Back to Journals » Clinical Ophthalmology » Volume 16
Post-Market Evaluation of Rotational Stability and Visual Performance of a New Toric Intraocular Lens with Frosted Haptics
Authors Chang DH ![]() , Hu J, Miller KM
, Hu J, Miller KM ![]() , Vilupuru S, Zhao W
, Vilupuru S, Zhao W ![]()
Received 9 September 2022
Accepted for publication 22 November 2022
Published 10 December 2022 Volume 2022:16 Pages 4055—4064
DOI https://doi.org/10.2147/OPTH.S389304
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Daniel H Chang,1 Jerry Hu,2 Kevin M Miller,3 Srividhya Vilupuru,4 Wuchen Zhao4
1Empire Eye and Laser Center, Bakersfield, CA, USA; 2Texas Eye & Laser Center, Hurst, TX, USA; 3Department of Ophthalmology, David Geffen School of Medicine at the University of California Los Angeles (UCLA), Los Angeles, CA, USA; 4Johnson & Johnson Surgical Vision, Inc., Irvine, CA, USA
Correspondence: Daniel H Chang, Empire Eye & Laser Center, 4105 Empire Dr, Bakersfield, CA, 93309, USA, Email [email protected]
Purpose: To evaluate 3-month rotational stability, and visual and refractive outcomes of a toric intraocular lens (IOL) with frosted haptics.
Patients and Methods: A post-market, prospective, multi-center, single-arm, open-label study conducted at seven clinical sites in the United States. Two hundred and two eyes of 133 subjects with unilateral or bilateral cataracts and corneal astigmatism were implanted with the Tecnis Toric II IOL, Models ZCU150 to 600 (Johnson & Johnson Surgical Vision, Inc.). Lens axis misalignment/rotation, visual acuity, manifest refraction, and surgeon and patient satisfaction were evaluated 3 months postoperatively. Lens rotation was determined with operative and postoperative visit photographs and was analyzed by two independent masked analysts.
Results: Mean absolute lens rotation was 0.82° ± 1.00° and 0.94° ± 0.71° at 1 day (n = 189 eyes) and 3 months (n = 185 eyes), respectively. Absolute lens rotation was ≤ 5° in 98.9% and 100% of eyes at 1 day and 3 months, respectively. At 3 months, postoperative monocular uncorrected and corrected distance visual acuities were 0.004 ± 0.115 LogMAR (20/20) and − 0.066 ± 0.092 LogMAR (20/17), mean spherical equivalent was − 0.25 D ± 0.35 D and residual refractive cylinder was +0.27 D ± 0.33 D. Surgeons were satisfied/very satisfied with overall clinical outcomes and rotational stability in 99% of eyes, and with uncorrected distance vision in 98.5% of eyes.
Conclusion: The study results demonstrate that the Tecnis Toric II IOL has excellent rotational stability with a high percentage of study eyes being within 5° of intended orientation. The study lens demonstrated excellent uncorrected distance visual acuity, reduction of cylinder, and exceptional patient and surgeon satisfaction.
Keywords: toric IOL, lens rotation, IOL misalignment, residual astigmatism
Introduction
Between 15% and 29% of patients1 and as many as 47% of eyes2 with cataract have levels of corneal or refractive astigmatism sufficient to impact clinical outcomes after cataract surgery. Review of the literature provides evidence that astigmatism management at the time of cataract surgery results in better postoperative visual outcomes, higher satisfaction with vision, greater spectacle independence, and improvement in patients’ vision-related quality of life compared to patients in whom astigmatism management is not attempted during cataract surgery. Moreover, astigmatism management during cataract surgery is a cost-effective approach compared to postoperative vision correction with spectacles.2 Unfortunately, as late as 2016, data from the American Society of Cataract and Refractive Surgery showed that the usage rate of toric IOLs was only 10%, despite sufficient evidence to show that it may be a more reliable and satisfying option for astigmatism management than other procedures like corneal relaxing incisions.3
The surgical management of astigmatism requires the integration of multiple steps throughout the preoperative period to achieve an optimal outcome. An error in one or more of these steps can result in a lens axis misalignment or postoperative residual astigmatism. Preoperatively, the corneal astigmatic power and axis must be stable and accurately measured. The toric intraocular lens (IOL) power must be properly calculated and selected. Intraoperatively, the axis of astigmatism must be properly identified, the toric IOL accurately positioned, and the anterior chamber adequately stabilized with proper wound closure. Postoperatively, the IOL must remain stable at its intraoperative position. Toric IOL stability has been implicated as a potential source of postoperative rotational malposition. In spite of excellent demonstrated clinical results as the first toric IOL to meet ANSI standards,4 some reports suggest a greater tendency for unacceptable postoperative rotational misalignment with the original Tecnis Toric 1-piece IOL (Model ZCT, Johnson & Johnson Surgical Vision, Inc.) versus competitor products.5–7
Differences in material, design, and haptic surface characteristics such as a smooth versus frosted finish can influence postoperative IOL rotational stability.8 Based on the design of the original Tecnis Toric IOL, a new IOL platform was created with modifications to the haptic design to limit change in position to ≤5 degrees (⁰) of the intraoperative position at the end of surgery.
The Tecnis Toric II (Model ZCU) IOL is an ultraviolet light-absorbing posterior chamber lens designed to compensate for the spherical aberration of the average cornea and correct astigmatism. The IOL incorporates a proprietary wavefront-designed toric aspheric optic with a square posterior optic edge that provides a 360⁰ barrier to reduce cell migration across the posterior capsule. The edge of the optic is frosted to reduce potential edge glare effects. The anteriorly located cylinder axis marks denote the lens meridian with the lowest power which should be aligned with the steep corneal meridian with the highest power.
Vukich et al proposed that introducing frosted haptics would create more surface texture and friction between the lens haptics and the capsular bag.8 Further, this change, while maintaining the overall lens geometry, diameter, and haptic shape, was predicted to improve rotational stability with little or no adjustment to surgical technique. Thus, this design and one other prototype with additional modifications to the size of the lens were tested in two proof-of-concept clinical studies using a photographic technique to document the lens rotational position immediately following implantation, and at the postoperative visits.8 Two prototype test IOLs with anteriorly located fiducial marks were implanted and assessed for lens rotation in the study using a novel validated photographic technique to assess lens alignment.9 When compared to the Tecnis Toric 1-piece IOL (Model ZCT), both prototypes demonstrated improved rotational stability. The best performing prototype IOL was selected and commercialized as the Tecnis Toric II (Model ZCU) IOL.
This post-market study was conducted to determine the rotational stability of these frosted haptic IOLs. Short-term rotational stability, defined as 1-day and 1-week postoperatively, and clinical performance of the Tecnis Toric II (Model ZCU) IOL from this were described in a previous publication.10 In the current manuscript, short- and long-term lens rotation, visual acuity, manifest refraction, and patient and surgeon satisfaction were evaluated over a 3-month period following implantation.
Materials and Methods
This prospective, multicenter, single-arm, open-label clinical investigation was conducted at seven sites in the United States in accordance with the Declaration of Helsinki, ISO 14155:2011 and all other applicable laws and regulations. Institutional review board approval was obtained prior to beginning the study and the study was registered on www.clinicaltrials.gov as NCT04327518. The clinical study was reviewed and approved by Salus Institutional Review Board and Office of the Human Research Protection Program (OHRPP, University of California, Los Angeles). After informed consent was obtained and confirmation that all eligibility criteria were met, the eyes were treated with the study lens.
All subjects were planned to undergo primary cataract extraction and posterior chamber IOL implantation in one or both eyes. Eligible subjects were 22 years or older with pre-existing corneal astigmatism of one diopter (D) or greater, predicted residual refractive cylinder ≤0.50 D based on a toric IOL calculator,11 potential for postoperative best-corrected distance visual acuity (CDVA) of 20/30 Snellen, clear intraocular media (other than cataract), and ability to understand and respond to a questionnaire in English. Exclusion criteria included irregular corneal astigmatism, corneal pathology or abnormality, previous corneal or intraocular surgery, inability to focus or fixate for prolonged periods, pupil abnormalities, dilated pupil size <6.0 mm, recurrent ocular inflammation or uveitis, conditions associated with increased risk of zonular rupture, ocular or systemic disease that may affect visual acuity or require surgical intervention during the study, use of systemic or ocular medications that may affect vision, confound the outcome of the study or increase risk to the subject, pregnancy, lactation or planned pregnancy, participation in concurrent clinical study or one within 30 days of the pre-operative visit, and planned monovision correction.
The primary outcome was the percentage of eyes with lens rotation ≤5° at postoperative visits. Lens rotation was defined as the absolute difference between IOL orientation intraoperatively at the end of the surgery and postoperatively at specified visit(s).12 Rotational stability of the IOL was defined as the change in lens rotation from one postoperative visit to the next.12 Both were measured using a validated photographic measurement technique described below. Other endpoints included residual mean manifest cylinder and spherical equivalent for all eyes, percentage of eyes that achieved uncorrected distance visual acuity (UDVA) of 20/40, 20/32, 20/25 and 20/20, percentage of eyes that achieved accuracy of cylinder (to target) within: ± 0.50 D and ± 1.00 D, analysis of lens rotation including mean absolute and signed value of the lens rotation, percentage of eyes with lens rotation ≤5°, <10°, <20° and >30°, medical findings/lens findings/complications, patient satisfaction questionnaire responses for those with bilateral implantation, investigator satisfaction questionnaire responses for all implanted eyes, and adverse event rates including IOL repositioning and/or IOL exchange primarily due to IOL misalignment.
Intraocular Lens Implantation
All subjects had unilateral or bilateral cataract surgery with the study lens (Tecnis Toric II, Models ZCU150, ZCU225, ZCU300, ZCU375, ZCU450, ZCU525, ZCU600). In bilateral subjects, second eye surgery occurred no more than 30 days after first eye surgery. Procedures for calculating IOL power and axis alignment are detailed in a prior publication.10 Briefly, preoperative keratometry and biometry data including axial length, incision location, spherical equivalent IOL power, and the surgeon’s estimated surgically induced corneal astigmatism were used as inputs for the TECNIS Toric Calculator (www.TecnisToricCalc.com) or the surgeon’s preferred Toric Calculator. The investigators were instructed to use their standard IOL axis marking and small-incision, phacoemulsification, cataract extraction surgical technique. Lenses were to be folded for implantation and inserted into the capsular bag using an insertion system validated by the study sponsor. Following lens implantation within the capsular bag, the lens was rotated/positioned to align the lens axis with the intended orientation using the axis fiducial marks at each of the haptic-optic junctions of the IOL. Viscoelastic was removed, the incision was hydrated, and the IOL position was confirmed with the eye at normal tension. Fine repositioning was done as needed at the discretion of the surgeon. Eye images were captured, and the lid speculum was removed.
Examinations
For all subjects, the operative eye was examined 1 day and approximately 3 months postoperatively. For bilateral subjects, both eyes were evaluated at the same 3-month postoperative visit based on the date of the second eye surgery. Unscheduled visits were conducted as necessary at the discretion of the investigator for medically indicated follow-up.
A novel validated photographic technique was used to assess lens alignment.9 At the time of surgery, a minimum of three baseline photographs of IOL position were captured through the surgical microscope to document the final position of the IOL following surgery (Figure 1A). At each follow-up visit, three pupil-dilated retro-illuminated digital slit lamp photographs showing the location of the IOL axis markings, limbal vessels and iris detail were also taken (Figure 1B). Details of the photographic procedure and analysis have been published elsewhere.8,9 In brief, two trained, independent photo-analysts chose one operative and one postoperative photo with the best quality to analyze to determine the IOL rotation. The operative and postoperative images were analyzed using ocular landmarks to determine the change in lens orientation using the AMO Tecnis Toric Lens Axis Measurement Program8,9 Both analysts were masked to each other’s assessment. If the signed misalignment value was less than or equal to ± 3° the data were averaged across analysts. If the signed misalignment value was greater than ± 3°, both analysts reassessed the images, and if agreement could not be reached the data were deemed “unreliable” and excluded from analysis.
 |
Figure 1 (A) Final position of the IOL following surgery. (B) Postoperative retro-illuminated slit lamp photograph of the same eye with visualization of at least one IOL axis mark on each side, iris, limbal and scleral details. |
Descriptive statistics (mean, SD, minimum and maximum) were calculated for all other variables. Visual acuity was assessed using an Early Treatment Diabetic Retinopathy Study chart at 4.0 meters (13 feet), under photopic (85–110 cd/m2) conditions and letter scores were converted to LogMAR prior to analysis. The frequency and proportion of eyes achieving each acuity line were reported for UDVA and CDVA. The frequency and proportion of eyes with medical/lens findings or adverse events were also reported. For patient and investigator satisfaction questionnaires, the frequency and proportion of each response are reported.
Results
A total of 133 subjects were enrolled, with 8 screen failures, for a total of 125 subjects implanted across 7 clinic sites in the United States. Mean ± SD subject age was 68.4 ± 8.3 years (range 31–88 years); 57.6% were female, 42.4% male; and 89.6% Caucasian, 1.6% Asian, and 7.2% African American. A total of 202 eyes were implanted during the study, with 157 eyes (77.7%) from 77 bilaterally treated subjects and 45 eyes (22.3%) from unilaterally-treated subjects. Two eyes were discontinued for all visit intervals, resulting in 200 eyes at each visit. Valid IOL axis rotation data at the intraoperative and postoperative visits were obtained for 189 subjects at the 1-day visit and 185 subjects at the 3-month visit.
Lens Rotation and Rotational Stability
Mean absolute rotation was 0.82° ± 1.00° and 0.94° ± 0.72° at 1 day (n = 189 eyes) and 3 months (n = 185 eyes), respectively. From the final intraoperative position, 187 of 189 eyes (98.9%) exhibited ≤5° of lens rotation at the 1-day visit and 185 of 185 eyes (100.0%) exhibited ≤5° lens rotation at postoperative 3-months (Figure 2A). The mean signed lens rotation was +0.23° ± 1.27° of counterclockwise change (range 8.32° clockwise to 5.67° counterclockwise) at 1 day and −0.41° ± 1.11° of clockwise change (range 3.01° clockwise to 3.10° counterclockwise, with 67% clockwise and 33% counterclockwise) at 3 months. Between the 1-day and the 3-months visits, 181 eyes exhibited ≤5° of lens rotation with nearly 90% of lenses rotating by ≤2° (Figure 2B). At 3 months, there was no significant correlation between axial length and absolute IOL rotation (linear regression analysis R2 = 0.010, P = 0.09).
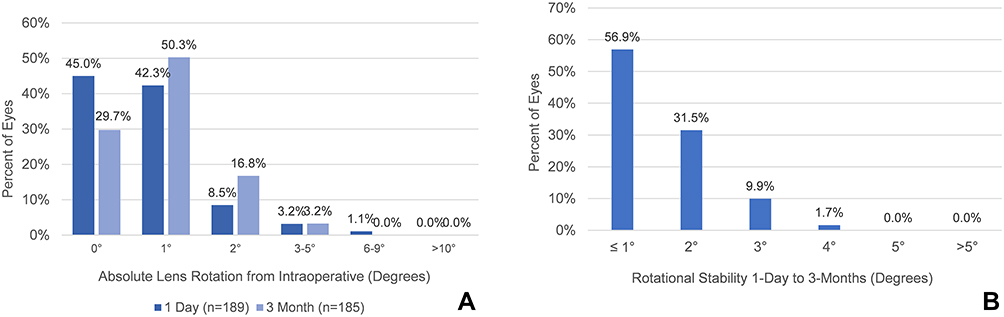 |
Figure 2 (A) Percentage distribution of absolute lens rotation at the 1-day and 3-month visits relative to intraoperative position. (B) Percentage distribution of rotational stability between 1-day and 3-month visits with valid axis data at both visits. |
Performance by Lens Model
Figure 3A shows the distribution of eyes implanted with the different lens models. Figure 3B shows the distribution of eyes with ≤5° of absolute rotation at the 1-day (n = 189 eyes) and 3-month (n = 185 eyes) postoperative visits. Only eyes with valid lens rotation data for these visits are shown. Two lenses (1 model ZCU 225 and 1 ZCU 300) were aligned between 6° and 9° from the intraoperative location at the 1-day visit, but the 3-month data for these two eyes were deemed invalid due to inter-reader differences in axis location determinations. Figure 3C and D show the averaged data of the absolute lens rotation from each analyst at the 1-day and 3-month visits, respectively. The results remained consistent across the lens models used in this study.
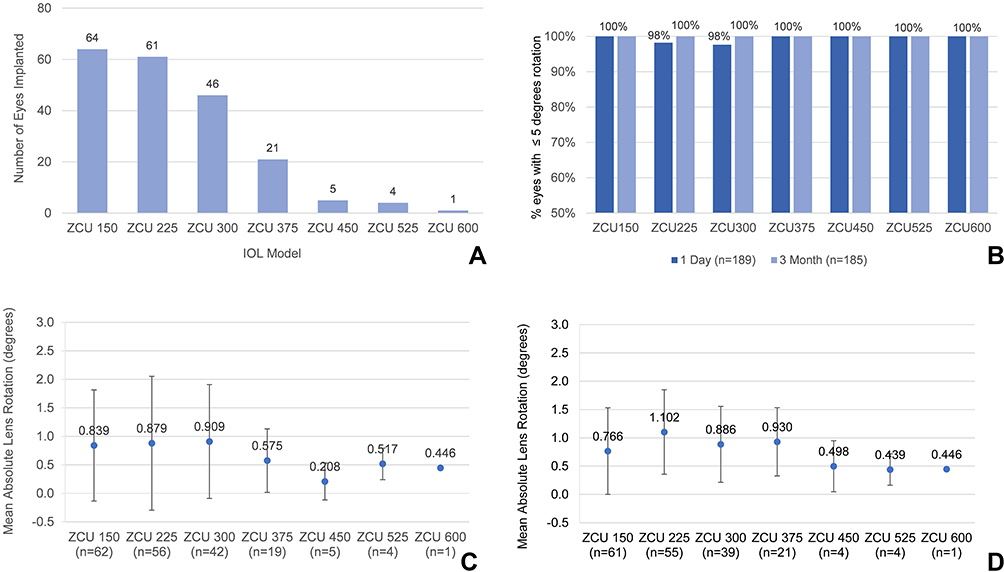 |
Figure 3 (A) Distribution of number of eyes implanted with Tecnis toric II models (Model ZCU). (B) Percentages of eyes with absolute lens rotation of ≤5° at the 1-day and 3-month visits relative to intraoperative position. (C) Mean and standard deviation of absolute lens rotation measured at the 1-day visit by lens model. (D) Mean and standard deviation of absolute lens rotation measured at the 3-month visit by lens model. |
Visual Acuity and Manifest Refraction
At the 3-month visit, mean UDVA and CDVA in logMAR and Snellen equivalent were 0.004 ± 0.115 (20/20) and −0.066 ± 0.092 (20/17), respectively. At 3 months, 180 of 200 (90.0%) of eyes achieved 20/25 or better UDVA and 195 of 200 (97.5%) were correctable to 20/25 or better (Figure 4A).
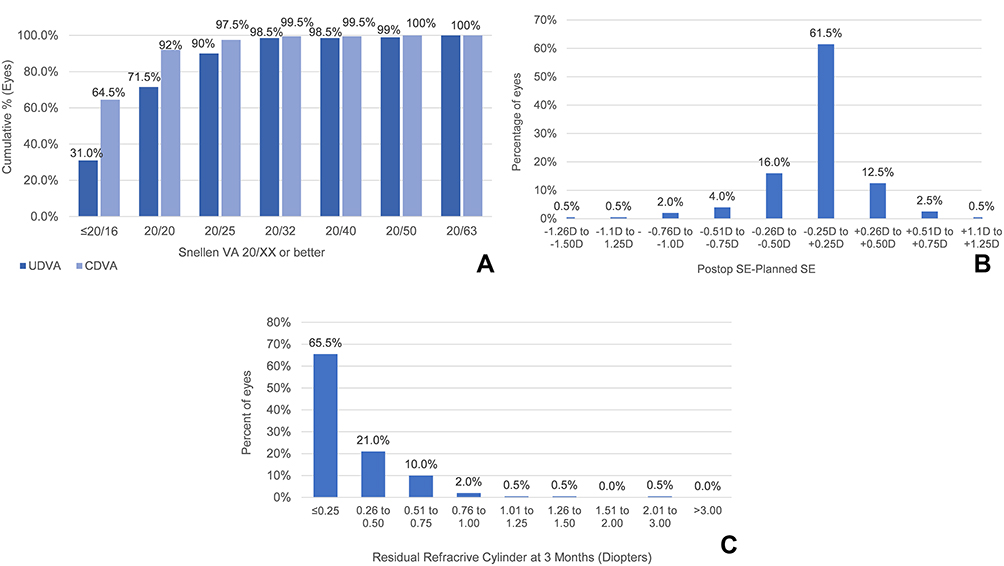 |
Figure 4 (A) Cumulative Snellen uncorrected (UDVA) and corrected (CDVA) distance visual acuity distribution for eyes at 3 months. (B) Percentage distribution of difference between achieved vs planned spherical equivalent refraction at 3 months. (C) Percentage distribution residual refractive cylinder at 3 months. |
Mean refractive results for all implanted eyes were captured at the 3-month visit (Figure 4B and C and Table 1). The mean spherical equivalent (SE) refraction at the 3-month visit was −0.25 ± 0.35 diopters (D). The mean difference between achieved and intended SE was −0.05 ± 0.34 D. The absolute value of the achieved SE versus intended was ± 0.50 D or less for 90% of eyes at the 3-month visit (Figure 4B). For residual refractive cylinder (Figure 4C and Table 1), the results were similarly robust at the 3-month visit with 86.5% of eyes measuring 0.50 D or less residual cylinder, with a mean difference from intended of +0.12 ± 0.35 D (Table 1). The mean percent reduction was 91.9% at 3 months.
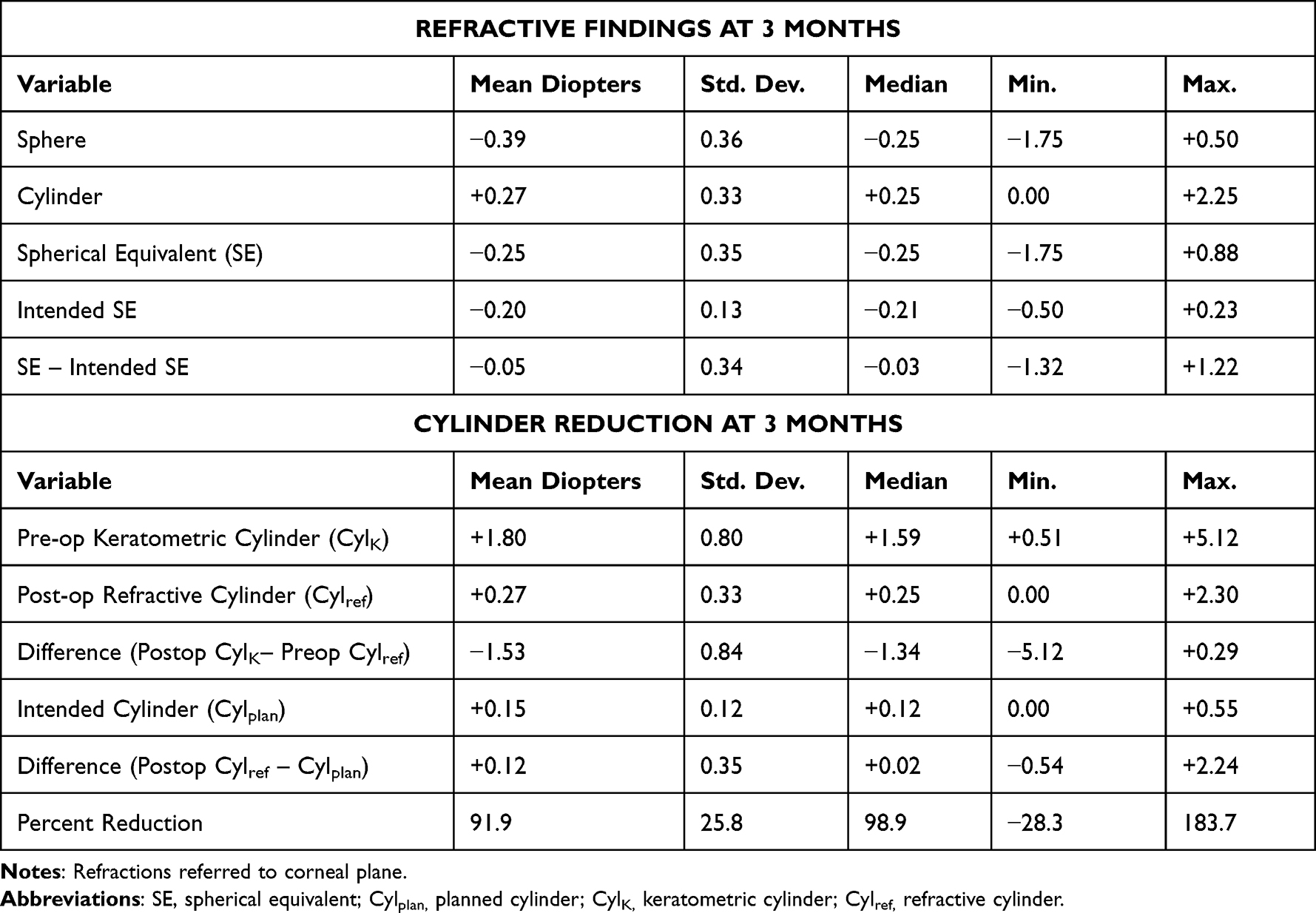 |
Table 1 Refractive Findings and Cylinder Reduction at 3-Month Visit |
Medical Findings and Adverse Events
Four subjects from three sites experienced non-device related, non-ocular serious adverse events. These events required hospitalization but resolved without sequelae. Postoperative IOL repositioning or IOL exchange for IOL misalignment were not required for any eyes. By 3 months, 56 eyes (28%) had developed posterior capsule opacification. Of these, 37 eyes (18.5%) were graded as trace, 16 (8%) as mild, and 3 (1.5%) as moderate. There were no instances of severe posterior capsule opacification.
Surgeon and Patient Satisfaction Questionnaires
Satisfaction questionnaires were completed by surgeons and patients following the 3-month visit. Surgeons were asked to assess clinical outcomes, rotational stability and UDVA performance for all implanted eyes (Figure 5A). Surgeons were satisfied/very satisfied with overall clinical outcomes and rotational stability in 99% of eyes, and with UDVA in 98.5% of eyes. Patient satisfaction was assessed in the 77 bilaterally implanted patients with two questions. When asked about satisfaction with far vision without eyeglasses or contact lenses, 73 of 77 (94.8%) of patients reported being satisfied/very satisfied at the 3-month visit (Figure 5B). Regarding the need to wear eyeglasses or contact lenses to improve distance vision, 68 of 77 (89.5%) reported never feeling the need for distance correction following surgery (Figure 5C).
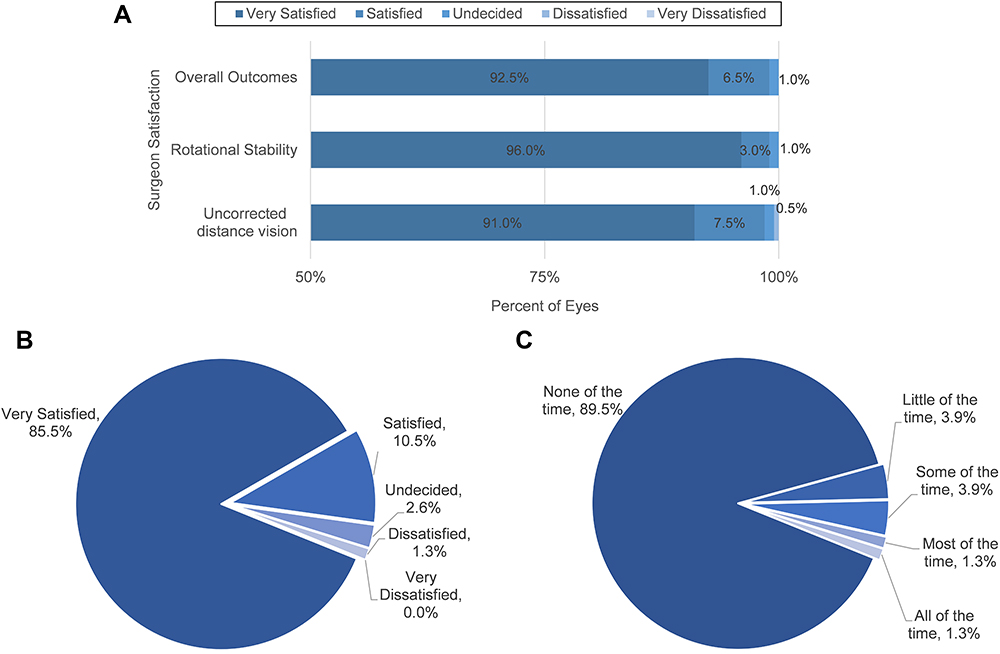 |
Figure 5 (A) Surgeon satisfaction of overall outcomes, rotational stability, and uncorrected distance visual acuity for all implanted eyes. (B) Patient satisfaction in bilaterally implanted study subjects for distance vision without glasses or contact lenses at 3-months. (C) Patient satisfaction in bilaterally implanted subjects on how often they felt the need to wear eyeglasses or contact lenses to improve distance vision at 3-months. |
Discussion
Rotational stability of toric IOLs following implantation is critical to good visual outcomes, particularly with higher magnitude of astigmatism. For each 10° of toric IOL rotation, the residual cylinder is equal to about one-third of the corneal cylinder, creating an under correction of the astigmatic refractive error.13 Most modern toric IOLs show a relatively low amount of misalignment.6,13,14 The original Tecnis toric IOLs (model ZCT) was the first to meet the ANSI standard for rotational stability for toric IOLs (>90% of eyes having ≤5° axis change between consecutive visits three months apart), with ≥93% of toric first eyes having a ≤ 5°axis change.4 However, 3–5° of rotation still amounts to a loss of approximately 10–15% of the astigmatism-reducing effect of a toric IOL, with amounts obviously higher for the outlying values of lens rotation.15
Lee et al reported that while mean misalignment was 2.72° for AcrySof (Alcon Laboratories, Inc., Fort Worth, TX, USA) toric IOLs and 3.79° for Tecnis Toric (Model ZCT) IOLs at the first postoperative check, 8.1% of AcrySof and 18.2% of Tecnis lenses (Model ZCT) were positioned more than 5° from the intended location.6 With the previous design of the Tecnis Toric IOL (Model ZCT), Waltz et al reported that five of 156 eyes (3.2%) rotated 10° or more between day 1 and 6 months: two eyes (1.3%) rotated over 30°, and three eyes (1.9%) rotated between 16° and 30°.4 The results of this study demonstrated a marked improvement in magnitude of lens rotation: mean rotation was less than 1° at both the 1-day and 3-month visits, no lenses rotated more than 10° at the 1-day visit, all were positioned within 5° at the 3-month visit, and 100% remained rotationally stable from 1 day to 3 months postoperatively (<5° rotation). The lens rotation results were very consistent between all seven study sites. The two eyes that displayed between 6° and 9° of misalignment at the 1-day visit were from two different sites, and both exited the study with good UDVA (20/20 and 20/25) and CDVA (20/16 and 20/16), though valid lens rotation data at 3 months were not obtained.
Srinivasan et al recently summarized the many factors that may affect the rotational stability of a toric IOL, including lens material, lens design, size of the capsulorhexis, and surgical technique.16 Of relevance to this study, the use of frosted haptics8,17 and less polished surfaces18 has been demonstrated to improve postoperative lens rotation. In a direct comparison of the new Tecnis Toric model ZCU with frosted haptics (Tecnis Toric II) to the former model ZCT with smooth haptic (Tecnis Toric I), Takaku et al were able to confirm a statistically significant reduction in both the amount and variability of axis misalignment and uncorrected astigmatism.17 They also documented a statistically significant increase in the speed of lens unfolding after ejection from the cartridge and hypothesized that the frosted haptics offer more surface texture, thus reducing the surface stickiness of the hydrophobic acrylic IOL.17
As noted by Inoue et al, the highest risk of post-implantation rotation likely occurs in the first hour after surgery.19 Early error is largely responsible for toric misalignment at future visits, accounting for almost two-thirds of the cases.19 A key question is whether these errors in alignment are due to lens movement from the intraoperative position or from inaccuracies in axis position determination. The use of more standardized and validated techniques for assessing axis location, as discussed below, may shed light on this question. The very low rate and magnitude of malpositioned lenses observed at 1 day following implantation can predict clinical performance, even before visual acuity stabilizes in the post-surgical eye. This premise is supported by the clinical data presented here: axis orientation was excellent at the 1-day postoperative visit, and lens positioning, visual acuity and refractive status remained highly stable over the 3-month study. Further, analysis of same-eye rotational stability between 1 day and 3 months postoperatively demonstrated exceptional performance, far exceeding the ANSI standard for toric lens rotational stability, with 100% of lenses exhibiting ≤5° change in position over the 3 month period. Feedback from both subjects and investigators at 3 months further reinforces the utility of the 1-day lens position data to be a good predictor of success. The data presented here are compelling support for improved rotational stability of this new design.
A key feature of this study was the use of a standardized photographic technique for accurately documenting lens position at the time of surgery and rotation at postoperative visits.9 As noted previously, the impact of IOL rotation can significantly impact efficacy, particularly for high powered toric IOLs, and inaccuracy around orientation measurement should be taken into account when assessing the performance of a given lens.5 Methods typically used for assessing IOL orientation can be affected by head malposition and ocular rotation as well as human error in estimations or measurements using a slit lamp biomicroscope.18 The use of slit lamp protractors by different examiners in other studies is subject to multiple errors in axis identification.14 The methodology utilized in this study can reduce the uncertainty identified by Potvin et al5 (5° in their analysis) considerably: software validation showed precision (repeatability plus reproducibility variation) of 2.22° using slit-lamp photographs.9 This method used iris and scleral landmarks to align the baseline image at the time of implantation, and again later for registration of the images for determination of axis alignment. The use of iris or scleral landmarks and fiducial marks helped control for head tilt, camera rotation and other anomalies that can affect the perceived orientation of the lens. The use of custom, proprietary software with repeated and masked observers helped to standardize measurements.
The novel validated photographic technique for assessing lens position provides evidence that this new toric IOL design with frosted haptics can help to increase surgical success, patient satisfaction, and surgeon confidence in a toric IOL approach for cataract patients with astigmatism. This study, while not a head to head comparison to other toric options, provides confirmation that this improved lens design yields robust technical and clinical outcomes that address past reports of rotational instability with the original Tecnis Toric IOL. This improved toric design is now incorporated into other IOL designs giving physicians presbyopia-correcting options for their patients with clinically significant levels of astigmatism.20,21 The ongoing improvements and continued success of toric IOLs is critical to meeting the needs of a greater proportion of the growing presbyopic population in the US and abroad.
Data Sharing Statement
The authors do not intend to share individual deidentified participant data. A summarized report with endpoints data tables based on statistical plan and analysis may be requested directly from the corresponding author for consideration. Access to anonymized data may be granted following review. Content with granted access will be available through email or other appropriate formats and for 3 months, upon review and consideration.
Acknowledgments
Manuscript development and editorial support was provided by C Schnider Insights (Vancouver, WA) and iBiomedical Consulting (Neptune Beach, FL), and funded by Johnson & Johnson Surgical Vision, Inc. The following surgeons participated in this clinical study: Jerry Hu, MD (Texas Eye & Laser Center, Hurst, TX), Daniel Chang, MD (Empire Eye & Laser Center, Bakersfield, CA), Jason Jones, MD (Jones Eye Clinic, Sioux City, IA), Michael Snyder, MD (Cincinnati Eye Institute, Cincinnati, OH), Jeffrey Whitman, MD (Key-Whitman Eye Center, Dallas TX), Kevin M. Miller, MD (The Regents of the University of California on behalf of its Los Angeles Campus UCLA Clinical Trials Contracts and Strategic Relations, Los Angeles, CA), Michael Greenwood, MD (Vance Thompson ND, Prof. LLC, West Fargo, ND)
Funding
This study was supported by Johnson & Johnson Surgical Vision, Inc., which participated in the design and conduct of the study.
Disclosure
D.C: Consultant for Johnson & Johnson Surgical Vision. He also reports grants, personal fees, and/or non-financial support from Johnson & Johnson Vision, Acufocus, and Carl Zeiss Meditec, outside the submitted work. J.H: Performs research supported by, speaks for Johnson & Johnson Surgical Vision. K.M.M.: Performs research supported by, speaks for Johnson & Johnson Surgical Vision. S.V and W.Z: Employees of Johnson & Johnson Surgical Vision. The authors report no other conflicts of interest in this work.
References
1. Miller KM, Oetting TA, Tweeten JP, et al. Cataract in the adult eye preferred practice pattern. Ophthalmology. 2022;129(1):P1–P126. doi:10.1016/j.ophtha.2021.10.006
2. Anderson DF, Dhariwal M, Bouchet C, Keith MS. Global prevalence and economic and humanistic burden of astigmatism in cataract patients: a systematic literature review. Clin Ophthalmol. 2018;12:439–452. doi:10.2147/OPTH.S146829
3. Nanavaty MA, Bedi KK, Ali S, Holmes M, Rajak S. Toric intraocular lenses versus peripheral corneal relaxing incisions for astigmatism between 0.75 and 2.5 diopters during cataract surgery. Am J Ophthalmol. 2017;180:165–177. doi:10.1016/j.ajo.2017.06.007
4. Waltz KL, Featherstone K, Tsai L, Trentacost D. Clinical outcomes of TECNIS toric intraocular lens implantation after cataract removal in patients with corneal astigmatism. Ophthalmology. 2015;122(1):39–47. doi:10.1016/j.ophtha.2014.06.027
5. Potvin R, Kramer BA, Hardten DR, Berdahl JP. Toric intraocular lens orientation and residual refractive astigmatism: an analysis. Clin Ophthalmol. 2016;10:1829–1836. doi:10.2147/OPTH.S114118
6. Lee BS, Chang DF. Comparison of the rotational stability of two toric intraocular lenses in 1273 consecutive eyes. Ophthalmology. 2018;125(9):1325–1331. doi:10.1016/j.ophtha.2018.02.012
7. Kramer BA, Hardten DR, Berdahl JP. Rotation characteristics of three toric monofocal intraocular lenses. Clin Ophthalmol. 2020;14:4379–4384. doi:10.2147/OPTH.S285818
8. Vukich JA, Ang RE, Straker BJK, et al. Evaluation of intraocular lens rotational stability in a multicenter clinical trial. Clin Ophthalmol. 2021;15:3001–3016. doi:10.2147/OPTH.S309214
9. Kasthurirangan S, Feuchter L, Smith P, Nixon D. Software-based evaluation of toric IOL orientation in a multicenter clinical study. J Refract Surg. 2014;30(12):820–826. doi:10.3928/1081597X-20141117-01
10. Quesada GA, Quesada RA, Jones JJ, et al. Reproducibility of the magnitude of lens rotation following implantation of a toric intraocular lens with modified haptics. Clin Ophthalmol. 2022;16:3213–3224. doi:10.2147/OPTH.S373976
11. Keshav V, Henderson BA. Astigmatism management with intraocular lens surgery. Ophthalmology. 2021;128(11):e153–e163. doi:10.1016/j.ophtha.2020.08.011
12. American National Standards Institute (ANSI). Z80.30-2018 Ophthalmics - Toric intraocular lenses; 2018.
13. Felipe A, Artigas JM, Diez-Ajenjo A, Garcia-Domene C, Alcocer P. Residual astigmatism produced by toric intraocular lens rotation. J Cataract Refract Surg. 2011;37(10):1895–1901. doi:10.1016/j.jcrs.2011.04.036
14. Bauer NJ, de Vries NE, Webers CA, Hendrikse F, Nuijts RM. Astigmatism management in cataract surgery with the AcrySof toric intraocular lens. J Cataract Refract Surg. 2008;34(9):1483–1488. doi:10.1016/j.jcrs.2008.05.031
15. Hirnschall N, Maedel S, Weber M, Findl O. Rotational stability of a single-piece toric acrylic intraocular lens: a pilot study. Am J Ophthalmol. 2014;157(2):405–411. doi:10.1016/j.ajo.2013.09.032
16. Srinivasan S. Correction of corneal astigmatism and stability of toric intraocular lenses. J Cataract Refract Surg. 2021;47(11):1385–1386. doi:10.1097/j.jcrs.0000000000000836
17. Takaku R, Nakano S, Iida M, Oshika T. Influence of frosted haptics on rotational stability of toric intraocular lenses. Sci Rep. 2021;11(1):15099. doi:10.1038/s41598-021-94293-3
18. Vandekerckhove K. Rotational stability of monofocal and trifocal intraocular toric lenses with identical design and material but different surface treatment. J Refract Surg. 2018;34(2):84–91. doi:10.3928/1081597X-20171211-01
19. Inoue Y, Takehara H, Oshika T. Axis misalignment of toric intraocular lens: placement error and postoperative rotation. Ophthalmology. 2017;124(9):1424–1425. doi:10.1016/j.ophtha.2017.05.025
20. Johnson & Johnson Vision. TECNIS Synergy IOL with TECNIS Simplicity Delivery System. TECNIS Synergy Toric II IOL with TECNIS Simplicity Delivery System; 2021. Available from: https://www.jnjvisionpro.com/sites/us/files/public/surgical/IOLs/tecnis_eyhance_toric_ii_iol_dfu_final.pdf.
21. Johnson & Johnson Vision. TECNIS Eyhance Toric II IOL with TECNIS Simplicity Delivery System; 2021. Available from: https://www.jnjvisionpro.com/sites/us/files/public/surgical/IOLs/tecnis_eyhance_toric_ii_iol_dfu_final.pdf.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.