Back to Journals » International Journal of General Medicine » Volume 18
Practical Applications of Artificial Intelligence Diagnostic Systems in Fundus Retinal Disease Screening
Authors Wei Q, Chi L, Li M, Qiu Q, Liu Q
Received 18 November 2024
Accepted for publication 9 February 2025
Published 1 March 2025 Volume 2025:18 Pages 1173—1180
DOI https://doi.org/10.2147/IJGM.S507100
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Satish Nair
Qingquan Wei,1 Lifang Chi,2 Meiling Li,3 Qinghua Qiu,1 Qing Liu1
1Department of Ophthalmology, Tong Ren Hospital, Shanghai Jiao Tong University School of Medicine, Shanghai, People’s Republic of China; 2Department of Anesthesia and Operating Room, Tong Ren Hospital, Shanghai Jiao Tong University School of Medicine, Shanghai, People’s Republic of China; 3Department of Ophthalmology, Shigatse People’s Hospital, Shigatse, Xizang, People’s Republic of China
Correspondence: Qinghua Qiu; Qing Liu, Department of Ophthalmology, Tong Ren Hospital, Shanghai Jiao Tong University School of Medicine, 1111 Xianxia West Road, Shanghai, People’s Republic of China, Email [email protected]; [email protected]
Purpose: This study aims to evaluate the performance of a deep learning-based artificial intelligence (AI) diagnostic system in the analysis of retinal diseases, assessing its consistency with expert diagnoses and its overall utility in screening applications.
Methods: A total of 3076 patients attending our hospital underwent comprehensive ophthalmic examinations. Initial assessments were performed using the AI, the Comprehensive AI Retinal Expert (CARE) system, followed by thorough manual reviews to establish final diagnoses. A comparative analysis was conducted between the AI-generated results and the evaluations by senior ophthalmologists to assess the diagnostic reliability and feasibility of the AI system in the context of ophthalmic screening.
Results: : The AI diagnostic system demonstrated a sensitivity of 94.12% and specificity of 98.60% for diabetic retinopathy (DR); 89.50% sensitivity and 98.33% specificity for age-related macular degeneration (AMD); 91.55% sensitivity and 97.40% specificity for suspected glaucoma; 90.77% sensitivity and 99.10% specificity for pathological myopia; 81.58% sensitivity and 99.49% specificity for retinal vein occlusion (RVO); 88.64% sensitivity and 99.18% specificity for retinal detachment; 83.33% sensitivity and 99.80% specificity for macular hole; 82.26% sensitivity and 99.23% specificity for epiretinal membrane; 94.55% sensitivity and 97.82% specificity for hypertensive retinopathy; 83.33% sensitivity and 99.74% specificity for myelinated fibers; and 75.00% sensitivity and 99.95% specificity for retinitis pigmentosa. Additionally, the system exhibited notable performance in screening for other prevalent conditions, including DR, suspected glaucoma, suspected glaucoma, pathological myopia, and hypertensive retinopathy.
Conclusions: : The AI-assisted screening system exhibits high sensitivity and specificity for a majority of retinal diseases, suggesting its potential as a valuable tool for screening practices. Its implementation is particularly beneficial for grassroots and community healthcare settings, facilitating initial diagnostic efforts and enhancing the efficacy of tiered ophthalmic care, with important implications for broader clinical adoption.
Keywords: artificial intelligence, retinal diseases, screening
Introduction
As the global population ages and the incidence of chronic diseases rises, retinal diseases have emerged as a significant public health concern.1 Among these conditions, proliferative diabetic retinopathy (PDR) and diabetic macular edema (DME) represent prevalent retinal vascular disorders, with their prevalence steadily increasing.2,3 Early screening and timely intervention have the potential to prevent the ocular damage associated with these diseases.4,5 However, the uneven distribution of healthcare resources and a notable shortage of ophthalmologists render large-scale manual screenings impractical.6 This context has spurred a growing interest in developing reliable and cost-effective screening methodologies for retinal diseases.
The rapid advancements in artificial intelligence (AI) technology, particularly deep learning-based diagnostic systems, have unveiled substantial potential within the medical field.7–10 These AI systems have been extensively applied in ophthalmic imaging, particularly for the detection of diabetic retinopathy (DR), glaucoma, age-related macular degeneration, and various retinal lesions.11–15 The integration of AI and deep learning technologies has facilitated routine large-scale DR screenings and screenings in underserved areas.4,16,17
In this study, the AI technology utilized has undergone prospective validation in a national cohort encompassing over 200,000 individuals.18 Our artificial intelligence is based on Comprehensive AI Retinal Expert (CARE), a single Convolutional Neural Network (CNN) model that is computationally efficient, offering lower computational costs compared to ensembles of binary Deep Learning Systems (DLSs) for individual abnormality detections. Leveraging this robust foundation, we aim to systematically analyze the application of AI technology in screening for retinal diseases, comparing its diagnostic outcomes with those of expert practitioners. The results of this research will contribute to an efficient, cost-effective, and broadly accessible solution for managing eye diseases among patients in our community.
Materials and Methods
Study Subjects
This study comprised 3076 participants recruited between March 1, 2024, and August 31, 2024. All participants were evaluated using a system based on the previously reported Comprehensive Artificial Intelligence Retinal Expert (CARE) system,18 and clinical data—including age, gender, history of chronic diseases, and retinal symptoms—were systematically recorded. The exclusion criteria included: (1) patients with corneal diseases, cataracts, vitreous opacities, or other conditions that could compromise the quality of color fundus images; (2) individuals with mental disorders or pregnant women who were unable to cooperate.
All research protocols adhered to the principles outlined in the Declaration of Helsinki. All participants were included in the study after providing written informed consent, and those under the age of 18 were included only after obtaining written informed consent from their parents or legal guardians. This study received ethical approval from the Research Ethics Committee of Tong Ren Hospital, Shanghai Jiao Tong University School of Medicine (Approval Number: K2024-033-01).
Fundus Image Acquisition and Diagnostic Standards
Each participant underwent bilateral fundus examinations conducted using a fully automated non-mydriatic fundus camera (Airdoc, AI-FD16aF) and the images generated by the portable camera are 40-degree field images. The acquired color fundus images were comprehensively assessed in a double-blind manner by two associate chief ophthalmologists specializing in retinal diseases. When their diagnoses were consistent, a final diagnosis was established directly. In cases of diagnostic disagreement, a third chief ophthalmologist specializing in retinal diseases was consulted for a collaborative diagnosis, resulting in a definitive conclusion. The prevalence of fundus diseases was subsequently calculated. Additionally, the diagnostic results from the AI reading system were evaluated for consistency with expert diagnoses, while also assessing the screening performance for fundus diseases and analyzing the performance metrics.
Statistical Analysis
Statistical analyses were conducted utilizing SPSS version 25.0 and R version 3.6.1. Categorical variables were represented as counts and percentages, while continuous variables were reported as means and standard deviations. The diagnostic performance of the screening tests was assessed in terms of sensitivity, specificity, positive predictive value, and negative predictive value. Prevalence rates were determined using point estimates along with 95% confidence intervals, providing a robust evaluation of the diagnostic efficacy.
Results
Demographic and Clinical Characteristics
This study encompassed 3,076 participants, leading to the collection of 6,152 retinal fundus images. Among the included patients, 1,495 (48.7%) reported no comorbid systemic conditions; 742 (24.1%) had diabetes mellitus, 181 had Type 1 diabetes, and 561 had Type 2 diabetes; 586 (19.1%) had hypertension; 191 (6.2%) had heart disease; and 62 (2.0%) suffered from other systemic ailments. The age distribution of the participants ranged from 6 to 95 years, with 2,890 males (49.6%) and 1,960 females (50.4%) (Table 1).
 |
Table 1 Clinical Characteristics of the Patients |
Evaluation of Fundus Disease Screening Program
Among all the screened subjects included in this study, and after rigorous evaluation by senior ophthalmologists, the statistics for the positive detection of various fundus diseases are as follows: The positive detection rate for DR is 2.2% (136/6152), for AMD it is 3.9% (238/6152), for possible glaucoma it stands at 4.8% (296/6152), for pathological myopia it is 2.1% (130/ 6152), for retinal vein occlusion it is 0.6% (38/6152), for retinal detachment it is 0.7% (44/6152), for macular hole it is 0.3% (18/6152), for epiretinal macular membrane it is 1% (62/6152), for hypertensive retinopathy it reaches 3.3% (202/6152), for myelinated fibers it is 0.4% (24/6152), and finally, for retinitis pigmentosa, the positive detection rate is negligible at 0% (4/ 6152) (Table 2).
 |
Table 2 Overview of Fundus Disease Screening |
AI-Assisted Screening and Evaluation of Ocular Fundus Diseases
The AI screening and evaluation system achieved a sensitivity of 94.12% (95% CI 88.36~97.24) and a specificity of 98.60% (95% CI 98.27~98.88) in diabetic retinopathy (DR) compared to expert diagnoses. Consistency testing yielded a Kappa coefficient of 0.724 (P<0.001), indicating a high level of agreement. The ROC curve was further plotted (Figure 1A), with an AUC of 0.963. For age-related macular degeneration (AMD), the system showed a sensitivity of 89.50% (95% CI 84.71~92.96) and a specificity of 98.33% (95% CI 97.96~98.63) compared to expert diagnoses. Consistency testing yielded a Kappa coefficient of 0.761 (P<0.001), indicating a high level of agreement. The ROC curve was further plotted (Figure 1B), with an AUC of 0.939. In suspected glaucoma, the system showed a sensitivity of 91.55% (95% CI 87.64~94.35) and a specificity of 97.40% (95% CI 96.96~97.79) compared to expert diagnoses. Consistency testing yielded a Kappa coefficient of 0.738 (P<0.001), indicating a high level of agreement. The ROC curve was further plotted (Figure 1C), with an AUC of 0.945. For pathological myopia, the system showed a sensitivity of 90.77% (95% CI 84.10~94.93) and a specificity of 99.10% (95% CI 98.82~99.32) compared to expert diagnoses. Consistency testing yielded a Kappa coefficient of 0.773 (P<0.001), indicating a high level of agreement. The ROC curve was further plotted (Figure 1D), with an AUC of 0.949. In retinal vein occlusion, the system showed a sensitivity of 81.58% (95% CI 65.11~91.68) and a specificity of 99.49% (95% CI 99.27~99.65) compared to expert diagnoses. Consistency testing yielded a Kappa coefficient of 0.611 (P<0.001), indicating a high level of agreement. The ROC curve was further plotted (Figure 1E), with an AUC of 0.905. For retinal detachment, the system showed a sensitivity of 88.64% (95% CI 74.65~95.74) and a specificity of 99.18% (95% CI 98.91~99.39) compared to expert diagnoses. Consistency testing yielded a Kappa coefficient of 0.578 (P<0.001), indicating moderate agreement. The ROC curve was further plotted (Figure 1F), with an AUC of 0.939. In macular hole, the system showed a sensitivity of 83.33% (95% CI 57.74~95.59) and a specificity of 99.80% (95% CI 99.65~99.89) compared to expert diagnoses. Consistency testing yielded a Kappa coefficient of 0.769 (P<0.001), indicating a high level of agreement. The ROC curve was further plotted (Figure 1G), with an AUC of 0.916. For epiretinal membrane, the system showed a sensitivity of 82.26% (95% CI 70.05~90.40) and a specificity of 99.23% (95% CI 98.97~99.43) compared to expert diagnoses. Consistency testing yielded a Kappa coefficient of 0.629 (P<0.001), indicating a high level of agreement. The ROC curve was further plotted (Figure 1H), with an AUC of 0.907. For hypertensive retinopathy, the system showed a sensitivity of 94.55% (95% CI 90.21~97.11) and a specificity of 97.82% (95% CI 97.40~98.16) compared to expert diagnoses. Consistency testing yielded a Kappa coefficient of 0.718 (P<0.001), indicating a high level of agreement. The ROC curve was further plotted (Figure 1I), with an AUC of 0.962. In myelinated fibers, the system showed a sensitivity of 83.33% (95% CI 61.81~94.52) and a specificity of 99.74% (95% CI 99.56~99.85) compared to expert diagnoses. Consistency testing yielded a Kappa coefficient of 0.700 (P<0.001), indicating a high level of agreement. The ROC curve was further plotted (Figure 1J), with an AUC of 0.916. For retinitis pigmentosa, the system showed a sensitivity of 75.00% (95% CI 21.94~98.68) and a specificity of 99.95% (95% CI 99.84~99.99) compared to expert diagnoses. Consistency testing yielded a Kappa coefficient of 0.600 (P<0.001), indicating moderate agreement. The ROC curve was further plotted (Figure 1K), with an AUC of 0.875.(Table 3) Figure 2 demonstrated normal fundus photographs, abnormal fundus photographs, and the analysis results from the AI software. Figure 2A illustrated the AI software’s analysis results for a normal fundus photograph, while Figures 2B and C showed the DR and ERM fundus photographs, respectively, along with the AI software’s analysis results. Figure 2D presented the analysis of a misclassified image: the patient’s left eye with AMD was only identified as having macular abnormalities.
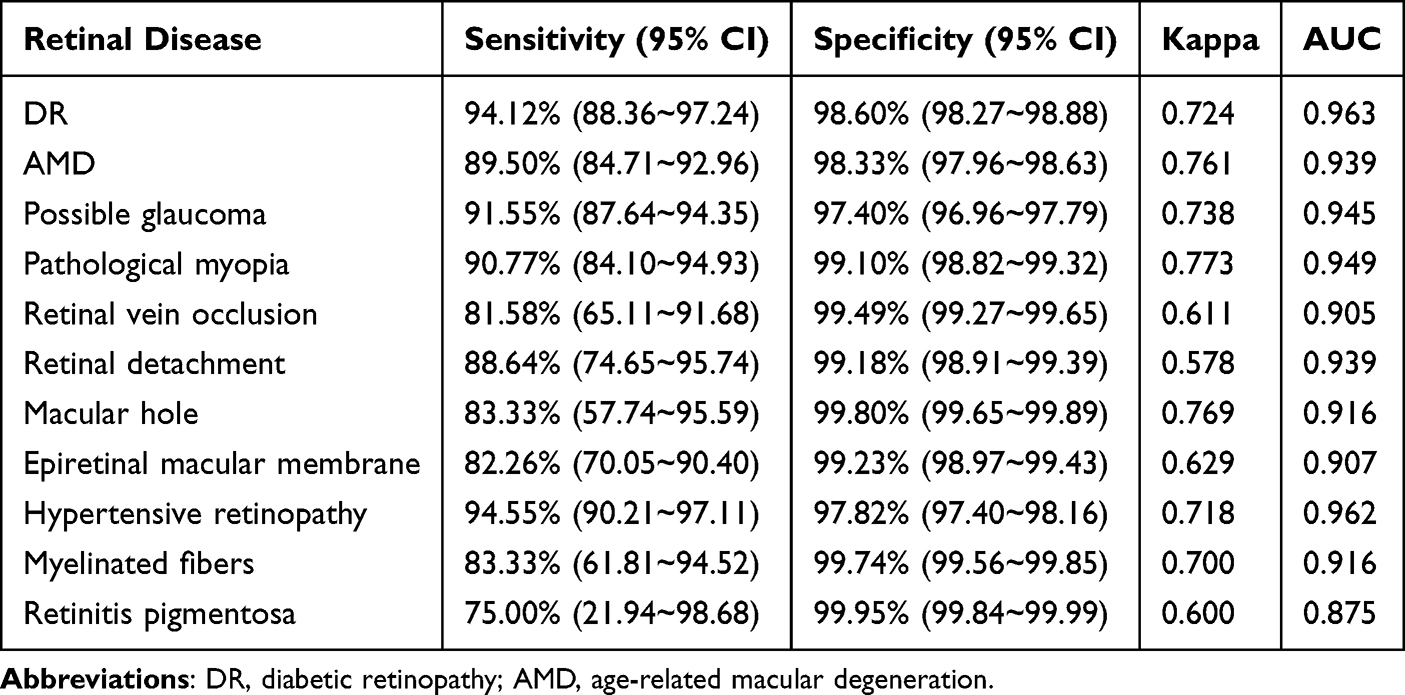 |
Table 3 ROC Curves for AI Diagnosis of Retinal Diseases |
 |
Figure 1 Receiver Operating Characteristic (ROC) curves for AI diagnosis of retinal diseases. (A) Diabetic retinopathy (DR); (B) Age-related macular degeneration (AMD); (C) Possible glaucoma; (D) Pathological myopia; (E) Retinal vein occlusion; (F) Retinal detachment; (G) Macular hole; (H) Epiretinal macular membrane; (I) Hypertensive retinopathy; (J) Myelinated fibers; (K) Retinitis pigmentosa. |
 |
Figure 2 Examples of normal fundus photographs and abnormal fundus photographs with the analysis results from the AI software. (A) Analysis of a normal fundus photograph; (B) Analysis of a diabetic retinopathy (DR) fundus photograph; (C) Analysis of an epiretinal membrane (ERM) fundus photograph; (D) Analysis of a misclassified case: the patient’s left eye with age-related macular degeneration (AMD) was only identified as having macular abnormalities. |
Discussion
The advent of multi-disease AI screening for fundus pathology marks a significant advancement over traditional single-disease screening approaches, such as those targeting DR.11,13,19,20 This innovative screening model simultaneously addresses multiple blinding eye conditions, which has not yet been realized in commercially available medical device software, either domestically or internationally. Prior investigations have conducted multi-center validations of artificial intelligence systems for detecting a range of fundus diseases or confirming normal fundus status. For instance, Burlina et al established a deep learning model utilizing a large dataset to detect 12 types of retinal anomalies, achieving diagnostic accuracies comparable to those of clinical experts, with average AUC values surpassing 95%. However, this research was limited by the model’s focus on identifying abnormalities rather than specific retinal diseases, rendering it unsuitable for direct screening applications.21 In a more recent study, Lin et al developed a robust deep learning-based system capable of identifying 14 retinal diseases, exceeding the 10 diseases evaluated in our current research.18 The study utilizes the AI fundus camera for multi-disease screening within a real-world clinical setting, contributing to the validation of multi-disease AI technology in relation to the observed disease distribution in our sample population.
This study demonstrated the AI’s diagnostic performance characteristics across 11 pathologies, showcasing sensitivities ranging from 75.00% to 94.55%, specificities from 97.40% to 99.74%, Kappa coefficients of at least 0.600 (P<0.001), and AUC values of 0.905 or more. These results indicate that AI has the potential to deliver autonomous and automated feedback within healthcare settings and to generate referral recommendations, thus addressing disparities in resource allocation and enhancing the diagnostic capabilities of primary care institutions across various regions. Moreover, the integration of AI technology with the clinical assessments performed by ophthalmologists yielded similar diagnostic accuracy to those obtained through examinations conducted solely by ophthalmologists, while concomitantly significantly reducing examination duration. The CARE system implemented has exhibited robust diagnostic capabilities in multi-disease classification tasks.22 However, it’s recognized that increasing the number of disease categories can lead to a decrease in diagnostic accuracy. To mitigate this, we need to employ advanced techniques such as data augmentation to enhance sample diversity, integrate multi-modal data fusion to leverage complementary information from different data sources, and implement hierarchical classification strategies to systematically categorize diseases at different levels of granularity. These approaches are anticipated to improve the precision of retinal abnormality screening in a multi-disease context, thereby enhancing clinical outcomes.
Nevertheless, this study is not without limitations. Firstly, it is a retrospective, single-center investigation. Secondly, the AI’s diagnostic capabilities are based on analysis of a single fundus color photograph, necessitating future studies to incorporate patient medical history and other multimodal diagnostic modalities for comprehensive diagnosis. Furthermore, the non-mydriatic camera, which provides only a 40-degree field of view, may compromise the diagnostic accuracy for conditions such as RP or partial RD, where the pathology is primarily localized to the peripheral retina while the macula remains unaffected. Lastly, the sample sizes for certain conditions were limited. Consequently, future research should aim to aggregate a larger volume of ophthalmic examination results. By harnessing advanced big data techniques, this endeavor will facilitate the development of a comprehensive deep learning-based fundus disease screening and diagnostic system, continually enhancing the AI diagnostic framework to optimize the efficiency and intelligence of healthcare services.
Conclusion
In conclusion, the AI screening system exhibits elevated sensitivity and specificity for the majority of retinal diseases (with the exception of certain peripheral retinal manifestations), establishing its suitability for screening applications in ophthalmology. This system is particularly beneficial for primary and community healthcare facilities in facilitating the initial diagnosis of fundus conditions, thereby reinforcing the implementation of a tiered ophthalmic care model. Such advancements not only enhance diagnostic precision but also optimize the allocation of healthcare resources, ultimately promoting improved patient outcomes and systemic efficiency.
Availability of Data and Materials
The original contributions presented in the present study are included in the article material. Further inquiries can be directed to the corresponding authors.
Ethics Approval and Consent to Participate
All procedures of this study were in accordance with the tenets of the Declaration of Helsinki and approved by the medical ethics committee.
Patient Consent for Publication
All Patients declare that they consent for publication.
Acknowledgment
We would like to thank all patients and healthy people who participated in this study.
Funding
This study was supported by the Shanghai Key Laboratory of Ocular Fundus Diseases (No. 20180801), the 6th Three-year Action Program of Shanghai Municipality for Strengthening the Construction of Public Health System (No. GWVI-11.1-30), the Changning District Health and Family Planning Commission Fund (No. 2022QN04), Scientific Research Fund of Compound Chinese Medicine for the Treatment of diabetes Microangiopathy (No. Z-2017-26-2302), the Research Fund of Shanghai Tongren Hospital, Shanghai Jiaotong University School Medicine (No. TRYJ2024LC07), the Norman Bethune Public Welfare Foundation’s “Bright Vision,Bathing in Light” Project (No.BCF-KH-YK-20240906-12), Shanghai Municipal Health Commission Clinical Research Special Project in the Health Industry (No.20244Y0213) and High Altitude Ocular Disease Research Center of People’s Hospital of Shigatse City and Tongren Hospital Affiliated to Shanghai Jiao Tong University School of Medicine, P. R. China.
Disclosure
The authors declare that they have no competing interests.
References
1. Sun Y, Li F, Liu Y, et al. Targeting inflammasomes and pyroptosis in retinal diseases-molecular mechanisms and future perspectives. Prog Retin Eye Res. 2024;101:101263. doi:10.1016/j.preteyeres.2024.101263
2. Lundeen EA, Burke-Conte Z, Rein DB, et al. Prevalence of diabetic retinopathy in the US in 2021. JAMA Ophthalmol. 2023;141(8):747–754. doi:10.1001/jamaophthalmol.2023.2289
3. Lundeen EA, Kim M, Rein DB, et al. Trends in the prevalence and treatment of diabetic macular edema and vision-threatening diabetic retinopathy among commercially insured adults aged <65 years. Diabetes Care. 2023;46(4):687–696. doi:10.2337/dc22-1834
4. Dai L, Wu L, Li H, et al. A deep learning system for detecting diabetic retinopathy across the disease spectrum. Nat Commun. 2021;12(1):3242. doi:10.1038/s41467-021-23458-5
5. Vujosevic S, Aldington SJ, Silva P, et al. Screening for diabetic retinopathy: new perspectives and challenges. Lancet Diabetes Endocrinol. 2020;8(4):337–347. doi:10.1016/S2213-8587(19)30411-5
6. Berkowitz ST, Finn AP, Parikh R, Kuriyan AE, Patel S. ophthalmology workforce projections in the United States, 2020 to 2035. Ophthalmology. 2024;131(2):133–139. doi:10.1016/j.ophtha.2023.09.018
7. Bhinder B, Gilvary C, Madhukar NS, Elemento O. Artificial intelligence in cancer research and precision medicine. Cancer Discov 2021;11(4):900–915.
8. Mullowney MW, Duncan KR, Elsayed SS, et al. Artificial intelligence for natural product drug discovery. Nat Rev Drug Discov. 2023;22(11):895–916. doi:10.1038/s41573-023-00774-7
9. Lotter W, Hassett MJ, Schultz N, Kehl KL, Van Allen EM, Cerami E. Artificial intelligence in oncology: current landscape, challenges, and future directions. Cancer Discov. 2024;14(5):711–726. doi:10.1158/2159-8290.CD-23-1199
10. Perez-Lopez R, Ghaffari Laleh N, Mahmood F, Kather JN. A guide to artificial intelligence for cancer researchers. Nat Rev Cancer. 2024;24(6):427–441. doi:10.1038/s41568-024-00694-7
11. Wolf J, Rasmussen DK, Sun YJ, et al. Liquid-biopsy proteomics combined with AI identifies cellular drivers of eye aging and disease in vivo. Cell. 2023;186(22):4868–4884e4812. doi:10.1016/j.cell.2023.09.012
12. Dai L, Sheng B, Chen T, et al. A deep learning system for predicting time to progression of diabetic retinopathy. Nat Med. 2024;30(2):584–594. doi:10.1038/s41591-023-02702-z
13. Li JO, Liu H, Ting DSJ, et al. Digital technology, tele-medicine and artificial intelligence in ophthalmology: a global perspective. Prog Retin Eye Res. 2021;82:100900. doi:10.1016/j.preteyeres.2020.100900
14. Li F, Su Y, Lin F, et al.. A deep-learning system predicts glaucoma incidence and progression using retinal photographs. J Clin Invest. 2022;132(11). doi:10.1172/JCI157968
15. Yim J, Chopra R, Spitz T, et al. Predicting conversion to wet age-related macular degeneration using deep learning. Nat Med. 2020;26(6):892–899. doi:10.1038/s41591-020-0867-7
16. Schmidt-Erfurth U, Sadeghipour A, Gerendas BS, Waldstein SM, Bogunovic H. Artificial intelligence in retina. Prog Retin Eye Res. 2018;67:1–29. doi:10.1016/j.preteyeres.2018.07.004
17. Rajesh AE, Davidson OQ, Lee CS, Lee AY. Artificial intelligence and diabetic retinopathy: ai framework, prospective studies, head-to-head validation, and cost-effectiveness. Diabetes Care. 2023;46(10):1728–1739. doi:10.2337/dci23-0032
18. Lin D, Xiong J, Liu C, et al. Application of Comprehensive Artificial intelligence Retinal Expert (CARE) system: a national real-world evidence study. Lancet Digit Health. 2021;3(8):e486–e495. doi:10.1016/S2589-7500(21)00086-8
19. Wong TY, Bressler NM. Artificial intelligence with deep learning technology looks into diabetic retinopathy screening. JAMA. 2016;316(22):2366–2367. doi:10.1001/jama.2016.17563
20. Wolf RM, Channa R, Liu TYA, et al. Autonomous artificial intelligence increases screening and follow-up for diabetic retinopathy in youth: the ACCESS randomized control trial. Nat Commun. 2024;15(1):421. doi:10.1038/s41467-023-44676-z
21. Burlina P, Paul W, Liu TYA, Bressler NM. Detecting anomalies in retinal diseases using generative, discriminative, and self-supervised deep learning. JAMA Ophthalmol. 2022;140(2):185–189. doi:10.1001/jamaophthalmol.2021.5557
22. Choi JY, Yoo TK, Seo JG, et al. Multi-categorical deep learning neural network to classify retinal images: a pilot study employing small database. PLoS One. 2017;12(11):e0187336. doi:10.1371/journal.pone.0187336
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.