Back to Journals » Neuropsychiatric Disease and Treatment » Volume 18
Posttraumatic Stress Disorder, Suicidal Behavior, Substance Use, and Sexual Victimization Among Adolescent Girls Aged 10-19 Years Living Under Ethnic-Based Civil War in Ethiopia
Authors Wolde A ![]() , Dessalegn N
, Dessalegn N ![]()
Received 7 July 2022
Accepted for publication 1 October 2022
Published 11 October 2022 Volume 2022:18 Pages 2239—2250
DOI https://doi.org/10.2147/NDT.S381461
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Roger Pinder
Asrat Wolde,1 Nigatu Dessalegn2
1Department of Psychiatry, School of Medicine, Mizan Tepi University, Mizan Aman, Ethiopia; 2Department of Pediatric Health Nursing, Mizan Tepi University, Mizan Aman, Ethiopia
Correspondence: Asrat Wolde, Department of Psychiatry, School of Medicine, Mizan Tepi University, Mizan Aman, Ethiopia, Tel +251916389179, Email [email protected]
Background: Posttraumatic stress disorder (PTSD) is a chronic, impairing mental disorder that develops after exposure to a traumatic event. Despite many factors putting adolescent girls at risk of PTSD, little is known about the prevalence and how adolescent girls cope with the PTSD burden. So, this study aimed to investigate the prevalence of PTSD and associated factors among adolescent girls in three selected towns in Southwest Ethiopia.
Methods: A community-based cross-sectional study was conducted among 397 adolescent girls from May 27 to July 27, 2021. The participants were selected by a systematic random sampling method. PTSD and substance use disorder were assessed by DSM V criteria for mental disorders. The data was entered into Epi Data Manager Version 4.0.2 before being exported to SPSS Version 25 for analysis. A logistic regression model was used, and variables with a p-value less than 0.05 in the final fitting model were stated as independent predictors of PTSD.
Results: The prevalence of PTSD among the adolescent girls was 22%, and about three in four (72.7%) of the adolescent girls developed PTSD after exposure to sexual violence. Furthermore, PTSD was associated with Khat use disorder (AOR, 95% CI: 2.79 (1.47– 5.30), alcohol use disorder (AOR, 95% CI: 5.27 (2.21– 12.60), and suicidal behavior (AOR, 95% CI: 2.12 (1.20– 3.74)).
Conclusion: The prevalence of PTSD was high among adolescent girls, and suicidal ideation or attempt, khat use disorder, and alcohol use disorder were risk factors for PTSD. Therefore, early screening for PTSD and comorbid risk factors among this particular age group and managing accordingly is warranted.
Keywords: sexual violence, adolescent girls, khat use disorder, suicide, posttraumatic stress disorder, Ethiopia
Background
Posttraumatic stress disorder is a non-adaptive stress response phenomenon that can impair normal functionality and is characterized by repetitive intrusive thoughts, staying away from reminders, and re-experiencing traumatic experiences.1,2 PTSD can develop at any age after being exposed to injuries, death threats, or sexual abuse.3,4 Traumatic experiences can include physical abuse, sexual abuse, violent personal assault, terrorism, and partner violence.5–8The occurrence of any negative life events may not be sufficient to cause PTSD, but the degree to which an individual perceives them can lead to the development of PTSD.9
Posttraumatic stress disorder affects maternal and child health.10–12 PTSD can contribute to poverty, violence, unemployment, and poor social support.13,14 Many factors can contribute to the development of PTSD: such as genetics (family history of mental illness), substance use disorder, the degree of exposure to trauma, and other factors.15–17 PTSD can also be associated with suicide, exposure to sexual violence, and childhood sexual or physical abuse.18–20 Furthermore, PTSD has been linked to chronic medical illness, depression, and anxiety;21 poor quality of life;22–24 being a woman; lower educational level; age; unemployment; and marital status.25–27
Many PTSD patients develop substance abuse problems in their lifetime, and comorbid substance use disorder and posttraumatic stress disorder pose many psychosocial complications.28,29 Posttraumatic stress disorder was a risk factor for substance use relapse.30,31The self-medication hypothesis identifies that people with PTSD use substances to treat trauma-related negative emotional experiences.32 Furthermore, substance abusers had an increased vulnerability to trauma exposure due to immature coping or neurochemical brain changes due to substance abuse.33
Most of the studies examining PTSD among young women were conducted in western countries, giving priority to veterans only among older women.34–37 Only a few studies have been conducted in Africa. The lifetime and 12-month PTSD prevalence among the general population in South Africa was 2.3 and 0.7%, respectively,7 and another community survey of adult women in South Africa disclosed a prevalence of 11.6%.37 The prevalence of PTSD in South Africa among female rape survivors and adolescents was 87% and 6%, respectively.38,39 Several studies disclosed that the prevalence of PTSD was up to 66.7% in Nigeria.40–43
Despite the fact that females are three times more likely to develop posttraumatic stress disorder than males due to rape, childhood sexual assault, exposure to intimate partner violence,44 and having a more sensitized hypothalamic-pituitary-adrenal axis,45 little is known about posttraumatic stress disorder and associated factors among adolescent girls in low-income countries, including our own country, Ethiopia. To our knowledge, PTSD and its predictive factors among adolescent girls have not been investigated in our country, Ethiopia, or elsewhere. Therefore, the aim of this study was to assess posttraumatic stress disorder and associated factors among adolescent girls in Bonga, Mizan Aman, and Tepi towns located in an ethnic-based civil war region in southwest Ethiopia.
Methods and Materials
Study Design, Setting, and Period
The study was carried out in Mizan-Aman, Bonga, and Tepi Towns among adolescent girls aged 10–19 years from May 27 to July 27, 2021. Mizan-Aman town is located in Bench Sheko zone, 561 km away from Addis Ababa, which is the capital city of Ethiopia. Bonga town is located in the Kafa zone, 460 km away from Addis Ababa, while Tepi Town is located in the Masha zone, 611 km southwest of Addis Ababa. Mizan Aman town has two health centers and one teaching hospital, while there is one health center and one general hospital for both Bonga and Tepi Towns.
Study Population
The source population for this study was all adolescent girls in Bonga, Mizan Aman, and Tepi Towns. Any women who were unable to respond due to underlying physical and mental illness were excluded from the study.
Sample Size Determination and Sampling Techniques
The minimum required sample size for this study was calculated using a single population proportion formula. Since there was no previous study regarding posttraumatic stress disorder among adolescent girls in Ethiopia, we assumed a 50% proportion of Posttraumatic stress disorder, a precision level of 5%, a 95% confidence interval, and a 10% non-response rate. Accordingly, the estimated sample size was 422.
Then a systematic random sampling method was employed to select households in selected Kebele, which is the lowest administrative unit in Ethiopia. Mizan-Aman, Bonga, and Tepi Towns were specifically chosen due to their large population sizes. Thirty percent of each town’s kebele were chosen. Based on the total number of households in each kebele, the sample size was allocated proportionally. A list of respondents’ households was obtained from health extension workers. After obtaining a list of participant households, every 10th household was recruited by labeling each household that had adolescent girls aged 10–19 years, and the initial household was selected by a lottery method. A lottery method was also used if there were more than one eligible adolescent girl in a household.
Study Variables, Data Collection Tools, and Measurement
The dependent variable of the study was posttraumatic stress disorder. Age, religion, marital status, ethnicity, educational status, income status, employment, and residence were all independent variables, as were clinical factors (depression, chronic medical illness, suicidal ideation or attempt), lifetime trauma exposure (exposure to car accidents, war zones, violent death, and so on); childhood abuse (physical abuse, sexual abuse, or both); and social support.
Posttraumatic stress disorder was measured using the posttraumatic Stress Disorder Checklist for DSM V (PCL-5) to screen for PTSD symptoms. It is a twenty-item PTSD screening instrument for people who have experienced any type of traumatic event. It is the most commonly used instrument in cross-cultural settings. PCL-5 has a 5-point Likert scale from “not at all” (0) to “extremely” (4). From the total of 80, the cut point of 33 and above was considered for adolescent girls with PTSD. In this study, PCL-5 has a sensitivity of 0.96 and a specificity of 0.81.46–48
Substance (alcohol, khat, inhalants, cannabis, caffeine, and nicotine) use patterns were assessed using the DSM V criteria of substance use disorder, which included the following components: the amount of specific substance use for at least a year; the desire to cut down or many unsuccessful attempts to cut down or stop; spending a significant amount of time while using or obtaining a substance; the strong desire to use the substance; continuing substance use despite persistent social problems; preferring substance use over family, occupational, and recreational activities; using a substance in situations where it is physically hazardous (while driving, manipulating a machine, etc.); using a substance despite knowing that it has psychological and/or physical health problems; increasing the dose of the substance to achieve the desired effect or reduced efficacy when the usual amount is used; and experiencing psychological or physiological symptoms if the dose is decreased or stopped at all. In order to score a substance use disorder, adolescents must score two out of the eleven criteria for at least a year. Adolescents with mild, moderate, or severe substance use disorders must fulfill 2–3, 4–5, and 6 or more of the eleven criteria, respectively.49
The Patient Health Questionnaire-9 (PHQ-9) was used to assess depression, and study participants were considered depressed if their PHQ-9 score was 5 or higher.50 Suicidal ideation and attempt was assessed with the World Health Organization suicidal behavior assessment.51 The Oslo-3 social support scales were used to assess the social support status. According to the Oslo-3 social support scale, those who scored 3–8 were considered poor social support, those who scored 9–11 were considered moderate social support, and those who scored 12–14 were considered good social support.52
A life event check list was used to assess lifetime trauma exposure.53 If the adolescent girls were exposed to at least one traumatic life event, they had lifetime trauma exposure. The life event checklist was developed by the National Center for Posttraumatic Stress Disorder in order to detect post-traumatic stress symptoms. It was used in cross-cultural settings and was predictive of substance use disorders, anxiety symptoms, depression, and post-traumatic stress disorder.53
Childhood trauma was assessed using the Childhood Trauma Questionnaire (CTQ). The childhood trauma questionnaire has twenty-eight items: mini-scales with five items each quantifying emotional and physical neglect, and emotional, physical, and sexual abuse, and the last three items measure denial symptoms. Emotional abuse is all about verbal assaults and threatening behavior toward a person by someone who is older than a child. Physical abuse is all about bodily assaults, which can result in physical injury. Sexual abuse is all about sexual contact with a child or elderly person. Emotional neglect is all about the failure of caretakers to provide belongingness, love, encouragement, and help. Physical neglect is about being unable to meet basic biological needs such as food, shelter, and safety. The denial scale is about underreporting early trauma experiences. Each item has a score on a 5-point Likert scale. The higher the scores are, the more severe the intensity of childhood trauma. This study used the cut points used in other studies; greater than nine for physical neglect and abuse, greater than fourteen for emotional abuse, greater than twelve for emotional abuse, and greater than seven for sexual abuse. Adolescent girls who scored moderate-to-severe on one or more subscales were considered to have a history of childhood trauma.54
Data Quality Control
The information was gathered through the use of a standardized, structured, and interviewer administered questionnaire by a psychiatric clinicians. The English version of the questionnaires was translated into the local language of Amharic for the data collection. Three trained data collectors and two supervisors with a Bachelor of Science degree in psychiatry collected the data. The collected data were evaluated for completeness, clarity, and consistency by the supervisor and investigators on a daily basis.
Data Processing and Analysis
The collected data were coded and entered into Epi Data Manager Version 4.0.2 before being exported to SPSS Version 25 for analysis. Descriptive statistics like frequency distribution mean and SD were done for different variables. Bivariable logistic regression was used to identify the associations between the dependent and independent variables. Those variables with a p-value of< 0.25 on the bivariable logistic regression analysis were transferred to multivariable logistic regression. To include significant variables that might have clinical and practical reasoning, it is recommended to use a higher significance level (p-value of< 0.25) to a final model.55 In a multivariable logistic regression analysis, the adjusted odds ratio with a corresponding 95% CI was considered to declare the level of significance for PTSD.
Results
Socio-Demographic and Economic Characteristics
Of the total of 422 participants required to participate, only 397 adolescent girls participated due to refusal of 25 respondents, yielding a response rate of 94.07%. The mean of the participants’ ages was 14.34 years (SD = 2.78). All of the respondents were members of certain religions. The most common religion in this study was Ethiopian Orthodox Tewahido Church. Socio-demographic information is provided below in Table 1.
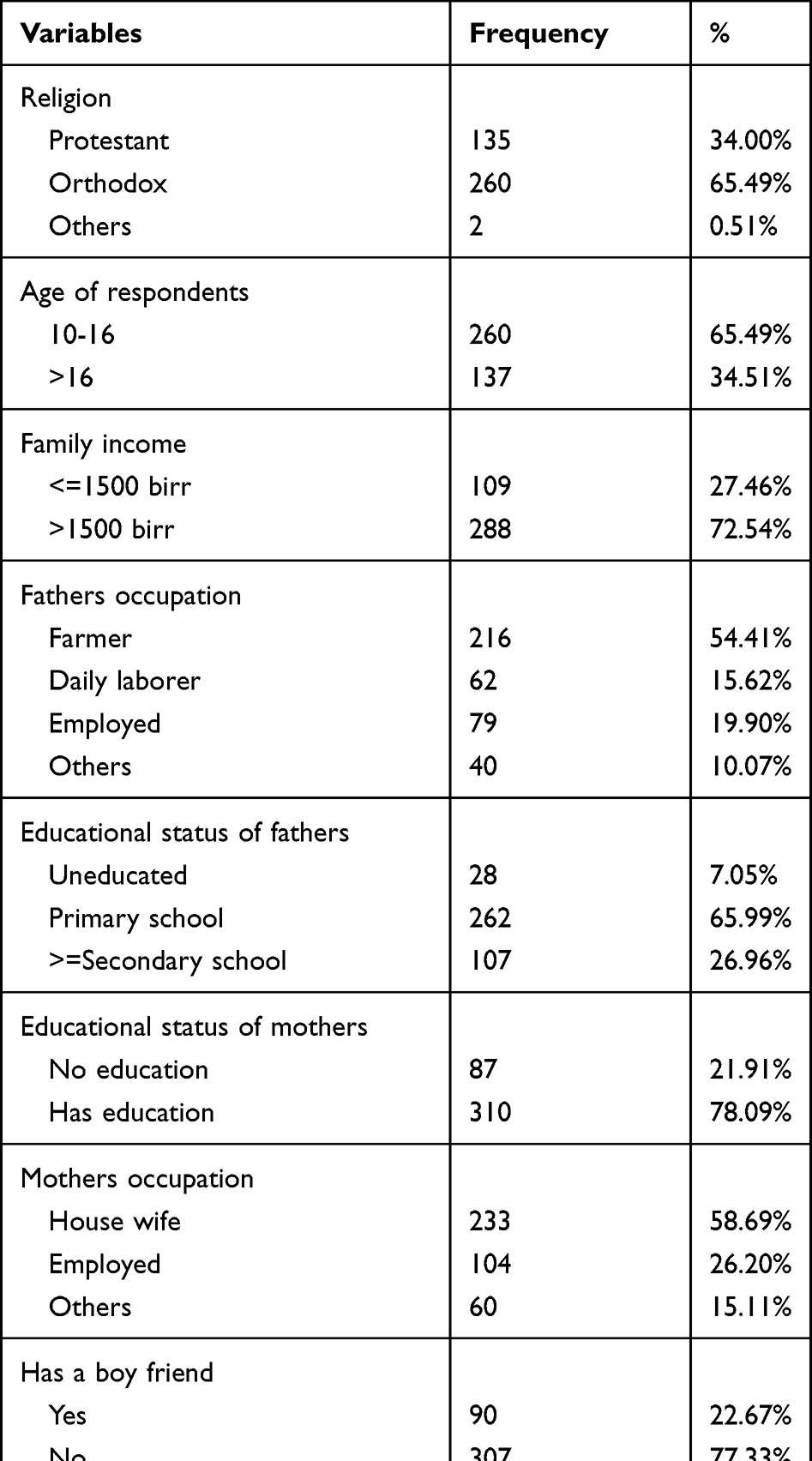 |
Table 1 The Socio-Demographic Factors of Adolescent Girls from Three Selected Towns in South West, Ethiopia (n=397) |
The Prevalence of Posttraumatic Stress Disorder
Although 66% of participants went through traumatic experiences, only 22% had or met the criteria for PTSD. In addition, 55(13.82%) of the respondents were exposed to violent death.
Substance-Related Variables
Of the total participants, 146 (36.78%) had alcohol use disorder; among them, 57 (14.36%), 48 (12.09%), and 41(10.33%) had mild, moderate, and severe alcohol use disorders, respectively. Of the total participants, 105 (26.45%) had a khat use disorder; among them, 95 (23.93%), 2 (0.50%), and 8(2.02%) had mild, moderate, and severe khat use disorders, respectively. Of the total participants, 56(14.11%) had a nicotine use disorder; among them, 5 (1.26%), 2 (0.50%), and 49(12.34%) had mild, moderate, and severe nicotine use disorders, respectively. Of the total participants, 35 (8.82%) had an inhalant use disorder; among them, 10(2.52%), 21 (5.29%), and 4(1.00%) had mild, moderate, and severe inhalant use disorders, respectively. Of the total participants, 346 (87.15%) had a caffeine use disorder; among them, 202 (51.88%), 138(34.76%), and 6(1.51%) had mild, moderate, and severe caffeine use disorders, respectively. Furthermore, of the total participants, 4 (1.01%) had a cannabis use disorder; among them; all of them had severe cannabis use disorder. Furthermore, only 77 (19.40%) of the total respondents were addicted to the internet. See Table 2
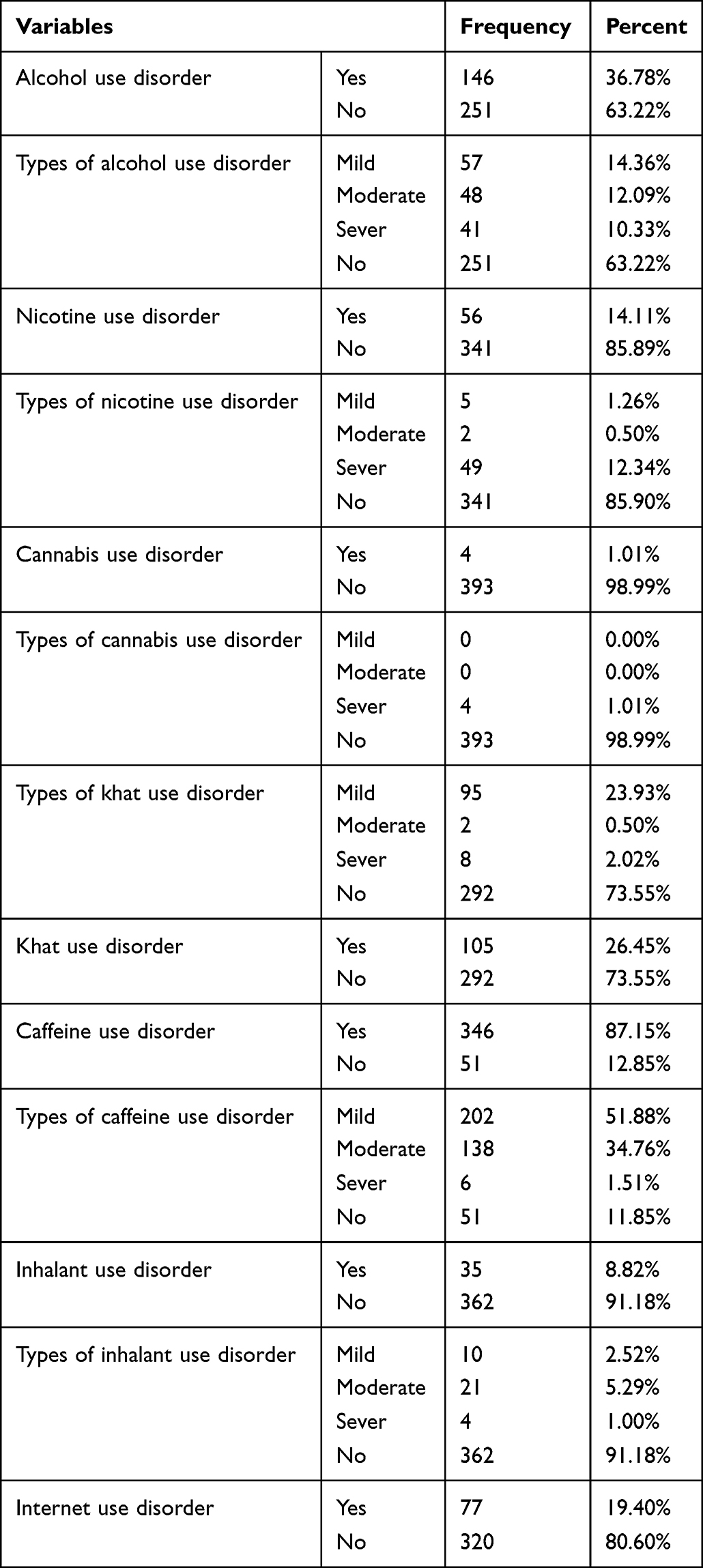 |
Table 2 The Specific Substance Use Disorder of Adolescent Girls from Three Selected Towns in South West, Ethiopia (n=397) |
The Clinical and Social Factors
Almost one in eight of the total participants, 52 (13.10%) had a chronic physical illness, and none of the respondents had regular physical exercise. More than half, 214(53.90%) of the adolescent girls had poor social support, and one fourth, 100 (25.19%) of the adolescent girls had poor sleep quality. Furthermore, more than one in four, 107(26.95%) of the adolescent girls had depression, and 60(15.11%) of the respondents had suicidal ideation or attempt. Table 3
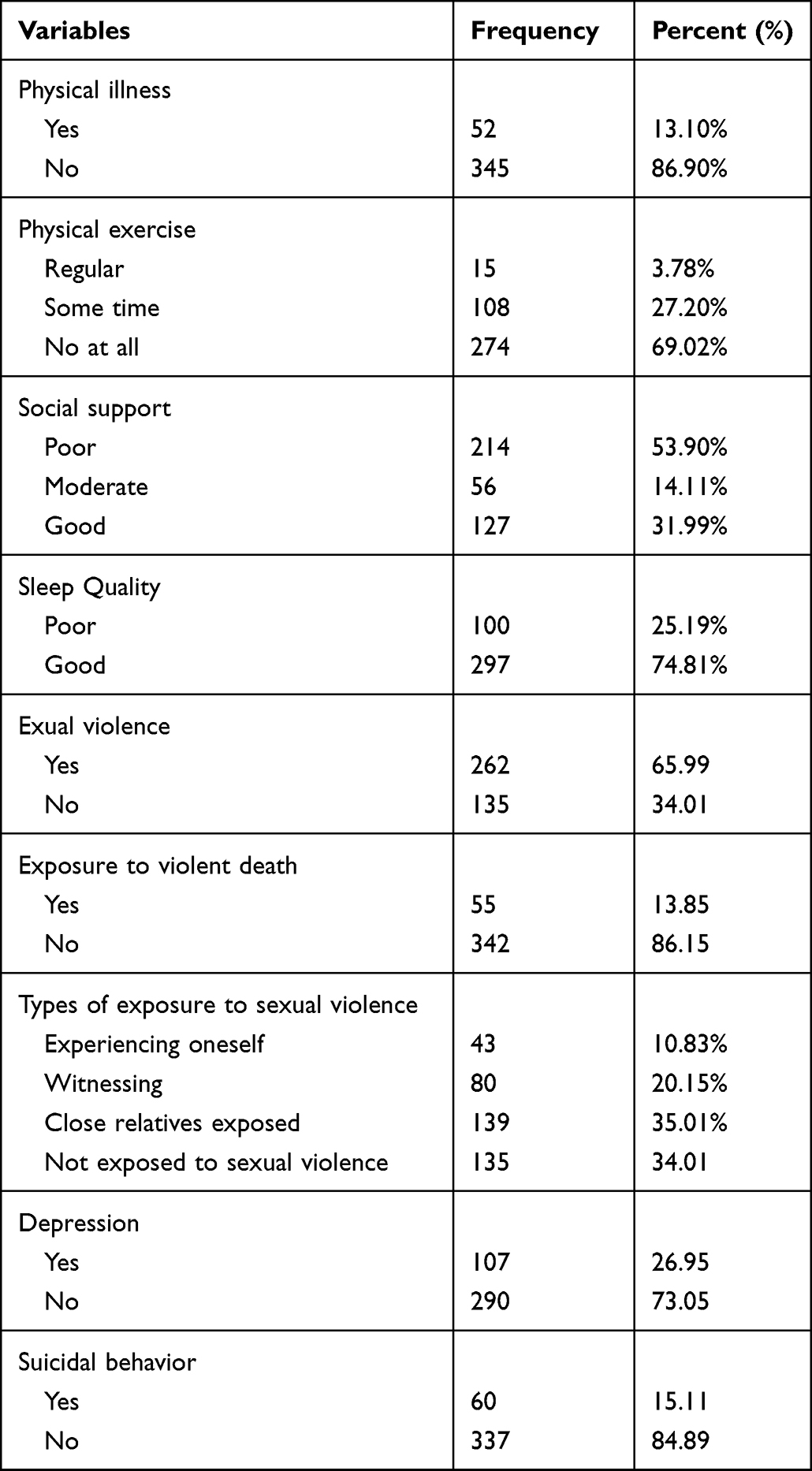 |
Table 3 The Clinical and Trauma-Related Factors of Adolescent Girls from Three Selected Towns in South West, Ethiopia (n=397) |
Factors Associated with Posttraumatic Stress Disorder Among Adolescent Girls
After bivariate analysis was conducted, those variables with p values of less than 0.25 in bivariable logistic regression analysis were entered into multivariable logistic regression analysis. However, khat use disorder, alcohol use disorder, and having suicidal behavior were independently associated with posttraumatic stress disorder among adolescent girls.
The odds of PTSD were 2.79 and 5.27 times higher in adolescent girls who had a khat use disorder and an alcohol use disorder, respectively, than their counterparts. Furthermore, girls who had suicidal ideation or attempts were 2.12 times more likely to have posttraumatic stress disorder. See Table 4
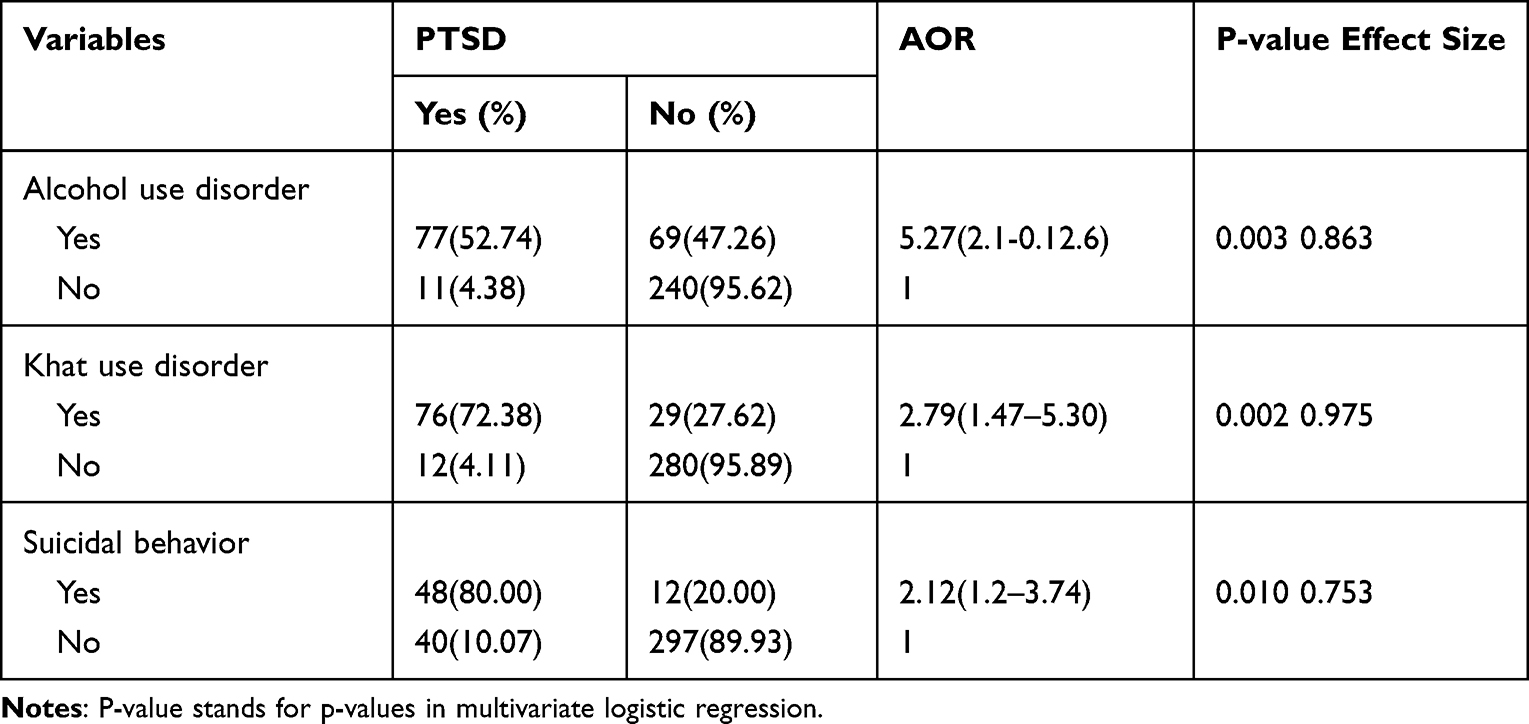 |
Table 4 Factors Associated with Posttraumatic Stress Disorder |
Discussion
This study was aimed at determining the prevalence of posttraumatic stress disorder and associated factors among adolescent girls. Accordingly, the prevalence of posttraumatic stress disorder was 22%, and alcohol use disorder, khat use disorder, and having suicidal behavior were independently associated with posttraumatic stress disorder among adolescent girls.
The magnitude of the PTSD in this study was comparable to that of a study conducted among women in Kenya.56 However, this finding was lower than the studies done in South Africa and the USA.57,58 The possible explanation for this variation could be the socio-economic and socio-cultural differences in the countries. Low-income countries such as Ethiopia are more vulnerable to traumatic events and people are not surprised when something terrible happen to them because they perceive the world as much more dangerous than they expect.59 Moreover, this finding is higher than the study done in Nigeria among slum dwellers.60 The possible reason could be that this study was done among adolescent girls displaced from their original home and girls living in a civil war region.
This study also discovered that khat use disorder was positively and significantly associated with posttraumatic stress disorder among adolescent girls. Adolescent girls with khat use disorder had about three times higher odds of being associated with PTSD than their counterparts. This finding was in line with the study conducted on the Somali refugee population and newly admitted Ethiopian prisoners, where khat use disorder was linked with more lifetime trauma experience and PTSD symptoms than non-khat users.61,62 The possible explanation for the association could be that adolescent girls with trauma experience might use khat to relieve trauma-related psychological distress, depressed mood, low concentration, and anxiety-related distress.63 The self-medication hypothesis of substance use and trauma might also work for khat users with trauma exposure and posttraumatic stress disorder. As a result, traumatized women might consume khat to deal with trauma-related negative emotional conditions.64–67
In addition, posttraumatic stress disorder was more common among adolescent girls who had suicidal ideation or attempts when compared with their counterparts. This finding was supported by studies done in other countries among adolescents.68,69The possible explanation could be that the lower serotonin level among patients with posttraumatic stress disorder is responsible for having an increased level of suicidal behavior.70 This study showed that more than half, 48(54.00%) of PTSD patients had suicidal behavior, which supports the previous finding that 80% of adolescent girl PTSD patients had suicidal behavior. This could be due to increased sexual violence among adolescent girls.71
This study also discovered that alcohol use disorder was a risk factor for posttraumatic stress disorder. This finding was in line with studies done in Florida and Washington in USA.72,73 The possible explanation could be people with substance use disorder were more vulnerable to trauma and PTSD due to their poor impulse control and risky behaviors such as careless driving and physical attack, and they place themselves and others in danger.33,72 The another possible explanation could be that adolescent girls exposed to PTSD might use alcohol to cope with unpleasant emotional symptoms such as flashbacks, intrusive thoughts, sleep disturbances, concentration problems, and aggressive or irritable reactions towards others.65,67
Finally, victims were referred to mental health centers, and since majority of perpetrators were armed, it was very difficult to catch them. We did, however, report any child abuse to the children and women affairs office, which was in charge of legal issues involving child and women abuse. In addition, we recommend using an integrated treatment approach for the treatment of PTSD and comorbid substance use disorder, as well as other psychiatric and medical comorbidities, rather than a traditional sequential intervention. The treatment approaches include psychopharmacological, exposure, and cognitive behavioral therapy, which was well tolerated and effective for PTSD patients. In addition, it is very important to consider the biological, sociological, and psychological intervention approaches for management of adolescent girls with PTSD.74
Limitation of the Study
As the existing data shows, this study is the first among adolescents, specifically adolescent girls in Ethiopia or elsewhere, to investigate PTSD and associated factors. Yet, the scientific community needs to understand some of the following gaps while understanding the results. Interviewer and recall bias, and participants might deny using substances. It is difficult to generalize to girls suffering from serious medical and mental illnesses. Medical history was also assessed by only a follow up card. Moreover, the chronological order or sequence of which came first, the substance use or the trauma, was not assessed, and comorbid psychiatric disorders except depression, suicide, substance use disorders, and sleep were not assessed.
Conclusion
This study showed that about one in five adolescent girls had posttraumatic stress disorder. Khat use disorder, alcohol use disorder, and suicidal behavior were identified as significant predictors of posttraumatic stress disorder among adolescent girls in Ethiopia. Therefore, screening and early intervention for posttraumatic stress disorder among this particular age group is crucial, specifically among girls displaced from or living in a civil war region. It is also imperative to design effective health education and promotion considering the identified predictors of posttraumatic stress disorder among this segment of the population.
Abbreviations
AOR, Adjusted Odds Ratio; CI, Confidence Interval; PTSD, Post Traumatic Stress Disorder; DSM V, Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition.
Data Sharing Statement
Data will be available from the corresponding author upon reasonable request.
Ethical Approval
For the commencement of data collection, ethical clearance and a supportive letter were obtained from Mizan Tepi University College of Medicine and Health Sciences. Informed consent and assent was obtained from study subjects, and their guardians after the objective of the study was clearly informed. Personal identifiers were omitted to maintain the confidentiality of the information. Moreover, the collected data is kept safe throughout the whole data collection and analysis process. This study was conducted in accordance with the Helsinki Declaration for Research Ethics.
Acknowledgments
We would like to thank the data collectors and supervisors for their cooperation. We also extend our appreciation to the study participants for their kind support during data collection.
Author Contributions
The authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that they have no conflicts of interest.
References
1. Scher CD, McCreary DR, Asmundson GJG, Resick PA. The structure of posttraumatic stress disorder symptoms in three female trauma samples: a comparison of interview and self-report measures. J Anxiety Disord. 2008;22(7):1137–1145. doi:10.1016/j.janxdis.2007.11.012
2. Radell ML, Beck KD, Gilbertson MW, Myers CE. Post-traumatic stress disorder symptom burden and gender each affect generalization in a reward- and punishment-learning task. PLoS One. 2017;12(2):e0172144. doi:10.1371/journal.pone.0172144
3. Iribarren J, Prolo P, Neagos N, Chiappelli F. Post-traumatic stress disorder: evidence-based research for the third millennium. Evid Based Complement Alternat Med. 2005;2(4):503–512. doi:10.1093/ecam/neh127
4. Stein DJ, Karam EG, Shahly V, et al. Posttraumatic stress disorder associated with life-threatening motor vehicle collisions in the WHO world mental health surveys. BMC Psychiatry. 2016;16(1):1–14. doi:10.1186/s12888-016-0957-8
5. Chemtob CM, Gudiño OG, Luthra R, et al. Child trauma exposure and posttraumatic stress disorder: identification in community mental health clinics. Evid Based Pract Child Adolescent Mental Health. 2016;1(2–3):103–115. doi:10.1080/23794925.2016.1227949
6. Sheriff RS, van Hooff M, Malhi G, Grace B, McFarlane A. Associations of childhood trauma and childhood mental disorder with past year mental disorder in military and civilian employedmen. Psychiatry Res. 2019;280:1–36. doi:10.1016/j.psychres.2019.112482
7. Atwoli L, Stein DJ, Williams DR, et al. Trauma and posttraumatic stress disorder in South Africa: analysis from the South African stress and health study. BMC Psychiatry. 2013;13(1):182. doi:10.1186/1471-244X-13-182
8. Kleber RJ. Trauma and public mental health: a focused review. Front Psychiatry. 2019;10(451):1–6. doi:10.3389/fpsyt.2019.00451
9. Willard VW, Long A, Phipps S. Life stress vs traumatic stress: the impact of life events on psychological functioning in children with and without serious illness. Psychol Trauma Theory Res Pract Policy. 2016;8(1):63–71. doi:10.1037/tra0000017.Life
10. Garthus-Niegel S, Horsch A, Handtke E, et al. The Impact of Postpartum Posttraumatic Stress and Depression Symptoms on Couples’ Relationship Satisfaction: a Population-Based Prospective Study. Front Psychol. 2018;9:1728.
11. Dekel S, Stuebe C, Dishy G. Childbirth Induced Posttraumatic Stress Syndrome: a Systematic Review of Prevalence and Risk Factors. Front Psychol. 2017;8:560. doi:10.3389/fpsyg.2017.00560
12. Garthus-Niegel S, Horsch A, Ayers S, Junge-Hoffmeister J, Weidner K, Eberhard-Gran M. The influence of postpartum PTSD on breastfeeding: a longitudinal population-based study. Birth. 2018;45:193–201. doi:10.1111/birt.12328
13. Akinyemi OO, Owoaje ET, Ige OK, Popoola OA. Comparative study of mental health and quality of life in long term refugees and host populations in Oru-Ijebu, Southwest Nigeria. BMC Res Notes. 2012;5:394. doi:10.1186/1756-0500-5-39435
14. Priebe S, Matanov A, Janković Gavrilović J, McCrone P, Ljubotina D, Knežević G. Consequences of untreated posttraumatic stress disorder following war in former Yugoslavia: morbidity, subjective quality of life, and care costs. Croat Med J. 2009;50(5):465–475. doi:10.3325/cmj.2009.50.46536
15. Keane TM, Marshall AD, Taft CT. Posttraumatic stress disorder: etiology, epidemiology, and treatment outcome. Annu Rev Clin Psychol. 2006;2(1):161–197. doi:10.1146/annurev.clinpsy.2.022305.09530537
16. Essizoglu A, Keser I. Post-traumatic stress disorder in internally displaced people subjected to displacement by armed forces. J Trauma Stress Disor Treat. 2014;3(2):2–6.
17. Ergun D, Çakici M, Çakici E. Comparing psychological responses of internally displaced and non-displaced Turkish Cypriots. Torture. 2008;18(1):20–28.
18. Andersen LB, Melvaer LB, Videbech P, Lamont RF, Joergensen JS. Risk factors for developing post-traumatic stress disorder following childbirth: a systematic review. ACTA Obstet Gynecol Scand. 2012;91:1261–1272. doi:10.1111/j.1600-0412.2012.01476.x
19. Stramrood CAI, Paarlberg KM, Huis In ’t Veld EMJ, et al. Posttraumatic stress following childbirth in homelike- and hospital settings. J Psychosom Obstet Gynaecol. 2011;32(2):88–97. doi:10.3109/0167482X.2011.569801
20. Hernández-Martínez A, Rodríguez-Almagro J, Molina-Alarcón M, Infante-Torres N, Rubio-álvarez A, Martínez-Galiano JM. Peri-natal factors related to post-traumatic stress disorder symptoms 1–5 years following birth. Women Birth. 2020;33:129–135. doi:10.1016/j.wombi.2019.03.008
21. Flory JD, Yehuda R. Comorbidity between post-traumatic stress disorder and major depressive disorder: alternative explanations and treatment considerations. Dialogues Clin Neurosci. 2015;17(2):141–150. doi:10.31887/DCNS.2015.17.2/jflory
22. Lohr JB, Palmer BW, Eidt CA, et al. Is post-traumatic stress disorder associated with premature senescence? A review of the literature HHS public access. Am J Geriatr Psychiatry. 2015;23(7):709–725. doi:10.1016/j.jagp.2015.04.001
23. McMillan KA, Asmundson GJG, Sareen J. ComorbidPTSD and social anxiety disorder: associations with quality of life and suicide attempts. J Nerv Ment Dis. 2017;205(9):732–737. doi:10.1097/NMD.0000000000000704
24. Danielsson FB, Schultz Larsen M, Nørgaard B, Lauritsen JM. Quality of life andlevel of post-traumatic stress disorder among trauma patients: a comparative study between a regional and a university hospital’. Scand J Trauma Resusc Emerg Med. 2018;26(1):1–9. doi:10.1186/s13049-018-0507-0
25. Olff M. Sex and gender differences in post-traumatic stress disorder: an update. Eur J Psychotraumatol. 2017;8(sup4):1351204. doi:10.1080/20008198.2017.1351204
26. Frankenberg E, Sikoki B, Sumantri C, Suriastini W, Thomas D. Education, vulnerability, and resilience after a natural disaster. Ecol Soc. 2013;18:2. doi:10.5751/ES-05377-180216
27. Jacobsen LK, Southwick SM, Kosten TR. Substance use disorders in patients with posttraumatic stress disorder: a review of the literature. Am J Psychiatry. 2001;158(8):1184–1190. doi:10.1176/appi.ajp.158.8.1184
28. Gros DF, Flanagan JC, Korte KJ, Mills AC, Brady KT, Back SE. Relations between Social Support, PTSD Symptoms, and Substance Use in Veterans. Psychol Addict Behav. 2016;30(7):764–770. doi:10.1037/adb0000205
29. Odenwald M, Semrau P. Reducing dropout among traumatized alcohol patients in detoxification treatment: a pilot intervention study. Eur Addict Res. 2012;18(2):54–63. doi:10.1159/000333336
30. Waldrop AE, Back SE, Verduin ML, Brady KT. Triggers for cocaine and alcohol use in the presence and absence of posttraumatic stress disorder. Addict Behav. 2007;32(3):634–639. doi:10.1016/j.addbeh.2006.06.001
31. Boys A, Marsden J, Stillwell G, Hatchings K, Griffiths P, Farrell M. Minimizing respondent attrition in longitudinal research: practical implications from a cohort study of adolescent drinking. J Adolesc. 2003;26(3):363–373. doi:10.1016/S0140-1971(03)00011-3
32. Brown PJ, Wolfe J. Substance abuse and post-traumatic stress disorder comorbidity. Drug Alcohol Depend. 1994;35(1):51–59. doi:10.1016/0376-8716(94)90110-4
33. Ryb GE. PTSD after severe vehicular crashes. Ann Adv Automot Med. 2009;53:177–193.
34. Richardson LK, Frueh BC, Acierno R. Prevalence estimates of combat-related post-traumatic stress disorder: critical review. Aust N Z J Psychiatry. 2010;44(1):4–19. doi:10.3109/00048670903393597
35. Dursa EK, Reinhard MJ, Barth SK, Schneiderman AI. Prevalence of a positive screen for PTSD among OEF/OIF and OEF/OIF-era veterans in a large population-based cohort. J Trauma Stress. 2014;27(5):542–549. doi:10.1002/jts.21956
36. Magruder K, Serpi T, Kimerling R, et al. Prevalence of posttraumatic stress disorder in Vietnam-era women veterans: the health of Vietnam-era women’s study (HealthVIEWS). JAMA Psychiatry. 2015;72(11):1127–1134. doi:10.1001/jamapsychiatry.2015.1786
37. Machisa MT, Christofides N, Jewkes R. Mental ill health in structural pathways to women’s experiences of intimate partner violence. PLoS One. 2017;12(4):e0175240. doi:10.1371/journal.pone.0175240
38. Mbalo N, Zhang M, Ntuli S. Risk factors for PTSD and depression in female survivors of rape. Psychol Trauma Theory Res Pract Policy. 2017;9(3):301–308. doi:10.1037/tra0000228
39. Swain KD, Pillay BJ, Kliewer W. Traumatic stress and psychological functioning in a South African adolescent community sample. S Afr J Psychiatry. 2017;23(1):1–6. doi:10.4102/sajpsychiatry.v23i0.1008
40. Sheikh TL, Mohammed A, Eseigbe E, et al. Descriptive characterization of psycho-trauma, psychological distress, and post-traumatic stress disorder among children and adolescent Internally Displaced persons in Kaduna, Nigeria. Front Psychiatry. 2016;7:179. doi:10.3389/fpsyt.2016.00179
41. Iteke O, Bakare MO, Agomoh AO, Uwakwe R, Onwukwe JU. Road traffic accidents and posttraumatic stress disorder in an orthopedic setting in south-Eastern Nigeria: a controlled study. Scand J Trauma Resusc Emerg Med. 2011;19(1):39. doi:10.1186/1757-7241-19-39
42. Asuquo JE, Edet BE, Abang IE, et al. ‘Depression and posttraumatic stress disorder among road traffic accident victims managed in a tertiary hospital in southern Nigeria’. Niger J Clin Pract. 2017;20(2):170–175. doi:10.4103/1119-3077.196114
43. Mishara WL, Gbaden EA. The prevalence of depression among the youths as an aftermath of the internal insurgency attacks in Maiduguri, Nigeria\n. IOSR J Hum Soc Sci. 2014;19(10):32–35. doi:10.9790/0837-191073235
44. McLaughlin KA, Koenen KC, Hill ED, et al. Trauma exposure and posttraumatic stress disorder in a national sample of adolescents. J Am Acad Child Adolesc Psychiatry. 2013;52:815–830. doi:10.1016/j.jaac.2013.05.011
45. Olff M. Sex and gender differences in post-traumatic stress disorder: an update. Eur J Psychotraumatol. 2017;8:1351204. doi:10.1080/20008198.2017.1351204
46. Weathers FW, Litz BT, Herman DS, Huska JA, Keane TM. The PTSD Checklist: reliability, validity, & diagnositic utility. Annu Meet Int Soc. 1993;1:548.
47. Weathers FW, Blake DD, Schnurr PP, Kaloupek DG, Max BP, Keane TM. The life event checklist for DSM-5 (LEC-5). National Center for PTSD; 2013. Available from: Www.ptsd.va.gov.
48. Blanchard EB, Jones-Alexander J, Buckley TC. Forneris. CA Psychometric properties of the PTSD Checklist (PCL). Behav Res Ther. 1996;34:669–673. doi:10.1016/0005-7967(96)00033-2
49. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders.
50. Gelaye B, Williams MA, Lemma S, et al. Validity of the patient health questionnaire-9 for depression screening and diagnosis in East Africa. Psychiatry Res. 2013;210(2):653–661. doi:10.1016/j.psychres.2013.07.015
51. World Health Organization. Suicidal Ideation and Attempt Screening Tool. World Health Organization; 2015
52. Bøen H, Dalgard OS, Bjertness E. The importance of social support in the associations between psychological distress and somatic health problems and socio-economic factors among older adults living at home: a cross sectional study. BMC Geriatr. 2012;12(1):27. doi:10.1186/1471-2318-12-27
53. Gray MJ, Litz BT, Hsu JL, Lombardo TW. Psychometric properties of the life events checklist, Assessment. Assessment. 2004;11(4):330–341. doi:10.1177/1073191104269954
54. Choi JY, Choi YM, Kim B, Lee DW, Gim MS, Park SH. The effects of childhood abuse on self-reported psychotic symptoms in severe mental illness: mediating effects of posttraumatic stress symptoms. Psychiatry Res. 2015;229(1–2):389–393. doi:10.1016/j.psychres.2015.05.112
55. Hosmer DW, Lemeshow S, Sturdivant RX. Applied Logistic Regression. New YORK: John Wililey & Sons, Incorporated; 2013.
56. Mbwayo AW, Ndetei DM, Mutiso V, Khasakhala LI. Traditional healers and provision of mental health services in cosmopolitan informal settlements in Nairobi, Kenya. Afr J Psychiatry. 2013;16(2):134–140. doi:10.4314/ajpsy.v16i2.17
57. Jain KM, Davey-Rothwell M, Crossnohere NL, Latkin CA. Post-traumatic stress disorder, neighborhood residency and satisfaction, and social network characteristics among underserved women in Baltimore, Maryland. Womens Health Issues. 2018;28(3):273–280. doi:10.1016/j.whi.2018.02.004
58. Ndungu J, Ramsoomar L, Willan S, Washington L, Ngcobo-Sithole M, Gibbs A. Depression, posttraumatic stress disorder (PTSD) and their comorbidity: implications of adversity amongst young women living in informal settlements in Durban, South Africa. J Affect Disorders Rep. 2020;1:100022. doi:10.1016/j.jadr.2020.100022
59. Michel LA, Duckers EA, Brown CR. A vulnerability paradox in the cross-national prevalence of posttraumatic stress disorder.Br. J Psychiatry. 2016;209(4):300–305. doi:10.1192/bjp.bp.115.176628
60. Sekoni O, Mall S, Christofides N. Prevalence and factors associated with PTSD among female urban slum dwellers in Ibadan, Nigeria: a cross-sectional study. BMC Public Health. 2021;21:1546. doi:10.1186/s12889-021-11508-y
61. MarinaWidmann A, HusseinWarsame J, Mikulica J, et al. Khat use, PTSD and psychotic symptoms among Somali refugees in Nairobi – a pilot study. Frontiers in Public Health. 2014. doi:10.3389/fpubh.2014.00071
62. Wolde A. The Relationship Between Khat Use Disorder and Post-Traumatic Stress Disorder Among Prisoners with Life Time Trauma Exposure in Ethiopia: a Cross-Sectional Study. Neuropsychiatr Dis Treat. 2021;17:3669–3681. doi:10.2147/NDT.S336877
63. Odenwald M, Hinkel H, Schauer E, et al. Use of khat and posttraumatic stress disorder as a risk factor for psychotic symptoms: a study of Somali combatants. Soc Sci Med. 2009;69(7):
64. Khantzian EJ. The self-medication hypothesis of substance use disorders: a reconsideration and recent applications. Harv Rev Psychiatry. 1997;4(5):231–244. doi:10.3109/10673229709030550
65. Khantzian EJ. The self-medication hypothesis of addictive disorders: focus on heroin and cocaine dependence. Am J Psychiatry. 1985;142(11):1259–1264. doi:10.1176/ajp.142.11.1259
66. Lembke A. Time to abandon the self-medication hypothesis in patients with psychiatric disorders. Am J Drug Alcohol Abuse. 2012;38(6):524–529. doi:10.3109/00952990.2012.694532
67. Leconte C, Mongeau R, Noble F. Traumatic Stress-Induced Vulnerability to Addiction: critical Role of the Dynorphin/Kappa Opioid System. Front Pharmacol. 2022;9. doi:10.3389/fphar.2022.856672
68. Eskander N, Vadukapuram R, Zahid S, et al. Post-traumatic Stress Disorder and Suicidal Behaviors in American Adolescents: analysis of 159,500 Psychiatric Hospitalizations. Cureus. 2020;12(5):e8017. doi:10.7759/cureus.8017
69. Ganz D, Sher L. Suicidal behavior in adolescents with post-traumatic stress disorder. Minerva Pediatr. 2010;62:363–370.
70. James W, Murrough YH, Jian HU, et al. Reduced Amygdala serotonin transporter binding in posttraumatic stress disorder. Bio Psychiatry. 2011;70(11):1033–1038. doi:10.1016/j.biopsych.2011.07.003
71. Davidson JR, Hughes DC, George LK, Blazer DG. The association of sexual assault and attempted suicide within the community. Arch Gen Psychiatry. 1996;53:550–555. doi:10.1001/archpsyc.1996.01830060096013
72. Cottler LB, Compton WM, Mager D, Spitznagel EL, Janca A. Posttraumatic stress disorder among substance users from the general population. Am J Psychiatry. 1992;149(5):664–670. doi:10.1176/ajp.149.5.664
73. Nathan DL, Linda B. Cottler. The Epidemiology of Post-Traumatic Stress Disorder and Alcohol Use Disorder. Alcohol Research. 2018;39(2):113–120.
74. McCauley JL, Killeen T, Gros DL, Brady KT, Back SE. Posttraumatic Stress Disorder and Co-Occurring Substance Use Disorders: advances in Assessment and Treatment. Clin Psycho l. 2012;19(3). doi:10.1111/cpsp.12006
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
A Community-Based Exploratory Cross-Sectional Study of Elder Abuse Perpetration or Victimization Among Elders in Ethiopia, 2022
Wolde A, Wolancho W, Belay Y, Alemu A, Asefa A, Gebremedhin T
Clinical Interventions in Aging 2022, 17:957-969
Published Date: 15 June 2022