Back to Journals » Clinical Ophthalmology » Volume 16
Potential Delay of Diagnosing Infraorbital Skin Tumors Due to Coverage by Face Masks During the COVID-19 Pandemic: An Observational Study
Authors Klingenstein A ![]() , Samel C, Hintschich C
, Samel C, Hintschich C
Received 29 July 2022
Accepted for publication 11 October 2022
Published 25 October 2022 Volume 2022:16 Pages 3581—3587
DOI https://doi.org/10.2147/OPTH.S384217
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Annemarie Klingenstein,1 Christina Samel,2 Christoph Hintschich1
1Department of Ophthalmology, Ludwig-Maximilians-University, Klinikum der Universität München, Campus Innenstadt, Munich, D-80336, Germany; 2Institute of Medical Statistics and Computational Biology, Faculty of Medicine, University of Cologne, Cologne, D-50924, Germany
Correspondence: Annemarie Klingenstein, Tel +49 89 44005 3811, Fax +49 89 44005 5160, Email [email protected]
Aim: To assess the potential danger of belated diagnosis or underdiagnosis of cutaneous infraorbital pathologies that are partially or fully covered by face masks worn due to the COVID-19 pandemic.
Methods: We evaluated data of 257 patients with infraorbital pathologies presenting at a large tertiary German university center between 04/2020 and 06/2021. This mono-centric, retrospective analysis included descriptive statistics and non-parametric tests.
Results: Out of 257 cutaneous infraorbital pathologies, 32 (12.5%) were partially and 20 (7.8%) fully covered by the required face mask. Significantly more patients with lesions that were partially or fully covered came from a single household (p=0.003, Fisher’s exact test) with 125 (48.6%) patients reportedly living alone. In patients with multiple periocular pathologies (n = 51, 19.8%), the risk of at least one periocular lesion being covered by the face mask was significantly elevated (p=0.009, Fisher’s exact test). As expected, malignant tumors were significantly larger than benign pathologies (largest diameter, malignant median 9.0mm, range 1.3– 34.0mm, mean 10.5mm, and benign median 3.0mm, range 1.0– 7.0mm, mean 4.3mm, respectively; p< 0.001, Mann–Whitney-U test) and patients presenting with malignant lesions were significantly older (median age 78.4, range 33– 93, mean 73.7 years versus median age 57.9, range 18– 90, mean 59.8 years, respectively; p< 0.001, Mann–Whitney-U test). Additionally, in subgroup analysis, patients with malignant lesions coming from single households were significantly older (p=0.041, Mann–Whitney-U test).
Conclusion: For adequate and timely treatment of infraorbital lesions, patients should be examined without their face mask. This is of utmost importance for the elderly (being at greater risk for malignant pathologies) and patients coming from single households. The presence of multiple pathologies must always be excluded.
Trial Registration Number: Not applicable.
Keywords: eyelid tumors, infraorbital, face mask, COVID-19 pandemic
Introduction
Due to safety regulations regarding the COVID-19 (Corona Virus Disease 2019) pandemic, all citizens ≥6 years of age in Bavaria, Germany, were required by law to wear a face mask covering the mouth and nose in all public areas from 27/04/20201 to the beginning of 2022 and are still strongly advised to do so as basic measure of protection.2 International medical societies recommend a minimum of face masks and face shields for all patients in order to slow the spread of COVID-19.3 Additionally, in Germany, contact with people outside the same household was temporarily restricted to one person and personal contact to residents in nursing homes by relatives was prohibited, therefore oftentimes widely limiting personal contact.
We could find no reports in common literature databases regarding the potential delay of tumor diagnosis due to coverage by face masks which is of importance for the Ophthalmologist regarding infraorbital lesions, but also for ENT (ear, nose and throat) or maxillofacial physicians.
Timely diagnosis of cutaneous tumors will facilitate surgical reconstruction, improve aesthetic results and even impact patient survival in cases of malignancies at risk of developing systemic disease such as eyelid squamous cell carcinoma.4,5
During the pandemic, examinations were largely symptom-oriented, performed without accompanying people allowed and, for safety reasons, time and potential virus distribution without face masks was reduced to a minimum.
We hypothesized that covering parts of the infraorbital and nasal regions by masks might result in belated diagnosis or potential miss of tumorous lesions in these areas by the treating general Ophthalmologists especially regarding elderly patients and patients living alone. We therefore retrospectively evaluated all patients having presented at our large tertiary university center with infraorbital skin tumors from 04/2020 to 06/2021.
Materials and Methods
For inclusion in this retrospective, mono-centric, observational study, patients were identified by searching the electronic database of the oculoplastic department of the eye clinic of Ludwig-Maximilians-University, Munich/Germany, for the diagnosis “lower eyelid tumor” and “infraorbital tumor”. Patients were clinically diagnosed with infraorbital lesions between 04/2020 and 06/2021. Only patients over 18 years of age at presentation and with histopathology findings were included into this study. Clinical data was extracted from the original patient files.
Approval was obtained from the ethics committee of Ludwig-Maximilians-University, Munich/Germany (vote number 21–0870). The patients photographed in Figures 1 and 2 have seen the photos and have read the article as presented for publication. Individual written informed consent was obtained. The study is in accordance with the Declaration of Helsinki.
 |
Figure 1 Outline demonstrating the average coverage of the mid-face due to masks on frontal portrait photography: Infraorbital line below the lower orbital fat pad over the lower orbital rims following a V-shape over the bridge of the nose (red line). This 83-year-old patient presented with 2 BCCs of which the infraorbital BCC was fully covered by the face mask. |
 |
Figure 2 Exemplary image of an infraorbital BCC that was partially covered by the patient’s face mask in an 81-year-old male patient from a single household. |
Data collected included histologic diagnosis as well as tumor extent (including largest tumor diameter in mm). Potential confounders included patient gender (female or male), patient age at diagnosis, time from first symptoms to diagnosis and lesion laterality (right or left eye, both eyes). Dependent variables were considered best corrected visual acuity (BCVA) [logMAR], tumor recurrence, presence of multiple lesions and whether the registered contact person was living within the same household.
At presentation in the oculoplastic department of the eye clinic at Ludwig-Maximilians-University, a detailed photodocumentation is performed of the patients’ face in primary position (without mask). Additionally, a tumor close-up in a well-lit room is taken prior to further therapy.
Histopathology findings were taken from the original reports. All tumors included were treated by surgical excision: Depending on the clinical diagnosis, tumor excision was performed by small incision in the eyelid (anterior or posterior incision depending on the location and the size of the lesion) (chalazion) or, excisional biopsy (benign tumors), incisional biopsy (exclusion of malignancy or large malignant tumors requiring definitive treatment decision by the interdisciplinary tumor board with exact histologic diagnosis) or by histologically controlled excision examining the excision margins microscopically for remaining tumor cells until all tumorous cells had been removed (suspected small to medium sized malignant tumors). Histopathologic assessment was performed by a certified ocular histopathologist following formalin-fixation, paraffin embedding, sectioning, staining with haematoxylin and eosin, PAS (periodic acid-Schiff) staining and immunohistology when required.
In order to estimate relevant average coverage of the mid-face by masks, we performed evaluation of portrait photography assuming coverage of the face starting from an infraorbital line below the lower orbital fat pad over the lower orbital rims following a V-shape over the bridge of the nose (Figure 1).
Statistical data collection was performed using Microsoft Excel (Microsoft Corporation, Redmond, WA, USA) for Mac 2019. Data analysis was performed with SPSS 26.0 (IBM Corporation; Armonk, NY, USA). Descriptive statistics, Fisher’s exact test and Mann–Whitney U-test were employed to assess the patients’ clinical and functional data. To avoid bias when evaluating clinical, histopathological data and photography, respective histopathology and clinical data were first recorded separately and combined for analysis only after completion of the data collection process. Statistical significance of differences was accepted for p<0.05 in two-tailed tests. As all statistical procedures are of exploratory nature, no adjustment for multiple testing has been made.
Results
Analysis was completed in 257 patients. Demographic data are shown in Table 1.
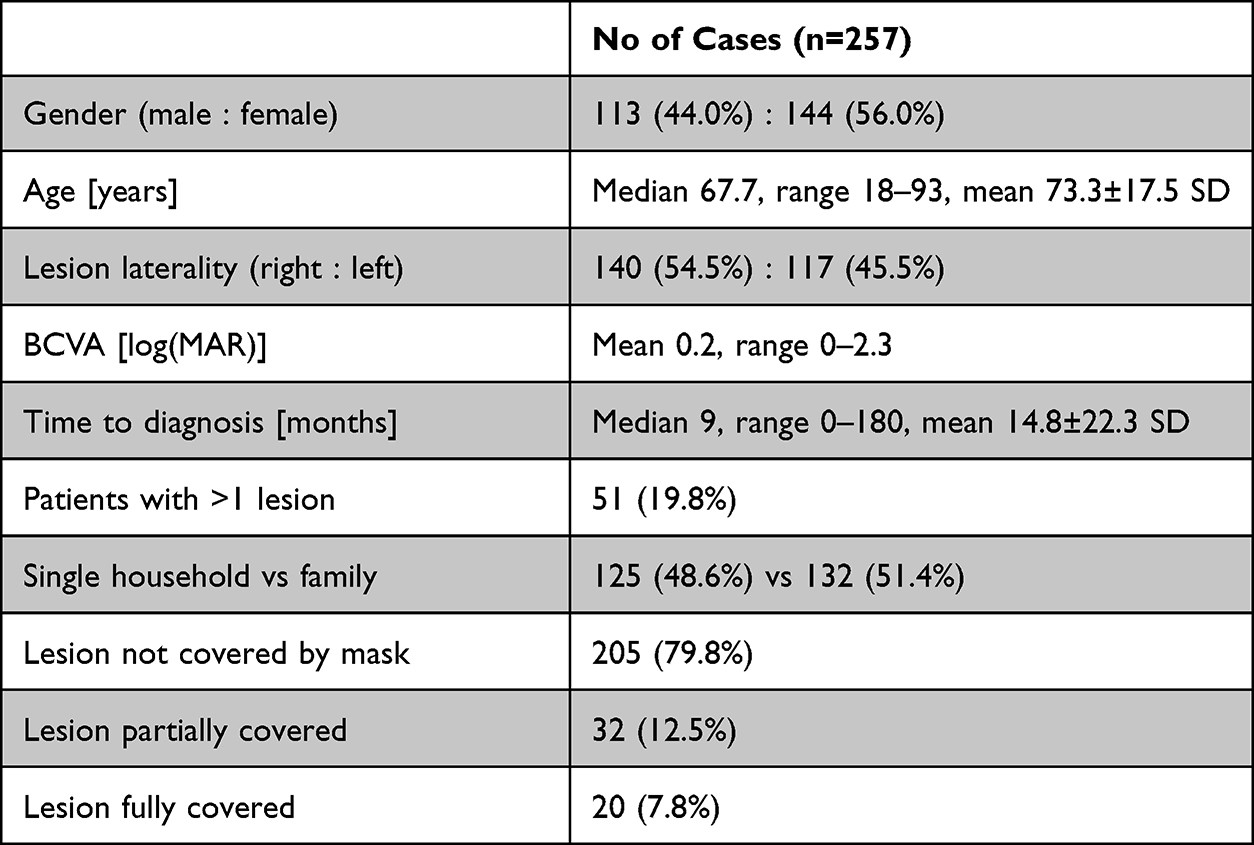 |
Table 1 Demographic Patient Data, SD: Standard Deviation |
A total of 112 patients (43.6%) presented with benign and 145 patients (56.4%) with malignant lesions.
Details on final diagnoses are elaborated in Table 2.
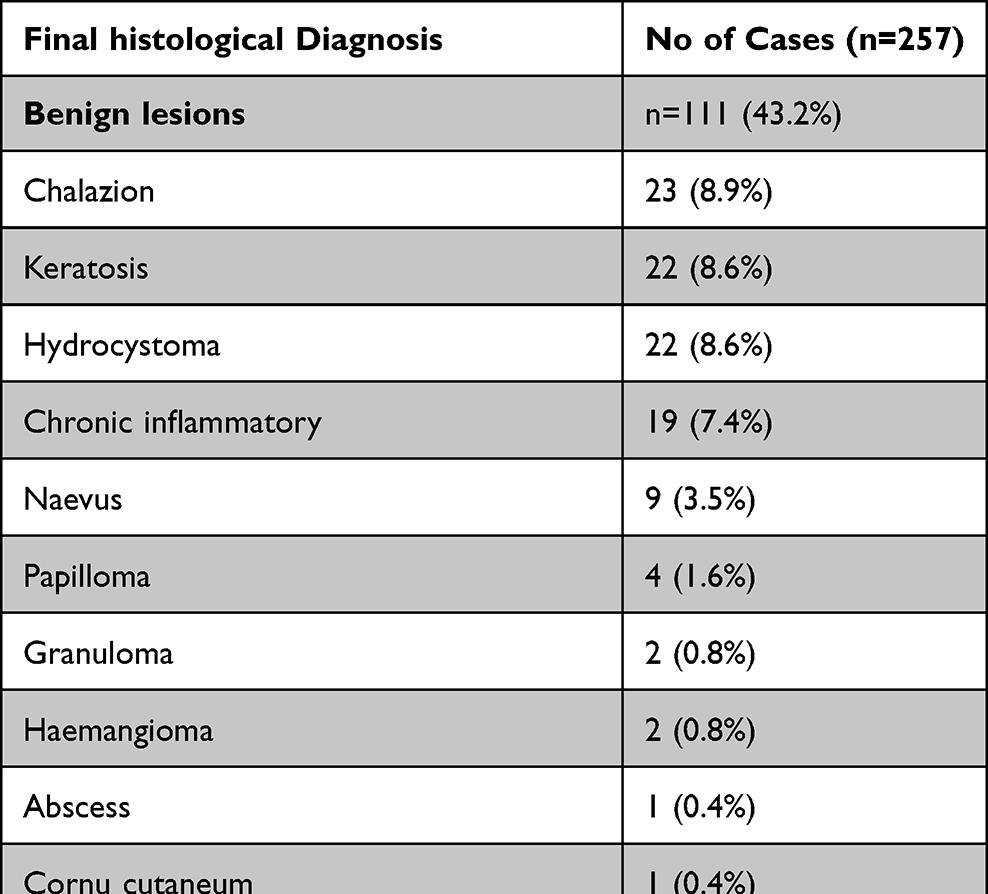 |
Table 2 Final Diagnosis of the Infraorbital Pathology from the Patients’ Medical File |
Documented surgical patient management included small incision in the eyelid depending on the location and the size of the lesion (chalazion), or excisional biopsy as a one-step procedure (n = 96, 37.4%), excision with microscopic examination of the margins for remaining tumor cells until all tumorous cells had been removed (two- or multiple step-procedure, respectively) (n = 141, 54.9%), and incisional biopsy (n = 20, 7.8%). Incisional biopsy resulted in malignant histology in 5 (of 20, 25%) cases and was followed by resection in 3 cases (1.2%) including additional adjuvant radiotherapy in one case and oral therapy with a hedgehog pathway inhibitor (vismodegib) alone in one case (0.4%). One patient declined further therapy after incisional biopsy (0.4%).
Fifty-one (19.8%) patients presented with more than one periocular lesion (33 (64.7%) patients with solely benign and 18 (35.3%) with at least one malignant lesion). In these patients, the risk of at least one periocular lesion being covered by the face mask was significantly elevated (p=0.009, Fisher’s exact test; 6 (11.8%) of lesions partially and 3 (5.9%) fully covered).
The lesion in question was partially covered by the face mask in 32 (12.5%, for exemplary image see Figure 2) and fully covered by the face mask in 20 (7.8%) patients. The infraorbital and lower lid lesions were not covered by the face mask in 205 cases (79.8%).
A total of 125 patients (48.6%) reported to be living in a single household. Importantly, significantly more patients with lesions that were partially or fully covered by the face mask came from a single household (p=0.003, Fisher’s exact test). Figure 3 demonstrates that percentages of full coverage of the infraorbital lesions were especially high in patients living in single households.
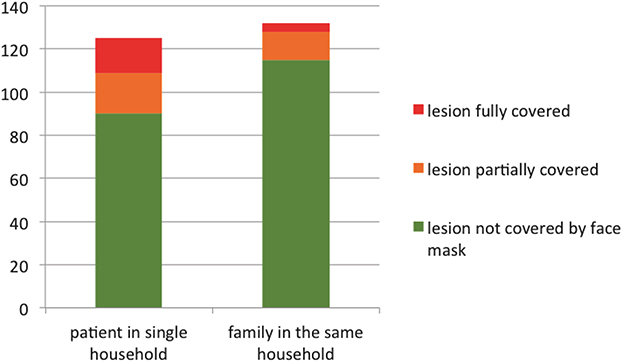 |
Figure 3 Diagram showing that 19 (15.2%) and 16 (12.8%) of 125 patients had partial and full coverage of an infraorbital lesion living in single households whereas 13 (9.8%) and 4 (3.0%) of 132 patients had partial and full coverage by the face mask in patients who reportedly lived in a household with family, respectively (p=0.003, Mann–Whitney-U test). |
BCVA was significantly lower in patients with larger tumor diameter (p < 0.001, Fisher’s exact test).
Malignant lesions were significantly larger than benign pathologies (largest diameter, malignant median 9.0mm, range 1.3–34.0mm, mean 10.5mm, and benign median 3.0mm, range 1.0–7.0mm, mean 4.3mm, respectively; p<0.001, Mann–Whitney-U test), and patients presenting with malignant lesions were significantly older (median age 78.4, range 33–93, mean 73.7, SD 13.1 years versus median age 57.9, range 18–90, mean 59.8, SD 19.3 years, respectively; p<0.001, Mann–Whitney-U test). In subgroup analysis that compared patients with malignant versus benign lesions, patients presenting with malignant lesions coming from a single household were significantly older (p=0.041, Mann–Whitney-U test) whereas there was no significant correlation between age and family status in patients presenting with benign lesions (p=0.943, Mann–Whitney-U test).
Discussion
The most important results of this study include that approximately 20% of infraorbital pathologies may be overlooked due to face masks if the mask is not transparent or removed during clinical examination. This number is meaningful, as predominantly malignant tumors have been reported to locate in the lower lid which, as in the present study, could be attributed to the majority of basal cell carcinomas (BCCs) with a predilection of the lower eyelid.6 Essentially, the present study shows that the presence of one periocular lesion warrants thorough examination for further pathologies. Furthermore, during isolation due to the pandemic, patients living in single households are at risk of underdiagnosis due to permanent coverage of the lesion by the face mask outside of the patients’ private household. This is especially important regarding malignant tumors in the elderly as these patients are at greater risk of presenting with malignant skin tumors7,8 due to longer duration of exposure to carcinogenic substances.7
Of course, large meta-analyses suggest that face masks provide a significant protective effect against the spread of SARS-CoV-2 (severe acute respiratory syndrome coronavirus 2).9
Yet, great benefit on the one hand may on the other hand also be accompanied by certain risks that must not be overlooked: As we could prove in this study, caution must be taken concerning potential coverage of lesions by face masks. In the literature, we retrieved a case report entitled “The COVID-19 facemask: Friend or foe?” reporting a non-viable median forehead interpolation flap due to compression caused by said face mask.10 The present study adds important data drawing attention to potential risks of wearing a face mask by reporting percentages of potential underdiagnosis of infraorbital tumors, more specifically for the elderly and patients living alone. The majority of data collected before the pandemic showed a higher percentage of benign compared to malignant lid tumors,8,11,12 which was in contrast to the findings in the present study and might be accounted for by the outer circumstances of the pandemic (fear of consultation at the hospital, restrictions in scheduling appointments etc). This is an interesting point for future research.
This study has certain limitations: During the pandemic, patients may have refrained from early presentation at their treating Ophthalmologists’ office due to the COVID-19 pandemic in general. Secondly, patients wear different types of masks that may cover variable parts of the mid-face. For the evaluation of this study, we assumed coverage of the face starting from a slightly V-shaped infraorbital line below the lower orbital fat pad over the lower orbital rims reaching the bridge of the nose centrally.
Furthermore, time from first symptoms to presentation in the clinic varied greatly (0–180 months) with patients with benign diagnosis generally presenting after a longer period in time due to only minor changes of the lesions in question. One could argument that these lesions might have been noticed by the patient and his environment prior to wear of a mask. Yet, for the purpose of this cross-sectional study, we wanted a clear cut-off period of cases presenting to our Ophthalmology department after legal requirement of wearing said face mask.
As expected, compared with the literature, patients presenting with malignant lesions (as cumulative solar damage mostly BCCs) were significantly older6–8,11,13 and malignant lesions significantly larger. BCC accounted for 83.0% of malignancies in this patient collective, which is in good accordance with previous publications from different parts of the world.7,8,12
We would assume from these presuppositions, that our meaningful number of patients represents good overall generalizability.
Conclusions
With the initiation of this study, we wanted to create general awareness that a thorough examination of each patient without the face mask should be included in every general ophthalmologic examination. This may specifically help timely diagnosis and treatment of infraorbital lesions in the elderly (who are at greater risk of developing cutaneous malignancies) as well as patients coming from single households and might uncover additional pathologies.
Abbreviations
BCC, basal cell carcinoma; COVID-19, corona virus disease 2019; PAS, periodic acid-Schiff; SARS-CoV-2, severe acute respiratory syndrome coronavirus 2; SD, standard deviation.
Data Sharing Statement
The blinded datasets used and analyzed during the current study are available from the corresponding author upon reasonable request.
Ethics Approval and Consent to Participate
Ethical approval for this study was obtained from and individual patient consent was waived by the ethics committee of Ludwig-Maximilians-University, Munich/Germany due to the retrospective, observational nature of this study (vote number 21-0870). All procedures performed (anonymous data analysis) in this retrospective study involving human participants were in accordance with the ethical standards of the institutional ethics committee and with the 1964 Helsinki declaration and its later amendments.
Consent for Publication
The patients photographed in Figures 1 and 2 have seen the photos and have read the article as presented for publication. Individual written informed consent for publication has been obtained from the patients.
Author Contributions
AK, CS and CH all made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. br24- Nachrichten. Ein Jahr Maskenpflicht in Bayern. One year of obligatory face masks in Bavaria [homepage on the Internet]; 2021. Available from: https://www.br.de/nachrichten/bayern/corona-ein-jahr-maskenpflicht-in-bayern,SVhTZwh.
2. Corona-Basisschutzmaßnahmen in Bayern verlängert bis zum 20. Basic corona protection measures prolonged until the 20th [homepage on the Internet]; August, 2022. Available from: https://www.vbw-bayern.de/vbw/vbw-Fokusthemen/Fokus-Corona/Allgemeines/16.-BayIfSMV.jsp.
3. MacKenzie EL, Poore SO. Slowing the spread and minimizing the impact of COVID-19: lessons from the past and recommendations for the plastic surgeon. Plast Reonstr Surg. 2020;146(3):681–689.
4. Xu S, Sagiv O, Rubin ML, et al. Validation study of the AJCC cancer staging manual, eighth edition, staging system for eyelid and periocular squamous cell carcinoma. JAMA Ophthalmol. 2019;37(5):537–542.
5. Klingenstein A, Samel C, Messmer EM, et al. Epidemiological characteristics and clinical course of eyelid squamous cell carcinoma patients from a large tertiary centre between 2009 and 2020. Br J Ophthalmol. 2022;106:1057–1062.
6. Huang YY, Liang WY, Tsai CC, et al. Comparison of the clinical characteristics and outcome of benign and malignant eyelid tumors: an analsysis of 4521 eyelid tumors in a tertiary medical center. Biomed Res Int. 2015;3:453091.
7. Pant N, Shrestha GB, Joshi SN, et al. Profile of ophthalmic tumors in adult Nepalese population in Central Nepal. Nepal J Ophthalmol. 2020;12(2):270–280.
8. Eren MA, Gündüz AK. Demographic features and histopathological diagnosis in primary eyelid tumors: results over 19 years from a tertiary center in Ankara, Turkey. Int J Ophthalmol. 2020;13(8):1287–1293.
9. Liang M, Gao L, Cheng C, et al. Efficacy of face mask in preventing respiratory virus transmission: a systematic review and meta-analysis. Travel Med Infect Dis. 2020;36:101751.
10. Hallock GG. The Covid-19 facemask: friend or foe? J Plast Reconst Aesthet Surg. 2021;74(5):1149–1150. doi:10.1016/j.bjps.2020.12.034
11. Deprez M, Uffer S. Clinicopathological features of eyelid skin tumors. A retrospective study of 5504 cases and review of literature. Am J Dermatopathol. 2009;31(3):256–262. doi:10.1097/DAD.0b013e3181961861
12. Yu SS, Zhao Y, Zhao H, et al. A retrospective study of 2228 cases with eyelid tumors. Int J Ophthalmol. 2018;11(11):1835–1841.
13. Asproudis I, Sotiropoulos G, Gartzios C, et al. Eyelid tumors at the university eye clinic of Ioannina, Greece: a 30-year retrospective study. Middle East Afr J Ophthalmol. 2015;22(2):230–232.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.