Back to Journals » Local and Regional Anesthesia » Volume 19
Postoperative Delirium Following Continuous Fascia Iliaca Compartment Block in Elderly Patients with Hip Fracture: A Case Series and Literature Review
Authors Cao L ![]() , Xu G
, Xu G ![]() , Liu Z, Bai X
, Liu Z, Bai X ![]() , Li L
, Li L ![]() , Gao H
, Gao H ![]()
Received 18 March 2026
Accepted for publication 3 June 2026
Published 15 June 2026 Volume 2026:19 609445
DOI https://doi.org/10.2147/LRA.S609445
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 6
Editor who approved publication: Prof. Dr. Stefan Wirz
Lei Cao,1,* Guoqiang Xu,2,* Zhenyu Liu,2 Xiaodong Bai,2 Li Li,1 Hua Gao2
1Department of Anesthesiology, Beijing Friendship Hospital, Capital Medical University, Beijing, People’s Republic of China; 2Department of Orthopaedics, Beijing Friendship Hospital, Capital Medical University, Beijing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Hua Gao, Department of Orthopaedics, Beijing Friendship Hospital, Capital Medical University, No. 95 Yongan Road, Xicheng District, Beijing, 100050, People’s Republic of China, Email [email protected] Li Li, Department of Anesthesiology, Beijing Friendship Hospital, Capital Medical University, No. 95 Yongan Road, Xicheng District, Beijing, 100050, People’s Republic of China, Email [email protected]
Background: Postoperative delirium (POD) is a common complication in elderly patients with hip fracture. This study aimed to investigate the occurrence of POD in patients receiving continuous fascia iliaca compartment block (CFICB) with an opioid-containing solution, and review current evidence.
Case Presentation: We retrospectively analyzed four elderly patients (aged 73– 90 years) who developed delirium after receiving opioid-containing CFICB for hip fracture surgery. All received ultrasound-guided CFICB with ropivacaine 0.25% (loading dose 40mL) followed by continuous infusion (sufentanil 50μg + ropivacaine 100mg in 240mL saline at 3mL/h). The Montreal Cognitive Assessment (MoCA) was administered on admission. Patient characteristics were: Case 1 (73-year-old female, delirium onset postoperative day 4, MoCA = 26); Case 2 (90-year-old male, delirium onset postoperative day 2, MoCA = 18, surgery delayed 6 days); Case 3 (75-year-old male, delirium onset within 24 hours of surgery, MoCA = 28); Case 4 (87-year-old female, delirium occurred on the day of the block placement, MoCA = 15). Despite excellent post-CFICB pain control Visual Analog Scale (resting VAS ≤ 3) in all patients, delirium occurred, with durations ranging from 36 hours to 120 hours.
Conclusion: This small case series (n = 4) suggests that opioid-containing CFICB provides effective perioperative analgesia for elderly hip fracture patients but does not completely prevent postoperative delirium, particularly in patients with advanced age, baseline cognitive dysfunction, or delayed surgery. Given the retrospective design and small sample size, these findings are exploratory only. Larger prospective studies are needed.
Keywords: elderly, hip fracture, continuous fascia iliaca compartment block, postoperative delirium
Introduction
Hip fractures, predominantly femoral neck and intertrochanteric fractures, represent a major public health challenge in aging populations worldwide.1,2 The global incidence continues to rise with demographic aging, with projections estimating over 6 million hip fractures annually by 2050.1 However, perioperative management of these vulnerable patients remains challenging due to multiple age-related comorbidities and high complication rates.
Postoperative delirium (POD) is one of the most concerning complications following hip fracture surgery, affecting 20–50% of elderly patients.3,4 Characterized by acute fluctuations in consciousness and cognitive dysfunction, POD is independently associated with poor functional recovery, prolonged hospital stay, and increased mortality.4,5 Among modifiable risk factors, inadequate pain control has been consistently identified as an important precipitant of POD.6
Traditional postoperative analgesia relies primarily on opioids; however, elderly patients have increased sensitivity to opioids and are prone to adverse effects such as respiratory depression and sedation, which may paradoxically increase the risk of delirium.7 This has driven the development of opioid-sparing analgesic strategies. Regional anesthesia techniques, particularly peripheral nerve blocks, have emerged as promising alternatives by providing targeted analgesia.
Fascia iliaca compartment block (FICB) provides anterior hip analgesia by injecting local anesthetic into the fascia iliaca compartment, thereby blocking the femoral nerve, lateral femoral cutaneous nerve, and part of the obturator nerve.8,9 Ultrasound guidance has significantly improved the safety and success rate of FICB.10,11 To overcome the limited duration of analgesia (12–24 hours) provided by a single injection, continuous fascia iliaca compartment block (CFICB) delivers a continuous infusion of local anesthetic (48–72 hours) through an indwelling catheter, providing superior analgesia and reducing opioid consumption.12
Of note, although CFICB theoretically offers opioid-sparing advantages, the elderly hip fracture patients in our center are generally of advanced age, have poor pain tolerance, and require substantial intraoperative analgesia.13,14 Therefore, we added a low dose of sufentanil (50μg/240mL) to the continuous infusion solution.15 This regimen was intended to provide more stable perioperative analgesia and to avoid delirium induced by inadequate pain control. Moreover, this dose is considerably lower than systemic administration levels, pharmacokinetic studies have demonstrated that sufentanil administered into tissue compartments exhibits slow systemic absorption, and the concentration reaching the central nervous system is unlikely to reach levels associated with significant direct effects.16
However, the existing evidence regarding the role of CFICB in preventing postoperative delirium is inconsistent. While some studies have shown that CFICB reduces the incidence of delirium,17 others have not observed a clear benefit, suggesting that adequate pain control alone may be insufficient to prevent delirium in high-risk patients. Patient-specific factors such as advanced age, pre-existing cognitive impairment, and surgical delay may outweigh the protective effects of regional anesthesia.
This small case series (n = 4) is descriptive in nature and intended to generate hypotheses for future prospective studies. It reports four elderly hip fracture patients who developed delirium despite receiving opioid-containing CFICB, with the following objectives: (1) describe the clinical characteristics and temporal patterns of delirium; (2) identify potential risk factors that may limit the protective effects of CFICB; (3) discuss the available evidence on CFICB in pain management and delirium prevention; and (4) propose directions for optimizing perioperative management in high-risk patients.
Case Presentation
Ethical Approval
This retrospective case series was approved by the Ethics Committee of Beijing Friendship Hospital, Capital Medical University (Approval Number: 2024-P2-169-01).
General Information of Patients
This case series included four elderly patients who developed postoperative delirium after receiving CFICB for hip fracture surgery at our institution between January and October 2024. Demographic characteristics, comorbidities, surgery-related variables, and key laboratory findings are presented in Table 1. No surgical complications, postoperative infections, or acid-base disturbances were observed in any of the four cases. Patients with incomplete clinical data or comorbidities that could directly induce delirium (eg, intracranial infection, acute stroke) were excluded.
 |
Table 1 Demographic, Clinical, and Laboratory Characteristics of Four Elderly Patients with Hip Fracture |
Case 1: Delayed-Onset Delirium Despite Optimal Pain Control
A 73-year-old female presented with left intertrochanteric fracture following a fall. Medical history included type 2 diabetes mellitus, bilateral basal ganglia lacunar infarcts, asthma, and chronic bronchitis. Cognitive function was assessed using the Montreal Cognitive Assessment (MoCA) on admission. She was alert and oriented, with a MoCA score of 26 indicating intact cognition. CFICB was initiated on the second day after the fracture, and she underwent open reduction and internal fixation (ORIF) on the third day after the fracture under combined spinal-epidural anesthesia (CSEA).
Postoperatively, pain was well-controlled (resting Visual Analog Scale [VAS] score 1–2). However, on postoperative day 4, she developed disorganized speech, attention deficits, and fluctuating awareness; the 4 ‘A’s Test (4AT) score was 6. The delirium gradually resolved over 48 hours with supportive care including reorientation, sleep hygiene, and Olanzapine 2.5 mg as needed. She was discharged on postoperative day 12 with improved but not fully recovered cognitive status.
Case 2: Hyperactive Delirium in Nonagenarian with Surgical Delay
A 90-year-old male sustained a right intertrochanteric fracture. Due to medical optimization for bilateral pneumonia, pleural effusion, atrial fibrillation, coronary artery disease, and pericardial effusion, surgery was delayed until 6 days post-fracture. The MoCA score on admission was 18, suggestive of mild cognitive impairment. CFICB was initiated on day 5 post-fracture for pre-operative analgesia, which reduced the VAS score from 6 to 2.
He underwent hemiarthroplasty on the sixth day after injury under CSEA. On postoperative day 2, he developed hyperactive delirium characterized by visual hallucinations, agitation, and sleep-wake cycle reversal (4AT score = 8). Delirium management included low-dose olanzapine (2.5 mg nightly) and intensive nursing protocols. Symptoms persisted for 120 hours, and he was transferred to a rehabilitation facility on postoperative day 14.
Case 3: Immediate-Onset Delirium with Intact Baseline Cognition
A 75-year-old male with left intertrochanteric fracture had a history of hypertension, emphysema, and remote stroke. He was alert and cognitively intact on admission, the MoCA score on admission was 28, indicating intact cognitive function. CFICB was placed on day 2, and he underwent ORIF on day 3 under CSEA.
Despite excellent intraoperative course and effective analgesia (VAS < 2), he developed acute confusion, short-term memory deficits, and disorientation within several hours postoperatively (4AT score = 5). Delirium resolved within 36 hours without pharmacological intervention, attributed to early mobilization and family presence. He was discharged on postoperative day 8 with complete cognitive recovery.
Case 4: Perioperative Delirium in Patient with Moderate Baseline Impairment
An 87-year-old female with right intertrochanteric fracture had hypertension and bilateral pneumonia. She appeared lethargic on admission, the MoCA score was 15, indicating moderate cognitive impairment. CFICB was initiated on day 2, and hemiarthroplasty under general anesthesia was performed on day 3.
Approximately two hours after ultrasound-guided CFICB placement, and prior to surgery, the patient developed worsening delirium symptoms, including sleep-wake reversal and inattention. This was confirmed by a 4AT score of 6. Postoperatively, confusion worsened but resolved by postoperative day 3 with multicomponent delirium prevention strategies. Pain control remained excellent throughout (VAS 1–3). She was discharged on postoperative day 10 to skilled nursing facility.
As this study is a descriptive case series (n = 4), no hypothesis testing or statistical inference was performed. Only descriptive statistics (eg, mean, range) were used to summarize patient characteristics.
CFICB Technique and Protocol
All CFICB procedures were performed by a single anesthesiologist with more than five years of experience in regional anesthesia, using a standardized ultrasound-guided technique. The patient was placed in the supine position with slight hip abduction. After sterile preparation and draping, a high-frequency linear ultrasound probe (6–13 MHz) was positioned parallel to the inguinal ligament, 2–3 cm medial to the anterior superior iliac spine. The fascia iliaca, iliopsoas muscle, and femoral neurovascular bundle were identified under ultrasound visualization. An 18-gauge Tuohy needle was inserted using an in-plane technique from lateral to medial. Correct needle tip position was confirmed by injecting 2–3 mL of 0.25% ropivacaine and visualizing separation of the fascial layers. After a loading dose of 40 mL of 0.25% ropivacaine, a 20-gauge catheter was advanced 3–5 cm beyond the needle tip. Catheter position was confirmed by ultrasound visualization, fluid spread, and negative aspiration. The catheter was then secured.18
Continuous infusion was initiated 2–4 hours after the loading dose using a disposable elastomeric pump. The infusion solution consisted of sufentanil 50 μg and ropivacaine 100 mg in normal saline to a total volume of 240 mL, infused at a rate of 3 mL/h, which is equivalent to ropivacaine 1.25 mg/h. The infusion continued for 48–72 hours postoperatively.
All patients received a standardized CFICB protocol and achieved good pain control (resting VAS ≤ 3) without requiring rescue opioids. Details regarding block timing, infusion formula, and pain assessment results are presented in Table 2.
 |
Table 2 CFICB Protocol and Pain Outcomes |
Pain was assessed using a 10-point VAS (0 = no pain, 10 = worst imaginable pain). Assessments were performed at rest and with movement at 6, 12, 24, 48, and 72 hours postoperatively.
Anesthesia Management
Anesthetic techniques were determined based on individual patient conditions and the anesthesiologist’s clinical judgment, with three patients undergoing CSEA and one receiving general anesthesia. Intraoperative monitoring was conducted in strict compliance with standard American Society of Anesthesiologists (ASA) guidelines. The intraoperative blood pressure management goal was to maintain mean arterial pressure ≥ 65 mmHg or a decline of no more than 20% from baseline. Vasoactive agents were administered when hypotension occurred. Intraoperative fluid management followed a goal-directed fluid therapy strategy.
Delirium Outcomes and Management
Cognitive Assessment: MoCA: Administered preoperatively (within 24 hours of admission). Scores range 0–30; interpretation: ≥ 26 normal, 18–25 mild cognitive impairment (MCI), 10–17 moderate cognitive impairment, < 10 severe cognitive impairment.19 4AT: Performed twice daily from postoperative day 0–7 by trained nurses blinded to the study hypothesis. Scores ≥ 4 indicate possible delirium; ≥ 1 indicates cognitive impairment requiring further evaluation.20
All four patients developed delirium: Case 1 on postoperative day 4, Case 2 on postoperative day 2, Case 3 within 24 hours of surgery, and Case 4 on the day of block placement (preoperatively). Details of delirium characteristics, management, and clinical outcomes are presented in Table 3. The median duration of delirium was 60 hours (range, 36–120 hours). Delirium subtypes included hyperactive (n = 1), hypoactive (n = 1), and mixed (n = 2).
 |
Table 3 Delirium Characteristics, Management, and Clinical Outcomes |
All patients received non-pharmacological interventions including frequent reorientation, early mobilization (when medically stable), circadian rhythm regulation, hearing/visual aid optimization, and family involvement. Two patients required pharmacological management.
Despite delirium occurrence, none of the patients developed complications directly attributable to CFICB (no catheter-site infection, local anesthetic toxicity, or catheter migration). All catheters were removed as planned after 2–4 days of infusion.
Discussion
This case series reports the clinical characteristics of four elderly patients with hip fracture who developed POD despite receiving CFICB with a sufentanil-containing solution. All patients achieved good pain control (resting VAS ≤ 3); however, POD still occurred, with onset ranging from the day of block placement to postoperative day 4. These findings are discussed in the context of the available literature.
The main finding of this study is the dissociation between effective analgesia and delirium prevention. All four patients in this case series achieved adequate perioperative pain control without requiring rescue opioids, consistent with evidence from previous randomized controlled trials.21,22 Nevertheless, delirium still occurred, with heterogeneous onset times and subtypes (hyperactive in one patients, hypoactive in one, and mixed in two). This observation challenges the conventional view that regional anesthesia alone can eliminate the risk of POD in high-risk elderly patients. Evidence regarding the role of CFICB in preventing POD is conflicting. While Hao et al (using an opioid-free protocol) reported that prophylactic CFICB significantly reduced the incidence of POD,17 whereas other studies have found no significant benefit. Mitchell et al reported that although CFICB improved pain control and reduced opioid consumption, the incidence of delirium was similar to that in the control group.23 Libos Zabala et al (n = 218) found no significant association between FICB and delirium.24 In the prospective observational study by Salottolo et al (n = 517), the POD rate was 5.8% in the FICB group versus 4.4% in the control group (odds ratio [OR] = 1.2, p = 0.65).25
Notably, the effect of FICB in high-risk patients appears particularly limited. Mouzopoulos et al found no significant difference between FICB and placebo in a high-risk subgroup (relative risk [RR] = 0.84, 95% confidence interval [CI]: 0.47–1.52),26 which is highly consistent with our observation that high-risk patients (advanced age, cognitive impairment, surgical delay) developed POD despite receiving CFICB. The findings of the present case series support the conclusion that the protective effect of CFICB against delirium may be context-dependent and influenced by individual patient characteristics.
Nevertheless, some studies have shown that an optimized clinical pathway including FICB significantly reduced the incidence of POD,27 suggesting that multimodal interventions may be superior to single analgesic strategies. Finch et al also noted in their review that the evidence on the preventive effect of FICB for delirium remains conflicting: a meta-analysis of seven RCTs showed benefit (pooled OR 0.46, 95% CI 0.30–0.69), whereas a large RCT found no significant difference between groups (16% vs 17%, p = 0.83)28 (Supplementary Table 1).
In this series, patient-specific factors played a dominant role. The severity and duration of delirium were closely associated with patients’ baseline characteristics rather than with analgesic efficacy.
The delayed delirium (postoperative day 4) in Case 1 (73 years, MoCA = 26) suggests a contribution from accumulative perioperative stress (eg, pain, sleep disturbance), which may have exceeded the protective capacity of CFICB.
Delirium in Case 2 (90 years, MoCA = 18, with a 6-day surgical delay and pneumonia) was the most severe and prolonged. Surgical delay represents the strongest modifiable risk factor (delay > 48 hours increases POD risk by 90%),29 and pneumonia-induced systemic inflammation may exacerbate delirium by disrupting the blood-brain barrier.30,31 Together, these factors, compounded by advanced age,32 contributed to the worst outcome in this patient.
In Case 3 (75 years, MoCA = 28), delirium occurred earliest (within 24 hours of surgery) but resolved fastest (36 hours) despite intact cognition. This pattern supports the cognitive reserve hypothesis,33 whereby preserved baseline function facilitates rapid recovery but does not prevent brief delirium triggered by acute perioperative stress.
In Case 4 (87 years, general anesthesia, MoCA = 15, pneumonia), delirium occurred on the day of block placement (preoperatively) without signs of local anesthetic systemic toxicity (LAST), suggesting that severe cognitive impairment confers hyper-susceptibility to procedural stress. This indicates that surgical stress is not the sole trigger for POD, and that preventive interventions should start earlier, ideally upon admission.14 We hypothesize that severe cognitive impairment involves baseline blood-brain barrier compromise, leading to central nervous system (CNS) hyper-reactivity to minor stimuli. Both mechanisms are potentially assessable via serum S100 calcium-binding protein β (S100β), neuron-specific enolase (NSE), or cerebrospinal fluid/serum albumin ratio (CSF/serum albumin ratio).
Laboratory evaluation revealed additional abnormalities that may have contributed to delirium. All four patients had anemia (hemoglobin 77.0–114.0 g/L), a confirmed independent risk factor for postoperative delirium.34 Cases 1 and 2 also presented with hypoalbuminemia (total protein 54.5 and 56.9 g/L) and hypocalcemia (serum calcium 2.06 and 1.17 mmol/L), both of which are recognized risk factors for delirium in elderly surgical patients.35,36 While these derangements were not uniformly present, they may have lowered the delirium threshold in patients already vulnerable due to advanced age, cognitive impairment, or infection.
A noteworthy paradoxical observation is that the delirium recovery time in Case 4 (MoCA = 15) was shorter (72 hours) than that in Case 2 (MoCA = 18, 120 hours). This may be explained by the fact that delirium in Case 4 was related to procedural stress rather than directly reflecting baseline cognitive status, whereas Case 2 had pneumonia, and systemic inflammation prolonged the course of delirium.
In summary, for patients with advanced age (≥ 85 years), cognitive impairment (MoCA < 19), or surgical delay (> 72 hours), even optimal regional analgesia may be insufficient to prevent postoperative delirium (Table 4). Notably, the presence of concomitant laboratory abnormalities, including anemia, hypoalbuminemia, and hypocalcemia, may further increase vulnerability to delirium in this population.
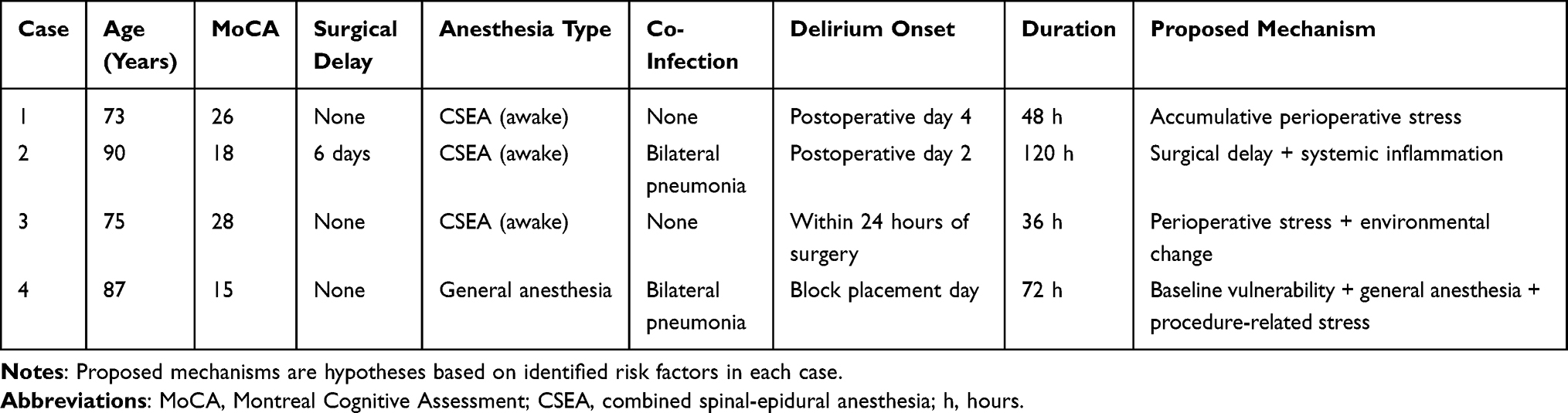 |
Table 4 Patient Characteristics and Proposed Mechanisms of Delirium |
The CFICB solution used in this study contained sufentanil (0.625 μg/h), which differs from CFICB regimens that have been shown to successfully prevent POD in the literature (typically opioid-free).17 Although low-dose sufentanil (0.2–0.5 μg/mL) has a synergistic analgesic effect,37 and was considered safe based on pharmacokinetic data suggesting limited central nervous system exposure, it may promote delirium through systemic absorption. The occurrence of delirium on the day of block placement in Case 4 supports this possibility. Therefore, the delirium observed in this series may partly reflect the systemic effects of sufentanil, which also explains why the use of opioids as adjuvants in regional blocks is generally not recommended in the literature.
The proposed mechanisms by which CFICB may prevent delirium include opioid sparing, modulation of inflammation, sleep protection, and facilitation of early mobilization.30,31,38–41 In this series, although CFICB achieved opioid sparing with no patient requiring rescue opioids, delirium still occurred. Three possible explanations are: insufficient modulation of inflammation (Cases 2 and 4 had pneumonia), uncovered mechanisms (eg, intraoperative cerebral hypoperfusion, residual anesthetics), and counteraction by sufentanil (the benefit of opioid sparing may have been partially offset by systemic absorption).
Based on the observations of this exploratory case series, we propose the following preliminary considerations that require further validation. First, surgical delay should be minimized, as the 6-day delay in Case 2 was associated with the most severe delirium; even in patients with comorbidities, surgery should proceed as early as possible or CFICB should be initiated preoperatively. Second, preoperative MoCA screening is useful for risk stratification, and patients with MoCA < 20 (Cases 2 and 4) warranted enhanced monitoring for delirium. Third, vigilance for infection is needed, as both patients with pneumonia developed severe delirium, suggesting that infection control is an important component of POD prevention. Fourth, anesthesia type should be individualized: the difference in delirium features between Case 4 (general anesthesia) and Cases 1–3 (neuraxial anesthesia) suggests that neuraxial anesthesia may be preferable to general anesthesia in patients with severe baseline cognitive impairment, though larger studies are needed. Finally, in patients with severe cognitive impairment (eg, Case 4), opioid-containing CFICB regimens should be used with caution, or non-pharmacological interventions should be initiated earlier.
This study has several limitations. First, the sample size was very small (n = 4) and the design was retrospective, precluding statistical inference and limiting the findings to exploratory observations that are not generalizable. Second, the absence of a control group makes it impossible to determine whether CFICB is superior to other analgesic regimens or whether delirium reflects failure of CFICB versus baseline patient vulnerability. Third, anesthesia type was inconsistent, with neuraxial anesthesia in Cases 1 to 3 (combined spinal-epidural anesthesia, awake) versus general anesthesia in Case 4, representing a confounder that prevents direct attribution of the observed outcomes to CFICB or sufentanil. Fourth, the opioid-containing regimen itself is a confounder, as systemic absorption of sufentanil may have contributed to delirium. Fifth, intraoperative parameters, including sedative use, blood pressure fluctuations, and anesthesia depth, were not systematically recorded; the lack of data on sedative type and dosage particularly limits precise mechanistic analysis of delirium. Finally, this was a single-center study, and the results may not be applicable to other institutions or different CFICB protocols.
Conclusion
This exploratory case series (n = 4) suggests that although opioid-containing CFICB provides effective analgesia for elderly patients with hip fracture, it does not completely prevent postoperative delirium, particularly in those with advanced age, baseline cognitive impairment, surgical delay, or concomitant infection. Given the limitations of a small sample size, absence of a control group, and inconsistent anesthesia techniques, these findings are hypothesis-generating only and require validation through prospective controlled studies.
Abbreviations
4AT, 4 ‘A’s Test for delirium; ASA, American Society of Anesthesiologists; CFICB, continuous fascia iliaca compartment block; CSEA, combined spinal-epidural anesthesia; FICB, fascia iliaca compartment block; LAST, local anesthetic systemic toxicity; MoCA, Montreal Cognitive Assessment; ORIF, open reduction and internal fixation; POD, postoperative delirium; VAS, visual analog scale.
Data Sharing Statement
All data generated or analyzed during this study are available from the corresponding author, Dr. Li Li ([email protected]), upon reasonable request.
Ethics Statement
This study was approved by the Ethics Committee of Beijing Friendship Hospital, Capital Medical University, approval number 2024-P2-169-01. All procedures performed were in accordance with the 1964 Helsinki Declaration and its later amendments. Written informed consent was obtained from all participants for their participation in the study.
Consent for Publication
Written informed consent was obtained from all patients for publication of clinical details and images. Patients were informed that they could withdraw their consent at any time prior to publication.
Acknowledgments
Lei Cao and Guoqiang Xu are co-first authors for this study. The authors thank all the medical staff who participated in treating these patients at Beijing Friendship Hospital. The authors are grateful to the patients and their families for allowing us to share these cases for educational purposes.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Adulkasem N, Chotiyarnwong P, Vanitcharoenkul E, Unnanuntana A. Ambulation recovery prediction after hip fracture surgery using the hip fracture short-term ambulation prediction tool. J Rehabil Med. 2024;56:jrm40780. doi:10.2340/jrm.v56.40780
2. van Bremen HE, Seppala LJ, Hegeman JH, van der Velde N, Willems HC, Dutch Hip Fracture Audit Group. Characteristics and outcomes of nonoperatively managed patients with hip fracture using the Dutch hip fracture audit. J Orthop Trauma. 2024;38(5):265–10. doi:10.1097/BOT.0000000000002778
3. Marcantonio ER, Flacker JM, Michaels M, Resnick NM. Delirium is independently associated with poor functional recovery after hip fracture. J Am Geriatr Soc. 2000;48(6):618–624. doi:10.1111/j.1532-5415.2000.tb04718.x
4. Jin Z, Hu J, Ma D. Postoperative delirium: perioperative assessment, risk reduction, and management. Br J Anaesth. 2020;125(4):492–504. doi:10.1016/j.bja.2020.06.063
5. Nie H, Zhao B, Zhang YQ, Jiang YH, Yang YX. Pain and cognitive dysfunction are the risk factors of delirium in elderly Hip fracture Chinese patients. Arch Gerontol Geriatr. 2012;54(2):e172–174. doi:10.1016/j.archger.2011.09.012
6. Morrison RS, Magaziner J, Gilbert M, et al. Relationship between pain and opioid analgesics on the development of delirium following hip fracture. J Gerontol a Biol Sci Med Sci. 2003;58(1):76–81. doi:10.1093/gerona/58.1.m76
7. Godwin B, Frank C, Molnar F, Dyks D, Akter R. Identification and management of opioid-induced neurotoxicity in older adults. Can Fam Physician. 2022;68(4):269–270. doi:10.46747/cfp.6804269
8. Dalens B, Vanneuville G, Tanguy A. Comparison of the fascia iliaca compartment block with the 3-in-1 block in children. Anesth Analg. 1989;69(6):705–713.
9. Hebbard P, Ivanusic J, Sha S. Ultrasound-guided supra-inguinal fascia iliaca block: a cadaveric evaluation of a novel approach. Anaesthesia. 2011;66(4):300–305. doi:10.1111/j.1365-2044.2011.06628.x
10. Marhofer P, Greher M, Kapral S. Ultrasound guidance in regional anaesthesia †. Br J Anaesth. 2005;94(1):7–17. doi:10.1093/bja/aei002
11. Sites BD, Chan VW, Neal JM, et al. The American Society of Regional Anesthesia and Pain Medicine and the European Society of Regional Anaesthesia and Pain Therapy joint committee recommendations for education and training in ultrasound-guided regional anesthesia. Reg Anesth Pain Med. 2010;35(Suppl 1):S74–80. doi:10.1097/AAP.0b013e3181d34ff5
12. Li CX, Ge WC, Yang KN, et al. Ultrasound-guided continuous fascia iliaca compartment block for perioperative pain management in elderly patients undergoing Hip fracture surgery. Zhongguo Gu Shang. 2023;36(11):1046–1051. doi:10.12200/j.issn.1003-0034.2023.11.008
13. Häusler G, van der Vet PCR, Beeres FJP, Kaufman T, Kusen JQ, Poblete B. The impact of loco-regional anaesthesia on postoperative opioid use in elderly Hip fracture patients: an observational study. Eur J Trauma Emerg Surg. 2022;48(4):2943–2952. doi:10.1007/s00068-021-01674-4
14. Garlich JM, Pujari A, Moak Z, et al. Pain management with early regional anesthesia in geriatric hip fracture patients. J Am Geriatr Soc. 2020;68(9):2043–2050. doi:10.1111/jgs.16547
15. Li Y, Gu Y, Liu W, et al. Effects of intrathecal sufentanil at different doses on postoperative pain relief and opioid consumption in elderly patients undergoing lower limb orthopedic surgery: a randomized controlled trial. J Pain Res. 2025;18:2439–2451. doi:10.2147/JPR.S512653
16. Bienert A, Moor ABD, Okuńska P, et al. Pharmacokinetics of sufentanil after epidural administration during the course of extensive abdominal surgery. Clin Pharmacokinet. 2025;64(9):1331–1340. doi:10.1007/s40262-025-01543-y
17. Hao J, Dong B, Zhang J, Luo Z. Pre-emptive analgesia with continuous fascia iliaca compartment block reduces postoperative delirium in elderly patients with Hip fracture. A randomized controlled trial. Saudi Med J. 2019;40(9):901–906. doi:10.15537/smj.2019.9.24483
18. Bhatia N. Fascia iliaca compartment block: a narrative review. Indian J Anaesth. 2026;70(1):200–204. doi:10.4103/ija.ija_1068_25
19. Nasreddine ZS, Phillips NA, Bédirian V, et al. The montreal cognitive assessment, MoCA: a brief screening tool for mild cognitive impairment. J Am Geriatr Soc. 2005;53(4):695–699. doi:10.1111/j.1532-5415.2005.53221.x
20. Bellelli G, Morandi A, Davis DHJ, et al. Validation of the 4AT, a new instrument for rapid delirium screening: a study in 234 hospitalised older people. Age Ageing. 2014;43(4):496–502. doi:10.1093/ageing/afu021
21. Gao Y, Li H, Hu H, Xu Y, Zhou J, Liu Y. Effects of continuous fascia iliaca compartment block on early quality of recovery after total hip arthroplasty in elderly patients: a randomized controlled trial. J Pain Res. 2022;15:1837–1844. doi:10.2147/JPR.S368285
22. Mostafa SF, Eid GM, Elkalla RS. Patient-controlled fascia iliaca compartment block versus fentanyl patient-controlled intravenous analgesia in patients undergoing femur fracture surgery. Egypt J Anaesth. 2018;34(1):9–13. doi:10.1016/j.egja.2017.12.002
23. Mitchell ML, Alassal S, Panza G, et al. Continuous fascia iliaca compartment block improves outcomes in hip fragility fracture patients. Cureus. 2025;17(9):e92634. doi:10.7759/cureus.92634
24. Libos Zabala A, Tihanyi Feldman J, Bernate JD, et al. Advantages of the standardized use of preoperative fascia iliaca block versus conventional analgesia in older adults with fragility Hip fracture: a retrospective cohort study at two hospitals in Colombia. Sci Prog. 2025;108(1):368504241305904. doi:10.1177/00368504241305904
25. Salottolo K, Meinig R, Fine L, et al. A multi-institutional prospective observational study to evaluate fascia iliaca compartment block (FICB) for preventing delirium in adults with Hip fracture. Trauma Surg Acute Care Open. 2022;7(1):e000904. doi:10.1136/tsaco-2022-000904
26. Mouzopoulos G, Vasiliadis G, Lasanianos N, Nikolaras G, Morakis E, Kaminaris M. Fascia iliaca block prophylaxis for Hip fracture patients at risk for delirium: a randomized placebo-controlled study. J Orthop Traumatol. 2009;10(3):127–133. doi:10.1007/s10195-009-0062-6
27. Corbella-Giménez C, Monge-Cid E, Gallo-Carrasco A, et al. Effect of an optimized clinical pathway protocol including fascia iliaca compartment block on delirium and postoperative complications in elderly hip fracture patients. J Clin Med. 2025;14(15):5284. doi:10.3390/jcm14155284
28. Finch AS, Keim SM, Bellamkonda VR, et al. Does point-of-care ultrasound-guided nerve block for geriatric hip fracture analgesia in the emergency department improve outcomes? J Emerg Med. 2026;80:81–90. doi:10.1016/j.jemermed.2025.10.014
29. Qi YM, Li YJ, Zou JH, Qiu XD, Sun J, Rui YF. Risk factors for postoperative delirium in geriatric patients with Hip fracture: a systematic review and meta-analysis. Front Aging Neurosci. 2022;14:960364. doi:10.3389/fnagi.2022.960364
30. Rudolph JL, Ramlawi B, Kuchel GA, et al. Chemokines are associated with delirium after cardiac surgery. J Gerontol Biol Sci Med Sci. 2008;63(2):184–189. doi:10.1093/gerona/63.2.184
31. Cape E, Hall RJ, van Munster BC, et al. Cerebrospinal fluid markers of neuroinflammation in delirium: a role for interleukin-1β in delirium after hip fracture. J Psychosom Res. 2014;77(3):219–225. doi:10.1016/j.jpsychores.2014.06.014
32. Wu Y, Shi Z, Wang M, et al. Different MMSE score is associated with postoperative delirium in young-old and old-old adults. PLoS One. 2015;10(10):e0139879. doi:10.1371/journal.pone.0139879
33. Stern Y. Cognitive reserve in ageing and Alzheimer’s disease. Lancet Neurol. 2012;11(11):1006–1012. doi:10.1016/S1474-4422(12)70191-6
34. Wan W, Li L, Zou Z, Chen W. Study on the predictive model of delirium risk after surgery for elderly Hip fractures based on meta-analysis. Eur Geriatr Med. 2025;16(1):245–270. doi:10.1007/s41999-024-01095-7
35. Albanese AM, Ramazani N, Greene N, Bruse L. Review of postoperative delirium in geriatric patients after hip fracture treatment. Geriatr Orthop Surg Rehabil. 2022;13:21514593211058947. doi:10.1177/21514593211058947
36. Venkatakrishnaiah NK, Anandkumar UM, Wooly S, Rajkamal G, Gadiyar HB, Janakiraman P. Identification of factors contributing to the development of postoperative delirium in geriatric patients with Hip fractures- A prospective study. J Family Med Prim Care. 2022;11(8):4785–4790. doi:10.4103/jfmpc.jfmpc_238_22
37. Thangaraju T, Kumar P, Daisy TM. Evaluation of local anaesthetic with adjuvants for postoperative analgesia through ultrasound-guided Fascia Iliaca compartment block in hip procedures. Indian J Clin Anaesthesia. 2024;11(4):538–544. doi:10.18231/j.ijca.2024.097
38. Maldonado JR. Neuropathogenesis of delirium: review of current etiologic theories and common pathways. Am J Geriatr Psychiatry. 2013;21(12):1190–1222. doi:10.1016/j.jagp.2013.09.005
39. Vaurio LE, Sands LP, Wang Y, Mullen EA, Leung JM. Postoperative delirium: the importance of pain and pain management. Anesth Analg. 2006;102(4):1267–1273. doi:10.1213/01.ane.0000199156.59226.af
40. Fadayomi AB, Ibala R, Bilotta F, Westover MB, Akeju O. A systematic review and meta-analysis examining the impact of sleep disturbance on postoperative delirium. Crit Care Med. 2018;46(12):e1204–e1212. doi:10.1097/CCM.0000000000003400
41. Schweickert WD, Pohlman MC, Pohlman AS, et al. Early physical and occupational therapy in mechanically ventilated, critically ill patients: a randomised controlled trial. Lancet. 2009;373(9678):1874–1882. doi:10.1016/S0140-6736(09)60658-9
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.