Back to Journals » International Journal of General Medicine » Volume 18
Post-Vaccination COVID-19 Side Effects and ABO Blood Type Correlation Among Healthcare Workers in Saudi Arabia: A Cross-Sectional Analysis
Authors Kabrah SM ![]()
Received 30 May 2025
Accepted for publication 25 August 2025
Published 29 August 2025 Volume 2025:18 Pages 4911—4922
DOI https://doi.org/10.2147/IJGM.S543906
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Woon-Man Kung
Saeed M Kabrah
Department of Clinical Laboratory Sciences, Faculty of Applied Medical Sciences, Umm Al-Qura University, Makkah, Eastern Province, Saudi Arabia
Correspondence: Saeed M Kabrah, Department of Clinical Laboratory Sciences, Faculty of Applied Medical Sciences, Umm Al-Qura University, Makkah, Saudi Arabia, Email [email protected]
Background: The global vaccination campaign against COVID-19 has necessitated monitoring vaccine-related adverse events among healthcare workers. This study aims to elucidate the relationship between ABO blood groups and the prevalence and perception of post-vaccination symptoms in this cohort.
Methods: A cross-sectional survey was conducted among 379 healthcare workers to collect demographic data, blood group information, vaccination status, symptom onset and duration, the impact of symptoms on work, and the efficacy of symptom relief measures.
Results: A total of 61.5% of participants reported post-vaccination symptoms, with those of blood group O showing the highest impact on work performance (51.2%). The chi-square test revealed no statistically significant association between blood group and the effect on work performance (p = 0.638). Although 7.9% of respondents reported being unable to perform surgeries due to symptoms, most continued working. Symptom onset varied without a significant difference across blood groups (p = 0.176). Vomiting was the only symptom significantly associated with ABO blood group (p = 0.012). The majority of respondents (77.2%) found analgesics, such as paracetamol or nonsteroidal anti-inflammatory drugs (NSAIDs), helpful in managing their symptoms, with no significant differences observed by blood group (p = 0.875). Regarding immune response expectations, 47.2% of participants felt their symptoms aligned with the expected vaccine effects, while 39.4% felt the symptoms were worse than anticipated.
Conclusion: Healthcare workers, especially those with Type O blood, reported greater disruption to work following COVID-19 vaccination. While most symptoms were not significantly associated with blood type, vomiting was an exception. These findings support the need for targeted post-vaccination monitoring and improved communication to manage expectations and side effects.
Keywords: COVID-19 vaccine, healthcare workers, ABO blood group, post-vaccination symptoms, symptom management, vaccine side effects, analgesics, immune response
Introduction
The coronavirus disease 2019 (COVID-19) pandemic has highlighted the vital role of vaccines in controlling infectious diseases. With the global rollout of COVID-19 vaccines, monitoring and understanding post-vaccination side effects have become imperative, especially among healthcare workers who are at the frontline of the pandemic response.1–3 Post-vaccination symptoms can range from mild, transient effects to more severe reactions, potentially affecting work capacity and healthcare service delivery.1,4
The ABO blood group system has been hypothesised to play a role in infectious diseases, with some studies suggesting blood-type-specific susceptibilities to specific pathogens. However, the association between ABO blood types and the prevalence or severity of COVID-19 vaccine side effects remains poorly understood.5–7 This is particularly relevant in countries like Saudi Arabia, where healthcare workers not only contend with the demands of their profession but also with the added pressure of pandemic-related healthcare challenges.2 Understanding these relationships is critical not only for enhancing the well-being of healthcare workers but also for informing vaccination protocols, post-vaccination care, and workplace policies that can support this essential workforce. Insights gleaned from this research may contribute to the broader knowledge base surrounding vaccine pharmacovigilance. They could potentially influence strategies to mitigate side effects in populations at high risk of exposure to severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2).
This study aims to investigate the relationship between ABO blood groups and the occurrence of post-vaccination side effects among healthcare workers in Saudi Arabia. It further examines the impact of these side effects on the professional duties of healthcare workers, including their ability to work and perform critical tasks, such as surgeries. In addition, the study examines the effectiveness of common symptom relief measures, such as the use of paracetamol and nonsteroidal anti-inflammatory drugs (NSAIDs), as well as the workers’ perceptions of their immune response to the vaccine.
Method
Study Design and Participants
This cross-sectional study was conducted across multiple healthcare institutions in five regions of Saudi Arabia (Western, Central, Northern, Southern, and Eastern) between January and December 2023, targeting healthcare workers employed in government, private, and non-profit hospitals. Participants were recruited from both clinical and pre-hospital settings, including emergency units, operating rooms, and general wards. The participants included both medics and paramedics who had received at least one dose of a COVID-19 vaccine. Healthcare workers who had not been vaccinated or had not been diagnosed with COVID-19 within 30 days before the survey were excluded to eliminate the possibility of confounding symptoms from active infections. The final sample consisted of 379 Saudi healthcare workers, both male and female, aged 20 years and older. The age group of 20 years and above was selected to ensure inclusion of professionally active healthcare workers who are legally eligible to provide informed consent. In Saudi Arabia, individuals typically enter the healthcare workforce at this age or older, making them relevant to the study’s focus on vaccine response and occupational health. This criterion also helped minimise variability related to age-dependent immune responses and ensured ethical participation. Participants were selected through a cluster random sampling method.
Sample Size Calculation
The sample size was determined based on a 95% confidence level and a 5% margin of error. Given the target population of healthcare workers across Saudi Arabia, a minimum sample size of 370 was calculated, which was subsequently rounded to 379 to account for potential non-responses.
Questionnaire Design and Data Collection
Data were collected through a self-administered questionnaire distributed electronically via internal hospital communication channels and professional social media networks, enabling a broad reach within the healthcare worker community. Participation was entirely voluntary, and reminders were issued two months after the initial distribution to enhance response rates.
The structured questionnaire was developed to gather detailed data on the participants’ demographic profiles and their experiences following COVID-19 vaccination. The first section collected demographic information, such as age, gender, marital status, professional designation (medic or paramedic), years of experience, educational background, and monthly income. The second section focused on the specifics of the COVID-19 vaccination, including the type of vaccine received, the number of doses administered, and the date of the last dose to account for any time-dependent side effects. Participants were also asked to report their ABO blood group.
In the post-vaccination symptoms section, participants were asked to detail any adverse reactions they experienced, including the onset, duration, and nature of the symptoms. Further questions explored how these symptoms impacted their professional duties, particularly for those performing tasks like surgery. Participants also provided information on any measures they took to alleviate symptoms, such as using over-the-counter medications like paracetamol or NSAIDs, taking rest, or seeking medical advice. Participants also provided information on any measures they took to alleviate symptoms, such as using over-the-counter medications like paracetamol or NSAIDs, taking rest, or seeking medical advice. Additionally, the survey included questions regarding participants’ expectations of the vaccine’s efficacy and whether their immune response post-vaccination aligned with these expectations. It is essential to note that the perception of a “proper immune response” was based solely on the participants’ subjective self-assessment, rather than on any clinical or laboratory confirmation, such as antibody testing. Therefore, participants’ impressions of whether their symptoms matched or exceeded expectations reflect personal interpretation rather than validated immunological outcomes. The questionnaire featured multiple-choice and yes/no questions to simplify completion and ensure clarity of responses.
Immunology, epidemiology, and survey methodology experts reviewed and validated the questionnaire to ensure the content was relevant and precise. A pilot test with a small group of healthcare workers helped refine the questions, estimate the time required for completion, and assess the user-friendliness of the survey. The reliability of the questionnaire was measured using Cronbach’s alpha coefficient (α = 0.061), ensuring internal consistency and stability.
Ethical Considerations
This study was approved by the Institutional Review Board at the Faculty of Medicine, King Saud University, Riyadh, Saudi Arabia (approval number: E-22-7389). It was conducted in accordance with the principles outlined in the Declaration of Helsinki. Participation was entirely voluntary. All participants provided electronic informed consent before beginning the survey, after being fully informed of the study’s objectives, data confidentiality measures, and their right to withdraw at any time. All responses were anonymous and used exclusively for research purposes.
Statistical Analysis
Descriptive statistics were used to summarise demographic characteristics and responses to the questionnaire. Age was categorised into nine groups to capture differences across career stages (eg, early, mid, and late-career professionals) and to explore potential age-related variability in immune response and perception of side effects Associations between ABO blood groups and key variables, such as vaccine type, post-vaccination symptoms, work impact, and effectiveness of symptom relief measures, were evaluated using the Chi-square (χ²) test. For variables where a statistically significant association was identified (p < 0.05), post hoc pairwise comparisons were conducted using the Bonferroni correction to control for Type I error across multiple comparisons. All analyses were performed using IBM SPSS Statistics for Mac, Version 29.0 (Armonk, NY, USA). A p-value less than 0.05 was considered statistically significant.
Results
Demographic, Professional, and COVID-19 Related Characteristics of Medical Professionals
The demographic and professional profiles of 386 medical professionals were assessed. The age distribution revealed that most participants were relatively young, with 36% aged between 20 and 25 years old, 21.4% in the 26–30 age group, and 13. % in the 31–35 years. Those aged 36–40 constituted 12.7%, while 7.5% were 41–45 years old. The remaining were over 45, with the least 1.8% above 60. Females accounted for 56.5% of the participants, while males represented 43.5%. When examining the residential area, the Western Region had the highest representation at 47.4%, followed by the Middle Region at 31.3%. The Northern, Southern, and Eastern regions had 6.7%, 3.9%, and 10.6% representation, respectively. Most participants were single (61.7%), with married individuals making up 35.8%. Participants who were divorced were notably fewer, (2.6%). Regarding education, most participants held a bachelor’s degree (62.2%), followed by those with a master’s degree (20.5%), and a minority had either a Ph.D. or a Medical Board (6.7%). Those with a diploma represented 10.6%. Income levels varied, with 44.3% of respondents earning up to 8699 Riyals per month. A similar proportion of participants earned between 8700 and 11999 Riyals (13.2%) and 12000 and 15299 Riyals (13.0%). Those earning between 15,300 and 20,159 Riyals comprised 14.2%, and the remaining earned more than 20,160 Riyals. Most participants were paramedics (80.3%), followed by medics. A significant majority (77.5%) worked in government hospitals, while private and non-profit hospitals employed 18.4% and 4.1%, respectively. The majority of participants had less than one year of work experience (early career, 34.7%), while 21% were in late career experience, with more than 10 years of work experience. The remaining participants were in mid-career. Regarding blood group distribution, it was O>A>B>AB (50.4%, 31.1%, 14.5% and 3.9%). The history of COVID-19 infection was reported by 53.9% of participants, while 45.1% did not report any previous infection. Notably, 97.9% of the participants had received the COVID-19 vaccine, while 2.1% had not received the vaccine (Table 1).
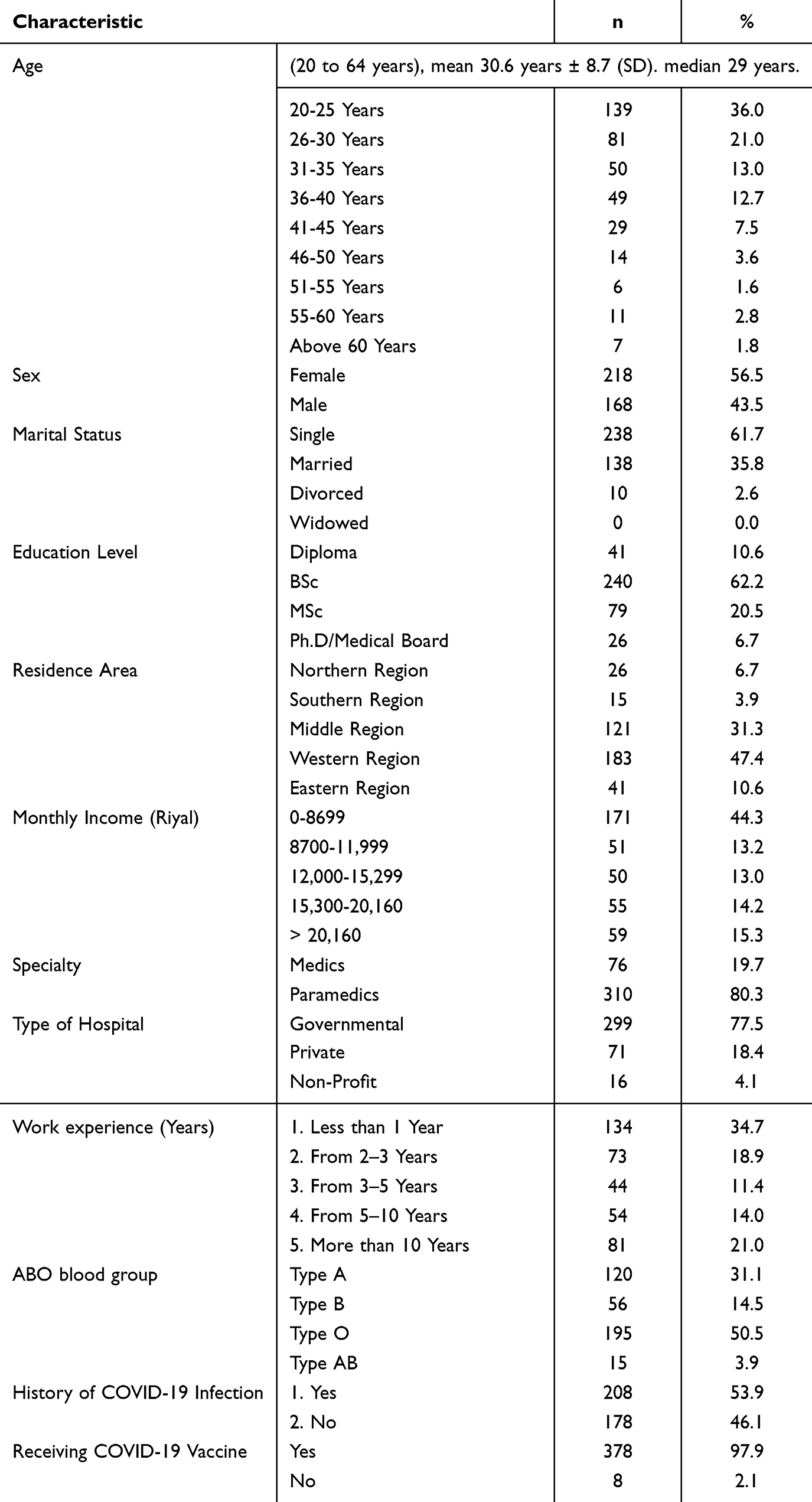 |
Table 1 Characteristics of the Study Participants (n=386) |
Vaccination Patterns and Blood Group Distribution Among Healthcare Workers
A total of 378 participants were included in the analysis of vaccine dose and type by ABO blood group (Table 2). The distribution of the number of COVID-19 vaccine doses received varied significantly across blood groups (χ² = 17.129, p = 0.047). The majority of participants (82.8%) received three doses, with the highest proportion among individuals with blood group O (43.9%), followed by group A (25.1%), group AB (11.4%), and group B (2.4%). Only a small fraction (5.6%) received four doses, with minimal variation between blood groups. Notably, Bonferroni-adjusted pairwise comparisons revealed that the proportion of participants with blood group O who received four doses was significantly higher than those with blood group AB (p < 0.05). Participants receiving only one dose represented 1.6% of the total sample, with no significant pairwise differences observed.
 |
Table 2 Distribution of COVID-19 Vaccine Doses Received and Vaccine Types Administered Among Medical Professionals Categorised by ABO Blood Group (n=378) |
In terms of vaccine type, most participants received the Pfizer-BioNTech vaccine (88.6%), followed by the AstraZeneca vaccine (37.6%) and the Moderna vaccine (14.6%). The distribution of vaccine types across ABO blood groups did not show statistically significant differences (p > 0.05). No significant pairwise differences were observed between blood groups in relation to the type of vaccine received after Bonferroni correction.
Post-Vaccination Adverse Events and Their Correlation with ABO Blood Groups Among Healthcare Workers
Among the 378 healthcare professionals included in the analysis (Table 3), 60.3% (n = 228) reported experiencing at least one symptom after receiving the COVID-19 vaccination. The distribution of post-vaccination symptoms did not significantly differ across ABO blood groups (χ² = 1.759, p = 0.624). Regarding the onset period of symptoms, although the most common time frames were 24 hours (15.1%) and more than 48 hours (15.3%) post-vaccination, the differences across blood groups were not statistically significant (χ² = 30.464, p = 0.170). Analysis of individual adverse events revealed that vomiting was the only symptom with a statistically significant association with ABO blood group (χ² = 10.892, p = 0.012). Bonferroni-adjusted post hoc comparisons indicated that participants with blood group A reported vomiting more frequently than those with blood group O. No cases of vomiting were reported among blood group AB or B participants. Other adverse events, such as headache (31.5%), tiredness (36.0%), fever (41.3%), body ache (19.3%), and joint pain (19.8%), were commonly reported but did not show statistically significant differences across blood groups (all p > 0.05). Similarly, rarer side effects such as allergic rash, syncope, and diarrhoea showed no significant variation by blood type.
 |
Table 3 Prevalence of Adverse Events Post-COVID-19 Vaccination in Relation to ABO Blood Groups Among Healthcare Professionals (n=378) |
These findings suggest that while most adverse symptoms post-vaccination were evenly distributed among ABO blood groups, vomiting may be more prevalent in certain blood types, affirming further investigation.
Impact of Post-Vaccination Symptoms on Work and Symptom Relief Measures by ABO Blood Group in Healthcare Workers
Out of 378 participants, 127 healthcare workers (55.7%) reported that post-vaccination symptoms affected their work (Table 4). The distribution across blood groups was not statistically significant (χ² = 0.987, p = 0.804), with the highest proportion in blood group O (28.5%).
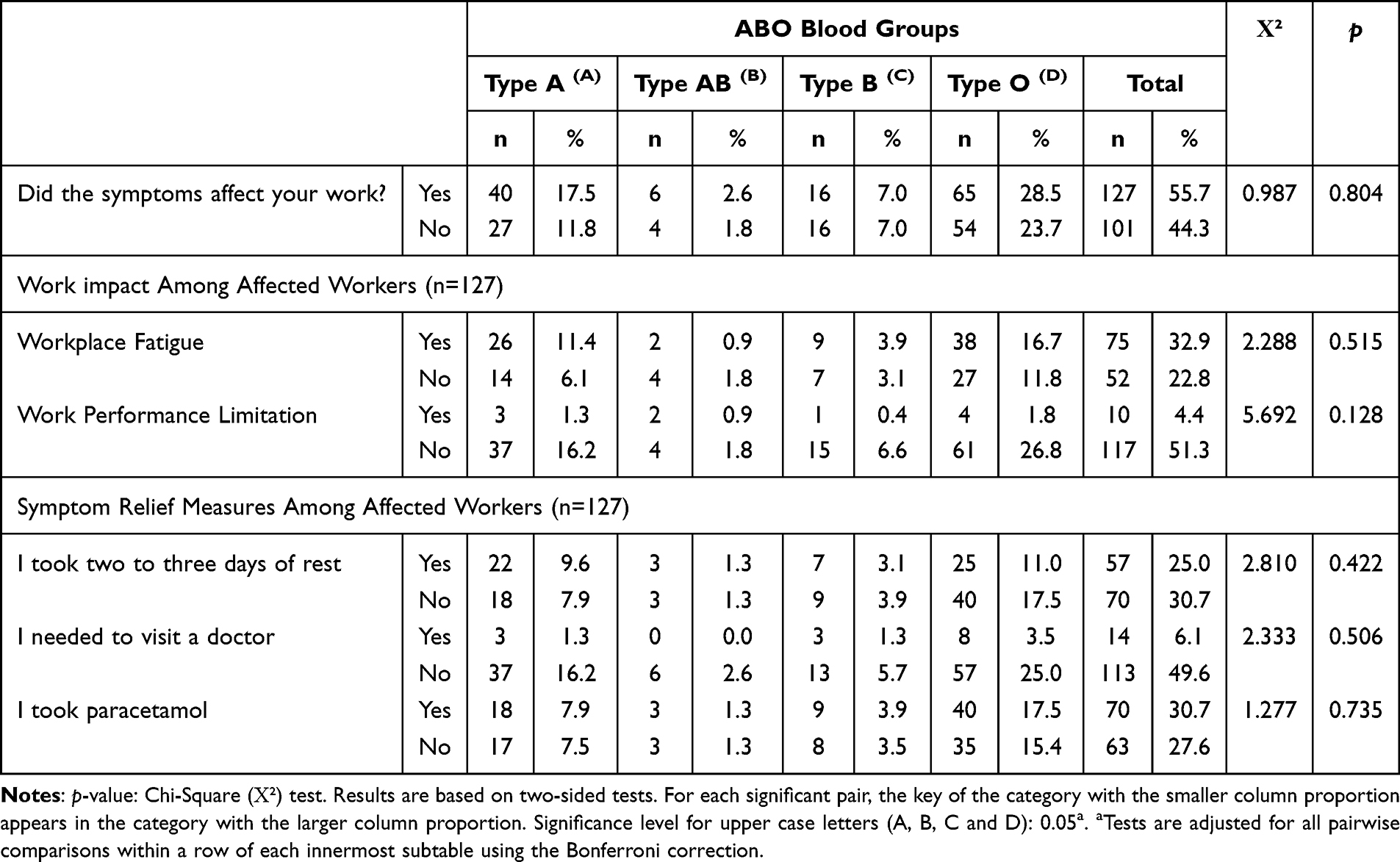 |
Table 4 Association of ABO Blood Group with Work-Related Impact and Symptom Relief Strategies Post-COVID-19 Vaccination |
Among those affected, workplace fatigue was the most frequently reported impact (32.9%), especially among participants with blood group O (16.7%). However, the association between blood group and workplace fatigue was not statistically significant (χ² = 2.288, p = 0.515). Similarly, worker performance limitations were reported by 10 participants (4.4%), with no significant difference across blood groups (χ² = 5.692, p = 0.128). In terms of symptom relief measures, 25.0% of affected individuals reported taking two to three days of rest, and 6.1% visited a doctor. Paracetamol was the most used remedy (30.7%), with the highest usage reported among individuals with blood group O (17.5%). None of these measures showed a significant association with blood group (rest: p = 0.422, doctor visit: p = 0.506, paracetamol use: p = 0.735).
These findings suggest that while a considerable proportion of vaccinated healthcare workers experienced temporary work-related impact due to symptoms, these effects were not significantly associated with ABO blood type.
Symptom Management and Immune Response Perception by ABO Blood Group
Among the 288 vaccinated healthcare workers analysed, 44.3% (n = 101) reported not taking any symptomatic relief medications such as NSAIDs (Table 5). The distribution across ABO blood groups was not statistically significant (χ² = 4.109, p = 0.662), with the highest proportions in blood groups A (11.8%) and O (7.0%).
 |
Table 5 Effectiveness of Symptomatic Treatment and Expectations of Immune Response by ABO Blood Group in Post-Vaccination Healthcare Workers (n=288) |
When asked whether the post-vaccination symptoms matched their expectations of an immune response, 26.3% of participants (n = 60) responded positively, stating they were satisfied with their body’s reaction. This perception was most commonly reported among individuals with blood group A (9.6%) and O (11.4%). A smaller proportion (7.5%) expected more symptoms than they experienced, while 21.9% (n = 50) indicated the symptoms were worse than anticipated. These differences in perception were not statistically significant across blood groups (p > 0.05 for all comparisons).
These findings suggest that there was no significant association between ABO blood group and either the choice to use symptom-relief medications or the perceived alignment of symptoms with expectations of immune response expectations.
Discussion
This study sheds light on the critical issue of post-vaccination adverse effects among healthcare workers in Saudi Arabia, with a focus on the role of ABO blood groups in influencing these outcomes. The findings have significant implications for healthcare management, particularly in environments where the workforce has been heavily relied upon during the COVID-19 pandemic. Understanding how vaccination impacts healthcare workers is crucial for developing effective support systems, maintaining productivity, and ensuring the well-being of these essential professionals.2,8
The fact that 32.9% of participants reported fatigue during work hours post-vaccination indicates that even mild or moderate side effects could affect daily operational efficiency in healthcare settings. Fatigue and other symptoms, such as severe local pain (29.6%) and headaches (31.5%), have the potential to reduce the performance of healthcare workers, especially those in high-pressure roles like paramedics and medics, who made up the bulk of this study’s participants. Similarly, a Saudi Arabian study involving general surgeons found a critical issue of post-vaccination adverse effects among health workers.2,8 These findings align with the current results, which suggest that this presents a critical challenge for hospital administrators and healthcare policymakers, as reduced workforce efficiency can hinder patient care quality and slow down essential healthcare services.9,10 In response to these findings, healthcare systems should consider implementing short-term workforce management strategies, such as flexible work hours, temporary workload reductions, or additional paid leave for staff who report significant post-vaccination symptoms.11
Additionally, the study’s finding that 4.4% of participants reported being unable to perform surgical procedures due to vaccine-related symptoms raises concerns about the potential for disruption in critical care services. Although the number appears small, in a healthcare environment already strained by the demands of the pandemic, even a slight reduction in capacity for performing surgeries or other high-skill tasks can exacerbate backlogs and negatively affect patient outcomes.11 This reinforces the importance of monitoring healthcare workers’ post-vaccination health closely, offering targeted support when needed, and ensuring that staffing levels can accommodate potential reductions in workforce availability during vaccination periods.12
Healthcare administrators must also pay attention to the fact that many participants chose self-care measures, such as using over-the-counter medications (49.6%) and rest (44.9%), rather than seeking medical consultation (only 11.0% did so). This reliance on self-management may indicate a reluctance among healthcare workers to further burden an already stretched healthcare system.13,14 However, it could also reflect an underestimation of the importance of addressing post-vaccination symptoms through professional medical guidance. This highlights the need for healthcare management to promote better awareness among staff about the importance of seeking appropriate medical care and support, rather than relying solely on self-care, to ensure they recover fully and can return to work at full capacity.
While previous studies have suggested that individuals with blood group O may have a lower susceptibility to SARS-CoV-2 infection and milder disease progression,2,7,8 the findings show that this group reported a higher rate of post-vaccination symptoms that impacted work performance. The reason for this discrepancy is not fully understood. One possible explanation may relate to innate immune response differences or inflammatory mediators associated with ABO antigens; however, these mechanisms were not evaluated in the current study or in other studies. Currently, there is limited literature directly supporting an increased susceptibility to vaccine-related adverse effects among individuals with blood group O. Some studies have indicated differing immune responses or symptom profiles post-infection or vaccination,6,15 but the findings remain inconsistent and inconclusive. Therefore, this unexpected trend observed in our study warrants further investigation in larger cohorts with immunological profiling to better understand the biological basis and clinical relevance of ABO blood group-related vaccine reactogenicity. Another nationwide study in Saudi Arabia reinforced these conclusions, finding no significant correlation between ABO blood group and the severity of vaccine-related adverse events, but highlighting other factors (such as gender, education level, and general health status) as more significant predictors of severe side effects. Both studies recommend further research to clarify these relationships in broader healthcare populations.16 These findings also align with international investigations that have reported that adverse events following vaccination were equally distributed across all ABO blood groups, with no significant differences in side effect profiles.17
This knowledge has critical implications for vaccine distribution and follow-up care strategies. Healthcare providers and policymakers could consider ABO blood groups when designing vaccination protocols or post-vaccination monitoring systems, allowing for more personalised care approaches.3 For instance, if further studies corroborate a heightened vulnerability to specific side effects in certain blood groups, those individuals could receive more targeted advice and care following their vaccinations. This approach could also help alleviate some of the hospital’s workload pressures by proactively addressing issues that may cause workers to take time off due to vaccine-related symptoms.18,19
The results of this study are of particular importance in the context of ongoing and future mass vaccination campaigns, whether related to COVID-19 boosters, new strains, or other vaccines. Several studies emphasise the need for a similar approach where they suggest a robust evaluation of AEFI protects both public health and healthcare staff, ensuring the smooth rollout of booster and future vaccination campaigns while maintaining public confidence.20 The lessons learned from how healthcare workers, the backbone of any healthcare system, respond to vaccination can inform broader public health strategies to minimise disruptions to essential services. Healthcare institutions can use this data to improve vaccine education programs, ensuring that healthcare workers have realistic expectations about post-vaccination symptoms and are prepared to manage them appropriately. Improved understanding and management of vaccine side effects could lead to higher vaccine uptake, especially in populations where hesitancy may be driven by fear of adverse reactions.18
The relatively low correlation between symptoms and ABO blood groups (p-values above 0.05 for most symptoms) also reinforces the need for comprehensive research that incorporates other variables, such as gender, genetic factors, environmental influences, or prior health conditions, in understanding individual responses to vaccination.1–3,11,21,22 By expanding the scope of inquiry beyond blood types, future research could uncover a more detailed understanding of the factors contributing to vaccine response variability.9,13
Another area that deserves further exploration is the discrepancy between healthcare workers’ expectations of immune responses and their actual experiences.11,23,24 A substantial proportion of participants felt their adverse effects were more severe than expected, which could indicate gaps in culture and communication or education about the expected side effects of vaccination.18 Strengthening the education and communication around vaccine safety, particularly for healthcare professionals, is critical to ensuring informed consent and maintaining trust in vaccination programs.
Conclusion
This study found no statistically significant association between ABO blood groups and most post-COVID-19 vaccination symptoms among healthcare workers in Saudi Arabia. However, individuals with blood group O reported a higher frequency of symptoms that negatively impacted their work performance, including fatigue, headache, and reduced ability to perform tasks such as surgery. Vomiting was the only symptom with a statistically significant correlation to blood group (p = 0.012).
Most participants used over-the-counter medications, such as paracetamol or NSAIDs, for symptom relief, and the majority found these effective, regardless of their blood type. Self-reported perceptions of immune response varied, with nearly half of the participants feeling that their symptoms matched expectations; however, this perception did not differ significantly by blood group.
These findings highlight the complexity of post-vaccination responses and the importance of recognising individual variability, even within a professional population. While ABO blood group may not be a decisive factor in vaccine-related side effects, the trend observed in blood group O suggests the need for further research into genetic or immunological factors influencing vaccine reactogenicity. Healthcare systems should consider proactive monitoring and supportive interventions for staff experiencing side effects to maintain workforce resilience and service continuity during mass vaccination efforts.
Data Sharing Statement
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.
Institutional Review Board Statement
The study received ethical approval from the Institutional Review Board of the College of Medicine, King Saud University, Saudi Arabia (E-22-7389).
Acknowledgments
I extend my heartfelt gratitude to the numerous research teams whose dedication and expertise in developing the current tools and databases have facilitated my study. Their contributions to the scientific community have not only enabled my research but have also significantly advanced the field of biomedical research. Their tireless efforts in creating and maintaining these valuable resources gave us the foundation to conduct my analysis and draw meaningful conclusions. I sincerely appreciate their commitment to advancing knowledge and their support in making this study possible.
Author Contribution
Dr Saeed Kabrah made a significant contribution to the work reported, including the conception, study design, execution, data acquisition, analysis, and interpretation. The author took part in drafting, revising, and critically reviewing the article; gave final approval of the version to be published; has agreed on the journal to which the article has been submitted; and agrees to be accountable for all aspects of the work.
Funding
This research received no external funding.
Disclosure
The author listed in this manuscript certify that he has no affiliations with or involvement in any organization or entity with any financial interest (such as honoraria, educational grants, participation in speakers’ bureaus, membership, employment, consultancies, stock ownership, or other equity interest; and expert testimony or patent-licensing arrangements), or non-financial interest (such as personal or professional relationships, affiliations, knowledge or beliefs) in the subject matter or materials discussed in this manuscript.
References
1. Alemayehu A, Demissie A, Yusuf M, et al. COVID-19 vaccine side effect: age and gender disparity in adverse effects following the first dose of AstraZeneca COVID-19 vaccine among the vaccinated population in Eastern Ethiopia: a community-based study. SAGE Open Med. 2022;10:20503121221108616. doi:10.1177/20503121221108616
2. Alessa MY, Aledili FJ, Alnasser AA, et al. The side effects of COVID-19 vaccines and its association with ABO blood type among the general surgeons in Saudi Arabia. Cureus. 2022;14(3). doi:10.7759/cureus.23628
3. Jensen A, Stromme M, Moyassari S, et al. COVID-19 vaccines: considering sex differences in efficacy and safety. Contemp Clin Trials. 2022;115:106700. doi:10.1016/j.cct.2022.106700
4. Pilishvili T, Fleming-Dutra KE, Farrar JL. Interim estimates of vaccine effectiveness of Pfizer-BioNTech and Moderna COVID-19 vaccines among health care personnel—33 US sites, January–March 2021. MMWR Morb Mortal Wkly Rep. 2021;70 20 753–758. doi:10.15585/mmwr.mm7020e2
5. Zhao J, Yang Y, Huang H, et al. Relationship between the ABO blood group and the coronavirus disease 2019 (COVID-19) susceptibility. Clinl Infect Dis. 2021;73(2):328–331. doi:10.1093/cid/ciaa1150
6. Kabrah SM, Abuzerr SS, Baghdadi MA, et al. Susceptibility of ABO blood group to COVID-19 infections: clinico-hematological, radiological, and complications analysis. Medicine. 2021;100(52):e28334. doi:10.1097/MD.0000000000028334
7. Kabrah SM, Kabrah AM, Flemban AF, Abuzerr S. Systematic review and meta-analysis of the susceptibility of ABO blood group to COVID-19 infection. Transfus Apher Sci. 2021;60(4):103169. doi:10.1016/j.transci.2021.103169
8. Almalki OS, Khalifa AS, Alhemeidi OF, Ewis AA, Shady AM, Abdelwahab SF. Correlation between the severity of COVID-19 vaccine-related adverse events and the blood group of the vaccinees in Saudi Arabia: a web-based survey. Front Pharmacol. 2022;13:1006333. doi:10.3389/fphar.2022.1006333
9. Elamin MY, Maslamani YA, Muaddi MA, et al. Real-world effectiveness of COVID-19 vaccines: a retrospective cohort study of vaccinated individuals in Jazan, Saudi Arabia. J Infect Public Health. 2023;16(9):1512–1517. doi:10.1016/j.jiph.2023.06.014
10. Sagherian K, Clinton ME, Abu-Saad Huijer H, Geiger-Brown J. Fatigue, work schedules, and perceived performance in bedside care nurses. Workplace Health Saf. 2017;65(7):304–312. doi:10.1177/2165079916665398
11. Valdes-Fernandez BN, Duconge J, Espino AM, Ruano G. Personalized health and the coronavirus vaccines-Do individual genetics matter? Bioessays. 2021;43(9):e2100087. doi:10.1002/bies.202100087
12. Szabo S, Nove A, Matthews Z, et al. Health workforce demography: a framework to improve understanding of the health workforce and support achievement of the sustainable development goals. Hum Resour Health. 2020;18(1):7. doi:10.1186/s12960-020-0445-6
13. Barnes K, Faasse K, Colagiuri B. The impact of side effect framing on COVID-19 booster vaccine intentions in an Australian sample. Vaccine. 2023;41(12):2046–2054. doi:10.1016/j.vaccine.2023.02.023
14. Butt S, Raza A, Siddiqui R, Saleem Y, Cook B, Khan H. Healthcare employment landscape: comparing job markets for professionals in developed and developing countries. J Work-Applied Manag. 2023;16(1):84–96
15. Majumder MAA, Bharatha A, Kumar S, et al. Self-reported side effects of COVID-19 vaccines among health professions students in India. PeerJ. 2024;12:e17083. doi:10.7717/peerj.17083
16. Almalki OS, Santali EY, Alhothali AA, et al. The role of blood groups, vaccine type and gender in predicting the severity of side effects among university students receiving COVID-19 vaccines. BMC Infect Dis. 2023;23(1):378. doi:10.1186/s12879-023-08363-0
17. Pandit N, Patel N. Adverse event following immunization and relation with blood group following COVID19 vaccination among Indian community: a cross-sectional study. J Integrated Health Sci. 2021;9(2):60–64. doi:10.4103/jihs.jihs_29_21
18. Lu JG. Two large-scale global studies on COVID-19 vaccine hesitancy over time: culture, uncertainty avoidance, and vaccine side-effect concerns. J Pers Soc Psychol. 2023;124(4):683–706. doi:10.1037/pspa0000320
19. Chandra LA, Nirwati H, Nugroho D. Immediate adverse events following immunization (AEFI) in drive-through COVID-19 vaccination campaign in Yogyakarta, Indonesia: a cross-sectional study. Indian J Med Res 2024;160(3&4):362–370. doi:10.25259/IJMR_992_2024
20. Amer SA, Al-Zahrani A, Imam EA, et al. Exploring the reported adverse effects of COVID-19 vaccines among vaccinated Arab populations: a multi-national survey study. Sci Rep. 2024;14(1):4785. doi:10.1038/s41598-024-54886-0
21. Khashoggi BF, Murad A. Use of 2SFCA method to identify and analyze spatial access disparities to healthcare in Jeddah, Saudi Arabia. Appl Sci. 2021;11(20):9537.
22. Alshamrani MM, Farahat FM, El-Saed A, et al. Post-vaccination SARS-CoV-2 infection among healthcare workers in tertiary care hospitals in Saudi Arabia: a case series. J Infect Public Health. 2022;15(1):10–12. doi:10.1016/j.jiph.2021.11.015
23. Fox T, Geppert J, Dinnes J, et al. Antibody tests for identification of current and past infection with SARS-CoV-2. Cochrane Database Syst Rev. 2022;11(11):CD013652. doi:10.1002/14651858.CD013652.pub2
24. Yap C, Ali A, Prabhakar A, et al. Comprehensive literature review on COVID-19 vaccines and role of SARS-CoV-2 variants in the pandemic. Ther Adv Vaccines Immunother. 2021;9:25151355211059791. doi:10.1177/25151355211059791
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.