Back to Journals » Journal of Pain Research » Volume 19
Postoperative Pain After Transapical Beating-Heart Septal Myectomy for Hypertrophic Obstructive Cardiomyopathy: A Retrospective Study
Authors Qiu J, Li Y, Li R, Fang J, Liu W, Mei W ![]() , Wei X, Yao W
, Wei X, Yao W
Received 20 August 2025
Accepted for publication 6 January 2026
Published 12 January 2026 Volume 2026:19 562160
DOI https://doi.org/10.2147/JPR.S562160
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Rushna Ali
Jin Qiu,1– 3 Yan Li,1– 3 Rui Li,4– 6 Jing Fang,4– 6 Wenhua Liu,7 Wei Mei,1– 3 Xiang Wei,4– 6 Wenlong Yao1– 3
1Department of Anesthesiology, Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, People’s Republic of China; 2Key Laboratory of Geriatric Anesthesia and Perioperative Brain Health, Hubei, People’s Republic of China; 3Clinical Research Center for Geriatric Anesthesia, Wuhan, People’s Republic of China; 4Division of Cardiovascular Surgery, Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, People’s Republic of China; 5Key Laboratory of Organ Transplantation, Ministry of Education, Wuhan, People’s Republic of China; 6NHC Key Laboratory of Organ Transplantation, Ministry of Health, Wuhan, People’s Republic of China; 7Clinical Research Center, Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, People’s Republic of China
Correspondence: Wenlong Yao, Email [email protected]
Objective: This study aimed to evaluate the postoperative pain in patients with hypertrophic cardiomyopathy who underwent transapical beating-heart septal myectomy (TA-BSM) and to explore whether a thoracic paravertebral nerve block (TPVB) can effectively alleviate the postoperative pain resulting from this surgical procedure.
Methods: Patients aged 18– 75 years, classified as American Society of Anesthesiologists II–III, who underwent TA-BSM between April and September 2023, were included. A total of 197 patients were initially enrolled and evaluated in this study. Following the application of the inclusion and exclusion criteria, 136 participants were allocated to two cohorts: a control group (CON group) and a TPVB group, based on whether a TPVB was administered before the surgical intervention. Demographic data, perioperative characteristics, visual analog scale scores, analgesic strategy, and Quality of recovery-15 scores were evaluated.
Results: After inverse probability of treatment weighting (IPTW) adjustment, the standardized mean difference in baseline characteristics between the two groups was < 0.1. The incidence of moderate-to-severe pain on postoperative day 7 was 51.7% in the TPVB group compared to 71.1% in the CON group. The adjusted relative risk for moderate-to-severe pain was 0.748 [95% CI, 0.565 to 0.990] via IPTW analysis. The oral morphine equivalent administered via PCA during the initial 48 hours post-surgery was significantly lower in the TPVB group than in the CON group (225 vs 195; median difference, 34.5 [95% CI, 21 to 48]; P < 0.001).
Conclusion: Preoperative administration of a single TPVB before TA-BSM was associated with a reduced postoperative pain intensity, ranging from moderate to severe, and a subsequent decrease in opioid usage. TPVB may be a beneficial analgesic strategy for patients undergoing TA-BSM.
Keywords: thoracic paravetebral nerve block, transapical beating-heart septal myectomy, postoperative pain, regional anesthesia, opioid-sparing strategy
Introduction
Pain can activate the sympathetic nervous system, which places a huge burden on the heart that has just undergone surgical injury. Inadequately managed acute pain can increase respiratory complications, heighten the risk of persistent postoperative pain, as well as contribute to prolonged hospital stay and higher medical costs.1 Although patients with cardiac conditions frequently exhibit complex clinical profiles accompanied by multiple comorbidities and experience significant postoperative pain, the strategies for effective postoperative pain management have become more complicated because use of high-dose opioids, which are associated with adverse effects such as respiratory depression, addiction, delirium, and gastrointestinal dysfunction, is no longer recommended.2 Optimizing pain management through multimodal non-opioid analgesia, such as regional anesthesia techniques, can reduce reliance on opioids and provide more comprehensive analgesic effects by acting on multiple pain pathways.2
Transapical beating-heart septal myectomy (TA-BSM) is a novel minimally invasive procedure for the management of hypertrophic obstructive cardiomyopathy (HOCM).3 TA-BSM is designed to minimize surgical trauma and expedite postoperative recovery. Although the procedure has been associated with shorter hospital stays, it remains unclear whether it effectively reduces postoperative pain, as no relevant reports have been published yet. Patients undergoing TA-BSM are typically discharged on postoperative day 8, rendering pain assessment on postoperative day 7 a clinically meaningful endpoint. This necessitates optimized pain management and presents new challenges in clinical anesthesia.
Thoracic paravertebral nerve block (TPVB) is a technique for administering local anesthetics to the paravertebral space, relieving both somatic and visceral pain within the targeted dermatomal region.4,5 The surgical incision for TA-BSM is similar to that of thoracoscopic surgery, typically made at the level of the fifth intercostal space near the mid-clavicular line. The analgesia range of TPVB can cover the surgical area of TA-BSM; however, to date, no studies have specifically evaluated the impact of TPVB on postoperative pain outcomes following TA-BSM. Therefore, its efficacy in this clinical setting remains uncertain. Ropivacaine, a long-acting amide local anesthetic, offers a favorable sensory-motor dissociation with a wide safety margin and has been extensively adopted in clinical practice for TPVB. This study aimed to retrospectively assess the postoperative pain outcomes in patients who have undergone TA-BSM and investigate the role of TPVB in the postoperative pain management of TA-BSM. It was hypothesized that TPVB would reduce postoperative pain in patients undergoing TA-BSM.
Materials and Methods
Study Design and Participants
The study was approved by the Ethics Committee of Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology (TJ-IRB20230910) and was registered at ClinicalTrials.gov (Identifier: NCT06433089). The study cohort comprised patients, aged 18–75 years, who were classified as American Society of Anesthesiologists (ASA) physical status II–III and underwent TA-BSM between April and September 2023. Exclusion criteria encompassed individuals undergoing additional surgical procedures, those requiring cardiopulmonary bypass during surgery, or those opting out of patient-controlled analgesia (PCA) postoperatively because of personal preferences. Participants were non-randomly allocated into two cohorts—a control group (CON group) and TPVB group—based on whether a TPVB was administered before the surgical intervention, which mainly depended on the anesthesiologist’s preference and patient’s own will.
Anesthesia and Surgical Technique
A standardized anesthesia protocol has been implemented at our center since the initial report of TA-BSM.6 Preoperatively, the need for TPVB was assessed by specialized anesthesiologists based on clinical judgment and patient-specific factors. Upon admission to the operating room, patients underwent electrocardiographic and pulse oximetry monitoring. Under local anesthesia, invasive blood pressure monitoring was performed by inserting a radial artery catheter. An experienced anesthesiologist performed ultrasound-guided TPVB in patients in the TPVB group who were positioned laterally. Ultrasonography was performed in the parasagittal plane. Using the out-of-plane puncture method, significant signs of subpleural pressure were observed in the T5–6, T6–7, and T7–8 interspaces. At each of these locations, 6–7 mL of local anesthetic was injected, resulting in a cumulative volume of 20 mL of 0.375% ropivacaine.7
Subsequently, all patients were placed in the supine position for induction of anesthesia with sufentanil, etomidate, and cisatracurium. A single-lumen endotracheal tube was inserted, and mechanical ventilation was used to maintain the PetCO2 levels between 35 and 40 mmHg. Central venous catheterization was performed with the patient in the Trendelenburg position. Anesthesia maintenance involved the inhalation of sevoflurane combined with an intravenous infusion of sufentanil, dexmedetomidine, and cisatracurium.
TA-BSM was performed via minithoracotomy using an innovative beating-heart myectomy device (BMD) under transesophageal echocardiography (TEE) guidance. Briefly,3 minithoracotomy was made within the fifth intercostal space along the left midclavicular line. Double-circumferential purse-string sutures were placed in the avascular zone at the apex to facilitate left ventricular (LV) access for BMD insertion. Following heparinization, LV apical pressure was measured using a manometric catheter inserted through the purse-string suture. Septal myectomy was performed using BMD-guided TEE imaging. After resection, manometric assessments were repeated, followed by protamine neutralization. During surgery, head-down positioning was used to prevent air embolism, and appropriate fluid resuscitation combined with the use of vasoactive medications was administered to maintain systolic blood pressure below 120 mmHg and heart rate below 80 beats per minute. Local infiltration anesthesia using ropivacaine was administered at the surgical incision sites. Patients were transferred back to the cardiac intensive care unit postoperatively while maintaining endotracheal intubation until fully awake for extubation.
Postoperative Analgesia Protocol and Rescue Analgesics
Postoperative analgesia was primarily managed through PCA, with no additional intravenous analgesics administered for mild pain, defined as a visual analog scale (VAS) score of 0–3. In instances where the PCA dosage was increased, and patients continued to experience moderate pain (VAS scores of 4–6), supplementary nonsteroidal anti-inflammatory drugs, such as diclofenac sodium or flurbiprofen axetil, were administered. For severe pain (VAS scores of 7–10), a single intravenous opioid analgesic, including dezocine, butorphanol, or nalbuphine, was administered.
Outcome Measures
All variables were sourced directly from electronic health records. The primary endpoint was the incidence of moderate-to-severe pain on postoperative day 7 following TA-BSM, defined as a VAS score greater than 3 on that day, encompassing moderate pain (VAS scores of 4–6) and severe pain (VAS scores of 7–10).
Secondary outcomes encompassed total morphine consumption during the first 48 hours following surgery, with all analgesics standardized to their oral morphine equivalent (OME) for the final analysis.8 Other secondary outcomes included the frequency of rescue analgesic administration for inadequate analgesia, VAS scores at 48 hours postoperatively, postoperative quality of recovery measured by Quality of recovery-15 (QoR-15) scores on postoperative day 7, and the length of hospital stay. The mean arterial pressure (MAP) data at five intraoperative time points were also analyzed: P1 = pre-induction, P2 = five minutes post-tracheal intubation, P3 = immediately pre-incision, P4 = five minutes post-incision, and P5 = five minutes post-placement of the rib spreader.
Statistical Analysis
Statistical analyses were performed using SPSS version 22.0. Continuous variables were expressed as means (standard deviations) or medians (interquartile ranges), depending on whether the data distribution was normal, as determined using the Kolmogorov–Smirnov test. Baseline characteristics between groups were balanced using inverse probability of treatment weighting (IPTW). The propensity score was determined using binary logistic regression analysis based on whether TPVB was administered, incorporating all relevant variables. All data in the CON group were weighted as 1/[1-propensity score]. The weighted values were used for the subsequent analysis with an IPTW tag or a weighted tag.
Baseline differences between groups were evaluated using the standardized mean difference (SMD), with a threshold of >0.1 deemed clinically significant. After IPTW analysis, baseline covariates were balanced, all with an SMD <0.1. Robust Poisson regression analysis was conducted to explore the primary outcome: risk of moderate-to-severe pain on the seventh postoperative day after TA-BSM. Univariable regression models were used to assess the associations between postoperative pain outcomes and potential predictors, including patient age, gender, BMI, ASA status, whether TPVB was administered, duration of anesthesia, and resected grams of myocardium. Candidate variables were selected based on established pain-associated factors from prior literature and clinically relevant parameters identified through expert consensus. A multivariable model was constructed incorporating variables with a univariable P <0.1. The final adjusted relative risk (RR) was obtained via the IPTW analysis. Alternative analytical methods were applied to secondary endpoints, with the choice of t-tests, Mann–Whitney U-tests, or chi-square tests determined by the nature and distribution of the observed data. All results were recalculated after IPTW. Statistical significance was defined as P <0.05. Hemodynamic comparisons utilized Mann–Whitney U-tests with Bonferroni correction (P <0.01 indicating significance). Median difference (MD), rate difference (RD) and 95% confidence interval (CI) were calculated.
Results
Patient Recruitment
A total of 197 patients were initially enrolled and evaluated in the study. 61 patients were excluded based on the exclusion criteria. After these exclusions, 136 patients remained: 76 (55.9%) in the CON group and 60 (44.1%) in the TPVB group (Figure 1).
 |
Figure 1 Flow diagram for enrolling patients. Abbreviations: CON, control group; CPB, cardiopulmonary bypass; PCA, patient-controlled analgesia; TPVB, thoracic paravertebral block group. |
Baseline Characteristics
The demographic and perioperative characteristics of patients are summarized in Table 1. TPVB did not significantly influence these baseline features. Further analysis showed SMD values>0.1 for age, gender, and BMI between the groups (Table 1). Following IPTW adjustments, the variables were well-balanced across both cohorts (Table 2).
 |
Table 1 Demographic and Perioperative Characteristics |
 |
Table 2 Demographic and Perioperative Characteristics by IPTWa |
Primary Outcome
The rate of moderate-to-severe pain associated with exercise on the seventh postoperative day after TA-BSM was markedly lower in the TPVB group than in the CON group (51.7 vs 71.1; MD, −19.4[95% CI, −35.9 to −2.9], P =0.02). This difference remained consistent post-IPTW adjustment (52.6 vs 70.1; MD, −17.6 [95% CI, −29.1 to −6.2], P =0.003).
Independent risk factors with P <0.1, including TPVB administration status and age were identified through univariate regression and included in the multivariate analyses. Robust Poisson regression indicated that participants receiving TPVB experienced a lower RR of moderate-to-severe pain than those in the CON cohort, with adjusted RR remaining stable before and after IPTW adjustment (0.739 [95% CI, 0.559 to 0.976], P =0.033 vs 0.748 [95% CI, 0.565 to 0.990], P =0.043) (Tables 3 and 4). This robust regression model has statistically significant (likelihood ratio χ2 = 7.580, P =0.023). Meanwhile, the ratio of the deviance to degrees of freedom is 1.166, indicating a good fit without overdispersion issues. Sensitivity analysis (including re-inclusion of all confounding factors and re-analysis with binary logistic regression, odds ratio is 0.445 [95% CI, 0.216–0.916], P =0.028) further confirmed that the association between the main exposure factor (TPVB use) and the outcome (moderate-to-severe pain) remained stable.
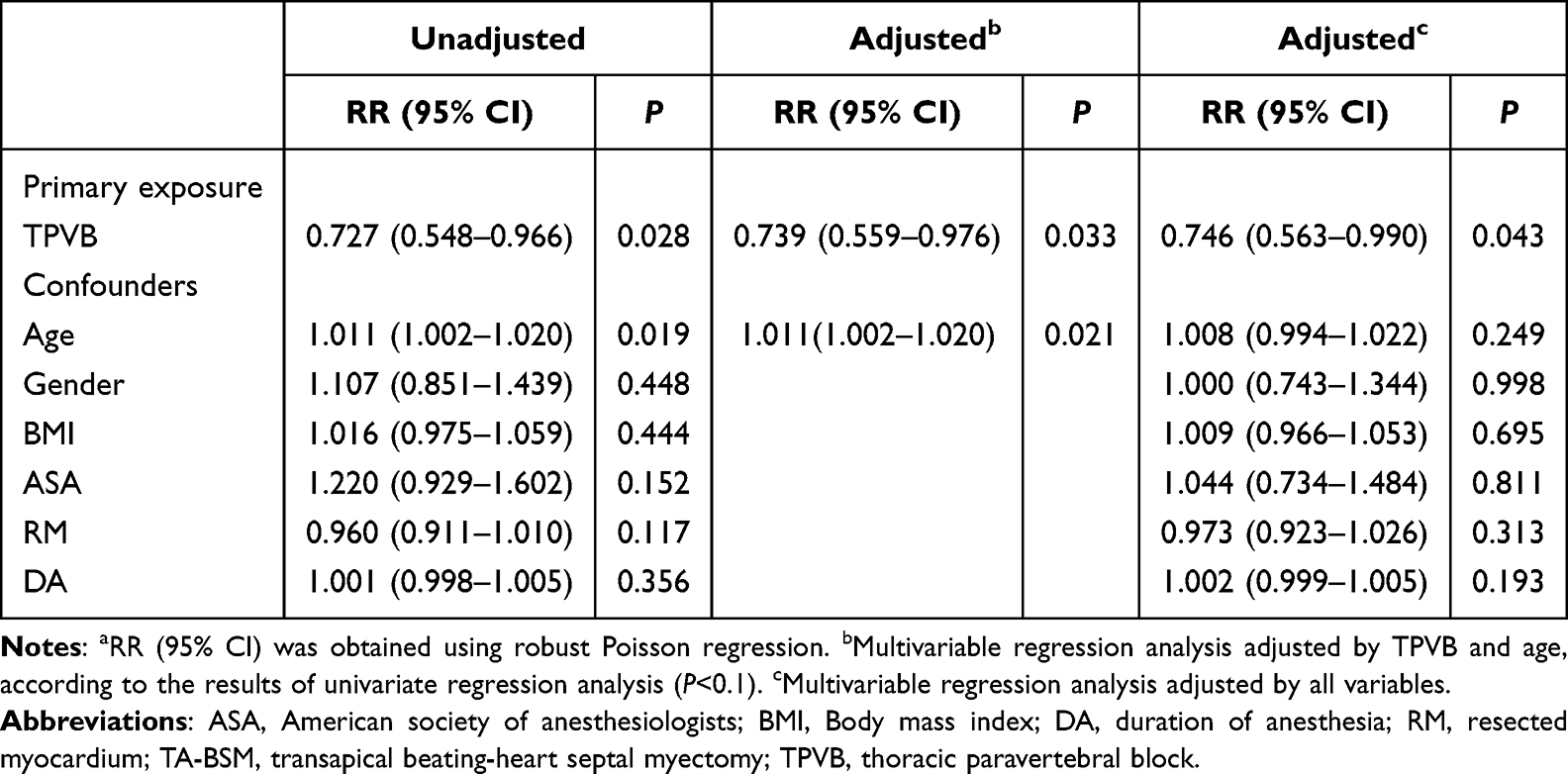 |
Table 3 Risk of Moderate-to-Severe Pain on the 7th Postoperative Day After TA-BSMa |
 |
Table 4 Risk of Moderate-to-Severe Pain on the 7th Postoperative Day After TA-BSM by IPTWa |
Secondary Outcomes
OMEs administered via PCA during the initial 48 hours post-surgery were significantly lower in the TPVB group than in the CON group (225 vs 195; MD, 34.5 [95% CI, 21 to 48]; P <0.001) (Table 5).
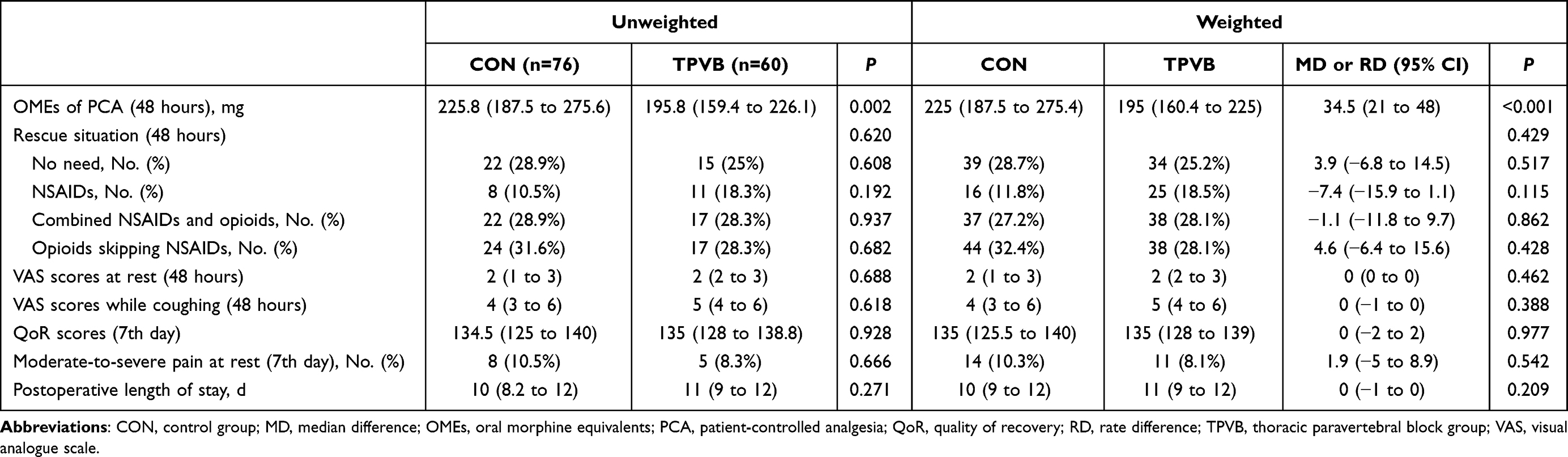 |
Table 5 Postoperative Differences Between the Two Groups |
Table 5 illustrates that no statistical disparities were observed in the residual indicators, including rescue interventions (within 48 hours), VAS scores (both at rest and during coughing at 48 hours), QoR-15 scores (on postoperative day 7), incidence of moderate-to-severe pain at rest (on postoperative day 7), and length of hospital stay (postoperative).
The differences in MAP at the five intraoperative time points are illustrated in Figure 2. As shown in Figure 2A, the MAP readings for the TPVB group were considerably lower than those for the CON group at P4 (MD, 8[95% CI, 5 to 11]; P <0.001) and P5 (MD, 6[95% CI, 3 to 10]; P <0.001). Furthermore, as shown in Figure 2B, these results remained consistent following IPTW adjustment, P4 (MD, 8[95% CI, 6 to 10] P <0.001) and P5 (MD, 6[95% CI, 4 to 9]; P <0.001).
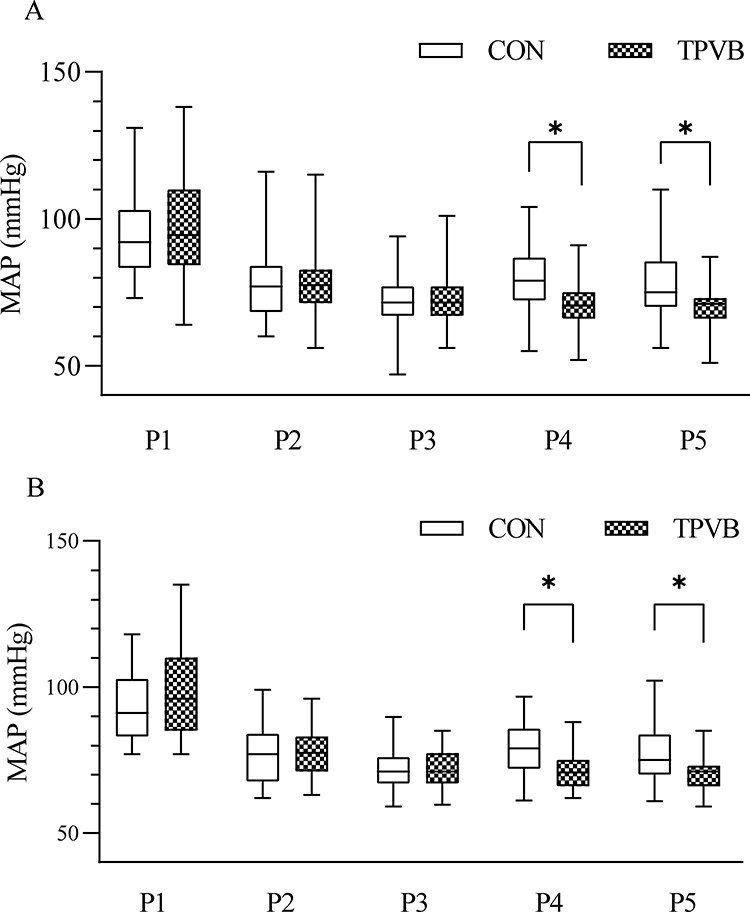 |
Figure 2 (A) Perioperative differences of MAP between the two groups. (B) Perioperative differences of MAP between the two groups by IPTW. Data are expressed as median (horizontal bar), interquartile range (box) and the maximum and minimum values (whiskers). Mann–Whitney U-test was used for comparison between groups, and *P <0.01 (Bonferroni correction) was considered significant. Abbreviations: CON, control group; IPTW, inverse probability of treatment weighting; MAP, mean arterial pressure; TPVB, thoracic paravertebral block group; P1, pre-induction; P2, five minutes post-tracheal intubation; P3, immediately pre-incision; P4, five minutes post-incision; P5, five minutes post-placement of the rib spreader. |
Discussion
This study demonstrated that administering a single TPVB prior to TA-BSM significantly reduces the incidence of exercise-related moderate-to-severe pain on post-TA-BSM day 7, with an adjusted RR of 0.748 [95% CI, 0.565 to 0.990] after application of IPTW. Furthermore, a significant reduction in PCA dosage was observed in the TPVB group compared to the CON group during the initial 48 hours post-TA-BSM.
As a technique for multimodal and opioid-sparing analgesia, TPVB aligns with the trends in enhanced recovery after cardiac surgery (ERACS) protocols and opioid stewardship initiatives. This reliable regional anesthesia technique is widely employed in various thoracic surgeries, particularly breast procedures, as it provides comprehensive pain relief while reducing opioid consumption.9–11 A study found that TPVB reduces immediate postoperative pain, with a 73% decrease in morphine consumption.12 Another study demonstrated that patients in the TPVB group received a lower dose of tramadol hydrochloride (221 ± 45 mg vs 250 ± 38 mg).13 Although the numerical results of different studies are difficult to compare directly, the role of TPVB in postoperative analgesia has been confirmed by a large number of studies. The surgical incision for TA-BSM, which is comparable to that used in thoracoscopic surgery, is typically located at the fifth intercostal space along the midclavicular line on the left side. Our findings further corroborate that TPVB could benefit patients undergoing TA-BSM, and patients in the TPVB group demonstrated a significant decrease in the PCA dosage.
Although opioid use was reduced, there were no significant differences in QoR-15 and length of hospital stay. This might be related to prompt rescue analgesia measures. To ensure adequate patient comfort in the CON group, standard anesthesia protocols included local infiltration around the incisions and prompt rescue analgesia measures. Consequently, no statistically significant differences were observed between the groups in terms of VAS scores both at rest and during coughing 48 hours post-surgery, indicating adequate pain management. This finding contrasts with those of previous studies that investigated the varying postoperative pain scores following TPVB during the early postoperative phase.7,14 However, the reduction in PCA dosages observed in our study supports TPVB’s potential for effective postoperative pain management.
Minimally invasive cardiac surgery facilitates accelerated postoperative recovery; however, management of postoperative pain remains a significant concern. This perspective has been corroborated by other studies, including those focusing on minimally invasive mitral valve repair.15 While hospitalized patients may receive substantial doses of analgesics for acute pain relief, challenges arise upon discharge when activity limitations due to persistent discomfort adversely affect their daily functioning and overall quality of life. The effect of inadequate pain management in the emergency department has been reported.16 Pain management after discharge, especially transitional pain services during the first week, should be evaluated from new perspectives.17 Our study primarily focused on evaluating pain scores on the 7th postoperative day, a critical time point for assessing patient discharge readiness, as many patients are discharged from the second day onward. While resting pain levels remained relatively low among participants undergoing this procedure, a marked increase was noted in instances involving severe exertional pain, which correlated with the administration of TPVB. It is important to distinguish between movement-evoked pain versus pain at rest.18,19 Hospitalized patients typically remain bedridden for extended periods, resulting in minimal manifestation of resting pain. However, following discharge, engagement in daily activities becomes necessary, making movement-evoked pain a clinically significant concern that warrants careful assessment. This prompted us to focus on assessing the occurrences related specifically to moderate-to-severe movement-evoked distress as pivotal indicators guiding decisions regarding discharge preparedness.
Furthermore, our findings suggest that TPVB can effectively reduce stress levels in patients during the perioperative period. Given that TA-BSM requires heart rate (HR) control through the administration of esmolol, no significant differences in HR were expected between the two groups; however, MAP was significantly lower in the TPVB group than in the CON group at P4 and P5. This indicates that TPVB may alleviate the stress associated with skin incision and rib spreader placement.
During TPVB administration, ultrasound-guided visualization is crucial to minimize complications, such as vascular injury and inadvertent epidural injection. Heparinization plays a critical role in TA-BSM. Therefore, meticulous attention must be directed toward preventing vascular injuries that could lead to hemorrhage from compromised vessels after heparinization, potentially resulting in additional complications. Intercostal nerve and serratus anterior plane blocks may serve as viable alternatives.20,21 Currently, comparative studies of regional anesthesia techniques such as TPVB and Erector Spinae Plane Block have demonstrated varying outcomes, providing novel perspectives for optimizing postoperative analgesia and highlighting the variability in therapeutic efficacy among these regional block approaches.7,22,23
This study has three primary limitations. First, the single-center retrospective design inherently precludes randomization of TPVB administration, potentially introducing selection bias caused by non-standardized application criteria used by clinicians. Second, the absence of longitudinal follow-up data precludes assessment of the enduring effects of TPVB on chronic pain development post-TA-BSM. Finally, the observational nature of the study restricts causal inference regarding the mechanistic pathways of TPVB’s opioid-sparing effects and pain state modulation.
This study suggests a significant difference in exercise-related pain levels after TA-BSM among patients receiving TPVB despite the administration of adequate rescue analgesia. The specific mechanisms underlying these findings warrant further investigation, given the retrospective nature of this study, and the role of reduced opioid doses within this mechanism is noteworthy. Multimodal analgesia reportedly reduces opioid use after thoracic surgery, thus further reducing opioid use after discharge. A recent randomized controlled study identified hypothermia as a possible novel risk factor associated with TPVB, noting that participants who underwent this procedure had considerably reduced body temperatures.24 Although hypothermia can serve as a protective mechanism for organs during cardiac surgery, this raises important questions regarding the application of TPVB in TA-BSM and necessitates further investigation.
Conclusion
This study demonstrates that TPVB improves postoperative analgesia in patients undergoing TA-BSM, with significantly lower PCA opioid use and better perioperative stress control. Notably, TPVB is associated with reduced exercise-related pain, highlighting its value during ERACS. Given the limitations of retrospective designs, prospective randomized controlled trials with systematic long-term follow-up are needed to assess TPVB’s impact on chronic postoperative pain and persistent opioid use. Linking the morphine equivalent threshold with clinical recovery outcomes may have greater clinical meaningfulness. However, these findings support integrating TPVB into multimodal analgesia for TA-BSM, alongside standardized protocols and further mechanistic research to help optimize its use.
Data Sharing Statement
Deidentified participant data will be available upon request from the corresponding author, Dr. Yao. The data will be available from 6 months to 2 years after publication.
Acknowledgments
The authors thank all participants in this study.
Disclosure
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
References
1. Makkad B, Heinke TL, Sheriffdeen R, et al. Practice advisory for preoperative and intraoperative pain management of cardiac surgical patients: part 2. Anesth Analg. 2023;137:26–11. doi:10.1213/ANE.0000000000006506
2. Grant MC, Chappell D, Gan TJ, et al. Pain management and opioid stewardship in adult cardiac surgery: joint consensus report of the perioperative quality initiative and the enhanced recovery after surgery cardiac society. J Thorac Cardiovasc Surg. 2023;166:1695–1706.e2. doi:10.1016/j.jtcvs.2023.01.020
3. Fang J, Liu Y, Zhu Y, et al. First-in-human transapical beating-heart septal myectomy in patients with hypertrophic obstructive cardiomyopathy. J Am Coll Cardiol. 2023;82:575–586. doi:10.1016/j.jacc.2023.05.052
4. Feray S, Lubach J, Joshi GP, et al. PROSPECT guidelines for video-assisted thoracoscopic surgery: a systematic review and procedure-specific postoperative pain management recommendations. Anaesthesia. 2022;77:311–325. doi:10.1111/anae.15609
5. Zhang W, Cong X, Zhang L, et al. Effects of thoracic nerve block on perioperative lung injury, immune function, and recovery after thoracic surgery. Clin Transl Med. 2020;10:e38. doi:10.1002/ctm2.38
6. Xu Q, Li R, Liu Y, et al. Anesthetic procedure for transapical beating-heart septal myectomy in patients with hypertrophic obstructive cardiomyopathy: report of three cases. J Anesth Transl Med. 2024;3:138–142. doi:10.1016/j.jatmed.2024.10.002
7. Chen N, Qiao Q, Chen R, et al. The effect of ultrasound-guided intercostal nerve block, single-injection erector spinae plane block and multiple-injection paravertebral block on postoperative analgesia in thoracoscopic surgery: a randomized, double-blinded, clinical trial. J Clin Anesth. 2020;59:106–111. doi:10.1016/j.jclinane.2019.07.002
8. Nielsen S, Degenhardt L, Hoban B, et al. Comparing opioids: a guide to estimating oral morphine equivalents (OME) in research [UNSW NDARC Web site. 2014. Available from: https://ndarc.med.unsw.edu.au/sites/default/files/ndarc/resources/TR.329.pdf.
9. Slinchenkova K, Lee K, Choudhury S, et al. A review of the paravertebral block: benefits and complications. Curr Pain Headache Rep. 2023;27:203–208. doi:10.1007/s11916-023-01118-1
10. Nair S, Gallagher H, Conlon N. Paravertebral blocks and novel alternatives. BJA Educ. 2020;20:158–165. doi:10.1016/j.bjae.2020.01.006
11. Abu Elyazed MM, Mostafa SF. Continuous pectoral nerve block compared with continuous thoracic paravertebral block and intravenous opioid analgesia for the postoperative analgesic efficacy in patients undergoing modified radical mastectomy: a prospective randomized trial. Clin J Pain. 2021;37:359–365. doi:10.1097/AJP.0000000000000932
12. Albi-Feldzer A, Dureau S, Ghimouz A, et al. Preoperative paravertebral block and chronic pain after breast cancer surgery: a double-blind randomized trial. Anesthesiology. 2021;135(6):1091–1103. doi:10.1097/ALN.0000000000003989
13. Zheng C, Wang J, Xie S. Ultrasound-guided thoracic paravertebral nerve block on postoperative pain, quality of life, and recovery in patients with non-small-cell lung cancer. Biomed Res Int. 2021;2021:6692815. doi:10.1155/2021/6692815
14. Sandeep B, Huang X, Li Y, et al. A comparison of regional anesthesia techniques in patients undergoing video-assisted thoracic surgery: a network meta-analysis. Int J Surg. 2022;105:106840. doi:10.1016/j.ijsu.2022.106840
15. Jahanian S, Arghami A, Wittwer ED, et al. Does minimally invasive mitral valve repair mean less postoperative pain? Ann Thorac Surg. 2023;115:1172–1178. doi:10.1016/j.athoracsur.2022.11.009
16. Ten Doesschate SFH, Kuijper TM, Koopman S, et al. Pain severity at emergency department discharge as a predictor for chronification of pain. Pain Rep. 2022;7:e1048. doi:10.1097/PR9.0000000000001048
17. Clarke H, Katz J. Patterns of opioid use after surgical discharge: pain management beyond the first postoperative week. Anaesthesia. 2024;79:909–913. doi:10.1111/anae.16352
18. Gilron I, Lao N, Carley M, et al. Movement-evoked pain versus pain at rest in postsurgical clinical trials and in meta-analyses: an updated systematic review. Anesthesiology. 2024;140:442–449. doi:10.1097/ALN.0000000000004850
19. Kehlet H. Postoperative pain, analgesia, and recovery-bedfellows that cannot be ignored. Pain. 2018;159 Suppl 1:S11–S16. doi:10.1097/j.pain.0000000000001243
20. Guerra-Londono CE, Privorotskiy A, Cozowicz C, et al. Assessment of intercostal nerve block analgesia for thoracic surgery: a systematic review and meta-analysis. JAMA Network Open. 2021;4:e2133394. doi:10.1001/jamanetworkopen.2021.33394
21. Baytar MS, Yilmaz C, Karasu D, et al. Comparison of ultrasonography guided serratus anterior plane block and thoracic paravertebral block in video-assisted thoracoscopic surgery: a prospective randomized double-blind study. Korean J Pain. 2021;34:234–240. doi:10.3344/kjp.2021.34.2.234
22. Swisher MW, Wallace AM, Sztain JF, et al. Erector spinae plane versus paravertebral nerve blocks for postoperative analgesia after breast surgery: a randomized clinical trial. Reg Anesth Pain Med. 2020;45:260–266. doi:10.1136/rapm-2019-101013
23. Jack JM, McLellan E, Versyck B, et al. The role of serratus anterior plane and pectoral nerves blocks in cardiac surgery, thoracic surgery and trauma: a qualitative systematic review. Anaesthesia. 2020;75:1372–1385. doi:10.1111/anae.15000
24. Yan Y, Geng J, Cui X, et al. Thoracic paravertebral block decreased body temperature in thoracoscopic lobectomy patients: a randomized controlled trial. Ther Clin Risk Manag. 2023;19:67–76. doi:10.2147/TCRM.S392961
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.