Back to Journals » OncoTargets and Therapy » Volume 11
Postoperative adjuvant chemo (embolization) therapy for hepatocellular carcinoma with portal vein tumor thrombosis
Authors Zhang YF ![]() , Shang H, Zeng XL, Ji H, Li YM, Lu HW
, Shang H, Zeng XL, Ji H, Li YM, Lu HW
Received 19 April 2018
Accepted for publication 9 July 2018
Published 3 September 2018 Volume 2018:11 Pages 5407—5417
DOI https://doi.org/10.2147/OTT.S171612
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr William C. Cho
Ya-Fei Zhang,1 Hao Shang,1 Xian-Ling Zeng,2 Hong Ji,1 Yi-Ming Li,1 Hong-Wei Lu1
1Department of General Surgery, The Second Affiliated Hospital of Xi’an Jiaotong University, Xi’an, Shaanxi, China; 2Department of Obstetrics and Gynecology, The First Affiliated Hospital of Xi’an Jiaotong University, Xi’an, Shaanxi, China
Background: The present meta-analysis was aimed to evaluate the effects of postoperative adjuvant chemotherapy/transarterial chemoembolization (TACE) on the survival/disease-free survival (DFS) rate in hepatocellular carcinoma (HCC) patients with portal vein tumor thrombosis (PVTT).
Methods: The relevant trials were collected using a database search of MEDLINE, Embase, Cochrane Library, Web of Science, ScienceDirect, the China Journal Full-text Database, and the National Institute of Health Clinical Trials Database. The 1-, 3-, and 5-year survival/DFS rates were considered to be the primary end points. A sensitivity analysis was conducted by reanalyzing the data using different statistical approaches.
Results: Eight studies met the inclusion criteria. When compared with surgery alone, the pooled OR showed that the postoperative adjuvant therapy significantly increased the 1-, 3-, and 5-year survival rates for HCC patients with PVTT (the pooled OR and 95% CI of the 1-, 3-, and 5-year survival rates, respectively, were as follows: 2.72, 1.98–3.74; 1.62, 1.13–2.33; 1.99, 1.20–3.29). In addition, when compared with surgery alone, subgroup analysis showed that the postoperative chemotherapy improved the 1-, 3-, and 5-year survival rates of HCC patients with PVTT.
Conclusion: Compared with surgery alone, postoperative adjuvant chemotherapy can improve the 1-, 3- and 5-year survival rates of HCC patients with PVTT. However, postoperative TACE can only increase the 1-year survival rate. However, due to the limitations of this meta-analysis, additional relevant trials are required to confirm these findings.
Keywords: hepatocellular carcinoma, portal vein tumor thrombosis, meta-analysis, transarterial chemoembolization, survival rate, postoperative, chemotherapy
Background
Hepatocellular carcinoma (HCC) is the fifth most common neoplasm and the second most frequent cause of cancer mortality worldwide.1,2 Globally, over 700,000 new cases are diagnosed every year, with an age-related incidence of 16 cases per 100,000 persons.3 Regarding advanced HCC, portal vein tumor thrombosis (PVTT) has been found in a substantial percentage of HCC patients who are alive and in up to 44% in HCC patients who died.4 HCC patients with PVTT have generally very poor prognosis when the treatment is delayed (median survival time: 2.7–4.0 months).5 According to Barcelona Clinic Liver Cancer (BCLC) staging system, HCC patients with PVTT are classified as BCLC stage C with various treatment options, such as chemotherapy, transarterial chemoembolization (TACE), molecular-targeted therapy, surgical resection, and liver transplantation.6 Although sorafenib target therapy is recommended to be the first-line treatment for BCLC criteria, operative resection and liver transplantation are still considered to be curative options.7,8 The efficacy of postoperative sorafenib vs surgery/sorafenib therapy has not been evaluated until now. The limited number of trials using sorafenib suggests that only descriptive analyses can be performed. Thus, additional trials are needed to assess the efficacy of postoperative sorafenib therapy and to compare the efficacy between adjuvant TACE/chemotherapy and sorafenib.
In recent years, the benefit of postoperative TACE and transarterial embolization has been confirmed in non-advanced HCC cases.9–14 In addition, a meta-analysis confirmed that postoperative TACE is a potential option for the curative resection of HCC with a mean tumor size larger than 5 cm.15 Furthermore, some literature sources have reported that multimodality treatment can prolong the survival rate of HCC patients with PVTT.16–26 The multimodality treatment includes postoperative hepatic artery infusion (HAI), portal vein chemotherapy/chemobiotherapy (PVC), and TACE. Nevertheless, the efficacy of the treatment methods mentioned above remains controversial. Due to potential increased risk of liver failure caused by TACE and chemotherapy, only a few literature sources have evaluated the efficacy and safety of TACE compared with other treatments in HCC patients with PVTT.18–26 This meta-analysis was aimed to evaluate the effects of postoperative adjuvant chemotherapy/TACE on survival time in HCC patients with PVTT.
Methods
Search strategy and selection criteria
We identified the studies by searching MEDLINE, Embase, Cochrane Library (CENTRAL) databases, Web of Science, ScienceDirect, the China Journal Full-text Database, and the National Institute of Health Clinical Trials Database (www.ClinicalTrials.gov) with the following keywords: “hepatocellular carcinoma” or “HCC” or “hepatic tumor” or “hepatic cancer” or “liver cancer” and “PVTT” or “portal vein tumor thrombi” or “portal vein tumor thrombosis” and “chemotherapy” and “TACE” or “chemoembolization” or “embolization” and “clinical trials” in the English language and in non-English languages (limits of the search period: from January 1990 to October 2014). The references of the retrieved literature were also screened. The search strategies are shown in Figure 1.
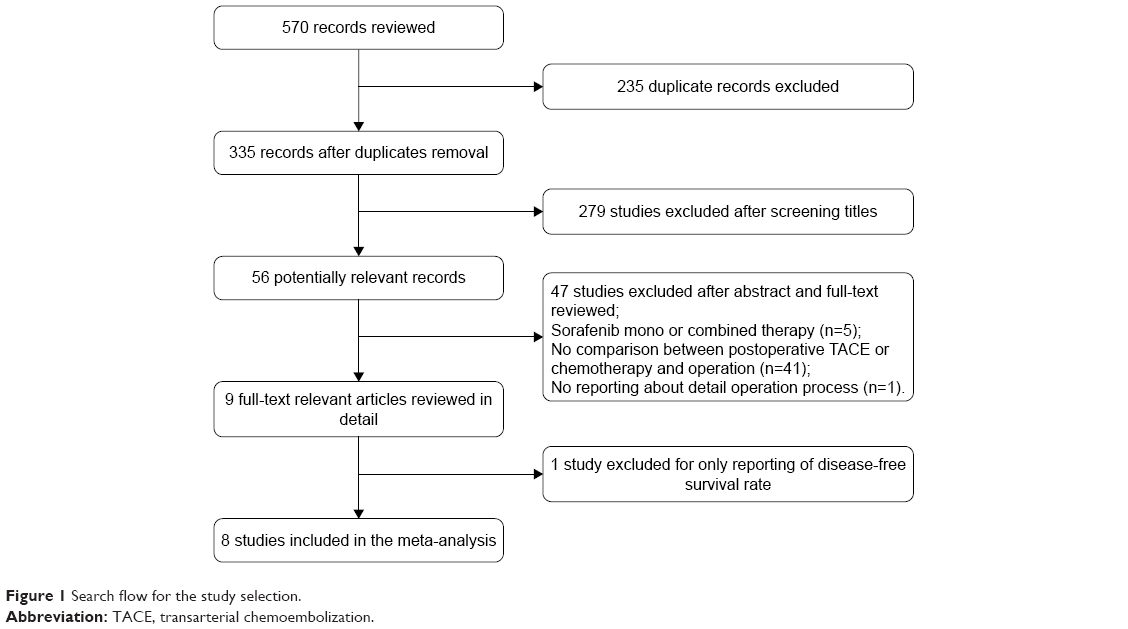 | Figure 1 Search flow for the study selection. |
The inclusion criteria were as follows:
- Trials: both randomized controlled studies (RCTs) and retrospective studies
- Patients: diagnosed with HCC with PVTT and without sex and age limits
- Interventions: postoperative adjuvant chemotherapy/TACE plus surgery vs surgery alone
- Chemotherapy: HAI and PVC
- Surgery: both hepatectomy and PVTT removal were conducted
- Follow-up: data available on the 1-, 3-, or 5-year survival rates and/or DFS rates
The exclusion criteria were as follows:
- Studies that included cholangiocellular carcinoma patients
- Studies that did not conduct PVTT removal
- Studies that involved duplicative publication
- Studies that did not report the 1-, 3-, or 5-year overall survival (OS) rates and/or DFS rates.
Data extraction and quality assessment
Two authors (Shang H and Zhang YF) independently extracted information and data from the studies including the author’s first name, year of publication, study methods, patient’s characteristics, interventions, and 1-, 3-, and 5-year OS rates (Table 1). Disagreements were resolved by consensus.
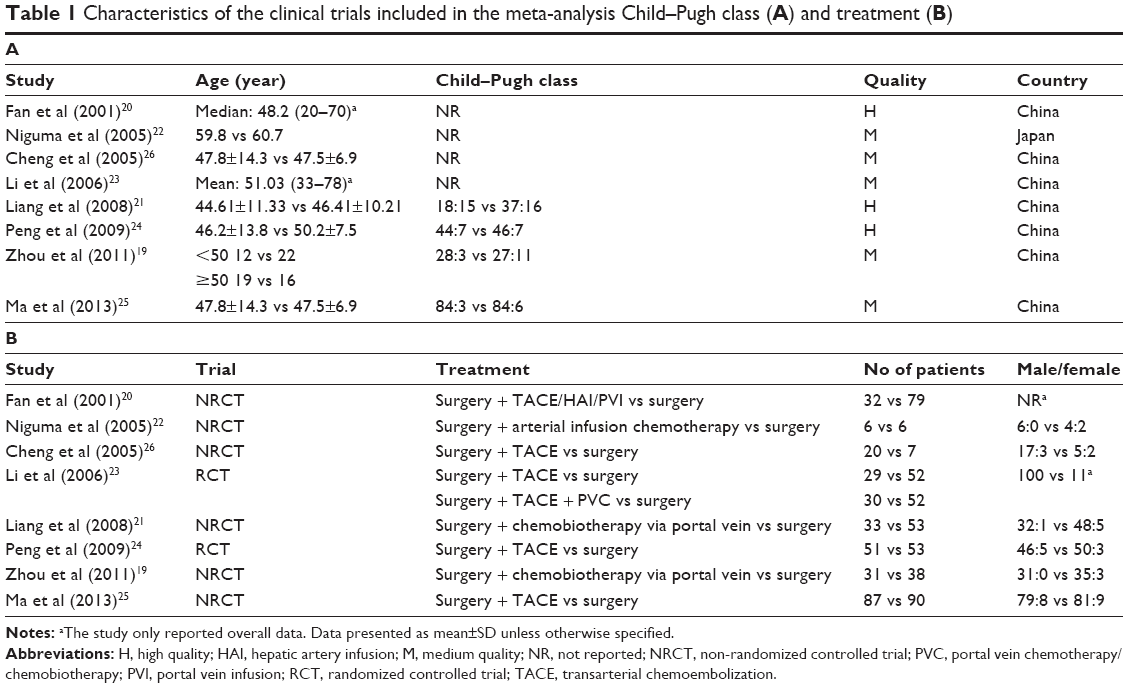 | Table 1 Characteristics of the clinical trials included in the meta-analysis Child–Pugh class (A) and treatment (B) |
Furthermore, we evaluated the methodological quality of each RCT according to the method described in the Cochrane Handbook for Systematic Reviews of Interventions.27 Random sequence generation, allocation concealment, blinding (patients, personnel, and outcomes assessment), incomplete outcome data, selective reporting, and whether the analysis referred to intention-to-treat were assessed to examine all of the included RCTs and were assigned values of “low risk”, “high risk”, or “unclear” (Figure 2). This five-point quality scale includes points for randomization (0–2 points), double blinding (0–2 points), and withdrawals and dropouts (0–1 point). Total scores of 0–2 indicated low quality, whereas studies with total scores ≥3 were defined as high quality. However, the quality of each retrospective study was assessed by the Newcastle–Ottawa Quality Assessment Scale, and studies were classified as high quality if they received more than seven stars, medium quality if they received between four and six stars, and poor quality if they received fewer than four stars (Table 2).
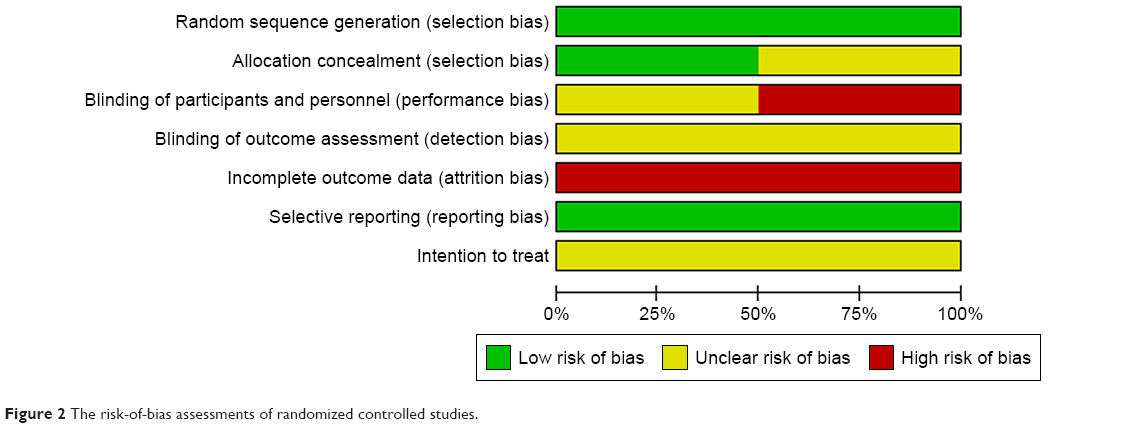 | Figure 2 The risk-of-bias assessments of randomized controlled studies. |
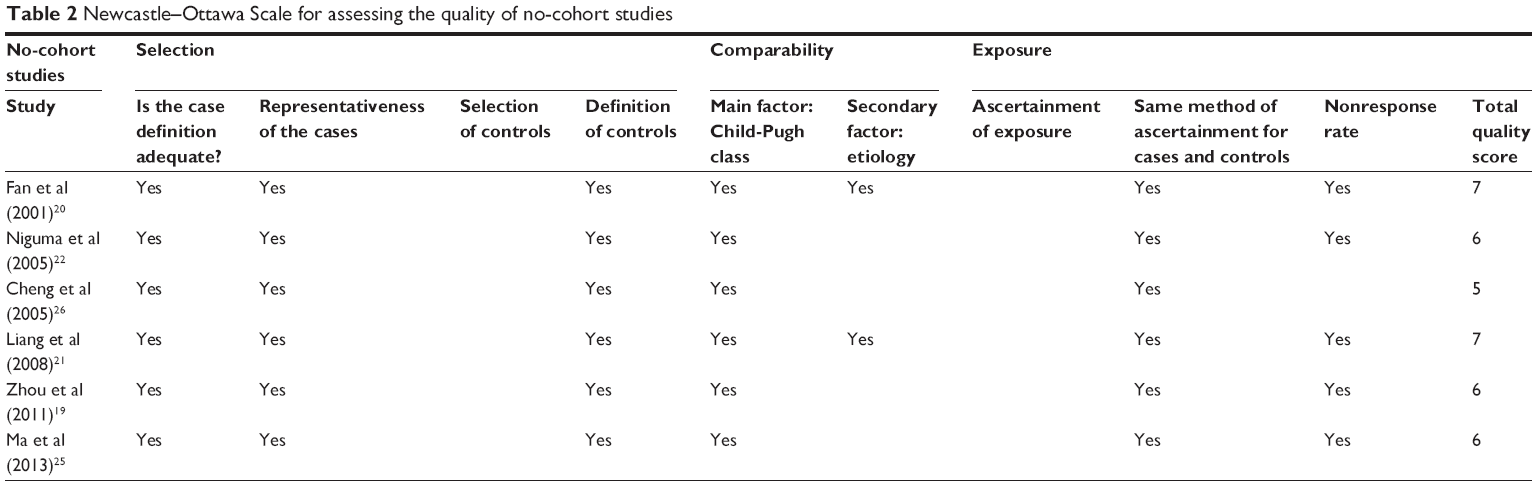 | Table 2 Newcastle–Ottawa Scale for assessing the quality of no-cohort studies |
Statistical analysis
The effects of the treatment options were evaluated by the 1-, 3-, and 5-year survival rates using the ORs with 95% CIs. The 1-, 3-, and 5-year survival rates were considered the primary end points. The homogeneity of the included trials was analyzed by the chi-squared test with Cochran’s Q statistic and I2 (statistical significance set at P>0.1 or I2<50%). The Mantel–Haenszel method with a fixed-effects model was used to analyze the pooled data when the homogeneity was significant. However, when heterogeneity between trials was observed, then instead of determining the causes of the heterogeneity, a random-effects model was used to analyze the data. Sensitivity analyses were performed to determine the stability of the overall treatment effects. The point estimate of the OR was used to assess the statistical significance of the outcomes (statistical significance was set at P<0.05 if the 95% CI did not include the value 1). The analyses of the data were performed using Review Manager, version 5.2 (The Cochrane Collaboration, Software Update, Oxford, UK).
Results
Eligible studies
The search strategies and processes are shown in Figure 1. Fifty-six potentially relevant records were identified, of which 47 studies were excluded after the abstract and full-text review for the following reasons: mono or combined sorafenib treatment was included (n=5), no comparison between postoperative TACE/chemotherapy and surgery (n=41), and no reporting about the details of the surgical procedure (n=1). Finally, only one study with a reported DFS rate was excluded that could not be subjected to a meta-analysis.18 A total of eight studies involving 697 patients were included to compare surgery plus postoperative adjuvant chemotherapy/TACE with surgery alone. Only these eight studies reported the OS rates.19–26 In addition, three articles that were reported in the Chinese language were retrieved using Web of Science and were included in the meta-analysis after evaluating the quality. The data of an article included both postoperative TACE and chemotherapy (we marked Li et al1 for TACE and Li et al2 for chemotherapy).23 Postoperative adjuvant chemotherapy included the following: HAI and PVC. The operative methods used in the included trials were hepatectomy and PVTT removal. The drugs, courses, and dosages of chemotherapy and TACE are listed in Table 3. Of the eight studies included, three articles reported 1-, 3-, and 5-year survival rates;20,23,24 three articles reported 1- and 3-year survival rates;19,21,25 and two articles reported only the 1-year survival rate.22,26 The characteristics of the included studies are shown in Table 1.
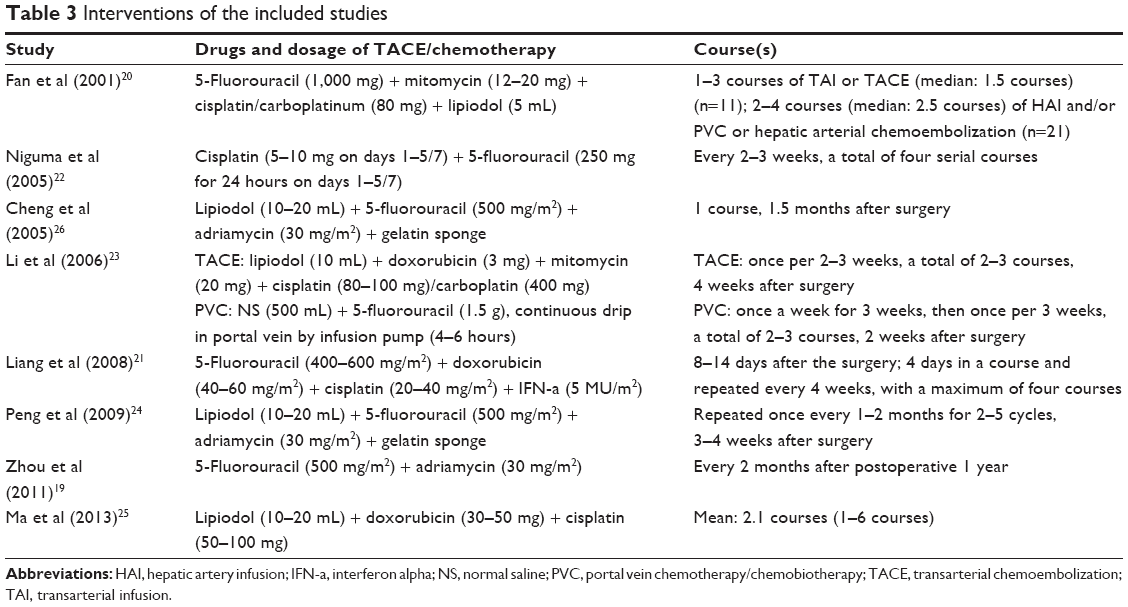 | Table 3 Interventions of the included studies |
Methodological quality of the included studies
The quality of each included study is shown in Table 1. The methodological quality of each included study was evaluated by the previously introduced principles. Three trials were considered to be of high quality, and five trials were considered to be of medium quality (Table 2). No signs of selective reporting were observed, and all of the trials did not state the intention-to-treat principle clearly.
Meta-analysis of the 1-, 3-, and 5-year survival rates
All of the eight included trials provided the 1-year survival rate. There was significant homogeneity among the eight studies (I2=0%, P=0.81), and a fixed-effects model was used to analyze the data. The pooled OR (2.72, 95% CI=1.98–3.74) showed a significantly increased 1-year survival rate for HCC patients with PVTT following postoperative adjuvant chemotherapy/TACE compared with surgery alone (P<0.00001). Similarly, six trials reported the 3-year survival rate and three trials reported the 5-year survival rate. Their pooled ORs calculated using the fixed-effect model showed a significantly increased 3- and 5-year survival rates for HCC patients with PVTT following postoperative adjuvant chemotherapy/TACE compared with surgery alone (P=0.009 and P=0.007, respectively), and the homogeneity was significant (3-year survival rate: pooled OR=1.62, 95% CI=1.13–2.33, I2=0%, P=0.69; 5-year survival rate: pooled OR=1.99, 95% CI=1.20–3.29, I2=0%, P=0.64) (Figure 3).
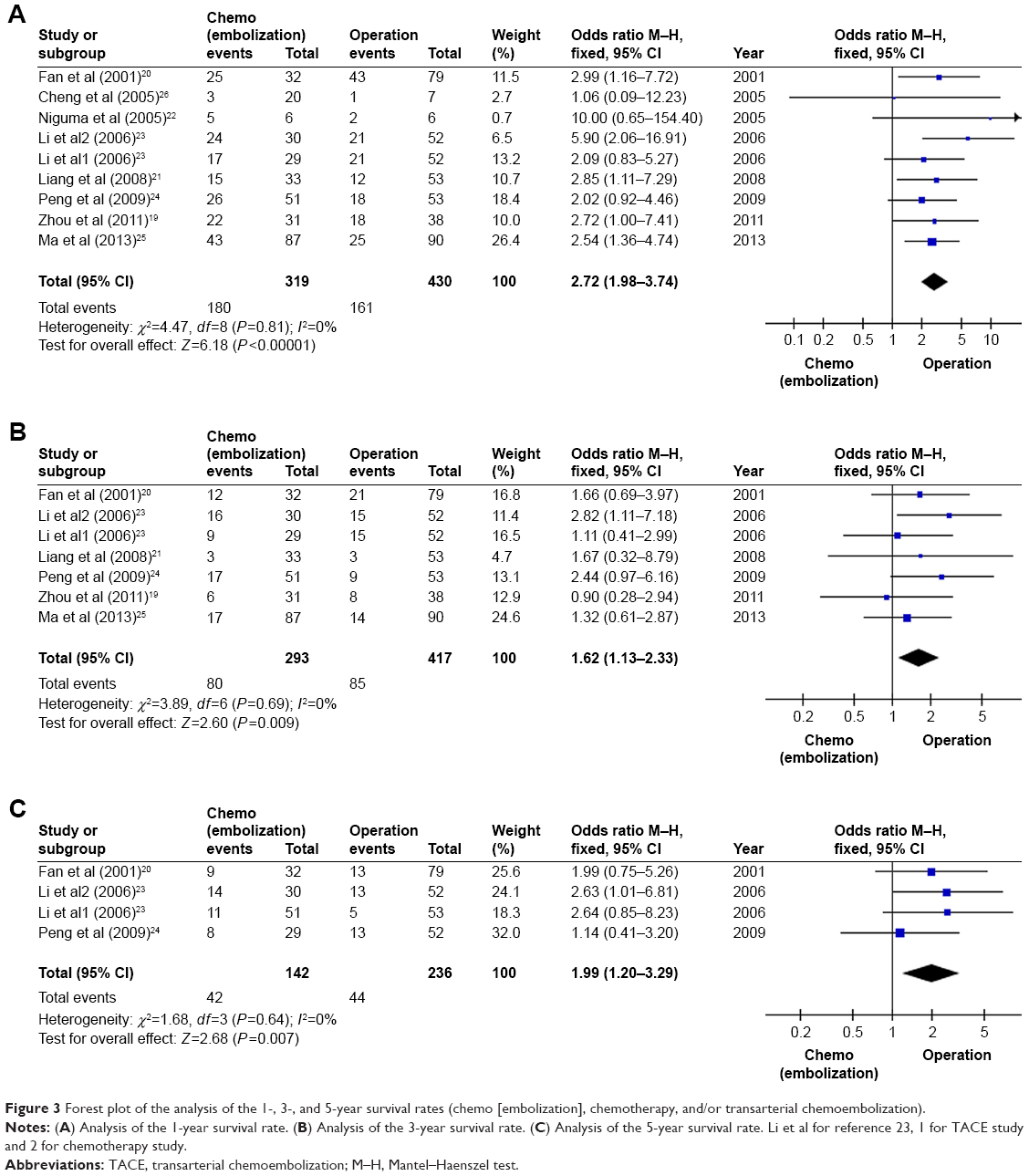 | Figure 3 Forest plot of the analysis of the 1-, 3-, and 5-year survival rates (chemo [embolization], chemotherapy, and/or transarterial chemoembolization). |
Subgroup analysis
A total of four trials reported the 1-year survival rate, which was compared between postoperative TACE and surgery alone for HCC patients with PVTT. Additionally, three trials reported the 3-year survival rate and two trials reported the 5-year survival rate. There was significant homogeneity among them, and fixed-effect models were used to analyze the data. The pooled OR calculated by the fixed-effect model indicated that postoperative adjuvant TACE significantly increased the 1-year survival rate compared with surgery alone for HCC patients with PVTT. However, the pooled OR of postoperative TACE regarding the 3- and 5-year survival rates showed that there were no statistical significances between postoperative TACE and surgery alone for HCC patients with PVTT because the 95% CI included the value 1 (Figure 4).
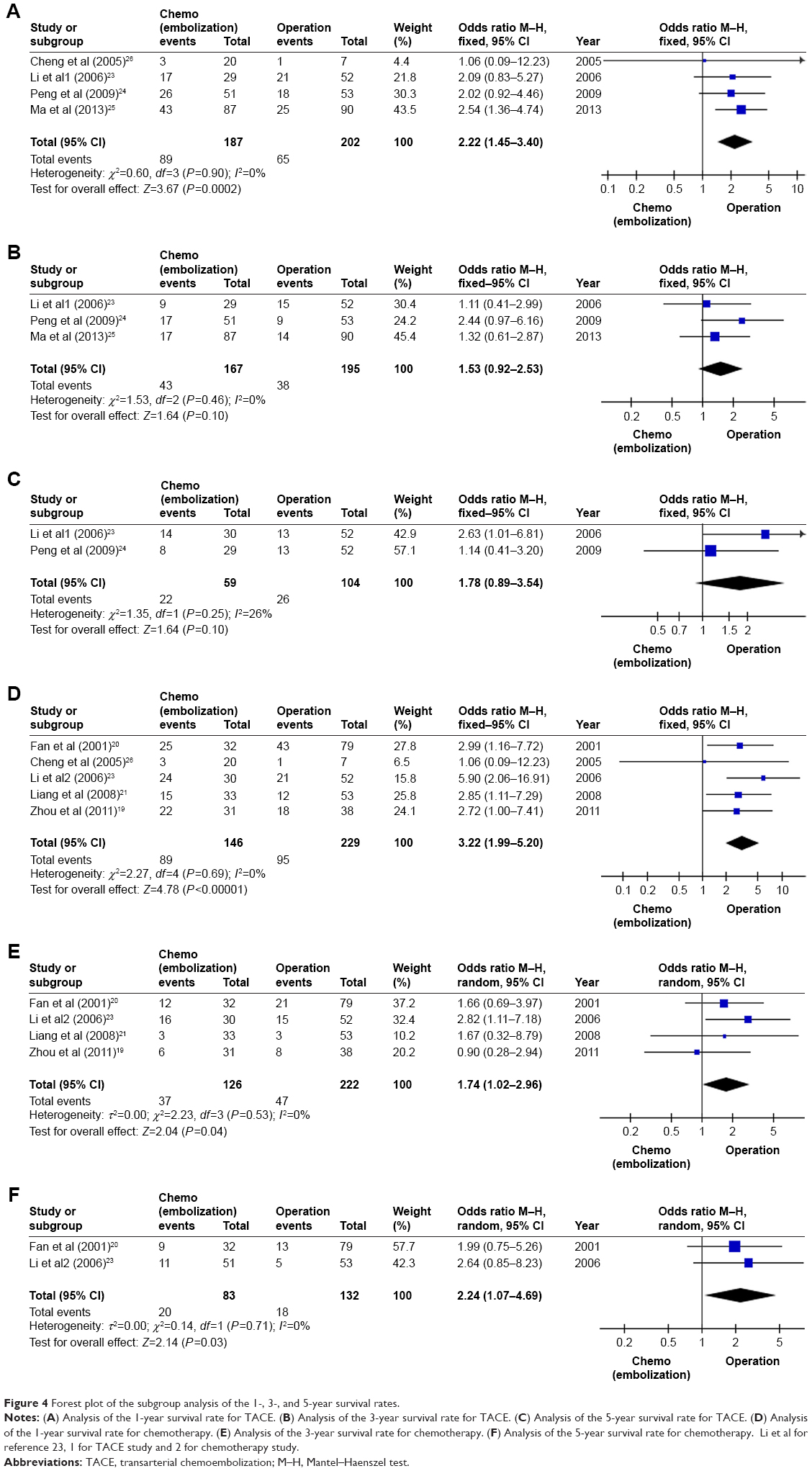 | Figure 4 Forest plot of the subgroup analysis of the 1-, 3-, and 5-year survival rates. |
Regarding postoperative adjuvant chemotherapy, the pooled ORs of the 1-, 3-, and 5-year survival rates indicated that postoperative adjuvant chemotherapy could significantly increase 1-, 3-, and 5-year survival rates compared with surgery alone for HCC patients with PVTT (1-year survival rate: pooled OR=3.22, 95% CI=1.99–5.20, I2=0%, P=0.69; 3-year survival rate: pooled OR=1.74, 95% CI=1.02–2.96, I2=0%, P=0.53; 5-year survival rate: pooled OR=2.24, 95% CI=1.07–4.69, I2=0%, P=0.71) (Figure 4).
Sensitivity analysis
Sensitivity analysis was performed using the fixed-effects model and random-effects model for the quality of the included studies and the effects of postoperative adjuvant chemotherapy/TACE and subgroup analysis. The change of the effects model did not result in the statistical significance of the pooled OR, indicating that the meta-analysis had good reliability.
Discussion
From 1990 to 2013, liver cancer ranked 21st among the leading causes of death worldwide. Furthermore, death due to liver cancer in all ages has increased from 510.1/1,000 to 818.0/1,000, and the age-standardized death rate has decreased from 13.7/100,000 to 13.0/100,000.28 All of the above indicate that, although the morbidity of liver cancer has been younger, the efficacy of the treatment has improved. Based on the BCLC staging system, HCC patients with PVTT are classified as BCLC stage C.6 The recommended treatment is sorafenib therapy. However, some studies have shown that hepatic arterial infusion chemotherapy (HAIC), radiotherapy (RT), TACE + RT, and sorafenib + TACE + RT can be an alternative treatment to sorafenib therapy in HCC patients with PVTT.18,29–33 In addition, an article reports that TACE–sorafenib combination treatment may improve OS in HCC patients with PVTT compared with patients who underwent TACE alone.34 Although the above-mentioned treatments have achieved satisfactory efficacy, operative resection and liver transplantation are still considered to be the curative options.7 Moreover, one case report indicates that sorafenib therapy combined with intermittent cisplatin HAIC is considered to be an effective therapy for advanced HCC with PVTT in the major trunk.35 Additionally, another case report involving two cases showed that preoperative sorafenib treatment provides an opportunity for HCC patients with PVTT to have curative resection.36 However, the efficacy of postoperative sorafenib therapy vs surgery/sorafenib therapy has not been evaluated until now. The limited number of trials concerning sorafenib suggests that we can only perform a descriptive analysis. Thus, additional trials are needed to assess the efficacy of postoperative sorafenib therapy and to compare the efficacy between adjuvant TACE/chemotherapy and sorafenib therapy.
Although there are various treatment options, the prognosis of HCC patients with PVTT remains very poor. This meta-analysis aimed to evaluate the effects of postoperative adjuvant chemotherapy and/or TACE on the survival time in HCC patients with PVTT. We systematically searched the main databases (MEDLINE, Embase, Cochrane Library [CENTRAL], Web of Science, ScienceDirect, the China Journal Full-text Database, and the National Institute of Health Clinical Trials Database), and eight studies were included in our meta-analysis. All of the included studies fulfilled the inclusion criteria: RCT or retrospective study; patients were diagnosed with HCC with PVTT and without sex and age limits; postoperative adjuvant chemotherapy/TACE plus surgery vs surgery alone was performed; both hepatectomy and PVTT removal were conducted; and data available on the 1-, 3-, or 5-year survival rates and/or DFS rates. For the statistical homogeneity of the included studies, outcomes were analyzed using the fixed-effects model. The fixed-effects model was used to analyze sensitivity and the random-effects model was used to evaluate the reliability of the meta-analysis. This meta-analysis indicated that postoperative adjuvant therapy showed improvement in the 1-year survival rate when compared to surgery alone. Similarly, benefits of the 3- and 5-year survival rates were also found (1-year survival rate: pooled OR=2.72, 95% CI=1.98–3.74, I2=0%, P=0.81; 3-year survival rate: pooled OR=1.62, 95% CI=1.13–2.33, I2=0%, P=0.69; 5-year survival rate: pooled OR=1.99, 95% CI=1.20–3.29, I2=0%, P=0.64). In subgroup analysis, the meta-analysis indicated that postoperative chemotherapy could increase the 1-, 3-, and 5-year survival rates compared with surgery alone for HCC patients with PVTT. However, postoperative TACE could only improve the 1-year survival rate, and no statistical significance was found in the improvement of the 3- and 5-year survival rates compared with surgery alone for HCC patients with PVTT. The results are partly consistent with a previous study.15 It was found that postoperative TACE could significantly improve the DFS and OS compared with surgery alone when the mean tumor size was bigger than 5 cm. However, the study failed to group OS by time.
Furthermore, of the included studies, Fan et al’s study evaluated the differences among different treatments in HCC patients with PVTT in the first branch and main trunk tumor thrombosis groups.20 The outcomes reported that postoperative TACE and chemotherapy showed better 1-, 3-, and 5-year survival rates than the others in both the first branch tumor thrombosis group and main trunk tumor thrombosis group. Additionally, with the same treatment, the outcomes indicated that the first branch tumor thrombosis group had better 1-, 3-, and 5-year survival rates than the main trunk tumor thrombosis group. Furthermore, in the study by Li et al,23 the 1-, 3-, and 5-year DFS rates in the surgery group were 50.7%, 17.8%, and 0% vs 62.3%, 23.7%, and 4.0% in the postoperative TACE group, respectively, indicating that postoperative TACE could increase the 1-, 3-, and 5-year DFS rates. These findings could guide the surgical method and subsequent treatment options for the different tumor thrombosis types in HCC patients with PVTT.
However, although TACE and chemotherapy can improve the survival of HCC patients with PVTT, the mild and severe adverse events should also be considered. The adverse events of TACE included the following: ascites, transient liver failure, deterioration of liver function, progression of tumor or metastases before surgery, bacteremia, and bleeding from the femoral puncture site.23,24 The adverse events of chemotherapy included nausea, loss of appetite, leukopenia, alopecia, drug fever, and deterioration of liver or renal function.20–22 All of the mild adverse events were common and easily resolved. However, although the severe adverse events were rare, they should be considered and treated well.
Finally, the limitations of this meta-analysis were analyzed. First, only two RCTs were analyzed, which possibly caused selection bias (Figure 2). Second, due to the lack of relevant studies, the conclusions of the subgroup analysis of postoperative TACE and postoperative chemotherapy were limited. Third, only three high-quality articles were included. Fourth, all of the included studies were from Asia. Therefore, more clinical trials and more relevant studies from different countries are needed to provide additional evidence to support the meta-analysis. Due to the limitations above, the outcomes and conclusion of the present meta-analysis should be interpreted cautiously. However, in the present study the effects of postoperative adjuvant chemotherapy/TACE on survival time in HCC patients with PVTT are evaluated and a valuable conclusion is drawn, which provided a good guiding principle for clinical application.
Conclusion
Our meta-analysis showed that postoperative adjuvant therapy could increase the 1-, 3-, and 5-year survival rates of HCC patients with PVTT. In subgroup analysis, postoperative chemotherapy can improve the 1-, 3-, and 5-year survival rates of HCC patients with PVTT vs surgery alone. Postoperative TACE can only increase the 1-year survival rate, and no statistical significance was found in the improvement of the 3- and 5-year survival rates compared with surgery alone for HCC patients with PVTT. However, due to the limitations of this meta-analysis, more relevant RCTs from different countries are required to further confirm these findings. Meanwhile, a subgroup analysis of postoperative TACE and postoperative chemotherapy should be performed. Based on the BCLC staging system, the efficacy between adjuvant TACE/chemotherapy and sorafenib should be compared to provide evidence of the clinical options.
Acknowledgment
This study was funded by the National Natural Science Foundation of China (grant no 81170454).
Disclosure
The authors report no conflicts of interest in this work.
References
Parkin DM, Bray F, Ferlay J, Pisani P. Estimating the world cancer burden: Globocan 2000. Int J Cancer. 2001;94(2):153–156. | ||
Jemal A, Bray F, Center MM, Ferlay J, Ward E, Forman D. Global cancer statistics. CA Cancer J Clin. 2011;61(2):69–90. | ||
Ferlay J, Shin HR, Bray F, Forman D, Mathers C, Parkin DM. Estimates of worldwide burden of cancer in 2008: GLOBOCAN 2008. Int J Cancer. 2010;127(12):2893–2917. | ||
Pirisi M, Avellini C, Fabris C, et al. Portal vein thrombosis in hepatocellular carcinoma: age and sex distribution in an autopsy study. J Cancer Res Clin Oncol. 1998;124(7):397–400. | ||
Minagawa M, Makuuchi M. Treatment of hepatocellular carcinoma accompanied by portal vein tumor thrombus. World J Gastroenterol. 2006;12(47):7561–7567. | ||
Forner A, Reig ME, de Lope CR, Bruix J. Current strategy for staging and treatment: the BCLC update and future prospects. Semin Liver Dis. 2010;30(1):061–074. | ||
Llovet JM, Ricci S, Mazzaferro V, et al. Sorafenib in advanced hepatocellular carcinoma. N Engl J Med. 2008;359(4):378–390. | ||
Fan ST, Lo CM, Liu CL, et al. Hepatectomy for hepatocellular carcinoma: toward zero hospital deaths. Ann Surg. 1999;229(3):322–330. | ||
Izumi R, Shimizu K, Iyobe T, et al. Postoperative adjuvant hepatic arterial infusion of Lipiodol containing anticancer drugs in patients with hepatocellular carcinoma. Hepatology. 1994;20(2):295–301. | ||
Li JQ, Zhang YQ, Zhang WZ, Yuan YF, Li GH. Randomized study of chemoembolization as an adjuvant therapy for primary liver carcinoma after hepatectomy. J Cancer Res Clin Oncol. 1995;121(6):364–366. | ||
Tacher V, Lin M, Bhagat N, et al. Dual-phase cone-beam computed tomography to see, reach, and treat hepatocellular carcinoma during drug-eluting beads transarterial chemo-embolization. J Vis Exp. 2013;82(82):50795. | ||
Zhong C, Guo RP, Li JQ, et al. A randomized controlled trial of hepatectomy with adjuvant transcatheter arterial chemoembolization versus hepatectomy alone for Stage III A hepatocellular carcinoma. J Cancer Res Clin Oncol. 2009;135(10):1437–1445. | ||
Li Q, Wang J, Sun Y, et al. Postoperative transhepatic arterial chemoembolization and portal vein chemotherapy for patients with hepatocellular carcinoma: a randomized study with 131 cases. Dig Surg. 2006;23(4):235–240. | ||
Jiang JH, Guo Z, Lu HF, et al. Adjuvant transarterial chemoembolization after curative resection of hepatocellular carcinoma: propensity score analysis. World J Gastroenterol. 2015;21(15):4627–4634. | ||
Cheng X, Sun P, Hu QG, Song ZF, Xiong J, Zheng QC. Transarterial (chemo)embolization for curative resection of hepatocellular carcinoma: a systematic review and meta-analyses. J Cancer Res Clin Oncol. 2014;140(7):1159–1170. | ||
Li Y, Zheng Y-B, Zhao W, et al. Sorafenib in combination with transarterial chemoembolization and radiofrequency ablation in the treatment for unresectable hepatocellular carcinoma. Med Oncol. 2013;30(4):730. | ||
Yang M, Fang Z, Yan Z, et al. Transarterial chemoembolisation (TACE) combined with endovascular implantation of an iodine-125 seed strand for the treatment of hepatocellular carcinoma with portal vein tumour thrombosis versus TACE alone: a two-arm, randomised clinical trial. J Cancer Res Clin Oncol. 2014;140(2):211–219. | ||
Song DS, Song MJ, Bae SH, et al. A comparative study between sorafenib and hepatic arterial infusion chemotherapy for advanced hepatocellular carcinoma with portal vein tumor thrombosis. J Gastroenterol. 2015;50(4):445–454. | ||
Zhou Q, Wang Y, Zhou X, et al. Prognostic analysis for treatment modalities in hepatocellular carcinomas with portal vein tumor thrombi. Asian Pac J Cancer Prev. 2011;12(11):2847–2850. | ||
Fan J, Wu ZQ, Tang ZY, et al. Multimodality treatment in hepatocellular carcinoma patients with tumor thrombi in portal vein. World J Gastroenterol. 2001;7(1):28–32. | ||
Liang LJ, Hu WJ, Yin XY, et al. Adjuvant intraportal venous chemotherapy for patients with hepatocellular carcinoma and portal vein tumor thrombi following hepatectomy plus portal thrombectomy. World J Surg. 2008;32(4):627–631. | ||
Niguma T, Mimura T, Tutui N. Adjuvant arterial infusion chemotherapy after resection of hepatocellular carcinoma with portal thrombosis: a pilot study. J Hepatobiliary Pancreat Surg. 2005;12(3):249–253. | ||
Li Q, Wang J, Sun Y, et al. Efficacy of postoperative transarterial chemoembolization and portal vein chemotherapy for patients with hepatocellular carcinoma complicated by portal vein tumor thrombosis – a randomized study. World J Surg. 2006;30(11):2004–2011; discussion 2012–2003. | ||
Peng BG, He Q, Li JP, Zhou F. Adjuvant transcatheter arterial chemoembolization improves efficacy of hepatectomy for patients with hepatocellular carcinoma and portal vein tumor thrombus. Am J Surg. 2009;198(3):313–318. | ||
Ma L, Jz Y, Xiang BD, Fx W, Zhao YN, Lq L. Impact of treatment strategies on patients with hepatocellular carcinoma of less than 10 cm but with portal vein tumor thrombus. Chin J Hepatobiliary Surg. 2013;3(19):165–170. | ||
Cheng SQ, Wu MC, Chen H, et al. Hepatocellular carcinoma with tumor thrombi in the portal vein. A comparison of therapeutic effects by different treatments. Zhonghua Zhong Liu Za Zhi. 2005;27(3):183–185. | ||
Higgins J, Green S. Cochrane Handbook for Systematic Reviews of Interventions. Hoboken: Wiley; 2010. | ||
Naghavi M, Wang HD, Lozano R. GBD 2013 Mortality and Causes of Death Collaborators. Global, regional, and national age-sex specific all-cause and cause-specific mortality for 240 causes of death, 1990–2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet. 2015;385(9963):117–171. | ||
Nakazawa T, Hidaka H, Shibuya A, et al. Overall survival in response to sorafenib versus radiotherapy in unresectable hepatocellular carcinoma with major portal vein tumor thrombosis: propensity score analysis. BMC Gastroenterol. 2014;14:84. | ||
Cho JY, Paik YH, Park HC, et al. The feasibility of combined transcatheter arterial chemoembolization and radiotherapy for advanced hepatocellular carcinoma. Liver Int. 2014;34(5):795–801. | ||
Li Y, Zheng YB, Zhao W, et al. Sorafenib in combination with transarterial chemoembolization and radiofrequency ablation in the treatment for unresectable hepatocellular carcinoma. Med Oncol. 2013;30(4):730. | ||
Yeh SA, Chen YS, Perng DS. The role of radiotherapy in the treatment of hepatocellular carcinoma with portal vein tumor thrombus. J Radiat Res. 2015;56(2):325–331. | ||
Yamada R, Sato M, Kawabata M, Nakatsuka H, Nakamura K, Takashima S. Hepatic artery embolization in 120 patients with unresectable hepatoma. Radiology. 1983;148(2):397–401. | ||
Zhu K, Chen J, Lai L, et al. Hepatocellular carcinoma with portal vein tumor thrombus: treatment with transarterial chemoembolization combined with sorafenib – a retrospective controlled study. Radiology. 2014;272(1):284–293. | ||
Ishizaki M, Kaibori M, Matsui K, et al. A case of curative resection for advanced hepatocellular carcinoma with portal vein tumor thrombus after hepatic arterial infusion chemotherapy. Gan To Kagaku Ryoho. 2012;39(12):1991–1993. | ||
Irtan S, Chopin-Laly X, Ronot M, Faivre S, Paradis V, Belghiti J. Complete regression of locally advanced hepatocellular carcinoma induced by sorafenib allowing curative resection. Liver Int. 2011;31(5):740–743. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.