Back to Journals » OncoTargets and Therapy » Volume 9
Postoperative hepatitis B virus reactivation in hepatitis B virus-related hepatocellular carcinoma patients with hepatitis B virus DNA levels <500 copies/mL
Authors Xie Z, Wang X, Fu D ![]() , Zhong J, Yang X, Li L
, Zhong J, Yang X, Li L
Received 15 January 2016
Accepted for publication 7 May 2016
Published 25 July 2016 Volume 2016:9 Pages 4593—4603
DOI https://doi.org/10.2147/OTT.S104300
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Min Li
Zhi-Bo Xie,1,2,* Xiao-Bo Wang,1,3,* De-Liang Fu,2 Jian-Hong Zhong,1,4 Xia-Wei Yang,1 Le-Qun Li1,4
1Department of Hepatobiliary Surgery, Affiliated Tumor Hospital of Guangxi Medical University, Nanning, 2Department of Pancreatic Surgery, Pancreatic Disease Institute, Huashan Hospital, Shanghai Medical College, Fudan University, Shanghai, 3Department of Hepatobiliary Surgery, Affiliated Minzu Hospital of Guangxi Medical University, 4Guangxi Liver Cancer Diagnosis and Treatment Engineering and Technology Research Center, Nanning, People’s Republic of China
*These authors contributed equally to this work
Background: Patients with hepatocellular carcinoma have the risk of postoperative hepatitis B virus (HBV) reactivation (PHR). Antiviral therapy was given to patients with detectable HBV DNA levels but not to patients with undetectable HBV DNA levels.
Methods: In this retrospective study, 258 patients were enrolled (HBV DNA levels <500 copies/mL group, n=159, and HBV DNA levels >500 copies/mL group, n=99).
Results: A total of 50 patients (19.4%) had PHR. The following significant factors related to PHR were found: without antiviral therapy (hazard ratio [HR] =0.17, 95% confidence interval [CI] 0.031–0.911), hepatitis B e antigen positivity (HR =5.20, 95% CI 1.931–14.007), hepatitis B core antigen S1 positivity (HR =2.54, 95% CI 1.116–5.762), preoperative HBV DNA levels ≥500 copies/mL (HR =1.28, 95% CI 1.085–2.884), hepatic inflow occlusion (HR =3.60, 95% CI 1.402–9.277), moderate liver cirrhosis or more (HR =2.26, 95% CI 1.001–5.121), and blood transfusion (HR =2.89, 95% CI 0.836–10.041). Recurrence-free survival time was significantly shorter in patients with PHR (23.06±2.46 months) than in patients without PHR (29.30±1.27 months).
Conclusion: Antiviral therapy could efficiently decrease the incidence of PHR. Patients with HBV DNA levels <500 copies/mL still have the risk of PHR. PHR remained as a prognostic risk factor for hepatocellular carcinoma recurrence and recurrence-free survival.
Keywords: hepatocellular carcinoma, hepatitis B virus, postoperative reactivation, hepatectomy, HBV DNA levels
Introduction
Hepatocellular carcinoma (HCC) is the fifth most common type of cancer in the world and is the third leading cause of cancer-related death.1 Hepatitis B virus (HBV) infection is the major risk factor for HCC patients, especially in Asia-Pacific region.2–4
Because of the high incidence of postoperative HCC recurrence, overall survival (OS) of HCC patients remains relatively low, despite surgery being a curative therapy.5,6 However, postoperative HBV reactivation (PHR) is one significant factor7,8 that contributes to HCC recurrence. Several trials9–12 and our previous study13 found that PHR occurs after hepatectomy in HBV-related HCC (HBV-HCC) patients. Hepatitis B e antigen (HBeAg), preoperative HBV DNA level, liver cirrhosis degree, blood transfusion, operating time, and preoperative antiviral therapy are independent risk factors for PHR.14 PHR occurs not only in HCC patients with high HBV DNA levels but also in HCC patients with low HBV DNA levels.14–16 According to the guidelines from the Asian Pacific Association for the Study of the Liver,17 antiviral therapy was available for patients with detectable HBV DNA levels. However, there are no obvious suggestions about using antiviral therapies in patients with undetectable HBV DNA levels.
Here, we aimed to evaluate the incidence of PHR in HBV-HCC patients with undetectable HBV DNA levels, thus finding out the difference of the short-term and long-term outcomes between patients with PHR and patients without PHR, with undetectable HBV DNA levels.
Patients and methods
Ethics statement
This study was approved by the Institutional Review Board of Guangxi Medical University and conducted in accordance with the Declaration of Helsinki and internationally accepted ethical guidelines. The patients enrolled in this study signed written consent during their admission for surgery for their information to be stored in hospital databases and used for research. During data collection, patient records were anonymized, as we previously mentioned in our former study.13
Patients
A total of 258 consecutive patients admitted to our hospital from 2011 to 2012 were retrospectively enrolled in our study. The inclusion criteria were as follows: 1) 18–75 years old; 2) HBV-infected HCC patients and first diagnosed in our hospital;17 3) Child-Pugh stages A to B; 4) resectable HCC patients;18 and 5) HCC confirmed by postoperative pathology.
Patients were divided into two groups based on their HBV DNA levels (Group A: patients with HBV DNA levels <500 copies/mL and Group B: patients with detectable HBV DNA levels). HCC was diagnosed based on the criteria of the European Association for the Study of the Liver.19
Preoperative management
A baseline assessment of HBV DNA; the presence of hepatitis B surface antigen, HBeAg, and against hepatitis B core antigen S1; serum levels of alanine aminotransferase (ALT), aspartate aminotransferase, total bilirubin (TBil), and albumin (ALB); prothrombin time (PT); levels of α-fetoprotein (AFP); and proportions of several T-lymphocyte subpopulations (CD3+CD4+ and CD3+CD8+) were tested within 1 week before hepatectomy.
Serum levels of HBV DNA were quantified using the PCR-based Care HBV V2 Assay Kit (Qiagen NV, Venlo, the Netherlands) in which the lower limit of detection was 500 copies/mL (1 IU/mL =1 copy/mL).
Entecavir (0.5 mg once a day; Tai-Tianqing Pharmaceutical Co., Jiangsu, People’s Republic of China) antiviral therapy was given to patients who fit the criteria of given antiviral therapy at least 3 days before hepatectomy.20
Surgical management
During hepatectomy, data on the surgical procedure, including tumor number, tumor diameter (the maximal tumor diameter), tumor rupture, complete capsule, surgical margin, tumor thrombus, hepatic inflow occlusion, operating time, blood loss, blood transfusion, and liver cirrhosis degree, were recorded.
Postoperative management
At the 1-month reexamination, the same blood tests and radiological examination as at baseline were repeated. Patients were monitored for PHR within postoperative 1 month. A tenfold increase in HBV DNA levels compared with preoperative levels as well as detectable level of HBV DNA postoperatively with undetectable level at baseline was defined as PHR.14 Patients with PHR were given antiviral therapy once upon the detection of reactivation.
Outcomes and follow-up
The primary outcomes in our study were recurrence-free survival (RFS). We compared the difference of RFS between patients with HBV DNA levels >500 copies/mL and <500 copies/mL. Subgroup analysis of RFS was conducted based on the status of PHR. As secondary outcomes, we compared postoperative complications between two subgroups. These complications were evaluated using the Clavien-Dindo scoring system.21
Statistical analysis
All data analyses were performed using SPSS 21.0 (IBM Corporation, Armonk, NY, USA) and with P<0.05 defined as the threshold of statistical significance. Normally distributed data were expressed as mean ± SD, while asymmetrically distributed data were expressed as median (range). Differences in outcomes between two groups were assessed using independent samples t-tests for measurement data or χ2 test for frequency of various attributes between groups. Factors significantly associated with PHR and HCC recurrence were identified first by univariate logistic regression, and then the significant univariate factors were examined by multivariate analysis using a stepwise logistic model. RFS curves were analyzed using the Kaplan–Meier method in which differences between curves were assessed using the log-rank test.
Comprehensive MEDLINE review
The following medical subject headings were comprehensively searched in the MEDLINE database: “hepatocellular carcinoma” or “primary liver carcinoma” or “primary liver cancer” or “liver cancer” or “liver tumor” and “hepatectomy” or “liver surgery” or “liver resection” or “hepatic resection” and “hepatitis B virus” and “reactivation”. Based on the following criteria, relevant references and review articles were manually searched: 1) evaluated PHR in HBV-HCC patients, 2) were published in English, and 3) outcomes were about survival outcomes, PHR rate, and HCC recurrence. We selected only the study with the largest number of participants when several studies were based on the same population.
Results
Characteristics of the study population
From January 2011 to 2012, 1,004 potentially eligible HCC patients were admitted to our hospital for hepatic resection. A total of 258 HCC patients satisfying the inclusion and exclusion criteria were enrolled. Of the 258 HCC patients, 159 patients with HBV DNA levels <500 copies/mL were defined as Group A and the remaining 99 patients with detectable HBV DNA levels were defined as Group B. Baseline characteristics were similar between the two groups (Table 1). Of the 258 HCC patients enrolled, 33 (12.8%) patients with detectable HBV DNA levels were given antiviral therapy. After hepatectomy, 50 (19.4%) patients (24 patients with HBV DNA levels <500 copies/mL and 15.1% and 26 patients with detectable HBV DNA levels, 26.3%) had PHR. Of the 33 patients with antiviral therapy, one (3.0%) patient had PHR.
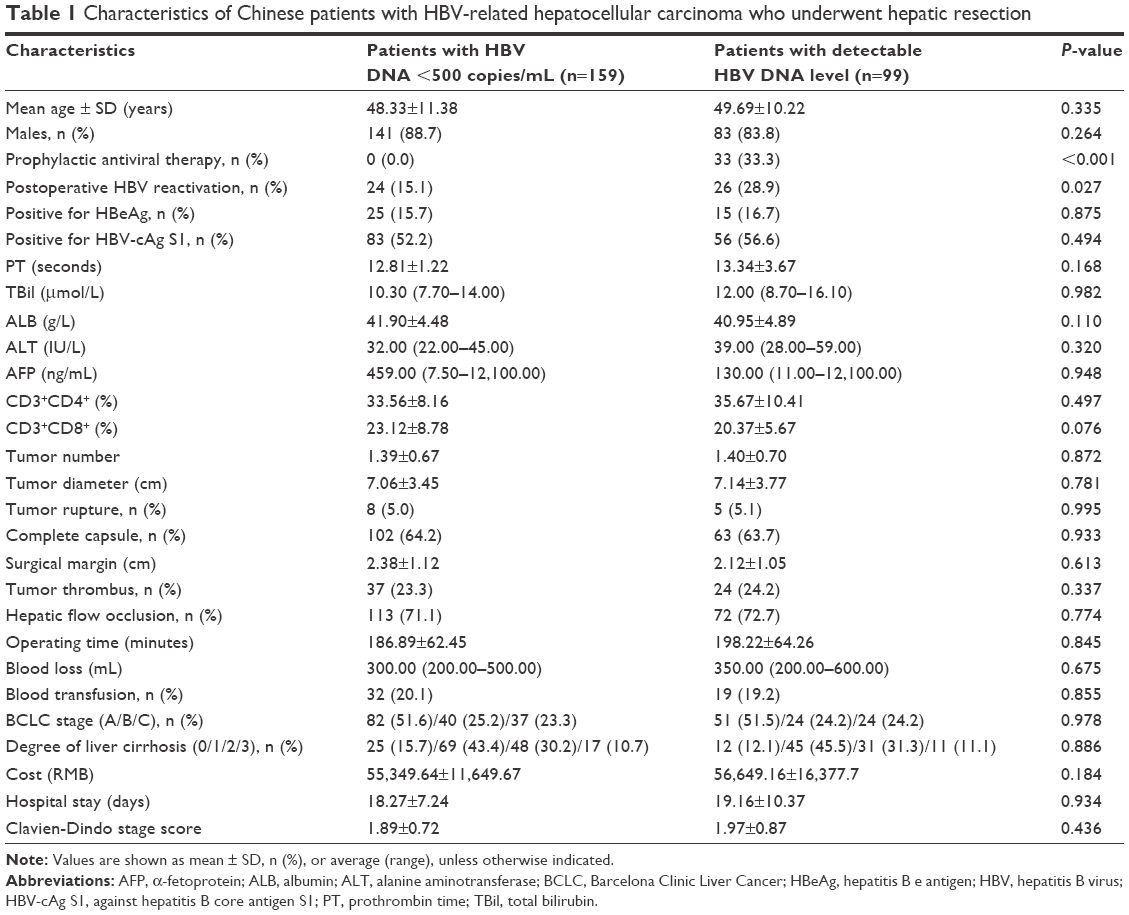 | Table 1 Characteristics of Chinese patients with HBV-related hepatocellular carcinoma who underwent hepatic resection |
PHR
A total of 50 (19.4%) patients had PHR of whom one (1/33, 3.0%) patient was given antiviral therapy and the remaining 49 (49/225, 21.8%) patients were without antiviral therapy. In patients with HBV DNA levels <500 copies/mL, 24 (15.1%) patients had PHR.
We conducted univariate and multivariate analyses and found the following significant factors related with PHR: without antiviral therapy (hazard ratio [HR] =0.17, 95% CI 0.031–0.911, P<0.001), HBeAg positivity (HR =5.20, 95% CI 1.931–14.007, P=0.001), against hepatitis B core antigen S1 positivity (HR =2.54, 95% CI 1.116–5.762, P=0.026), preoperative HBV DNA level of ≥500 copies/mL (HR =1.28, 95% CI 1.085–2.884, P=0.030), hepatic inflow occlusion (HR =3.60, 95% CI 1.402–9.277, P=0.008), moderate liver cirrhosis or more (HR =2.26, 95% CI 1.001–5.121, P=0.049), and blood transfusion (HR =2.89, 95% CI 0.836–10.041, P=0.043) (Table 2). Thus, HBV DNA levels >500 copies/mL and without preoperative antiviral therapy remained independent risk factors for PHR.
 | Table 2 Univariate and multivariate analyses of prognostic factors for HBV reactivation in Chinese patients with HBV-related HCC |
RFS
RFS (23.06±2.46 months) was significantly lower in patients with PHR than in patients without PHR (29.30±1.27 months, P=0.014) (Figure 1). One-year, 2-year, and 3-year RFS rates for patients with PHR were 75.8%, 38.1%, and 28.9%, respectively, and those for patients without PHR were 84.5%, 56.5%, and 40.7%, respectively.
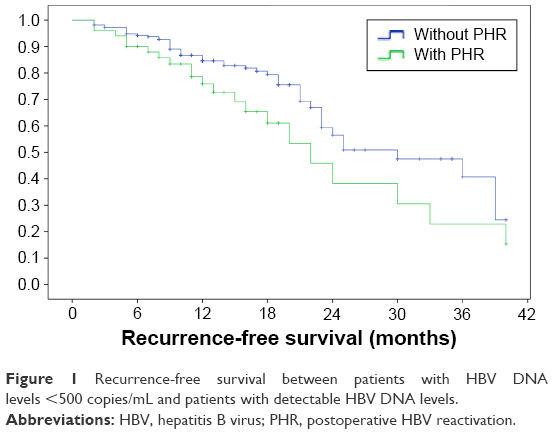 | Figure 1 Recurrence-free survival between patients with HBV DNA levels <500 copies/mL and patients with detectable HBV DNA levels. |
We conducted univariate and multivariate analyses and found the following significant risk factors for RFS: PHR (HR =1.48, 95% CI 1.228–2.023, P=0.047), HBeAg positivity (HR =4.84, 95% CI 2.617–8.941, P<0.001), surgical margin <1 cm (HR =0.53, 95% CI 0.290–0.964, P=0.038), moderate or serve liver cirrhosis (HR =1.88, 95% CI 1.040–3.377, P=0.036), and blood transfusion (HR =3.25, 95% CI 1.691–6.213, P<0.001) (Table 3).
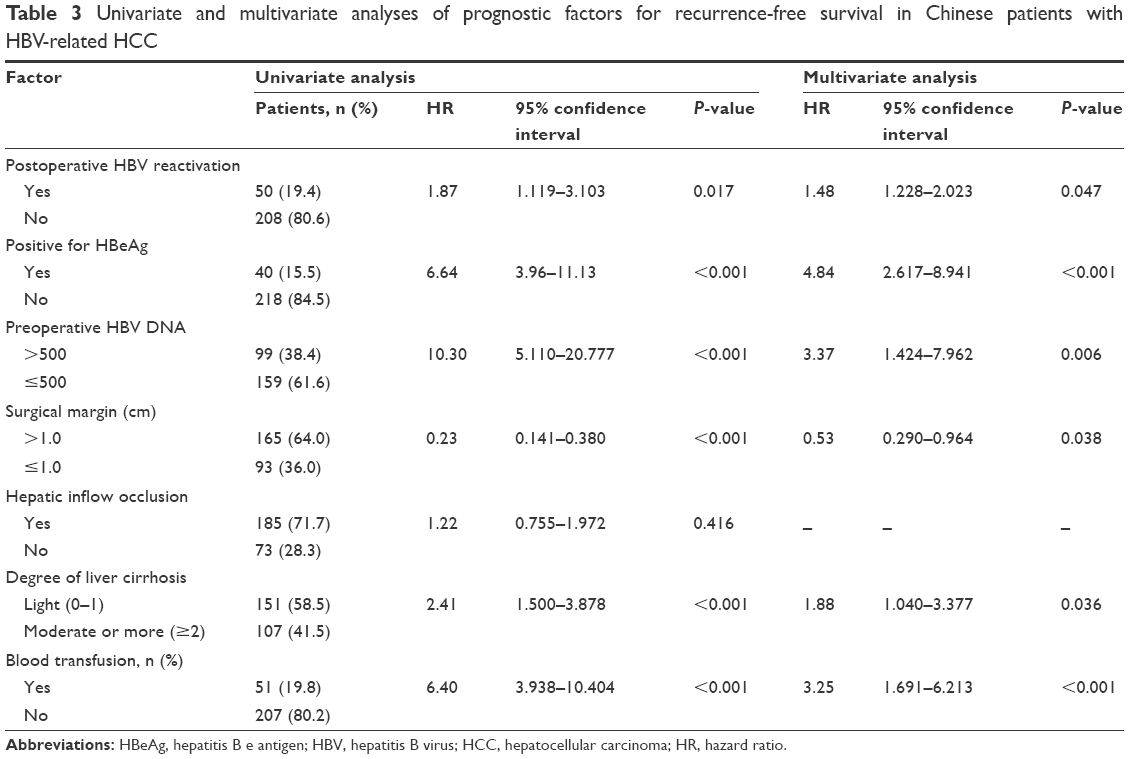 | Table 3 Univariate and multivariate analyses of prognostic factors for recurrence-free survival in Chinese patients with HBV-related HCC |
Subgroup analysis of RFS depending on antiviral therapy was also conducted. We found that patients with and without antiviral therapy had similar RFS (28.13 months and 27.82 months, respectively, P=0.996).
Postoperative complications and recurrence
Postoperative Clavein-Dindo stage score and hospital stay were similar between patients with HBV DNA levels <500 copies/mL and patients with detectable HBV DNA levels (P=0.436 and P=0.934).
Then, we compared the postoperative complications between patients with PHR and patients without PHR and found that patients with PHR had a significantly higher morbidity rate (P=0.048) and a higher Clavein-Dindo stage score (P=0.038) (Table S1).
We also conducted univariate and multivariate analyses of HCC recurrence and found the following risk factors: HBeAg positivity (HR =5.36, 95% CI 1.523–18.863, P=0.009), portal vein thrombus (HR =1.70, 95% CI 0.227–3.135, P=0.047), and blood transfusion (HR =218.15, 95% CI 21.946–2,168.391, P<0.001) (Table S2).
Perioperative changes
Both biochemical (PT, TBil, ALB, ALT, and AFP) and immune (CD3+CD4+ and CD3+CD8+) outcomes were compared between patients with PHR and patients without PHR (Table S3). We found that patients with PHR had significantly lower ALB levels not only preoperatively (P=0.001) but also postoperatively (P=0.032). However, levels of PT, TBil, ALT, and AFP were similar between the two groups. Patients with PHR had a significantly lower percentage of CD3+CD4+ (P=0.041) at baseline and a significantly lower percentage of CD3+CD4+ (P<0.001) and CD3+CD8+ (P<0.001) after hepatectomy when compared with patients without PHR.
Literature review
A total of eight studies were enrolled in our review.9–12,14,16,22,23 We analyzed the PHR, recurrence, RFS, and associated risk factors. Most patients were from Southeast Asia, which has the highest prevalence of HCC (Tables S4 and S5).
Discussion
Many studies9–11,14,16,22 and our previous study13 figured out that PHR occurred after hepatectomy. However, the mechanism of PHR is not clear. We previously inferred that PHR may be associated with the immunosuppression induced by hepatectomy. Also, some other studies claimed that increased apoptosis of CD4+/CD8+ T-cells and the immunosuppression associated with surgical injury.24,25 It is commonly believed that PHR remains the independent risk factor for HCC recurrence and RFS.14,23 Moreover, studies found that preoperative antiviral therapy could efficiently decrease the PHR rate and reduce the HCC recurrence, thus prolonging the RFS.14,16
In our study, PHR rates are 3.0% and 21.8% in patients with and without antiviral therapy, respectively. The results were similar to those of our previous prospective study13 (total PHR rate, 19.3%; PHR rate in patients with antiviral therapy, 2.2%; PHR rate in patients without antiviral therapy, 27.8%). In our literature review, total PHR rate varied from 6.1% to 40.7% and PHR rate varied from 0.0% to 4.7% in patients with antiviral therapy.9–12,14,16,22,23 For patients with antiviral therapy, PHR rate was significantly decreased. Studies claimed that antiviral therapy predicted good long-term survival.26,27 Other studies figured that antiviral therapy had no significant influence on HCC recurrence and OS.28–30 Hepatocarcinogenesis may be initiated by continuous HBV replication.31–33 Antiviral therapy may reduce HCC recurrence and prolong survival by suppressing and reducing continuous viremia and long-term hepatic inflammation. In our study, antiviral therapy remained the significant risk factor for PHR. However, antiviral therapy was not the independent risk factor for RFS and HCC recurrence. Also, we previously found that antiviral therapy failed to prolong short-term survival.34
PHR rate was lower in our study than that in the study conducted by Huang et al14 (16.7%). It is mainly because the HBV DNA lower limit is different. Our lower limit was 500 copies/mL (1 IU/mL =1 copy/mL according to the instruction of the kit), whereas their lower limit was 200 IU/mL (800 copies/mL, 1 IU/mL =4 copies/mL according to Chinese guidelines20). In our result, HBV DNA load is still regarded as a risk factor, and a high HBV DNA load has been reported to be associated with an increased incidence of PHR.14,35 In our literature review, antiviral therapy was found to be a protective factor.9,11,12,14
Due to the high incidence of HCC recurrence, OS of HCC patients still stays unsatisfied.36 In our study, patients with PHR suffered worse RFS (RFS: 23 months and 29 months for patients with and without PHR, respectively, and 1-year, 2-year, and 3-year RFS rates were 75.8%, 38.1%, and 28.9% and 84.5%, 56.5%, and 40.7% for patients with and without PHR, respectively). As described by Huang et al,14 PHR still remained the prognostic factor for RFS in multivariate regression analysis. Postoperative continuous HBV replication may constantly accelerate liver cirrhosis and give rise to HCC recurrence so as to decrease the RFS.37,38 Continuously, viremia may do harm to our immune system and cause multicentric carcinogenesis.39,40 Moreover, this replication may enhance tumor development and spread through the upregulation of adhesion molecules.39
We found that HBeAg positivity was the independent risk factor for HCC recurrence and OS. Many studies claimed that HBeAg-positive patients have a higher risk of PHR and are associated with HCC recurrence.14,23 Also, a change from HBeAg-negative to HBeAg-positive status still related to PHR.41,42 The immune system has been broken down in HCC patients, especially in postoperative HCC patients. Resection induces immunosuppression and permits enhanced viral replication. Therefore, patients in the immune clearance phase, especially HBeAg-positive patients, were at risk for reactivation of viral replication after surgery.
Several limitations could be found in this study. First, our retrospective design of the study was the biggest limitation. However, the baseline characteristics were similar between the two groups. This may decrease the selection bias to some extent. Second, we did not have long follow-ups, and we took only RFS into consideration. Ideally, we would continue to follow up on these patients for decades. In future, a better designed trial with a large sample and a long follow-up need to be further established.
Conclusion
PHR indeed occurs after hepatectomy in HBV-HCC patients. Antiviral therapy could efficiently decrease the incidence of PHR. Patients with PHR are associated with HCC recurrence and a worse RFS. Patients with HBV DNA levels <500 copies/mL still have the risk of PHR.
Acknowledgment
This work was supported by grants from the National Major Special Science and Technology Project (no 2012ZX10002010001009).
Disclosure
The authors report no conflicts of interest in this work.
References
Torre LA, Bray F, Siegel RL, Ferlay J, Lortet-Tieulent J, Jemal A. Global cancer statistics, 2012. CA Cancer J Clin. 2015;65(2):87–108. | ||
de Martel C, Ferlay J, Franceschi S, et al. Global burden of cancers attributable to infections in 2008: a review and synthetic analysis. Lancet Oncol. 2012;13(6):607–615. | ||
McGlynn KA, Tsao L, Hsing AW, Devesa SS, Fraumeni JF Jr. International trends and patterns of primary liver cancer. Int J Cancer. 2001;94(2):290–296. | ||
Kirk GD, Lesi OA, Mendy M, et al. The Gambia Liver Cancer Study: infection with hepatitis B and C and the risk of hepatocellular carcinoma in West Africa. Hepatology. 2004;39(1):211–219. | ||
Poon RT, Fan ST, Lo CM, Liu CL, Wong J. Long-term survival and pattern of recurrence after resection of small hepatocellular carcinoma in patients with preserved liver function: implications for a strategy of salvage transplantation. Ann Surg. 2002;235(3):373–382. | ||
Chen MF, Hwang TL, Jeng LB, Wang CS, Jan YY, Chen SC. Postoperative recurrence of hepatocellular carcinoma. Two hundred five consecutive patients who underwent hepatic resection in 15 years. Arch Surg. 1994;129(7):738–742. | ||
Hung IF, Poon RT, Lai CL, Fung J, Fan ST, Yuen MF. Recurrence of hepatitis B-related hepatocellular carcinoma is associated with high viral load at the time of resection. Am J Gastroenterol. 2008;103(7):1663–1673. | ||
Shah SA, Cleary SP, Wei AC, et al. Recurrence after liver resection for hepatocellular carcinoma: risk factors, treatment, and outcomes. Surgery. 2007;141(3):330–339. | ||
Huang L, Li J, Lau WY, et al. Perioperative reactivation of hepatitis B virus replication in patients undergoing partial hepatectomy for hepatocellular carcinoma. J Gastroenterol Hepatol. 2012;27(1):158–164. | ||
Huang L, Li J, Yan J, et al. Antiviral therapy decreases viral reactivation in patients with hepatitis B virus-related hepatocellular carcinoma undergoing hepatectomy: a randomized controlled trial. J Viral Hepat. 2013;20(5):336–342. | ||
Dan JQ, Zhang YJ, Huang JT, et al. Hepatitis B virus reactivation after radiofrequency ablation or hepatic resection for HBV-related small hepatocellular carcinoma: a retrospective study. Eur J Surg Oncol. 2013;39(8):865–872. | ||
Lao XM, Luo G, Ye LT, et al. Effects of antiviral therapy on hepatitis B virus reactivation and liver function after resection or chemoembolization for hepatocellular carcinoma. Liver Int. 2013;33(4):595–604. | ||
Xie ZB, Zhu SL, Peng YC, et al. Postoperative hepatitis B virus reactivation and surgery-induced immunosuppression in patients with hepatitis B-related hepatocellular carcinoma. J Surg Oncol. 2015;112(6):634–642. | ||
Huang G, Lai EC, Lau WY, et al. Posthepatectomy HBV reactivation in hepatitis B-related hepatocellular carcinoma influences postoperative survival in patients with preoperative low HBV-DNA levels. Ann Surg. 2013;257(3):490–505. | ||
Li X, Zhong X, Chen ZH, et al. Hepatitis B virus DNA negativity acts as a favorable prognostic factor in hepatocellular carcinoma patients. Asian Pac J Cancer Prev. 2014;15(22):9635–9641. | ||
Huang G, Lau WY, Shen F, et al. Preoperative hepatitis B virus DNA level is a risk factor for postoperative liver failure in patients who underwent partial hepatectomy for hepatitis B-related hepatocellular carcinoma. World J Surg. 2014;38(9):2370–2376. | ||
Liaw YF, Leung N, Kao JH, et al; Chronic Hepatitis B Guideline Working Party of the Asian-Pacific Association for the Study of the Liver. Asian-Pacific consensus statement on the management of chronic hepatitis B: a 2008 update. Hepatol Int. 2008;2(3):263–283. | ||
Zhong JH, Ke Y, Gong WF, et al. Hepatic resection associated with good survival for selected patients with intermediate and advanced-stage hepatocellular carcinoma. Ann Surg. 2014;260(2):329–340. | ||
Bruix J, Sherman M, Llovet JM, et al; EASL Panel of Experts on HCC. Clinical management of hepatocellular carcinoma. Conclusions of the Barcelona-2000 EASL conference. European Association for the Study of the Liver. J Hepatol. 2001;35(3):421–430. | ||
Chinese Society of Hepatology and Chinese Society of Infectious Diseases, Chinese Medical Association. The guideline of prevention and treatment for chronic hepatitis B (2010 version). Zhonghua Gan Zang Bing Za Zhi. 2011;19(1):13–24. | ||
Dindo D, Demartines N, Clavien PA. Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg. 2004;240(2):205–213. | ||
Huang G, Lau WY, Wang ZG, et al. Antiviral therapy improves postoperative survival in patients with hepatocellular carcinoma: a randomized controlled trial. Ann Surg. 2015;261(1):56–66. | ||
Sohn W, Paik YH, Cho JY, et al. Influence of hepatitis B virus reactivation on the recurrence of HBV-related hepatocellular carcinoma after curative resection in patients with low viral load. J Viral Hepat. 2015;22(6):539–550. | ||
Dietz A, Heimlich F, Daniel V, Polarz H, Weidauer H, Maier H. Immunomodulating effects of surgical intervention in tumors of the head and neck. Otolaryngol Head Neck Surg. 2000;123(1 Pt 1):132–139. | ||
Delogu G, Moretti S, Antonucci A, et al. Apoptosis and surgical trauma: dysregulated expression of death and survival factors on peripheral lymphocytes. Arch Surg. 2000;135(10):1141–1147. | ||
Yuen MF, Fong DY, Wong DK, Yuen JC, Fung J, Lai CL. Hepatitis B virus DNA levels at week 4 of lamivudine treatment predict the 5-year ideal response. Hepatology. 2007;46(6):1695–1703. | ||
Chan HL, Wong VW, Tse CH, et al. Early virological suppression is associated with good maintained response to adefovir dipivoxil in lamivudine resistant chronic hepatitis B. Aliment Pharmacol Ther. 2007;25(8):891–898. | ||
Kuzuya T, Katano Y, Kumada T, et al. Efficacy of antiviral therapy with lamivudine after initial treatment for hepatitis B virus-related hepatocellular carcinoma. J Gastroenterol Hepatol. 2007;22(11):1929–1935. | ||
Chuma M, Hige S, Kamiyama T, et al. The influence of hepatitis B DNA level and antiviral therapy on recurrence after initial curative treatment in patients with hepatocellular carcinoma. J Gastroenterol. 2009;44(9):991–999. | ||
Li N, Lai EC, Shi J, et al. A comparative study of antiviral therapy after resection of hepatocellular carcinoma in the immune-active phase of hepatitis B virus infection. Ann Surg Oncol. 2010;17(1):179–185. | ||
Colombo M, Sangiovanni A. Etiology, natural history and treatment of hepatocellular carcinoma. Antiviral Res. 2003;60(2):145–150. | ||
Lupberger J, Hildt E. Hepatitis B virus-induced oncogenesis. World J Gastroenterol. 2007;13(1):74–81. | ||
Chen JD, Yang HI, Iloeje UH, et al; Risk Evaluation of Viral Load Elevation and Associated Liver Disease/Cancer in HBV (REVEAL-HBV) Study Group. Carriers of inactive hepatitis B virus are still at risk for hepatocellular carcinoma and liver-related death. Gastroenterology. 2010;138(5):1747–1754. | ||
Ke Y, Ma L, You XM, et al. Antiviral therapy for hepatitis B virus-related hepatocellular carcinoma after radical hepatectomy. Cancer Biol Med. 2013;10(3):158–164. | ||
Zhong S, Yeo W, Schroder C, et al. High hepatitis B virus (HBV) DNA viral load is an important risk factor for HBV reactivation in breast cancer patients undergoing cytotoxic chemotherapy. J Viral Hepat. 2004;11(1):55–59. | ||
European Association for the Study of the Liver, European Organisation for Research and Treatment of Cancer. EASL-EORTC clinical practice guidelines: management of hepatocellular carcinoma. J Hepatol. 2012;56(4):908–943. | ||
Chang TT, Liaw YF, Wu SS, et al. Long-term entecavir therapy results in the reversal of fibrosis/cirrhosis and continued histological improvement in patients with chronic hepatitis B. Hepatology. 2010;52(3):886–893. | ||
Marcellin P, Gane E, Buti M, et al. Regression of cirrhosis during treatment with tenofovir disoproxil fumarate for chronic hepatitis B: a 5-year open-label follow-up study. Lancet. 2013;381(9865):468–475. | ||
Kubo S, Hirohashi K, Tanaka H, et al. Effect of viral status on recurrence after liver resection for patients with hepatitis B virus-related hepatocellular carcinoma. Cancer. 2000;88(5):1016–1024. | ||
Kubo S, Hirohashi K, Tanaka H, et al. Virologic and biochemical changes and prognosis after liver resection for hepatitis B virus-related hepatocellular carcinoma. Dig Surg. 2001;18(1):26–33. | ||
Yoshiba M, Sekiyama K, Sugata F, Okamoto H, Yamamoto K, Yotsumoto S. Reactivation of precore mutant hepatitis B virus leading to fulminant hepatic failure following cytotoxic treatment. Dig Dis Sci. 1992;37(8):1253–1259. | ||
Bird GL, Smith H, Portmann B, Alexander GJ, Williams R. Acute liver decompensation on withdrawal of cytotoxic chemotherapy and immunosuppressive therapy in hepatitis B carriers. Q J Med. 1989;73(270):895–902. |
Supplementary materials
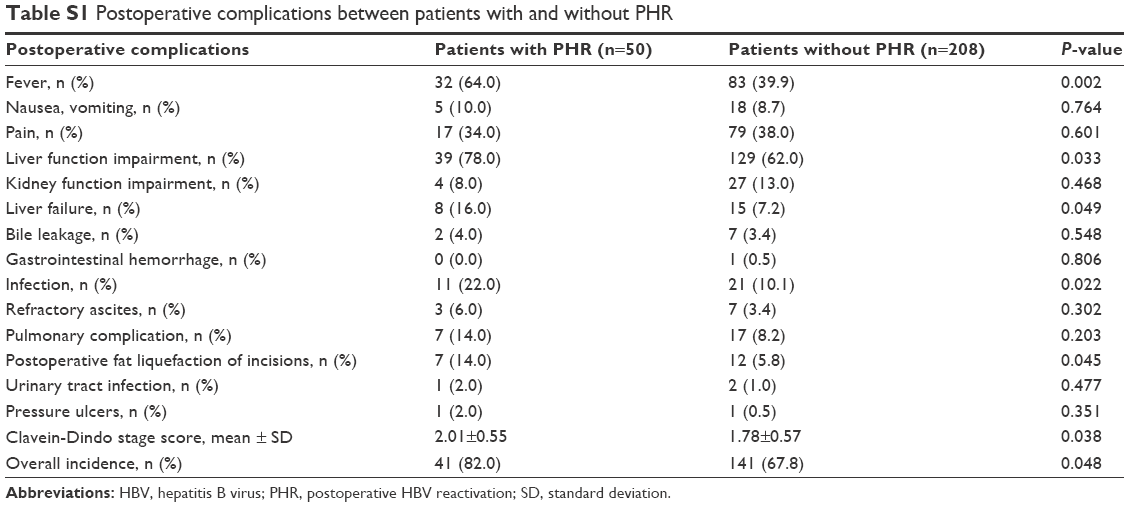 | Table S1 Postoperative complications between patients with and without PHR |
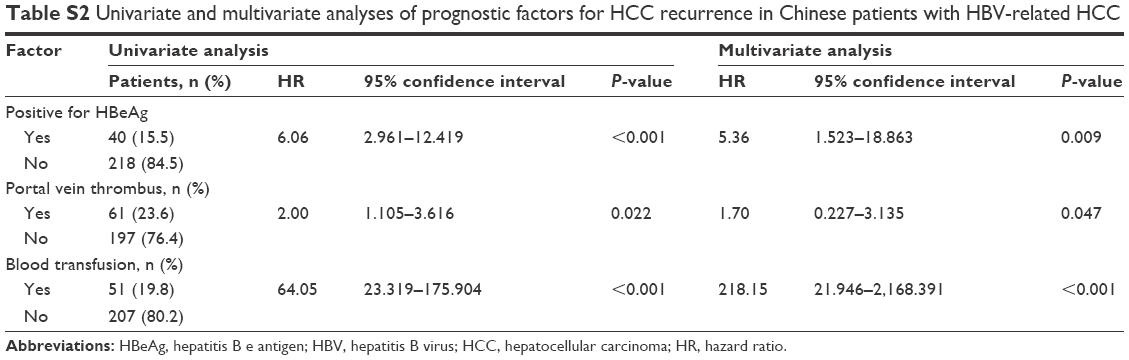 | Table S2 Univariate and multivariate analyses of prognostic factors for HCC recurrence in Chinese patients with HBV-related HCC |
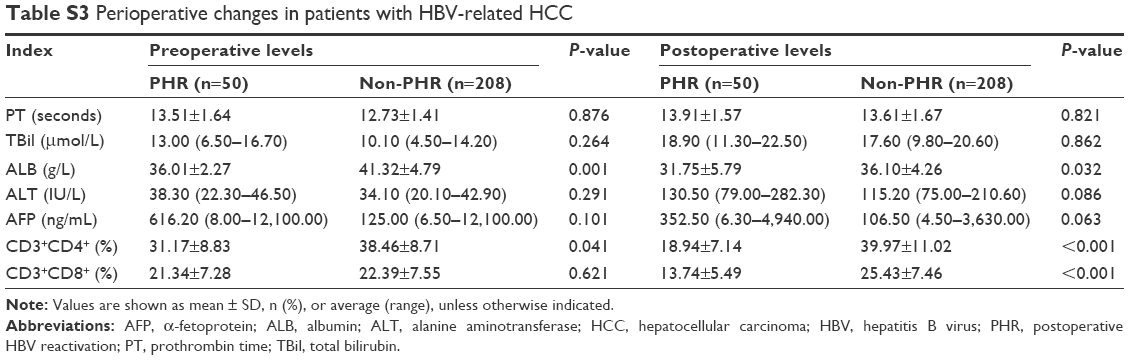 | Table S3 Perioperative changes in patients with HBV-related HCC |
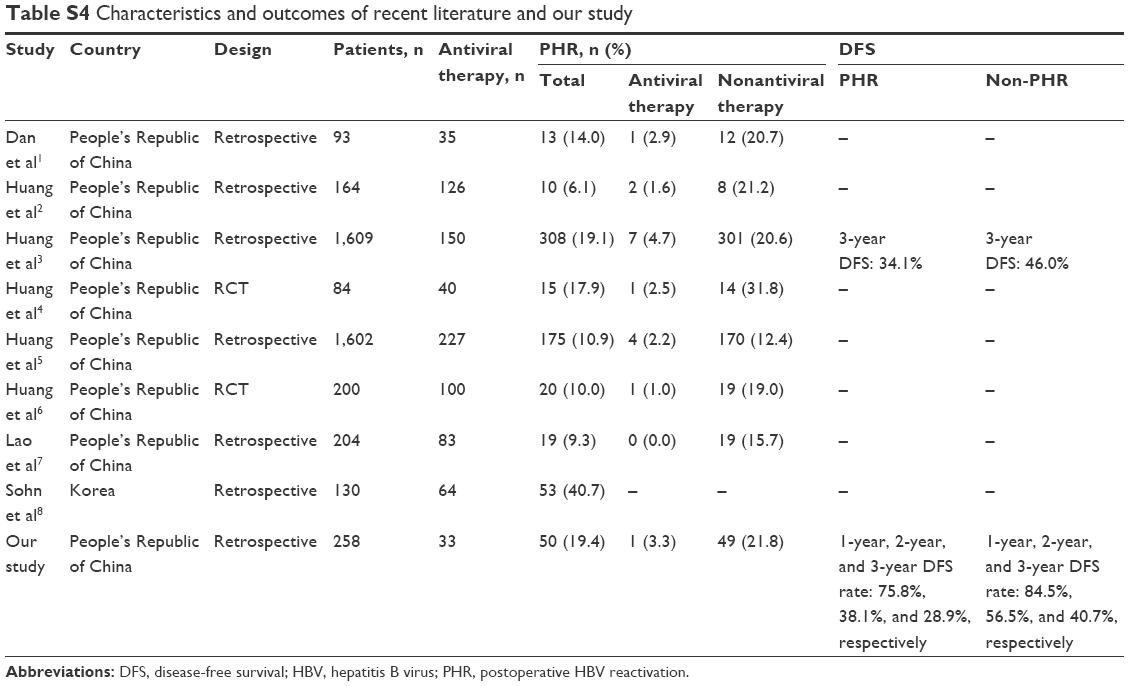 | Table S4 Characteristics and outcomes of recent literature and our study |
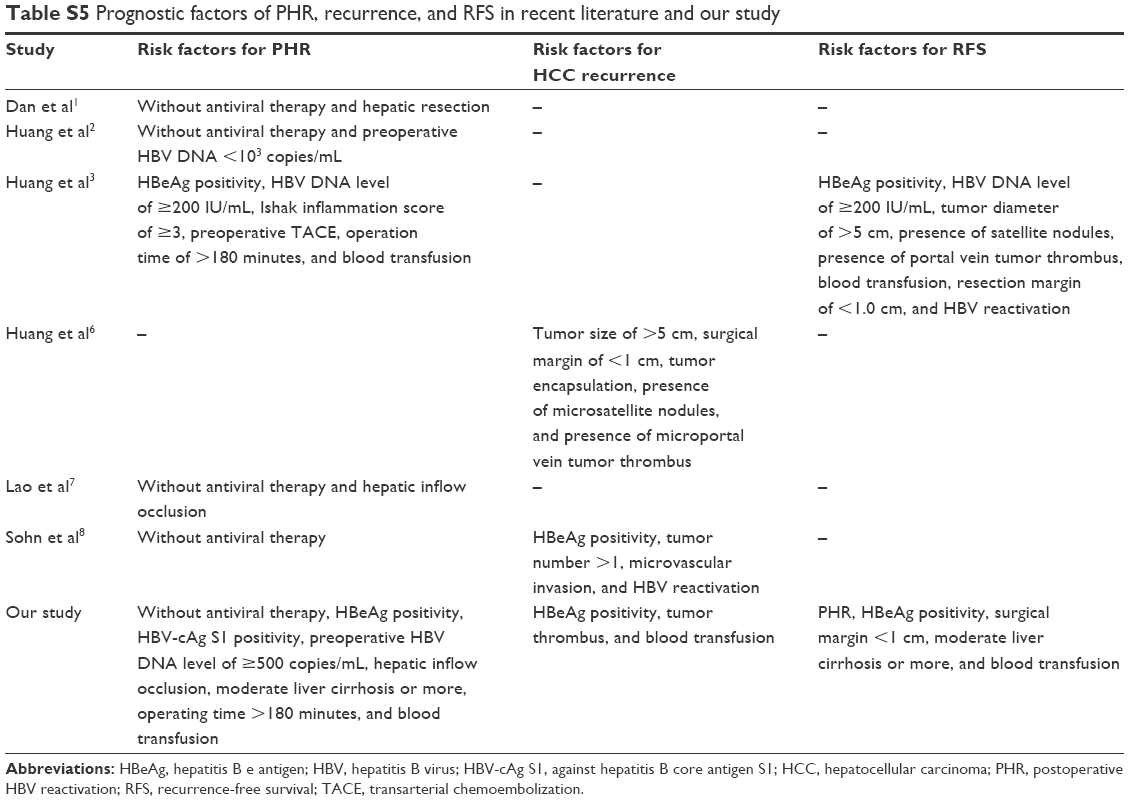 | Table S5 Prognostic factors of PHR, recurrence, and RFS in recent literature and our study |
References
Dan JQ, Zhang YJ, Huang JT, et al. Hepatitis B virus reactivation after radiofrequency ablation or hepatic resection for HBV-related small hepatocellular carcinoma: a retrospective study. Eur J Surg Oncol. 2013;39:865–872. | ||
Huang L, Li J, Lau WY, et al. Perioperative reactivation of hepatitis B virus replication in patients undergoing partial hepatectomy for hepatocellular carcinoma. J Gastroenterol Hepatol. 2012;27:158–164. | ||
Huang G, Lai EC, Lau WY, et al. Posthepatectomy HBV reactivation in hepatitis B-related hepatocellular carcinoma influences postoperative survival in patients with preoperative low HBV-DNA levels. Ann Surg. 2013;257:490–505. | ||
Huang L, Li J, Yan J, et al. Antiviral therapy decreases viral reactivation in patients with hepatitis B virus-related hepatocellular carcinoma undergoing hepatectomy: a randomized controlled trial. J Viral Hepat. 2013;20:336–342. | ||
Huang G, Lau WY, Shen F, et al. Preoperative hepatitis B virus DNA level is a risk factor for postoperative liver failure in patients who underwent partial hepatectomy for hepatitis B-related hepatocellular carcinoma. World J Surg. 2014;38:2370–2376. | ||
Huang G, Lau WY, Wang ZG, et al. Antiviral therapy improves postoperative survival in patients with hepatocellular carcinoma: a randomized controlled trial. Ann Surg. 2015;261:56–66. | ||
Lao XM, Luo G, Ye LT, et al. Effects of antiviral therapy on hepatitis B virus reactivation and liver function after resection or chemoembolization for hepatocellular carcinoma. Liver Int. 2013;33:595–604. | ||
Sohn W, Paik YH, Cho JY, et al. Influence of hepatitis B virus reactivation on the recurrence of HBV-related hepatocellular carcinoma after curative resection in patients with low viral load. J Viral Hepat. 2015;22:539–550. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.