Back to Journals » Psychology Research and Behavior Management » Volume 15
Practical Guidance for the Use of Long-Acting Injectable Antipsychotics in the Treatment of Schizophrenia
Authors Riboldi I ![]() , Cavaleri D
, Cavaleri D ![]() , Capogrosso CA
, Capogrosso CA ![]() , Crocamo C
, Crocamo C ![]() , Bartoli F
, Bartoli F ![]() , Carrà G
, Carrà G ![]()
Received 1 November 2022
Accepted for publication 19 December 2022
Published 30 December 2022 Volume 2022:15 Pages 3915—3929
DOI https://doi.org/10.2147/PRBM.S371991
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Igor Elman
Ilaria Riboldi,1 Daniele Cavaleri,1 Chiara A Capogrosso,1 Cristina Crocamo,1 Francesco Bartoli,1 Giuseppe Carrà1,2
1Department of Medicine and Surgery, University of Milano-Bicocca, Monza, Italy; 2Division of Psychiatry, University College London, London, UK
Correspondence: Ilaria Riboldi, Department of Medicine and Surgery, University of Milano-Bicocca, Via Cadore 48, Monza, 20900, Italy, Tel +39 0257998647, Email [email protected]
Abstract: Schizophrenia is a severe mental illness causing a high degree of disability. First- and second-generation antipsychotics (FGAs and SGAs) represent key resources for its acute and long-term management. Since a poor adherence to oral treatments may negatively impact the course of the disorder, long-acting injectable antipsychotics (LAIs) are often used to reduce clinical relapses. Notwithstanding their potential beneficial features, LAIs use in clinical practice remains somewhat hampered by the limited amount of relevant systematic information. This review thus aims at providing a clinical, practical guidance for the use of LAIs in the treatment of schizophrenia. We synthetized main information on indications, dosage, and administration of LAIs approved by the US Food and Drug Administration (FDA) and/or in EU countries, as well as evidence from the most recent systematic reviews and meta-analyses. Currently available information, though heterogeneous, shows that LAIs can prevent relapses and rehospitalizations, improving clinical outcomes and favouring sustained remission among people with schizophrenia. The use of SGA LAIs is supported by more robust evidence than FGA LAIs. Along with their positive impact on the prevention of treatment discontinuation, some LAIs might also enhance individual global functioning and quality of life, without additional adverse events or health-care costs, as compared with oral antipsychotics. Although which LAIs can be considered a first-choice option, as well as their superiority over oral antipsychotics, remain unclear issues, this review offers a comprehensive overview of information available on the use of LAIs for people with schizophrenia, providing clinicians with practical guidance in terms of efficacy and acceptability of single agents. Literature gaps and future research needs are also described.
Keywords: antipsychotic agents, injections, guidelines, schizophrenia
Introduction
Schizophrenia is a severe mental illness characterised by recurrent positive, negative, and cognitive features across various subtypes and courses.1–3 It affects about 1% of the population4 and represents one of the leading causes of disability worldwide.5 Since their discovery in the 1950s, antipsychotic drugs have been considered key elements for both acute and long-term management of schizophrenia.6,7 Although all antipsychotic drugs act on dopamine receptors, they have been classified into “typical” or first-generation (FGAs) and “atypical” or second-generation (SGAs) antipsychotics in view of the different pharmacological profile.2,8 Indeed, beyond D2-antagonism, SGAs involve different receptor targets (eg, D2 and 5-HT1A partial agonism), less associated with extrapyramidal side effects (EPS) linked to the strong blockade of D2-receptors, though increasing the burden in terms of weight gain and metabolic syndrome.9–11 Despite their potential effectiveness, the frequently low adherence to oral antipsychotic treatment negatively influences the course of the disorder, causing multiple relapses.12–14 Along with the use of clozapine in treatment-resistant schizophrenia,15,16 several antipsychotics have been proposed as long-acting injectables (LAIs) in order to improve adherence, reducing the risk of relapses for people with schizophrenia.10,17,18 Indeed, LAIs, also suitable to be combined with oral formulations in clinical practice, allow better adherence, reducing risks of misuse, discontinuation, and ultimately of hospitalization, relieving at the same time from the burden of exclusive oral administration.17,19–22 Although current guidelines primarily recommend initiating LAIs in patients with history of poor or uncertain adherence, a broader and earlier use has been proposed, mainly based on evidence of their effectiveness in preventing relapse and rehospitalization.23–25 Nevertheless, their use in clinical practice remains hampered by a number of barriers including perceived stigma, use as a “last resort” and/or as a coercive measure, and clinicians’ attitudes.26–28 Indeed, available research offers little information which can support evidence-based choices.19,29 In this review, we thus aimed at providing a practical guidance on the use of LAIs for the treatment of schizophrenia, summarizing the main characteristics of approved agents as well as the most recent evidence on relevant clinical outcomes.
Materials and Methods
In order to provide a comprehensive practical guidance on the use of LAIs for schizophrenia, we first synthesized main information on indications, dosage, and administration of FGA and SGA LAIs approved by the US Food and Drug Administration (FDA),30 the European Medicines Agency (EMA),31 or, for FGA LAIs marketed before EMA establishment (1995), European national authorities. Data on currently used LAIs were retrieved from: i) technical reports available from FDA (https://www.fda.gov), EMA (https://www.ema.europa.eu/en), and national registers; ii) datasheets supplied by drug manufacturers; iii) the Maudsley Prescribing Guidelines in Psychiatry, 14th Edition.32 In addition, we reviewed main findings from the most recent systematic reviews and meta-analyses19,33–44 in order to summarize evidence on the effectiveness of LAIs for the management of schizophrenia. Main clinical outcomes considered included: prevention of relapses and rehospitalizations; clinical improvement; clinical remission; treatment discontinuation; adverse effects; global functioning and quality of life; effects on mortality and suicidality; and economic impact.
Practical Guidelines
As a whole, 15 LAIs – seven FGAs and eight SGAs– are currently approved in the US and/or in EU member states for the treatment of schizophrenia. Among FGA LAIs, only two, ie, fluphenazine decanoate and haloperidol decanoate, are approved in both the US and the EU. Moreover, five other FGA LAIs – namely bromperidol decanoate, flupentixol decanoate, perphenazine decanoate, pipotiazine palmitate, and zuclopenthixol decanoate – are licensed to treat schizophrenia across some EU countries but not in the US. As regards SGA LAIs, aripiprazole monohydrate (AM), olanzapine pamoate, paliperidone palmitate 1-month (PP1M), 3-month (PP3M), and 6-month (PP6M) formulations, and risperidone microspheres are approved by both FDA and EMA. Moreover, the FDA has also recently authorised aripiprazole lauroxil (AL) and the once-monthly subcutaneous extended-release risperidone formulation named RBP-7000.
Important features of each LAI, including year of approval, primary biological targets, use in special populations, incidence of adverse effects, and main pharmacological interactions are reported in Table 1.
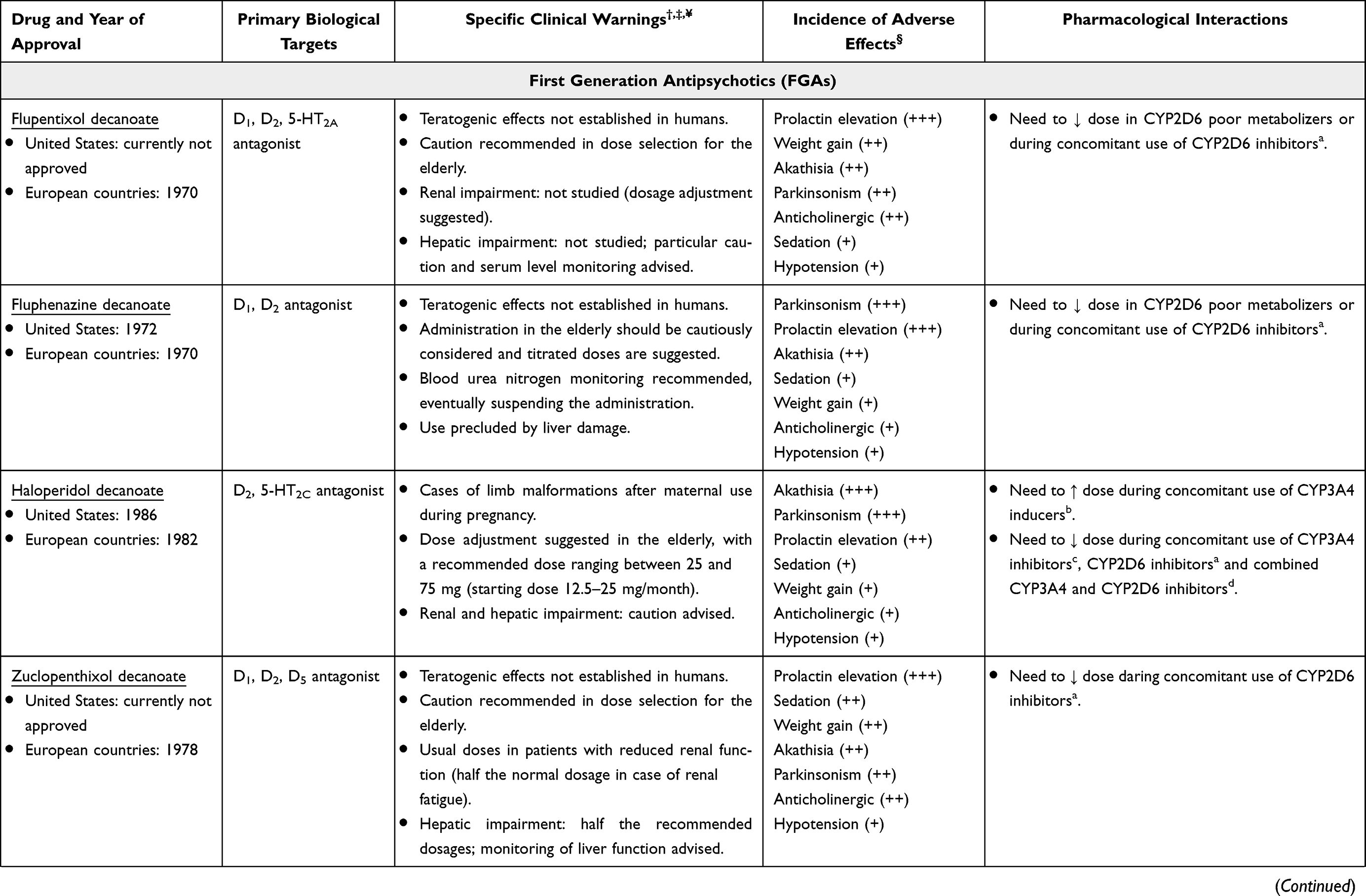 |  | 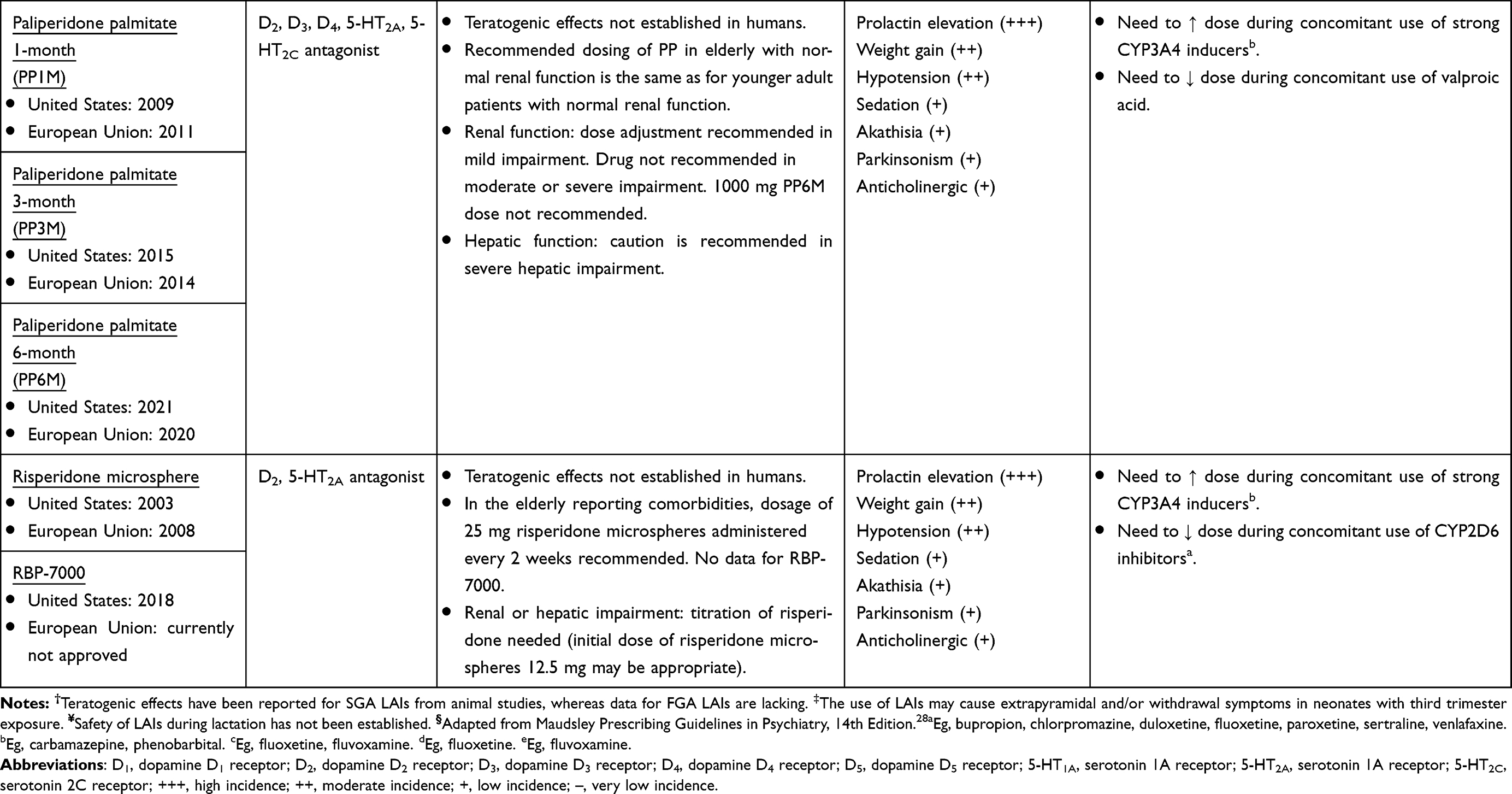 |
Table 1 Characteristics of Long-Acting Injectable Antipsychotics According to Relevant Technical Reports |
First-Generation Antipsychotics
Flupentixol Decanoate
Flupentixol decanoate is approved in several EU countries for the maintenance treatment of schizophrenia in subjects whose main manifestations do not include excitement, agitation, or hyperactivity, while it is not currently approved in the US. In individuals who have never received flupentixol LAI, the treatment is usually started with a low dose (eg, 20 mg) to assess tolerability.45 An interval of at least 1 week should be allowed before the second intramuscular injection, considering a dose consistent with the subject’s clinical condition. The plasma peak is reached 3 to 7 days after the intake of flupentixol decanoate, thus no oral integration is needed. The average dosage of flupentixol decanoate lies between 50 mg every 4 weeks and 300 mg every 2 weeks. However, while some people may be adequately maintained on dosages of 20–40 mg every 2–4 weeks, other individuals may require up to 400 mg weekly, which is the maximum dose. To calculate the dosage of flupentixol decanoate, the oral dose must be multiplied by four if administered every 2 weeks, or by eight if dosed monthly.
Fluphenazine Decanoate
Fluphenazine was the first antipsychotic drug produced in a LAI formulation, fluphenazine enanthate (1966), whilst fluphenazine decanoate was introduced 18 months later.46
Fluphenazine decanoate is licensed for the treatment of schizophrenia in both the US and a number of EU countries. It can be administered either intramuscularly or subcutaneously. For an appropriate dosage of fluphenazine decanoate, clinicians should consider that 20 mg/day of oral fluphenazine is equivalent to 25 mg of the LAI formulation administered every 3 weeks. The treatment should be started with a 12.5–25 mg injection every 2 weeks. There is no need for concomitant oral supplementation as the drug reaches sufficient plasma levels within 2–4 days. The maintenance dose ranges from 12.5 mg to 100 mg, reached with cautious increments of 12.5 mg. The administrations should be scheduled every 2 to 6 weeks.
Haloperidol Decanoate
Haloperidol decanoate is approved for the maintenance treatment of schizophrenia in both the US and the EU. The dose conversion approach from oral to LAI formulation should be made multiplying the oral daily dose by 10 to 20. Dosages between 50 and 100 mg/month are recommended to start treatment, whereas the target dose should range from 50 to 200 mg per month – with a maximum of 300 mg – although the efficacy of increases above 100 mg per month has been questioned.47 On average, the interval between injections is 4 weeks, but in special cases it can be shortened to 2 weeks or extended up to 8 weeks. Differently from most LAIs, haloperidol LAI can be administered exclusively in the gluteus maximus muscle. As several weeks are needed before reaching stable plasma levels, additional oral treatment for approximately 1 to 2 weeks is needed.45
Zuclopenthixol Decanoate
Zuclopenthixol decanoate is approved for the management of schizophrenia in EU countries but not in the US. The loading dose is usually 100 mg and, considering that maximum serum concentrations of zuclopenthixol decanoate are reached within 3 to 7 days, it should be combined with oral zuclopenthixol for the first week at decreasing dosages. The appropriate dose for a 2-week interval corresponds to approximately 5 times the daily oral dose, thus the maintenance therapy may vary between 200 mg/month and 600 mg/week (which is the maximum single dose at one time), usually administered in the gluteal region.
Other First-Generation Antipsychotics
Among FGA LAIs approved in the EU but not in the US, besides flupentixol decanoate and zuclopenthixol decanoate, also bromperidol decanoate, perphenazine decanoate, and pipotiazine palmitate are authorized. Nonetheless, their use is less common and limited to few countries across the EU to date: bromperidol decanoate is approved in Belgium, Luxembourg, and the Netherlands; perphenazine decanoate is licensed in Denmark, Finland, Iceland, Norway, and Sweden; pipotiazine palmitate is currently approved and available exclusively in France.
Notably, evidence supporting their clinical utilization is dated, limited, and less consistent as compared with the other LAIs considered in this review.
Second-Generation Antipsychotics
Aripiprazole LAI
Aripiprazole is the first and only D2 partial agonist developed as a LAI to date.32 It is produced in two formulations: a once-monthly injection, aripiprazole monohydrate (AM), and a newer formulation, aripiprazole lauroxil (AL), which is administered once every 4 to 8 weeks.
Aripiprazole Monohydrate
AM is approved for the treatment of adult people with schizophrenia both in the US and the EU. AM requires about 14 days to reach sufficient plasmatic concentrations. To overcome this issue, health-care providers can administer the loading dose following two different strategies: the first involves starting intramuscular injection of AM 400 mg followed by a 2-week period of concomitant oral aripiprazole (dosage between 10 and 20 mg per day); the second one, whose safety and tolerability was recently confirmed in clinical trials,32 suggests the injection of two separate doses of AM 400 mg (separate gluteal, separate deltoid, or gluteal and deltoid injection sites) followed by a single dose of 20 mg of oral aripiprazole. The latter approach allows avoiding oral concomitant treatment and therefore possible compliance issues. Maintenance doses of AM should be administered with a minimum interval of 26 days. A dosage decrease from 400 mg to 300 mg is suggested in case of tolerability issues.
Aripiprazole Lauroxil
AL is approved by the FDA – but not by the EMA yet – for the treatment of schizophrenia in adults. AL is a pro-drug of aripiprazole available in two distinct extended-release formulations: a nanocrystal formulation used as a one-time injection to initiate treatment with AL or to restart it after a missed dose, providing therapeutic blood levels within 4 days of injection,48 and a formulation for maintenance treatment marketed in four different dosages: 441 mg, 662 mg, 882 mg, and 1064 mg.49,50 Two options are available for the loading dose: the first one combines the one-time administration of AL nanocrystal formulation 675 mg with a single 30 mg dose of oral aripiprazole, followed by the administration of AL (in a separate muscle) on the same day or up to 10 days later; the second option involves the administration of AL followed by 21 additional days of concomitant oral treatment. For maintenance treatment, AL is administered intramuscularly with 1-month, 6-week, or 2-month intervals, subsequently adjusting the dose. The maintenance dose should be calculated observing conversion rules as it follows: 10 mg of oral aripiprazole per day is equivalent to AL 441 mg monthly; 15 mg per day correspond to AL 662 mg monthly or AL 882 mg every six weeks or AL 1064 mg every two months; 20 mg of oral aripiprazole per day can be reached with AL 882 mg monthly. The 441 mg dosage of AL can be administered alternatively in the deltoid or in the gluteus, while 662 mg, 882 mg, and 1064 mg dosages should be injected in the gluteal site only. When early dosing is needed, an injection should not be given before 14 days have passed since the previous injection.
Olanzapine Pamoate
Olanzapine pamoate is approved for the maintenance treatment of adults with schizophrenia in the US as well as in the EU. It consists of microcrystals dissolved in water, and only the gluteal injection is licensed. Olanzapine pamoate can be administered every 2 or 4 weeks, depending on the chosen dosage. During the initiation period (8 weeks), the loading dose should be calculated considering the oral dose: individuals treated with 10 mg of oral olanzapine should receive olanzapine pamoate 210 mg every 2 weeks or 405 mg every month for the first 8 weeks, while a current oral dosage of 15–20 olanzapine/day requires an olanzapine pamoate maximum dose of 300 mg every 2 weeks. Plasma peaks are reached as early as 4 days after the injection,32 hence continuing oral administration should not be needed. However, when oral supplementation is deemed necessary, the daily cumulative dose should not exceed 20 mg. After the first 8 weeks of treatment, dose reduction is generally recommended: people taking oral olanzapine 10 mg/day should be maintained on olanzapine pamoate 150 mg every 2 weeks or 300 mg every 4 weeks, while subjects on 15 mg oral per day should be administered olanzapine pamoate 210 mg twice a month or 405 mg monthly. Conversely, dose reduction from 300 mg every 2 weeks is not recommended in subjects previously treated with oral olanzapine 20 mg/day. When olanzapine pamoate is inadvertently exposed to high blood volumes (mainly because of accidental intravasation),51 a post-injection syndrome may occur, with symptoms of sedation (from mild severity to coma) and/or delirium, but also EPS, dysarthria, ataxia, aggression, dizziness, weakness, hypertension, and convulsions. In most cases, initial signs and symptoms related to this reaction appear within an hour after the injection, while full recovery usually occurs within 24–72 hours. For these reasons, people treated with olanzapine pamoate should be monitored by health-care staff for at least 3 hours after the injection.
Paliperidone Palmitate
Paliperidone palmitate, the palmitate ester of paliperidone, is available in three LAI formulations, which differ in terms of length of release and, subsequently, frequency of administration.
Paliperidone Palmitate 1-Month
PP1M is authorised for the treatment of schizophrenia by both FDA and EMA. The induction phase consists of a fixed-dose loading procedure with an intramuscular administration of PP1M 150 mg on day 1 followed by a second administration of PP1M 100 mg on day 8 (± 4 days).
Unlike other LAIs, PP1M can be used without prior stabilisation with oral treatment in selected individuals who previously responded to oral paliperidone or risperidone. After the first administration, effective plasma spikes are reached after about 1 day, therefore no concomitant oral administration is necessary.52 The recommended maintenance phase consists of monthly (± 7 days) administrations of 75 mg – corresponding to 6 mg of oral paliperidone – injected in the deltoid or in the gluteus maximus muscles. However, the dosage can be individualised, administering PP1M 25–50 mg to subjects previously on 3 mg oral paliperidone, PP1M 100 mg when the oral dose was 9 mg/day, or PP1M 150 mg to subjects with prior treatment with oral paliperidone 12 mg/day. Up to 2 months of treatment may be needed to achieve full efficacy.
Paliperidone Palmitate 3-Month
People with schizophrenia who have been adequately treated with PP1M for at least 4 months may be switched to PP3M, a formulation of paliperidone palmitate administered every 3 months approved in both the US and the EU. PP3M should be introduced on the day when the next PP1M injection is scheduled with a dose based on the previous PP1M dose, using the equivalent 3.5-fold higher dose: PP1M 50 mg corresponds to PP3M 175 mg, PP1M 75 mg to PP3M 263 mg, PP1M 100 mg to PP3M 350 mg, and PP1M 150 mg to PP3M 525 mg. If necessary, PP3M injections may be given with a ±2-week tolerance from the 3-month scheduled timepoint, even though, when the dose is missed for more than 2 weeks but less than 1 month, PP3M can be administered as soon as possible. On the other hand, if more than four months have passed since the previous injection, LAI treatment should be restarted with PP1M, adapting the re-initiation scheme to the time elapsed.
Paliperidone Palmitate 6-Month
People with schizophrenia who are adequately treated with PP1M at doses of 100 mg or 150 mg (preferably for 4 months or more) or with PP3M at doses of 350 mg or 525 mg (for at least one cycle), and who do not require dose adjustment, may be transitioned to PP6M injection, the most recently approved LAI formulation of paliperidone, available both in the US and in the EU. The dose of PP6M should be based on the previous PP1M or PP3M injectable dose following certain conversion rules: PP1M 100 mg corresponds to PP3M 350 mg and to PP6M 700 mg; PP1M 150 mg corresponds to 3-months PP3M 525 mg and to PP6M 1000 mg. If necessary, subjects may be given the injection up to 2 weeks before - or 3 weeks after - the 6-month scheduled timepoint. After such time window, the treatment should be re-initiated with PP1M, following different regimens, depending on the time from the last injection.
Risperidone LAI
Risperidone LAI was the first SGA to be made available in LAI formulation in 2003.53 It is currently offered in two formulations: a bimonthly injection, risperidone microsphere (RM), and a newer formulation, RBP-7000, a once-monthly extended-release injectable suspension.
Risperidone Microspheres
Risperidone microspheres is indicated for the treatment of schizophrenia in both the US and the EU. It has a peculiar formulation consisting of microspheres which hydrolyse slowly, allowing a steady release of risperidone molecules. Tolerability needs to be tested with oral risperidone before initiating the LAI formulation. Since it is released slowly, the first use of this intramuscular preparation requires the simultaneous administration of oral risperidone for the first 21 days.54 This formulation is available at dosages of 25 mg, 37.5 mg and 50 mg which, being administered every 2 weeks, correspond to oral doses of 2, 4 and 6 mg/day, respectively.55 The recommended maintenance dose for schizophrenia is 25 mg every 2 weeks, and higher dose adjustments should not be made more frequently than every 4 weeks.
RBP-7000
RBP-7000 is a newly FDA-approved56 risperidone drug-device combination which is administered subcutaneously. This formulation of risperidone is released from the injection site over 1 month. RBP-7000 is designed so that the drug achieves clinically relevant therapeutic plasma concentrations on the first day of dosing, with no need for a loading dose or supplemental oral therapy.56 RBP-7000 is available at dosages of 90 mg and 120 mg, administered monthly.
Clinical Outcomes
Prevention of Relapse and Rehospitalizations
Evidence from meta-analyses of randomized controlled trials (RCTs) suggests that most LAIs are likely to be superior to placebo in preventing relapse and rehospitalisation in schizophrenia.19,34,35
In terms of relapse prevention, SGA LAIs supported by the most robust evidence from RCTs are aripiprazole, olanzapine, and paliperidone (both PP1M and PP3M), for which moderate-to-high quality evidence exists.19,34,35 Available evidence suggests that risperidone may be equally effective in preventing relapse, but confidence seems only low-to-moderate.19,34,35 For what regards FGA LAIs, flupentixol, fluphenazine, and zuclopenthixol seem similarly superior to placebo, with effect estimates similar to those of SGA LAIs, although confidence in relevant evidence is low-to-moderate at best.19,34,35 In particular, findings on zuclopenthixol LAI are based on two small studies (56 total participants on zuclopenthixol LAI), thus estimates show very high uncertainty.35 Interestingly, the efficacy of haloperidol decanoate for relapse prevention has been questioned by a very recent network meta-analysis,34 while similar work had previously highlighted that it was significantly better than placebo.34,35 Nonetheless, the quality of the evidence on haloperidol LAI appears inconsistent across different network meta-analyses, having been deemed by some even as very low,19,34 and as moderate by others.35
Data on hospitalisation, albeit based on scarce information and often low events rates, suggest that, among LAIs, olanzapine, risperidone, PP3M, and fluphenazine may lead to a lower risk of rehospitalization than placebo, with a varying confidence in the estimates.19,34,35 Mixed findings are available for PP1M and haloperidol decanoate, considering the inconsistent conclusions of recent network meta-analyses.19,34,35 Evidence on aripiprazole LAI suggests that it is not significantly better than placebo in preventing rehospitalization.19,34,35
In comparison to oral antipsychotics, LAIs are likely to be superior in the prevention of relapse or hospitalisation across different settings, from RCTs to real-world cohort and pre-/post-studies.36 Although head-to-head comparisons are limited,43 overall evidence suggests that LAIs may be superior to their oral counterpart in preventing relapses.37 Similarly, although LAI treatment does not seem to reduce days of hospitalisation in RCTs and cohort studies, evidence from mirror-image studies highlights that switching from an oral AP to its LAI formulation may be an effective strategy to reduce the length of hospital treatment.37 Moreover, real-world evidence suggests that LAI treatment can reduce visits to the emergency department.37 Evidence about head-to-head comparisons derives from controlled settings, while real-world data are lacking. In RCTs, few relevant differences between LAIs in terms of relapse prevention emerge,35 although PP3M, aripiprazole LAI, and fluphenazine LAI seem more effective than haloperidol LAI.19 Nonetheless, considering that estimates are generally imprecise, confidence should be considered as low at best. No robust evidence from head-to-head RCTs supports the superiority of any LAI over the others in preventing hospitalisation,19,34 although it has been hypothesized that risperidone LAI might be more effective than aripiprazole LAI.35 As for 3-month follow-up, relative advantages for aripiprazole LAI over paliperidone LAI have been hypothesized.41 Lastly, it should be noted that low-dose LAIs seem to have significantly higher relapse risk than standard dose LAIs.36
Clinical Improvement
Although it was reported that changes in severity scores from baseline to study endpoint were not significantly different between SGA and FGA LAIs,39 SGA LAIs including risperidone, olanzapine (moderate confidence), PP1M, PP3M, and aripiprazole (low confidence) showed the largest reductions in overall symptoms at study endpoint.19,34,35 On the other hand, evidence on FGA LAIs is contrasting and of low quality, especially on fluphenazine and haloperidol.19,34,35 It must be considered that data on the efficacy of LAIs on overall symptoms reduction are largely derived from recent studies investigating SGAs. Moreover, caution is needed in the interpretation of findings since considerable inconsistency across studies emerges.19,35 Compared to oral antipsychotics, LAIs generally do not seem to be associated with a clinically meaningful improvement in RCTs, whereas cohort studies suggest that LAI treatment may be somehow more effective than oral antipsychotics in reducing scores on the Positive and Negative Symptoms Scale (PANSS) general psychopathology subscale and the Clinical Global Impression (CGI), respectively.16,31 However, no statistically significant differences emerge from head-to-head comparisons between different LAIs.19,35
Clinical Remission
Some evidence from RCTs suggests that SGA LAIs can favour sustained remission, achieving the remission criteria according to PANSS and/or CGI-Severity scores for at least 6 months.44 The confidence in the estimates is moderate for both risperidone and paliperidone LAIs, and low for aripiprazole LAI.35 No single agent seems significantly superior to the others in inducing sustained remission, possibly due to the paucity of data on this outcome.35 Finally, LAIs do not seem to perform better than their oral counterparts in terms of clinical remission in both experimental and real-world settings.37
Treatment Discontinuation
All-Cause Discontinuation
In terms of any-reason discontinuation, evidence from RCTs suggests that both FGA and SGA LAIs are more acceptable than placebo.19,34,35 Among them, aripiprazole seems the most promising.19 Head-to-head LAI comparisons have shown that treatment discontinuation is less likely in subjects treated with aripiprazole LAI as compared with those receiving fluphenazine LAI, PP1M, and risperidone LAI.19 Data from RCTs show that, when compared with oral antipsychotics, LAIs do not differ in terms of all-cause discontinuation. However, some non-randomized experimental evidence highlights that all-cause discontinuation in people treated with LAIs is significantly lower than in those on oral antipsychotics, supporting the utility of LAIs in real-world clinical practice.37
Discontinuation Due to Inefficacy
No statistically significant differences emerge in terms of dropout due to inefficacy in both RCTs and cohort studies,37 except for olanzapine, whose LAI formulation shows significantly higher rates of discontinuation due to inefficacy compared with its oral formulation.43
Discontinuation Due to Adverse Events
In terms of discontinuation due to adverse events, PP1M is the only LAI which performs worse than placebo.19 Compared to oral antipsychotics, LAIs do not seem to be associated with a higher likelihood of discontinuing treatment due to adverse events from both RCTs and non-randomized studies.37 Head-to-head LAI comparisons seem to favour aripiprazole LAI over PP1M19 as well as olanzapine pamoate over fluphenazine LAI,34 while no other significant differences emerge.
Adverse Effects
Evidence from RCTs suggests that LAIs have an almost negligible risk of causing at least one adverse effect as compared with oral antipsychotics.37 Moreover, oral antipsychotics and LAIs do not seem to differ in terms of likelihood of serious adverse events.37
In terms of specific side effects, no significant differences are reported between any single LAI and placebo in terms of sedation,34,35 although head-to-head LAI comparisons suggest that haloperidol decanoate is notably more sedative than aripiprazole LAI.35 Evidence regarding the sedative effects of risperidone LAI is inconsistent and mixed.34,35 Moreover, LAIs do not seem more sedative than the majority of oral antipsychotics.35
In terms of EPS, it seems that LAIs do not bring a significantly higher risk compared to placebo,19 even though low-to-moderate evidence quality suggests that subjects treated with fluphenazine, haloperidol, and aripiprazole LAIs may require more frequently antiparkinson medications.35 Conversely, olanzapine pamoate seems to induce less EPS than both other LAIs and placebo.35 Moreover, though based on scarce and uncertain findings, LAIs do not seem different from their oral counterparts in terms of EPS risk.37 Tardive dyskinesia with LAIs seems a rare event, occurring in about 1% of participants of RCTs.35
Regarding the risk of corrected QT (QTc) interval prolongation, known to be associated with severe arrhythmias,57,58 evidence is quite scarce and based on few recent studies. Aripiprazole and paliperidone are the only LAIs with available evidence on QTc interval, showing no statistically significant differences as compared with placebo.35 Moreover, PP3M seems to have a lower risk of QTc prolongation than PP1M.19
Body weight gain, a frequent issue related to antipsychotic treatment, seems to be significantly higher for paliperidone LAI (both PP1M and PP3M), risperidone LAI, and olanzapine LAI, when compared to placebo.19,35 Evidence on aripiprazole LAI is conflicting, with an unclear risk of inducing significant weight gain.19,35 Nonetheless, aripiprazole LAI seems preferable to other SGA LAIs – eg, olanzapine, paliperidone, and risperidone – for body weight control.35 Surprisingly, haloperidol decanoate appears to increase body weight less than placebo, albeit with low confidence in the estimates.35 It is worth mentioning that the influence on body weight seems related more to the drug itself than to the oral or LAI formulation.35
No significant differences between LAIs and oral antipsychotics have been detected in terms of change of blood concentrations of fasting glucose, total cholesterol, high-density lipoproteins, and triglycerides.37 However, compared to oral antipsychotics, LAIs seem associated with significantly higher low-density lipoprotein levels, although with a negligible effect size.37
Finally, compared to placebo, prolactin is significantly increased by both PP1M and PP3M, while there is conflicting evidence regarding risperidone and olanzapine LAIs.19,35 On the other hand, aripiprazole and haloperidol LAIs do not seem to significantly influence prolactin secretion.35 Furthermore, LAIs in general do not seem to increase prolactin more than oral antipsychotics.37 Thus, as for body weight, influence on prolactin concentration seems related more to the drug than to the formulation. An exception may be represented by risperidone, whose LAI formulation seems associated with a lower risk of developing hyperprolactinemia compared to the oral counterpart.35,43
Global Functioning and Quality of Life
Evidence regarding functioning in people with schizophrenia treated with LAIs is scarce and available only for SGA LAIs. It shows better outcomes in subjects treated with LAIs as compared with those on placebo35,40 or oral antipsychotics.40 This is confirmed in both short- and long-term investigations, with poorer psychosocial functioning predicted by treatment duration, symptom severity, and cognition and insight impairment.40 Regarding quality of life of people with schizophrenia using LAIs, considering the high inconsistency across studies in the assessment of this outcome, evidence is available only for paliperidone LAI, which seems superior to placebo.35
Effects on Mortality and Suicidality
SGA and FGA LAIs seem to be a protective strategy against all-cause mortality in people with schizophrenia.33 Nonetheless, both experimental and real-world studies do not show any statistically significant differences in terms of risk of death between people under LAI treatment and those taking oral antipsychotics.37 Data available on suicidality do not support any anti-suicidal effect of LAIs, including aripiprazole, fluphenazine, olanzapine, paliperidone, and risperidone, that do not seem to differ from placebo or oral antipsychotics in terms of rates of completed suicides.37,42
Economic Impact of LAI Treatment
The initiation of LAI treatment has been reported to be associated with higher per-patient-per-year (PPPY) pharmacy costs in the US. However, such costs seem counterbalanced by lower PPPY medical costs, resulting in no significant net difference in PPPY total all-cause health-care costs between people treated with LAI and those treated with oral antipsychotics.36 Regarding single agents, systematic evidence is available only for the comparison between PP1M and oral antipsychotics, with no significant differences between these two therapeutic strategies in terms of PPPY total health-care costs.36
Summary of Evidence
The most updated evidence, albeit heterogeneous, highlights a likely superiority of LAIs over placebo and oral antipsychotics in preventing disease relapse in both experimental19,34,35 and real-world37 settings. SGA LAIs effects are supported by more robust evidence than FGA LAIs,19,34,35 being based on more recent and higher-quality studies. LAIs seem to reduce also hospitalisations, but the body of evidence is somehow inconsistent. Interestingly, real-world evidence appears much more promising than experimental evidence,37 possibly because RCTs may not properly consider the high non-adherence rates typical of real-world clinical settings.59–61 LAIs seem more effective than oral antipsychotics also in improving symptoms, but only in terms of evidence from cohort studies,37 while no significant differences emerge between SGA and FGA LAIs.39 Data seem to suggest that PP1M, PP3M, and aripiprazole LAI may have larger effects in reducing symptom severity, while the quality of evidence for FGA LAIs is questionable.19,35 Nonetheless, no single LAI shows clear superiority,19,34,35 mainly because head-to-head comparisons are limited to very few RCTs.43 On the other hand, the use of haloperidol decanoate, a key element of schizophrenia treatment for decades, seems supported by uncertain and quite inconsistent evidence,19,34 possibly questioning its role when compared with other LAI options. In terms of treatment discontinuation, both FGA and SGA LAIs are more acceptable not only than placebo19,34,35 but also than oral antipsychotics,37 further supporting their utility in real-world clinical practice. Aripiprazole LAI seems the most acceptable LAI and is associated with lower rates of discontinuation.19 In general, LAIs do not seem to be discontinued for inefficacy more than their oral counterparts, except for olanzapine pamoate, which shows significantly higher rates of discontinuation due to inefficacy than the oral formulation. Moreover, LAIs do not seem to cause a higher likelihood of discontinuing treatment due to adverse effects.37 Interestingly, data from real-world settings suggest that LAIs and oral antipsychotics do not differ in terms of incidence of serious adverse events.37 Despite pharmacokinetic differences between oral and LAI formulations, theoretically accounting for different tolerability profiles,62 the majority of side effects of antipsychotics seem related more to the drug itself than to the formulation, with the exception of risperidone, whose LAI formulations seem at lower risk of causing hyperprolactinemia than the oral counterpart.35,43
In addition, LAIs seem to guarantee a better general functioning,35,40 and may also be protective in terms of all-cause mortality in people with schizophrenia, but not in terms of suicide prevention.33,37,42 Finally, LAIs do not seem to increase overall health-care costs when compared with oral antipsychotics.38
Conclusions
As a whole, although available research does not provide any “silver bullet” in terms of which LAIs should be preferred as first-choice option, a bulk of evidence offers robust information, useful to tailor single LAIs for the current clinical presentation of each individual. Further, while the efficacy and tolerability of LAI formulations may not be far superior to those of oral antipsychotics, the inherent improvement of treatment adherence in real-world clinical settings remains a key beneficial element. In this regard, also product characteristics need to be taken into account to favour treatment compliance and promote the therapeutic alliance. Indeed, considering the balance between efficacy and tolerability of each single LAI, people with doubtful compliance to medications could be preferably treated with LAIs not requiring oral supplementation. Additionally, LAIs with longer between-dosing intervals, such as AL, PP3M, or PP6M, may reduce the actual and perceived burden of being medicated. Considering the positive impact of a successful treatment on long-term outcomes for people with schizophrenia, additional RCTs, as well as real-world research, based on large samples are needed to guide clinicians as for the choice of the most appropriate LAI. Finally, future research should clarify comparative effectiveness among different LAIs, as well as potential benefits of augmentation strategies with oral antipsychotics.
Abbreviations
US, United States; EU, European Union; FGA, first-generation antipsychotic; SGA, second-generation antipsychotic; LAI, long-acting injectable; FDA, Food and Drug Administration; EMA, European Medicines Agency; EPS, extrapyramidal side effect; AM, aripiprazole monohydrate; AL, aripiprazole lauroxil; PP1M, paliperidone palmitate 1-month; PP3M, paliperidone palmitate 3-month; PP6M, paliperidone palmitate 6-month, RCT, randomized clinical trial; QTc, corrected QT.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research received no external funding.
Disclosure
The authors declare no competing interests in this work.
References
1. McCutcheon RA, Reis Marques T, Howes OD. Schizophrenia - an overview. JAMA Psychiatry. 2020;77(2):201–210. doi:10.1001/jamapsychiatry.2019.3360
2. Kahn R, Sommer I, Murray R, et al. Schizophrenia. Nat Rev Dis Primers. 2015;1:15067. doi:10.1038/nrdp.2015.67
3. Carrà G, Crocamo C, Angermeyer M, Brugha T, Toumi M, Bebbington P. Positive and negative symptoms in schizophrenia: a longitudinal analysis using latent variable structural equation modelling. Schizophr Res. 2019;204:58–64. doi:10.1016/j.schres.2018.08.018
4. Jongsma HE, Turner C, Kirkbride JB, Jones PB. International incidence of psychotic disorders, 2002–17: a systematic review and meta-analysis. Lancet Public Health. 2019;4(5):e229–e244. doi:10.1016/S2468-2667(19)30056-8
5. GBD. 2019 mental disorders collaborators. Global, regional, and national burden of 12 mental disorders in 204 countries and territories, 1990–2019: a systematic analysis for the global burden of disease study 2019. Lancet Psychiatry. 2022;9(2):137–150. doi:10.1016/S2215-0366(21)00395-3
6. Fountoulakis KN, Moeller HJ, Kasper S, et al. The report of the joint WPA/CINP workgroup on the use and usefulness of antipsychotic medication in the treatment of schizophrenia. CNS Spectr. 2020;29:1–25. doi:10.1017/S1092852920001546
7. Leucht S, Heres S, Kissling W, Davis JM. Evidence-based pharmacotherapy of schizophrenia. Int J Neuropsychopharmacol. 2011;14(2):269–284. doi:10.1017/S1461145710001380
8. Correll CU, Kane JM. Ranking antipsychotics for efficacy and safety in schizophrenia. JAMA Psychiatry. 2020;77:225–226. doi:10.1001/jamapsychiatry.2019.3377
9. Bartoli F, Carrà G, Crocamo C, Carretta D, Clerici M. Bipolar disorder, schizophrenia, and metabolic syndrome. Am J Psychiatry. 2013;170(8):927–928. doi:10.1176/appi.ajp.2013.13040447
10. Correll CU, Citrome L, Haddad PM, et al. The use of long-acting injectable antipsychotics in schizophrenia: evaluating the evidence. J Clin Psychiatry. 2016;77(suppl 3):1–242. doi:10.4088/JCP.15032su1
11. Bartoli F, Crocamo C, Clerici M, Carrà G. Second-generation antipsychotics and adiponectin levels in schizophrenia: a comparative meta-analysis. Eur Neuropsychophar. 2015;25(10):1767–1774. doi:10.1016/j.euroneuro.2015.06.011
12. Kim J, Ozzoude M, Nakajima S, et al. Insight and medication adherence in schizophrenia: an analysis of the CATIE trial. Neuropharmacology. 2020;15(168):107634. doi:10.1016/j.neuropharm.2019.05.011
13. Emsley R, Nuamah I, Gopal S, Hough D, Fleischhacker WW. Relapse after antipsychotic discontinuation in schizophrenia as a withdrawal phenomenon vs illness recurrence: a post hoc analysis of a randomized placebo-controlled study. J Clin Psychiatry. 2018;79(4):17m11874. doi:10.4088/JCP.17m11874
14. Higashi K, Medic G, Littlewood KJ, Diez T, Granström O, De Hert M. Medication adherence in schizophrenia: factors influencing adherence and consequences of nonadherence, a systematic literature review. Ther Adv Psychopharmacol. 2013;3(4):200–218. doi:10.1177/2045125312474019
15. Kane JM, Correll CU. The role of clozapine in treatment-resistant schizophrenia. JAMA Psychiatry. 2016;73(3):187–188. doi:10.1001/jamapsychiatry.2015.2966
16. Kokurcan A. Comparison of clinical characteristics between the patients with schizophrenia on clozapine treatment with those taking combination of long-acting injectable and oral antipsychotics. Noro Psikiyatr Ars. 2019;56(3):219–223. doi:10.29399/npa.23548
17. Kishimoto T, Hagi K, Nitta M, et al. Effectiveness of long-acting injectable vs oral antipsychotics in patients with schizophrenia: a meta-analysis of prospective and retrospective cohort studies. Schizophr Bull. 2018;44:603–619. doi:10.1093/schbul/sbx090
18. Ostuzzi G, Mazzi MA, Terlizzi S, et al. Factors associated with first- versus second-generation long-acting antipsychotics prescribed under ordinary clinical practice in Italy. PLoS One. 2018;13(8):e0201371. doi:10.1371/journal.pone.0201371
19. Ostuzzi G, Bertolini F, Del Giovane C, et al. Maintenance treatment with long-acting injectable antipsychotics for people with nonaffective psychoses: a network meta-analysis. Am J Psychiatry. 2021;178(5):424–436. doi:10.1176/appi.ajp.2020.20071120
20. Kane JM, Correll CU. Optimizing treatment choices to improve adherence and outcomes in schizophrenia. J Clin Psychiatry. 2019;80(5):IN18031AH1C. doi:10.4088/JCP.IN18031AH1C
21. Kishimoto T, Nitta M, Borenstein M, et al. Long-acting injectable versus oral antipsychotics in schizophrenia: a systematic review and meta-analysis of mirror-image studies. J Clin Psychiatry. 2013;74:957–965. doi:10.4088/JCP.13r08440
22. Kokurcan A, Güriz SO, Karadağ H, Erdi F, Örsel S. Treatment strategies in management of schizophrenia patients with persistent symptoms in daily practice: a retrospective study. Int J Psychiatry Clin Pract. 2021;25(3):238–244. doi:10.1080/13651501.2021.1879157
23. Tiihonen J, Mittendorfer-Rutz E, Majak M, et al. Real-world effectiveness of antipsychotic treatments in a nationwide cohort of 29 823 patients with schizophrenia. JAMA Psychiatry. 2017;74:686–693. doi:10.1001/jamapsychiatry.2017.1322
24. Correll CU, Martin A, Patel C, et al. Systematic literature review of schizophrenia clinical practice guidelines on acute and maintenance management with antipsychotics. Schizophrenia. 2022;8(1):5. doi:10.1038/s41537-021-00192-x
25. Pietrini F, Albert U, Ballerini A, et al. The modern perspective for long-acting injectables antipsychotics in the patient-centered care of schizophrenia. Neuropsychiatr Dis Treat. 2019;15:1045–1060. doi:10.2147/NDT.S199048
26. Paton C, Okocha CI, Patel MX. Can the use of long-acting injectable antipsychotic preparations be increased in routine clinical practice and the benefits realised? Ther Adv Psychopharmacol. 2022;12:20451253211072347. doi:10.1177/20451253211072347
27. Barbui C, Bertolini F, Bartoli F, et al. Reasons for initiating long-acting antipsychotics in psychiatric practice: findings from the STAR network depot study. Ther Adv Psychopharmacol. 2020;10:2045125320978102. doi:10.1177/2045125320978102
28. Parellada E, Bioque M. Barriers to the use of long-acting injectable antipsychotics in the management of schizophrenia. CNS Drugs. 2016;30(8):689–701. doi:10.1007/s40263-016-0350-7
29. Llorca PM, Abbar M, Courtet P, Guillaume S, Lancrenon S, Samalin L. Guidelines for the use and management of long-acting injectable antipsychotics in serious mental illness. BMC Psychiatry. 2013;13:340. doi:10.1186/1471-244X-13-340
30. U.S. Food and Drug Administration. Drugs@FDA: FDA-Approved Drugs. Available from: https://www.accessdata.fda.gov/scripts/cder/daf/index.cfm.
31. European Medicines Agency. Public Data from Article 57 Database. Available from: https://www.ema.europa.eu/en/human-regulatory/post-authorisation/data-medicines-iso-idmp-standards/public-data-article-57-database.
32. Taylor DM, Barnes TRE, Young AH. The Maudsley Prescribing Guidelines in Psychiatry.
33. Correll CU, Solmi M, Croatto G, et al. Mortality in people with schizophrenia: a systematic review and meta-analysis of relative risk and aggravating or attenuating factors. World Psychiatry. 2022;21(2):248–271. doi:10.1002/wps.20994
34. Ostuzzi G, Bertolini F, Tedeschi F, et al. Oral and long-acting antipsychotics for relapse prevention in schizophrenia-spectrum disorders: a network meta-analysis of 92 randomized trials including 22,645 participants. World Psychiatry. 2022;21(2):295–307. doi:10.1002/wps.20972
35. Schneider-Thoma J, Chalkou K, Dörries C, et al. Comparative efficacy and tolerability of 32 oral and long-acting injectable antipsychotics for the maintenance treatment of adults with schizophrenia: a systematic review and network meta-analysis. Lancet. 2022;399(10327):824–836. doi:10.1016/S0140-6736(21)01997-8
36. Højlund M, Kemp AF, Haddad PM, Neill JC, Correll CU. Standard versus reduced dose of antipsychotics for relapse prevention in multi-episode schizophrenia: a systematic review and meta-analysis of randomised controlled trials. Lancet Psychiatry. 2021;8(6):471–486. doi:10.1016/S2215-0366(21)00078-X
37. Kishimoto T, Hagi K, Kurokawa S, Kane JM, Correll CU. Long-acting injectable versus oral antipsychotics for the maintenance treatment of schizophrenia: a systematic review and comparative meta-analysis of randomised, cohort, and pre-post studies. Lancet Psychiatry. 2021;8(5):387–404. doi:10.1016/S2215-0366(21)00039-0
38. Lin D, Thompson-Leduc P, Ghelerter I, et al. Real-world evidence of the clinical and economic impact of long-acting injectable versus oral antipsychotics among patients with schizophrenia in the United States: a systematic review and meta-analysis. CNS Drugs. 2021;35(5):469–481. doi:10.1007/s40263-021-00815-y
39. Saucedo Uribe E, Carranza Navarro F, Guerrero Medrano AF, et al. Preliminary efficacy and tolerability profiles of first versus second-generation Long-Acting Injectable Antipsychotics in schizophrenia: a systematic review and meta-analysis. J Psychiatr Res. 2020;129:222–233. doi:10.1016/j.jpsychires.2020.06.013
40. Olagunju AT, Clark SR, Baune BT. Long-acting atypical antipsychotics in schizophrenia: a systematic review and meta-analyses of effects on functional outcome. Aust N Z J Psychiatry. 2019;53(6):509–527. doi:10.1177/0004867419837358
41. Pae CU, Wang SM, Han C, et al. Comparison between long-acting injectable aripiprazole versus paliperidone palmitate in the treatment of schizophrenia: systematic review and indirect treatment comparison. Int Clin Psychopharmacol. 2017;32(5):235–248. doi:10.1097/YIC.0000000000000177
42. Kishi T, Matsunaga S, Iwata N. Mortality risk associated with long-acting injectable antipsychotics: a systematic review and meta-analyses of randomized controlled trials. Schizophr Bull. 2016;42(6):1438–1445. doi:10.1093/schbul/sbw043
43. Ostuzzi G, Bighelli I, So R, Furukawa TA, Barbui C. Does formulation matter? A systematic review and meta-analysis of oral versus long-acting antipsychotic studies. Schizophr Res. 2017;183:10–21. doi:10.1016/j.schres.2016.11.010
44. Andreasen NC, Carpenter WT, Kane JM, Lasser RA, Marder SR, Weinberger DR. Remission in schizophrenia: proposed criteria and rationale for consensus. Am J Psychiatry. 2005;162(3):441–449. doi:10.1176/appi.ajp.162.3.441
45. Hasan A, Falkai P, Wobrock T, et al. World Federation of Societies of Biological Psychiatry (WFSBP) guidelines for biological treatment of schizophrenia, part 2: update 2012 on the long-term treatment of schizophrenia and management of antipsychotic-induced side effects. World J Biol Psychiatry. 2013;14(1):2–44. doi:10.3109/15622975.2012.739708
46. Johnson DA. Historical perspective on antipsychotic long-acting injections. Br J Psychiatry Suppl. 2009;52:S7–S12. doi:10.1192/bjp.195.52.s7
47. Taylor D. Establishing a dose–response relationship for haloperidol decanoate. Psychiatr Bull. 2005;29(3):104–107. doi:10.1192/pb.29.3.104
48. Ehret MJ, Davis E, Luttrell SE, Clark C. Aripiprazole lauroxil nanoCrystal® dispersion technology (Aristada Initio®). Clin Schizophr Relat Psychoses. 2018;12(2):92–96. doi:10.3371/CSRP.EHDA071918
49. Hard ML, Mills RJ, Sadler BM, Turncliff RZ, Citrome L. Aripiprazole lauroxil: pharmacokinetic profile of this long-acting injectable antipsychotic in persons with schizophrenia. J Clin Psychopharmacol. 2017;37(3):289–295. doi:10.1097/JCP.0000000000000691
50. Turncliff R, Hard M, Du Y, Risinger R, Ehrich EW. Relative bioavailability and safety of aripiprazole lauroxil, a novel once-monthly, long-acting injectable atypical antipsychotic, following deltoid and gluteal administration in adult subjects with schizophrenia. Schizophr Res. 2014;159(2–3):404–410. doi:10.1016/j.schres.2014.09.021
51. Luedecke D, Schöttle D, Karow A, Lambert M, Naber D. Post-injection delirium/sedation syndrome in patients treated with olanzapine pamoate: mechanism, incidence, and management. CNS Drugs. 2015;29(1):41–46. doi:10.1007/s40263-014-0216-9
52. Carter NJ. Extended-release intramuscular paliperidone palmitate: a review of its use in the treatment of schizophrenia. Drugs. 2012;72(8):1137–1160. doi:10.2165/11208640-000000000-00000
53. Citrome L. New second-generation long-acting injectable antipsychotics for the treatment of schizophrenia. Expert Rev Neurother. 2013;13(7):767–783. doi:10.1586/14737175.2013.811984
54. Jann MW, Penzak SR. Long-acting injectable second-generation antipsychotics: an update and comparison between agents. CNS Drugs. 2018;32(3):241–257. doi:10.1007/s40263-018-0508-6
55. Chue P, Eerdekens M, Augustyns I, et al. Comparative efficacy and safety of long-acting risperidone and risperidone oral tablets. Eur Neuropsychopharmacol. 2005;15(1):111–117. doi:10.1016/j.euroneuro.2004.07.003
56. Andorn A, Graham J, Csernansky J, et al. Monthly extended-release risperidone (RBP-7000) in the treatment of schizophrenia: results from the phase 3 Program. J Clin Psychopharmacol. 2019;39(5):428–433. doi:10.1097/JCP.0000000000001076
57. Carrà G, Crocamo C, Bartoli F, et al. First-generation antipsychotics and QTc: any role for mediating variables? Hum Psychopharmacol. 2016;31(4):313–318. doi:10.1002/hup.2540
58. Barbui C, Bighelli I, Carrà G, et al. Antipsychotic dose mediates the association between polypharmacy and corrected QT interval. PLoS One. 2016;11(2):e0148212. doi:10.1371/journal.pone.0148212
59. Aguglia A, Fusar-Poli L, Natale A, et al. Factors associated with medication adherence to long-acting injectable antipsychotics: results from the STAR Network depot study. Pharmacopsychiatry. 2022;55:281–289. doi:10.1055/a-1804-6211
60. Bartoli F, Cavaleri D, Callovini T, et al. Comparing 1-year effectiveness and acceptability of once-monthly paliperidone palmitate and aripiprazole monohydrate for schizophrenia spectrum disorders: findings from the STAR network depot study. Psychiatry Res. 2022;309:114405. doi:10.1016/j.psychres.2022.114405
61. Kane JM, Kishimoto T, Correll CU. Assessing the comparative effectiveness of long-acting injectable vs. oral antipsychotic medications in the prevention of relapse provides a case study in comparative effectiveness research in psychiatry. J Clin Epidemiol. 2013;66(8 Suppl):S37–S41. doi:10.1016/j.jclinepi.2013.01.012
62. Ereshefsky L, Mascarenas CA. Comparison of the effects of different routes of antipsychotic administration on pharmacokinetics and pharmacodynamics. J Clin Psychiatry. 2003;64(Suppl 16):18–23.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.