis, differential diagnosis, and treatment plan formulation within 30 minutes. Instructors scored based on “Diagnostic Accuracy (40 points)”, “Logical Clarity (30 points)”, and “Plan Rationality (30 points)”. A score ≥60 was considered a pass, and the pass rate was calculated.
Teaching Satisfaction
A questionnaire collected student evaluations of the teaching method, including five items such as “Does it help in understanding knowledge points?”, “Does it improve practical ability?”, and “Are you willing to continue using this method?”. A four-level scale (“Very Satisfied”, “Satisfied”, “Neutral”, “Dissatisfied”) was used. Satisfaction rate = (Number of “Very Satisfied” + Number of “Satisfied”) / Total number × 100%.
Comprehensive Self-Perceived Benefit Questionnaire
A self-designed questionnaire was used for effect analysis across three dimensions: 1) Whether the understanding of the neurosurgery specialty had improved; 2) Whether it was helpful for future learning and work; 3) Whether implementing the multimodal integrated teaching method was considered necessary.
Statistical Methods
All data collected in this study were analyzed using SPSS 26.0 statistical software. Categorical data were expressed as counts (n). Inter-group comparisons were performed using the chi-square test and the Mann–Whitney U-test. A P-value < 0.05 was considered statistically significant. For the primary outcome measures (theoretical knowledge assessment and clinical skill operation scores), post-hoc power analysis was performed and Cohen’s d was calculated as the effect size. With α=0.05 and a sample size of 30 per group, a moderate-to-large effect size (Cohen’s d ≥ 0.5) would yield a statistical power of approximately 0.80–0.85. The actual Cohen’s d values were 0.85 for skill operation scores and 0.79 for theoretical knowledge scores, both indicating large effect sizes, with corresponding power values around 0.85. These results suggest that the sample size was adequate to detect group differences.
Results
Comparison of Neurosurgical Skill Operation and Theoretical Knowledge Assessment Between the Two Groups
The results showed that the study group performed significantly better than the control group in both neurosurgical skill operation and theoretical knowledge assessment (P < 0.001). Details are presented in Table 2.
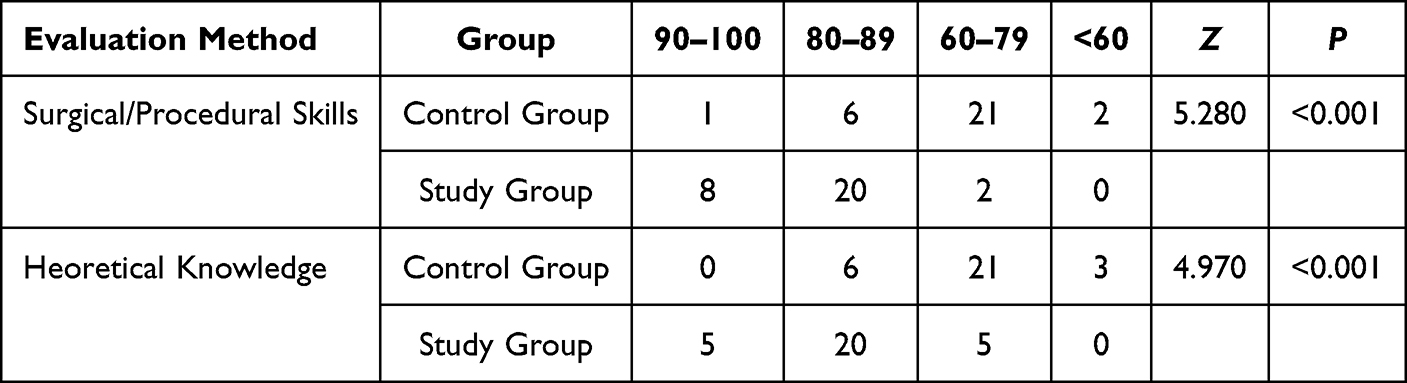 |
Table 2 Comparison of Neurosurgical Skill Operation and Theoretical Knowledge Assessment Between the Two Groups (n=30) |
Comparison of Case Analysis Ability Qualification Rates Between the Two Groups
The results showed that the case analysis ability qualification rate in the study group was significantly higher than that in the control group (P < 0.05), as detailed in Figure 1.
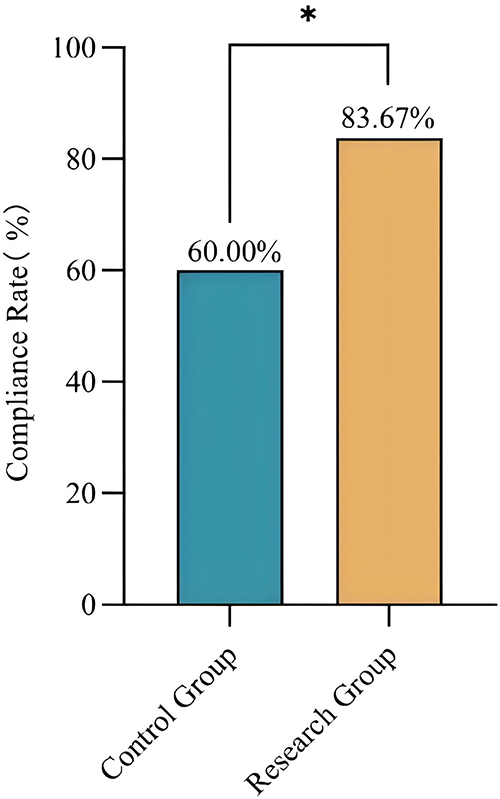 |
Figure 1 Comparison of Case Analysis Ability Qualification Rates Between the Two Groups (n=30, χ2=5.455, P=0.020), * p<0.05. |
Comparison of Teaching Satisfaction Between the Two Groups
The results showed that the teaching satisfaction rating in the study group was significantly higher than that in the control group (P < 0.001), as detailed in Figure 2.
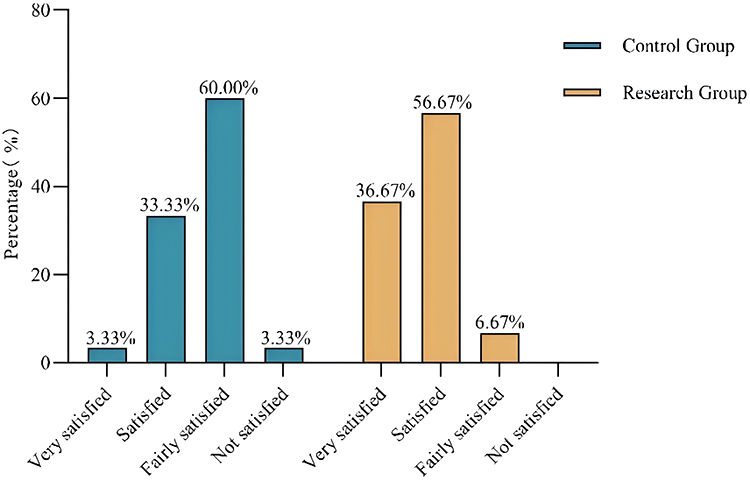 |
Figure 2 Comparison of Teaching Satisfaction Between the Two Groups (n=30, P<0.001). |
Comparison of the Comprehensive Self-Perceived Benefit Questionnaire Between the Two Groups of Students
The results showed that the study group outperformed the control group across all three dimensions of the comprehensive self-perceived benefit questionnaire (P < 0.05). Details are presented in Table 3.
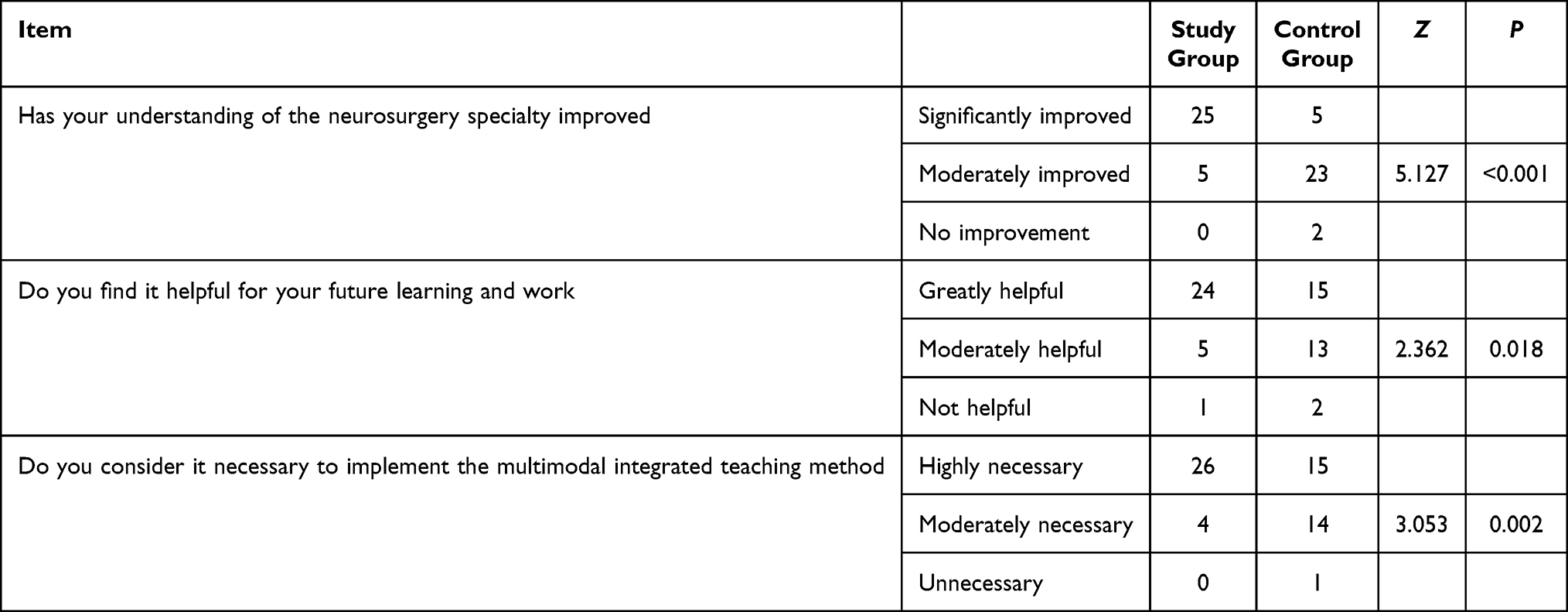 |
Table 3 Comparison of the Comprehensive Self-Perceived Benefit Questionnaire Between the Two Groups of Students (n=30) |
Comparison of Various Evaluation Indicators Between the Two Student Groups. After the teaching intervention, the study group demonstrated significantly superior performance compared to the control group across all evaluated indicators: theoretical knowledge assessment, clinical skill operation, case analysis ability qualification rate, teaching satisfaction, and the comprehensive self-perceived benefit questionnaire. The differences were all statistically significant (P < 0.05).
Discussion
The core objective of neurosurgery education is to cultivate students’ comprehensive capabilities encompassing “theoretical understanding, practical skill proficiency, and adept critical thinking”.5 The integrated model combining case-based teaching, scenario simulation, and the flipped classroom adopted in this study, through its closed-loop design of “pre-class self-directed learning, in-class interactive practice, and post-class extended application”, effectively overcomes the limitations inherent in traditional teaching methods. This approach strengthens the connection between theory and practice. Case-based teaching uses real patient cases as a link, integrating disparate knowledge points (such as anatomy, pathology, and treatment) into a coherent diagnostic and therapeutic chain.6,7 For instance, in the “hypertensive intracerebral hemorrhage” case, students must analyze the relationship between the hemorrhage location and limb hemiplegia based on the anatomical features of the basal ganglia region, and determine whether the hemorrhage volume visible on CT scans meets surgical intervention criteria. This “from case to knowledge” reverse learning approach is more conducive to forming deep memory than rote memorization of textbooks.3 The significantly higher theoretical knowledge assessment scores in the study group confirm this method’s role in promoting knowledge internalization. It enhances the proficiency and standardization of clinical skills. Scenario simulation provides students with a “safe space for trial and error”. During lumbar puncture simulation, students can repeatedly practice puncture site localization (L3-L4 interspace) and needle insertion angle adjustment. Instructors provide real-time feedback to correct issues such as “excessive needle insertion depth risking spinal cord injury” and “failure to maintain strict aseptic technique”. In cerebral herniation emergency simulation, students must make rapid decisions under pressure (eg, immediate intravenous mannitol administration), thereby honing their emergency response capabilities. This “simulation-feedback-correction” cycle resulted in the study group’s clinical skills scores being significantly superior to the control group’s, indicating that improving practical ability relies not merely on “observation” but more crucially on “hands-on practice coupled with precise guidance”. It stimulates students’ active learning awareness. The flipped classroom moves the “knowledge transmission” phase forward, compelling students to shift from “passive listening” to “active preparation”. Furthermore, the clash of perspectives during case discussions and role immersion in scenario simulations further enhance learning engagement, signifying that students have transitioned from a mindset of “being required to learn” to one of “I want to learn”.8,9
In practice, to ensure teaching effectiveness, attention to the following details is necessary. First, the multimodal approach imposes significantly higher demands on instructors compared to traditional teaching. Teachers must not only master domain knowledge but also develop skills in case design, simulation scenario scripting, standardized patient training, and debriefing facilitation. They need to invest substantial pre-class time in selecting appropriate cases, preparing video materials, and anticipating student questions. During in-class sessions, instructors shift from lecturing to real-time guidance—moderating group discussions without providing direct answers, observing simulation performances while avoiding interruption, and conducting video-assisted debriefings that pinpoint specific technical errors. This requires training in educational methodologies, such as how to ask probing questions (eg, “What would you do if the patient had renal failure?”) and how to give constructive feedback. Furthermore, institutions should provide workload compensation and faculty development workshops to sustain this teaching model. Without such support, teacher burnout may undermine the long-term implementation of multimodal integration. Graduated Case Selection: Initially, typical and straightforward cases (eg, “epidural hematoma”) can be used, gradually introducing more complex cases (eg, “multiple intracranial hematomas combined with cerebral herniation”) later. Appropriately incorporating “misdiagnosis cases” (eg, misdiagnosing “brain metastasis” as “brain abscess”) can cultivate students’ differential diagnosis skills through comparative analysis. Authenticity of Scenario Simulation: Beyond hardware facilities (eg, simulation models, monitors), training standardized patients is paramount.10 For example, when simulating a “patient with cerebral herniation”, the standardized patient needs to be trained to demonstrate the progression of consciousness from “agitation to drowsiness to coma”, and signs such as “pupils initially constricting then dilating”, providing students with a more authentic clinical experience. Transformation of the Teacher’s Role: In the new teaching model, instructors must transition from “knowledge transmitters” to “facilitators” and “organizers”. During case discussions, they should avoid providing direct answers. Instead, they should guide students towards deeper thinking through questioning (eg, “If the patient also had renal insufficiency, how might the treatment plan be adjusted?”).11–13 After scenario simulations, instructors should conduct “debriefing-style” reviews using video playback, pointing out specific issues (eg, “failing to stabilize the patient’s head during needle insertion, leading to positional change”) rather than offering general evaluations. Nevertheless, the combination of these methods is likely synergistic: flipped classroom ensures pre-class preparation, case-based learning activates clinical reasoning, and scenario simulation consolidates hands-on skills.14,15 The integrated closed-loop design may yield greater benefits than the sum of its parts, which is why we advocate for the multimodal package rather than isolated techniques.
Limitations
This study has certain limitations. First, the sample size is relatively small (30 per group), and it is a single-center study, which may affect the generalizability of the findings. Second, the evaluation was conducted immediately after the teaching intervention, without tracking the long-term performance of students after they entered clinical practice. Future research could involve multi-center, large-sample studies and include follow-ups over 1–2 years to analyze the sustained impact of the new teaching method on students’ clinical work capabilities. Third, this study applied the three teaching methods (case-based learning, scenario simulation, and flipped classroom) as a bundled intervention. Therefore, the observed improvements cannot be quantitatively attributed to any single component. Whether each method contributes equally or synergistically remains unclear. Future research could employ factorial designs or component analysis to disentangle the individual effects. Furthermore, the sample size was relatively small (30 per group) and no a priori sample size calculation was performed. Although post-hoc power analysis indicated a power close to 0.85 for the primary outcomes, small-sample studies may still affect the robustness and generalizability of the findings. Future multi-center studies with larger samples are warranted to confirm our conclusions.
Conclusion
The multimodal integrated teaching method combining case-based teaching, scenario simulation teaching, and the flipped classroom can effectively enhance postgraduate surgical education in neurosurgery, as evidenced by improved mastery of theoretical knowledge, clinical skill level, case analysis ability, and learning initiative in neurosurgery education, with high student satisfaction. This model aligns with the “student-centered” philosophy of modern medical education, provides a viable pathway for neurosurgery teaching reform, and is worthy of further promotion and refinement.
Ethics Declaration
The study was conducted in accordance with the Declaration of Helsinki and approved by Medical Ethics Committee of Wannan Medical College (No. 2024114). All subjects provided informed consent for the study. Acknowledgments We appreciate the support and assistance provided by other students and teachers.
Funding
Funding support of the study was provided by Teaching Research Project of Anhui Provincial Department of Education and Higher Education Teaching Reform of Wannan Medical College Quality Project (2024jyxm44), Educational and Teaching Reform Research Project (2025jyxm062).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Liu P, Xu J, Liu Y, Wang X, Tan Q, Wang Y. Application of modified early warning score system (MEWS) in the assessment of disease condition and prognosis of patients after neurosurgical procedure or intervention. Risk Manag Healthc Policy. 2025;18:2693–9. doi:10.2147/RMHP.S532103
2. Yao Q, Zhu P, Zou Z, Cheng Y, Liang Y, Huang W. Synergising flipped classroom and case-based learning in resource-intensive anatomy education in China: a quasi-experimental study. BMJ Open. 2025;15(11):e102001. doi:10.1136/bmjopen-2025-102001
3. Zhu Q, Jamaludin KA, Li J. Development of flipped classroom module fcm for music theory instruction: an innovative approach to music education. PLoS One. 2025;20(11):e0337590. doi:10.1371/journal.pone.0337590
4. Gopalan C, Halpin PA, Selvam AAA, Hung WC. Exploring educational transformations through the innovative flipped learning instruction project symposium. Adv Physiol Educ. 2024;48(3):505–511. doi:10.1152/advan.00027.2024
5. Khalid SI, Mehta AI, Atwal G, Hogan SO, Park YS, Charbel FT. A national study of neurosurgical residency competency development. J Neurosurg. 2025;143(4):1089–1095. doi:10.3171/2025.4.JNS243272
6. Gutiérrez-González R, Zamarron A, Royuela A, Rodriguez-Boto G. Flipped classroom applied to Neurosurgery in undergraduate medical education. BMC Med Educ. 2023;23(1):170. doi:10.1186/s12909-023-04158-8
7. McDaniel KE, Suarez A, Rowe DG, et al. Beyond medical knowledge: a didactic curriculum focused on knowledge, wisdom, and application. J Neurosurg. 2024;141(3):860–864. doi:10.3171/2024.2.JNS232775
8. Liu SM, Ou P, Li H, Hu ZL, Luo RY. Flipped classroom combined with case-based learning enhances ventilator management training for non-anesthesiology medical undergraduates: a randomized controlled study. BMC Med Educ. 2025;26(1):135. doi:10.1186/s12909-025-08380-4
9. Expósito-Hernández J, Fernández MF, Villalobos M, et al. Teaching oncology in the medical degree: integrating knowledge and experience of a multidisciplinary tumour board. J Cancer Educ. 2025. doi:10.1007/s13187-025-02784-y
10. Lau MY, Obaidellah UH, Ponnampalavanar S, et al. Evaluating hand hygiene compliance: a digital-based approach for assessing healthcare worker practices in the teaching hospitals in Malaysia. Antimicrob Resist Infect Control. 2026;15(1). doi:10.1186/s13756-025-01679-3
11. Cherney SM, Barnes CL, Blasier RD, Montgomery CO, Montgomery CO. The effect of a flipped classroom didactic curriculum on orthopaedic in-training examination scores for a resident cohort. JBJS Open Access. 2024;9(4):e2400107. doi:10.2106/JBJS.OA.24.00107
12. Dagher T, Kessler M, Levin A, et al. OrthoACCESS 2.0: redesigning a national orthopaedic surgery curriculum for medical students using a flipped-classroom blended learning model. J Surg Educ. 2025;82(1):103337. doi:10.1016/j.jsurg.2024.10.002
13. Finn A, Nugent JL, Qi SS, et al. Flipping the classroom in residency didactics leads to higher American Board of Surgery in-training examination scores. J Surg Educ. 2024;81(6):786–793. doi:10.1016/j.jsurg.2024.02.012
14. Mokadam NA, Dardas TF, Hermsen JL, et al. Flipping the classroom: case-based learning, accountability, assessment, and feedback leads to a favorable change in culture. J Thorac Cardiovasc Surg. 2017;153(4):987–996.e1. doi:10.1016/j.jtcvs.2016.10.012
15. Stippler M, Blitz SE, Quinsey C, et al. Active teaching techniques using virtual didactics: novel experience from a national neurosurgery resident course. J Surg Educ. 2023;81(2):283–290. doi:10.1016/j.jsurg.2023.11.001
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.