Back to Journals » Neuropsychiatric Disease and Treatment » Volume 22
Postsurgical Seizure Outcome for Epilepsy Patients According to Histopathological Diagnosis: A Single-Center Experience
Authors Chen R, Hong ST, Wu SY, Jiang XQ, Su XJ, Zhang YQ, Mei Z, Lin H, Lin H, Hu XQ, Lin YX, Wang F
Received 12 December 2025
Accepted for publication 10 February 2026
Published 24 February 2026 Volume 2026:22 585977
DOI https://doi.org/10.2147/NDT.S585977
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Taro Kishi
Rong Chen,1– 3,* Shu-Ting Hong,1,2,* Shi-Ying Wu,3 Xiao-Qi Jiang,3 Xue-Jiao Su,3 Ying-Qi Zhang,3 Zhen Mei,1,2 Han Lin,1,2 Heng Lin,1,2 Xue-Qun Hu,1,2 Yuan-Xiang Lin,1,2,4 Feng Wang1,2,4
1Department of Neurosurgery, Neurosurgery Research Institute, the First Affiliated Hospital, Fujian Medical University, Fuzhou, Fujian, People’s Republic of China; 2Department of Neurosurgery, National Regional Medical Center, Binhai Campus of the First Affiliated Hospital, Fujian Medical University, Fuzhou, Fujian, People’s Republic of China; 3School of Clinical Medicine, Fujian Medical University, Fuzhou, Fujian, People’s Republic of China; 4Fujian Provincial Institutes of Brain Disorders and Brain Sciences, First Affiliated Hospital, Fujian Medical University, Fuzhou, Fujian, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Feng Wang, Department of Neurosurgery, Neurosurgery Research Institute, The First Affiliated Hospital, Fujian Medical University, Fuzhou, Fujian, People’s Republic of China, Tel +8615005018772, Email [email protected] Yuan-Xiang Lin, Department of Neurosurgery, Neurosurgery Research Institute, The First Affiliated Hospital, Fujian Medical University, Fuzhou, Fujian, People’s Republic of China, +8613906918894, Email [email protected]
Purpose: This study aimed to further explore the association between histopathology of the epileptogenic zone and postsurgical seizure outcome in epilepsy patients, with a specific focus on dual or multiple pathologies.
Patients and Methods: In this single-center retrospective cohort study, 449 patients who underwent epilepsy surgery between 2017 and 2024 at The First Affiliated Hospital of Fujian Medical University were included. Clinical data were collected, including histopathological diagnoses and seizure outcome at ≥ 12 months postoperatively. We investigated the association of histopathology, epilepsy duration, the number of preoperative antiseizure medications (ASMs), and MRI findings with seizure outcome, using logistic regression analysis.
Results: Among 449 patients, the most common histopathological diagnoses were low-grade epilepsy associated neuroepithelial tumors (LEAT, 34.3%) and cerebral vascular malformations (24.5%). Of 382 patients with complete follow-up data, 76.4% achieved seizure freedom (Engel I), with a median follow-up of 47 months. Patients with LEAT had the highest seizure-free rate (88.4%), whereas worse seizure outcome was observed in patients with focal cortical dysplasia (FCD) and gliosis, with 59.2% and 58.8% remaining free from disabling seizure, respectively. Multivariate logistic regression analysis identified FCD (OR = 4.290), gliosis (OR = 4.359), and dual or multiple pathologies (OR = 3.558) as independent predictors of seizure recurrence. Longer epilepsy duration (OR = 1.005) and a greater number of preoperative ASMs (OR = 1.235) were associated with an unfavorable prognosis. Preoperative MRI results are not an independent predictor of postoperative seizure recurrence in epilepsy patients.
Conclusion: Histopathological diagnosis, shorter epilepsy duration, and fewer preoperative ASMs predicted favorable surgical outcome in epilepsy patients. In contrast, dual/multiple pathologies, FCD, and gliosis carried an increased risk of postoperative seizure recurrence. These results highlight the importance of early surgical intervention, detailed histopathological assessment, and precise localization of the epileptogenic zone to improve outcome.
Keywords: epilepsy, surgery, histopathology, focal cortical dysplasia, dual or multiple pathologies
Introduction
Epilepsy is a prevalent neurological disorder, affecting an estimated 10 million people in China.1 It is characterized by recurrent, abnormal electrical discharges in the cerebral cortex, clinically manifesting as seizures.2 These recurrent seizures not only impair patients’ physical and mental health but also impose a heavy financial burden on families and the healthcare system, consuming substantial societal resources.3,4
Focal epilepsy results from abnormal electrical discharges that originate in specific, localized regions of the brain.5 Although seizures can be controlled with medications in most patients, more than one-third of individuals with focal epilepsy continue to experience recurrent seizures. The epileptogenic zones in these patients may display complex pathological features, such as structural lesions (eg hippocampal sclerosis or malformations of cortical development) or functional network reorganization.6 Recent studies suggested that sustained overactivation of neuroinflammatory pathways, such as the HMGB1-TLR4 axis, can perpetuate network hyperexcitability, resulting in persistent seizures.7 Furthermore, the dysfunction of functional proteins like the Sigma-1 receptor may lead to the collapse of intracellular homeostasis, thereby diminishing neuronal responsiveness to treatment.8 Epilepsy surgery is the most effective treatment to control seizures in these patients, further improving cognitive function, behavior, and quality of life.9,10 In fact, approximately 65% of patients with focal epilepsy have been reported to achieve seizure freedom following surgery.10
Favorable surgical outcome is been linked to younger age at surgery, shorter epilepsy duration, and lower preoperative antiseizure-medication burden.9,11,12 Recent evidence shows that the histopathology of the epileptogenic zone is closely associated with prognosis. However, studies on histopathology report wide variations in the rates of seizure freedom after surgery. In analyses focusing on focal cortical dysplasia (FCD), the proportions of patients with FCD achieving seizure freedom range from 8.3% to 86.4%.13,14 Other research suggests that patients with FCD often fare worse than those with other pathologies.10,15,16 While some MRI-diagnosed FCD cohorts report favorable outcome in up to ~70% of cases.17
Although the prognostic importance of histopathology in the epileptogenic zone is increasingly recognized, most prior studies have been constrained by small cohort sizes, limiting detailed histopathological subtyping. Moreover, most investigations have focused on only one pathology, rather than examining multiple coexisting histopathologies. In particular, the impact of dual or multiple pathologies on surgical outcome remains poorly explored.
Based on this, we assembled a large cohort of patients to ensure sufficient representation across all histopathological categories. We systematically analyzed their preoperative, surgical, and postoperative data to further explore the relationship between histopathology and postsurgical outcome.
Materials and Methods
Patient Selection
This study screened 974 epilepsy patients treated at the Department of Neurosurgery, First Affiliated Hospital of Fujian Medical University from 2017 to 2024. First, 243 patients lacking postoperative histopathological diagnoses were excluded. Then, 11 patients without presurgical MRI results were excluded. Additionally, 271 patients with specific histopathology diagnoses (such as malignant lymphoma, metastatic carcinoma, meningioma, high-grade neuroepithelial tumors, and melanoma) were removed. Ultimately, 449 patients met our inclusion criteria and were enrolled in the study (Figure 1).
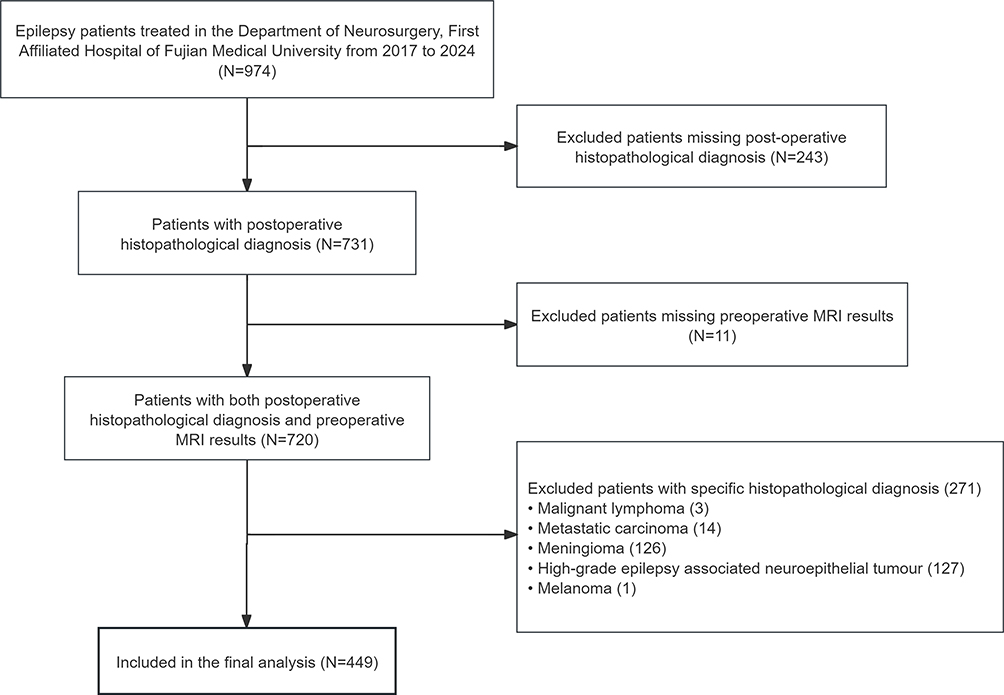 |
Figure 1 Selection of study participants. |
Data Collection
We systematically collected patient demographics (sex, age at seizure onset, age at surgery), clinical characteristics (epilepsy duration, number of preoperative ASMs), imaging and monitoring data (presurgical MRI, use of stereoelectroencephalography [sEEG]), surgical parameters (type and anatomical site of surgery, use and result of intraoperative electrocorticography [ECoG]), histopathological diagnosis, and seizure outcome (Engel classification). Surgical interventions were classified into two types: resective surgery and minimally invasive laser interstitial thermal therapy (LITT). We categorized MRI findings into four distinct groups: MRI+/pathology+: structural abnormality evident on both MRI and histopathology; MRI-/pathology+: no lesion on MRI, but structural abnormality confirmed by histopathology; MRI-/pathology-: no structural abnormality on either MRI or histopathology; MRI+/pathology-: lesion visible on MRI without a matching histopathological abnormality.
Histopathological Assessment
Postoperative histopathological diagnoses were classified into 10 categories: low-grade epilepsy-associated neuroepithelial tumor (LEAT), cerebral vascular malformations (including cavernous malformation, arteriovenous malformation, and venous malformation), malformations of cortical development, subdivided into focal cortical dysplasia (FCD) and other non-FCD cortical malformations (MCD-nFCD); nonspecific lesion (including gliosis and “no lesion”), hippocampal sclerosis (HS), dual or multiple pathologies (ie more than one coexisting pathology), and other rarer entities (such as extranodal sinusoidal histiocytosis, schwannoma, epidermoid cyst, pituitary adenoma, etc.). “no lesion” refer to the absence of discernible structural abnormalities on histopathologic examination.
Statistical Analysis
Baseline characteristics for patients achieving Engel I versus Engel II–IV at ≥12 months after surgery were compared using χ2 tests for categorical variables and the Mann–Whitney U-test for continuous variables. Categorical data are reported as proportions, and continuous variables as medians. The interactions and multicollinearity among relevant variables were examined. Univariate and multivariate logistic regression analyses were performed to estimate odds ratios (ORs) for seizure freedom (Engel I) versus recurrent seizures, stratified by histopathological diagnoses to evaluate how different subtypes influence prognosis. In addition, univariate and multivariate logistic regression models assessed other potential predictors of seizure outcome, including age at seizure onset, age at surgery, epilepsy duration, and the number of preoperative ASMs and MRI results. Apply propensity score matching to balance data imbalance in MRI results. Statistical analyses were conducted using IBM SPSS 24 and R version 4.4.2 through RStudio 2026.01.0, and p < 0.05 was considered statistically significant.
Results
Patient Characteristics
Of the 449 patients, 158 (35.2%) had epilepsy onset before 18 years of age, and 98 (21.8%) were under 18 at the age of surgery. Age at seizure onset ranged from less than 1 year to 75 years, while age at surgery spanned from 1 to 75 years. One hundred and seventy (37.9%) were female. The median epilepsy duration was 6 months (interquartile range [IQR]: 0.0007–480 months), with 155 (34.5%) patients having a duration of one year or less and 294 (65.5%) exceeding one year. The number of preoperative ASMs ranged from 0 to 14. The median follow-up duration was 47 months (IQR: 12–90 months). Demographic characteristics of the study patients were shown in Table 1.
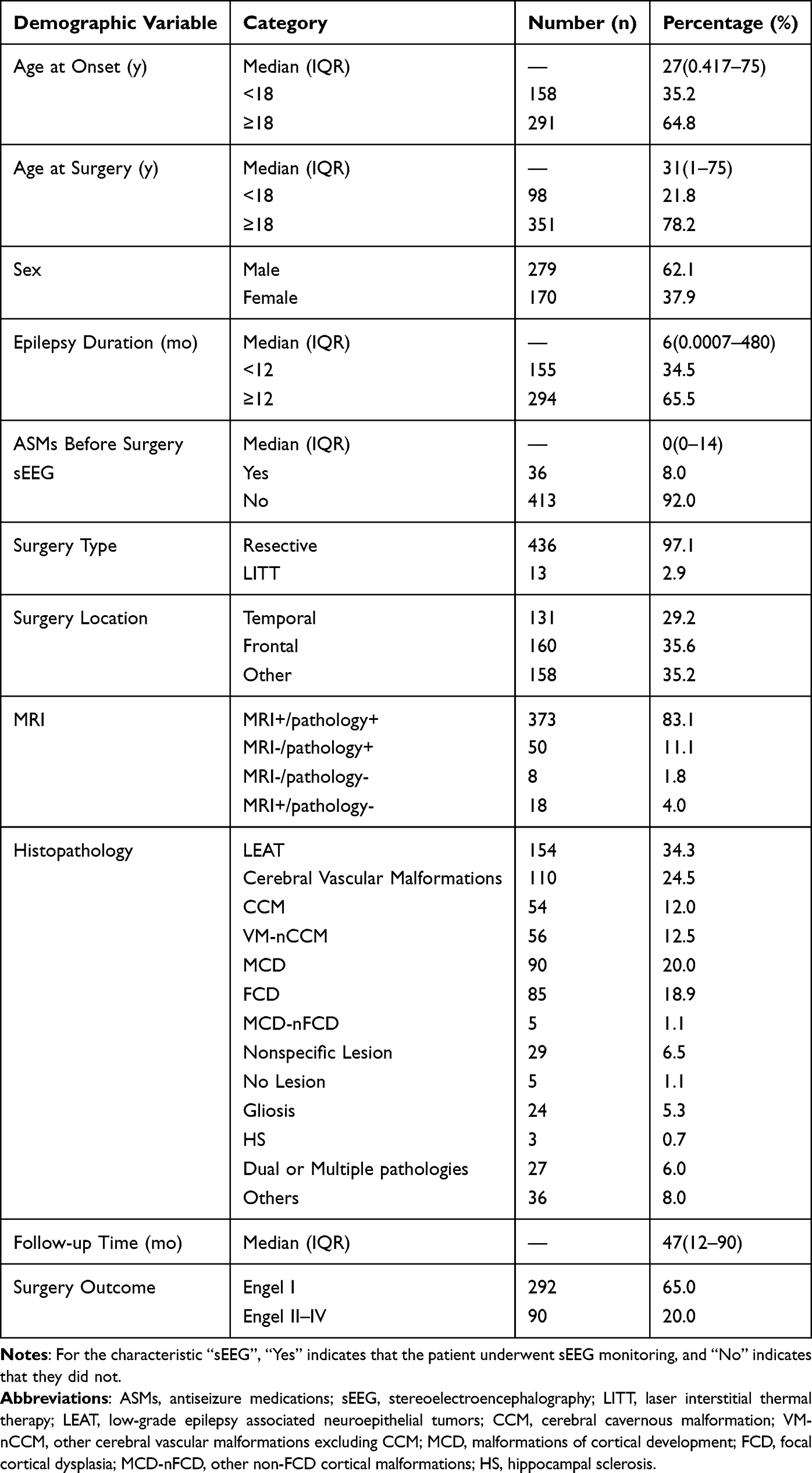 |
Table 1 Demographic Characteristics of the Study Population (n = 449) |
Surgical Results and Risk Factors
Of the 449 patients included, complete postoperative outcome data were available for 397 (88.4%). Among them, 15 patients had died, leaving 382 for further analysis. Their basic characteristics were shown in Table 2. Among these 382 patients, 292 (76.4%) achieved Engel I, while 90 (23.6%) fell into Engel II–IV categories. There were no significant differences between these two groups with respect to age at seizure onset, age at surgery, or surgical type. However, patients with recurrent seizures (Engel II–IV) had a significantly longer duration of epilepsy (median 36 months vs 3 months, p < 0.001) and were prescribed a greater number of preoperative ASMs (median 1 [range 0–14] vs.0 [range 0–7], p < 0.001) compared to seizure-free patients. Additionally, a higher proportion of recurrence cases had undergone sEEG monitoring (14.4% vs 6.5%, p = 0.027).
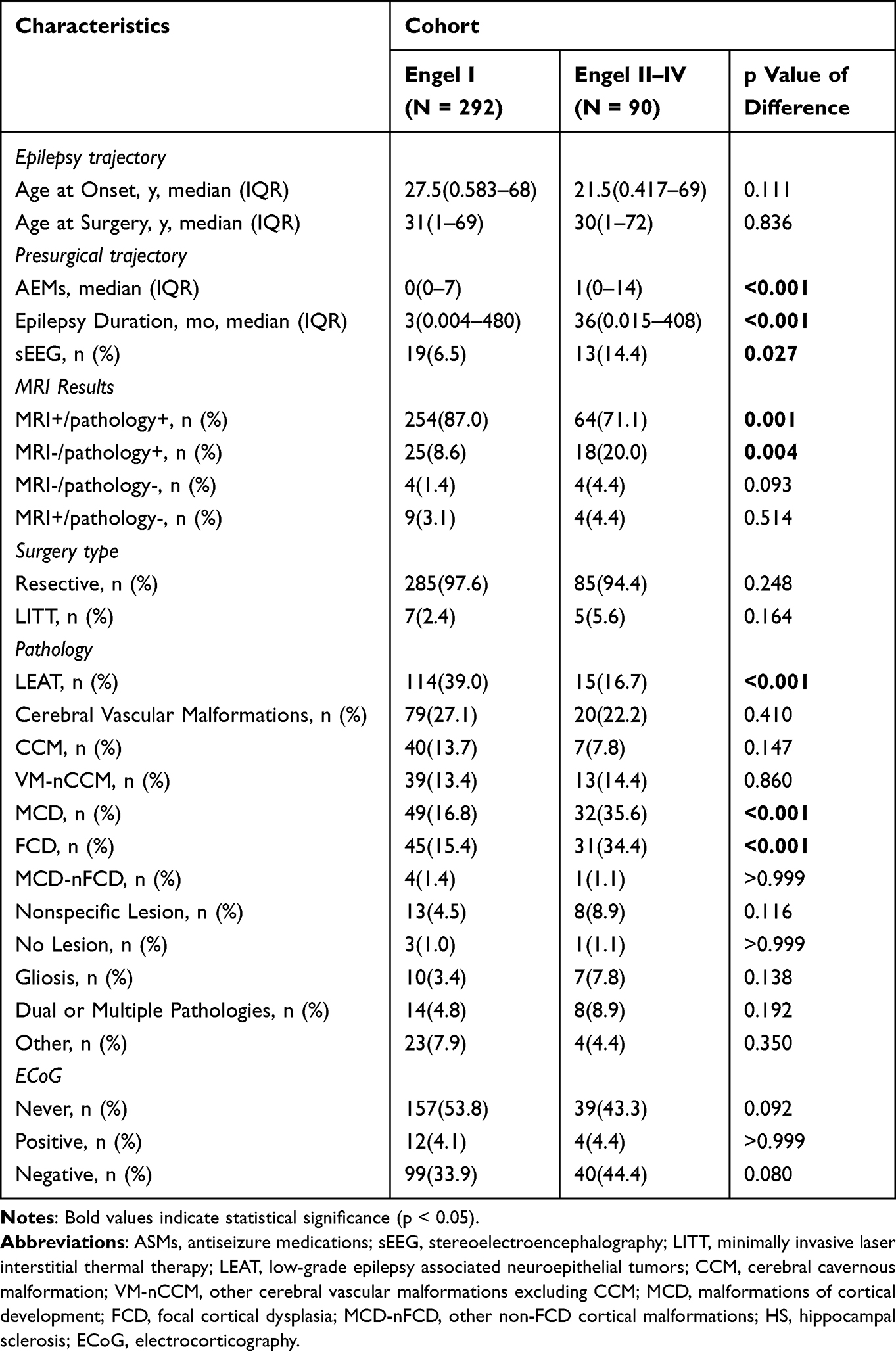 |
Table 2 Baseline Characteristics of Patients with Complete Data (N = 382) |
Analysis of presurgical MRI findings revealed that the largest subgroup was MRI+/pathology+ (83.1%, n = 373). While the MRI-/pathology- group was the smallest (only 8 cases, 1.8%). MRI-/pathology+ was observed in 50 cases (11.1%) and MRI+/pathology- in 18 cases (4.0%). Notably, all patients with LEAT showed MRI+/pathology+. Among the MRI-/pathology+ group, FCD accounted for the largest proportion (72.0%, n = 36). Fisher’s exact test identified a significant difference in prognosis between the MRI+/pathology+ group and the MRI-/pathology+ group (p = 0.003). There were more patients with recurrent seizures among the MRI-/pathology+ group (20.0% vs 8.6%, p = 0.004), while Engel II–IV outcome was less common in the MRI+/pathology+ group (71.1% vs 87.0%, p = 0.001).
Given the potential complex relationship between MRI findings, preoperative ASMs, and epilepsy duration, we specifically explored interactions as well as multicollinearity among these three variables and a Mann–Whitney U-test between duration, ASMs, and MRI findings. The result shows that the interaction between MRI and ASMs (p = 0.842), the interaction between MRI and duration (p = 0.901), and the interaction between ASMs and epilepsy duration (p = 0.381) were all insignificant. In addition, the multicollinearity analysis shows that the VIF values of the three types of independent variables are all well below the critical value of 10 (MRI: 1.175, ASMs: 1.400, duration: 1.383), and the tolerances are all well above 0.1 (MRI: 0.851, ASMs: 0.714, duration: 0.723). There is no serious multicollinearity problem among these independent variables. However, the Mann–Whitney U-test revealed that MRI-negative patients generally had longer epilepsy duration (p < 0.001) and greater use of ASMs (p < 0.001), indicating substantial baseline confounding. To control for this imbalance and explore the independent effects of factors, we performed logistic regression analysis. Due to sample size imbalance in the MRI groups, we merged the two subgroups with negative postoperative histopathology (MRI-/pathology- group and MRI+/pathology- group).
Univariate logistic regression analysis was performed to assess the association between surgical outcome and the following variables: age at seizure onset, age at surgery, epilepsy duration, number of preoperative ASMs, intraoperative ECoG results, and MRI results. The analysis revealed that recurrent seizures after surgery were significantly associated with longer duration of epilepsy (OR = 1.006, 95% CI 1.004–1.009), a higher number of preoperative ASMs (OR = 1.357, 95% CI 1.172–1.572), and the result of MRI-/pathology+ (OR = 2.857, 95% CI 1.470–5.556). In multivariate logistic regression, both longer epilepsy duration (adjusted OR = 1.005, 95% CI 1.001–1.010) and a greater number of preoperative ASMs (adjusted OR = 1.235, 95% CI 1.026–1.487) remained independently associated with increased odds of seizure recurrence. MRI findings showed no independent predictive value (p = 0.724). The multicollinearity diagnosis shows that the variance inflation factors of all independent variables are well below 10 (all VIFs ≤ 3.461, all tolerances ≥ 0.289), indicating that there is no serious multicollinearity in the model and that the estimation results are reliable. Results of univariate and multivariate analyses were shown in Table 3.
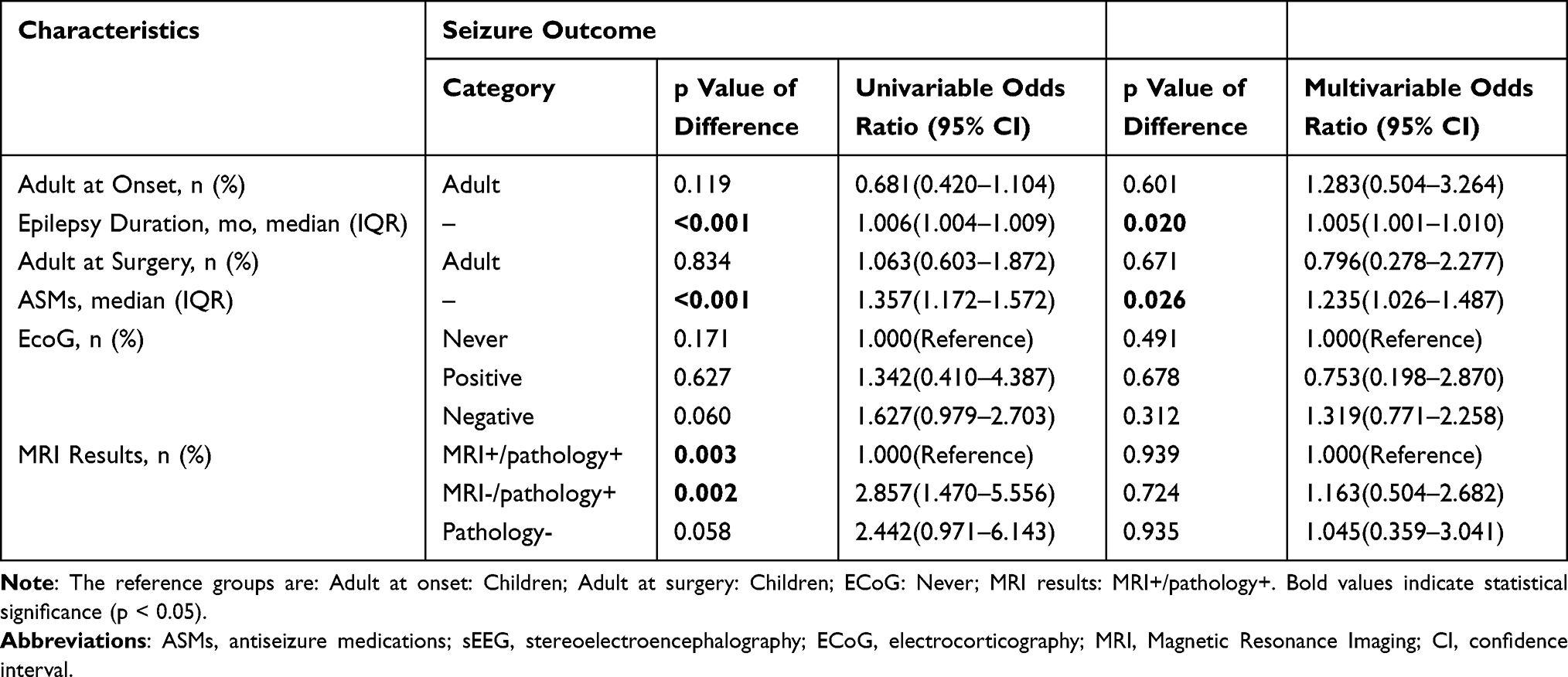 |
Table 3 Uni- and Multivariate Regression Analysis About Basic Characteristics in Patients with Favorable vs Unfavorable Outcome (N = 382) |
To solve the imbalance between the groups of MRI+/pathology+ and MRI-/pathology+, we conducted a 1:1 nearest neighbor matching method based on propensity scores. Using MRI grouping (MRI+/pathology+ vs MRI-/pathology+) as the treatment variable and key baseline covariates, including age at seizure onset, age at surgery, epilepsy duration, number of preoperative ASMs, and intraoperative ECoG results, we successfully constructed a baseline-balanced cohort (all test SMD > 0.1). The results show that the prognostic difference between MRI+/pathology+ and MRI-/pathology+ groups was no longer statistically significant (p = 0.262).
Surgery Characteristics
Most of the 449 patients (97.1%, n = 436) underwent resective surgery, including 24 patients who had prior sEEG monitoring. The remaining 13 patients were treated with MRI-guided LITT. Among the 292 patients with Engel I outcome, the proportion of resection was 97.6% (n = 285), and only 7 (2.4%) underwent LITT. In contrast, of the 90 patients with Engel II–IV outcome, resective surgery was performed in 85 cases (94.4%) and LITT in 5 cases (5.6%).
Postoperative Histopathological Diagnosis
The distribution of histopathological diagnoses among the 449 patients was as follows: LEAT 34.3% (n = 154); cerebral vascular malformations 24.5% (n = 110), including cerebral cavernous malformation (12.0%, n = 54) and other cerebral vascular malformations (12.5%, n = 56); malformations of cortical development 20.0% (n = 90), including FCD (18.9%, n = 85) and MCD-nFCD (1.1%, n = 5); nonspecific lesion 6.5% (n = 29), consisting of gliosis (5.3%, n = 24) and “no lesion” (1.1%, n = 5); HS 0.7% (n = 3); dual or multiple pathologies (6.0%, n = 27); and others rare entities 8.0% (n = 36). The two largest categories of histopathological diagnosis were LEAT and cerebral vascular malformations. LEAT had the highest rate of favorable outcome (Engel I, 88.4%). In contrast, FCD and gliosis were associated with substantially lower seizure-free rates. (59.2% and 58.8%, respectively). Notably, Engel II–IV patients had a significantly lower proportion of LEAT compared to patients with Engel I (16.7% vs 39.0%, p < 0.001) and a higher rate of malformations of cortical development (35.6% vs 16.8%, p < 0.001), particularly FCD (34.4% vs 15.4%, p < 0.001).
Univariate logistic regression analysis was conducted for the six main histopathological categories: LEAT, MCD, cerebral vascular malformations, nonspecific lesion, dual or multiple pathologies, and others. The analysis showed that LEAT showed a significant association with a reduced risk of postoperative seizure recurrence compared to the other five categories (OR = 0.312, 95% CI 0.171–0.570), whereas MCD was closely related to seizure recurrence (OR = 2.736, 95% CI 1.611–4.647). No statistically significant relationships were found for cerebral vascular malformations (p = 0.361, OR = 0.770, 95% CI 0.440–1.349), nonspecific lesion (p = 0.113, OR = 2.094, 95% CI 0.839–5.225), dual or multiple pathologies (p = 0.151, OR = 1.937, 95% CI 0.785–4.779), or others (p = 0.273, OR = 0.544, 95% CI 0.183–1.617). In multivariate logistic regression, MCD remained an independent predictor of seizure recurrence (adjusted OR = 4.136, 95% CI 2.122–8.063). Furthermore, nonspecific lesion (adjusted OR = 3.897, 95% CI 1.418–10.715) and dual or multiple pathologies (adjusted OR = 3.619, 95% CI 1.330–9.846) emerged as significant risk factors for recurrence. No independent associations were observed for cerebral vascular malformations (p = 0.185, OR = 1.603, 95% CI 0.797–3.224) or others (p = 0.872, OR = 1.101, 95% CI 0.341–3.557). Results of univariate and multivariate analyses were shown in Table 4. These findings indicate that MCD, nonspecific lesion, and dual or multiple pathologies are independent predictors for unfavorable postsurgical outcome.
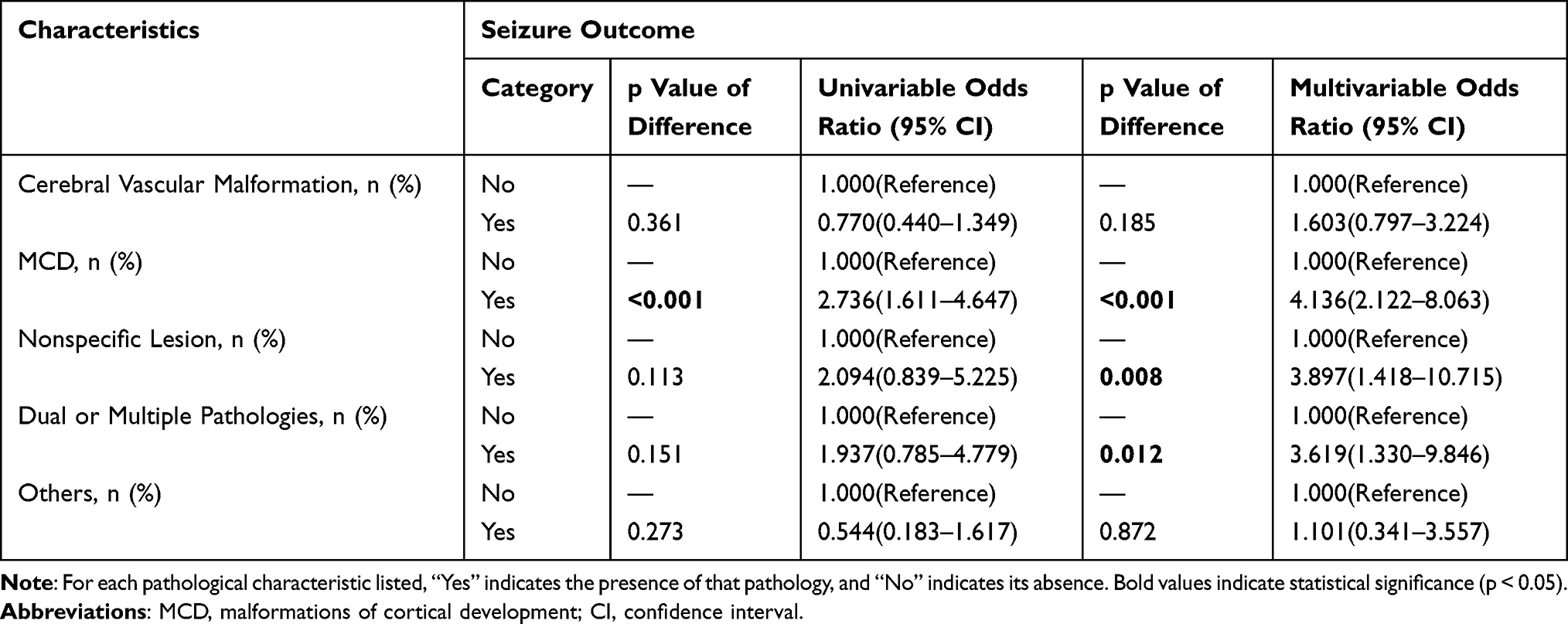 |
Table 4 Uni- and Multivariate Regression Analysis About Histopathologic Results of Patients with Favorable vs Unfavorable Outcome (N = 382) |
Univariate logistic regression was performed for six histopathological subtypes: cerebral cavernous malformation (CCM), other cerebral vascular malformations excluding CCM (VM-nCCM), FCD, MCD-nFCD, gliosis, and “no lesion”. The analysis indicated that FCD was associated with a significantly increased risk of postoperative seizure recurrence (OR = 2.884, 95% CI 1.683–4.941). By contrast, MCD-nFCD showed no significant association with recurrence (p = 0.850, OR = 0.809, 95% CI 0.089–7.332). This indicates that the association between MCD and poorer surgical outcome is primarily observed in its FCD subtype. No statistically significant associations were observed for CCM (p = 0.140, OR = 0.531, 95% CI 0.229–1.231), VM-nCCM (p = 0.792, OR = 1.095, 95% CI 0.556–2.157), gliosis (p = 0.088, OR = 2.378, 95% CI 0.878–6.442), or “no lesion” (p = 0.946, OR = 1.082, 95% CI 0.111–10.536). A multivariate logistic regression model was then constructed, including these six subtypes, plus the category of dual or multiple pathologies. In this model, FCD (OR = 4.290, 95% CI 2.258–8.151), gliosis (OR = 4.359, 95% CI 1.502–12.653), and dual or multiple pathologies (OR = 3.558, 95% CI 1.338–9.466) emerged as independent predictors of postoperative seizure recurrence. No significant association were found for CCM (p = 0.855, OR = 1.090, 95% CI 0.434–2.736), VM-nCCM (p = 0.064, OR = 2.076, 95% CI 0.959–4.494), MCD-nFCD (p = 0.698, OR = 1.557, 95% CI 0.166–14.581), and “no lesion” (p = 0.535, OR = 2.076, 95% CI 0.207–20.860). Results of univariate and multivariate analyses were shown in Table 5. These findings further indicate that FCD, gliosis, and dual or multiple pathologies are important determinants for unfavorable postsurgical outcome.
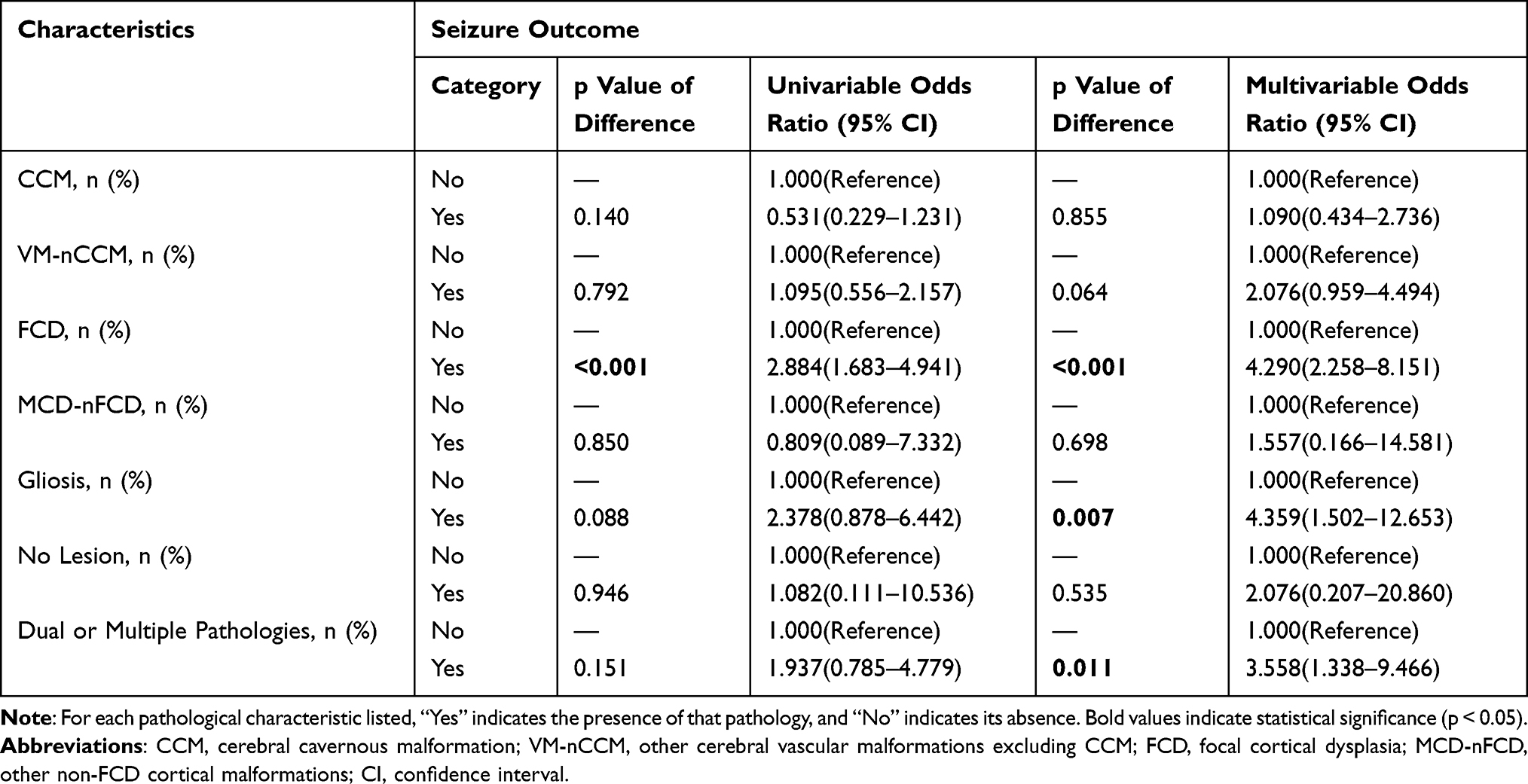 |
Table 5 Uni- and Multivariate Regression Analysis About Detailed Histopathologic Results in Patients with Favorable vs Unfavorable Outcome (N = 382) |
Discussion
This study demonstrated that seizure outcome of focal epilepsy patients is highly associated with specific histopathological subtypes, with histopathological diagnosis serving as an important and independent predictor of surgical success. LEAT was related to a markedly higher probability of achieving seizure freedom. In contrast, MCD (especially FCD), nonspecial lesion, dual or multiple pathologies, and gliosis were independently associated with an increased risk of recurrent seizures.
In this study, 59.2% patients with FCD achieved Engel I, which aligns closely with a meta-analysis of 37 studies reporting an average seizure-freedom rate of 55.8% ± 16.2% in FCD cohorts.18 FCD location is known to influence lesion size, age at epilepsy onset, and surgical outcome.19 Presurgical Evaluation, such as MRI, may fail to localize the FCD in some patients, contributing to unfavorable surgical outcome. Recent research using graph neural networks has shown promise for detecting FCD in MRI-negative epilepsy patients, potentially leading to better outcome.20
Focal seizure affects both local epileptogenic networks and distributed structural-functional network reorganization, characterized chiefly by reduced connectivity between the lesion and the rest of the brain.21–23 Surgical disconnection may promote compensatory increase in postoperative network integration; However, persistently low integration can allow residual pathological network to reactivate (eg under stress or fatigue), leading to seizure recurrence.6 The functional MRI studies in MCD patients demonstrate altered functional network at the lesion, perilesional areas, and distant neocortex,21,24 suggesting that impaired structural-functional connectivity may contribute to unfavorable surgical outcome in temporal MCD and FCD patients. New study demonstrates that clemastine, a non-selective σ1 receptor agonist, exhibits significant neuroprotective effects against PTZ-kindled seizures and cognitive deficits. Its anti-seizure and pro-cognitive actions are mediated by acting on σ1 receptors, highlighting the crucial role of σ1 receptors in improving seizures and protecting cognitive function.8 This discovery offers hope for treating epilepsy in patients with poor surgical prognosis.
Patients with gliosis had a lower chance of achieving seizure freedom. Studies reported that a well-defined aura and the disappearance of epileptiform discharges on intraoperative ECoG were predictive of favorable postoperative seizure outcome.25 Conversely, absence of auras may indicate rapid propagation of epileptiform discharges to remote brain regions, hindering precise localization of the epileptogenic zone. Persistent frequent spikes on post-resection ECoG may suggest incomplete resection of the epileptogenic zone. Taken together, these factors may contribute to recurrent seizures after surgery.
This study specifically focused on dual or multiple pathologies, which were characterized by the concurrent presence of two or more lesions. In such cases, it is often unclear whether seizure originates from a single lesion or from multiple independent lesions. sEEG may help to identify the epileptogenic focus; However, if sEEG captures only a limited number of seizures, localization remains highly uncertain.26 In patients with dual or multiple pathologies, separate lesions and adjacent tissue changes may reflect the sequential evolution of a single pathological process and thereby contribute to an expanded epileptogenic zone.27 In addition, a recent study suggested that HMGB1 activates the TLR4/NF-κB signaling pathway and stimulates RAGE, causing hyperexcitability and acute or chronic epilepsies. This is mediated by glial cell activation and the release of proinflammatory cytokines, establishing a self-sustaining cycle of neuroinflammation.7 This may explain the pathological progression and expansion of the epileptogenic zone. These complexities can preclude complete resection of the epileptogenic focus and consequently contribute to unfavorable surgical outcome.28 When technically and clinically feasible, simultaneous resection of all identifiable lesions is generally recommended for patients with dual or multiple pathologies.29,30
This study found that preoperative MRI results are not an independent predictor of postoperative seizure recurrence in epilepsy patients with positive histopathology. MRI-negative and pathology-positive status is a marker of more severe epilepsy, characterized by longer duration and greater use of ASMs. Clinical prognosis assessment should prioritize these severity indicators over MRI findings alone. A study examining the prognosis of MRI-negative pediatric epilepsy patients demonstrated favorable postoperative outcome with the employment of video electroencephalography, magnetic resonance spectroscopy, and magnetoencephalography to localize the epileptogenic focus.31 In another study, MR-negative and positive FCD patients had a comparable surgical prognosis, emphasizing the importance of comprehensive presurgical evaluations.32 These suggest that with precise localization of the epileptogenic focus, MRI-negative/pathology-positive patients may achieve comparable favorable surgical outcome to MRI-positive patients.
Furthermore, the lack of significant prognostic differences between the MRI-/pathology- and MRI+/pathology- groups may be attributable to their relatively small sample sizes. This limitation may undermine the comprehensiveness of our analysis linking MRI-negative findings to prognosis, explaining discrepancies with prior studies. A recent study suggested that patients with an electroclinically identified focus achieve better surgical outcome compared to those patients with negative MRI findings and negative pathology results.33 Future prospective studies with larger cohorts are needed, with particular consideration of pathology-negative patients’ prognoses.
Limitation
Several limitations of our study should be acknowledged. First, patients with isolated hippocampal sclerosis were too few for regression analysis, and FCD was not analyzed by subtype, which may have prognostic relevance. The prognosis of FCD patients needs more detailed discussion. Furthermore, due to the retrospective design, although we adjusted for key surgical and demographic confounders, other unmeasured factors that may affect surgical results, such as detailed nutritional status and socioeconomic determinants of health, were not available for analysis.34 These factors should be further explored. Additionally, the retrospective design led to a notable imbalance in sample size between MRI groups. Despite applying multivariable logistic regression and propensity score matching, unmeasured confounding may persist.
Conclusion
This single-center retrospective cohort study explored the relationship between histopathology and surgical outcome in epilepsy patients. Specific histopathological categories, including FCD, gliosis, and dual or multiple pathologies, were significantly associated with seizure recurrence after surgery, while LEAT was linked to a lower risk of recurrence. Shorter duration of epilepsy and a lower number of presurgical ASMs were identified as independent predictors of favorable surgical outcome. However, the relationship between MRI findings and prognosis was not significant, suggesting that patients with negative MRI but positive pathology may achieve a favorable prognosis as MRI-positive patients.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request. Requests should be directed to Feng Wang at [email protected]. The corresponding author will coordinate with the first author Rong Chen, who is the steward of the primary data, to evaluate and fulfill reasonable requests.
Ethical Approval
This retrospective study was reviewed and approved by the Ethics Committee of The First Affiliated Hospital of Fujian Medical University (Approval No. [2024]514). The requirement for written informed consent was waived by the Ethics Committee due to the retrospective nature of the study and the use of anonymized patient data. All patient data were handled with strict confidentiality. The study was conducted in compliance with the Declaration of Helsinki.
Consent for Publication
The details of any images, videos, recordings, etc can be published, and that the people providing consent have been shown the article contents to be published. All data reported in this manuscript are anonymized.
Acknowledgment
Rong Chen and Shu-Ting Hong are co-first authors for this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by Young and Middle-aged Key Personnel Training Project of Fujian Provincial Health Commission [grant number 2024GGA024]; Joint Funds for the Innovation of Science and Technology, Fujian Province [grant number 2024Y9168]; Fujian Medical University Student Innovation and Entrepreneurship Training Project [grant number C2024219].
Disclosure
The authors report no conflicts of interest in this work.
References
1. Ding D, Zhou D, Sander JW, Wang W, Li S, Hong Z. Epilepsy in China: major progress in the past two decades. Lancet Neurol. 2021;20(4):316–12. doi:10.1016/s1474-4422(21)00023-5
2. Gao P, Chen H, Sun Y, et al. ALG13-related epilepsy: current insights and future research directions. Neurochem Res. 2024;50(1). doi:10.1007/s11064-024-04300-y
3. Jędrzejczak J, Majkowska-Zwolińska B, Chudzicka-Bator A, Żerda I, Władysiuk M, Godman B. Economic and social cost of epilepsy in Poland: 5-year analysis. Eur J Health Econ. 2021;22(3):485–497. doi:10.1007/s10198-021-01269-1
4. Begley C, Wagner RG, Abraham A, et al. The global cost of epilepsy: a systematic review and extrapolation. Epilepsia. 2022;63(4):892–903. doi:10.1111/epi.17165
5. Aronica E, Mühlebner A. Neuropathology of epilepsy. In: Handbook of Clinical Neurology. Elsevier; 2018:193–216.
6. Larivière S, Park BY, Royer J, et al. Connectome reorganization associated with temporal lobe pathology and its surgical resection. Brain. 2024;147(7):2483–2495. doi:10.1093/brain/awae141
7. Shokr MM, Eladawy RM. HMGB1: different secretion pathways with pivotal role in epilepsy and major depressive disorder. Neuroscience. 2025;570:55–67. doi:10.1016/j.neuroscience.2025.02.023
8. Badawi GA, Shokr MM, Elshazly SM, Zaki HF, Mohamed AF. Sigma-1 receptor modulation by clemastine highlights its repurposing as neuroprotective agent against seizures and cognitive deficits in PTZ-kindled rats. Eur J Pharmacol. 2024;980:176851. doi:10.1016/j.ejphar.2024.176851
9. Ryvlin P, Cross JH, Rheims S. Epilepsy surgery in children and adults. Lancet Neurol. 2014;13(11):1114–1126. doi:10.1016/s1474-4422(14)70156-5
10. West S, Nolan SJ, Cotton J, et al. Surgery for epilepsy. Cochrane Database Syst Rev. 2015. doi:10.1002/14651858.CD010541.pub2
11. Perucca P, Scheffer IE, Kiley M. The management of epilepsy in children and adults. Med j Aust. 2018;208(5):226–233. doi:10.5694/mja17.00951
12. Yu H, Sun Y, Liu C, et al. Clinical characteristics and post-operative outcomes in children with malformation of cortical development related drug-resistant epilepsy: 428 cases in one pediatric epilepsy center. CNS Neurosci Ther. 2024;30(9):e70031. doi:10.1111/cns.70031
13. Palmini A, Andermann F, Olivier A, Tampieri D, Robitaille Y. Focal neuronal migration disorders and intractable partial epilepsy: results of surgical treatment. Ann Neurol. 1991;30(6):750–757. doi:10.1002/ana.410300603
14. Urbach H, Scheffler B, Heinrichsmeier T, et al. Focal cortical dysplasia of Taylor’s balloon cell type: a clinicopathological entity with characteristic neuroimaging and histopathological features, and favorable postsurgical outcome. Epilepsia. 2002;43(1):33–40. doi:10.1046/j.1528-1157.2002.38201.x
15. Blumcke I, Spreafico R, Haaker G, et al. Histopathological findings in brain tissue obtained during epilepsy surgery. N Engl J Med. 2017;377(17):1648–1656. doi:10.1056/NEJMoa1703784
16. Lamberink HJ, Otte WM, Blümcke I, et al. Seizure outcome and use of antiepileptic drugs after epilepsy surgery according to histopathological diagnosis: a retrospective multicentre cohort study. Lancet Neurol. 2020;19(9):748–757. doi:10.1016/s1474-4422(20)30220-9
17. Willard A, Antonic-Baker A, Chen Z, O’Brien TJ, Kwan P, Perucca P. Seizure outcome after surgery for MRI-diagnosed focal cortical dysplasia: a systematic review and meta-analysis. Neurology. 2022;98(3):e236–e248. doi:10.1212/wnl.0000000000013066
18. Rowland NC, Englot DJ, Cage TA, Sughrue ME, Barbaro NM, Chang EF. A meta-analysis of predictors of seizure freedom in the surgical management of focal cortical dysplasia. J Neurosurg. 2012;116(5):1035–1041. doi:10.3171/2012.1.Jns111105
19. Wagstyl K, Whitaker K, Raznahan A, et al. Atlas of lesion locations and postsurgical seizure freedom in focal cortical dysplasia: a MELD study. Epilepsia. 2022;63(1):61–74. doi:10.1111/epi.17130
20. Ripart M, Spitzer H, Williams LZJ, et al. Detection of Epileptogenic Focal Cortical Dysplasia Using Graph Neural Networks. JAMA neurol. 2025;82(4):397. doi:10.1001/jamaneurol.2024.5406
21. Diehl B, Tkach J, Piao Z, et al. Diffusion tensor imaging in patients with focal epilepsy due to cortical dysplasia in the temporo-occipital region: electro-clinico-pathological correlations. Epilepsy Res. 2010;90(3):178–187. doi:10.1016/j.eplepsyres.2010.03.006
22. Luo C, Qiu C, Guo Z, et al. Disrupted functional brain connectivity in partial epilepsy: a resting-state fMRI study. PLoS One. 2011;7(1):e28196. doi:10.1371/journal.pone.0028196
23. Pittau F, Grova C, Moeller F, Dubeau F, Gotman J. Patterns of altered functional connectivity in mesial temporal lobe epilepsy. Epilepsia. 2012;53(6):1013–1023. doi:10.1111/j.1528-1167.2012.03464.x
24. Hong SJ, Kim H, Schrader D, Bernasconi N, Bernhardt BC, Bernasconi A. Automated detection of cortical dysplasia type II in MRI-negative epilepsy. Neurology. 2014;83(1):48–55. doi:10.1212/wnl.0000000000000543
25. Dash GK, Rathore C, Jeyaraj MK, Wattamwar P, Sarma SP, Radhakrishnan K. Predictors of seizure outcome following resective surgery for drug-resistant epilepsy associated with focal gliosis. J Neurosurg. 2019;130(6):2071–2079. doi:10.3171/2018.3.Jns172949
26. Cook MJ, O’Brien TJ, Berkovic SF, et al. Prediction of seizure likelihood with a long-term, implanted seizure advisory system in patients with drug-resistant epilepsy: a first-in-man study. Lancet Neurol. 2013;12(6):563–571. doi:10.1016/s1474-4422(13)70075-9
27. Palmini A, Paglioli E, Silva VD. Developmental tumors and adjacent cortical dysplasia: single or dual pathology? Epilepsia. 2013;54(Suppl 9):18–24. doi:10.1111/epi.12438
28. Blume WT. Principles of clinical investigation of surgical patients. Int Anesthesiol Clin. 1986;24(3):47–73. doi:10.1097/00004311-198602430-00008
29. Li LM, Cendes F, Watson C, et al. Surgical treatment of patients with single and dual pathology: relevance of lesion and of hippocampal atrophy to seizure outcome. Neurology. 1997;48(2):437–444. doi:10.1212/wnl.48.2.437
30. Li LM, Cendes F, Andermann F, et al. Surgical outcome in patients with epilepsy and dual pathology. Brain. 1999;122(Pt 5):799–805. doi:10.1093/brain/122.5.799
31. Saito Y, Sugai K, Iwasaki M, et al. Surgical outcome and contributing presurgical evaluations in children with magnetic resonance imaging-negative epilepsy and periodic seizure cycles. Epilepsy Res. 2025;209:107492. doi:10.1016/j.eplepsyres.2024.107492
32. Seong MJ, Choi SJ, Joo EY, et al. Surgical outcome and prognostic factors in epilepsy patients with MR-negative focal cortical dysplasia. PLoS One. 2021;16(4):e0249929. doi:10.1371/journal.pone.0249929
33. Sanders MW, Van der Wolf I, Jansen FE, et al. Outcome of epilepsy surgery in MRI-negative patients without histopathologic abnormalities in the resected tissue. Neurology. 2024;102(4). doi:10.1212/wnl.0000000000208007
34. Shokr MM, Eladawy RM, Azar YO, Al Raish SM. Probiotics and the Gut–brain axis: emerging therapeutic strategies for epilepsy and depression comorbidity. Foods. 2025;14(17):2926. doi:10.3390/foods14172926
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
18F-FDG-PET/CT for Localizing the Epileptogenic Focus in Patients with Different Types of Focal Cortical Dysplasia
Wang F, Hong ST, Zhang Y, Xing Z, Lin YX
Neuropsychiatric Disease and Treatment 2024, 20:211-220
Published Date: 3 February 2024
Giant Granular Cell Tumor of the Left Thigh, a Rare Case Report and Literature Review
Liu Q, Kong X, Yang J, Zhang D
Orthopedic Research and Reviews 2025, 17:1-7
Published Date: 7 January 2025