Back to Journals » Cancer Management and Research » Volume 13
Potential Effects of the FLT3-ITD Mutation on Chemotherapy Response and Prognosis of Acute Promyelocytic Leukemia
Authors Song Y ![]() , Peng P, Qiao C, Li J, Long Q, Lu H
, Peng P, Qiao C, Li J, Long Q, Lu H
Received 20 December 2020
Accepted for publication 24 February 2021
Published 12 March 2021 Volume 2021:13 Pages 2371—2378
DOI https://doi.org/10.2147/CMAR.S297421
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Seema Singh
Yu-hua Song,1 Peng Peng,1 Chun Qiao,2 Jian-yong Li,2 Qi-qiang Long,1 Hua Lu2
1Department of Haematology, The Second Hospital of Nanjing, Nanjing University of Chinese Medicine, Nanjing, Jiangsu, People’s Republic of China; 2Department of Haematology, First Affiliated Hospital of Nanjing Medical University, Jiangsu Province Hospital, Nanjing, Jiangsu, People’s Republic of China
Correspondence: Hua Lu
Department of Haematology, First Affiliated Hospital of Nanjing Medical University, Jiangsu Province Hospital, No. 300 Guangzhou Road, Gulou District, Nanjing, 210029, Jiangsu Province, People’s Republic of China
Tel +86 13951717512
Fax +86 025-83626373
Email [email protected]
Purpose: To evaluate the influence of FLT3-ITD mutations on the treatment response and long-term survival of newly-diagnosed patients with acute promyelocytic leukemia (APL) treated with all-trans retinoic acid and arsenic trioxide.
Methods: The long-term survival of 90 newly-diagnosed APL patients (age range 12– 75 years) was retrospectively analyzed.The FLT3-ITD mutation rate was assayed by polymerase chain reaction (PCR) amplification and sequencing analysis. Its impact on the treatment response, event-free survival(EFS), or overall survival(OS) was investigated in patients with and without the mutations.
Results: The FLT3-ITD mutation rate in newly-diagnosed APL patients was 20% (18/90). The white blood cell (WBC) count at diagnosis in patients with mutations was significantly higher than that in patients without mutations while the FLT3-ITD mutation rate was higher in the high-risk group than in the low/intermediate-risk group. Patients with mutations had a significantly higher early death (ED) rate (16.67% vs 1.39%) for those lacking the mutation (P =0.024). However, the complete remission (CR) and differentiation syndrome (DS) rates in the two groups were similar. Kaplan Meier analysis for EFS and OS at five years showed a significant difference between the patients stratified by FLT3-ITD mutation status (log-rank P =0.010 and P =0.009, respectively).
Conclusion: FLT3-ITD mutations can be related to high peripheral WBC counts in APL patients. APL patients with mutations displayed a higher ED rate compared to those without mutations. Patients carrying mutations had reduced five-year EFS and OS rates. Thus, reducing the overall death rate during induction treatment might be an effective way to improve the prognosis of patients with FLT3-ITD mutations.
Keywords: acute promyelocytic leukemia, APL, FLT3-ITD, internal tandem duplication, ITD, prognosis, survival
Introduction
With the introduction of all-trans retinoic acid (ATRA) and arsenic trioxide (ATO), substantial advances have been made in the treatment profile for acute promyelocytic leukemia (APL) in the last two decades. APL treatment has evolved from ATRA + chemotherapy as a standard regimen to a dual-induction regimen involving a combination of ATO and ATRA as a new standard treatment for low/intermediate-risk patients. ATRA and ATO bind specifically to the retinoic acid receptor alpha (RARα) and promyelocytic leukemia protein (PML, a component of the PML-RARα fusion protein), leading to there degradation. In addition, ATRA and ATO can induce the differentiation and apoptosis of APL cells. FLT3 (fms-like tyrosine kinase 3) belongs to the type ш tyrosine kinase receptor family and is a cell membrane-expressed proto-oncogene. FLT3 mutations are mainly tandem repeats within the framework of the proximal membrane region and are collectively termed the FLT3 internal tandem duplication (FLT3-ITD). FLT3-ITD mutations are often associated with specific cytogenetic changes or mutations in other genes. FLT3-ITD mutations, although common, are not the only type of FLT3 mutations seen in AML. FLT3-ITD mutations have a high incidence in patients with t (15; 17) chromosomal abnormalities, especially in the M3 mutation with PML-RARα and shortened mRNAs. FLT3-ITD mutations are often considered to be related to high white blood cell (WBC) counts in APL patients undergoing ATRA+ chemotherapy and are considered to be indicators of poor prognosis.1–5 Studies on induction therapy with ATO as the main agent have suggested that ATO can effectively neutralize the adverse prognostic effects of FLT3-ITD mutations.6–8 In addition, animal studies have also suggested that FLT3-ITD can inhibit ATRA-induced differentiation and clearance of APL in vivo and that its combined application with arsenic can eliminate such resistance.9 However, the value of FLT3-ITD mutations in evaluating the prognosis of APL requires further investigation.
This study has investigated the status of FLT3-ITD gene mutations in newly-diagnosed APL patients treated with the ATRA+ATO-based induction regimen, excluding patients with PML-RARα.The primary aim was to clarify its potential biological and clinical implications and to further improve the prognostic stratification system in APL patients.
Materials and Methods
Study Subjects and Ethics Statement
A total of 90 newly-diagnosed APL patients, hospitalized in the Jiangsu Province Hospital, the first affiliated hospital of Nanjing Medical University (Nanjing, China) from February 2010 to March 2017. Fifty male and forty female patients, with a median age of 43 (12–75) years, were included in the study. All the patients had been diagnosed with APL according to clinical manifestations, routine blood tests, bone marrow cell morphology, leukemia immunotyping, fusion genes, and chromosome karyotypes, and the diagnostic criteria were in line with the criteria for the diagnosis and efficacy of hematologic diseases. We collected the clinical data and identified the diagnostic information during and after data collection. Following the Chinese guidelines for AML diagnosis and treatment,10 all patients were treated with 0.16 mg/(kg·d) ATO in combination with 20 mg/(m2·d) ATRA until a complete response was observed. If WBC>10×109/L, idarubicin (IDA) 8–12 mg/(m2·d) was added for 3–4 days or daunorubicin (DNR) 45 mg/(m2·d) for 3–4 days of chemotherapy. In addition, chemotherapy consolidation therapy and ATRA/ATO maintenance therapy was administered after complete remission was achieved. According to the presence of FLT3-ITD mutations, the patients were divided into a positive group and a negative group, and the clinical laboratory characteristics, response to induction therapy, and prognosis of the two groups were analyzed and compared. The study was approved by the ethics committee of the First Affiliated Hospital of Nanjing Medical University, Jiangsu Province Hospital. All the participants received and signed written informed consent, including legal guardians representing the minors recruited in our study. All clinical investigations were conducted in accordance with the principles expressed in the Declaration of Helsinki.
Extraction of Genomic DNA
Five milliliters of bone marrow fluid were extracted for routine immunophenotypic and cytogenetic analysis. The mononuclear cells were isolated from the remaining bone marrow solution with lymphocyte separation solution, and the DNA was extracted using the traditional phenol-chloroform extraction. The OD values of the samples were determined by a biophotometer (Eppendorf AG, Hamburg, Germany). The DNA was diluted to 50 ng/μL in deionized water and stored at −20°C for later experiments.
FLT3-ITD Mutation Detection
PCR amplification was performed as previously described.11,12 The primers were designed for exons 14 and 15 of the FLT3 gene and were synthesized by Shanghai Thermo Fisher Scientific Co. Ltd. (Shanghai, China). The primers were the transgenic sense: 5ʹ-GCAATTTAGGTATGAAAGCCAGC-3ʹ and antisense: 5ʹ-CTTTCAGCATTTTGACGGCAACC-3ʹ.The reaction conditions included incubation at 5°C for 5 minutes, the cycling conditions followed for each reaction were 95°C for 30 seconds, annealing at 60°C for 45 seconds, and elongation at 72°C for 1 minute, lasting for 35 cycles. This was followed by a final elongation at 72°C for 8 minutes, after which the reaction products were stored at 4°C. The wild-type amplification products showed a single peak at 329 bp, and the ITD mutant amplification products showed specific bands at greater than 329 bp. The positive samples from agarose gel electrophoresis were selected and the PCR products were analyzed by capillary electrophoresis. The results were further confirmed by fragment analysis. FLT3-ITD electrophoresis and direct sequencing of the positive specimens were performed for PCR amplification and sent to Shanghai Thermo Fisher Scientific Company for cloning and sequencing; the sequencing results were compared with the wild-type gene sequence.
Statistical Analysis
SPSS 16.0 software (SPSS, Chicago, IL, USA) was used for all statistical analyses. The measurement data were expressed as mean ± standard deviation (x̄±SD), and comparisons between the two groups were measured by the t-test. The chi-square test and Fisher exact test were used for counting data (small sample data). The Kaplan-Meier method was used to draw the survival curve and P<0.05 was considered as statistically significant.
Results
Relationship Between FLT3-ITD Mutations and Clinical and Laboratory Characteristics of Patients with APL
Among the 90 patients with APL, 18 had positive FLT3-ITD mutations, with a positive rate of 20% (95% confidence interval 11.6–28.4%). Of these, 11 were males (61.1%) and 7 females (38.9%), with no statistically significant difference. The initial WBC count of the APL patients were noted to be significantly higher in the positive mutation group (P<0.01). However, age, hemoglobin, platelet (PLT), lactate dehydrogenase (LDH), and the bone marrow primordial promyelocytic granulocyte ratio showed no correlation with the presence of a mutation. There was no significant difference in the coagulation indices between the two groups (prothrombin time; partial thromboplastin time; D-dimer; fibrinogen) (Table 1). The patients were further divided into two groups for analysis. The incidence of FLT3-ITD mutations in the high-risk APL patients with WBC≥10×109/L was 45.2% (14/31; 95% confidence interval 26.6–63.7%) and 6.8% (4/59; 95% confidence interval 2–13.4%) in Intermediate/Low Risk patients with WBC<10×109/L. This difference was significant (P<0.001). The APL patients were further divided into a CD34+ group and a CD34- group according to the status of CD34 expression. The incidence of FLT3-ITD mutations was 62.5% (10/16; 95% confidence interval 35.9–89.1%) in the CD34+ group and 10.6% (7/66; 95% confidence interval 3–18.2%) in the CD34- group, with significant differences (P<0.001).
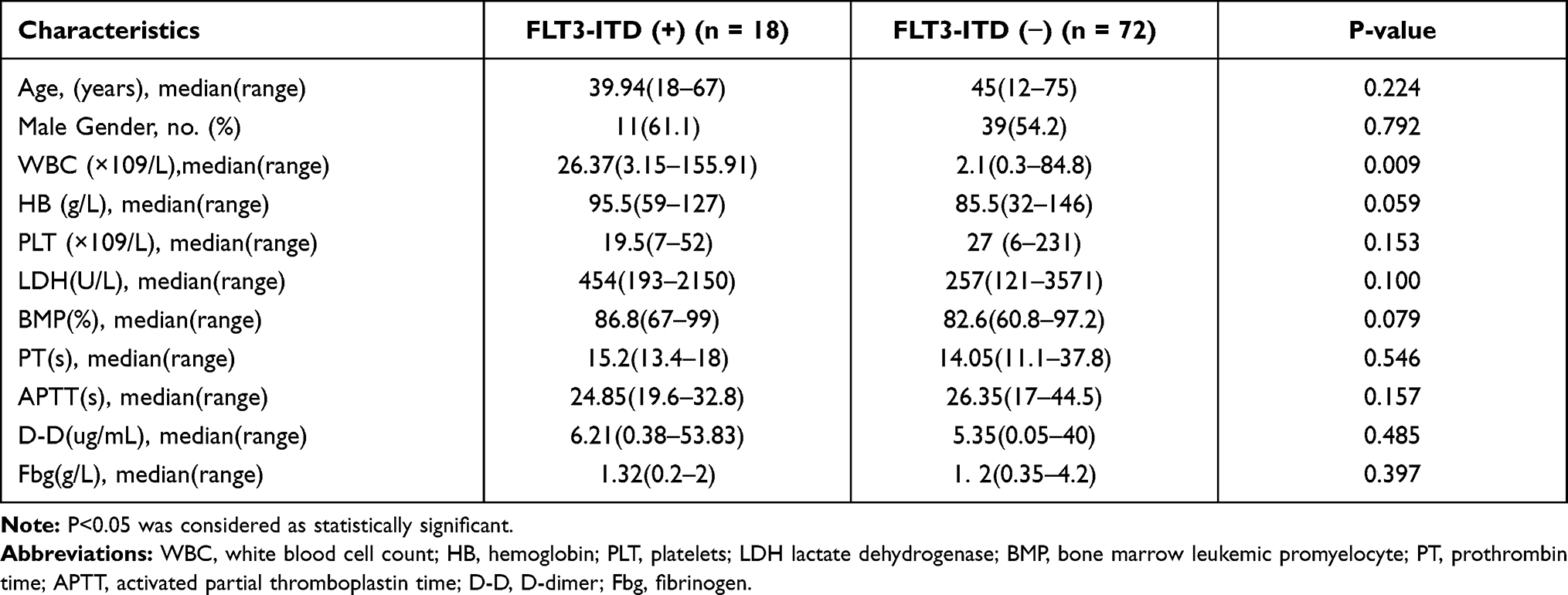 |
Table 1 Presenting Features of APL Patients According to FLT3-ITD Mutation Status |
Effect of FLT3-ITD Mutations on Response to Induction Therapy and Prognosis
After induction therapy, 16 of the 18 patients positive for FLT3-ITD mutations obtained CR (88.9%) compared to 71 patients out of 72 (98.6%) in the negative group. However, no significant difference was noted between the two groups (P= 0.101). In this study, 30 cases of differentiation syndrome (DS) occurred, and 6 cases (33.3%; 95% confidence interval 9.2–57.5%) of DS occurred during induction therapy in 18 patients in the positive group, and 23 cases (31.9%; 95% confidence interval 20.9–43%) of DS occurred in the negative group. There was no significant difference between the two groups (P=0.559). The overall rate of early death (ED) was 4.4% (4/90) and three patients died from intracranial hemorrhage, including one patient with concurrent pulmonary hemorrhage. The fourth patient died of post-chemotherapy infection. This patient had type 2 diabetes, which was not completely treated, and had poorly-controlled blood sugar levels. The disease-induced mortality was 16.7% (3/18) in the positive group and 1.39% (1/72) in the negative group, which was significantly different (P=0.024) (Table 2). The effect of FLT3-ITD mutations on the survival of APL patients was also analyzed. In the positive group, three patients died, all in the early stages. Two patients died from intracranial hemorrhages, including one patient with a pulmonary hemorrhage, and the third patient died from post-chemotherapy infection. In the negative group, one patient died of intracranial hemorrhage during the early stages, and the other patient underwent AML-M1 chemotherapy and died from poor efficacy three years after the onset. However, compared with the negative group, the EFS and OS in the positive group decreased significantly for five years, and the difference was found to be statistically significant (P=0.010; P=0.009) (Figures 1 and 2).
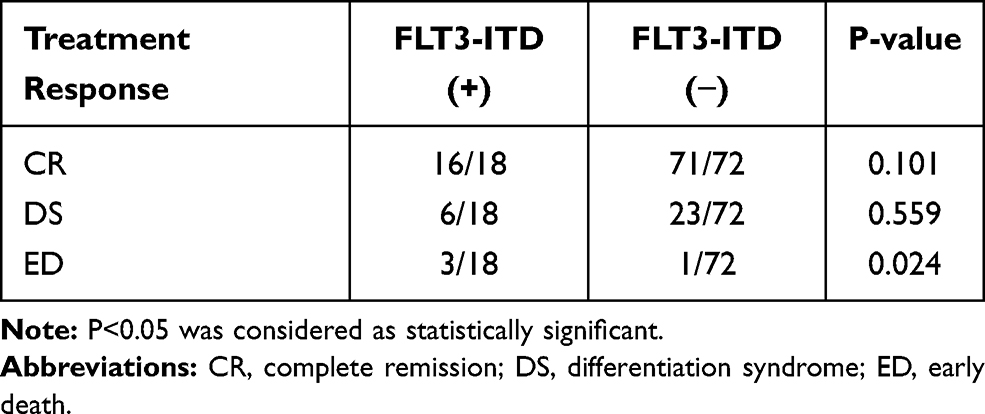 |
Table 2 Treatment Response Between FLT3-ITD Positive and FLT3-ITD Negative Patients |
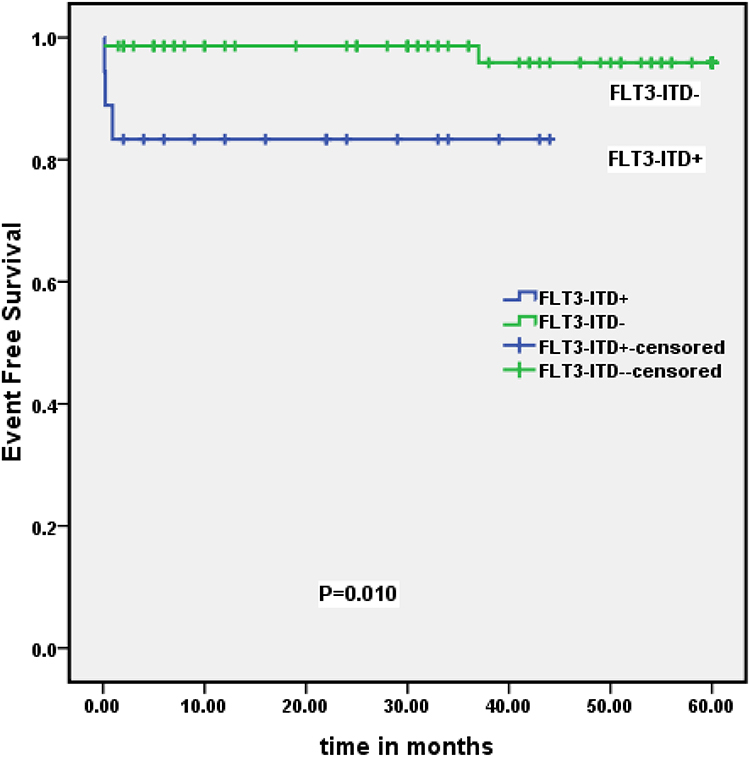 |
Figure 1 Association between the rate of 5-year event-free survival and FLT3-ITD gene mutation in patients’ groups. |
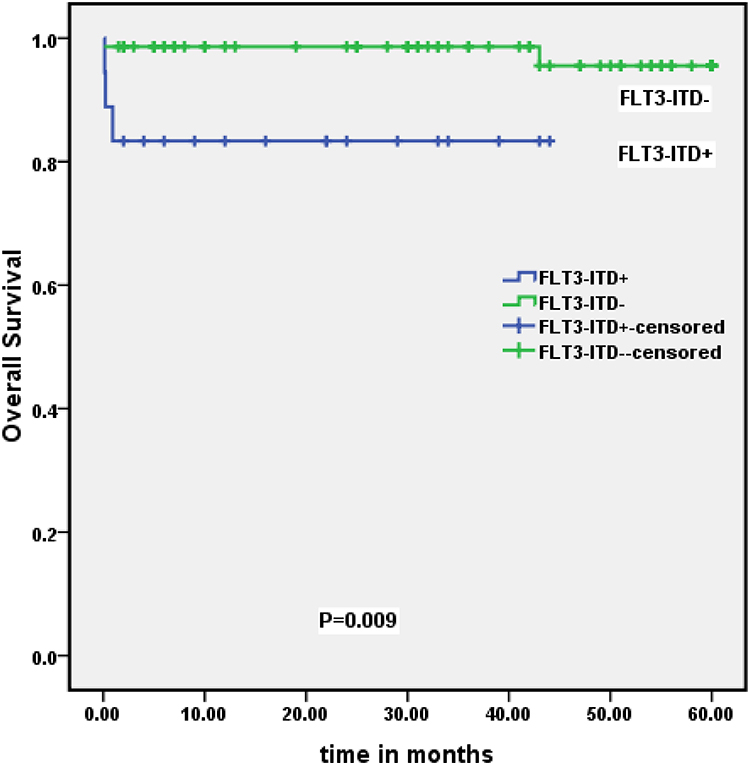 |
Figure 2 Association between the rate of overall survival and FLT3-ITD gene mutation in patients’ groups. |
Discussion
ATRA-based therapy has become the standard care for APL and can significantly extend both the DFS and OS in patients with APL. Since the 1990s, ATO has proved to a breakthrough in the treatment of recurrent and newly-diagnosed APL patients. APL has shifted from being a highly lethal to a manageable malignancy in most patients treated with ATRA and ATO therapy. However, APL is not a homogeneous disease. The Sanz score, based on initial WBC and PLT counts, has been widely used and accepted as a risk stratification as well as the treatment option as a practical prognostic model for APL patients.13 However, based on the various complexities involved in the molecular pathogenesis of APL, such as the occurrence of random mutations, the identification of novel sensitive markers may have practical clinical implications for APL risk stratification, and even for designing individualized treatment modalities. In addition to the PML-RARα fusion, the adverse effects of gene mutations, especially FLT3-ITD, on the prognosis of APL have attracted great attention in recent years. There is considerable evidence that molecular markers are associated not only with clinical characteristics at the onset of disease but can also be correlated to the drug response and the prognosis of acute myeloid leukemia (AML). Interestingly, the FLT3 gene, located on chromosome 13q12, can effectively regulate the proliferation and differentiation of hematopoiesis/progenitor cells through activating a signal transduction pathway upon interacting with its ligand (FL). FLT3 mutations are significantly common in AML, consisting mostly of internal tandem duplication mutations in the juxtamembrane domain of the gene (FLT3-ITD). Interestingly, the frequency of FLT3-ITD mutations has not been found to be consistent in APL patients (12–38%), and their presence did not necessarily affect all reported survival curves significantly.1–3,14 The prognostic significance of FLT3-ITD mutations in APL remains uncertain. The latest guidelines from the European Expert Group on Leukemia provide specific recommendations for optimizing the treatment of high-risk APL but do not provide specific recommendations for patients harboring FLT3 mutations.15 In this study, we retrospectively analyzed 90 newly-diagnosed APL patients who were treated with the ATRA+ATO dual induction regimen. The mutation rate of FLT3-ITD was 20%, lower than the 31–32% rate reported in Europe and America and more consistent with the 14.1–23.6% rate reported in China.6,8,16–18 While the incidence of FLT3-ITD mutations in patients with APL in China may be lower than that reported in the western countries, it may also be related to the smaller number of cases and selection bias in this study.
Our study found that the FLT3-ITD mutations was closely associated with high WBC counts in the newly-diagnosed patients, and the FLT3-ITD mutation rate in high-risk patients (WBC≥10×109/L) was significantly higher than that in medium-low risk patients (WBC<10×109//L). The baseline WBC count is one of the most powerful known prognostic factors in APL, and patients with a high WBC count (WBC≥10×109/L) generally have a poor prognosis. However, the role of the high WBC count in APL is not completely understood, and a considerable number of these patients may have FLT3-ITD mutations. Additionally, studies have found that PML-RARα can play a vital role in determining the disease phenotype of APL. However, evidence from transgenic mouse models showed that PML-RARα alone was not sufficient to induce significant development of leukemia.19,20 The effect on cell differentiation caused by t (15; 17) may cooperate with the promotion of proliferation conferred by the FLT3-ITD mutation, thereby leading to the development of promyelocytic leukemia. This carcinogenic collaboration has been demonstrated in the mouse models.21,22 FLT3-ITD mutations can lead to constitutive activation of the FLT3 in a ligand-independent manner, and thus can further activate abnormal signal transduction in downstream signaling pathways influencing cellular proliferation and differentiation (such as Jak-2/STAT5 and MAPK/Akt), thus promoting cell proliferation and inhibiting cellular apoptosis.23,24 Fan et al also reported that FLT3-ITD may be associated with leukocytosis and that FLT3-ITD can enhance the proliferation of leukemic cells.4 Interestingly, FLT3-ITD mutations have been found to be associated with high WBC counts and hemoglobin levels in patients with APL.1,2 Shen et al found that FLT3-ITD mutations were associated with both high WBC counts and sex during the initial diagnosis.25 The detection rate of FLT3-ITD mutations was higher in males. Luo et al found that not only were FLT3-ITD mutations associated with high WBC counts and hemoglobin levels in APL at the initial diagnosis, but were also associated with low PLT counts.6 Our study confirmed that FLT3-ITD mutations were associated with a high baseline WBC counts, but no significant correlations with other hematological characteristics were observed.
The remission rate of induction therapy in APL patients has been closely related to the prognosis, and the effect of FLT3-ITD mutations on the potential impact of ATRA+ATO chemotherapy in APL patients is still controversial. Poiré et al found that APL patients frequently displayed FLT3-ITD mutations and those without mutations had similar CR rates.8 However, other studies have indicated that the CR rate of patients with FLT3-ITD mutations is significantly lower than that of patients without the mutation.26,27 In this report, no statistical difference was observed in CR rates between patients with and without FLT3-ITD mutations, which is consistent with the results of Poiré et al.8 ATRA can also induce the maturation of immature cells, and the most common complication associated with the application of ATRA is DS. DS is an important cause of early death in APL and is characterized by increased WBC counts, fever, weight gain, and fluid retention (pulmonary infiltration and pleural effusion). In addition, various studies have shown that leukocytosis can be an independent prognostic factor for DS.28,29 Moreover, in the treatment plan based on ARTA + chemotherapy (AIDA), Breccia et al found that the incidence of ATRA syndrome in patients with FLT3-ITD mutations was significantly higher than that in patients lacking these mutations.30 However, in our study, the results showed that there was no statistical difference in DS incidence between patients with FLT3-ITD mutations and those without mutation after the ATRA+ATO dual-induction regimen. This observation may be related to the reduction or suspension of ATRA when leukocyte levels are significantly increased. It also suggested that the incidence of DS may be reduced compared with ATRA+ATO use alone, but large-scale controlled trials are needed to confirm this. Additionally, studies have also suggested that FLT3-ITD mutations may be correlated with early death in APL patients.27,31 Early death remains the leading cause of APL treatment failure. The early mortality of patients positive for FLT3-ITD mutations was also significantly higher than that of patients without mutations, which also confirmed these findings.
In APL patients, the FLT3-ITD mutation is common genetic event together wth t (15;17). Souza et al suggested that FLT3-ITD mutations may constitute different biological subsets of patients with APL, but the effect of such mutations on the patients’ prognosis remains uncertain.1,2,32 Based on ATRA and anthracycline chemotherapy, different studies have shown that FLT3-ITD can independently predict shorter survival rates in patients with APL.1,3 Other studies have also suggested that the addition of ATO to the induction therapy can eliminate the adverse prognosis caused by FLT3-ITD mutations. Moreover, FLT3-ITD mutations were not found to be associated with OS or DFS rates in patients treated with ATRA and ATO.25,33 On the contrary, some studies have indicated that there is no significant association between FLT3 mutations and OS or DFS regardless of whether patients are treated with standard treatment or consolidation regimens plus ATO. In this study, five-year EFS and OS rates of FLT3-ITD mutants were significantly lower compared to non-mutants, which was mainly attributed to the high early mortality rate of mutants. The reduction of disease-induction mortality in patients with FLT3-ITD mutations remains the key focus to improve the survival rate of these patients. However, induction therapy with ATO has failed to reverse the high-risk characteristics of FLT3-ITD mutations. The presence of FLT3-ITD mutation was still considered a poor prognostic factor of APL after ATRA+ATO induction regimen. The addition of novel drugs such as FLT3-ITD inhibitors, HDAC inhibitors, and CD33 monoclonal antibodies (GO) in APL patients with FLT3-ITD mutations may be a feasible strategy to adopt to develop individualized treatment regimens. Currently, Cenozoic FLT3 inhibitors have shown beneficial results in clinical trials of AML induction therapy combined with chemotherapy, which needs further confirmation in APL.34
Limitations of This Study
The study is primarily a single-center retrospective study; therefore, the sample size should be expanded to further confirm the significance of FLT3-ITD mutations in the prognosis of APL.
Disclosure
All authors declare that there are no conflicts of interest.
References
1. Lucena-Araujo AR, Kim HT, Jacomo RH, et al. Internal tandem duplication of the FLT3 gene confers poor overall survival in patients with acute promyelocytic leukemia treated with all-trans retinoic acid and anthracycline-based chemotherapy: an International Consortium on Acute Promyelocytic Leukemia study. Ann Hematol. 2014;93:2001–2010. doi:10.1007/s00277-014-2142-9
2. Souza Melo CP, Campos CB, Dutra ÁP, et al. Correlation between FLT3-ITD status and clinical, cellular and molecular profiles in promyelocytic acute leukemias. Leuk Res. 2015;39:131–137. doi:10.1016/j.leukres.2014.11.010
3. Beitinjaneh A, Jang S, Roukoz H, et al. Prognostic significance of FLT3 internal tandem duplication and tyrosine kinase domain mutations in acute promyelocytic leukemia: a systematic review. Leuk Res. 2010;34:831–836. doi:10.1016/j.leukres.2010.01.001
4. Fan Y, Cao Y, Bai X, et al. The clinical significance of FLT3 ITD mutation on the prognosis of adult acute promyelocytic leukemia. Hematology. 2018;23(7):379–384. doi:10.1080/10245332.2017.1415717
5. Picharski GL, Andrade DP, Fabro ALMR, et al. The impact of Flt3 gene mutations in acute promyelocytic leukemia: a meta-analysis. Cancers (Basel). 2019;11(9):1311. doi:10.3390/cancers11091311
6. Lou Y, Ma Y, Suo S, et al. Prognostic factors of patients with newly diagnosed acute promyelocytic leukemia treated with arsenic trioxide-based frontline therapy. Leuk Res. 2015;39(9):938–944. doi:10.1016/j.leukres.2015.05.016
7. Cicconi L, Divona M, Ciardi C, et al. PML-RARα kinetics and impact of FLT3-ITD mutations in newly diagnosed acute promyelocytic leukaemia treated with ATRA and ATO or ATRA and chemotherapy. Leukemia. 2016;30(10):1987–1992. doi:10.1038/leu.2016.122
8. Poiré X, Moser BK, Gallagher RE, et al. Arsenic trioxide in front-line therapy of acute promyelocytic leukemia (C9710): prognostic significance of FLT3 mutations and complex karyotype. Leuk Lymphoma. 2014;55(7):1523–1532. doi:10.3109/10428194.2013.842985
9. Cécile E, Ramy R, Kim LR, et al. FLT3-ITD impedes retinoic acid, but not arsenic, responses in murine acute promyelocytic leukemias. Blood. 2019;133(13):1495–1506. doi:10.1182/blood-2018-07-866095
10. Zhang ZN, Shen T. The Third Edition of the Criteria for Diagnosis and Efficacy of Blood Diseases. Beijing Science Press; 2007:106–116.
11. Zhang SJ, Li JY, Shi JY. Study on FLT3 gene mutations in acute myeloid leukemia. Chin J Hematol. 2007;28:124–126.
12. Han YL, Zhang SJ, Qiao C, et al. Study on FLT3 gene mutation in acute myeloid leukemia. Chin J Exp Hematol. 2009;17(5):1135–1139.
13. Sanz MA, Lo Coco F, Martin G, et al. Definition of relapse risk and role of nonanthracycline drugs for consolidation in patients with acute promyelocytic leukemia: a joint study of the PETHEMA and GIMEMA cooperative groups. Blood. 2000;96:1247–1253.
14. Barragán E, Montesinos P, Camos M, et al. Prognostic value of FLT3 mutations in patients with acute promyelocytic leukemia treated with all-trans retinoic acid and anthracycline monochemotherapy. Haematologica. 2011;96:1470–1477. doi:10.3324/haematol.2011.044933
15. Sanz MA, Fenaux P, Tallman MS, et al. Management of acute promyelocytic leukemia: updated recommendations from an expert panel of the European LeukemiaNet. Blood. 2019;133:1630–1643. doi:10.1182/blood-2019-01-894980
16. Gale RE, Hills R, Pizzey AR, et al. Relationship between FLT3 mutation status, biologic characteristics, and response to targeted therapy in acute promyelocytic leukemia. Blood. 2005;106(12):3768–3776. doi:10.1182/blood-2005-04-1746
17. Gong BF, Wang Y, Lin D, et al. Analysis of FLT3-ITD mutation in acute promyelocytic leukemia. Chin J Exp Hematol. 2016;24(6):1615–1621. doi:10.7534/j.issn.1009-2137.2016.06.001
18. Xu HL. The clinical significance of FLT3 gene mutation in acute promyelocytic leukemia. China Modern Med Appl. 2016;10(8):27–28.
19. Westervelt P, Ley TJ. Seed versus soil: the importance of the target cell for transgenic models of human leukemias. Blood. 1999;93:2143–2148. doi:10.1182/blood.V93.7.2143
20. Grimwade D, Enver T. Acute promyelocytic leukemia: where does it stem from? Leukemia. 2004;18:375–384. doi:10.1038/sj.leu.2403234
21. Kelly L, Kutok J, Williams I, et al. PML/RARalpha and FLT3-ITD induce an APL-like disease in a mouse model. Proc Natl Acad Sci U S A. 2002;99(12):8283–8288. doi:10.1073/pnas.122233699
22. Le Beau MM, Davis EM, Patel B, et al. Recurring chromosomal abnormalities in leukemia in PML-RARA transgenic mice identify cooperating events and genetic pathways to acute promyelocytic leukemia. Blood. 2003;102(3):1072–1074. doi:10.1182/blood-2003-01-0155
23. Meshinchi S, Appelbaum FR. Structural and functional alterations of FLT3 in acute myeloid leukemia. Clin Cancer Res. 2009;15(13):4263–4269. doi:10.1158/1078-0432.CCR-08-1123
24. Spiekermann K, Bagrintseva K, Schwab R, et al. Overexpression and constitutive activation of FLT3 induces STAT5 activation in primary acute myeloid leukemia blast cells. Clin Cancer Res. 2003;9(6):2140–2150.
25. Shen Y, Fu YK, Zhu YM, et al. Mutations of epigenetic modifier genes as a poor prognostic factor in acute promyelocytic leukemia under treatment with all-trans retinoic acid and arsenic trioxide. EBio Med. 2015;2(6):563–571.
26. Hong SD, Kim YK, Kim HN, et al. Treatment outcome of all-trans retinoic acid/anthracycline combination chemotherapy and the prognostic impact of FLT3/ITD mutation in acute promyelocytic leukemia patients. Korean J Hematol. 2011;46(1):24–30. doi:10.5045/kjh.2011.46.1.24
27. Kutny MA, Moser BK, Laumann K, et al. FLT3 mutation status is a predictor of early death in pediatric acute promyelocytic leukemia: a report from Children’s Oncology Group. Pediatr Blood Cancer. 2012;59:662–667. doi:10.1002/pbc.24122
28. Montesinos P, Bergua JM, Vellenga E, et al. Differentiation syndrome in patients with acute promyelocytic leukemia treated with all-trans retinoic acid and anthracycline chemotherapy: characteristics, outcome, and prognostic factors. Blood. 2009;113(4):775–783. doi:10.1182/blood-2008-07-168617
29. Jeddi R, Ghédira H, Mnif S, et al. High body mass index is an independent predictor of differentiation syndrome in patients with acute promyelocytic leukemia. Leuk Res. 2010;34(4):545–547. doi:10.1016/j.leukres.2009.09.017
30. Breccia M, Loglisci G, Loglisci MG, et al. FLT3-ITD confers poor prognosis in patients with acute promyelocytic leukemia treated with AIDA protocols: long-term follow-up analysis. Haematologica. 2013;98(12):e161–e163. doi:10.3324/haematol.2013.095380
31. Gale RE, Hills R, Pizzey A, et al. Relationship between FLT3 mutation status, biologic characteristics, and response to targeted therapy in acute promyelocytic leukemia. Blood. 2005;106:3768–3778.
32. Molica M, Breccia M. FLT3-ITD in acute promyelocytic leukemia: clinical distinct profile but still controversial prognosis. Leuk Res. 2015;39(4):397–399. doi:10.1016/j.leukres.2015.01.004
33. Hu J, Liu YF, Wu CF, et al. Long-term efficacy and safety of all-trans retinoic acid/arsenic trioxide-based therapy in newly diagnosed acute promyelocytic leukemia. Proc Natl Acad Sci. 2009;106:3342–3347. doi:10.1073/pnas.0813280106
34. Fathi AT, Chen YB. The role of FLT3 inhibitors in the treatment of FLT3-mutated acute myeloid leukemia. Eur J Haematol. 2017;98(4):330–336. doi:10.1111/ejh.12841
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.