Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 15
Post-Traumatic Stress in Vitiligo Patients: A Neglected but Real-Existing Psychological Impairment
Authors Liu JW, Tan Y, Chen T, Liu W, Qian YT ![]() , Ma DL
, Ma DL
Received 25 November 2021
Accepted for publication 20 January 2022
Published 5 March 2022 Volume 2022:15 Pages 373—382
DOI https://doi.org/10.2147/CCID.S350000
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jeffrey Weinberg
Jia-Wei Liu, Yan Tan, Tian Chen, Wei Liu, Yue-Tong Qian, Dong-Lai Ma
Department of Dermatology, Peking Union Medical College Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, National Clinical Research Center for Skin and Immune Diseases, Beijing, 100730, People’s Republic of China
Correspondence: Dong-Lai Ma, Department of Dermatology, Peking Union Medical College Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, National Clinical Research Center for Skin and Immune Diseases, Beijing, 100730, People’s Republic of China, Tel +86-10-69151543, Fax +86-10-69151502, Email [email protected]
Background: Vitiligo is the most common depigmentation disorder. This disease causes disfiguration and induces psychological burdens, leading to significantly impaired quality of life. Limited research about disease-related post-traumatic stress (PTS) has been conducted in vitiligo patients.
Objective: To evaluate the prevalence, severity, and risk factors of post-traumatic stress in vitiligo patients.
Methods: This case-control study was performed from January 2021 to April 2021. A survey questionnaire including baseline information, post-traumatic stress symptoms evaluation, life quality evaluation was conducted. According to the severity of post-traumatic stress symptoms, patients were grouped and compared. The logistic regression model was conducted to analyze the risk factors for post-traumatic stress disorder (PTSD).
Results: A total of 337 patients were included. A 30.3% of vitiligo patients (102/337) in present cohort had PTS and 12.5% patients (42/337) were confirmed for developing into PTSD. The multivariate logistic regression revealed educational level
Keywords: vitiligo, post-traumatic stress, risk factors, quality of life, psychodermatology
Introduction
Vitiligo is a chronic dermatosis characterized by hypopigmented macules, and the condition results from wholly or partly destructed melanocytes in the affected skin.1 This disorder affects approximately 0.5–2% of the population worldwide.2 Unfortunately, the exact etiology of vitiligo remains unknown at present. Several factors, such as genetic, autoimmune, psychological, and environmental factors, are believed to be involved in the occurrence and development of this disorder.1,3,4 Despite the fact that the onset of the condition can occur at any point in life, vitiligo occurs before 20 years of age in 50% of patients5,6.Vitiligo is generally asymptomatic and neither reduces individual physical activity nor shortens life expectancy. However, this chronic disease may significantly impair quality of life for individuals. It is associated with experiencing vitiligo-related discrimination, social isolation, and even sexual exclusion, which can result in psychological problems such as lowered self-esteem, embarrassment, anxiety, and depression.7,8 Social stigma can last for decades and even throughout an individual’s lifetime, and suicidal ideation has been reported in some individuals under chronic stress.9 Therefore, vitiligo-related psychiatric disorders ought to be thoroughly investigated.
Traditionally, post-traumatic stress disorder (PTSD) has been reported to occur only due to physical trauma such as violence, severe injuries, earthquakes, and rape.10,11 However, several recent studies have found that several chronic diseases, such as coronary heart disease and inflammatory bowel disease, are closely related with PTSD due to experiences associated with the disease (eg, surgery, financial burden, and uncertainty of treatment effects).12–14 Considering the adverse effects of PTSD on health-related quality of life, it is of great necessity for dermatologists to evaluate psychological distress in patients with vitiligo in the early stage. To the best of our knowledge, the relationship between PTSD and vitiligo has never been studied before. Therefore, the present study intended to i) design a case-control study to determine whether PTSD is associated with vitiligo-related experiences and ii) investigate how PTSD affects patients with vitiligo if this relationship exists.
Materials and Methods
Design
This study was designed as a retrospective case-control study performed from January 2021 to April 2021. The research protocol of the study followed the Declaration of Helsinki and obtained approval from the Ethics Committee of the Peking Union Medical College Hospital (Ethical No: S-K1651). PTS-related instruments were carried out via one-on-one anonymous interviews with a senior psychiatrist in separate rooms to protect personal information. Vitiligo-related assessments were conducted by senior dermatologists.
Patients
All patients were informed that their information could be used for this study and their written consent was obtained. Vitiligo patients who attended the dermatology outpatient clinic at a tertiary care hospital, Peking Union Medical College Hospital, were included. The exclusion criteria included: (1) being under 18 years old or above 80 years old, (2) being unwilling to participate in this study, (3) failure to understand the questions or failure to give an adequate response due to cognitive impairment, and (4) having ever suffered major adverse events in their lives, such as bankruptcy, rape, or a severe earthquake. According to whether they had PTS/PTSD, the included patients were dichotomized into a case group and a control group.
Instruments
Post-Traumatic Stress (PTS) and Post-Traumatic Stress Disorder (PTSD)
The PTSD Checklist–Civilian Version (PCL-C)15 was utilized to evaluate PTS symptoms and PTSD.16 This self-reported instrument comprises 17 items with responses ranging from 1 (not at all) to 5 (extremely). A total score greater than 37 indicates PTS. A total score greater than or equal to 50 is the cutoff value for the diagnosis of PTSD.15 A higher total score indicates greater severity. Previous studies have verified good internal consistency and effectiveness of the Chinese version of PCL-C.17
The diagnostic symptoms of PTSD were defined based on the 4th edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV).18 Except for PCL-C, PTSD also requires a clinical interview by a senior psychiatrist to evaluate whether the symptoms of PTS developed into PTSD based on the severity of the symptoms and the patient’s specific condition. Information such as demographic data, medical history, comorbidities, and cause for PTS or PTSD were recorded and used for analysis.
Vitiligo-Related Evaluation
The area affected by vitiligo was assessed by the Vitiligo Area Scoring Index (VASI). VASI=∑[HAND UNITS] × [RESIDUAL DEPIGMENTATION].19
The Vitiligo Disease Activity (VIDA) score was used to evaluate vitiligo activity. The VIDA score was a six-point scale graded according to the patient’s self-report on disease activity: a) 4, disease progression in six weeks or less; b) 3, disease progression in six weeks to three months; c) 2, disease progression in three to six months; d) 1, disease progression in six to twelve months; e) 0, stable for one year or more; and f) −1, stable with spontaneous repigmentation for one year or more. Disease progression was defined as the expansion of existing lesions or the appearance of new lesions.20
Life Quality Evaluation
The Dermatology Life Quality Index (DLQI) was adapted to evaluate the quality of life of vitiligo patients. This is a validated, dermatology-specific quality of life assessment form that focuses on dermatosis-related disruption in different aspects, namely, symptoms and feelings, daily activities, leisure, work or school, personal relationships, and side effects of treatment. The instrument is scored based on patients’ self-report: a) 0, not bothered at all or not relevant; b) 1, a little; c) 2, a lot; and d) 3, very much.21
Statistical Analysis
Data were analyzed using SPSS version 22 (IBM Corp., Armonk, NY, USA). Continuous variables are presented as the mean ± standard deviation (S.D.) and ordinal variables as proportions. Student’s t-tests were performed to test the differences between groups for continuous variables, while either Fisher’s exact test or Pearson’s chi-square test was used for ordinal variables. Univariate logistic regression analysis was conducted to calculate the odds ratio (OR) and 95% confidence interval (CI) to investigate the risk factors for PTSD in vitiligo. The Pearson correlation coefficient (coefficient, r) was performed to determine the correlation between the PCL-C score and VASI and between the PCL-C score and DQLI score. Spearman’s rank correlation (coefficient, rho) was performed to determine the correlation between and between the PCL-C score and VIDA score controlling the variables with a correlation value of more than 0.5. After adjusting for confounding factors, the significant variables in the univariate logistic regression were analyzed in the multivariate model. P values=0.05 and β=0.8 were defined as the statistical significance and power analysis, respectively.
Results
According to the inclusion and exclusion criteria, a total of 337 vitiligo patients (mean age±SD: 30.0±11.4 years; female: 59.9%) completed this study. The basic information of the included patients is shown in Table 1. A total of 102 patients were diagnosed with PTS, while 42 patients were diagnosed with vitiligo-related PTSD.
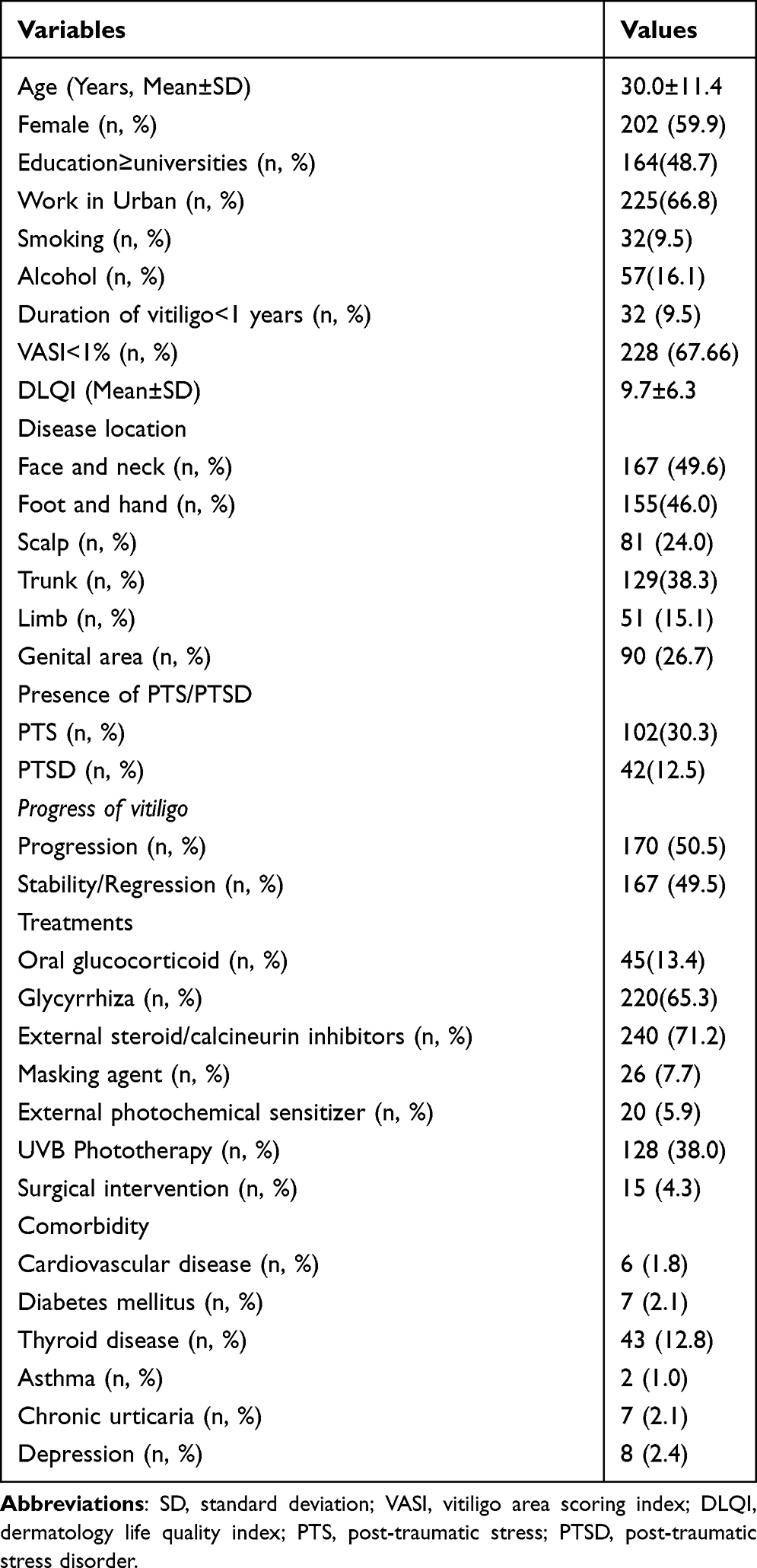 |
Table 1 Basic Information of the Included Patients |
Analysis for PTS and PTSD in Patients with Vitiligo
30.3% of vitiligo patients (102/337) in the sample had PTS, and another 12.5% of patients (42/337) were diagnosed with PTSD (Table 1). Only 5.9% (6/102) of those with a clinical diagnosis of PTS and 11.9% of those with PTSD (5/42) had ever sought any type of treatment such as psychotherapy or medication.
Compared to vitiligo patients without PTS or PTSD, patients with either PTS or PTSD had a lower level of education (the percentage of those with more than or equal to a college-level education with PTS, 35.29% vs 54.47%, P=0.001; PTSD, 28.57% vs 51.53%, P=0.005), a higher incidence of vitiligo in the face and neck (PTS, 63.73% vs 43.40%, P=0.001; PTSD, 69.05% vs 46.78%, P=0.007), vitiligo in the feet and hands (PTS, 55.88% vs 41.70%, P=0.016; PTSD, 71.43% vs 42.37%, P<0.001), vitiligo in the limbs (PTS, 23.53% vs 11.49%, P=0.005; PTSD, 28.57% vs 13.22%, P=0.009), and significantly different surgical treatments for vitiligo (PTS, 9.80% vs 2.13%, P=0.002; PTSD, 19.05% vs 2.37%, P=0.001).
Significant differences in the percentage of vitiligo duration of less than one year (17.65% vs 5.96%, P=0.001), total area of vitiligo<1% (55.88% vs 72.77%, P=0.002) and masking agent use (20.59% vs 2.13%, P<0.001) were found between the PTS and non-PTS groups. However, no significant differences in these three variables was found between the PTSD and non-PTSD groups: vitiligo duration less than one year (14.29% vs 8.81%, P=0.258), total area of vitiligo<1% (57.14% vs 69.15%, P=0.12) and masking agent use (14.29% vs 6.78%, P=0.088), as illustrated in Table 2.
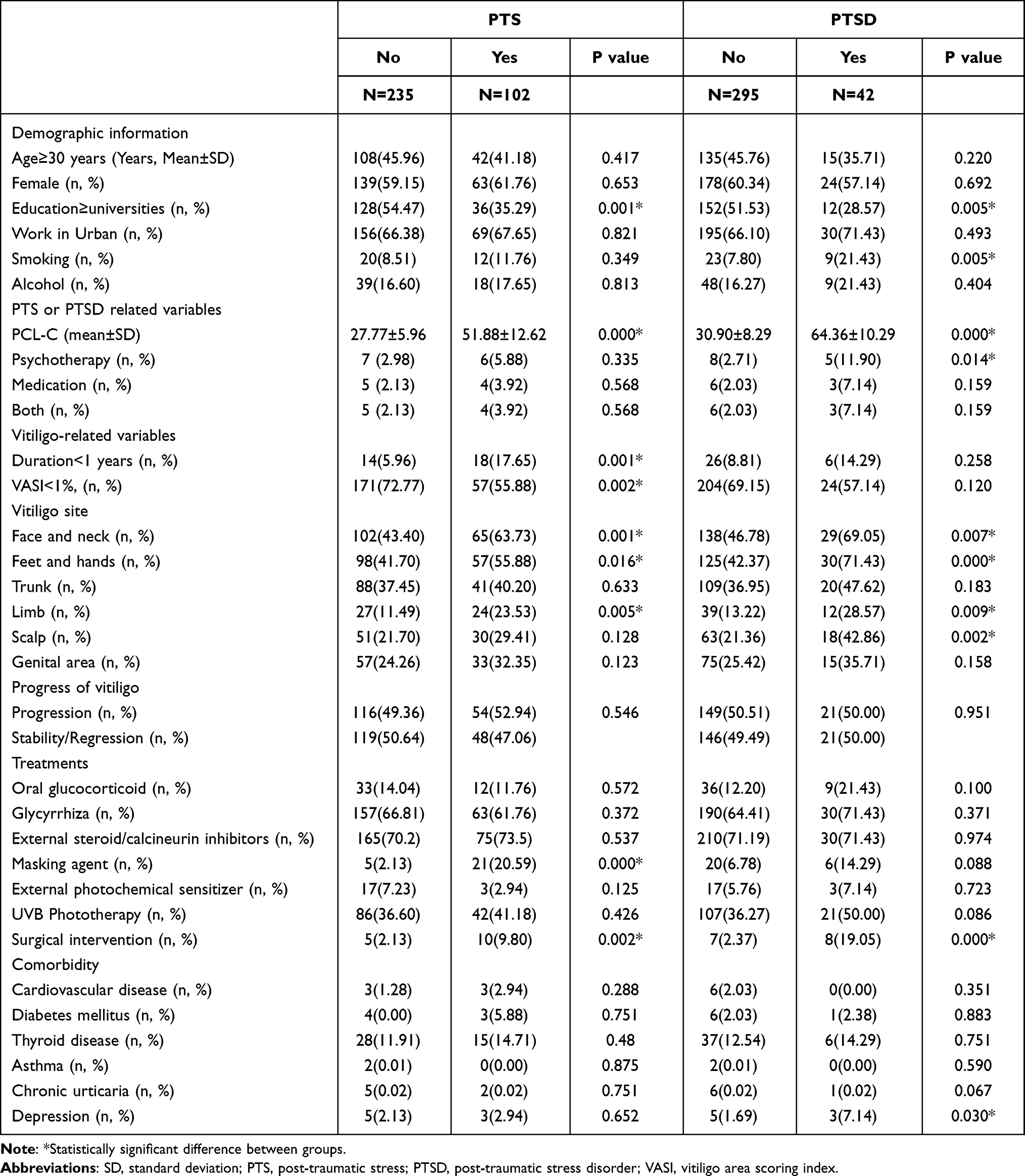 |
Table 2 PTS and PTSD in Patients with Vitiligo |
Significant differences in the percentages of smoking (21.43% vs 7.8%, P=0.005), vitiligo in the scalp (42.86% vs 21.36%, P=0.002), and depression (7.14% vs 1.69%, P=0.030) were found between the PTSD and non-PTSD groups. However, no significant differences in these two variables existed between the PTS and non-PTS groups: smoking (11.76% vs 8.51%, P=0.349), vitiligo in the scalp (29.41% vs 21.70%, P=0.128) and depression (2.13% vs 2.94%, P=0.652), as illustrated in Table 2.
Analysis for Separate Symptom in PCL-C
The most common symptom of PTS in the present sample of vitiligo patients was sleep disturbance (48.79%), followed by emotionally triggered (46.28%), intrusive thoughts (42.01%), avoidance of certain situations (34.19%), and irritability (29.92%) (Figure 1).
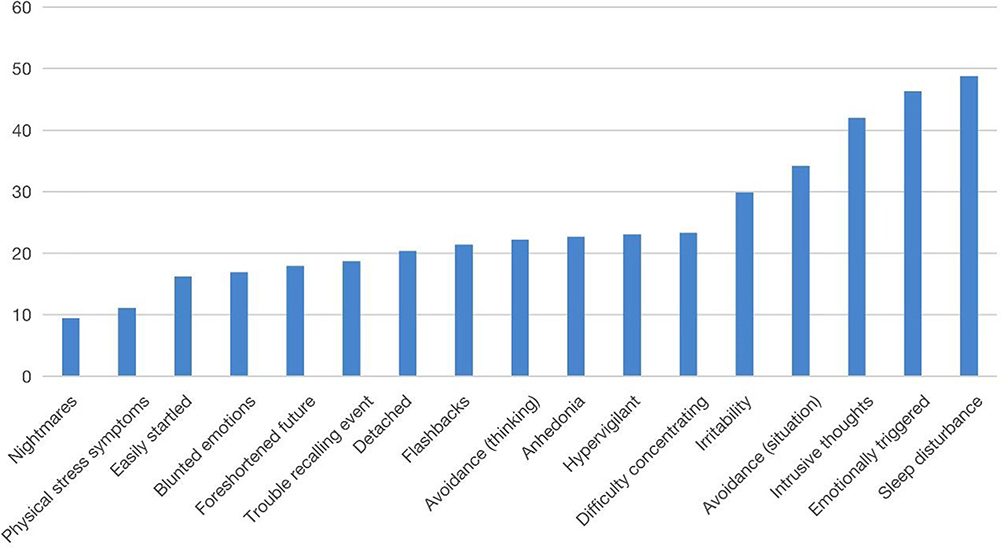 |
Figure 1 Percentage of vitiligo patients selecting “moderate” or “greater” in individual items of the PCL-C. |
Logistic Regression Analysis for PTSD in Patients with Vitiligo
Potential risk factors for PTSD identified in the previous analyses were included in separate regression models for vitiligo patients, including having less than a college level of education (OR=2.12, 95% CI=1.74–2.76, P=0.003), vitiligo in the face and neck (OR= 2.45, 95% CI=1.98–2.98, P=0.044), vitiligo in the feet and hands (OR=1.65, 95% CI=1.23–2.09, P<0.001), vitiligo on limbs (OR=1.43, 95% CI=1.12–1.73, P=0.035), and invasive treatment (OR=3.25, 95% CI=2.87–3.87, P=0.002). These factors were analyzed in the multivariate regression analysis.
Multiple logistic regression analysis demonstrated that having less than a college level of education (OR=2.32, 95% CI=1.97–2.93, P=0.003), vitiligo in the face and neck (OR=2.65, 95% CI=2.08–3.12, P=0.008), vitiligo in the feet and hands (OR=1.86, 95% CI=1.54–2.12, P<0.001), and surgical treatment (OR=3.53, 95% CI=3.12–4.02, P<0.001) were risk factors for PTSD.
Correlation Analysis
PTS severity as assessed by the PCL-C score was significantly associated with vitiligo activity by the VIDA score (rho=0.54, R2=0.29, P=0.002). There was a significant association between VASI and PCL-C score (r=0.55, R2=0.30, P=0.012). In addition, the PCL-C score was significantly associated with the DLQI (r=0.61, R2=0.37, P=0.004).
Reliability
The intraclass correlation coefficient (ICC) for each item in the PCL-C questionnaire in this study ranged from 0.79 to 0.88. Cronbach’s alpha coefficient of this measure was 0.85.
Discussion
This is the first study to investigate PTS and PTSD in vitiligo patients. A total of 30.3% of vitiligo patients (102/337) in the present sample had PTS, and 12.5% of patients (42/337) were confirmed to have PTSD (Table 1). Those who had to seek physiological interventions to treat PTS or PTSD are only a small subset of the population of those affected by vitiligo (5.9% and 11.9%, respectively). The figures highlight the urgent need to assess PTS more comprehensively and offer care for vitiligo patients affected by PTS and PTSD.
Previous studies have demonstrated that psychological stressors play a role in vitiligo.22,23 Significant adverse events in life, such as work and financial problems, death of a family member, and critical illness, have been considered preceding factors for the onset and development of vitiligo.23 This may be associated with the severe psychological effects that vitiligo patients experienced, such as anxiety, depression, social stigma, and impaired quality of life.24–26 Stress increases the levels of catecholamines, neuropeptides, and cortisol, which are higher in vitiligo patients,27–29 suggesting their role in the pathogenesis of vitiligo. The present results revealed that in our sample, nearly one-third of vitiligo patients experienced PTS, and one-tenth had PTSD. Therefore, there appears to be an interaction between vitiligo and PTS/PTSD. Even though the exact mechanism of how post-traumatic stress acts upon the pathogenesis of vitiligo has not been discovered, it is reasonable to assume that if the shadow of PTS/PTSD persist, then the disease progression may not be terminated.
The present study revealed that in our sample, patients with less than a college level of education, vitiligo in the face and neck, vitiligo in the hands and feet, and surgical treatment are at higher risk of developing severe PTS and PTSD (Table 2). The results align with that of previous studies concerning the relationship between stress symptoms and vitiligo.24,30,31 Among the vitiligo patients included in our sample, female vitiligo patients were not significantly likelier to develop PTS or PTSD than male patients. However, several studies have found that women are more likely to be affected by PTS/PTSD.32 Whether female vitiligo patients are more vulnerable to disease-related PTS/PTSD may need further investigation. In vitiligo, depigmentation itself can also cause stress; in fact, self-reported depigmentation was the highest on the face and hands.30 In the current study, vitiligo in the face and neck, vitiligo in the hands and feet, and having less than a college level of education were associated with PTSD. This may imply that the level of cognitiveness of one patient is associated with PTSD. There was a significant difference in the duration of vitiligo between those who had PTS and those who did not. This implies the existence of a “time-effect” curve. Typically, its initial stage vitiligo causes greater psychological burden on patients. Of course, as a chronic disease, the cumulative stress from a variety of psychologically adverse experiences associated with vitiligo are difficult to manager for the majority of patients, and these experiences are sometimes more harmful than the disease itself despite the disease being neither contagious nor life-threatening.33 Therefore, we did not detect a significant difference in the duration of vitiligo between individuals who were affected by PTSD and those who were not. Depending on the type, extent, and duration of vitiligo, conventional treatments such as topical and systemic corticosteroids, topical immunomodulators, and phototherapy fail to be consistently effectiveness, and repigmentation is generally incomplete. Vitiliginous lesions occurring on sites such as lips, acral areas, nipples, and genitals are generally resistant to medical treatment.34 This has resulted in the evolution of some surgical modalities to treat recalcitrant stable lesions. The conventional surgical modalities for vitiligo are miniature punch grafting, suction blister grafting, and thin split-thickness skin grafting.33,34 However, these invasive treatments may produce extra psychological stress on patients.
The present findings relevant to the percentage of “moderate” or “greater” in each item in the PCL-C survey indicated that more than one-third of vitiligo patients reported autonomic nervous system arousal and emotional PTS symptoms on nearly half of the 17 items (Figure 1). “Moderate” or “greater” sleep disturbance occurred in up to 45% of vitiligo patients, indicating their significantly impaired quality of life. The most common symptom of PTS in the present sample of vitiligo patients was sleep disturbance (45%). This figure is in line with a previous study showing that sleep disorders are a common problem in vitiligo patients.35 Moreover, the higher percentage of physical stress symptoms may suggest that stress does not affect vitiligo patients’ psychological status or physical condition. The common symptoms were autonomic nervous system arousals such as racing heartbeat and shallow breathing. These symptoms caused some patients to seek medical consultations and treatments, thereby increasing the financial burden of vitiligo and putting elderly patients with chronic comorbidities at greater risk of complications. Another higher incidence of PTS symptoms was emotionally triggered (46.28%), intrusive thoughts (42.01%), avoidance of certain situations (34.19%), and irritability (29.92%), which may indicate that the occurrence of vitiligo in their lives makes individuals more neurotic and emotionally vulnerable. In severe cases, suicidal ideation occurred in some individuals under chronic stress.9 These data indicated that psychological intervention is necessary for vitiligo patients with PTS or PTSD to avoid further adverse consequences.
Implications
Vitiligo has a psychologically devastating impact and significantly influences patients’ quality of life. PTSD was traditionally considered to result from stressors associated with trauma.36 However, an increasing number of studies should include chronic life stress, psychological disorders, and critical illness in the diagnosis of PTSD.37–40 While PTSD is most often associated with occurring after “trauma” events, non-trauma events, such as deteriorated health-related quality of life in most vitiligo patients, psychological distress resulting from social stigma, financial burden, relapse, and aggravation of the disease, and treatment side effects, may also contribute to the onset of PTSD. The occurrence of PTSD often leads to decreased quality of life, such as recurrent frightening thoughts, difficulty concentrating, hypervigilance, dissociative feelings, and trouble sleeping.41 Undoubtedly, this psychological disorder negatively affects vitiligo treatments. Therefore, it may be beneficial for dermatologists to be aware of the possibility of vitiligo-related PTS and PTSD and to offer proactive early interventions such as physical activity, support groups, counseling, cognitive-behavioral interventions, and pharmacological treatments.42,43
Limitations
There are some limitations that are worth noting. First, the case-control design of our study failed to give any causal conclusions, except for the finding that vitiligo is associated with PTS and PTSD. A future prospective study is needed to demonstrate a definitive relationship between vitiligo and PTS or PTSD. In addition, the relatively small sample size limits the generalizability of this study. A more extensive and multicenter study would add credibility. Finally, vitiligo is a chronic disease whose course may last for several decades. Recall bias was difficult to avoid in interview questions concerning PTS.
Conclusion
A total of 30.3% of vitiligo patients (102/337) in the present sample had PTS, and 12.5% of patients (42/337) were confirmed to have PTSD. In addition, having less than a college level of education (OR=2.32, 95% CI=1.97–2.93, P=0.003), vitiligo in the face and neck (OR= 2.65, 95% CI=2.08–3.12, P=0.008), vitiligo in the feet and hands (OR=1.86, 95% CI=1.54–2.12, P<0.001), and surgical treatment (OR=3.53, 95% CI=3.12–4.02, P<0.001) were risk factors for PTSD. Our results may spread awareness among dermatologists about the possibility of vitiligo-related PTS and PTSD and help provide proactive intervention to improve the efficacy of treatments.
Acknowledgment
We would like to thank all patients involved in this study.
Funding
The research has no funding source.
Disclosure
All authors stated no conflicts of interest for this work.
References
1. Tarlé RG, Nascimento LM, Mira MT, Castro CC. Vitiligo–part 1. An Bras Dermatol. 2014;89:461–470. doi:10.1590/abd1806-4841.20142573
2. Bergqvist C, Ezzedine K. Vitiligo: a review. Dermatology. 2020;236:571–592. doi:10.1159/000506103
3. Laddha NC, Dwivedi M, Mansuri MS, et al. Vitiligo: interplay between oxidative stress and immune system. Exp Dermatol. 2013;22:245–250. doi:10.1111/exd.12103
4. Silverberg NB. The epidemiology of vitiligo. Curr Dermatol Rep. 2015;4:36–43. doi:10.1007/s13671-014-0098-6
5. Whitton ME, Ashcroft DM, Barrett CW, Gonzalez U. Interventions for vitiligo. Cochrane Database Syst Rev. 2006;25:CD003263.
6. Mumtaz H, Anis S, Akhtar A, et al. Efficacy of tacrolimus versus clobetasol in the treatment of vitiligo. Cureus. 2020;12:e11985. doi:10.7759/cureus.11985
7. Porter J, Beuf AH, Nordlund JJ, Lerner AB. Psychological reaction to chronic skin disorders: a study of patients with vitiligo. Gen Hosp Psychiatry. 1979;1:73–77. doi:10.1016/0163-8343(79)90081-1
8. Porter JR, Beuf AH, Lerner AB, Nordlund JJ. The effect of vitiligo on sexual relationships. J Am Acad Dermatol. 1990;22:221–222. doi:10.1016/0190-9622(90)70028-G
9. Pahwa P, Mehta M, Khaitan BK, Sharma VK, Ramam M. The psychosocial impact of vitiligo in Indian patients. Indian J Dermatol Venereol Leprol. 2013;79:679–685. doi:10.4103/0378-6323.116737
10. Elklit A, Christiansen DM. ASD and PTSD in rape victims. J Interpers Violence. 2010;25:1470–1488. doi:10.1177/0886260509354587
11. Qi W, Gevonden M, Shalev A. Prevention of post-traumatic stress disorder after trauma: current evidence and future directions. Curr Psychiatry Rep. 2016;18:20. doi:10.1007/s11920-015-0655-0
12. van Zelst WH, de Beurs E, Beekman AT, van Dyck R, Deeg DD. Well-being, physical functioning, and use of health services in the elderly with PTSD and subthreshold PTSD. Int J Geriatr Psychiatry. 2006;21:180–188. doi:10.1002/gps.1448
13. Taft TH, Bedell A, Craven MR, Guadagnoli L, Quinton S, Hanauer SB. Initial assessment of post-traumatic stress in a U.S. cohort of inflammatory bowel disease patients. Inflamm Bowel Dis. 2019;25:1577–1585. doi:10.1093/ibd/izz032
14. Kubzansky LD, Koenen KC, Spiro A, Vokonas PS, Sparrow D. Prospective study of post-traumatic stress disorder symptoms and coronary heart disease in the Normative Aging Study. Arch Gen Psychiatry. 2007;64:109–116. doi:10.1001/archpsyc.64.1.109
15. Weathers FW, Litz BT, Herman D, Huska J, Keane T. The PTSD Checklist-Civilian Version (PCL-C). Boston, MA: National Center for PTSD; 1994:10.
16. Ruggiero KJ, Del Ben K, Scotti JR, Rabalais AE. Psychometric properties of the PTSD checklist-civilian version. J Trauma Stress. 2003;16:495–502. doi:10.1023/A:1025714729117
17. Zhang Q, Zheng R, Fu Y, Mu Q, Li J. Mental health consequences during alerting situations and recovering to a new normal of coronavirus epidemic in 2019: a cross-sectional study based on the affected population. BMC public Health. 2021;21:1499. doi:10.1186/s12889-021-11550-w
18. Battle DE. Diagnostic and statistical manual of mental disorders (DSM). Codas. 2013;25:191–192. doi:10.1590/s2317-17822013000200017
19. Hamzavi I, Jain H, McLean D, Shapiro J, Zeng H, Lui H. Parametric modeling of narrowband UV-B phototherapy for vitiligo using a novel quantitative tool: the Vitiligo Area Scoring Index. Arch Dermatol. 2004;140:677–683. doi:10.1001/archderm.140.6.677
20. Njoo MD, Das PK, Bos JD, Westerhof W. Association of the Köbner phenomenon with disease activity and therapeutic responsiveness in vitiligo Vulgaris. Arch Dermatol. 1999;135:407–413. doi:10.1001/archderm.135.4.407
21. Finlay AY, Khan GK. Dermatology Life Quality Index (DLQI)–a simple practical measure for routine clinical use. Clin Exp Dermatol. 1994;19:210–216. doi:10.1111/j.1365-2230.1994.tb01167.x
22. Papadopoulos L, Bor R, Legg C, Hawk JL. Impact of life events on the onset of vitiligo in adults: preliminary evidence for a psychological dimension in aetiology. Clin Exp Dermatol. 1998;23:243–248. doi:10.1046/j.1365-2230.1998.00384.x
23. Silverberg JI, Silverberg NB. Vitiligo disease triggers: psychological stressors preceding the onset of disease. Cutis. 2015;95:255–262.
24. Cupertino F, Niemeyer-Corbellini JP, Ramos ESM. Psychosomatic aspects of vitiligo. Clin Dermatol. 2017;35:292–297. doi:10.1016/j.clindermatol.2017.01.001
25. Thompson AR, Kent G, Smith JA. Living with vitiligo: dealing with difference. Br J Health Psychol. 2002;7:213–225. doi:10.1348/135910702169457
26. Stangier U, Ehlers A, Gieler U. Measuring adjustment to chronic skin disorders: validation of a self-report measure. Psychol Assess. 2003;15:532–549. doi:10.1037/1040-3590.15.4.532
27. Krüger C, Schallreuter KU. Stigmatisation, avoidance behaviour and difficulties in coping are common among adult patients with vitiligo. Acta Derm Venereol. 2015;95(5):553–558. doi:10.2340/00015555-1981
28. Parsad D, Dogra S, Kanwar AJ. Quality of life in patients with vitiligo. Health Qual Life Outcomes. 2003;1:58. doi:10.1186/1477-7525-1-58
29. Amer AA, Gao XH. Quality of life in patients with vitiligo: an analysis of the dermatology life quality index outcome over the past two decades. Int J Dermatol. 2016;55:608–614. doi:10.1111/ijd.13198
30. Henning SW, Jaishankar D, Barse LW, et al. The relationship between stress and vitiligo: evaluating perceived stress and electronic medical record data. PLoS One. 2020;15:e0227909. doi:10.1371/journal.pone.0227909
31. Manolache L, Benea V. Stress in patients with alopecia areata and vitiligo. J Eur Acad Dermatol Venereol. 2007;21:921–928. doi:10.1111/j.1468-3083.2006.02106.x
32. Tolin DF, Foa EB. Sex differences in trauma and post-traumatic stress disorder: a quantitative review of 25 years of research. Psychol Bull. 2006;132:959–992. doi:10.1037/0033-2909.132.6.959
33. Ramzi TM, Afra TP, Parsad D. Vitiligo surgery: a journey from tissues via cells to the stems! Exp Dermatol. 2019;28:690–694. doi:10.1111/exd.13807
34. Khunger N, Kathuria SD, Ramesh V. Tissue grafts in vitiligo surgery - past, present, and future. Indian J Dermatol. 2009;54:150–158. doi:10.4103/0019-5154.53196
35. Seo HM, Kim TL, Kim JS. The risk of alopecia areata and other related autoimmune diseases in patients with sleep disorders: a Korean population-based retrospective cohort study. Sleep. 2018;41:1–8. doi:10.1093/sleep/zsy111
36. Strelchuk D, Hammerton G, Wiles N, et al. PTSD as a mediator of the relationship between trauma and psychotic experiences. Psychol Med. 2020;14:1–9. doi:10.1017/S0033291720004821
37. Watanabe Y, Arase S, Nagaoka N, Kawai M, Matsumoto S. Chronic psychological stress disrupted the composition of the murine colonic microbiota and accelerated a murine model of inflammatory bowel disease. PLoS One. 2016;11:e0150559. doi:10.1371/journal.pone.0150559
38. Cámara RJ, Gander ML, Begré S, von Känel R. Post-traumatic stress in Crohn’s disease and its association with disease activity. Frontline Gastroenterol. 2011;2:2–9. doi:10.1136/fg.2010.002733
39. Jones C, Bäckman C, Capuzzo M, et al. Intensive care diaries reduce new onset post-traumatic stress disorder following critical illness: a randomised, controlled trial. Crit Care. 2010;14:R168. doi:10.1186/cc9260
40. Neuendorf R, Harding A, Stello N, Hanes D, Wahbeh H. Depression and anxiety in patients with Inflammatory Bowel Disease: a systematic review. J Psychosom Res. 2016;87:70–80. doi:10.1016/j.jpsychores.2016.06.001
41. PDQ Supportive and Palliative Care Editorial Board. Cancer-related post-traumatic stress (PDQ®): health professional version. PDQ Cancer Information Summaries. Bethesda (M.D.): National Cancer Institute (U.S.); 2002.
42. Rosenbaum S, Vancampfort D, Steel Z, Newby J, Ward PB, Stubbs B. Physical activity in the treatment of Post-traumatic stress disorder: a systematic review and meta-analysis. Psychiatry Res. 2015;230:130–136. doi:10.1016/j.psychres.2015.10.017
43. Kearns MC, Ressler KJ, Zatzick D, Rothbaum BO. Early interventions for PTSD: a review. Depress Anxiety. 2012;29:833–842. doi:10.1002/da.21997
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.