Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 16
Post-Treatment of Micro-Needling with a Dexpanthenol-Containing Ointment Accelerates Epidermal Wound Healing in Human 3D Skin Models
Authors Weßollek K, Marquardt Y, Wagner-Schiffler S, Baron JM, Huth S
Received 22 February 2023
Accepted for publication 22 May 2023
Published 14 June 2023 Volume 2023:16 Pages 1533—1538
DOI https://doi.org/10.2147/CCID.S409310
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Anne-Claire Fougerousse
Katharina Weßollek,1 Yvonne Marquardt,1 Sylvia Wagner-Schiffler,2 Jens Malte Baron,1,* Sebastian Huth1,*
1Department of Dermatology and Allergology, University Hospital RWTH Aachen, Aachen, Germany; 2Praxis für Dermatologie, Aachen, Germany
*These authors contributed equally to this work
Correspondence: Katharina Weßollek, Department of Dermatology and Allergology, University Hospital RWTH Aachen, Aachen, Germany, Tel +49 241 7501 8240, Fax +49 241 7501 8290, Email [email protected]
Purpose: In vitro study on the molecular effects of post-treatment after micro-needling applications with a dexpanthenol-containing ointment (DCO) using 3D skin models.
Patients and Methods: In this in vitro study, full-thickness human 3D skin models were treated with a micro-needling device according to its clinical application. For post-treatment, some of the models were additionally treated with a dexpanthenol-containing ointment (DCO). Histological samples were taken at 0, 24 and 48 hours. Gene expression analysis was performed after 24 hours.
Results: Histological examination showed that DCO post-treated 3D skin models revealed a completed wound closure 24 hours after the micro-needling procedure. In contrast, DCO-untreated models still clearly exhibited the micro-needling lesions after the same period of time. After 48 hours, all models revealed a completed wound healing. In skin models that received micro-needling but no post-treatment with DCO, microarray analysis identified an upregulation of proinflammatory cytokines and chemokines and a downregulation of skin barrier and differentiation markers. In contrast, post-treatment with DCO leads to accelerated wound healing without affecting the initial inflammatory response caused by micro-needling, which leads to the subsequent collagen expression. This data was supported by qRT-PCR analyses.
Conclusion: Post-treatment with DCO accelerates epidermal wound healing after micro-needling of 3D skin models without impairing the immunostimulatory properties of micro-needling. These findings can help to optimise the aftercare routine after micro-needling procedures and to shorten the downtime for the patient after treatment.
Keywords: in vitro models, cosmetic procedures, aftercare, skin needling, molecular effects, human organotypic skin equivalents
Introduction
Aesthetic dermatology has been on the rise for years. Micro-needling is a relatively new procedure. First described in 1995, it became more popular after the 2006 introduction of the product that later became the Dermaroller®.1–3
Micro-needling is safe and cost efficient. It is used to treat different dermatologic conditions, such as scars, alopecia and hyperhidrosis.1,2,4,5 In cosmetic dermatology micro-needling is used for skin rejuvenation.6 The 0.5–1.5 mm long needles penetrate the skin and the resulting lesions, although superficial, initiate the wound healing cascade.7 Activation of various growth factors leads to increased collagen synthesis.6 Gene expression and histopathological changes caused by micro-needling have been studied in animals, 3D skin models and humans.6–11 Upregulation of genes associated with wound healing, epithelial proliferation/differentiation, immune cell recruitment and tissue remodeling genes has been described.6 Micro-needling has relatively few side effects compared to other cosmetic procedures such as ablative laser treatment or dermabrasion.12 The importance of adequate post-procedural aftercare in cosmetic dermatology to prevent adverse events and optimize outcome is well documented.13–15 However, it is not known to date whether topical wound healing agents after micro-needling treatment may influence the effectiveness of the procedure. This study investigates the histological and underlying molecular effects of post-treatment after micro-needling applications with a dexpanthenol-containing ointment (DCO) using 3D skin models. Since we have previously shown that micro-needling mediates most of its effect on dermis remodeling via upregulation of pro-inflammatory genes, which then lead to chemotaxis of immune cells, it was important to prove that this initial inflammatory effect is not attenuated by topical aftercare.6
Material and Methods
Isolation and Cultivation of Normal Human Epidermal Keratinocytes (NHEK) and Normal Human Dermal Fibroblasts (NHDF)
Primary NHDF and NHEK cells were isolated and cultivated as described previously.16–18 This study was conducted in accordance with the Declaration of Helsinki. The ethics committee of University Hospital RWTH Aachen approved this study prior to its conduction. A written informed consent was obtained from all participants.
3D Skin Models and Micro-Needling Procedure
Full-thickness 3D skin models were developed as previously described.6 Construction of the dermal part was done by using a collagen-elastin scaffold (MatriDerm®, MedSkin Solutions Dr. Suwelack AG, Billerbeck, Germany) on which 2×105 NHDF cells were seeded in bovine collagen I solution (Vitrogen, Cohesion Technologies, Palo Alto, CA, USA). After incubating the models for two days at 37 °C and 5% CO2, 2×106 NHEK cells were seeded on top of the dermal equivalent. Next day, skin models were lifted to the air-liquid interface (ALI). On day 7 of ALI, micro-needling of the models was performed with amiea med® EXCEED (MT.DERM GmbH, Berlin, Germany) using a six needle plate (1.5 NM615LS16309, MT.DERM GmbH). One hundred insertions were made per second at a penetration depth of 1.0 mm and with three passes, according to the manufacturer´s and clinical treatment recommendations. Immediately after micro-needling, the models were topically treated with a dexpanthenol-containing wound care ointment (Bepanthen® wound and healing ointment; Bayer Vital, Leverkusen, Germany). After 24 and 48 hours models were harvested for histology and gene expression analyses. An untreated model was maintained as a negative control at any given time. Experiments were performed four times independently with three different cell donors.
RNA-Isolation and Microarray Analysis
Total RNA from the micro-needled 3D skin models was extracted with the Nucleo Spin RNA kit (Macherey and Nagel, Düren, Germany), according to the manufacturer’s instructions. Microarray analysis was done as previously described19 by using Clariom™ S assays (Thermo Fisher, Waltham, USA). Expression values of each probe set were determined and data were analyzed using the TAC software (Thermo Fisher Scientific) with normalization method quantile.
Real-Time PCR Analysis
Assessment of isolated RNA was carried out using NanoDrop (Thermo, Erlangen, Germany), and the RNA integrity was checked using the 2100 Bioanalyzer (Agilent Technologies, Palo Alto, CA, USA). Reverse transcriptase-PCR was performed with TaqMan Reverse Transcription Reagents (Applied Biosystems, Weiterstadt, Germany) and the qRT-PCR analyses were executed on an ABI PRISM 7300 Sequence Detection System (Applied Biosystems). Assay-on-Demand gene expression products (Applied Biosystems) were used to study quantitative expression of LOR (Hs01894962_m1), CXCL5 (Hs00171085_m1), CXCL8 (Hs00174103_m1), FLG (Hs00856927_g1), HRNR (Hs02385268_m1), IL36G (Hs00219742_m1), FGF2 (Hs00266645_m1), IL1A (Hs00174092_m1), IL1B (Hs00174097_m1), IL1RL1 (Hs00249384_m1), IL20 (Hs00218888_m1), IL37 (Hs00367201_m1), IL24 (Hs01114274_m1) and MMP3 (Hs00233962_m1).
Light Microscopy
For histological analyses, 5 µm cryosections of 3D skin models were embedded in Tissue-Tek O.C.T. ™ compound (Sakura Finetek). Sections were stained with haematoxylin and eosin (H&E) and subsequently assessed by a photomicroscope (DMIL, Leitz, Wetzlar, Germany).
Statistical Analyses
Data are given as arithmetical means ± standard deviation (SD). Mann–Whitney U-test was performed with GraphPad PRISM version 7 (La Jolla, CA, USA). Values of *p < 0.05 were considered significant and are indicated in the figures.
Results
Histological differences between the DCO post-treated and the DCO-untreated micro-needling skin models were visible (Figure 1). Complete wound closure was evident in the DCO post-treated models after 24 hours. In the DCO-untreated skin models, the micro-needling lesions were still clearly recognizable after 24 hours.
 |
Figure 1 Histological analysis of micro-needling-treated 3D skin models. Upper row shows hematoxylin and eosin stainings of untreated controls and skin models immediately after micro-needling treatment (0 h). The middle row shows untreated controls, micro-needling-treated models, and models that were additionally post-treated with DCO, 24 h after treatment. The bottom row shows the corresponding models 48 h after treatment. Shown are representative images from four independent experiments. h = hours. Scale bar: 200 µm. The black arrows indicate the lesions. |
Since there were no histological differences between the models after 48 hours, we focused our gene expression analysis at 24 hours after treatment (Figure 2).
 |
Figure 2 Gene expression profiling in micro-needling-treated 3D skin models. Microarray analysis in models 24 h after (a) micro-needling treatment in comparison to untreated controls, (b) micro-needling treatment and additional post-treatment with a dexpanthenol-containing ointment (DCO) in comparison to untreated controls, and (c) micro-needling treatment and additional post-treatment with DCO compared to micro-needling-treated models without post-treatment. |
In 3D-skin models that have been treated with micro-needling but have not received post-treatment with DCO, microarray analysis showed an upregulation of pro-inflammatory cytokines and chemokines (eg, IL1RL1, IL24, IL1a, CXCL8) compared to the controls that were not treated with micro-needling (Figure 2a). In addition, anti-inflammatory genes (IL37) as well as skin barrier and differentiation markers (filaggrin (FLG), loricrin (LOR), hornerin (HRNR)) were downregulated. Additional post-treatment of the micro-needling models with DCO also preserved the initial upregulation of inflammatory markers (eg, CXCL8, CXCL5, IL24), but revealed no downregulation of skin barrier and differentiation markers compared to untreated controls reflecting the accelerated wound closure (Figure 2b).
To study the effects of DCO separately, we also carried out a microarray analysis by examining gene regulation in micro-needling models post-treated with DCO compared to micro-needling models without post-treatment (Figure 2c). In particular, we detected an upregulation of skin barrier and epidermal differentiation-associated genes (eg HRNR, LOR, FLG) in the DCO post-treated models compared to the non-DCO post-treated micro-needling models.
Independent RT-PCR analyses confirmed the microarray data (Figure 3). While micro-needling caused a significant downregulation of differentiation markers (LOR, FLG) in contrast to the untreated controls, almost the same expression levels as in the untreated models were observed after treatment with DCO. On the other hand, post-treatment with DCO did not adversely regulate inflammation-associated genes (eg, CXCL5, IL36G, IL24) compared with models that received micro-needling alone.
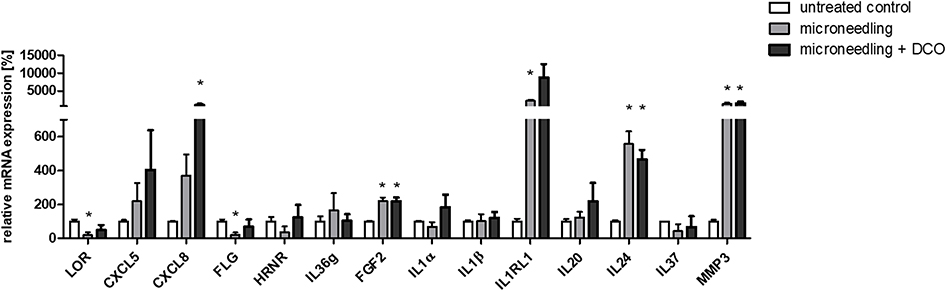 |
Figure 3 RT-PCR analysis of four independent experiments displaying the expression of selected genes. Selective gene expressions in micro-needling-treated skin models and micro-needling-treated skin models that received post-treatment with DCO were normalized to untreated controls. *p < 0.05. |
Discussion
Generally, the wound healing process is described in three overlapping phases. Inflammation phase begins immediately after injury occurs and usually lasts for 48–96 hours. The proliferative phase follows the inflammation phase and finally the wound enters its remodeling phase.20
Through micro-needling a controlled stimulus is set. This stimulus triggers the wound healing cascade. As mentioned above, an injury initially causes inflammation. Platelets and neutrophils migrate to the wound area.21 As a result, pro-inflammatory cytokines are released.21,22 The various growth factors activate epithelization23 and collagen synthesis is stimulated.24 The desired effect of micro-needling (collagen synthesis) is therefore created by the inflammatory stimulus.
In a previous paper we showed molecular changes at day 5 after micro-needling that are consistent with the timeline of the wound healing process described above. For instance, several collagen synthesizing genes (eg COL3A1, COL8A1) were upregulated. In contrast to ablative CO2 laser treatments these effects are not directly mediated, eg, by upregulation of heat shock proteins, but seem to be mainly conveyed indirectly by upregulation of inflammatory mediators and subsequent chemotaxis leading to the upregulation of collagen synthesis in dermal fibroblasts.6,17
Our present study, on the other hand, focused on investigating the molecular and histological changes in wound healing caused by post-treatment with DCO after micro-needling. We detected an upregulation of genes associated with epidermal differentiation and skin barrier forming (FLG, LOR) 24 hours after micro-needling and post-treatment with DCO.25,26
Aware of the wound healing cascade explained above, this is earlier than one would expect. Congruently, we did not detect an upregulation of such genes in the skin models not receiving DCO, strongly indicating that the molecular changes facilitating wound healing are attributed to DCO-post treatment. Topical dexpanthenol treatment has a variety of beneficial effects on intact skin. It moisturizes and hydrates, also minimizes transepidermal water loss.27,28 It is known that topical treatment with dexpanthenol accelerates wound healing in damaged skin. These insights have been demonstrated in several in vivo and in vitro studies.13,27,29,30
Moreover, and of high relevance, according to our findings, the desired inflammatory stimulus caused by micro-needling to trigger collagen synthesis remains unimpaired by applying DCO as aftercare. We conclude that DCO may provide an excellent after-treatment for micro-needling by accelerating wound healing while not interfering with molecular processes substantial to obtain optimal results regarding skin rejuvenation.
Conclusion
We provide evidence that post-treatment with a dexpanthenol-containing ointment after micro-needling facilitates epidermal wound healing without impairing the micro-needling-induced inflammatory response needed to achieve collagen induction. These findings can help to optimize the aftercare of micro-needling procedures in the future.
Acknowledgments
This work was supported by a grant from Bayer Vital GmbH.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Iriarte C, Awosika O, Rengifo-Pardo M, Ehrlich A. Review of applications of microneedling in dermatology. Clin Cosmet Investig Dermatol. 2017;10:289–298. doi:10.2147/CCID.S142450
2. Singh A, Yadav S. Microneedling: advances and widening horizons. Indian Dermatol Online J. 2016;7(4):244–254. doi:10.4103/2229-5178.185468
3. Doddaballapur S. Microneedling with dermaroller. J Cutan Aesthet Surg. 2009;2(2):110–111. doi:10.4103/0974-2077.58529
4. Juhasz MLW, Cohen JL. Microneedling for the treatment of scars: an update for clinicians. Clin Cosmet Investig Dermatol. 2020;13:997–1003.
5. Hou A, Cohen B, Haimovic A, Elbuluk N. Microneedling: a comprehensive review. Dermatol Surg. 2017;43(3):321–339. doi:10.1097/DSS.0000000000000924
6. Schmitt L, Marquardt Y, Amann P, et al. Comprehensive molecular characterization of microneedling therapy in a human three‐dimensional skin model. PLoS One. 2018;13(9):e0204318. doi:10.1371/journal.pone.0204318
7. Gupta AK, Quinlan EM, Venkataraman M, Bamimore MA. Microneedling for hair loss. J Cosmet Dermatol. 2022;21(1):108–117. doi:10.1111/jocd.14525
8. Bao L, Zong H, Fang S, Zheng L, Li Y. Randomized trial of electrodynamic microneedling combined with 5% minoxidil topical solution for treating androgenetic alopecia in Chinese males and molecular mechanistic study of the involvement of the Wnt/β-catenin signaling pathway. J Dermatol Treat. 2022;33(1):483–493. doi:10.1080/09546634.2020.1770162
9. Zeitter S, Sikora Z, Jahn S, et al. Microneedling: matching the results of medical needling and repetitive treatments to maximize potential for skin regeneration. Burns. 2014;40(5):966–973. doi:10.1016/j.burns.2013.12.008
10. Helbig D, Mobius A, Simon JC, Paasch U. Heat shock protein 70 expression patterns in dermal explants in response to ablative fractional photothermolysis, microneedle, or scalpel wounding. Wounds. 2011;23(3):59–67.
11. Abdou AG, Farag AGA, Rashwan M, Shehata WA. The clinical and pathological effectiveness of microneedling and topical 5-fluorouracil in vitiligo treatment: an association with matrix metalloproteinase 2 immunohistochemical expression. J Cosmet Dermatol. 2021;21(5):2153–2161.
12. Ramaut L, Hoeksema H, Pirayesh A, Stillaert F, Monstrey S. Microneedling: where do we stand now? A systematic review of the literature. J Plast Reconstr Aesthet Surg. 2018;71(1):1–14. doi:10.1016/j.bjps.2017.06.006
13. Gorski J, Proksch E, Baron JM, Schmid D, Zhang L. Dexpanthenol in wound healing after medical and cosmetic interventions (postprocedure wound healing). Pharmaceuticals. 2020;13(7):138. doi:10.3390/ph13070138
14. Baron JM, Glatz M, Proksch E. Optimal support of wound healing: new insights. Dermatology. 2020;236(6):593–600. doi:10.1159/000505291
15. Anitha B. Prevention of complications in chemical peeling. J Cutan Aesthet Surg. 2010;3(3):186–188. doi:10.4103/0974-2077.74500
16. Cornelissen C, Marquardt Y, Czaja K, et al. IL-31 regulates differentiation and filaggrin expression in human organotypic skin models. J Allergy Clin Immunol. 2012;129(2):426–433, 433.e421–428. doi:10.1016/j.jaci.2011.10.042
17. Schmitt L, Huth S, Amann PM, et al. Direct biological effects of fractional ultrapulsed CO2 laser irradiation on keratinocytes and fibroblasts in human organotypic full-thickness 3D skin models. Lasers Med Sci. 2017;33:765–772.
18. Marquardt Y, Amann PM, Heise R, et al. Characterization of a novel standardized human three-dimensional skin wound healing model using non-sequential fractional ultrapulsed CO2 laser treatments. Lasers Surg Med. 2015;47(3):257–265. doi:10.1002/lsm.22341
19. Huth S, Huth L, Marquardt Y, Cheremkhina M, Heise R, Baron JM. MMP-3 plays a major role in calcium pantothenate-promoted wound healing after fractional ablative laser treatment. Lasers Med Sci. 2021;37(2):887–894.
20. Broughton G II, Janis JE, Attinger CE. Wound healing: an overview. Plast Reconstr Surg. 2006;117(7S):1e-S–32e–S. doi:10.1097/01.prs.0000222562.60260.f9
21. McCrudden MTC, McAlister E, Courtenay AJ, González-Vázquez P, Raj Singh TR, Donnelly RF. Microneedle applications in improving skin appearance. Exp Dermatol. 2015;24(8):561–566. doi:10.1111/exd.12723
22. Alster TS, Graham PM. Microneedling: a review and practical guide. Dermatol Surg. 2018;44(3):397–404. doi:10.1097/DSS.0000000000001248
23. Martin P, Nunan R. Cellular and molecular mechanisms of repair in acute and chronic wound healing. Br J Dermatol. 2015;173(2):370–378. doi:10.1111/bjd.13954
24. El-Domyati M, Barakat M, Awad S, Medhat W, El-Fakahany H, Farag H. Multiple microneedling sessions for minimally invasive facial rejuvenation: an objective assessment. Int J Dermatol. 2015;54(12):1361–1369. doi:10.1111/ijd.12761
25. Nithya S, Radhika T, Jeddy N. Loricrin - an overview. J Oral Maxillofac Pathol. 2015;19(1):64–68. doi:10.4103/0973-029X.157204
26. Makino T, Mizawa M, Yamakoshi T, Takaishi M, Shimizu T. Expression of filaggrin-2 protein in the epidermis of human skin diseases: a comparative analysis with filaggrin. Biochem Biophys Res Commun. 2014;449(1):100–106. doi:10.1016/j.bbrc.2014.04.165
27. Ebner F, Heller A, Rippke F, Tausch I. Topical use of dexpanthenol in skin disorders. Am J Clin Dermatol. 2002;3(6):427–433. doi:10.2165/00128071-200203060-00005
28. Proksch E, Nissen HP. Dexpanthenol enhances skin barrier repair and reduces inflammation after sodium lauryl sulphate-induced irritation. J Dermatolog Treat. 2002;13(4):173–178. doi:10.1080/09546630212345674
29. Proksch E, de Bony R, Trapp S, Boudon S. Topical use of dexpanthenol: a 70th anniversary article. J Dermatolog Treat. 2017;28(8):766–773. doi:10.1080/09546634.2017.1325310
30. Heise R, Skazik C, Marquardt Y, et al. Dexpanthenol modulates gene expression in skin wound healing in vivo. Skin Pharmacol Physiol. 2012;25(5):241–248. doi:10.1159/000341144
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.