Back to Journals » Clinical Interventions in Aging » Volume 13
PPARgamma-2 and ADRB3 polymorphisms in connective tissue diseases and lipid disorders
Authors Grygiel-Górniak B ![]() , Ziółkowska-Suchanek I, Kaczmarek E, Mosor M, Nowak J, Puszczewicz M
, Ziółkowska-Suchanek I, Kaczmarek E, Mosor M, Nowak J, Puszczewicz M
Received 16 November 2017
Accepted for publication 8 January 2018
Published 22 March 2018 Volume 2018:13 Pages 463—472
DOI https://doi.org/10.2147/CIA.S157186
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Richard Walker
Bogna Grygiel-Górniak,1 Iwona Ziółkowska-Suchanek,2 Elżbieta Kaczmarek,3 Maria Mosor,2 Jerzy Nowak,2 Mariusz Puszczewicz1
1Department of Rheumatology and Internal Diseases, Poznan University of Medical Sciences, Poznan, Poland; 2Institute of Human Genetics, Polish Academy of Sciences, Poznan, Poland; 3Department of Bioinformatics and Computational Biology, Poznan University of Medical Sciences, Poznan, Poland
Background: The aim of the research genetic study was to investigate the association between variants (C1431T and Pro12Ala) of the peroxisome proliferator-activated receptor (PPARgamma-2) gene, Trp64Arg polymorphism of the beta-3-adrenergic receptor gene and lipid profile in Polish population including group of 103 patients with connective tissue disease (CTD) and 103 sex- and age-matched controls in context of statin use.
Methods: Anthropometric and biochemical parameters were measured by routine methods, followed by genotyping (TagMan® Genotyping Assays, PCR-restriction fragment length polymorphism analysis). Nearly 30% of CTD patients used statins and 10% of the control group.
Results: Although there were no differences between alleles and genotypes prevalence between CTD vs control groups, interesting lipid-gene associations were noted in this study. A higher level of triglycerides (TAG) and TAG/high-density lipoprotein (HDL) ratios was observed in CTD patients compared to controls. Similar differences were noted in CTD and control groups without statin treatment. Atherogenic markers: the atherogenic index of plasma, TAG/HDL and low-density lipoprotein/HDL ratio were low in the analyzed groups. Of the six analyzed polymorphisms, the Pro12Pro or C14131C or Trp64Trp genotypes were related to higher TAG and TAG/HDL ratios in patients with CTD; however, the highest TAG values were observed in the presence of the Trp64Trp genotype.
Conclusion: Lipid disorders were present in both groups independent of statin treatment (mixed dyslipidemia and hypercholesterolemia were observed in the CTD and control groups, respectively). The risk of dyslipidemia increases with age. The presence of Pro12Pro, C14131C and Trp64Trp genotypes is related to higher TAG level in CTDs, and of these the Trp64Trp variant most reliably predicts hypertriglyceridemia.
Keywords: C1431T, Pro12Ala, Trp64Arg polymorphisms, lipoproteins, rheumatic diseases, statins
Introduction
Development of atherosclerosis increases with age, and cardiovascular disorder in connective tissue disease (CTD) is related to genetic factors, auto-antibody production, reactivation of lymphocytes and nutritional behavior.1 Dyslipidemia decisively affects the long-term prognosis of autoimmune diseases with regard to cardiovascular events. But the synthesis of proinflammatory cytokines during CTD accelerates this risk.2,3 The development of cardiovascular disorders also depends on PPARgamma-2, which causes metabolic changes and is related to lipid disorders.4,5 For example, the common Pro12Ala polymorphism of PPARgamma-2 is associated with dyslipidemia and many studies suggest its functional and prognostic consequences in cardiometabolic diseases (mainly the protective effect of the Ala12 allele on diabetes and myocardial infarction).6,7 Moreover, activation of the PPARgamma-2 gene changes inflammatory processes and is suspected to participate in the development of CTD, eg, rheumatoid arthritis.7,8 But some studies do not confirm the association of the Pro12Ala polymorphism with rheumatoid arthritis.9 Another PPARgamma-2 polymorphism, C1431T, is associated with the risk of diabetes, obesity, metabolic syndrome and coronary artery disease.10,11 Nevertheless, the role of this polymorphism in CTD is not well defined.7–9
Besides PPARgamma-2, the beta-3-adrenergic receptor (ADRB3) gene influences metabolic and lipid disorders. The Trp64Arg polymorphism of ADRB3 is related to hypertriglyceridemia and increased levels of low-density lipoproteins (LDLs).12 Some studies have shown the association of the Arg64 allele with higher body mass index (BMI) and total cholesterol (TC) level,13 whereas others have not confirmed such correlations.14,15 Thus, the prevalence of the Pro12Ala, C1431T and Trp64Arg polymorphisms needs exploration because their exact effect on metabolic parameters in CTD has not been precisely defined.8,9
In view of the increased cardiovascular risk in CTD, many patients should be monitored for lipid parameters. If hypercholesterolemia is present (elevated LDL level), statins are used as a first-line treatment for prevention of coronary artery disease and reduction of the incidence of heart attack and stroke.16,17 Some data even show the protective effect of these medications against the development of rheumatic arthritis in patients with hyperlipidemia.18 Statins are also effective ligands for PPARalpha and PPARgamma genes.19
Since the specific activity of statins as ligands of PPARgamma-2 and metabolic disorders are related to PPARgamma-2 and ADRB3 gene polymorphisms, we intended to show the associations of the mentioned variants with lipid disorders in the context of hypolipidemic treatment in a group of patients with CTD.
Methods
Study group
In this study, patients with CTD and healthy subjects were involved. Selection of subjects was based on the absence of infectious diseases, cancer, acute renal or liver failure, untreated thyroid disease and use of lipid-lowering medications except for statins. The criteria were used in both groups: CTD and control group.
First, 110 patients with CTD were included in the study; however, 7 patients taking fenofibrate or ezetimibe were eliminated. In summary, 30 patients (29%) with CTD and 10 subjects (9.7%) in control group used statins. All patients with CTD included in the study were on disease-modifying antirheumatic drugs and 72 patients used glucocorticosteroids. The subjects in control group were recruited from Poznan Outpatient Clinic and consisted of subjects without rheumatic diseases. The control group was matched according sex, age, body mass and waist circumference (which determined visceral or gynoidal adiposity), what allowed to select the patient with the same body fat distribution.
As kidney involvement is frequently observed in rheumatic diseases, atorvastatin is mainly used in most patients.20 For calculation of the average dose of statins, the dosage equivalence of HMG-CoA reductase inhibitors was applied. For the statistical analysis, the average dose of simvastatin or rosuvastatin was expressed as mg/day of atrovastatin.21,22 The amount of glucocorticosteroids administered orally (prednisone and methylprednisolone) were transformed into the amount of methylprednisolone (mg/day). The Ethical Committee of Poznan University of Medical Sciences approved this study as protocol no 791/15. All the subjects gave written informed consent. All the procedures used in this study were in accordance with the guidelines of the Helsinki Declaration on Human Experimentations.
Anthropometric evaluation
Weight was measured on a calibrated standard scale with the precision of 0.1 g and height with a cotton ruler. BMI was calculated as weight (kg) to height squared (m2). Waist circumference was evaluated above the iliac crest at the natural waistline.23 Body fat was determined by bioelectrical impedance analysis (Bodystat 1500, Bodystat Ltd, Douglas, UK).
Biochemical analysis
All selected participants underwent a biochemical and genetic parameter measurement following an overnight fast (10–12 hours). Venous blood samples (10.0 mL) were collected into tubes containing EDTA at 7:00 AM. The serum samples were collected from clotted (15 min, room temperature) and centrifuged (15 min, 3,000 × g) blood. TC, triglyceride (TAG) and high-density lipoprotein (HDL) cholesterol were analyzed by enzymatic colorimetric assays (Pentra400, Horiba ABX, Montpellier, France). Serum LDL cholesterol was determined according to the Friedewald formula: LDL cholesterol = TC − (HDL + TAG/5).24 The atherogenic index of plasma (AIP) was defined as Log (TAG/HDL [mmol]).25 Other atherogenic indices were calculated, such as TAG to HDL and LDL to HDL ratios.26,27
Genetic evaluation
A detailed description of the methodology was included in our previous studies.4 DNA samples from patients and controls were isolated from peripheral blood lymphocytes with a GentraPuregene Blood Kit (Qiagen, Hilden, Germany). DNA purity and concentration were confirmed using a NanoDrop ND-1000 spectrophotometer.
We selected those single nucleotide polymorphisms (SNPs) previously associated with CTDs. We chose genomic regions based on a review of the literature and used the most significant reported SNPs, which had been analyzed in relatively large groups of cases. All polymorphisms selected for this study had minor allele frequencies >0.4 to achieve sufficient statistical power. Altogether, two SNPs in PPARgamma-2 gene (rs1801282, rs3856806) and one in β3-AR gene (rs4994) were analyzed.
The SNPs were genotyped using predesigned TaqMan® SNP genotyping assays (Life Technologies, Carlsbad, CA, USA; assay IDs: PPARgamma-2 [rs1801282: C_1129864_10] and β3-AR gene [rs4994: C_2215549_20]). The PCR was performed with HOT FIREPol Probe qPCR Mix Plus (no ROX) according to the manufacturer’s instructions provided by Solis BioDyne (Tartu, Estonia). The PCR thermal cycling was as follows: initial denaturation at 95°C for 15 min; 40 cycles at 95°C for 15 sec and 60°C for 60 sec. Thermal cycling was performed using a CFX96 Touch™ Real-Time PCR Detection System (Bio-Rad, Hercules, CA, USA). As a quality control measure, negative controls and ~5% of samples were genotyped in duplicate to check genotyping accuracy. The genotypes of selected samples were confirmed by direct sequencing (OLIGO, IBB, Warsaw, Poland).
In the case of C1431T (rs3856806) in PPARgamma-2 genes, the PCR-restriction fragment length polymorphism method was applied. The 170 bp PCR product of exon 6 was digested with the Eco72I enzyme (according to the manufacturer’s instructions: Fermentas, Vilnius, Lithuania). Digestion products were separated by 2.5% agarose gel electrophoresis. For wild-type DNA, two bands of 127 bp and 43 bp were present. The wild-type form was not digested by this endonuclease. The genotypes of selected samples were confirmed by direct sequencing (OLIGO, IBB).
Statistical analysis
Each group was then divided into two subgroups according to genotype (Pro12Pro and Pro/Ala+Ala/Ala for Pro12Ala); (C1431C and CT+TT for C1431T); (Trp64Trp and Trp/Arg+Arg/Arg for Trp64Arg). GraphPad PRISM 5 Software (GraphPad, San Diego, CA, USA) was used for statistical calculations. Genotype data were tested for deviations from the Hardy–Weinberg equilibrium. The chi-square test was used to analyze the differences in genotype/allele frequencies between CTD patients and the controls as well as between normotensive and hypertensive patients. The strength of associations between the PPARgamma-2 genotypes (Pro12Ala and C1431T) among studied group and the ADRB3 gene (Trp64Arg) was calculated using logistic regression and expressed as an OR (95% CI), and the differences were considered significant if the value of probability (P) was less than 0.05. Module contingency tables were used in these calculations. For polymorphisms, the wild-type or ancestral genotype/allele served as a reference category.
The distributions of the anthropometrical and biochemical data were tested with the Shapiro–Wilk normality test. If analyzed data were not normally distributed, nonparametric tests were used. Since the number of Ala12Ala homozygotes was small (in both CTD patients and the control group) compared to Pro12Pro homozygotes, these were calculated together with Pro12Ala heterozygotes for all the analyzes and are presented as Ala12/X in Table 1. Similarly, patients with C1431T+T14131T polymorphisms were collapsed together and are presented as T1431/X and in the same way Trp64Arg+Arg64Arg polymorphisms were analyzed as Arg64/X.
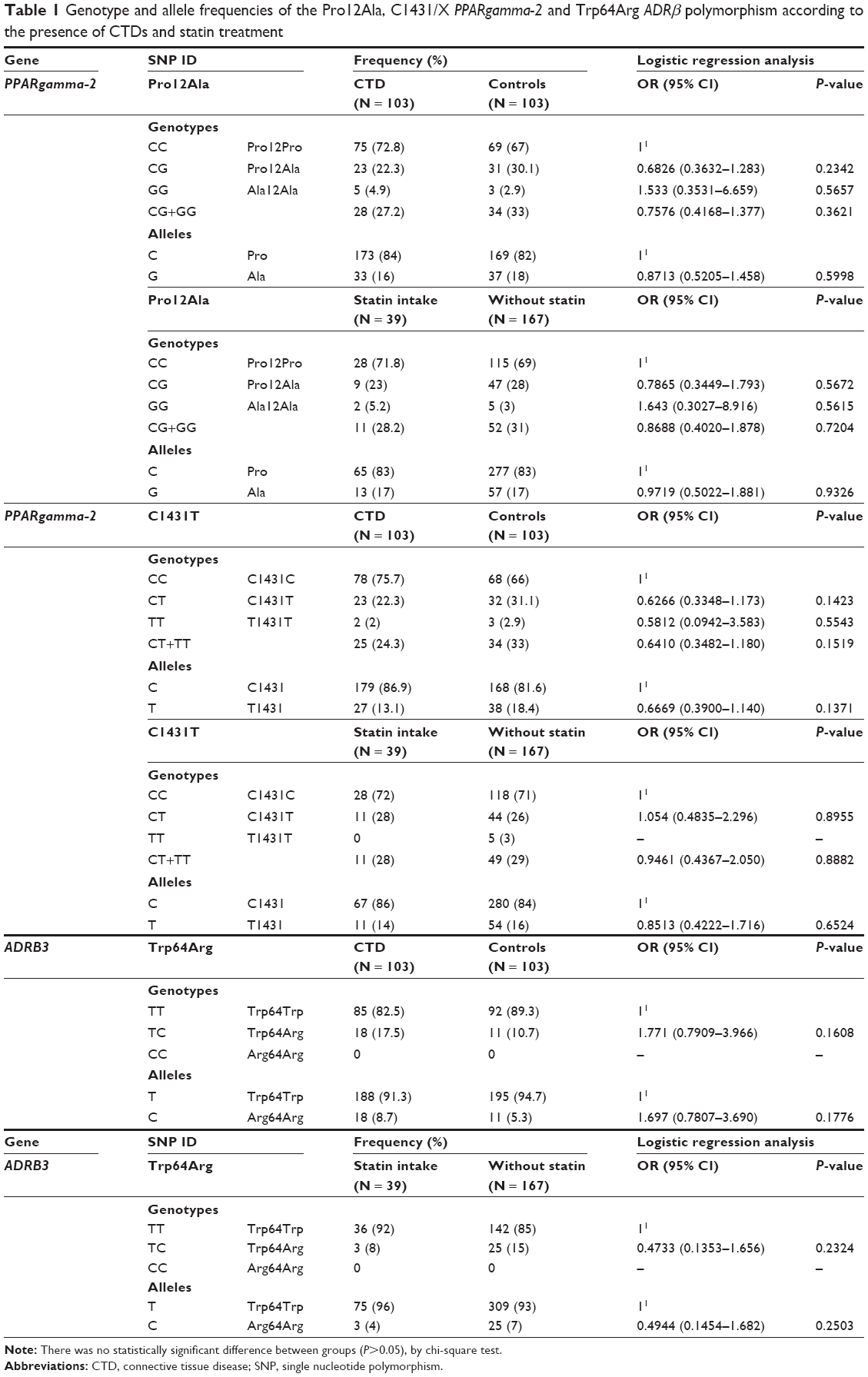 | Table 1 Genotype and allele frequencies of the Pro12Ala, C1431/X PPARgamma-2 and Trp64Arg ADRβ polymorphism according to the presence of CTDs and statin treatment |
The Student’s t-test was used to compare continuous variables between two groups if the data distribution was concordant with the normal distribution (Shapiro–Wilk test). If the data did not meet the aforementioned criteria, the nonparametric Mann–Whitney U-test was used. For normally distributed data, a multifactor analysis of variance analysis was performed to determine whether the dependent variables were significantly different between study and control groups in relation to polymorphism and statin intake. Otherwise, the nonparametric Kruskal–Wallis test was used. A P-value less than 0.05 was regarded as statistically significant. The statistical analyzes were performed with STATISTICA 12 (including STATISTICA Medical Package 2.0; StatSoft, Inc. 2014 software; StatSoft Polska Sp.zo.o., Kraków, Poland) and SPSS 22 (IBM, Inc, Chicago, IL, USA). Associations between analyzed groups (CTD, control group) lipid fractions, polymorphisms, statin and steroids intake were studied by log-linear analysis with maximum likelihood chi-square test.
Results
The prevalence of analyzed genotypes and allele frequencies were comparable in CTD patients and control group (Table 1). The analysis in Table 2 shows that patients with CTD have lower body fat content and LDL level, higher TAG, TAG/HDL ratio and used higher average doses of statin (Table 2A). The analysis of statin treatment (independent of CTD presence) reveals that patients with statin supplementation were older and characterized by higher TAG and TAG/HDL ratios (Table 2B). The comparison of subjects who were not on lipid-lowering treatment revealed that CTD patients were younger, had lower body fat mass and higher TAG and TAG/HDL (Table 2C).
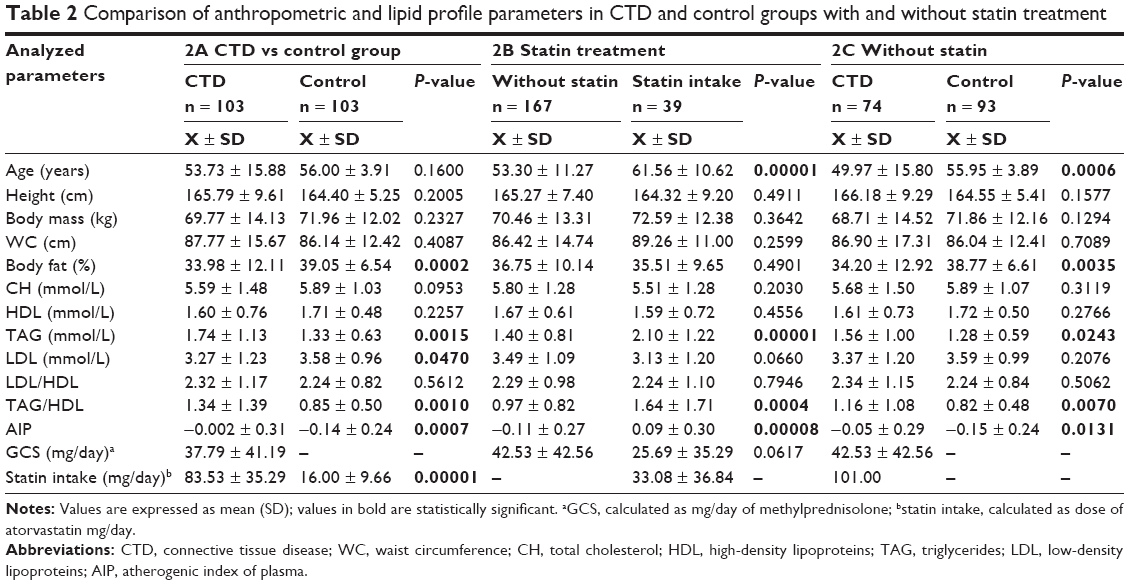 | Table 2 Comparison of anthropometric and lipid profile parameters in CTD and control groups with and without statin treatment |
The genetic analysis presented in Table 3 shows that patients with CTD and Pro12Pro or C14131C or Trp64Arg genotypes have higher TAG level and TAG/HDL ratios compared to the control group (Table 3A). Similar associations between the analyzed genotypes were observed in CTD patients and these showed higher TAG and TAG/HDL ratios in patients using statins when compared to subjects without such treatment (Table 3B). The multifactor analysis of co-existing polymorphisms showed that if the Pro12Pro and C1431C genotypes were present in CTD, the TAG and TAG/HDL ratios were mainly determined by the Trp64Arg variant (Table 3C).
 | Table 3 Multifactor analysis of PPARgamma-2 and ADRB3 polymorphisms in CTD patients and control group in the context of statin treatment |
To study the interactions between analyzed parameters, the log-linear analysis was used and two models were built. In the first model, the interaction between analyzed group (CTD, control), Trp64Trp polymorphism and parameters of lipid profile were tested (maximum-likelihood chi-square test = 0.00209). In the second model, extra variable (statin) was added. Statin increased the influence of HDL on the significance of this model (maximum-likelihood chi-square test = 0.00001). Such relations were not observed if other polymorphisms were analyzed.
Discussion
Cardiovascular risk increases in CTDs and this is associated with auto-antibody production, cytokine synthesis, oxidative stress and dyslipidemia state.28,29 Patients with rheumatoid arthritis have up to 50% increased cardiovascular morbidity and mortality compared to the general population.30 Cardiovascular diseases are the leading cause of death not only in rheumatoid arthritis but also in other CTDs.30,31 Moreover, the lipid paradox is described during CTD as a paradoxical inversion of the relationship between cardiovascular risk and lipid levels in patients with untreated rheumatic arthritis.32 Since PPARgamma-2 is an important regulator of lipid homeostasis and inflammation, it is therefore suspected to affect the development of CTD and related cardiovascular disorders.6–8 However, the exact role of PPARgamma-2 and ADRB3 genes in CTD and the prevalence of selected polymorphisms is not well known. Thus, in this study, we intended to elucidate its genetic role in lipid disorders, which affects the cardiovascular risk during CTD.
In our study, we did not find any differences in genotypes/alleles prevalence between CTD and control group (Table 1). Similar data were observed in a Korean population,9 whereas a higher prevalence of Pro12Ala genotype with rheumatoid arthritis was described in patients from Pakistan.8 An inflammatory status present in chronic diseases is related to lower fat mass, and such changes were also present in the analyzed CTD patients (Table 2A).33,34 Inflammation during CTD is linked to accelerated atherosclerosis and is associated with qualitative as well as quantitative changes in lipoproteins.32 Similarly, in this study, lipoproteins were elevated and patients with CTD were characterized by mixed dyslipidemia (CH > 5.0 mmol/L, LDL > 3.0 mmol/L and TG > 1.7 mmol/L), whereas the control group was characterized by hypercholesterolemia (increased CH and LDL).20,35 The prevalence of dyslipidemia varies in CTD from 20% (hypercholesterolemia in rheumatoid arthritis), through 28% of hypertriglyceridemia in rheumatoid arthritis36 to 36% of patients with systemic lupus erythematosus at diagnosis to 60% after 3 years of the duration of this disease.37 In this study, the prevalence of lipid disorders is comparable if we consider the amount of patients using statins (29%); however, the values of selected fractions of the lipid profile in CTD subjects have still been higher than recommended norms, which indicates a higher occurrence of dyslipidemia in this group.20,35
The comparison of two groups based only on statin treatment (independent of CTD presence) showed that patients with statin supplementation were older (Table 2B). This corresponded to the fact that the risk of dyslipidemia increases with age.38,39 The levels of CH and LDL were higher than the recommended norm in groups with and without statin intake (CH > 5.0 mmol/L and LDL > 3.0 mmol/L). Moreover, higher TAG (> 1.7 mmol/L) and TAG/HDL ratios were observed in the group with statin intake. Statins first have a good effect in lowering the LDL fraction40,41 and are implemented if hypercholesterolemia is diagnosed.20,35 For example, the implementation of atorvastatin or rosuvastatin at a dose of 10 mg/day during 6 weeks diminishes the LDL level by about 36.8% and 45.8%, respectively, and the hypolipemic effect is potentiated with increasing doses.40 Statins also decrease TAG levels (eg, atorvastatin at a dose of 10 mg/day by about 20% while rosuvastatin at 10 mg about 19.8%).41 Supplementation of statins reduces not only cardiovascular risk but also some studies even show that they may lower CTD risk.42 But these medications are also capable of inducing or exacerbating symptoms of rheumatic diseases.43
The comparison of groups without statin intake (Table 2C) showed that CTD patients were younger and had higher TAG and TAG/HDL ratios. Many studies have revealed that dyslipidemia is associated with a variety of inflammatory arthritis such as gout, migratory polyarthritis, early arthritis, rheumatoid arthritis as well as systemic diseases such as systemic lupus erythematosus or vasculitis.18,37,44,45 However, exacerbated inflammatory state is also related to increased levels of lipid fractions.3,46 For example, in rheumatoid arthritis, inflammation alters HDL constituents and the concentration of LDL and HDL. As a result, an increased development of atherosclerosis and cardiovascular disorders is observed. On the other hand, exacerbated inflammatory processes present in many CTD induce atherosclerosis.2 Considering this fact, as systemic inflammation is a background of symptoms in CTD, it can be a prominent contributor to lipid profile changes.47 However, lipid disorders can also modulate inflammation, eg, hypercholesterolemia, directly stimulates inflammation by increasing circulating inflammatory cells.48,49 In this study, levels of CH and LDL higher than the recommended norms were observed in all subjects without lipid-lowering treatment (Table 2C), which indicates a tendency to hypercholesterolemia in this group. Since the levels of CH and LDL were slightly elevated, a new dietary regimen should be implemented in this group as a first step in lipid disorder treatment.20
In recent years, various markers of atherosclerosis and cardiovascular disorders have started to gain importance.25 One of these is the AIP, which predicts the risk of atherosclerosis and coronary heart disease.50,51 An AIP value of under 0.11 is associated with low risk of cardiovascular diseases, whereas a value higher than 0.21 is associated with increased risk of cardiovascular diseases (the values between 0.11 and 0.21 reflect intermediate risk).25,52,53 In our study and independent of the analyzed group in Table 2, the AIP was low, similar to the situation in other atherogenic indices used in the assessment of coronary heart disease risk (LDL/HDL < 3 and TAG/HDL < 5).26,27
Not only statin intake influences the lipid profile54,55 but also genetic background plays a role in dyslipidemia development. Moreover, numerous studies have suggested that PPARgamma-2 gene is activated by statins such as atorvastatin17 or simvastatin.56 The first analysis, presented in Table 3A, compares CTD patients with control groups and both groups are without statin treatment, which could affect the PPARgamma-2 activity. CTD subjects with Pro12Pro or C14131C or Trp64Trp variants have higher TAG levels and TAG/HDL compared to the control group. These data show that such constellations of genotypes can influence the tendency to higher TAG levels in CTD. A similar tendency was observed in patients using statins (Table 3B). Studies describing the association between the analyzed polymorphism in CTD are very scarce. In the general population, the Ala12 allele is related to better lipid profile (higher HDL level and lower TAG and LDL level) when compared to the 12Pro allele.6 There are few studies analyzing the effects of the C1431T or Trp64Arg polymorphisms and most of these do not find significant associations between this gene variants and lipid-related variables in the general population.10,14,15,57,58 In this study, we showed that the presence of Pro12Pro, C14131C or Trp64Trp genotypes is related to lipid disorders in CTD.
Multifactor analyzes of three polymorphisms in CTD patients (Table 3C) revealed that the higher TAG and TAG/HDLs were mainly determined by the presence of the Trp64Trp genotype. In this study, the log-linear analysis of Trp64Trp polymorphism and lipid parameters showed that adding statin to the second model increased the influence of HDL on the significance of this model. In the literature, data on the ADRB3 gene mutation effect on lipid metabolism are inconsistent and heterogeneous.13–15 Some studies do not find any correlation between Arg64 allele and serum lipids,14,15 whereas others show associations with hypertriglyceridemia and increased LDL level.12 Recently published data in hypertensive subjects show a relationship between Trp64Arg genotype and higher BMI and TC level13 and decreased HDL level.59 Since TAG concentration exceeded the recommended 1.7 mmol/L in patients with Trp64Trp genotype, we conclude that the presence of this variant determines the tendency to hypertriglyceridemia.
Conclusion
Patients with CTD were characterized by mixed dyslipidemia, whereas the control group demonstrated hypercholesterolemia. This shows the common tendency to lipid disorders in rheumatic patients and the general population, which increased with age. The analysis of lipoproteins in patients without statin therapy showed hypercholesterolemia in both groups; however, even though the values of TAG and TAG/HDL were within the recommended range, they were higher in CTD patients. This fact suggests a certain propensity to higher TAG levels in CTD patients, when compared to the general population. As the lipoproteins fractions were slightly elevated in the analyzed groups, dietary intervention is needed.
Although the frequency of analyzed alleles and genotypes did not differ between CTD subjects and the control group, the CTD patients with Pro12Pro, C14131C or Trp64Trp variants tended to hypertriglyceridemia, which increases mainly if Trp64Trp genotype is present. Further research is needed to understand fully the changes in lipid profiles in the context of the present polymorphisms. Nevertheless, the tendency to hypertriglyceridemia in CTD is present, which increases with the constellation of Pro12Pro, C1431C and Trp64Trp genotypes. Analysis of the discussed polymorphic variants can help in metabolic risk evaluation in CTD.
Study strengths and limitations
This is the first study showing the relations between lipid disorders in CTD in the context of PPARgamma-2 and ADRB3 gene polymorphisms. However, the present study had some limitations. First, the case–control nature of the study lacks information about the causal relationship between variables. This needs to be elucidated in future prospective studies. Second, the groups of CTD patients and controls should be enlarged to find more detailed information about the relationships between lipid disorders, specific CTD and analyzed polymorphisms.
Acknowledgment
We are especially grateful to our volunteers and patients for their unconditional participation in the study.
Author contributions
BGG: conception or design of the work, data acquisition, data analysis and interpretation, drafting the article, accountability for all aspects of the work (ensuring accuracy or integrity of any part of the work). IZS: data analysis and interpretation, critically revising the article. EK: data analysis and interpretation, critically revising the article, final approval of the version to be published. MM: critically revising the article. JN: final approval of the version to be published. MP: critically revising the article, final approval of the version to be published. All authors contributed toward data analysis, drafting and critically revising the paper and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
Shoenfeld Y, Gerli R, Doria A, et al. Accelerated atherosclerosis in autoimmune rheumatic diseases. Circulation. 2005;112(21):3337–3347. | ||
Cavagna L, Boffini N, Cagnotto G, Inverardi F, Grosso V, Caporali R. Atherosclerosis and rheumatoid arthritis: more than a simple association. Mediators Inflamm. 2012;2012:147354. | ||
Ku IA, Imboden JB, Hsue PY, Ganz P. Rheumatoid arthritis: model of systemic inflammation driving atherosclerosis. Circ J. 2009;73(6):977–985. | ||
Grygiel-Gorniak B, Mosor M, Marcinkowska J, Przyslawski J, Nowak J. Impact of the PPAR gamma-2 gene polymorphisms on the metabolic state of postmenopausal women. J Biosci. 2016;41(3):427–437. | ||
Grygiel-Górniak B. Peroxisome proliferator-activated receptors and their ligands: nutritional and clinical implications – a review. Nutr J. 2014;13:17. | ||
Pihlajamäki J, Schwab U, Kaminska D, et al. Dietary polyunsaturated fatty acids and the Pro12Ala polymorphisms of PPARG regulate serum lipids through divergent pathways: a randomized crossover clinical trial. Genes Nutr. 2015;10(6):43. | ||
Regieli JJ, Jukema JW, Doevendans PA, et al. PPAR gamma variant influences angiographic outcome and 10-year cardiovascular risk in male symptomatic coronary artery disease patients. Diabetes Care. 2009;32(5):839–844. | ||
Jalil SF, Ahmed I, Gauhar Z, et al. Association of Pro12Ala (rs1801282) variant of PPAR gamma with rheumatoid arthritis in a Pakistani population. Rheumatol Int. 2014;34(5):699–703. | ||
El-Sohemy A, Cornelis MC, Park YW, Bae SC. Catalase and PPARgamma2 genotype and risk of rheumatoid arthritis in Koreans. Rheumatol Int. 2006;26(5):388–392. | ||
Doney A, Fischer B, Frew D, et al. Haplotype analysis of the PPARgamma Pro12Ala and C1431T variants reveals opposing associations with body weight. BMC Genet. 2002;3:21. | ||
Zhou X, Chen J, Xu W. Association between C1431T polymorphism in peroxisome proliferator-activated receptor-γ gene and coronary artery disease in Chinese Han population. Mol Biol Rep. 2012;39(2):1863–1868. | ||
Urhammer SA, Clausen JO, Hansen T, Pedersen O. Insulin sensitivity and body weight changes in young white carriers of the codon64 amino acid polymorphism of the beta3-adrenergic receptor gene. Diabetes. 1996;45(8):1115–1120. | ||
Corella D, Guillén M, Portolés O, et al. Gender specific associations of the Trp64Arg mutation in the beta3-adrenergic receptor gene with obesity-related phenotypes in a Mediterranean population: interaction with a common lipoprotein lipase gene variation. J Intern Med. 2001;250(4):348–360. | ||
Widén E, Lehto M, Kanninen T, Walston J, Shuldiner AR, Groop LC. Association of a polymorphism in the beta 3-adrenergic receptor gene with features of the insulin resistance syndrome in Finns. N Engl J Med. 1995;333(6):348–351. | ||
Gagnon J, Mauriege P, Roy S, et al. The Trp64 Arg mutation of the β3-adrenergic receptor gene has no effect on obesity phenotypes in the Quebec family study and Swedish obese subjects cohorts. J Clin Invest. 1996;98:2086–2093. | ||
Lee CH, Olson P, Evans RM. Minireview: lipid metabolism, metabolic diseases, and peroxisome proliferator-activated receptors. Endocrinology. 2003;144(6):2201–2207. | ||
Ye Y, Nishi SP, Manickavasagam S, et al. Activation of peroxisome proliferator-activated receptor-gamma (PPAR-gamma) by atorvastatin is mediated by 15-deoxy-delta-12.14-PGJ2. Prostaglandins Other Lipid Mediat. 2007;84(1–2):43–53. | ||
Jick SS, Choi H, Li L, McInnes IB, Sattar N. Hyperlipidaemia, statin use and the risk of developing rheumatoid arthritis. Ann Rheum Dis. 2009;68(4):546–551. | ||
Sanz J, Moreno PR, Fuster V. Update on advances in atherothrombosis. Nat Clin Pract Cardiovasc Med. 2007;4(2):78–89. | ||
European Association for Cardiovascular Prevention & Rehabilitation, Reiner Z, Catapano AL, De Backer G; ESC Committee for Practice Guidelines (CPG) 2008–2010 and 2010–2012 Committees. ESC/EAS Guidelines for the management of dyslipidaemias: the Task Force for the management of dyslipidaemias of the European Society of Cardiology (ESC) and the European Atherosclerosis Society (EAS). Eur Heart J. 2011;32(14):1769–1818. | ||
McLain K, Edlund BJ. Statin drugs: reducing cardiovascular risk in older adults. J Gerontol Nurs. 2012;38(10):9–13. | ||
Karlson BW, Palmer MK, Nicholls SJ, Lundman P, Barter PJ. Doses of rosuvastatin, atorvastatin and simvastatin that induce equal reductions in LDL-C and non-HDL-C: results from the VOYAGER meta-analysis. Eur J Prev Cardiol. 2016;23(7):744–747. | ||
World Health Organization. Diet, nutrition and the prevention of chronic diseases. WHO Technical Report Series 916, chapter 5. Geneva: WHO; 2003. | ||
Friedewald WT, Levy RI, Fredrickson DS. Estimation of the concentration of low-density lipoprotein cholesterol in plasma, without use of the preparative ultracentrifuge. Clin Chem. 1972;18(6):499–502. | ||
Dobiásová M, Frohlich J. The plasma parameter log (TG/HDL-C) as an atherogenic index: correlation with lipoprotein particle size and esterification rate in apoB-lipoprotein-depleted plasma (FER(HDL)). Clin Biochem. 2001;34(7):583–588. | ||
Arsenault BJ, Rana JS, Stroes ES, et al. Beyond low-density lipoprotein cholesterol: respective contributions of non-high-density lipoprotein cholesterol levels, triglycerides, and the total cholesterol/high-density lipoprotein cholesterol ratio to coronary heart disease risk in apparently healthy men and women. J Am Coll Cardiol. 2009;55(1):35–41. | ||
Tian L, Fu M. The relationship between high density lipoprotein subclass profile and plasma lipids concentrations. Lipids Health Dis. 2010;9:118. | ||
Soltész P, Kerekes G, Dér H, et al. Comparative assessment of vascular function in autoimmune rheumatic diseases: considerations of prevention and treatment. Autoimmun Rev. 2011;10:416–425. | ||
Grygiel-Górniak B, Puszczewicz M. Oxidative damage and antioxidative therapy in systemic sclerosis. Mediators Inflamm. 2014;2014:389582. | ||
Peters MJ, Symmons DP, McCarey D, et al. EULAR evidence-based recommendations for cardiovascular risk management in patients with rheumatoid arthritis and other forms of inflammatory arthritis. Ann Rheum Dis. 2010;69(2):325–331. | ||
Gullick NJ, Scott DL. Co-morbidities in established rheumatoid arthritis. Best Pract Res Clin Rheumatol. 2011;25(4):469–483. | ||
Choy E, Ganeshalingam K, Semb AG, Szekanecz Z, Nurmohamed M. Cardiovascular risk in rheumatoid arthritis: recent advances in the understanding of the pivotal role of inflammation, risk predictors and the impact of treatment. Rheumatology (Oxford). 2014;53(12):2143–2154. | ||
Tilg H, Moschen AR. Adipocytokines: mediators linking adipose tissue, inflammation and immunity. Nat Rev Immunol. 2006;6(10):772–783. | ||
Stavropoulos-Kalinoglou A, Metsios GS, Koutedakis Y, et al. Redefining overweight and obesity in rheumatoid arthritis patients. Ann Rheum Dis. 2007;66(10):1316–1321. | ||
Sánchez T, Contreras-Yáñez I, Elías-López D, Aguilar Salinas CA, Pascual-Ramos V. Prevalence of lipid phenotypes, serum lipid behaviour over follow-up and predictors of serum lipid levels in a cohort of Mexican Mestizo early rheumatoid arthritis patients treated with conventional disease-modifying anti-rheumatic drugs. Clin Exp Rheumatol. 2014;32(4):509–515. | ||
Śliż D, Mamcarz A, Filipiak KJ, et al. 3ST-POL trial: standards of statin use in Poland in the context of the European Society of Cardiology guidelines. Pol Arch Med Wewn. 2010;120:328–333. | ||
Tselios K, Koumaras C, Gladman DD, Urowitz MB. Dyslipidemia in systemic lupus erythematosus: just another comorbidity? Semin Arthritis Rheum. 2016;45(5):604–610. | ||
Cigolle CT, Blaum CS, Halter JB. Diabetes and cardiovascular disease prevention in older adults. Clin Geriatr Med. 2009;25(4):607–641. | ||
Shanmugasundaram M, Rough SJ, Alpert JS. Dyslipidemia in the elderly: should it be treated? Clin Cardiol. 2010;33(1):4–9. | ||
Jones PH, Davidson MH, Stein EA, et al; STELLAR Study Group. Comparison of the efficacy and safety of rosuvastatin versus atorvastatin, simvastatin, and pravastatin across doses (STELLAR* Trial). Am J Cardiol. 2003;92(2):152–160. | ||
Banach M, Rizzo M, Toth PP, et al. Statin intolerance – an attempt at a unified definition. Position paper from an International Lipid Expert Panel. Arch Med Sci. 2015;11(1):1–23. | ||
Schmidt T, Battafarano DF, Mortensen EM, Frei CR, Mansi I. Frequency of development of connective tissue disease in statin-users versus nonusers. Am J Cardiol. 2013;112(6):883–888. | ||
Verdelli A, Antiga E, Bonciolini V, Bonciani D, Volpi W, Caproni M. Drug induction in connective tissue diseases. G Ital Dermatol Venereol. 2014;149(5):573–580. | ||
Turk SA, Heslinga SC, Dekker J, et al. The relationship between cardiac conduction times, cardiovascular risk factors, and inflammation in patients with early arthritis. J Rheumatol. 2017;44(5):580–586. | ||
Yoo WH. Dyslipoproteinemia in patients with active rheumatoid arthritis: effects of disease activity, sex, and menopausal status on lipid profiles. J Rheumatol. 2004;31(9):1746–1753. | ||
Gonzalez-Juanatey C, Llorca J, Testa A, Revuelta J, Garcia-Porrua C, Gonzalez-Gay MA. Increased prevalence of severe subclinical atherosclerotic findings in long-term treated rheumatoid arthritis patients without clinically evident atherosclerotic disease. Medicine (Baltimore). 2003;82(6):407–413. | ||
Myasoedova E, Crowson CS, Kremers HM, et al. Lipid paradox in rheumatoid arthritis: the impact of serum lipid measures and systemic inflammation on the risk of cardiovascular disease. Ann Rheum Dis. 2011;70(3):482–487. | ||
Drechsler M, Megens RT, van Zandvoort M, Weber C, Soehnlein O. Hyperlipidemia-triggered neutrophilia promotes early atherosclerosis. Circulation. 2010;122:1837–1845. | ||
Swirski FK, Libby P, Aikawa E, et al. Ly-6Chi monocytes dominate hypercholesterolemia-associated monocytosis and give rise to macrophages in atheromata. J Clin Invest. 2007;117(1):195–205. | ||
Daniels LB, Laughlin GA, Sarno MJ, Bettencourt R, Wolfert RL, Barrett-Connor E. Lipoprotein-associated phospholipase A2 is an independent predictor of incident coronary heart disease in an apparently healthy older population: the Rancho Bernardo Study. J Am Coll Cardiol. 2008;51(9):913–919. | ||
Tan MH, Johns D, Glazer NB. Pioglitazone reduces atherogenic index of plasma in patients with type 2 diabetes. Clin Chem. 2004;50(7):1184–1188. | ||
Dobiásová M. AIP – atherogenic index of plasma as a significant predictor of cardiovascular risk: from research to practice. Vnitr Lek. 2006;52(1):64–71. | ||
Dobiášová M, Frohlich J, Šedová M, Cheung MC, Brown BG. Cholesterol esterification and atherogenic index of plasma correlate with lipoprotein size and findings on coronary angiography. J Lipid Res. 2011;52(3):566–571. | ||
Wang Z, Ge J. Managing hypercholesterolemia and preventing cardiovascular events in elderly and younger Chinese adults: focus on rosuvastatin. Clin Interv Aging. 2014;9:1–8. | ||
Long SB, Blaha MJ, Blumenthal RS, Michos ED. Clinical utility of rosuvastatin and other statins for cardiovascular risk reduction among the elderly. Clin Interv Aging. 2011;6:27–35. | ||
Ali FY, Armstrong PC, Dhanji AR, et al. Antiplatelet actions of statins and fibrates are mediated by PPARs. Arterioscler Thromb Vasc Biol. 2009;29(5):706–711. | ||
Meirhaeghe A, Fajas L, Helbecque N, et al. A genetic polymorphism of the peroxisome proliferator-activated receptor gamma gene influences plasma leptin levels in obese humans. Hum Mol Genet. 1998;7(3):435–440. | ||
XL, Oosterhof J, Duarte N. Peroxisome proliferator-activated receptor gamma C161→T polymorphism and coronary artery disease. Cardiovasc Res. 1999;44(3):588–594. | ||
Dunajska K, Lwow F, Milewicz A, et al. Beta(3)-adrenergic receptor polymorphism and metabolic syndrome in postmenopausal women. Gynecol Endocrinol. 2008;24(3):133–138. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.