Back to Journals » Clinical Ophthalmology » Volume 19
Post-Cataract Surgery Endophthalmitis Prophylaxis Survey in Thai Ophthalmologists
Authors Kasetsuwan P ![]() , Chansangpetch S, Pruksacholavit J, Surawatsatien N
, Chansangpetch S, Pruksacholavit J, Surawatsatien N ![]() , Pongsaschareonnont PF
, Pongsaschareonnont PF ![]() , Reinprayoon U
, Reinprayoon U
Received 21 August 2025
Accepted for publication 3 November 2025
Published 12 December 2025 Volume 2025:19 Pages 4585—4596
DOI https://doi.org/10.2147/OPTH.S562258
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Bharat Gurnani
Pimpetch Kasetsuwan,1,2 Sunee Chansangpetch,1,3 Jipada Pruksacholavit,1,2 Nuntachai Surawatsatien,1,4 Pear Ferreira Pongsaschareonnont,4,5 Usanee Reinprayoon1,6
1Department of Ophthalmology, King Chulalongkorn Memorial Hospital, Thai Red Cross Society, Bangkok, Thailand; 2Department of Ophthalmology, Faculty of Medicine, Chulalongkorn University, Bangkok, Thailand; 3Center of Excellence in Glaucoma, Department of Ophthalmology, Faculty of Medicine, Chulalongkorn University, Bangkok, Thailand; 4Center of Excellence in Retina, Department of Ophthalmology, Faculty of Medicine, Chulalongkorn University, Bangkok, Thailand; 5Department of Ophthalmology, Faculty of Health Sciences, Queen’s University, Kingston, Ontario, Canada; 6Center of Excellence for Cornea and Stem Cell Transplantation, Department of Ophthalmology, Faculty of Medicine, Chulalongkorn University, Bangkok, Thailand
Correspondence: Usanee Reinprayoon, Center of Excellence for Cornea and Stem Cell Transplantation, Department of Ophthalmology, Faculty of Medicine, Chulalongkorn University, 1873 Rama IV Road, Pathumwan, Bangkok, Thailand, Email [email protected]
Purpose: To determine current perioperative practice patterns for the prevention of endophthalmitis following cataract surgery in Thailand.
Design: Cross-sectional Survey Study.
Methods: An online questionnaire was distributed nationwide to certified ophthalmologists, consisting of 21 questions covering 10 preoperative, 7 intraoperative, and 4 postoperative measures for the prevention of post-cataract surgery endophthalmitis. Subgroup analyses were performed to compare practices between general ophthalmologists, retina/uveitis specialists (R/U), and other subspecialists (Non-R/U).
Results: A total of 426 responses were analyzed. Preoperative topical antibiotics (21.1%, n = 90) and oral antibiotics (4.9%, n = 21) were rarely prescribed. The most common antiseptic for skin preparation was 10% povidone-iodine (72.3%, n = 308). Intracameral antibiotics were adopted by 54.7% of respondents (n = 233). Postoperative topical antibiotics were almost universally prescribed (99.5%, n = 424). Moxifloxacin was the most preferred topical (preoperative: 45.6%, n = 41, postoperative: 46.4%, n = 197) and intracameral (57.1%, n = 133) antibiotic. Subspecialty analysis revealed that R/U specialists were more prone to use 10% povidone-iodine (relative risk ratio [RRR] 2.37, 95% CI 1.16 to 4.82) and antiseptic applied to fornix (RRR 2.62, 95% CI 1.26 to 5.46) than the general ophthalmologist group.
Conclusion: Although the majority of Thai ophthalmologists align their practices with international endophthalmitis prevention guidelines, certain practices were less frequently adopted than recommended. These findings emphasize the need for standardized national practice patterns to enhance surgical outcomes.
Keywords: phacoemulsification, infection, prevention, antiseptics, intracameral, antibiotics
Introduction
Cataract surgery is the most frequently performed ophthalmic surgery worldwide, with over 20 million surgeries conducted per year.1 Postoperative endophthalmitis represents one of the most serious vision threatening complications of cataract surgery, leading to high medical costs and socioeconomic burdens. Globally, the incidence of postoperative endophthalmitis show substantial country-specific variation. In the United States, rates ranged from 0% to 0.61%, whereas the frequency reached 0.01% to 0.71%, and 0.03% to 0.7%, in Asian and European countries, respectively.2
International organizations worldwide have established numerous clinical practice guidelines to implement perioperative interventions to dampen the incidence of postoperative endophthalmitis. For instance, the European Society of Cataract and Refractive Surgeons (ESCRS) conducted a study on identifying risk factors of ocular infection following cataract surgery in 2007, and subsequently recommended prophylactic antimicrobial measures.3 Similarly, in 2021, the American Academy of Ophthalmology (AAO) released preferred practice guidelines for the management of cataract in adults.4 While these guidelines largely impacted the clinical practices of ophthalmologists globally, these practices must be tailored with the regional settings and, notably, to fit with the healthcare infrastructure.
Despite these guidelines, the health system of Thailand currently lacks a national consensus or guidelines on prophylactic measures for preventing postoperative endophthalmitis. In 2014, a survey of 72 Thai ophthalmologists assessed the practices related to endophthalmitis prophylaxis following cataract surgery.5 Since then, strategies for preventing endophthalmitis after cataract surgery were updated worldwide. In the absence of a clear national consensus, these new recommendations were differently adopted by Thai ophthalmologists.
In the present study, a newly designed nationwide survey was conducted on the prevention of endophthalmitis after cataract surgery to identify current trends in perioperative interventions used by Thai ophthalmologists and to explore potential differences in practice between subspecialties, capturing changes over the past decade and providing broader national representation compared with the 2014 survey.5
Methods
This cross-sectional study was approved by The Institutional Review Board of the Faculty of Medicine, Chulalongkorn University, Bangkok, Thailand (IRB No. 0462/66). An online survey was designed with Google Forms (Google LLC, California, USA) and reviewed by the research team of the Department of Ophthalmology, Chulalongkorn University. Participants were invited to respond the survey during The Royal College of Ophthalmologist of Thailand (RCOPT) annual meeting held in November, 2023. They accessed the survey with an online link and QR code. Additionally, the survey was posted on Line, the most commonly used messaging application in Thailand (Line Corporation, LY Corporation, Tokyo, Japan).6 RCOPT and subspecialty societies then distributed the survey using their official LINE accounts, enhancing visibility of the survey in the hope of attracting more participants from across the country. Responses were collected over a period of 4 months, from November 27, 2023, to March 26, 2024.
The survey comprised four sections. The first section covered general participant information. Subsequent sections investigated perioperative measures for the endophthalmitis prevention following cataract surgery including preoperative, intraoperative, and postoperative practice patterns. These sections encompassed various aspects such as the application of antiseptics, the use of antibiotics, including class of antibiotics, route of administration, and duration, as well as postoperative recommendations. The questions were developed based on recommendations from major international guidelines and evidence from previous literature on endophthalmitis prophylaxis following cataract surgery.2,3,7,8 The translated version of the questionnaire is provided in Supplementary Material.
Participants provided implied consent by voluntarily completing and submitting the survey. All participants completed the survey anonymously. Data adjudication was conducted by two independent researchers (PK and SC). Descriptive statistics were used to summarize the responses and background characteristics of survey participants. The association between variables was examined using the Chi-square or Fisher’s exact test, when appropriate. The preferred practice was compared between groups defined by subspecialties, namely general ophthalmologists (GenOph), retina/uveitis (R/U) specialists, and other subspecialists (Non-R/U). Binary logistic regression or multinomial logistic regression was used for pairwise comparisons with an adjustment for experience factors, ie, year in practice and volume of cataract surgery performed. Data were analyzed using Stata version 16.0 (StataCorp, College Station, Texas, USA). P value < 0.05 was considered statistically significant.
Results
Four hundred and twenty-six ophthalmologists from across Thailand participated in the study. Most respondents (60.1%, n = 256) had less than ten years of experience in ophthalmology. Nearly half of the participants performed more than twenty cataract surgeries per month. One-third of the participants were general ophthalmologists. Specialists on retina or uveitis accounted for 19.9% of the participants (n = 85), whereas practitioners with other subspecialties reached 47.2% (n = 201). Most respondents (97.7%, n = 416) routinely performed phacoemulsification, while only ten individuals did not. Of these, nine were general ophthalmologists, and the other practitioner was an oculoplastic surgeon. Table 1 shows demographic data of the participants.
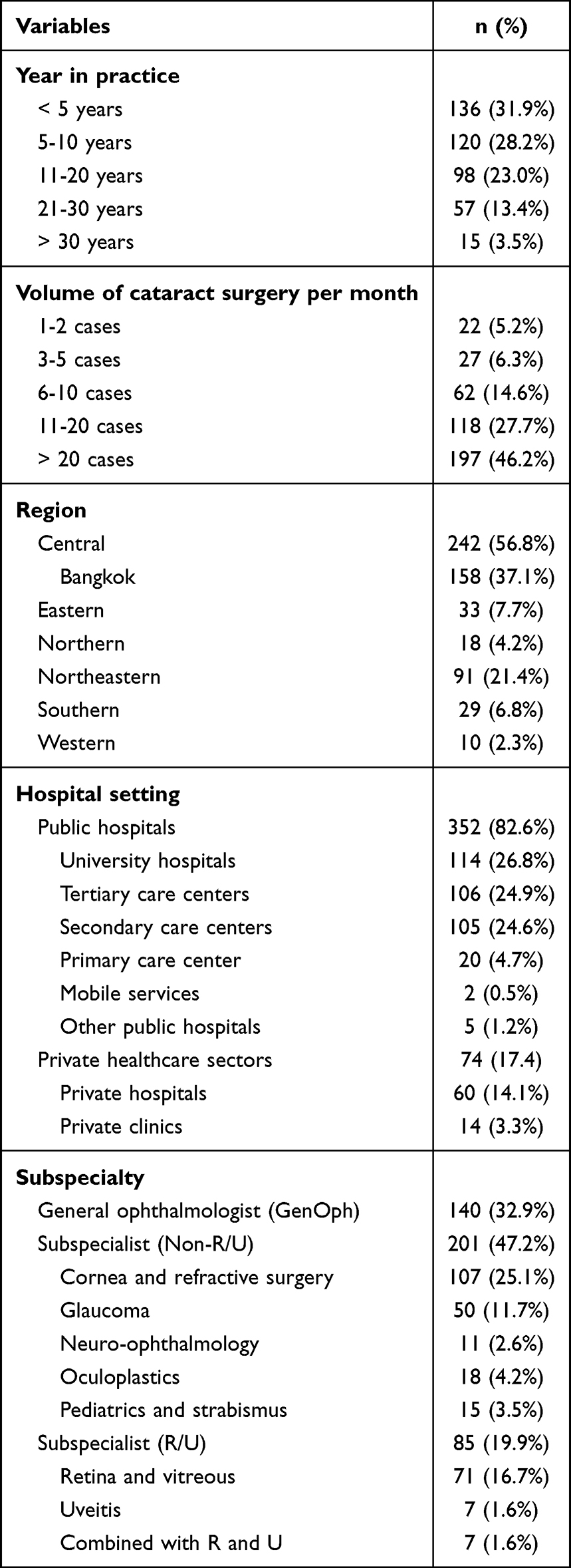 |
Table 1 Demographic Data |
Topical antibiotics (21.1%, n = 90) and oral antibiotics (4.9%, n = 21) were not prescribed, and eyelash trimming (5.4%, n = 23) was not performed by most respondents as preoperative measures. In contrast, face washing was a routine practice adopted by most participants (65.3%, n = 278), with soap being the most commonly used cleaning agent (45.3%, n = 126 of 278), followed by chlorhexidine (37.1%, n = 103 of 278), and povidone-iodine (PVI) (16.9%, n = 47 of 278) scrub. The most common antiseptic agents used for skin preparation was PVI at a concentration of 10% (72.3%, n = 308) or 5% (26.8%, n = 114) and typically applied for 3 minutes (33.8%, n = 144). Additional preoperative measures were implemented by most surveyed ophthalmologists including scrubbing the eyelids and eyelashes (66.9%, n = 285), administration of antiseptic into the conjunctival fornix (71.1%, n = 303), and irrigation of the eye with diluted PVI solution (63.8%, n = 272). The large majority of cataract surgery was performed by sutureless (96.1%, n = 398) clear corneal incisions (99.5%, n = 413), with incision sizes of 2.75 to 3 mm (94.0%, n = 390). Intracameral administration of antibiotics was adopted by a slight majority of respondents (54.7%, n = 233), whereas very few surgeons administered subconjunctival antibiotics (1.6%, n = 7). However, most respondents instilled topical antibiotics (88.0%, n = 375) and applied ophthalmic ointment (69.5%, n = 296) at the end of cataract surgery. Maxitrol was the most used ointment formulation consisted of a combination of neomycin sulfate, polymyxin B sulfate, and dexamethasone. Table 2 shows the preferred surgical technique, preoperative and perioperative measures to prevent endophthalmitis.
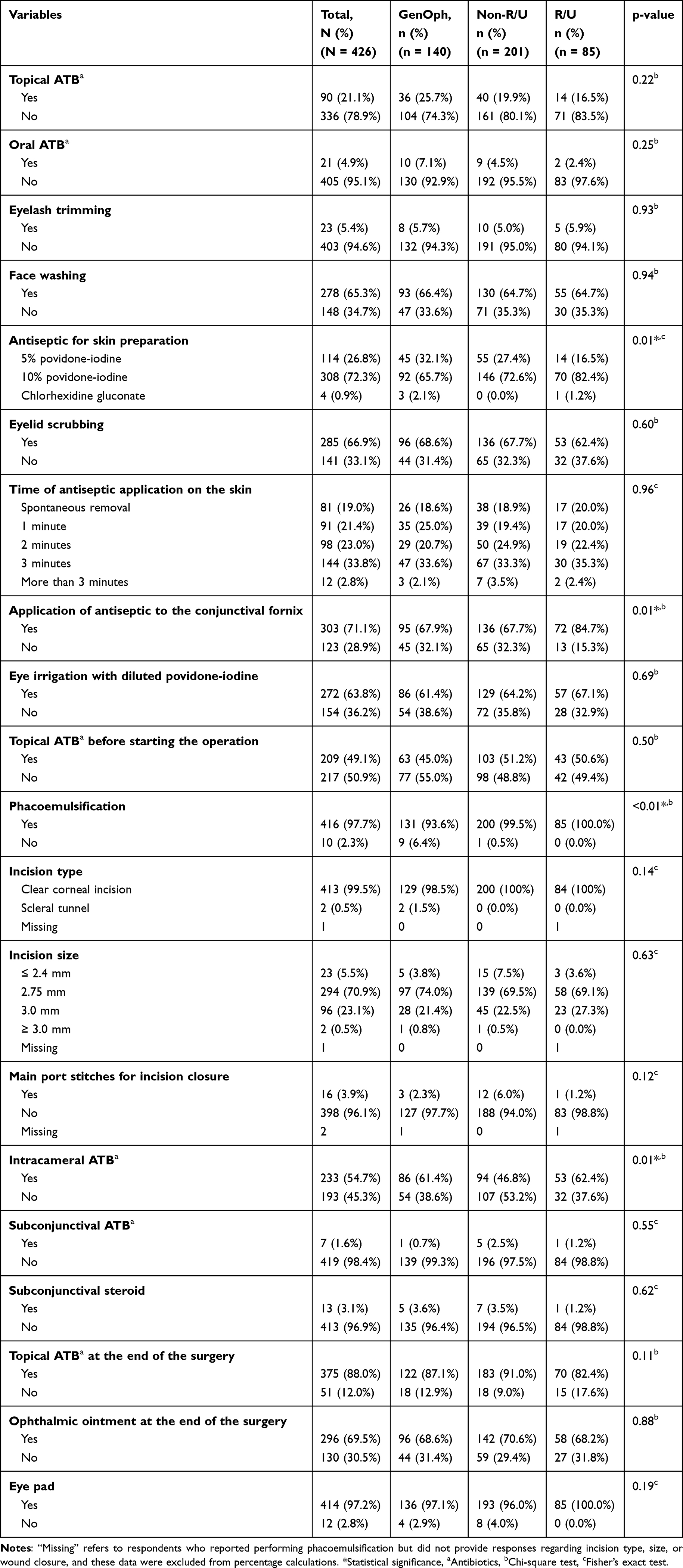 |
Table 2 Preoperative and Intraoperative Prophylactic Measures, and Surgical Techniques |
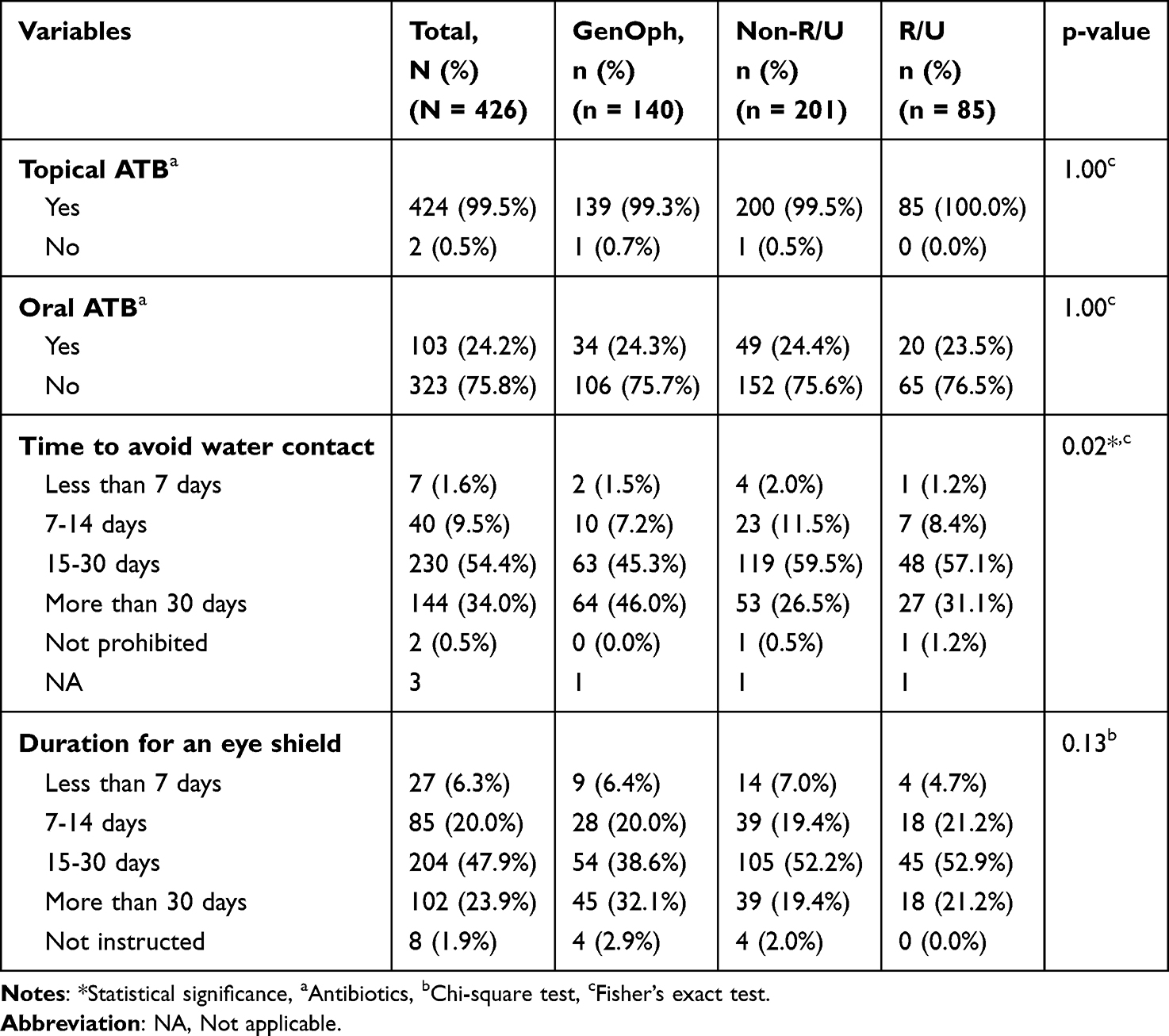 |
Table 3 Postoperative Prophylactic Measures |
Almost all respondents prescribed postoperative antibiotics in topical form (99.5%, n = 424), while oral antibiotics were much less frequently prescribed (24.2%, n = 103). Table 3 shows the preferred postoperative measures.
For subspecialty analysis, significant differences regarding preoperative antiseptic measures were observed among GenOph, R/U, and non-R/U groups. R/U specialists were prone to use 10% PVI solution and apply antiseptic over the fornix before surgery compared with the other groups (type of antiseptic, p = 0.03; antiseptic applied to the fornix, p = 0.01). Logistic regression, following the adjustment for experience factors, evidenced a greater tendency to use 10% PVI solution (relative risk ratio [RRR] 2.37, 95% CI 1.16 to 4.82, p = 0.18) and antiseptic (RRR 2.62, 95% CI 1.26 to 5.46, p = 0.10) applied to fornix among R/U doctors compared with general ophthalmologists.
Both R/U specialists and general ophthalmologists showed a greater preference for intracameral antibiotics usage than the other subspecialties group (p = 0.01). However, this difference was no longer significant by the adjustment for experience factors (all p > 0.05).
The three preferred preoperative topical, topical before starting the surgery, intracameral, and postoperative topical antibiotics are presented in Table 4. These antibiotics were similarly adopted by each subspecialty subgroup (all p > 0.05, data not shown).
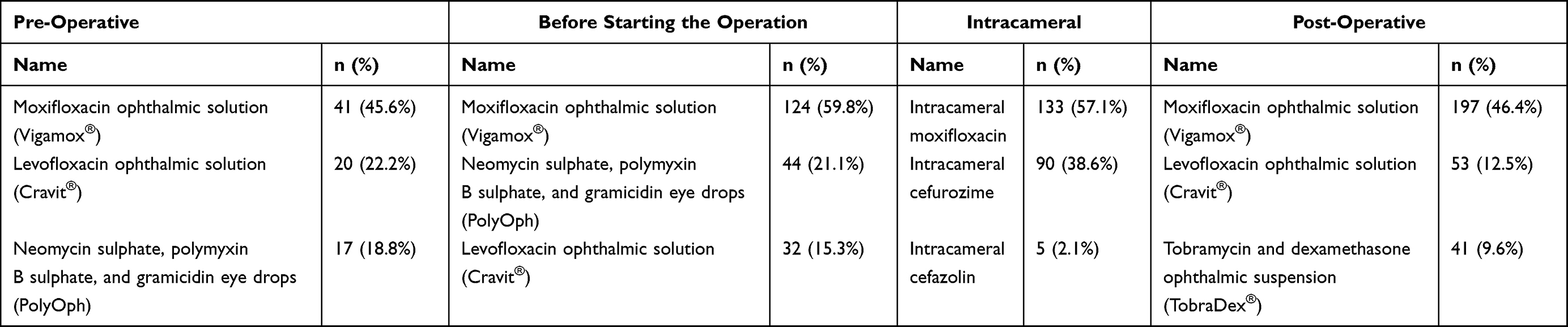 |
Table 4 The Three Most Preferred Antibiotics for Antimicrobial Prophylaxis |
Discussion
The present survey provided an overview of the current preferred practices adopted by Thai ophthalmologists for preventing endophthalmitis after cataract surgery. To our knowledge, the survey, by successfully reaching 27% of currently active ophthalmologists across Thailand, is the largest one in the ophthalmology field. The interest of our study was also driven by examining variations in practices among different subspecialties, as it included a wide range of subspecialty-trained ophthalmologists.
The majority of the respondents were shown to perform sutureless clear corneal phacoemulsification, reflecting a practice that aligns with the preferred standard technique for cataract surgery worldwide.9 Although the type and size of the incision have been proposed as potential risk factors for endophthalmitis,3,10 strong evidence supporting this association is missing so far. Furthermore, wound suturing is not universally recommended.
Preoperative skin preparation to improve lid hygiene and minimize bacterial contamination in the periorbital area is routinely performed by surgeons and includes face washing, eyelash trimming, antiseptic application, and eyelid scrubbing. Our study confirmed that 65.3% of respondents recommended a face wash before cataract surgery, even if the direct effectiveness of preoperative facial cleansing in preventing postoperative endophthalmitis is poorly evidenced.11
Many studies have reported that eyelash trimming provides no significant benefit in reducing periocular bacterial flora. Consequently, ESCRS guidelines do not recommend this measure for post-cataract surgery endophthalmitis prophylaxis.3,12,13 Of note, 94.6% of respondents in our study did not perform eyelash trimming before cataract surgery.
Prophylactic antiseptic application is widely adopted for almost all surgical procedures. In ocular surgeries, PVI and chlorhexidine, due to their broad-spectrum antimicrobial activity, are commonly used for preoperative preparation of the periocular area. However, chlorhexidine is less frequently used because of its potential risk of corneal toxicity.14–16 Together with antiseptic application, some surgeons also included eyelid scrubbing into their routine practice. Eyelid scrubbing was adopted by two-thirds of the surveyed surgeons, despite the lack of evidence supporting a significant reduction in conjunctival bacterial load or additional antibacterial benefits during cataract surgery.17,18
The Asia-Pacific Association of Cataract and Refractive Surgeons (APACRS), AAO, and ESCRS guidelines advocate PVI as an essential preoperative measure for endophthalmitis prevention. Both AAO and APACRS recommend instillation of 5% PVI solution into the conjunctival sac, with APACRS specifying a minimum contact time of 2 minutes. ESCRS not only promotes the concentration of 5% PVI but also advises higher concentration, such as 10%, to be applied to the conjunctival sac and periorbital area, with a minimum application time of 3 minutes. ESCRS additionally notes that 5% PVI solutions contain more free iodine than 10% PVI solutions, which might give better bactericidal activity.3,4,7 Our survey showed that nearly 60% of respondents adhered to these recommendations and applied antiseptics for at least 2 minutes, while the other ophthalmologists reported using shorter contact times. As 10% PVI solution is more readily available in Thailand, the 5% PVI concentration, as expected, is used by a minority of surveyed surgeons (26.8%). Moreover, the instillation of antiseptics into the conjunctival sac was routinely performed by 71.1% of respondents, while 63.8% additionally reported irrigating the eyes with a diluted PVI solution. In Thailand, this is commonly prepared by diluting a stock PVI solution to 1% using normal saline or balanced salt solution. Although evidence suggests that low concentrations of PVI (0.1–1.0%) release higher levels of free iodine and provide superior bactericidal activity compared with more concentrated solutions, this effect is short-acting. Thus, this lower concentration not only reduces the risk of ocular surface irritation but also offers strong bactericidal efficacy. However, excessive dilution may compromise antimicrobial persistence and require repeated application to maintain its effect.19–21 Further evidence is needed to determine whether a one-time application by irrigating with a diluted solution is adequate.
Whereas the use of preoperative antibiotics is widely endorsed to prevent the development of endophthalmitis after cataract surgery, there is no consensus regarding the type of antibiotics, the route of administration, and the optimal duration of application.22 Although topical antibiotics remain so far the most commonly used form preoperatively, their use has recently declined due to insufficient supporting evidence. Several studies reported that PVI alone or combined with fourth-generation topical antibiotics produces similar effects on the conjunctival bacterial load.23,24 ESCRS and AAO guidelines also concluded that preoperative topical antibiotics offer no significant benefit and even may induce the development of antibiotic resistance.3,4
Despite the lack of evidence on their efficacy, many ophthalmologists continue to incorporate preoperative topical antibiotics into their standard practice. A survey conducted by the American Society of Cataract and Refractive Surgery (ASCRS) revealed that the use of preoperative topical antibiotics remains relatively high, even if a light decline was observed over time (from 88% in 2007 to 85% in 2014, and to 73% in 2021). According to this survey, the application of topical gatifloxacin or moxifloxacin for three days was the most frequently prescribed preoperative regimen.25
Our survey clearly showed that preoperative topical antibiotics are no longer routinely prescribed in Thailand. Indeed, whereas a study in 2014 reported that 83.4% of Thai ophthalmologists incorporated this practice into their routine, typically within one day before surgery, 78.9% of respondents in this present survey abandoned it.5 This shift likely reflects increasing awareness of the appropriate use of antibiotics and growing concern about antimicrobial resistance, which has become a major public health issue worldwide.2 The unnecessary use of preoperative prophylactic antibiotics may contribute to the development of resistant ocular flora, complicate the management of postoperative infections, and increase the overall healthcare burden.2–4
About 55% of the respondents used intracameral antibiotics during cataract surgery. This rate substantially increased as, in 2014, only 19.4% of Thai ophthalmologists adopted this measure.5 The present rate is comparable to those reported in several Asian and European countries.8,26–29 The ESCRS study, a large randomized control trial, demonstrated that intracameral cefuroxime significantly reduces the endophthalmitis rate.3 Subsequent studies showed that adding intracameral cefuroxime or moxifloxacin to postoperative topical antibiotics lowers the incidence of endophthalmitis, with no evidence supporting the superiority of one antibiotic over the other.4 Despite strong evidence of efficacy, the routine use of intracameral antibiotics in cataract surgery is not implemented in many countries including Thailand, primarily due to the lack of commercially available preparations.8,29 Our study showed that the unpreserved topical moxifloxacin (Vigamox) is the most selected option for intracameral injection. This preference is likely explained by the potential concentration issues during on-site compounding of cefuroxime, which can lead to severe toxicity in case of dilution errors.4
To date, no conclusive evidence supports the efficacy of antibiotic eye ointments applied at the end of cataract surgery. A retrospective study by Zhang et al found no significant difference in infection rates between patients who received tobramycin-dexamethasone ointment at the end of intraocular surgery and those who did not. The ointment group reported more post-operative discomfort and worse anterior chamber reactions.30 Whereas ointment application at the end of cataract surgery remains a common practice in Thailand (adopted by 69.5% of respondents), its role requires further evaluation due to a lack of proven benefits and potential associated risks.30
In our survey, 99.5% of respondents reported using postoperative antibiotic eye drops. This percentage is consistent with findings from previous surveys, including those measured by the All India Ophthalmological Society (AIOS) in 2017 (94.4%), the ASCRS survey in 2021 (86%), and a survey of Asian eye institutions in 2023 (88–95%), where moxifloxacin, gatifloxacin, and levofloxacin were preferred antibiotics based on patient risk factors.8,25,31 However, a systematic review and meta-analysis did not find strong evidence to conclude that postoperative topical antibiotic therapy prevents endophthalmitis but also raised concerns about its potential contribution to antimicrobial resistance.2
In summary, intracameral antibiotics have demonstrated clear benefits in preventing postoperative endophthalmitis. In contrast, the use of topical antibiotics before or after cataract surgery remains controversial, as there is no strong evidence supporting their efficacy. Moreover, concerns regarding potential adverse effects, such as antibiotic resistance, have been raised.3,32
Practices Among Subspecialties
A previous study showed that surgical practices for the management of open globe injuries were differently adopted by vitreoretinal surgeons and other subspecialists.33 As patients with endophthalmitis are typically referred to retinal or uveitis specialists, our analysis evaluated whether practice patterns differed by subspecialty. Our findings suggested that R/U specialists tend to adhere more closely to ASCRS and ESCRS endophthalmitis prevention guidelines, especially for the use of antiseptics in the conjunctival fornix and intracameral antibiotics.3,25 Additionally, R/U specialists were less likely to use preoperative oral antibiotics and perioperative topical antibiotics compared with other groups, though these differences were not statistically significant. Notably, the R/U group showed the highest proportion (82.4%) of practitioners using 10% PVI solution as a preoperative antiseptic, whereas about one-third of general ophthalmologists and one-fourth of other subspecialties utilized 5% solution. Further research is needed to evidence the effects of practice differences on the rate of post-cataract surgery endophthalmitis.
Summary
In conclusion, this assessment provided insight into the common practices implemented by ophthalmologists from Thailand for endophthalmitis prevention following cataract surgery. Although most practices complied with the international endophthalmitis prevention guidelines, our study identified some barriers for the full adherence to these recommendations and found that certain measures, particularly the routine use of preoperative and postoperative antibiotics, continue to be practiced despite limited evidence supporting their efficacy and potential associated risks. The survey also indicated that subspecialty training may affect practice variation. These findings emphasize the need of developing a national consensus guidelines on endophthalmitis prophylaxis to align clinical practice with evidence-based recommendations, promote standardized approaches across institutions, and improve cataract surgery outcomes in Thailand.
Strengths and Limitations
The strength of this study is characterized by the number of respondents. The present survey on endophthalmitis prevention practice is the largest survey conducted in Thailand, enrolling ophthalmologists from different regions and various hospital settings. However, there are some limitations. First, although it is the largest nationwide survey in this field, it included only approximately one-quarter of Thai ophthalmologists, which may limit the generalizability of our conclusions. Second, more than half of the respondents were from the central region of Thailand, while the rest were from other regions, with relatively few responses from some areas. Therefore, regional analysis was not included, as it may not accurately represent variations in clinical practice patterns among ophthalmologists across Thailand. Third, the respondents were instructed to report only their routine surgical practices in their primary settings. Thus, specific practices for complex cases and operations such as extracapsular cataract extraction (ECCE) or small-incision cataract surgery, which are typically reserved in some selected cases or occasional settings like cataract camp, were not included in this study. Lastly, given the survey was conducted electronically, most respondents were relatively young in their career, with more than half having less than 10 years of experience, potentially influencing the reported practice patterns.
Value Statement
This nationwide study provides insights into perioperative endophthalmitis prevention practices among Thai ophthalmologists, identifying common practices and variations across subspecialties. It also examines adherence to international guidelines. Our findings reveal certain common practices with limited supporting evidence and potential risks. These findings underscore the need for improved standardization and alignment with evidence-based recommendations. This research serves as a reference for monitoring trends, informing policy, and enhancing patient safety in cataract surgery across Thailand.
Acknowledgment
We sincerely thank all ophthalmologists across Thailand who participated in this survey. We also acknowledge the support of the Royal College of Ophthalmologists of Thailand (RCOPT) for facilitating the survey and ensuring its reach.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, data acquisition, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The research publication received funding support from the Medical Council of Thailand (Police General Dr. Jongjate Aojanepong Foundation). The funding source had no influence on the study design, data collection, analysis, interpretation, report writing, review, or the decision to submit the manuscript for publication.
Disclosure
Mr Nuntachai Surawatsatien reports personal fees from Alcon, Roche, Bayer, Santen, AbbVie, and Kowa, outside the submitted work. The authors have no other conflicts of interest or disclosures to the report for this work.
References
1. Rossi T, Romano MR, Iannetta D, et al. Cataract surgery practice patterns worldwide: a survey. BMJ Open Ophthalmol. 2021;6(1):e000464. doi:10.1136/bmjophth-2020-000464
2. Kessel L, Flesner P, Andresen J, Erngaard D, Tendal B, Hjortdal J. Antibiotic prevention of postcataract endophthalmitis: a systematic review and meta-analysis. Acta Ophthalmol. 2015;93(4):303–317. doi:10.1111/aos.12684
3. ESCRS Endophthalmitis Study Group. Prophylaxis of postoperative endophthalmitis following cataract surgery: results of the ESCRS multicenter study and identification of risk factors. J Cataract Refract Surg. 2007;33(6):978–988. doi:10.1016/j.jcrs.2007.02.032
4. Miller KM, Oetting TA, Tweeten JP, et al. Cataract in the adult eye preferred practice pattern. Ophthalmology. 2022;129(1):P1–p126. doi:10.1016/j.ophtha.2021.10.006
5. Kanchanaranya N, Bhornmata A, Sabsanhor S. Survey of prevention of postoperative endophthalmitis after cataract surgery in Thailand. EyeSEA. 2021;16(1):84–93. doi:10.36281/2021010209
6. The Nation. 2024 Thai online media usage: ‘Day-Part’ key for targeted strategies. Available from: https://www.nationthailand.com/blogs/news/general/40040147.
7. Principles of Preferred Practice in Cataract Surgery. Asia-Pacific Association of Cataract & Refractive Surgeons (APACRS); 2017.
8. Garg P, Khor WB, Roy A, Tan DT. A survey of Asian eye institutions on perioperative antibiotic prophylaxis in cataract surgery. Int Ophthalmol. 2023;43(11):4151–4162. doi:10.1007/s10792-023-02816-w
9. Matossian C, Makari S, Potvin R. Cataract surgery and methods of wound closure: a review. Clin Ophthalmol. 2015;9:921–928. doi:10.2147/opth.S83552
10. Cooper BA, Holekamp NM, Bohigian G, Thompson PA. Case-control study of endophthalmitis after cataract surgery comparing scleral tunnel and clear corneal wounds. Am J Ophthalmol. 2003;136(2):300–305. doi:10.1016/s0002-9394(03)00202-2
11. Bekibele CO, Kehinde AO, Ajayi BG. Effect of face washing with soap and water and cleaning with antiseptics on upper-lid bacteria of surgical eye patients. Can J Ophthalmol. 2010;45(6):637–641. doi:10.3129/i10-052
12. Perry LD, Skaggs C. Preoperative topical antibiotics and lash trimming in cataract surgery. Ophthalmic Surg. 1977;8(5):44–48.
13. Schmitz S, Dick HB, Krummenauer F, Pfeiffer N. Endophthalmitis in cataract surgery: results of a German survey. Ophthalmology. 1999;106(10):1869–1877. doi:10.1016/s0161-6420(99)90395-0
14. Epstein NE. Review: perspective on ocular toxicity of presurgical skin preparations utilizing Chlorhexidine Gluconate/Hibiclens/Chloraprep. Surg Neurol Int. 2021;12:335. doi:10.25259/sni_566_2021
15. Ciulla TA, Starr MB, Masket S. Bacterial endophthalmitis prophylaxis for cataract surgery: an evidence-based update. Ophthalmology. 2002;109(1):13–24. doi:10.1016/s0161-6420(01)00899-5
16. Althiabi S, Aljbreen AJ, Alshutily A, Althwiny FA. Postoperative endophthalmitis after cataract surgery: an update. Cureus. 2022;14(2):e22003. doi:10.7759/cureus.22003
17. Ali T, Jung K, Montan PG. Eyelid skin disinfecting and conjunctival bacteria in cataract surgery. Acta Ophthalmol. 2013;91(2):114–117. doi:10.1111/j.1755-3768.2012.02401.x
18. Thanathanee O, Pulnitiporn R, Anutarapongpan O, Suwan-Apichon O, Bhoomibunchoo C. Effect of eyelid margin cleaning on conjunctival and eyelid bacterial flora before intraocular surgery. Semin Ophthalmol. 2018;33(6):808–812. doi:10.1080/08820538.2018.1504973
19. Shimada H, Nakashizuka H. Cataract surgery by intraoperative surface irrigation with 0.25% povidone-iodine. J Clin Med. 2021;10(16):3611. doi:10.3390/jcm10163611
20. Ta CN, Singh K, Egbert PR, de Kaspar HM. Prospective comparative evaluation of povidone-iodine (10% for 5 minutes versus 5% for 1 minute) as prophylaxis for ophthalmic surgery. J Cataract Refract Surg. 2008;34(1):171–172. doi:10.1016/j.jcrs.2007.08.035
21. Gotttardi W. The influence of the chemical behaviour of iodine on the germicidal action of disinfectant solutions containing iodine. J Hosp Infect. 1985;6(1):1–11. doi:10.1016/S0195-6701(85)80040-2
22. Haripriya A, Baam ZR, Chang DF. Endophthalmitis Prophylaxis for Cataract Surgery. Asia Pac J Ophthalmol. 2017;6(4):324–329. doi:10.22608/apo.2017200
23. Halachmi-Eyal O, Lang Y, Keness Y, Miron D. Preoperative topical moxifloxacin 0.5% and povidone-iodine 5.0% versus povidone-iodine 5.0% alone to reduce bacterial colonization in the conjunctival sac. J Cataract Refract Surg. 2009;35(12):2109–2114. doi:10.1016/j.jcrs.2009.06.038
24. Friling E, Lundström M, Stenevi U, Montan P. Six-year incidence of endophthalmitis after cataract surgery: swedish national study. J Cataract Refract Surg. 2013;39(1):15–21. doi:10.1016/j.jcrs.2012.10.037
25. Chang DF, Rhee DJ. Antibiotic prophylaxis of postoperative endophthalmitis after cataract surgery: results of the 2021 ASCRS member survey. J Cataract Refract Surg. 2022;48(1):3–7. doi:10.1097/j.jcrs.0000000000000757
26. Gore DM, Angunawela RI, Little BC. United Kingdom survey of antibiotic prophylaxis practice after publication of the ESCRS Endophthalmitis Study. J Cataract Refract Surg. 2009;35(4):770–773. doi:10.1016/j.jcrs.2009.01.004
27. Behndig A, Cochener-Lamard B, Güell J, et al. Surgical, antiseptic, and antibiotic practice in cataract surgery: results from the European Observatory in 2013. J Cataract Refract Surg. 2015;41(12):2635–2643. doi:10.1016/j.jcrs.2015.06.031
28. Grosso A, Pertile G, Marchini G, et al. Adherence to European society for cataract and refractive surgery recommendations among Italian cataract surgeons: a survey. Eur J Ophthalmol. 2016;26(5):398–404. doi:10.5301/ejo.5000738
29. Haripriya A, Chang DF. Intracameral antibiotics during cataract surgery: evidence and barriers. Curr Opin Ophthalmol. 2018;29(1):33–39. doi:10.1097/icu.0000000000000445
30. Zhang W, Han H, Feng K, et al. Is it necessary to use tobramycin-dexamethasone eye ointment prophylactically in eyes at the end of intraocular surgery? BMC Ophthalmol. 2020;20(1):208. doi:10.1186/s12886-020-01476-z
31. Maharana PK, Chhablani JK, Das TP, Kumar A, Sharma N. All India Ophthalmological Society members survey results: cataract surgery antibiotic prophylaxis current practice pattern 2017. Indian J Ophthalmol. 2018;66(6):820–824. doi:10.4103/ijo.IJO_1336_17
32. Recchia FM, Busbee BG, Pearlman RB, Carvalho-Recchia CA, Ho AC. Changing trends in the microbiologic aspects of postcataract endophthalmitis. Arch Ophthalmol. 2005;123(3):341–346. doi:10.1001/archopht.123.3.341
33. Han IC, Puri S, Wang J, Sikder S. Impact of surgeon subspecialty training on surgical outcomes in open globe injuries. Clin Ophthalmol. 2015;9:1807–1813. doi:10.2147/opth.S85953
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Use of Methenamine Hippurate in an Ageing Population: National Prescription Trends from Norway (2004–2020)
Juliebø-Jones P, Somani BK, Beisland C
Research and Reports in Urology 2026, 18:596007
Published Date: 21 April 2026