")
Back to Journals » Risk Management and Healthcare Policy » Volume 16
Post-War Assessment of the Prevalence and Determinants of Unplanned Pregnancy Among Pregnant Women Attending Public Hospitals in Conflict-Zones of South Wollo, Northeast Ethiopia, 2022, Multi-Center Study
Authors Berihun Erega B , Ferede WY , Sisay FA, Dagnaw EH, Ayaliew AB , Ketema WG , Shite Lake E
Received 29 April 2023
Accepted for publication 26 July 2023
Published 9 August 2023 Volume 2023:16 Pages 1489—1497
DOI https://doi.org/10.2147/RMHP.S419346
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jongwha Chang
Besfat Berihun Erega,1 Wassie Yazie Ferede,1 Fillorenes Ayalew Sisay,1 Eyaya Habtie Dagnaw,1 Abeba Belay Ayaliew,1 Wondimnew Gashaw Ketema,2 Eyob Shite Lake3
1Department of Midwifery, College of Medicine and Health Sciences, Debre Tabor University, Debre Tabor, Ethiopia; 2Department of Midwifery, College of Medicine and Health Sciences, Wollo University, Dessie, Ethiopia; 3Department of Midwifery, College of Medicine and Health Sciences, Woldia University, Woldia, Ethiopia
Correspondence: Besfat Berihun Erega, Email [email protected]
Background: Worldwide, although unplanned pregnancy seems decreasing, 38% of pregnancies are unintended. In sub-Saharan Africa, unintended pregnancy accounts for more than a quarter of the 40 million pregnancies that occur annually.
Objective: The study aimed to assess the prevalence and determinants of unplanned pregnancy among pregnant women attending public hospitals in conflict-zones of South Wollo zone, Northeast Ethiopia, 2022.
Methods: A multi-center facility-based cross-sectional study was conducted from December 20, 2021 to February 30, 2022 among the hospitals of South Wollo zone that that were destructed by the armed conflict.
Results: The prevalence of unplanned pregnancy in our study was 44.72% (CI=39.40– 48.08%).
Conclusion: In this study nearly half of the pregnancies were unplanned, which is shocking to the health care system in the 21st century.
Keywords: unplanned pregnancy, armed conflict, post-war assessment, Ethiopia
Introduction
Unplanned pregnancy is defined as any form of conception that is mistimed (pregnancy that comes earlier than the time) or pregnancy that is unwanted at all.1,2 Unplanned pregnancy is one of the most common root causes of maternal morbidity like mental, physical, economical, and other health related crises, mainly through unsafe abortion and other related sexually transmitted diseases.3,4 Unplanned pregnancy is found to have an increased public health importance in determining the quality-of-life for the woman, the fetus in utero, children, and family as a whole, both in developed and developing countries.5,6 A complex set of social and psychological factors puts women at risk of unintended pregnancy. Abortion, infertility, child abandonment, and maternal deaths are negative consequences of unintended pregnancies.7,8 Worldwide, although unplanned pregnancy seems to be decreasing, 38% of pregnancies are unintended (that is, 80 million pregnancies annually). In sub-Saharan Africa, unintended pregnancy accounts for more than a quarter of the 40 million pregnancies that occur annually.4,9 The magnitude of unplanned pregnancy is a good indicator for evaluation of women’s reproductive health, women’s right to decide when to have children, level of unwanted sexual acts happening to women, and proportions of limitations to have better opportunities on social, economical, and other health care guarantees given to women.
Globally, from all pregnancies, 44% of them are unplanned, of which, more than half (56%) ended up in termination before viability by the year 2014.10 Worldwide, in 2015, 303,000 women died due to terminating a pregnancy; of these women, 99% of the deaths were from developing counties, with sub-Saharan Africa accounting for the majority of deaths, followed by South Asia (22%).11
Available literature in Africa showed that the prevalence of unplanned pregnancy was 53.3%, 31.1%, and 24% in Malawi,12 southern Nigeria,7 and Kenya,3 respectively. Other available studies done in Ethiopia showed that the figure was 37.8%, 36.9%, 33.3%, 36.5%, 32.9% 22.3%, and 13.7% in Addis Ababa,13 Dilla,14 Harare,15 Wellega,16 and North Shoa,17 respectively.
Worldwide, according to available findings, the common determinant factors of unplanned pregnancy were age greater than 40 years,6,9 unemployment, higher education,6,18 being unmarried women,3,19 age less than 30,3,5 contraceptive failure,18,20 contraceptive inconsistent use,7,18 not using contraceptive,2,18 rural residence,18,19 absence of male involvement,9,18 lack of knowledge about contraceptives,7,18 short birth interval,5 high parity,2,6 and no formal education.6,18
Despite the fact that the global health policy gives an emphasis on the reduction of maternal mortality and family planning coverage women are still dying from pregnancy related complications and unintended pregnancy is still on the national health public health agenda. Hence, this study was, as it was the first of its nature, aimed to assess the prevalence and determinants of unintended pregnancy among pregnant women attending antenatal clinics in the conflict zone of South Wollo hospitals. The study also aimed to signify the impact of the armed conflict on the women’s desire when to conceive. The findings of this study will be used for policy makers in order to properly allocate resources and intervene in maternal and child health problems. In addition, the concerned stockholder will also intervene and compensate damages due to the conflict that had an impact on reproductive and family health.
Methods and Materials
Study Design and Setting
An institutional-based cross-sectional study was employed. The study was conducted in selected public hospitals of South Wollo zone, Ethiopia, immediately after the armed conflict (after the Tigray People Liberation Front (TPLF)’s withdrawal) from December 20, 2021 to February 30, 2022. Among the hospitals of South Wollo zone that were attacked by the armed conflict, especially by the TPLF’s forces, four government hospitals (Borumeda Hospital, Delanta Hospital, Hayq Hospital, and Mekaneselam Hospital) were selected using a simple random sampling technique.
Source Population
All pregnant women who attended antenatal clinics of government hospitals of South Wollo zone.
Study Population
All pregnant women who attended antenatal clinics of selected public hospitals of South Wollo zone during the study period.
Sample Size and Sampling Procedure
The sample size was calculated by using the assumption of a single population proportion formula considering the prevalence of unplanned pregnancy in Debre Markos as 32.9%, with a 95% confidence interval, a margin of error of 5%, and a 10% non-response rate. Then the final sample size was calculated to be 369. To reach the study participants, systematic random sampling was employed after investigating the case flow of each study hospital before the armed conflict. This was because the case flow was considered to be affected due to the fact that the hospitals were in the conflict zone. Finally, the sampling interval was determined by dividing two months case report to sample size in each hospital, and the final kth value for Mekaneselam Hospital, Delanta Hospital, Borumeda Hospital, and Mekaneselam Hospital was 2.2, 2.5, 2.3, and 2.7, respectively. Hence the first case to come was taken as participant one and every two cases were selected.
Data Collection Procedure
The data was collected by four BSc degree holder midwives using structured questionnaires after training was given for a day. The questionnaire was prepared originally in English and was translated into local language (Amharic) for the purpose of data collection. It was translated back to English again for consistency and accuracy by language experts. Pretesting was also done in two primary hospitals outside the study areas. To avoid a chicken and egg dilemma on the possible reasons for the pregnancy to be unplanned, the data collectors were provided with a clear explanation.
Ethical Approval and Consent to Participate
Ethical clearance was obtained from the Institutional Review Board of Debre Tabor University, School of Midwifery College of Medicine and Health Sciences (CMHS) with a reference number DTU/RE/1104/2022. A letter of permission was obtained from the clinical coordinator of each study hospital. Clear explanations about the purpose of the study were given, along with the letter of support for all concerned bodies. Finally, written informed consent was obtained from all respondents after thoroughly explaining the aim of the study to them. In addition, all methods were performed in accordance with the relevant guidelines and regulations. The guidelines outlined in the Declaration of Helsinki were also followed.
Study Variables
Dependent Variable
- Unplanned pregnancy.
Independent Variables
- Sociodemographic variables.
- History of sexual and reproductive health.
Data Processing and Analysis
After manually checking its completeness and consistency, the data were entered using Epi-data version 4.6 software and analyzed using SPSS version 23 software. Then the crude association between unplanned pregnancy and determinant factors crude odds ratio (COR) was calculated with a 95% confidence interval (CI). Variables with an odds ratio of ≤0.2 were considered for multivariate analysis. Variables with an adjusted odds ratio of ≤0.05 were considered to determine a significant association. Hosmer–Lemeshow goodness-of-fit test was used to check the model fitness, and poor fit was considered by a value less than 0.05. It is considered to have multi-collinearity when the variance inflation factor (VIF) is greater than 10. There was no multi-collinearity poor fit as the calculated VIF was less than 10.
Operational Definitions
Family Planning Knowledge
The respondents’ level of knowledge about family planning was reported as good knowledge if the study participant correctly responded to more than or equal to 80% of knowledge assessment tools, and poor for <80%.
Unmet Need of Family Planning
The percentage of women of reproductive age, either married or in any other relationship who wish to stop or delay childbirth but are not using contraceptives.
Unwelcomed Sex
Expressions of sexual interests that are unwelcome, unreciprocated, or offensive to those targeted to the sexual act.
Results
Socio Demographic Characteristics
A total of 369 respondents were included in this study, with a response rate of 100%. The majority of the respondents were in the age group 25–34 years (45.80%), rural residents (67.21%), ethnic Amhara (84.55%), married (75.34%), and had a monthly income of between 1,001–3,000 ETB (47.78%) in this post war study. The mean age of the study participants was 24.61 (±5.85 SD) (Table 1).
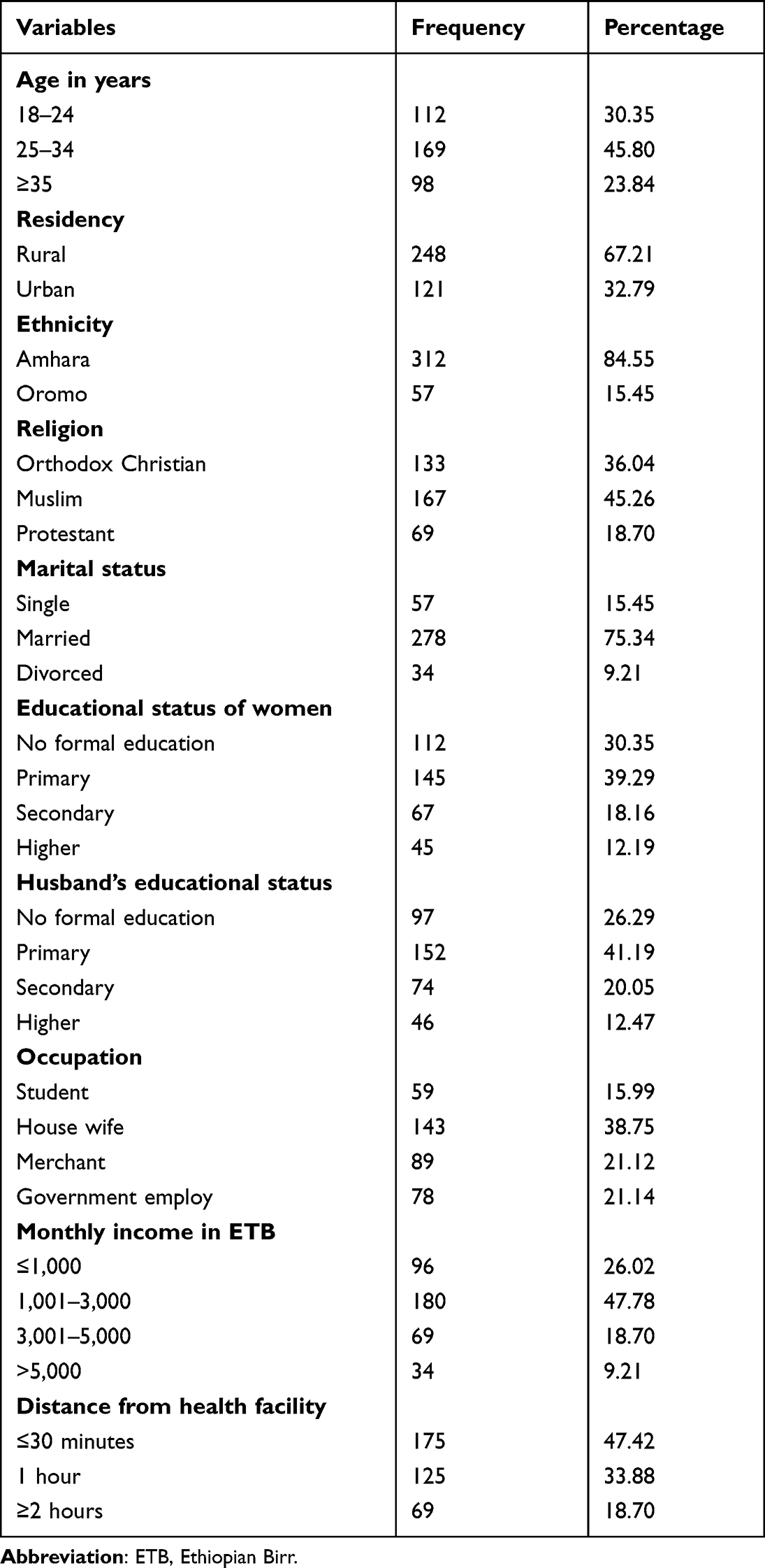 |
Table 1 Socio-Demographic Characteristics of the Respondents at Public Hospitals of South Wollo Zone, Northwest Ethiopia, 2022 (N=369) |
Reproductive Characteristics
In this study, a high proportion (44.72%) of the pregnancies were unplanned, but wanted (74.25%) and supported (82.38%) after the pregnancy had occurred. The majority of the respondents also had parity between one and four (50.14%), a birth interval of less than 2 years (51.22%) and had alive children of less than 5 years old (78.59%). In addition, most of the respondents faced an unmet need of FP (59.08%), and lack of a functioning health facility during the war (79.95%) in our post conflict assessment (Table 2).
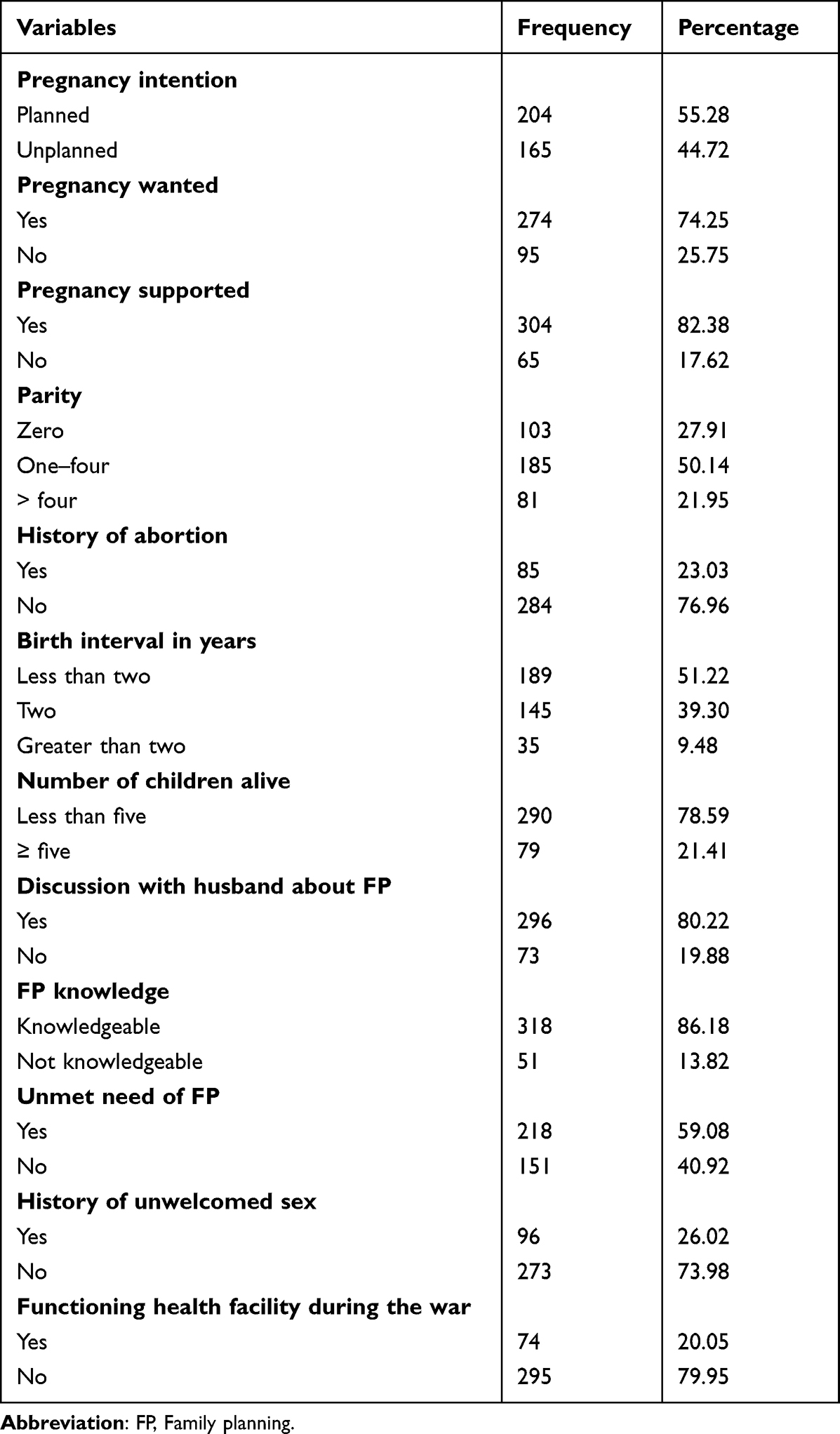 |
Table 2 Reproductive Characteristics of the Respondents at Public Hospitals of South Wollo Zone, Northwest Ethiopia, 2022 (N=369) |
Post War Reasons for Unplanned Pregnancy
According to this post war assessment, the most common reasons for the women to think of their pregnancy as unplanned were pregnancy due to contraceptive failure, pregnancy due to unmet need of FP, the need to postpone the pregnancy, not supported by their family, abandoned by their partner, and extramarital pregnancy (Table 3).
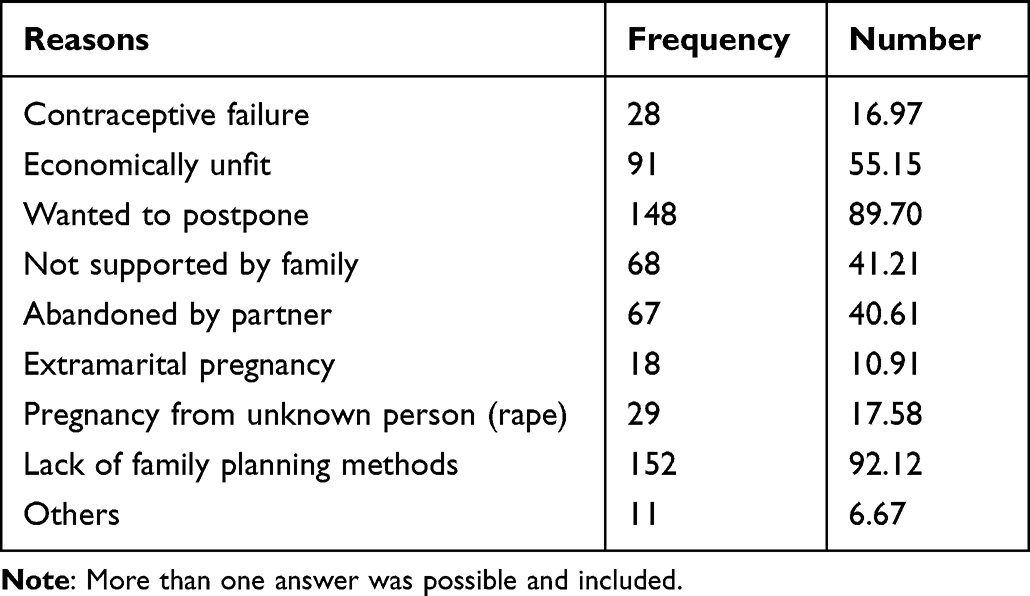 |
Table 3 Percentage Distribution of the Reasons for Unplanned Pregnancy Among Women with Unplanned Pregnancy in South Wollo Zone, Ethiopia, 2022 (N=165) |
Post War Determinants of Unplanned Pregnancy
Under possible adjustment for other confounding variables, rural residency (0.59; 0.06–0.89), being single (9.34; 6.65–12.11), having an occupation of student (7.91; 6.42–10.04) and house wife (2.01; 1.94–4.21), unmet need for family planning (3.12; 1.76–4.28); and lack of functioning health facility during the armed conflict (7.45; 5.25–9.04) were found to be the factors associated with unplanned pregnancy in this post war assessment of the conflict zones immediately after the armed conflict (Table 4).
 |
Table 4 Bivariate and Multivariate Logistic Regression Analysis of Determinants Associated with Unplanned Pregnancy in Public Hospitals of South Wollo Zone, Northwest Ethiopia, 2022 (N=369) |
Discussion
The primary findings of our study are the prevalence and common determinants of unplanned pregnancy in the conflict zones of South Wollo zone. This post war assessment specifically aimed to report the negative burden of the armed conflict on unplanned pregnancy. The prevalence of unplanned pregnancy in our study was 44.72% (CI=39.40–48.08%). This finding is much higher than in studies done in Nigeria (31.1%), Kenya (24%), and other sub-Saharan countries.20 Our study finding is also extensively higher than studies reported in Mizzan-tepi (13.3%),18 Dilla (36.9%),14 Wolega (32.9%),16 Harare (33.3%),15 and Addis Zemen (26.1%).2 The most likely reason for this higher prevalence of unplanned pregnancy in our study was the greatimpact of the armed conflict on the health system, specifically of the reproduction and reproductive health areas. Since there was no functional reproductive health clinic during the armed conflict in our study area, women of reproductive age could not access any options of family planning methods. Other possible explanations for the increased prevalence of unplanned pregnancy could be the presence of illegal and un-welcomed sexual acts either by the conflict handlers or their close relatives and lack of awareness about post coital family planning methods. Surprisingly, the prevalence of unplanned pregnancy in our study was found to be lower than a study prevalence reported in Malawi (53.3%).12,19 The possible justification for the lower prevalence could be the difference in study nations and the study done in Malawi was done before eight years when people were not aware of family planning methods.
In our study, rural residency (0.59; 0.06–0.89) decreases the odds of unplanned pregnancy by 41%. This finding was the reverse of other studies done in Mchinji district of Malawi and Mizzan-tepi of Ethiopia.18,19
Our study finding also opposes the logical notion that urban populations are more aware of family planning methods and can access it easier than the rural community. The possible justification for this different finding could be due to the control and use of urban rather than rural areas for the temporary living environment of the armed forces. This indirectly exposes the urban women to un-welcomed sex along with greater difficulty of getting family-planning methods. Our study also reported that being single (9.34; 6.65–12.11) increases the odds of unplanned pregnancy by a factor of 9.34-times. This finding is also supported by studies done in Malawi,19 Kenya,3 and Suhul of Northern Ethiopia.1 The possible reasons for this association could be due to the tradition that pregnancies before marriage are not supported by the community, and most commonly occurred after un-welcomed sex, contraceptive failure, or unmet need of family planning.
Our study also showed that occupation of being a student (7.91; 6.42–10.04) and house wife (2.01; 1.94–4.21) increases the odds of unplanned pregnancy by 7.91-times and 2.01-times, respectively. This study finding is also supported by studies done in Nigeria,8,21 Egypt,5 Malawi,12,19 Kenya,3 and Ethiopia.9,18 The possible reason for the association could be students and housewives were the ones with lower economic status and can not afford to migrate to the conflict free areas and are affected by the armed conflict. Another possible explanation for this could be the attractive nature of students due to the difference in age (mostly younger) and dressing (mostly modernized).
In addition our study also reported that the unmet need for family planning (3.12; 1.76–4.28) and lack of a functioning health facility during the armed conflict (7.45; 5.25–9.04) increased the odds of unplanned pregnancy by a factor of 3.12-times and 7.45-times, respectively, in this post war assessment in the conflict zones immediately after the armed conflict. Unless we retrospectively look for outdated research reports, unmet need of contraceptive due to unavailability of functional health facilities for family planning and other reproductive health services is not a problem anywhere currently. But, in our post-war assessment, the root cause for the extremely higher prevalence of unplanned pregnancy in the conflict zones were women could not get any type of contraceptives because of the colonization and destruction of health facilities by the armed forces. They could not even get post coital pills after sexual acts,whether the sex was voluntry or un-welcomed.
Study Limitations
Despite the novelty of the study to assess the effect of the armed conflict on unplanned pregnancy in the conflict zones of Ethiopia, the cross-sectional nature of the study might have chicken and egg like dilemma on the possible reasons of unplanned pregnancy. In addition the effect of religiosity on unplanned pregnancy was not addressed.
Conclusion and Recommendations
In this study nearly half (44.72%; CI=39.40–48.08%) of the pregnancies were unplanned, which is shocking to the health care system in the 21st century. Rural residency, being single, having an occupation of student and house wife, unmet need of family planning, and lack of a functioning health facility during the armed conflict were found to be the factors associated with unplanned pregnancy in this post war assessment of the conflict zones immediately after the armed conflict.
There should be an extensive health care mobilization including psychological and other health related infrastructure and even access to family planning options to reverse the unmet need of family planning methods in all the conflict zones. The impact of armed conflicts to the health care system should be protected by international laws.
Abbreviations
AOR, Adjusted odds ratio; BSc, Bachelor of Sciences; CI, Confidence interval; COR, Crude odds ratio; ETB, Ethiopian Birr; FP, family planning; SGZ, South Gondar zone; SPSS, Statistical Package for Social Sciences; TPLF, Tigray People Liberation Front; VIF, variance inflation factor; WHO, World Health Organization.
Data Sharing Statement
All data included in this manuscript can be accessed from the corresponding author upon request through the email address after the negotiation is over. In addition, the authors don’t have any access privileges that others don’t have.
Acknowledgments
We are thankful to Debre Tabor University for giving us ethical clearance. We are also grateful to the data collectors, women who participated in the data collection, hospital managers, health professionals, and all individuals who were willing to support us in any kind.
Author Contributions
All authors made a significant contribution to the work reported and took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that they have no competing interests.
References
1. Alene M, Yismaw L, Berelie Y, Kassie B, Yeshambel R, Assemie MA. Prevalence and determinants of unintended pregnancy in Ethiopia: a systematic review and meta-analysis of observational studies. PLoS One. 2020;15(4):e0231012. doi:10.1371/journal.pone.0231012
2. Goshu YA, Yitayew AE, Adu-Afarwuah S. Prevalence and determinant factors of unintended pregnancy among pregnant women attending antenatal clinics of Addis Zemen hospital. PLoS One. 2019;14(1):e0210206. doi:10.1371/journal.pone.0210206
3. Ikamari L, Izugbara C, Ochako R. Prevalence and determinants of unintended pregnancy among women in Nairobi, Kenya. BMC Pregnancy Childbirth. 2013;13(1):1–9. doi:10.1186/1471-2393-13-69
4. Kassa GM, Arowojolu A, Odukogbe A, Yalew AW. Prevalence and determinants of adolescent pregnancy in Africa: a systematic review and meta-analysis. Reprod Health. 2018;15(1):1–17. doi:10.1186/s12978-018-0640-2
5. Mohamed EA, Hamed AF, Yousef F, Ahmed EA. Prevalence, determinants, and outcomes of unintended pregnancy in Sohag district, Egypt. J Egypt Public Health Assoc. 2019;94(1):1–9. doi:10.1186/s42506-018-0001-6
6. Ali SA, Tikmani SS, Qidwai W. Prevalence and determinants of unintended pregnancy: systematic review. World Fam Med J. 2016;99(3671):1–10.
7. Yaya S, Amouzou A, Uthman OA, et al. Prevalence and determinants of terminated and unintended pregnancies among married women: analysis of pooled cross-sectional surveys in Nigeria. BMJ Global Health. 2018;3(2):e000707. doi:10.1136/bmjgh-2018-000707
8. Lamina MA. Prevalence and determinants of unintended pregnancy among women in South-Western Nigeria. Ghana Med J. 2015;49(3):187–194. doi:10.4314/gmj.v49i3.10
9. Tsegaye AT, Mengistu M, Shimeka A. Prevalence of unintended pregnancy and associated factors among married women in west Belessa Woreda, Northwest Ethiopia, 2016. Reprod Health. 2018;15(1):1–8. doi:10.1186/s12978-018-0649-6
10. Bearak J, Popinchalk A, Alkema L, Sedgh G. Global, regional, and subregional trends in unintended pregnancy and its outcomes from 1990 to 2014: estimates from a Bayesian hierarchical model. Lancet Global Health. 2018;6(4):e380–e389. doi:10.1016/S2214-109X(18)30029-9
11. World Health Organization. Trends in Maternal Mortality: 1990–2015: Estimates from WHO, UNICEF, UNFPA, World Bank Group and the United Nations Population Division. World Health Organization; 2015.
12. Palamuleni ME, Adebowale AS. Prevalence and determinants of unintended pregnancies in Malawi. Afr Popul Stud. 2014;28(1):551–563. doi:10.11564/28-1-507
13. Sharief M, Alharoon D, Mohammed H. Inhibin B as a marker for detection of ovarian activity in premature ovarian failure. J Womens Health Care. 2018;7(03):2167–0420.1000434. doi:10.4172/2167-0420.1000434
14. Feyisso M, Girma A, Yimam H, Hailu S. Magnitude of unintended pregnancy and its determinants among pregnant women visiting Dilla University Referral Hospital, South Ethiopia. J Womens Health Care. 2017;6(388):2167–0420.1000388. doi:10.4172/2167-0420.1000388
15. Worku S, Fantahun M. Unintended pregnancy and induced abortion in a town with accessible family planning services: the case of Harar in eastern Ethiopia. Ethiop J Health Dev. 2006;20(2):79–83.
16. Teshome FT, Hailu AG, Teklehaymanot AN. Prevalence of unintended pregnancy and associated factors among married pregnant women in Ganji woreda, west Wollega Oromia region, Ethiopia. Sci J Public Health. 2014;2(2):92–101.
17. Ayele M, Hamba N, Gudeta B. Assessment of the prevalence of unplanned pregnancy and associated factors among pregnant women attending antenatal care unit at Hambiso Health Center Hambiso, North Shewa, Ethiopia. J Womens Health Care. 2017;6(408):2167–0420.1000408.
18. Gizaw W, Fetene G, Mohammed S, Alemu A. Magnitude of unplanned pregnancy and its associated factors among pregnant women attending antenatal care at Tepi General Hospital Sheka Zone, Southwest Ethiopia, 2017. Insights Reprod Med. 2018;2(2):1.
19. Hall JA, Barrett G, Phiri T, Copas A, Malata A, Stephenson J. Prevalence and determinants of unintended pregnancy in Mchinji District, Malawi; using a conceptual hierarchy to inform analysis. PLoS One. 2016;11(10):e0165621. doi:10.1371/journal.pone.0165621
20. Ameyaw EK, Budu E, Sambah F, et al. Prevalence and determinants of unintended pregnancy in sub-Saharan Africa: a multi-country analysis of demographic and health surveys. PLoS One. 2019;14(8):e0220970. doi:10.1371/journal.pone.0220970
21. Okonofua FE, Odimegwu C, Ajabor H, Daru PH, Johnson A. Assessing the prevalence and determinants of unwanted pregnancy and induced abortion in Nigeria. Stud Fam Plan. 1989;20:342–355.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.