Back to Journals » Clinical Ophthalmology » Volume 17
Posterior-Chamber Phakic Implantable Collamer Lenses with and without a Central Hole: A Comparative Study
Authors Amer AA, Ahmed Ghanem Abu El Wafa Ali E, Sayed Ahmed E, Ateto Hamed M ![]() , el Shazly Eata W, Amer I
, el Shazly Eata W, Amer I
Received 2 February 2023
Accepted for publication 13 March 2023
Published 16 March 2023 Volume 2023:17 Pages 887—895
DOI https://doi.org/10.2147/OPTH.S405689
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Ahmed Ali Amer,1,* Esam Ahmed Ghanem Abu El Wafa Ali,2,* Esam Sayed Ahmed,2,* Mohamed Ateto Hamed,3,* Wael el Shazly Eata,1,* Ibrahim Amer2,*
1Ophthalmology Department, Qena Faculty of Medicine, South Valley University, Qena, Egypt; 2Ophthalmology Department, Al Azhar University, Assuit, Egypt; 3Ophthalmology Department, Luxor University, Luxor, Egypt
*These authors contributed equally to this work
Correspondence: Ahmed Ali Amer, Tel +20 101 182 7000, Email [email protected]
Purpose: This study aimed to compare the short-term outcome of implanting the Visian implantable collamer lens V4 ICL versus the Visian V4c ICL in patients with moderate and high myopia.
Patients and Methods: This is a retrospective that was conducted on patients with moderate or high myopia who were scheduled for ICL implantation at our institution, Patients who underwent V4 ICL implantation with peripheral iridectomy were assigned to group A, and those who underwent V4c ICL implantation without peripheral iridectomy were assigned to group B. In group A, a preoperative peripheral iridectomy was performed. In group B, the patients received cycloplegic and dilating agents. The patients underwent a complete ocular examination preoperatively and during the follow-up visits that were conducted at 3, 6, and 12 months postoperatively.
Results: This study included 214 eyes from 107 patients; group A included 110 eyes, and group B included 104 eyes. Postoperatively, the UCVA and BCVA showed statistically significant improvement across the follow-up time points (p< 0.001), with no significant difference between the two groups. No statistically significant difference was found between the two groups in the mean achieved correction or the residual refraction. Both groups showed a strong correlation between the target and the achieved correction, with R2 = 0.99 in the two groups. No significant difference was found between the two groups in the IOP across all time measures. However, the intraocular pressure showed a statistically significant postoperative increase in group A (p=0.004), and no significant change in group B (p=0.817). There was a downward slope in the vaults of both groups across time, with significant variation in the last follow-up measure compared to the 3-month measure in the two groups (p< 0.001). No significant difference was found between the two groups across all time measures.
Conclusion: The current study adds new evidence concerning the feasibility, safety, and efficacy of ICL V4c implantation for the treatment of moderate and high myopia, with safer postoperative IOP.
Keywords: moderate and high myopia, Visian implantable collamer lens, central hole, peripheral iridectomy
Introduction
Myopia is one of the most prevalent ophthalmologic disorders that is commonly encountered during clinical practice.1 The surgical management of moderate and high myopia includes refractive lens exchange, corneal refractive surgery, and phakic intraocular lens (pIOL) implantation.2 Refractive lens exchange can treat severe myopia but causes accommodation loss in addition to other potential adverse effects; hence, it is typically not recommended for patients who are not presbyopic.2 Patients with high myopia are typically not candidates for corneal refractive surgery since, above a certain point, both the quality of vision and the complication risk increase. Phakic intraocular lens implantation may produce superior vision and have considerable advantages over corneal refractive surgery in terms of quality-of-life factors relating to vision.3,4 In patients with moderate or high myopia who refuse or are not candidates for corneal refractive surgery, it has been found that pIOL implantation is a particular and reproducible approach that is frequently employed.5
Iris-fixated anterior chamber lenses, angle-supported anterior chamber lenses, and posterior chamber lenses have all been employed for intraocular implantation.4,6 Posterior-chamber phakic lenses have received particular attention, with the Visian implantable Collamer lens (ICL) having been found to be an efficient, secure, and reliable way to correct moderate to high myopia.7,8 The intraocular pressure (IOP) and aqueous humor flow, however, may necessitate a second peripheral iridotomy either before or during the operation. To address these concerns, the V4c Visian ICL model was designed with a 360 µm central hole. This central hole was designed to increase the aqueous circulation in the eye and allow the aqueous humor to flow more naturally. Thus, there is no more need for peripheral iridectomy.9,10 Numerous clinical studies have demonstrated that V4C-Visian ICL is currently stable, safe, predictable, and efficacious.11–16 Most recently, the FDA approved the EVO/EVO+ VISIAN Implantable Collamer Lens – P030016/S035 with a center hole in March 2022.17
To date, a few studies compared the outcome of traditional V4 ICL with that of V4c ICL, especially in the region of the Middle East. This study aimed to compare the short-term outcomes of implanting V4 ICL versus V4c ICL in patients with moderate and high myopia.
Materials and Methods
This is a retrospective that was conducted on patients with moderate to high myopia who were scheduled for ICL implantation at our institution during the period from December 2020 to January 2023. The study was commenced after approval by the institutional review board at Qena Faculty of Medicine and followed the Declaration of Helsinki.
Adult patients with a clear central cornea who had a stable refraction for 2 years and a best-corrected visual acuity (BCVA) of 20/40 were eligible for the study. Patients with cataracts, an endothelial cell count (ECC) of less than 2000 cells/mm2, and an anterior chamber depth (ACD) of less than 2.8 mm were excluded from the study. Patients with a history of retinopathy, macular degeneration, retinal detachment, glaucoma, neuro-ophthalmic diseases, ophthalmic surgery, or chronic systemic diseases were also excluded from this study.
Patients who underwent V4 ICL implantation with peripheral iridectomy were assigned to group A, and those who underwent V4c ICL implantation without peripheral iridectomy were assigned to group B.
In group A, preoperative peripheral iridectomy was performed (single-hole Nd:YAG; LIGHTMED laser iridectomy) at the location 11:00 or 1:00. The diameter of the hole was 1 mm. No peripheral iridectomy was performed for patients in group B, otherwise, they received cycloplegic and dilating agents.
In both groups, the surgery was performed under topical anesthesia, as previously described.12 Postoperatively, topical antibiotics and steroids were administered 4 times per day for 2 weeks, and then doses were reduced gradually.
Follow-up visits were planned 3, 6, and 12 months after surgery. The patients underwent a complete ocular examination preoperatively and during the follow-up visits, including the assessment of the uncorrected visual acuity (UCVA) and the best-corrected visual acuity (BCVA), which were measured in Snellen’s values, then their LogMar values were obtained. Manifest refraction (spherical equivalent, SE), the anterior chamber (anterior segment optical coherence tomography; AS-OCT, Visante, Zeiss Meditec AG, Jena, Germany), horizontal white-to-white distance (WTW; AS-OCT), central corneal thickness (CCT; AS-OCT), intraocular pressure (IOP; the Goldmann applanation tonometer, AT 900, Haag-Streit, Zug, Switzerland), and mean keratometry (K; RM-8800 Autorefractor, Topcon, Tokyo, Japan) were assessed before and after surgery. Vault assessment was done using AS-OCT at the follow-up visits. The preoperative ICL sizing was performed based on the WTW and anterior chamber depth.18 The efficacy index was estimated as the 12-month UCVA divided by the preoperative BCVA, and the safety index was estimated as the 12-month BCVA divided by the preoperative BCVA. In this study, the emmetropia was considered the target refraction correction.
Study Outcomes
The primary outcome of our study was the difference in visual quality between the two groups. The secondary outcomes were the safety of the procedures, IOP, and adverse events.
Statistical Analysis
The patient’s data and the eye measurements in both groups were assessed using SPSS statistical software, version 26 (IBM Corp., Armonk, NY, USA). Categorical values were presented as frequencies and percentages and compared using the Chi-square test. Numerical values were presented as mean and standard deviation and compared using the independent t-test. A repeated measures analysis of variation (ANOVA) test was used to compare numerical data across multiple time points. A p-value less than 0.05 was considered statistically significant.
Results
This study included 214 eyes from 107 patients with a mean age of 23.21 ± 5.16 years. Fifty-nine patients were male (55.1%) and 48 were female (44.9%). Fifty-five patients (110 eyes) underwent V4 ICL implantation with peripheral iridectomy (group A), and fifty-two patients (104 eyes) underwent V4c ICL implantation (group B).
The baseline data are shown in Table 1. No statistically significant differences were noted between the two groups in the ophthalmic measures (p>0.05).
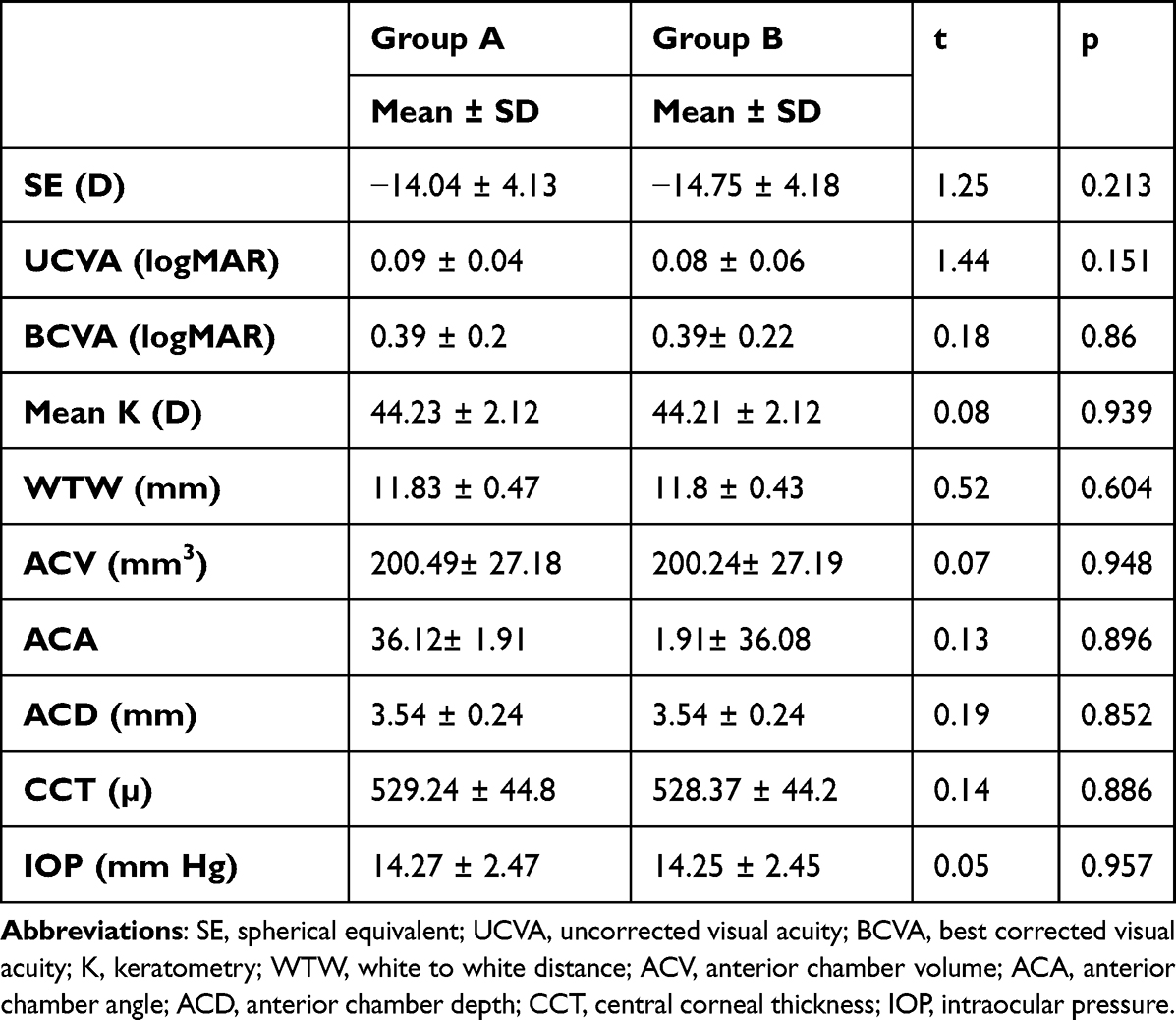 |
Table 1 Baseline Data of the Examined Eyes |
Postoperatively, the UCVA and BCVA showed statistically significant improvement across the follow-up time points (p<0.001), with no significant difference between the two groups, as the UCVA changed from 0.09 ± 0.04 and 0.08 ± 0.06 logMAR preoperatively to 0.556 ± 0.159 and 0.557 ± 0.16 logMAR at 12 months postoperatively in the two groups, respectively, with a p-value of 0.985. The BCVA changed from 0.387 ± 0.2 logMAR preoperatively to 0.605 ± 0.191 logMAR at 12 months postoperatively in group A and from 0.392 ± 0.22 logMAR preoperatively to 0.607 ± 0.192 logMAR in group B (p=0.933).
The mean efficacy index was 1.86 ± 1.01 in group A and 1.72 ± 0.63 in group B, with no statistically significant difference (p=0.245). The mean safety index was 2 ± 1.16 in group A and 1.85 ± 0.73 in group B, with no statistically significant difference (p=0.243).
The spherical equivalent showed statistically significant improvement in both groups compared to the preoperative values (p<0.001). There was evident stability in the SE values across the postoperative time measures in the two groups with a 3-month mean SE of - 0.659 ± 0.45 in group A and - 0.658 ± 0.44 in group B (p=0.994), 6-month mean SE of - 0.641 ± 0.43 in group A and - 0.639 ± 0.43 in group B (p=0.98), and 12-month mean SE of - 0.614 ± 0.415 in group A and −0.62 ± 0.421 in group B (p=0.909) (Figure 1). Across the postoperative measures, the difference in mean SE was 0.045 ± 0.21 in group A and 0.039 ± 0.19 in group B (p=0.8).
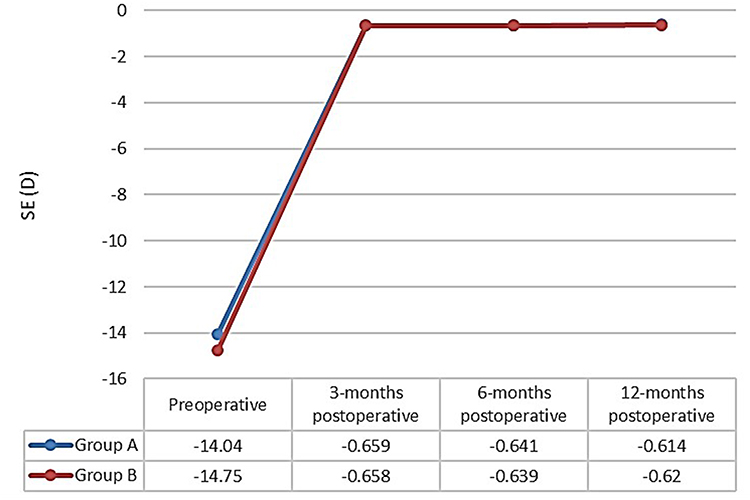 |
Figure 1 The preoperative and follow-up spherical equivalent in group A (patients who underwent ICL V4 implantation with peripheral iridectomy) and group B (Patients who underwent ICL V4c implantation without peripheral iridectomy). |
No statistically significant difference was found between the two groups in the mean achieved correction (−13.42 ± 4.19 in group A and −14.13 ± 4.22 in group B, p=0.223) or the residual refraction (- 0.614 ± 0.415 in group A and −0.62 ± 0.421 in group B, p=0.909). At the 12-month follow-up, ninety-nine eyes in group A (90%) were within ± 1.0 D of the target correction, and sixty-six eyes (60%) were within ± 0.5 D. In group B, ninety-four eyes (89.4%) were within ± 1.0 D, and sixty-two eyes (59.6%) were within ± 0.5 D. No statistically significant difference was found between the two groups (p=0.954). Both groups showed a strong correlation between the target and the achieved correction, with R2 = 0.99 in the two groups (Figures 2 and 3).
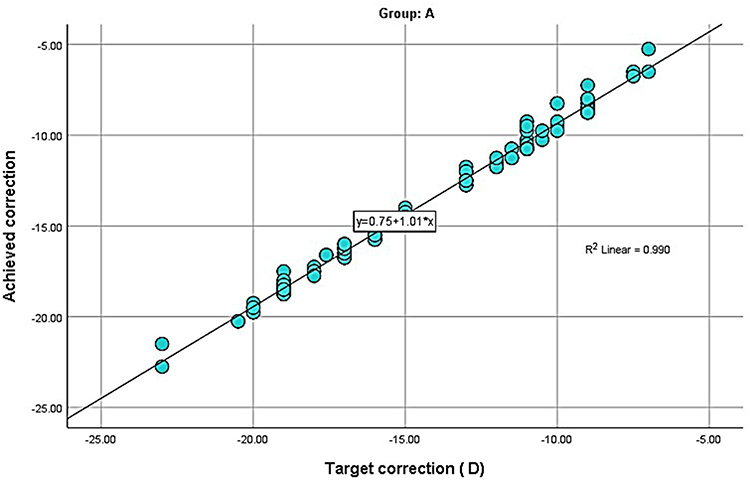 |
Figure 2 The correlation between the target and achieved correction in group A (patients who underwent ICL V4 implantation with peripheral iridectomy). |
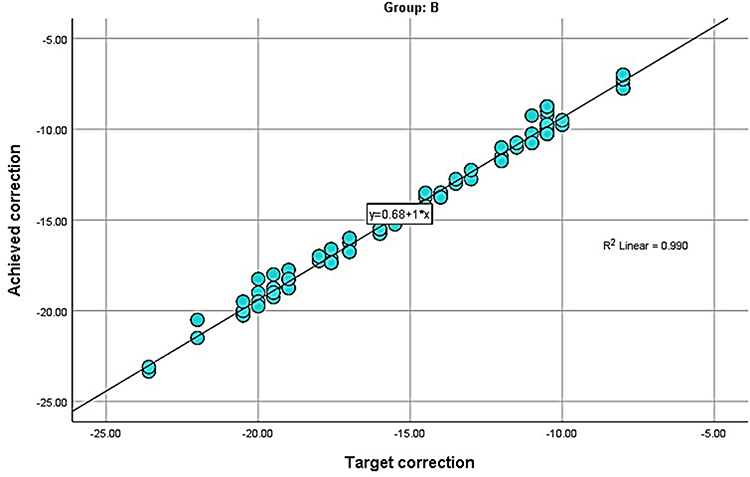 |
Figure 3 The correlation between the target and achieved correction in group B (patients who underwent ICL V4c implantation without peripheral iridectomy). |
No significant difference was found between the two groups in the IOP across all time measures (p=0.991 preoperatively, p=0.208 at 3 months, p =0.339 at 6 months, and p= 0.556 at 12 months) (Figure 4). However, the intraocular pressure showed a statistically significant postoperative increase in group A (p=0.004), and no significant change in group B (p=0.817). Post-hoc correction demonstrated that the significant difference in group A was found only between the preoperative and the 3-month postoperative reading (p=0.021).
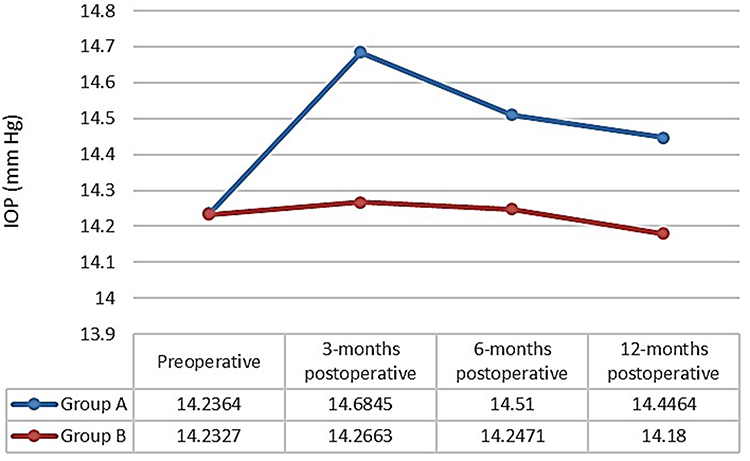 |
Figure 4 The preoperative and follow-up IOP in group A (patients who underwent ICL V4 implantation with peripheral iridectomy) and group B (patients who underwent ICL V4c implantation without peripheral iridectomy). |
There was a downward slope in the vaults of both groups across time, with significant variation in the last follow-up measure compared to the 3-month measure in the two groups (p<0.001). No significant difference was found between the two groups across all time measures (p=0.271 at 3 months, p=0.369 at 6 months, and p=0.603 at 12 months) (Figure 5). All cases had a vault ranging between 0.25 and 0.75 mm.
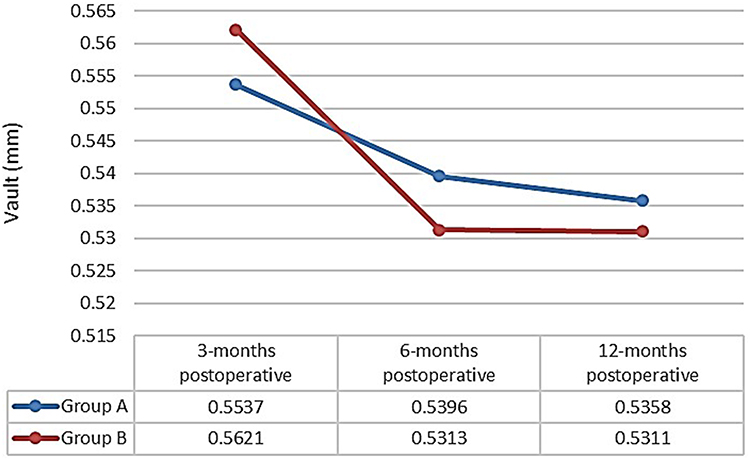 |
Figure 5 The follow-up vault measure in group A (patients who underwent ICL V4 implantation with peripheral iridectomy) and group B (Patients who underwent ICL V4c implantation without peripheral iridectomy). |
During the follow-up period, no cases of sight-threatening complications were encountered.
Discussion
The unique central hole in ICL V4c offers several advantages. First, it leads to the avoidance of peripheral iridectomy and hence precludes its associated adverse outcome. Second, it re-establishes the physiological cycle of aqueous humor, which helps to reduce the incidence of posterior capsule turbidity and then reduces the potentiality of postoperative cataracts. In addition, this central hole ensures the IOP’s stability.19
Despite the reported Visian V4c ICL efficacy, it has been argued that its central hole may impact the quality of vision in patients with high myopia. In the present study, there was evidently comparable and significant improvement of UCVA and BCVA in both groups. Likewise, several previous studies reported significant improvement in the visual acuity after ICL V4c implantation,20–27 and found no significant difference between ICL with or without the central hole in the visual outcome.21,22,24,27 These findings were further corroborated by the efficacy and safety indices. In this study, we found the efficacy index to be 1.86 in group A and 1.72 in group B. These figures reflect that the mean UCVA at the last follow-up was considerably better than the preoperative BCVA in both groups. In addition, the improvement in BCVA of the patients was reflected in high safety indices in the two groups (2 and 1.85). Higher than one efficacy and safety index was also found in the literature-reported outcome of central hole ICL,20–29 which confirms the improvement of UCVA and BCVA.
The present study showed that patients in the two groups achieved similar levels of correction and had similar residual refraction errors. Both groups showed a strong correlation between the target and the achieved correction. At the final follow-up, we achieved SE values within ± 1.0 D of the target in 90% of group A and 89.4% of group B, and SE values within ± 0.5 D of the target in 60% of group A and 59.6% of group B. This was in agreement with the study of Yaşa et al28 who found that at one year, 62% and 93% of the eyes were within ± 0.50D and ±1.00D of the target refraction, respectively. A similar achievement was obtained by 69% and 87.2% of the eyes, respectively, in the study of Lee et al.30 Our findings were also supported by the study of Shimizu et al12 who found that using ICL V4c and ICL V4 showed a similarly strong correlation between the achieved and attempted correction.
We found that there was a steep postoperative rise in the IOP in both groups that showed regression after the 3-month follow-up. Interestingly, the difference was significant in the group who had ICL V4 implantation, while it was non-significant in the group who had the new ICL V4c implantation. The postoperative elevation of IOP is likely attributable to the postoperative inflammatory changes and trabeculitis that regress gradually over time. Although no peripheral iridectomy was performed in the ICL V4c group, an appropriate flow of aqueous was maintained as a result of the central hole. From our findings, it seems that the fluid circulation function of the central hole is more effective than that of peripheral iridectomy. In consistency with our findings, it has been proposed that the ICL V4c central flow technology can hinder the effect of metabolism on its crystal, leading to reduced risks of high IOP.31–33 This finding was not reported previously in a similar cohort of patients, making us unable to compare our results. However, this indicates an appropriate effect if the central hole keeps the aqueous humour flowing naturally and alleviates the postoperative inflammatory process with its related effect on metabolism, even more than peripheral iridectomy can do.
The non-significant differences between the two groups in the IOP measures along the study are consistent with the studies of Shimizu et al12 and Higueras-Esteban et al,34 that revealed that no statistically significant difference was found in the IOP after implantation of either type of ICL.
Other than elevated IOP, vault extremes predispose to adverse events including pupillary block, glaucoma, and cataract. However, there are still no definite cutoff values for inadequate and excessive values of the vault. The safe vault has been reported to range from 50–250 µ, as a lower bound to about 1000 µ, as an upper bound.29,35–37 However, it is currently advised not to be outside the range of 250 µ to 750 µ whenever possible. The appropriate vault is intimately dependent on the proper pIOL size of the posterior chamber. In this study, at the last follow-up, all cases had a vault ranging between 250 and 750µ, with no significant difference between the two groups across all time measures, indicating that the ICL sizing was well-matched with the posterior chambers in the studied eyes. There has been a wide variation of vault measures among the studies that evaluated ICL V4 and ICL V4c implantation. Our result is within the range of data reported in the literature, where vault measures ranged from values varying from 340 µm38 to 637 µm.39 A pooled mean of 486 µm was described in the meta-analysis conducted by Montés-Micó et al11 and 357 µm in the meta-analysis of Fernández-Vega-Cueto et al.40
In agreement with the previous studies on pIOL implantation, during the follow-up period, no sight-threatening complications were encountered.
Overall, this study provided equal efficacy for both procedures, however, with interesting evidence about the ICL V4c central flow technology being safer than the traditional ICL V4 even with peripheral iridectomy in terms of IOP after surgery. Therefore, this finding could tilt the odds in favor of adopting ICL V4c implantation rather than ICL V4. This should be the focus of more research studies. Notably, there was a downward slope in the vaults of both groups across time, with significant variation in the last follow-up measure compared to the 3-month measure in the two groups. All patients had a proper vault, indicating that the ICL sizing was well-matched with the posterior chambers in the studied eyes.
This study is limited by the retrospective design and the short-term follow-up. Also, it is limited by the non-assessment of the endothelial cell count which was not available in the patients’ registry. However, it is one of few studies investigating the outcome of ICL V4c versus ICL V4 implantation in a sample exceeding 200 eyes. Moreover, no similar previous studies were conducted in our geographical region.
Conclusion
The current study adds new evidence concerning the feasibility, safety, and efficacy of ICL V4c implantation for the treatment of moderate and high myopia.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Pan CW, Ramamurthy D, Saw SM. Worldwide prevalence and risk factors for myopia. Ophthalmic Physiol Opt. 2012;32:3–16. doi:10.1111/j.1475-1313.2011.00884.x
2. Lundström M, Manning S, Barry P, et al. The European registry of quality outcomes for cataract and refractive surgery (EUREQUO): a database study of trends in volumes, surgical techniques and outcomes of refractive surgery. Eye and Vision. 2015;2(1):8. doi:10.1186/s40662-015-0019-1
3. Kobashi H, Kamiya K, Igarashi A, et al. Long-term quality of life after posterior chamber phakic intraocular lens implantation and after wavefront-guided laser in situ keratomileusis for myopia. J Cataract Refract Surg. 2014;40(12):2019. doi:10.1016/j.jcrs.2014.03.028
4. Güell JL, Morral M, Kook D, Kohnen T. Phakic intraocular lenses part 1: historical overview, current models, selection criteria, and surgical techniques. J Cataract Refract Surg. 2010;36(11):1976–1993. doi:10.1016/j.jcrs.2010.08.014
5. Schallhorn SC, Farjo AA, Huang D, et al.; American Academy of Ophthalmology. Phakic intraocular lens implantation for the correction of myopia; a report by the American Academy of Ophthalmology (Ophthalmic Technology Assessment). Ophthalmology. 2009;116:2244–2258.
6. Kohnen T, Kook D, Morral M, Güell JL. Phakic intraocular lenses: part 2: results and complications. J Cataract Refract Surg. 2010;36:2168–2194.
7. Pérez-Cambrodí RJ, Blanes-Mompó FJ, García-Lázaro S, et al. Visual and optical performance and quality of life after implantation of posterior chamber Phakic intraocular Lens. Graefes Arch Clin Exp Ophthalmol. 2013;251:331–340. doi:10.1007/s00417-012-2041-5
8. Igarashi A, Shimizu K, Kamiya K. Eight-year follow-up of posterior chamber Phakic intraocular Lens implantation for moderate to high myopia. Am J Ophthalmol. 2014;157(3):532–539. doi:10.1016/j.ajo.2013.11.006
9. Kawamorita T, Uozato H, Shimizu K. Fluid dynamics simulation of aqueous humour in a posterior-chamber Phakic intraocular Lens with a central perforation. Graefes Arch Clin Exp Ophthalmol. 2012;250:935–939. doi:10.1007/s00417-011-1850-2
10. Fujisawa K, Shimizu K, Uga S, et al. Changes in the crystalline Lens resulting from insertion of a Phakic IOL (ICL) into the porcine eye. Graefes Arch Clin Exp Ophthalmol. 2007;245:114–122. doi:10.1007/s00417-006-0338-y
11. Montés-Micó R, Ruiz-Mesa R, Rodríguez-Prats JL, Tañá-Rivero P. Posterior-chamber phakic implantable collamer lenses with a central port: a review. Acta Ophthalmol. 2021;99(3):e288–e301. doi:10.1111/aos.14599
12. Shimizu K, Kamiya K, Igarashi A, Kobashi H. Long-term comparison of posterior chamber phakic intraocular lens with and without a central hole (Hole ICL and Conventional ICL) implantation for moderate to high myopia and myopic astigmatism. Medicine. 2016;95:e3270. doi:10.1097/MD.0000000000003270
13. Packer M. Meta-analysis and review: effectiveness, safety, and central port design of the intraocular collamer lens. Clin Ophthalmol. 2016;10:1059–1077. doi:10.2147/OPTH.S111620
14. Tian Y, Jiang HB, Jiang J, Wen D, Xia XB, Song WT. Comparison of implantable collamer lens Visian ICL V4 and ICL V4c for high myopia: a cohort study. Medicine. 2017;96(25):e7294. doi:10.1097/MD.0000000000007294
15. Tang Y, Ye J. Phakic posterior chamber intraocular lens with a central hole in treating patients with moderate to high myopia: a meta-analysis. J Ophthalmol. 2019;2019:e9496326. doi:10.1155/2019/9496326
16. Packer M. The implantable collamer lens with a central port: review of the literature. OPTH. 2018;12:2427–2438. doi:10.2147/OPTH.S188785
17. Approval for the EVO/EVO+ Visian implantable collamer lens. Available from: https://www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfpma/pma.cfm?id=P030016S035.
18. Singh R, Vanathi M, Kishore A, et al. An anterior segment optical coherence tomography study of the anterior chamber angle after implantable collamer lens-V4c implantation in Asian Indian Eyes. Indian J Ophthalmol. 2020;68(7):1418–1423. doi:10.4103/ijo.IJO_1540_19
19. Fernández-Vega-Cueto L, Alfonso-Bartolozzi B, Lisa C, et al. Seven-year follow-up of posterior chamber phakic intraocular lens with central port design. Eye Vis. 2021;8(1):23. doi:10.1186/s40662-021-00247-1
20. Shimizu K, Kamiya K, Igarashi A, Shiratani T. Early clinical outcomes of implantation of posterior chamber phakic intraocular lens with a central hole (hole ICL) for moderate to high myopia. Br J Ophthalmol. 2012;96:409–412. doi:10.1136/bjophthalmol-2011-300148
21. Cao X, Wu W, Wang Y, et al. Comparison over time of vault in Chinese eyes receiving implantable contact lenses with or without a central hole. Am J Ophthalmol. 2016;172:111–117. doi:10.1016/j.ajo.2016.09.016
22. Ganesh S, Brar S, Pawar A. Matched population comparison of visual outcomes and patient satisfaction between 3 modalities for the correction of low to moderate myopic astigmatism. Clin Ophthalmol. 2017;11:1253–1263. doi:10.2147/OPTH.S127101
23. Pjano MA, Pidro A, Biscevic A, et al. Refractive outcomes of posterior chamber phakic intraocular lens implantation for correction of myopia and myopic astigmatism. Med Arch. 2017;71(2):93–96. doi:10.5455/medarh.2017.71.93-96
24. Kojima T, Kitazawa Y, Nakamura T, et al. Prospective randomized multicenter comparison of the clinical outcomes of V4c and V5 implantable collamer lenses: a contralateral eye study. J Ophthalmol. 2018;2018:7623829. doi:10.1155/2018/7623829
25. Lee H, Kang DSY, Choi JY, et al. Rotational stability and visual outcomes of V4c toric phakic intraocular lenses. J Refract Surg. 2018;34:489–496. doi:10.3928/1081597X-20180521-01
26. Chen X, Shen Y, Xu H, et al. One‐year natural course of corneal densitometry in high myopic patients after implantation of an implantable collamer lens (model V4c). BMC Ophthalmol. 2020;20:50. doi:10.1186/s12886-020-1320-x
27. Huseynova T, Ozaki S, Ishizuka T, et al. Comparative study of 2 types of implantable collamer lenses, 1 with and 1 without a central artificial hole. Am J Ophthalmol. 2014;157(6):1136–1143. doi:10.1016/j.ajo.2014.01.032
28. Yaşa D, Ürdem U, Ağca A, et al. Early results with a new posterior chamber phakic intraocular lens in patients with high myopia. J Ophthalmol. 2018;2018:1329874. doi:10.1155/2018/1329874
29. Lisa C, Naveiras M, Alfonso-Bartolozzi B, et al. Posterior chamber collagen copolymer phakic intraocular lens with a central hole to correct myopia: one-year follow-up. J Cataract Refract Surg. 2015;41(6):1153–1159. doi:10.1016/j.jcrs.2014.10.030
30. Lee J, Kim Y, Park S, et al. Long-term clinical results of posterior chamber phakic intraocular lens implantation to correct myopia. Clin Exp Ophthalmol. 2016;44(6):481–487. doi:10.1111/ceo.12691
31. Alfonso JF, Lisa C, Fernandez-Vega L, et al. Prevalence of cataract after collagen copolymer phakic intraocular lens implantation for myopia, hyperopia, and astigmatism. J Cataract Refract Surg. 2015;41(4):800–805. doi:10.1016/j.jcrs.2014.07.039
32. Goukon H, Kamiya K, Shimizu K, Igarashi A. Comparison of corneal endothelial cell density and morphology after posterior chamber phakic intraocular lens implantation with and without a central hole. Br J Ophthalmol. 2017;101(11):1461–1465. doi:10.1136/bjophthalmol-2016-309363
33. Guber I, Mouvet V, Bergin C, et al. Clinical outcomes and cataract formation rates in eyes 10 years after posterior phakic lens implantation for myopia. JAMA Ophthalmol. 2016;134(5):487–494. doi:10.1001/jamaophthalmol.2016.0078
34. Higueras-Esteban A, Ortiz-Gomariz A, Gutiérrez-Ortega R, et al. Intraocular pressure after implantation of the Visian implantable collamer lens with CentraFLOW without iridotomy. Am J Ophthalmol. 2013;156(4):800–805. doi:10.1016/j.ajo.2013.05.018
35. Maeng HS, Chung TY, Lee DH, Chung ES. Risk factor evaluation for cataract development in patients with low vaulting after phakic intraocular lens implantation. J Cataract Refract Surg. 2011;37(5):881–885. doi:10.1016/j.jcrs.2010.11.037
36. Schmidinger G, Lackner B, Pieh S, Skorpik C. Long-term changes in posterior chamber phakic intraocular collamer lens vaulting in myopic patients. Ophthalmology. 2010;117(8):1506–1511. doi:10.1016/j.ophtha.2009.12.013
37. Zeng QY, Xie XL, Chen Q. Prevention and management of collagen copolymer phakic intraocular lens exchange: causes and surgical techniques. J Cataract Refract Surg. 2015;41(3):576–584. doi:10.1016/j.jcrs.2014.06.036
38. Alfonso JF, Fernández‐Vega‐Cueto L, Alfonso‐Bartolozzi B, et al. Five‐year follow‐up of correction of myopia: posterior chamber phakic intraocular lens with a central port design. J Refract Surg. 2019;35:169–176. doi:10.3928/1081597X-20190118-01
39. Eissa SA, Sadek SH, El‐Deeb MW. Anterior chamber angle evaluation following phakic posterior chamber collamer lens with CentraFLOW and its correlation with ICL vault and intraocular pressure. J Ophthalmol. 2016;2016:1383289. doi:10.1155/2016/1383289
40. Fernández-Vega-Cueto L, Lisa C, Esteve-Taboada JJ, et al. Implantable collamer lens with central hole: 3-year follow-up. OPTH. 2018;12:2015–2029. doi:10.2147/OPTH.S171576
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.