Back to Journals » OncoTargets and Therapy » Volume 10
Potential role of immunotherapy in advanced non-small-cell lung cancer
Authors de Mello RA, Veloso AF, Esrom Catarina P, Nadine S, Antoniou G
Received 22 April 2016
Accepted for publication 6 July 2016
Published 16 December 2016 Volume 2017:10 Pages 21—30
DOI https://doi.org/10.2147/OTT.S90459
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Min Li
Video abstract presented by Professor Ramon de Mello.
Views: 386
Ramon Andrade de Mello,1–3 Ana Flávia Veloso,4 Paulo Esrom Catarina,4 Sara Nadine,5 Georgios Antoniou6
1Department of Biomedical Sciences and Medicine, University of Algarve, Faro, 2Faculty of Medicine, University of Porto, Porto, Portugal; 3Research Center, Cearense School of Oncology, Instituto do Câncer do Ceará, 4Oncology & Hematology League, School of Medicine, State University of Ceará (UECE), Fortaleza, Brazil; 5Instituto de Ciências Biomédicas Abel Salazar (ICBAS), University of Porto, Porto, Portugal; 6Department of Medical Oncology, The Royal Marsden NHS Foundation Trust, London, UK
Abstract: Immuno checkpoint inhibitors have ushered in a new era with respect to the treatment of advanced non-small-cell lung cancer. Many patients are not suitable for treatment with epidermal growth factor receptor tyrosine kinase inhibitors (eg, gefitinib, erlotinib, and afatinib) or with anaplastic lymphoma kinase inhibitors (eg, crizotinib and ceritinib). As a result, anti-PD-1/PD-L1 and CTLA-4 inhibitors may play a novel role in the improvement of outcomes in a metastatic setting. The regulation of immune surveillance, immunoediting, and immunoescape mechanisms may play an interesting role in this regard either alone or in combination with current drugs. Here, we discuss advances in immunotherapy for the treatment of metastatic non-small-cell lung cancer as well as future perspectives within this framework.
Keywords: immunotherapy, non-small-cell lung cancer, nivolumab, pembrolizumab, ipilimumab, clinical trials, PD1, PDL1, CTLA4
Introduction to the development of immunotherapy for cancer and NSCLC
According to the World Health Organization, lung cancer is currently the leading cause of cancer mortality worldwide and of tobacco-related death.1–3 The 5-year overall survival (OS) rate is only 15% for all stages.4 These results also revealed that invasion and metastasis are the primary causes of recurrence and death in patients with lung cancer.4 Historical approaches to nonspecific cytotoxic chemotherapy are associated with severe adverse effects (AEs), selection of drug-resistant tumor cells (TCs), and failure to resolve metastatic or subclinical disease.3
Lung cancer can be generally divided into small-cell lung cancer and non-small-cell lung cancer (NSCLC). NSCLC accounts for >80% of all lung cancers, and patients with this type demonstrate a limited response to chemotherapy when they are in advanced stages.5 Approximately 75% of all NSCLC cases are diagnosed at an advanced stage of the disease,6,7 which means that these patients will have a median survival time of 4–5 months after diagnosis, and only 10% of them will survive for 1 year.8,9
Despite this scenario, the search for safe and specific NSCLC treatments found an opportunity in various immunotherapeutic agents. Vaccines, cytokines, and monoclonal antibodies (mAbs) have become promising drugs that may either help to generate an active immune response against neoplastic antigens or stimulate a nonspecific immune attack against various tumors; in addition, external antibodies may be used as a mechanism for a brief targeted response.2 Increased knowledge of the intricacies of the immune system and how it might act in synergy with conventional chemotherapy has generated new perspectives for NSCLC therapy, which may change its prognosis.
In recent years, many attempts have been made to obtain consistent benefits from tumor vaccines and cytokines: belagenpumatucel-L (an allogeneic TC vaccine) and tecemotide (a peptide vaccine) did not meet survival end points over the placebo in Phase III trials.10,11 The use of IL-2 and interferons (cytokines) generated infrequent responses, and these were observed in only a few types of cancers. Researchers question whether this limited response is actually caused by a tumor mechanism of immune escape.12
The last drug class, mAbs, became applicable as part of a very specific strategy: not as a direct immune system activator against cancerous cells but rather as an instrument to free T-cells from negative regulatory breaks and to promote their cytotoxicity so that they may bind to distinct sites.12 Research has revealed that the targeted proteins that are responsible for such negative regulations are PD-1, PD-L1, and CTLA-4. Ipilimumab, pembrolizumab, tremelimumab, and nivolumab are all immune checkpoint inhibitors that are capable of binding and inactivating the effects of the above-mentioned proteins. These drugs have demonstrated positive results in the treatment of many cancers and have been studied for use in NSCLC. The US Food and Drug Administration (FDA) has recently approved nivolumab for therapeutic use.13
This review aims to discuss the role and evidence of immune response in cancer pathology, the mechanisms of immune checkpoint inhibitors, clinical trials and their results with respect to efficacy and safety, and future perspectives for patients’ quality of life (QoL).
Rationale for the development of immunotherapies
The immune system functions as an adaptable and specific system that distinguishes self from nonself and attacks foreign pathogens and infected self tissues. The innate immune system acts as a nonspecific first line of defense and includes a vast array of components, including antigen-presenting cells (APCs). In contrast, the adaptive immune response results in the development of cytotoxic CD8+ T-cells, helper CD4+ T-cells, and antibody-producing plasma cells.14,15 The presence of an adaptive immune system endows vertebrates with a unique ability to develop highly specific responses. The adaptive immune system is driven by a multitude of highly specific antigen receptors on T-cells (T-cell receptor) and B-cells (B-cell receptor). The cognate binding of an antigen to the B- or T-cell receptor promotes the development of a vigorous antigen-specific immune response and the development of long-lived memory cells. After the eradication of cancer, the presence of memory cells potentially prevents tumor regrowth, decreases metastatic spread, and can limit the de novo induction of a second malignancy.8
In antitumor immune responses, CD8+ T-cells and CD4+ T-cells recognize tumor antigens in the context of major histocompatibility complex class I and class II molecules, respectively. Following initial APC-driven activation, CD8+ T-cells function in cell-mediated cytotoxicity and have the ability to kill cells that are recognized as nonself and cells with altered self-antigens. It is thought that CD8+ T-cells play a key role in the antitumor immune response. On the contrary, CD4+ T-cells differentiate into several types of helper CD4+ T-cells. In a noninflamed environment, CD4+ T-cells can differentiate into regulatory T-cells (Tregs). These cells are able to inhibit the host’s antitumor immune response as they are important negative regulators of the immune system. When this is taken into account, Tregs are considered as a good target for cancer immunotherapy.8
Published data on animal studies have revealed that lymphocytes and natural killer cells contribute to host antitumor defense mechanisms. These data show that deficiencies in key immunologic molecules, such as the perforin,7 RAG2,16 or IFN-γ,17 lead to the development of spontaneous tumors. These studies clarify the cellular basis of cancer immunosurveillance, which is a hypothesis that was proposed decades ago by Burnet18 and Thomas.19
A clear difference in the interpretations of Burnet and Thomas in regard to this hypothesis was the nature of tumor recognition by immune cells (ICs). Burnet considered the self- versus nonself-discrimination hypothesis in which the development of cancers is inhibited. The hypothesis devised by Thomas was different in that he proposed that organisms must possess a primary defense, similar to homograft rejection, against neoplasia.4 The immune surveillance theory, which was validated after technological advances in mouse genetics and mAb production, involves a set of cells and immune system molecules that play a role in the active elimination of immunogenic TCs.
However, many have acknowledged that cancer immunosurveillance is just one step in a larger process termed cancer immunoediting9,20,21 (Figure 1). This concept recognizes that even after the phase of elimination when the tumor escapes immunosurveillance, the fate of the tumor may ultimately be sculpted by immunity and may experience two subsequent phases, as follows: the equilibrium phase, during which the tumor may either be dormant or be immunologically sculpted by immune “editors” to produce new variants that carry more mutations, which would increase resistance to immune attack; this phase would be followed by the escape phase, when the tumor becomes clinically detectable. The elimination of the tumor or the long-term control of cancer in equilibrium represents a potential goal for immunotherapy.21
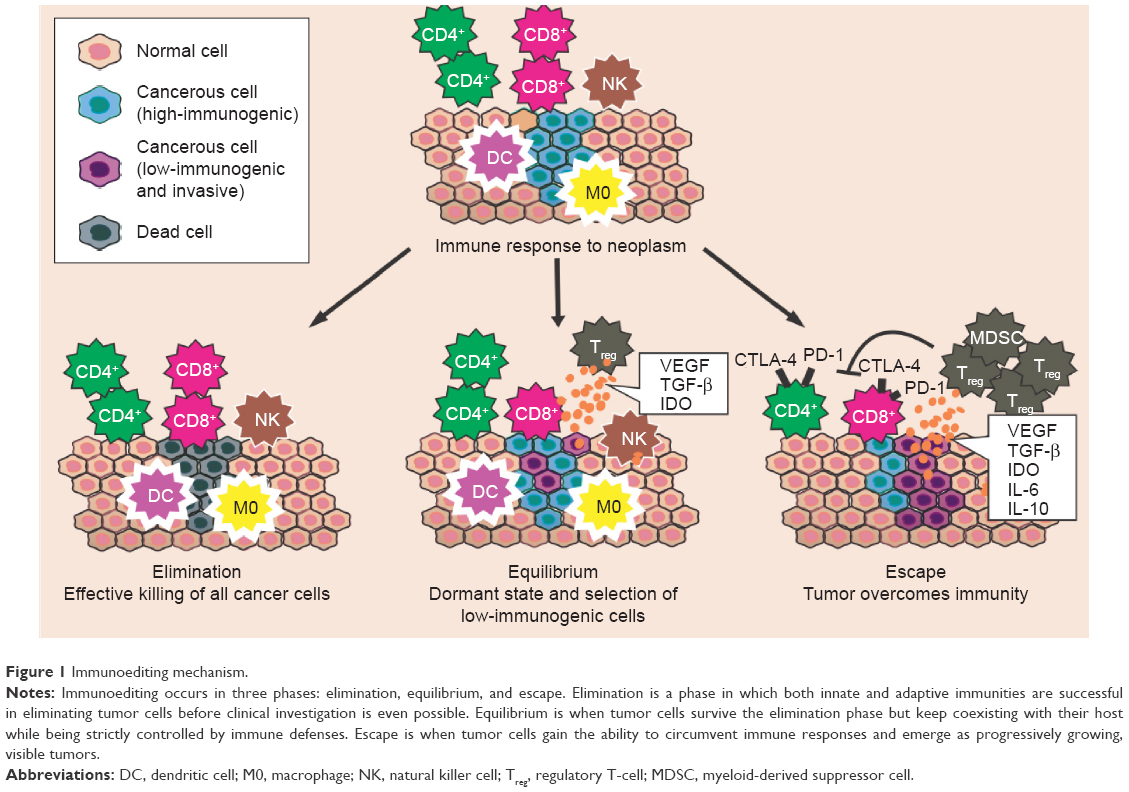 | Figure 1 Immunoediting mechanism. |
The immune system is suppressed by several factors. It would be a great challenge if the elaboration of immunotherapeutic strategies could determine which immunosuppressive factors are required for the maintenance of immune tolerance to various types of cancers.22 The immune responses can be inhibited when certain TCs overproduce and express several molecules with proapoptotic or immune suppressive properties, such as TGF-β; this protein constitutes one of the most important immunosuppressive factors because it inhibits the activation, proliferation, and activity of lymphocytes. In addition, IL-10, which is an anti-inflammatory or immunosuppressive cytokine, is associated with tumor growth and with the regulation of the maturation of APCs as well as their capacity to produce inflammatory cytokines, such as IL-12.23
The number or frequency of tumor-infiltrating lymphocytes is usually used as a prognostic factor, where an increase in tumor-infiltrating lymphocytes is usually a marker of a good prognosis and is associated with prolonged survival of cancer patients.24,25 Nevertheless, the protective functions of the immune system, in which normal conditions are essential to induce immune tolerance to self-antigens, may also provide the means for tumor escape. Thymus-derived or peripherally induced Foxp3+ Tregs act to inhibit autoimmune responses, but in the tumor microenvironment, these cells have the ability to suppress the tumor-specific T-cell response via the production of immunosuppressive cytokines (IL-10 and TGF-β) and via the expression of negative co-stimulatory molecules (CTLA-4, PD-1, and PD-L1). An increased number of Foxp3+ Tregs has been found in the blood of patients with cancer.26 Myeloid-derived suppressor cells (MDSCs) play key roles in the inhibition of host-protective antitumor responses via the induction of Tregs.9 In addition, IDO, which is an enzyme involved in the tryptophan catabolism pathway, may elicit the suppression of T and natural killer cells, the generation and activation of Tregs and MDSCs, and the promotion of tumor angiogenesis. IDO is also overexpressed in TCs.27
The TCs can also induce an upregulation of CTLA-4 for their own advantage. The CTLA-4/B7 engagement inhibits lymphocyte activation and proliferation, which may alter the immune response and promote tumor escape. The interaction of PD-1 and its ligand has also been described to negatively regulate the proliferation and cytokine production of T-cells. The ability of TCs to induce a hostile microenvironment through immunosuppression is a significant barrier to effective cell-mediated immunity and immunotherapy.26
Mechanism of action of emerging immunotherapies such as PD-1 inhibitors
Mechanisms that are used by cancer cells to evade the host immune response are valuable targets for immunotherapy. The loss of antigen expression and resistance to cytotoxicity are the two ways that TCs overcome immunity. Most likely, cells with those advantages experience random mutations and natural selection because T-cells or phagocytes do not easily destroy them. Cancer cells, however, can also change their microenvironment to an immunosuppressive state via cytokine expression (TGF-β, VEGF, or IDO) (Figure 1). In addition, through the recruitment of Tregs (a subtype of helper T-cells) and MDSCs, TCs can actively induce a state of immunosuppression. Thus, with the ultimate goal of reshaping the tumor microenvironment, several immunotherapeutic strategies that inhibit tumor-induced immunosuppression have been developed. Specifically, the use of mAbs directed at PD-1, PD-L1, and CTLA-4 has shown promising results.28
CTLA-4 was the first immune checkpoint receptor to be a clinical target. This protein is normally expressed on the plasma membranes of Tregs and memory T-cells. There, it downregulates T-cell activation by competing with CD28 for its ligands, CD80 and CD86, and by inducing cell cycle arrest in T-cells.29 CTLA-4, whose action occurs 24–48 hours after antigen presentation, primarily regulates CD4+ T-cells and enhances the immunosuppressive activity of Tregs.30 PD-1 allows for immune resistance because it leads to the inhibition of effector T-cell activity when it binds to ligands such as PD-L1, which is a protein expressed by tumor and stromal Tregs. Similar to CTLA-4, PD-L1 can also compete with CD28. Because cancer cells induce a microenvironment that is highly populated by Tregs, they are very dependent on CTLA-4, PD-1, and PD-L1 activities to promote immunosuppression.31 Ipilimumab and tremelimumab are mAbs that were developed to inhibit CTLA-4. Nivolumab, pembrolizumab, atezolizumab, and durvalumab were developed to inhibit PD-1 and PD-L1. Through a reduction in immune checkpoint activity in a Treg-rich microenvironment, they are able to diminish tumor evasion (Figure 2).32
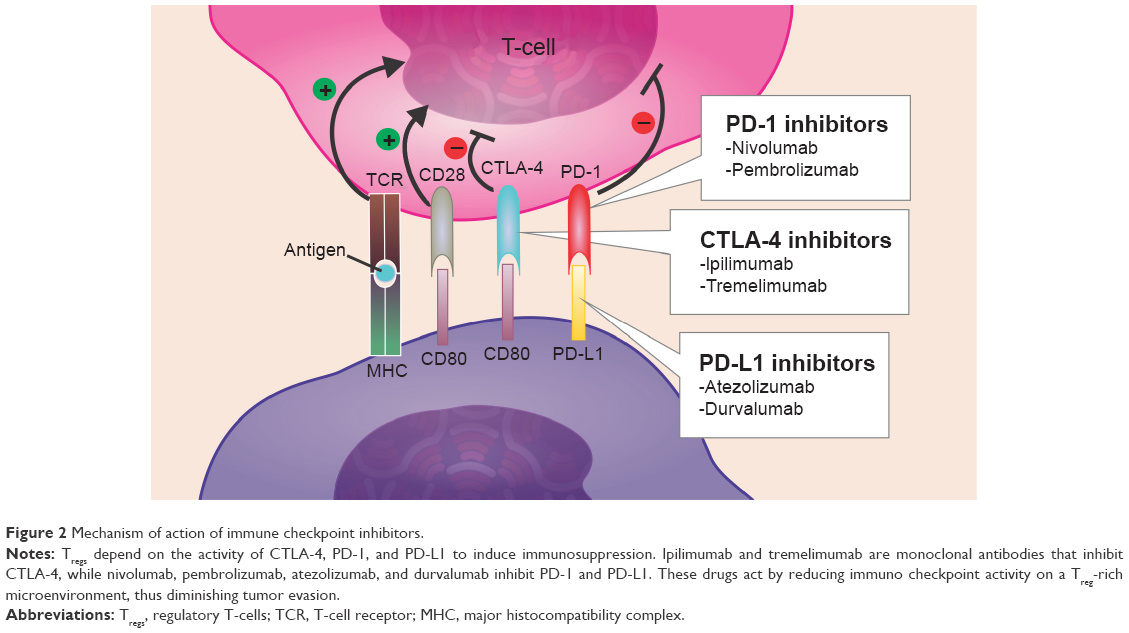 | Figure 2 Mechanism of action of immune checkpoint inhibitors. |
Currently, preclinical studies of CTLA-4 and PD-1 showed that the inhibition of either of these pathways stimulates an antitumor immune response, which increases their validity as therapeutic targets. Furthermore, other studies based on different trials have shown that patients whose tumors overexpress PD-L1 tend to demonstrate an increased response to anti-PD-L1-directed therapy.33
Efficacy and safety of immunotherapy for NSCLC
A blockade of immune checkpoints, including the inhibition of the CTLA-4 and PD-1/PD-L1 pathways, has introduced a new era in cancer treatment, as advances in intratumoral immune responses have been observed in numerous preclinical studies.34 This section features the major results of Phase I–III trials that primarily involve the efficacy and safety of the use of mAbs in NSCLC, as well as studies of a combination of these immunotherapies (Table 1).
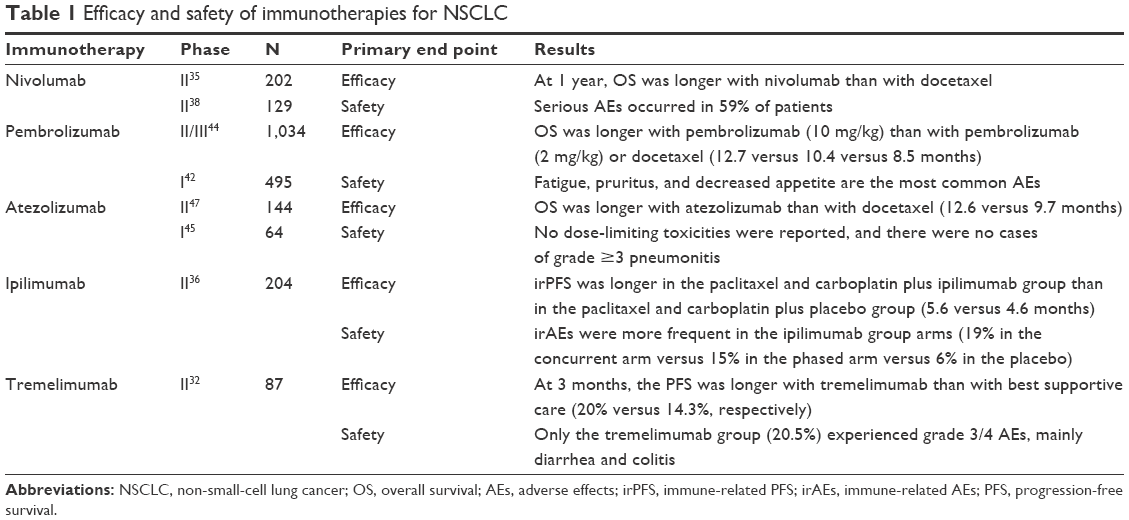 | Table 1 Efficacy and safety of immunotherapies for NSCLC |
Anti-PD-1 mAb inhibitors
Nivolumab
Nivolumab is a fully humanized IgG4 mAb that targets PD-1. This mAb has shown anticancer activity against several tumor types including NSCLC.35 The first Phase I clinical trial of an anti-PD-1 antibody showed activity in NSCLC, and subsequent studies have demonstrated that a PD-1 pathway blockade supports durable tumor responses.36 Completed Phase I and II clinical trials have recently led to the FDA approval of second-line chemotherapy treatment for resistant squamous NSCLC.37
In a Phase I study of ~300 patients with advanced solid tumors, 22 (17%) of 129 patients with NSCLC achieved an interesting objective response after nivolumab treatment. Treatment with nivolumab also resulted in an OS rate of 42% (95% confidence interval [CI] 33–50) at 1 year, 24% (95% CI 17–33) at 2 years, and 18% (95% CI 11–25) at 3 years; similar results have been reported for the nonsquamous and squamous histological subtypes.35 In another Phase I study that included 122 patients with NSCLC, nivolumab was administered once every 2 weeks at doses of 0.1–10 mg/kg. The results of this study showed that the objective response rate (ORR) across all doses was 18% (95% CI 11–29). Previously, patients were highly treated (54% received more than three lines of chemotherapy), and responses were seen across all dose levels; however, the ORR was longer for the 3 mg/kg dose (32%).3
The safety of nivolumab in patients with NSCLC, specifically in those with squamous cell cancer, was established in a Phase II trial (CHECKMATE-063) in patients who had progressed after systemic chemotherapy. The most common AEs were fatigue (50%), dyspnea (38%), musculoskeletal pain (36%), decreased appetite (35%), cough (32%), nausea (29%), and constipation (24%). Serious AEs occurred in 59% of patients and included dyspnea, pneumonia, exacerbation of COPD, pneumonitis, pleural effusion, and hemoptysis. These adverse reactions led to the discontinuation of treatment in 27% of patients.38
One randomized trial, in which patients received monotherapeutic nivolumab (3 mg/kg every 2 weeks, intravenously) or docetaxel (75 mg/m2 every 3 weeks, intravenously), showed that the median OS was higher in patients in the nivolumab group than in the docetaxel group (9.2 versus 6.0 months) (95% CI 7.3–13.3) (hazard ratio [HR] 0.59, 95% CI 0.44–0.79; P<0.001). At 1 year, the OS rate was 42% (95% CI 34–50) in the nivolumab group and 24% (95% CI 17–31) in the docetaxel group. Nine (7%) out of 131 patients in the nivolumab group and 71 (55%) out of 129 in the docetaxel group had grade 3/4 treatment-related adverse events.39
The successful use of nivolumab as a second-line therapy has led to studies of nivolumab as a first-line treatment. Currently, nivolumab is being studied in a Phase I trial to assess its safety and tolerability as a first-line combination therapy or monotherapy in chemotherapy-naïve patients.40
Pembrolizumab
Pembrolizumab is a humanized anti-PD-1 mAb of the IgG4 kappa isotype that blocks the interaction between PD-1 and its ligands, PD-L1 and PD-L2.38 The results of the KEYNOTE-010 trial support the recent approval of pembrolizumab for the management of advanced NSCLC.41
Based on a Phase I clinical trial of 495 patients who received pembrolizumab, fatigue, pruritus, and decreased appetite are its most common AEs. A clear difference based on the dose or schedule was demonstrated.42 In terms of safety, another study showed that grade 3/4 AEs occurred in only 6% of this population. Recently, the use of pembrolizumab (10 mg/kg every 2 or 3 weeks) showed an ORR of 36% in patients with advanced NSCLC.43
In terms of efficacy, a large randomized Phase II/III study was performed at 202 academic medical centers in 24 countries and involved 1,034 patients with previously treated NSCLC. The tumors of these patients expressed PD-L1 on at least 1% of TCs. Patients in this trial demonstrated that the median OS was 10.4 months with 2 mg/kg of pembrolizumab, 12.7 months with 10 mg/kg of pembrolizumab, and 8.5 months with docetaxel. The OS was longer for 2 mg/kg pembrolizumab versus docetaxel (HR 0.71, 95% CI 0.58–0.88; P=0.0008) and for 10 mg/kg pembrolizumab versus docetaxel (HR 0.61, 95% CI 0.49–0.75; P=0.004). Furthermore, among patients with at least 50% of TCs that expressed PD-L1, the OS was significantly longer with 2 mg/kg of pembrolizumab than with docetaxel (14.9 versus 8.2 months; HR 0.54, 95% CI 0.38–0.77; P=0.0002) and with 10 mg/kg of pembrolizumab than with docetaxel (17.3 versus 8.2 months; HR 0.50, 95% CI 0.36–0.70; P<0.0001).44
Anti-PD-L1 mAb inhibitors
Atezolizumab
Atezolizumab (MPDL3280A) is an engineered human IgG1 mAb against PD-L1.3 A Phase I study investigated the use of the atezolizumab in pretreated advanced cancer patients at doses between 1 and 20 mg/kg given three times per week. Approximately, 23 patients with advanced NSCLC were studied for safety and 41 for efficacy and response. As a result, the ORR and 6-month progression-free survival (PFS) rate were 21% and 45%, respectively. No maximum tolerated dose or dose-limiting toxicities were reported, and there were no cases of grade ≥3 pneumonitis.45
According to preliminary data from a Phase I expansion study in 37 patients with evaluable NSCLC, four of five (80%) with strong PD-L1 expression found by immunohistochemistry responded to atezolizumab versus only four of 28 patients (14%) who were PD-L1-negative. These results were confirmed in a later analysis of the full dataset of 53 patients with NSCLC. High PD-L1 expression on tumor-infiltrating ICs was significantly correlated with response to atezolizumab (P=0.0015), while high PD-L1 expression by TCs was not correlated with response to this drug (P=0.920). The ORR in patients with the highest level of PD-L1 expression on ICs was 83%, while the ORR in patients with high tumor PD-L1 expression was only 38%. On the contrary, the response rates were 14%–20% in patients with no or low PD-L1 expression, respectively.46
The single-group Phase II trial BIRCH showed that atezolizumab monotherapy (1,200 mg, intravenously, every 3 weeks until disease progression, unacceptable toxicity, or loss of clinical benefit) demonstrated efficacy in 659 assessable patients with PD-L1-selected stage IIIB/IV or recurrent NSCLC without active central nervous system metastases.47 The population (24%–27%) that achieved an objective response comprised patients who showed the highest expression of PD-L1 on TCs or ICs.17 Another randomized Phase II trial, POPLAR, included patients with nonsquamous or squamous NSCLC with disease progression after platinum treatment. In this trial, 144 patients received atezolizumab monotherapy (1,200 mg, intravenously, every 3 weeks), and 143 received docetaxel (75 mg/m2, intravenously, every 3 weeks). The results showed that in the intention-to-treat population, the median OS was longer in the atezolizumab group compared with the docetaxel group (12.6 versus 9.7 months; HR 0.73, 95% CI 0.53–0.99; P=0.040). In addition, patients with the highest PD-L1 expression on their TCs or ICs showed the largest improvement. Unexpected AEs did not occur in either study. The results from both studies indicate that the selection of patients according to PD-L1 expression could enable the identification of those who are likely to benefit from atezolizumab treatment.47 Currently, the aim of several ongoing trials is to evaluate atezolizumab in pretreated advanced NSCLC (NCT01846416) and the use of this drug in a first-line setting (NCT02409342, NCT02367781, and NCT02367794).3
Durvalumab
Durvalumab (MEDI4736) is a human IgG1 anti-PD-L1 antibody that has shown a satisfactory safety profile and antitumor activity.48 Currently, there is an ongoing placebo-controlled durvalumab trial (called PACIFIC) in patients with stage III unresectable NSCLC following definitive chemoradiation; other studies are likely to be conducted in the future.49
Anti-CTLA-L4 mAb inhibitors
Ipilimumab
Ipilimumab is a fully humanized IgG1 anti-CTLA-4 mAb that blocks the binding of CTLA-4 to its ligand. In terms of efficacy, a randomized Phase II clinical trial assessed treatment with paclitaxel and carboplatin with or without ipilimumab in treatment-naïve stage IV NSCLC patients. The patients showed improvement in immune-related PFS when ipilimumab was administered after chemotherapy (5.7 versus 4.6 months; P=0.05).34 According to a subset analysis, the immune-related PFS in the phased cohort was longer in patients with squamous histology (HR 0.55) than in patients with nonsquamous histology (HR 0.82, 95% CI 0.52–1.28).36
A recent report that pooled data from clinical trials of ipilimumab showed that ~20% of patients will have a long-term survival of at least 3 years after ipilimumab therapy and that the longest reported survival reached 10 years.29
In terms of safety, grade 3/4 AEs occurred with similar frequency across the different arms (control, 37%; concurrent, 41%; phased, 39%), although grade 4 events appeared more frequently in the ipilimumab arms. Among a total of 204 patients, serious immune-related events, including rash (4%), colitis (10%), and hypophysitis (one case), occurred with similar frequency as in previous studies of ipilimumab.50
Currently, an ongoing Phase III clinical trial is testing whether ipilimumab plus paclitaxel and carboplatin will extend the lives of patients with squamous NSCLC more than placebo plus paclitaxel and carboplatin (ClinicalTrials.gov identifier: NCT01285609).
Tremelimumab
Tremelimumab is a fully humanized IgG2 mAb to CTLA-4.22 One randomized Phase II trial involved 87 advanced NSCLC patients with stable disease who responded after four cycles of first-line platinum-based chemotherapy. The patients were randomized between tremelimumab (15 mg/kg) and best supportive care (BSC). As a result, the rate of PFS at 3 months was similar in each arm, with 20% (90% CI 11.4–33.7) and 14.3% (90% CI 6.4–26.3) in the tremelimumab and BSC arms, respectively.32
In terms of safety, the incidence of grade 3/4 AEs was 20.5% in the tremelimumab group (n=44) and 0% in the BSC group (n=43); the most common grade 3/4 AEs due to the use of tremelimumab were diarrhea and colitis (9.1%).51
Combining anti-PD-1, anti-PD-L1, and anti-CTLA-4 therapies
New studies of novel approaches that incorporate checkpoint inhibitors have shown promising preliminary results, and durable responses have been obtained in patients with NSCLC. The combination of two immunotherapies that target a variety of signaling pathways has added an additional treatment modality to immuno-oncology.34
A completed study in mice demonstrated that, compared with single checkpoint inhibition, double blockade promoted tumor repression in 67% (two-thirds) of mice.25 Some current studies are focused on the combination of checkpoint inhibitors; for example, CA209-012 is an ongoing Phase I trial that aims to compare nivolumab as a monotherapy or combined with chemotherapy, targeted therapy, or ipilimumab in patients with NSCLC (ClinicalTrials.gov identifier: NCT01454102).
The results from a Phase I study of the combination of nivolumab and ipilimumab were recently presented. This study divided the patients into two groups: the first arm received 1 mg/kg of nivolumab plus 3 mg/kg of ipilimumab, while the second arm was given 3 mg/kg of nivolumab plus 1 mg/kg of ipilimumab for four cycles. Both arms then received 3 mg/kg of nivolumab until disease progression or unacceptable toxicity occurred.25 In terms of efficacy, the ORR was 11% and 13% for patients in the first arm with squamous and nonsquamous histology, respectively, and was 33% and 13% for the corresponding groups of patients in the second arm. The ORR, in turn, was higher in the nivolumab (3 mg/kg) and ipilimumab (1 mg/kg) treatment arm. After a comparison of the PFS at 24 weeks, the results showed ORRs of 41% versus 29% (the first arm versus the second arm). Grade 3/4 AEs were reported in 49% of patients across both arms. An analysis showed that the most common severe AEs were pneumonitis, diarrhea, colitis, elevated advanced solid tumors, and ALT enzymes. Three of the 49 patients died due to drug-related toxicities.25
Another Phase I trial that assessed the combination of immunotherapies was performed by Rizvi et al and showed that durvalumab (20 mg/kg every 2 or 4 weeks) plus tremelimumab (1 mg/kg every 4 weeks) has a manageable tolerability profile and antitumor activity in patients with NSCLC. Despite the benefit of anti-PD-1/PD-L1 monotherapy, the combination of durvalumab plus tremelimumab appears to be effective regardless of PD-L1 status, even in patients with no PD-L1 staining in the TC membrane; this is a setting where patients would not be expected to derive significant benefit from anti-PD-1/PD-L1 monotherapy over the current standard of care.48
Currently, other clinical trials are ongoing and involve different combinations of immunotherapies. Tremelimumab is being studied in combination with durvalumab (MEDI4376) for advanced NSCLC (ClinicalTrials.gov identifier: NCT2000947, NCT02453282, and NCT02352948). Other studies of ipilimumab plus pembrolizumab in KEYNOTE-021 and of ipilimumab plus atezolizumab are being pursued (ClinicalTrials.gov identifier: NCT02039674 and NCT02174172, respectively).
Chimeric antigen receptor T-cells
Targeted immunotherapies using chimeric antigen receptors (CARs) to redirect and reprogram patient T-cells have shown promising results in the treatment of acute lymphoblastic leukemia and non-Hodgkin’s lymphoma. CARs are genetically engineered synthetic receptors that endow T-cells with the ability to target specific tumor surface antigens. Second-generation CARs, which combine the activation and co-stimulatory signaling domains, have enabled the design of more potent T-cells that can mediate complete responses in patients with chemo-refractory B-cell malignancies. Although the therapeutic potential of CAR T-cells against solid cancers remains unknown, a recent study has indicated the therapeutic potential of regional CAR T-cell therapy for pleural malignancies (both primary and metastatic). Through CAR T-cells that are specific to mesothelin, a cell surface molecule that is overexpressed in >90% of epithelioid malignant pleural mesotheliomas, the authors show that early antigen activation of mesothelin by CD4+ CAR T-cells can lead to enhanced antitumor efficacy.20,21
Impact of patient-focused perspectives such as QoL
In spite of the advances in immune checkpoint inhibitors for NSCLC treatment, due to unrestrained T-cell activation, immunotherapy can lead to manifestations of toxicity, such as autoimmune breakthrough or immune-related adverse events (irAEs).52 During the past 2 decades until 2010, 32 mAbs have been approved by the FDA for use as drugs, but two of the three drugs that might be the focus of clinical trials have been removed from the market due to the occurrence of severe AEs in human patients.53
Both education and communication among patients, caregivers, and the clinical team are vital for appropriate recognition and management of irAEs.52 For instance, the most common AEs in patients who receive ipilimumab include fatigue, diarrhea, rash, pruritus, and colitis. In addition, irAEs that result from the use of PD-1 inhibitors are similar. In an assessment of patients with NSCLC who were treated with immune checkpoint inhibitors, it is extremely important to recognize that immunotherapy is different from chemotherapy; the irAEs observed with immunotherapy have a completely distinct underlying mechanism compared with the toxicity that is observed with chemotherapy.52
In this context, even though the OS is an important outcome with respect to which treatment a patient should receive, the possible AEs and the symptomatic benefits of therapy must always be considered. Although assessment of QoL is greatly important to patients and clinicians, the evaluation of QoL data is a feature in a minority of trials of patients with NSCLC, and has contributed to the failure of lung cancer research.54
Some tools help researchers to assess QoL. Among them, the Lung Cancer Symptom Scale consists of a lung cancer-specific measure of QoL. This scale is used particularly in clinical trials and assesses six common symptoms associated with lung cancer, such as loss of appetite, fatigue, cough, dyspnea, hemoptysis, and pain.55 This evaluation involves the use of the visual analog scale. Furthermore, other methods include the background demographic questionnaire and the Palliative Performance Scale. The latter, which is adapted from the Karnofsky Performance Rating Scale, rates physical performance and has five functional dimensions: ambulation, activity level and evidence of disease, self-care, oral intake, and level of consciousness. The Karnofsky Performance Rating Scale ranged from 0% (death) to 100% (fully ambulatory and healthy).55
Positive outcomes including improved QoL, improved mood, care that is directed less at an increase in lifespan, and longer survival have been demonstrated from the delivery of palliative care services that are integrated into oncology care among patients with advanced cancers.24 Reinke et al found that, among patients with stage IV lung cancer, the weekly assessment of symptoms in the outpatient setting by a palliative care team improved the QoL and the symptom burden and increased survival, compared with patients in a traditional treatment setting.24
Currently, with attention focused on immune checkpoint inhibitors, several questions about irAEs will likely be resolved with more widespread clinical trials. It is not clear, for instance, if autoimmune disease is an absolute contraindication for this type of therapy. In this context, studies that identify biomarkers and other factors involved in response and resistance to immunotherapy, in addition to trials that assess the combination of immunotherapy and chemotherapy, targeted therapy, or multiple immune modulators, are underway to better define this treatment modality for cancer.52
Conclusion
Considering all the aspects discussed in this manuscript, it is noteworthy that immuno checkpoint inhibitors have established a new era for the treatment of advanced NSCLC. The large set of susceptible patients for this scenario emerges concurrently with the competitive research trials among the main pharmaceutical sponsors and clinical research officers in an attempt to find the best setting for their innovative drugs. Nevertheless, this is a very difficult task because the data change rapidly and sometimes show the limitations and important concerns of the current trial designs. The major sponsors and clinical research officers have launched several of the current trials in the last 3–5 years. This has led to the identification of potential limitations, such as the biomarker selection implementation (eg, in the case of PD-L1 expression as an inclusion criterion, which would restrict patient selection and possible benefits), as well as the image response criteria assessment protocols (eg, CheckMate 063 assessed the ORR using the traditional Response Evaluation Criteria in Solid Tumors version 1.1 criteria, which was not appropriate for immunotherapy).56 Advances in research are occurring more quickly than changes in traditional practices, and perhaps, some protocol amendments are difficult to implement in such multicentric randomized control trials. However, the data regarding the outcomes, toxicity profile control, cost-effective analysis, and patient QoL have emerged in an attempt to determine the best approaches to improve patient care.
Disclosure
RAM has received honoraria from the Pfizer Advisory Board, Zodiac Advisory Board, AstraZeneca, and the National Science Centre (Krakow, Poland), and an educational grant from Pierre Fabre. RAM is an ad hoc consultant at the Ministry of Health, Brasília, Brazil. The other authors have no conflicts of interest related to this manuscript.
References
Torre LA, Bray F, Siegel RL, Ferlay J, Lortet-Tieulent J, Jemal A. Global cancer statistics, 2012. CA Cancer J Clin. 2015;65(2):87–108. | ||
Thomas A, Giaccone G. Why has active immunotherapy not worked in lung cancer? Ann Oncol. 2015;26(11):2213–2220. | ||
La-Beck NM, Jean GW, Huynh C, Alzghari SK, Lowe DB. Immune checkpoint inhibitors: new insights and current place in cancer therapy. Pharmacotherapy. 2015;35(10):963–976. | ||
Ada G. The coming of age of tumour immunotherapy. Immunol Cell Biol. 1999;77(2):180–185. | ||
Borghaei H, Paz-Ares L, Horn L, et al. Nivolumab versus docetaxel in advanced nonsquamous non-small-cell lung cancer. N Engl J Med. 2015;373(17):1627–1639. | ||
Reiman JM, Kmieciak M, Manjili MH, Knutson KL. Tumor immunoediting and immunosculpting pathways to cancer progression. Semin Cancer Biol. 2007;17(4):275–287. | ||
Smyth MJ, Thia KY, Street SE, MacGregor D, Godfrey DI, Trapani JA. Perforin-mediated cytotoxicity is critical for surveillance of spontaneous lymphoma. J Exp Med. 2000;192(5):755–760. | ||
Page DB, Bourla AB, Daniyan A, et al. Tumor immunology and cancer immunotherapy: summary of the 2014 SITC primer. J Immunother Cancer. 2015;3(1):25. | ||
Schreiber RD, Old LJ, Smyth MJ. Cancer immunoediting: integrating immunity’s roles in cancer suppression and promotion. Science. 2011;331(6024):1565–1570. | ||
Giaccone G, Bazhenova LA, Nemunaitis J, et al. A phase III study of belagenpumatucel-L, an allogeneic tumour cell vaccine, as maintenance therapy for non-small cell lung cancer. Eur J Cancer. 2321;51(16):2321–2329. | ||
Butts C, Socinski MA, Mitchell PL, et al. Tecemotide (L-BLP25) versus placebo after chemoradiotherapy for stage III non-small-cell lung cancer (START): a randomised, double-blind, phase 3 trial. Lancet Oncol. 2014;15(1):59–68. | ||
Ribas A. Releasing the brakes on cancer immunotherapy. N Engl J Med. 2015;373(16):1490–1492. | ||
Aguiar PN Jr, Santoro IL, Tadokoro H, et al. A pooled analysis of nivolumab for the treatment of advanced non-small-cell lung cancer and the role of PD-L1 as a predictive biomarker. Immunotherapy. 2016;8(9): 1011–1019. | ||
Madureira P, de Mello RA, de Vasconcelos A, Zhang Y. Immunotherapy for lung cancer: for whom the bell tolls? Tumor Biol. 2015;36(3):1411–1422. | ||
Ernst B, Anderson KS. Immunotherapy for the treatment of breast cancer. Curr Oncol Rep. 2015;17(2):5. | ||
Shankaran V, Ikeda H, Bruce AT, et al. IFNγ and lymphocytes prevent primary tumour development and shape tumour immunogenicity. Nature. 2001;410(6832):1107–1111. | ||
Dighe AS, Richards E, Old LJ, Schreiber RD. Enhanced in vivo growth and resistance to rejection of tumor cells expressing dominant negative IFN gamma receptors. Immunity. 1994;1(6):447–456. | ||
Burnet M. Cancer: a biological approach. III. Viruses associated with neoplastic conditions. IV. Practical applications. Br Med J. 1957;1(5023):841–847. | ||
Thomas L. On immunosurveillance in human cancer. Yale J Biol Med. 1982;55(3–4):329–333. | ||
Dunn GP, Bruce AT, Ikeda H, Old LJ, Schreiber RD. Cancer immunoediting: from immunosurveillance to tumor escape. Nat Immunol. 2002;3(11):991–998. | ||
Dunn GP, Old LJ, Schreiber RD. The immunobiology of cancer immunosurveillance and immunoediting. Immunity. 2004;21(2):137–148. | ||
Stagg J, Johnstone RW, Smyth MJ. From cancer immunosurveillance to cancer immunotherapy. Immunol Rev. 2007;220(1):82–101. | ||
Khong HT, Restifo NP. Natural selection of tumor variants in the generation of “tumor escape” phenotypes. Nat Immunol. 2002;3(11):999–1005. | ||
Reinke LF, Feemster LC, Backhus LM, Gylys-Colwell I, Au DH. Assessment and management of symptoms for outpatients newly diagnosed with lung cancer. Am J Hosp Palliat Care. 2016;33(2):178–183. | ||
Antonia S, Gettinger S, Chow LM, et al. Nivolumab (anti-PD-1; BMS-936558, ONO-4538) and ipilimumab in first-line NSCLC: interim Phase I results. J Clin Oncol. 2014;32(Suppl 15):Abstract 8023. | ||
Stewart TJ, Abrams SI. How tumours escape mass destruction. Oncogene. 2008;27(45):5894–5903. | ||
Prendergast GC, Smith C, Thomas S, et al. Indoleamine 2,3-dioxygenase pathways of pathogenic inflammation and immune escape in cancer. Cancer Immunol Immunother. 2014;63(7):721–735. | ||
Vesely MD, Kershaw MH, Schreiber RD, Smyth MJ. Natural innate and adaptive immunity to cancer. Annu Rev Immunol. 2011;29:235–271. | ||
Postow MA, Callahan MK, Wolchok JD. Immune checkpoint blockade in cancer therapy. J Clin Oncol. 2015;33(17):1974–1982. | ||
Domingues D, Turner A, Silva MD, et al. Immunotherapy and lung cancer: current developments and novel targeted therapies. Immunotherapy. 2014;6(11):1221–1235. | ||
Ostrand-Rosenberg S, Horn LA, Alvarez JA. Novel strategies for inhibiting PD-1 pathway-mediated immune suppression while simultaneously delivering activating signals to tumor-reactive T cells. Cancer Immunol Immunother. 2015;64(10):1287–1293. | ||
Ghosh RK, Sharma A, Sharma N. Immune checkpoint inhibitors in advanced nonsmall cell lung cancer. Curr Opin Oncol. 2015;27(2):108–117. | ||
Patel SP, Kurzrock R. PD-L1 expression as a predictive biomarker in cancer immunotherapy. Mol Cancer Ther. 2015;14(4):847–856. | ||
Dempke WCM, Sellmann L, Fenchel K, Edvardsen K. Immunotherapies for NSCLC: are we cutting the gordian helix? Anticancer Res. 2015;35(11):5745–5757. | ||
Mayor M, Yang N, Sterman D, Jones DR, Adusumilli PS. Immunotherapy for non-small cell lung cancer: current concepts and clinical trials. Eur J CardioThoracic Surg. 2016;49(5):1324–1333. | ||
Ang YLE, Tan H-L, Soo RA. Best practice in the treatment of advanced squamous cell lung cancer. Ther Adv Respir Dis. 2015;9(5):224–235. | ||
Rizvi NA, Mazières J, Planchard D, et al. Activity and safety of nivolumab, an anti-PD-1 immune checkpoint inhibitor, for patients with advanced, refractory squamous non-small-cell lung cancer (CheckMate 063): a phase 2, single-arm trial. Lancet Oncol. 2015;16(3):257–265. | ||
Le DT, Uram JN, Wang H, et al. PD-1 blockade in tumors with mismatch-repair deficiency. N Engl J Med. 2015;372(26):2509–2520. | ||
Yaqub F. Nivolumab for squamous-cell non-small-cell lung cancer. Lancet Oncol. 2015;16(7):e319. | ||
Rounds A, Kolesar J. Nivolumab for second-line treatment of metastatic squamous non-small-cell lung cancer. Am J Health Syst Pharm. 2015;72(21):1851–1855. | ||
Mok TSK, Loong HH. Are we ready for immune checkpoint inhibitors for advanced non-small-cell lung cancer? Lancet. 2016;387(10027):1488–1490. | ||
Garon EB, Rizvi NA, Hui R, et al. Pembrolizumab for the treatment of non-small-cell lung cancer. N Engl J Med. 2015;372(21):2018–2028. | ||
Swaika A, Hammond WA, Joseph RW. Current state of anti-PD-L1 and anti-PD-1 agents in cancer therapy. Mol Immunol. 2015;67(2):4–17. | ||
Herbst RS, Baas P, Kim D-W, et al. Pembrolizumab versus docetaxel for previously treated, PD-L1-positive, advanced non-small-cell lung cancer (KEYNOTE-010): a randomised controlled trial. Lancet. 2016;387(10027):1540–1550. | ||
Monteiro ID, Califano R, Mountzios G, de Mello RA. Immunotherapy with checkpoint inhibitors for lung cancer: novel agents, biomarkers and paradigms. Future Oncol. 2016;12(4):551–564. | ||
Garon EB. Current perspectives in immunotherapy for non-small cell lung cancer. Semin Oncol. 2015;42(Suppl 2):S11–S18. | ||
Lee JS, Collard HR. Immunotherapy: the third wave in lung cancer treatment. Lancet Respir Med. 2015;3(12):923–924. | ||
Rizvi N, Chaft J, Balmanoukian A, et al. Tumor response from durvalumab (MEDI4736) + tremelimumab treatment in patients with advanced non-small cell lung cancer (NSCLC) is observed regardless of PD-L1 status. J Immunother Cancer. 2015;3(Suppl 2):P193. | ||
Socinski MA. Incorporating immunotherapy into the treatment of non-small cell lung cancer: practical guidance for the clinic. Semin Oncol. 2015;42(Suppl 2):S19–S28. | ||
Johnson DB, Rioth MJ, Horn L. Immune checkpoint inhibitors in NSCLC. Curr Treat Options Oncol. 2014;15(4):658–669. | ||
Zatloukal P, Heo DS, Park K, et al. Randomized phase II clinical trial comparing tremelimumab (CP-675,206) with best supportive care (BSC) following first-line platinum-based therapy in patients (pts) with advanced non-small cell lung cancer (NSCLC). J Clin Oncol. 2009;27(Suppl 15):abstr 8071. | ||
Villadolid J, Amin A. Immune checkpoint inhibitors in clinical practice: update on management of immune-related toxicities. Transl Lung Cancer Res. 2015;4(5):560–575. | ||
Wang J, Zou Z-H, Xia H-L, et al. Strengths and weaknesses of immunotherapy for advanced non-small-cell lung cancer: a meta-analysis of 12 randomized controlled trials. PLoS One. 2012;7(3):e32695. | ||
Brown T, Pilkington G, Boland A, et al. Clinical effectiveness of first-line chemoradiation for adult patients with locally advanced non-small cell lung cancer: a systematic review. Health Technol Assess. 2013;17(6):1–99. | ||
O’Mahony S, Nathan S, Mohajer R, et al. Survival prediction in ambulatory patients with stage III/IV non-small cell lung cancer using the palliative performance scale, ECOG, and lung cancer symptom scale. Am J Hosp Palliat Care. 2016;33(4):374–380. | ||
de Mello RA, Pousa I, Pereira D, et al. Nivolumab for advanced squamous cell lung cancer: what are the next steps? Lancet Oncol. 2015;16(3):234–235. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.