Back to Journals » Clinical Epidemiology » Volume 18
Positive Predictive Values of ICD-10-CM Diagnostic Codes in Identifying Diabetic Macular Edema in Claims Data: A Multi-Institutional Study in Taiwan
Authors Huang YC, Hwang YS, Wu WC, Lai C, Yeung L, Shao SC ![]()
Received 28 October 2025
Accepted for publication 26 February 2026
Published 16 March 2026 Volume 2026:18 577256
DOI https://doi.org/10.2147/CLEP.S577256
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Thomas Ahern
Yao-Chi Huang,1,2 Yih-Shiou Hwang,2,3 Wei-Chi Wu,2,3 Chi‐Chun Lai,2,4 Ling Yeung,1,2 Shih-Chieh Shao5,6
1Department of Ophthalmology, Keelung Chang Gung Memorial Hospital, Keelung, Taiwan; 2College of Medicine, Chang Gung University, Taoyuan, Taiwan; 3Department of Ophthalmology, Chang Gung Memorial Hospital, Linkou, Taiwan; 4Department of Ophthalmology, New Taipei Municipal TuCheng Hospital, New Taipei, Taiwan; 5School of Pharmacy, Institute of Clinical Pharmacy and Pharmaceutical Sciences, College of Medicine, National Cheng Kung University, Tainan, Taiwan; 6Department of Pharmacy, Keelung Chang Gung Memorial Hospital, Keelung, Taiwan
Correspondence: Ling Yeung, Department of Ophthalmology, Keelung Chang Gung Memorial Hospital, No. 222, Maijin Road, Anle District, Keelung, 204, Taiwan, Email [email protected] Shih-Chieh Shao, Department of Pharmacy, Keelung Chang Gung Memorial Hospital, No. 222, Maijin Road, Anle District, Keelung, 204, Taiwan, Email [email protected]
Purpose: To evaluate the accuracy of ICD-10-CM diagnostic codes when identifying diabetic macular edema (DME) in claims data.
Methods and Materials: We analyzed electronic medical records data from four hospitals in Taiwan, and included patients who received first-time ICD-10-CM DME diagnosis codes of E08-13.311, E08-13.321, E08-13.331, E08-13.341 or E08-13.351 during outpatient visits between 2017 and 2022. Two ophthalmologists independently reviewed medical records to confirm the DME diagnosis among a 15% simple random sample of patients assigned the ICD-10-CM DME diagnosis codes. The positive predictive value (PPV) was calculated as the proportion of true DME cases among patients identified by ICD-10-CM DME diagnosis codes. Additionally, we determined the PPVs to identify true DME cases when (1) the ICD-10-CM codes for DME were in the primary diagnosis position only, and (2) when ICD-10-CM DME coding was combined with first-line treatment (intravitreal anti-VEGF drugs covered by Taiwan’s national health insurance program within 3 months following code assignment).
Results: In total, 4,962 patients newly assigned ICD-10-CM codes for DME were identified, of which 745 patients (15%) (mean age: 62.7 years; females: 47.1%) were randomly selected for electronic medical records review. The PPV for the ICD-10-CM codes to identify true DME cases was 26.4% (197/745, 95% CI: 0.23– 0.30). Among the 548 false-positive cases identified by ICD-10-CM DME codes, 516 (94.2%) were tentative diagnoses, 12 (2.2%) involved other retinal diseases, and 20 (3.6%) were remote DME. Among the 402 cases where ICD-10-CM DME diagnostic codes were present only in the primary diagnosis position, the PPV of ICD-10-CM codes for true DME cases remained similar (126/402=31.3%, 95% CI: 0.27– 0.36). However, when coding was combined with intravitreal anti-VEGF treatment within 3 months following ICD-10-CM code assignment (55 cases), the PPV for true DME cases was high (55/55=100%, 95% CI: 0.94– 1.00), and all confirmed cases were center-involved DME.
Conclusion: ICD-10-CM codes alone showed suboptimal accuracy for identifying DME in Taiwan. However, when coding was combined with intravitreal anti-VEGF drug use, they reliably identified center-involved DME in routine care in Taiwan. These findings can inform future claims-based research requiring DME case identification and avoid misclassification bias.
Keywords: diabetic macular edema, positive predictive value, diagnostic codes, ICD-10-CM
Introduction
Diabetic macular edema (DME) is a major complication in patients with diabetes mellitus, leading to blindness in those affected. It has been estimated that 28.61 million people will be affected by 2045.1 Intravitreal anti-vascular endothelial growth factor (anti-VEGF) drugs are recommended as the first-line treatment for DME due to their pronounced effect in mitigating the swelling of the macula and improving visual acuity.2,3 Previous studies based on secondary data sources, including electronic medical records and claims data from health insurance, have reported the clinical characteristics, risk factors, and treatment results of DME.4,5 For example, Lundeen et al analyzed health insurance data in the United States and observed a 1.5-fold increase in the annual prevalence of DME from 2009 to 2018.4 Analyzing Taiwanese claims data, Lee WA et al found that, compared to ranibizumab, aflibercept was associated with a greater risk of adverse renal events in patients with DME.5 Since these studies relied on diagnostic codes to identify patients with DME, the validity of the findings may be subject to misclassification bias if the accuracy of these codes in capturing true DME cases is uncertain.6
To date, only one validation study in the United States has investigated the accuracy of International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) DME diagnosis codes, and it reported a sensitivity of 0.88 and a specificity of 0.96 in identifying DME for a series of ICD-9-CM codes 250.xx and 362.53.7 Although the accuracy of ICD-9-CM codes in identifying DME has previously been established, validation studies of ICD-10-CM codes for this purpose have yet to be conducted. The United States and many other countries transitioned from ICD-9-CM to ICD-10-CM on October 1st, 2015,8 introducing substantial changes in code structure, granularity, and classification logic. Unlike ICD-9-CM systems, ICD-10-CM systems include laterality and more detailed clinical descriptors,9 which may affect how coders assign diagnostic codes in real-world settings.
Given the structural and coding differences between ICD-9-CM and ICD-10-CM systems, the diagnostic accuracy of ICD-10-CM codes cannot be assumed from prior ICD-9-CM validations. As most secondary data sources now use ICD-10-CM systems, validation of their accuracy in identifying true DME cases is essential to ensure study validity. Since no study to date has evaluated the validity of ICD-10-CM codes for DME, this study aimed to assess the accuracy of ICD-10-CM diagnosis codes in identifying true DME cases, using claims data from Taiwan.
Methods
Design and Setting
This retrospective study analyzed electronic medical records data from four regional hospitals (Taipei, Keelung, Linkou and Taoyuan) within the Chang Gung Medical Foundation (CGMF) in Taiwan.10 CGMF represents the largest multi-institutional healthcare system in Taiwan, and its electronic medical records data has provided abundant real-world evidence for research in various medical fields,11–13 and especially in ophthalmology.14–16 This study was approved by the Institutional Review Board of CGMF (IRB No: 202200229B0) and was conducted in accordance with the principles outlined in the Declaration of Helsinki. The requirement for informed consent was waived due to its retrospective design.
Data Sources
In Taiwan, the ICD-10-CM coding system was introduced in 2016.17 This study retrieved claims data reported by the four study hospitals to Taiwan’s National Health Insurance Administration, and included patients newly assigned the ICD-10-CM DME diagnostic codes E08-13.311, E08-13.321, E08-13.331, E08-13.341 or E08-13.351 in outpatient settings between 2017 and 2022.4 The details of ICD-10-CM DME diagnostic codes used in this study were presented in Supplementary Table 1. The study index date was defined as the first assignment date of an ICD-10-CM diagnostic code for DME. We randomly selected 15% of patients from the original cohort using simple random sampling for clinical ascertainment of DME based on electronic medical records. Similar validation steps have been followed by several other published studies, using electronic medical records data from CGMF, to validate diagnostic codes for cerebral venous sinus thrombosis, myocarditis, Guillain-Barré syndrome, anaphylaxis, carbon monoxide poisoning and glaucoma.18–23
Ascertainment of DME
Two ophthalmologists (YCH and LY) independently reviewed the electronic medical records of the cases randomly selected from the original cohort to identify true DME cases based on examination reports (fundus photos, fluorescein angiography (FA), and optical coherence tomography (OCT)), laboratory data (hemoglobin A1c levels), medical history (diabetes), and medication history (use of anti-hyperglycemic drugs). Any discrepancies in judgment between the reviewers were resolved through discussion. According to the International Council of Ophthalmology Guidelines for Diabetic Eye Care,24 DME was traditionally defined as retinal thickening proximal to the fovea. Due to advances in OCT, however, DME is now more commonly classified as center-involved or non-center-involved DME, respectively defined as retinal thickening in the macula with or without involvement of the central subfield zone (1 mm in diameter), Center-involved DME is defined if the retinal thickness ≥ 300 µm assessed by OCT. Overall, the kappa statistics were 0.80, indicating substantial agreement and consistent adjudication of DME diagnoses between two ophthalmologists.
Data Analyses
We calculated the positive predictive value (PPV) of the ICD-10-DME codes as the proportion of diagnostically ascertained DME cases among patients identified by ICD-10-CM DME diagnosis codes. We also determined the PPVs to identify true DME cases for (1) cases with ICD-10-CM coding for DME in the primary diagnosis position only, and (2) combinations of ICD-10-CM coding for DME with first-line treatment (ie., intravitreal anti-VEGF drugs covered by Taiwan’s National Health Insurance (NHI) within 3 months of diagnosis). We used the Clopper–Pearson exact method to calculate 95% confidence intervals (CI) for the PPVs. Data analyses were performed using SPSS (version 25.0; IBM Corp., Armonk, NY, USA).
Results
We identified a total of 4,962 patients newly assigned ICD-10-CM diagnosis codes for DME from 4 study hospitals between 2017 and 2022, of which 745 patients (15% of the total) were randomly sampled for detailed review of their electronic medical records (Figure 1). Within this sample cohort, 197 cases (26.4%) were confirmed as true-positive DME cases, while 548 cases (73.6%) were classified as false-positives. Among the false-positive DME cases, 94.2% (516/548) were considered tentative diagnoses, 2.2% (12/548) were actually other retinal diseases, and 3.6% (20/548) were remote DME.
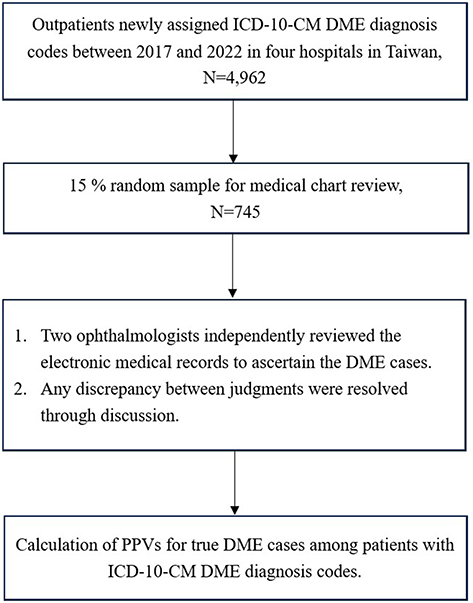 |
Figure 1 Validation study flow chart. Abbreviations: ICD-10-CM, International Classification of Diseases, 10th Revision; DME, diabetic macular edema. |
PPVs of ICD-10-CM DME Diagnostic Codes
The demographics and general clinical characteristics of the 197 true DME cases are summarized in Table 1. The mean (SD) age was 61.2 (11.5) years, and 82 (41.6%) of the true DME patients were female. Among the 197 true DME cases, 196 (99.5%) were diagnosed with type 2 diabetes, with one case of type 1 diabetes. The detailed PPVs for each ICD-10-CM DME code are presented in Table 2. Using the ICD-10-CM codes for DME in any of the three positions of the diagnosis yielded a PPV of 26.4% (95% CI: 0.23–0.30), Among the 402 cases where all ICD-10-CM DME diagnostic codes were present only in the primary diagnosis position, the PPV of ICD-10-CM codes for true DME cases remained similar (31.3% or 126/402, 95% CI: 0.27–0.36). Of the various coding patterns, the ICD-10-CM DME code E08–E13.311 (Unspecified diabetic retinopathy with macular edema) in any of the three positions of the diagnosis accounted for 108 true-positive cases, yielding a PPV of 21.6% (95% CI: 0.18–0.25). When the analysis was restricted to the primary diagnosis position only, the PPV improved slightly to 24.0% (95% CI: 0.19–0.30), but at the expense of a lower number of true DME patients identified.
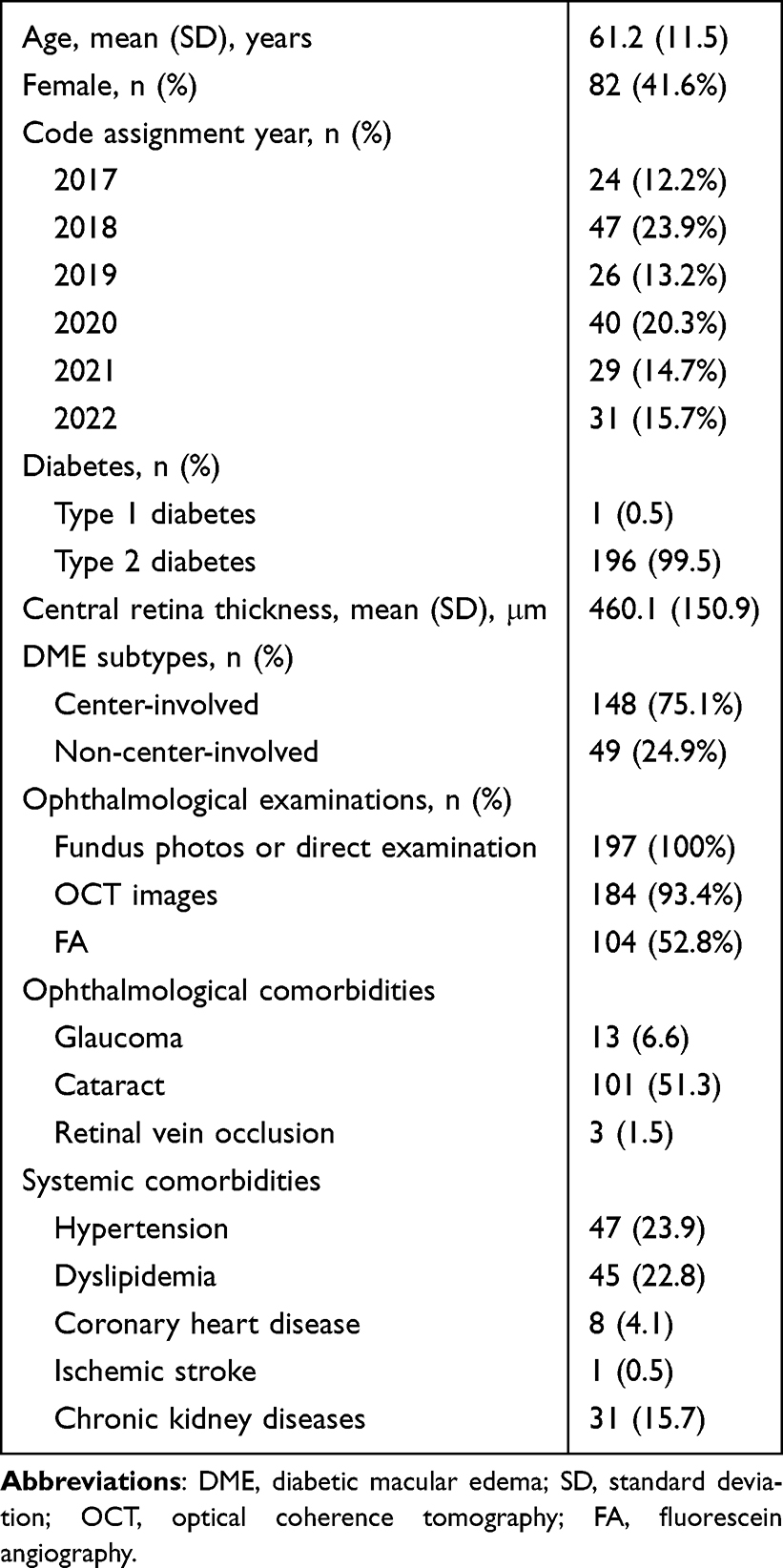 |
Table 1 Clinical Characteristics of 197 Ascertained DME Cases |
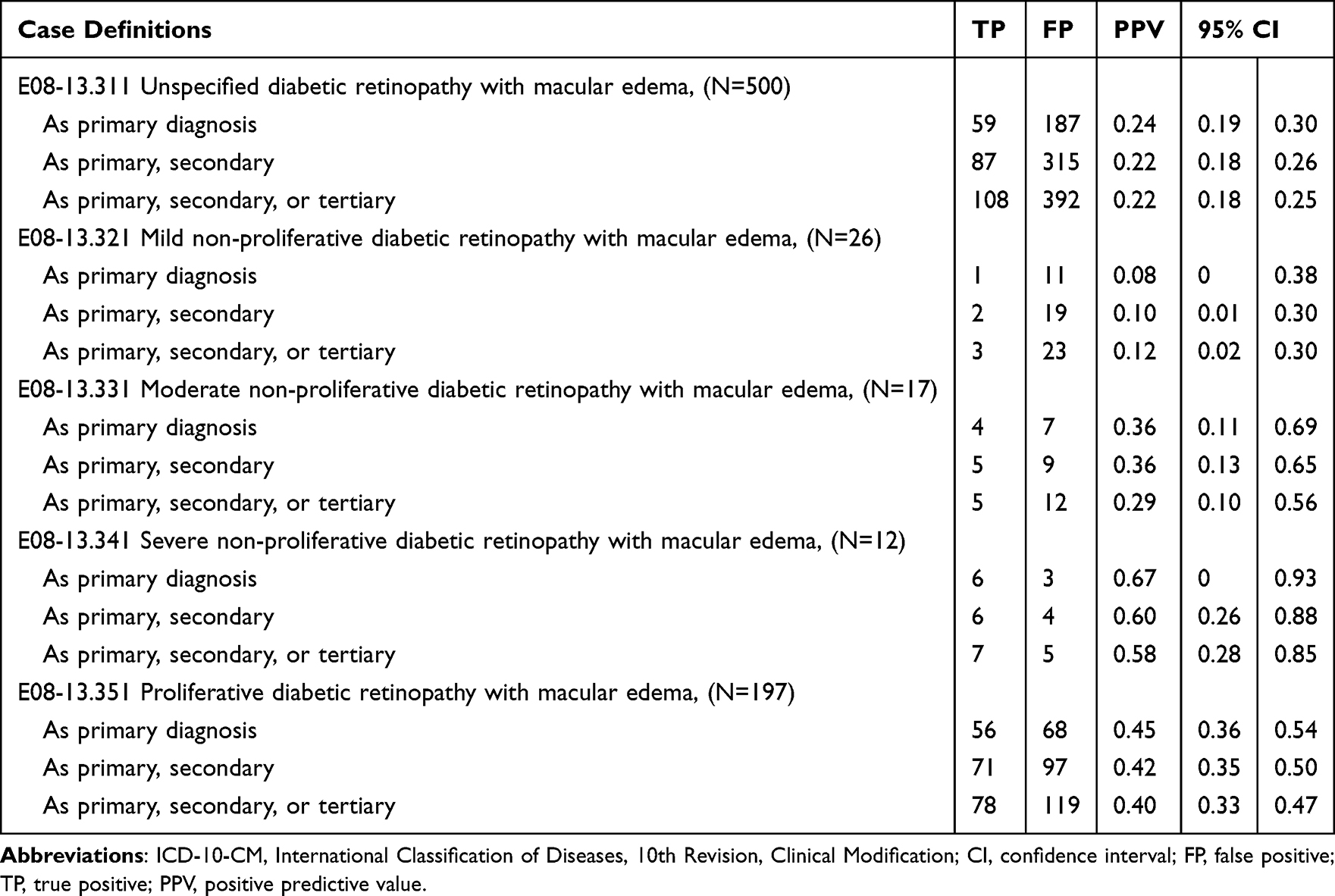 |
Table 2 Accuracy of ICD-10-CM Codes to Identify DME |
PPVs of ICD-10-CM DME Diagnostic Codes Combined with Intravitreal Anti-VEGF Drug Uses
However, when ICD-10-CM DME coding was combined with NHI-covered intravitreal anti-VEGF drugs administered within 3 months, all 55 identified patients were confirmed as true-positive cases of DME, all with center-involved DME, resulting in a high PPV (100%, 95% CI: 0.94–1.00) (Table 3).
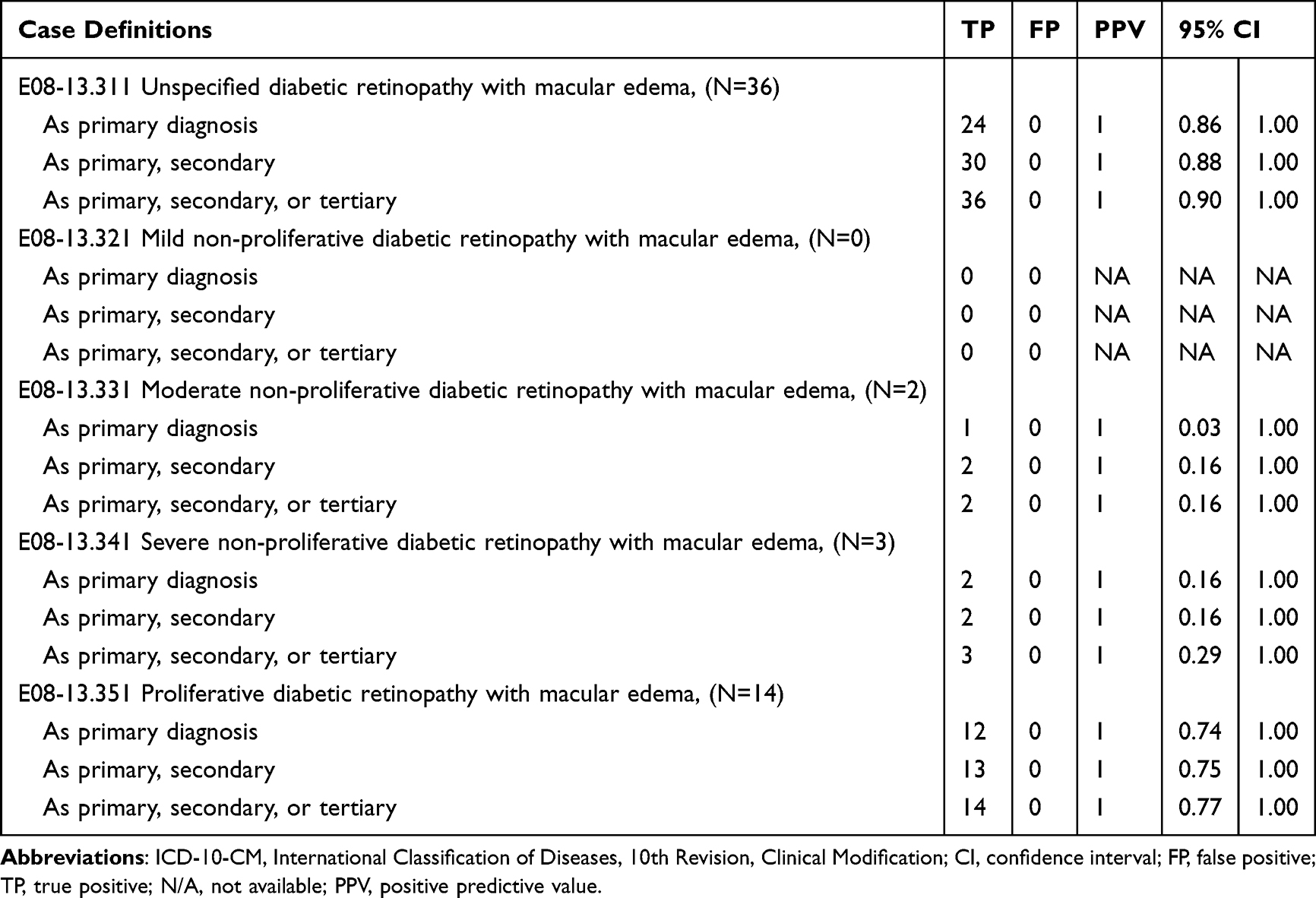 |
Table 3 Accuracy of ICD-10-CM Codes Plus Intravitreal Anti-VEGF Drug Use to Identify DME |
Discussion
In this validation study using electronic medical records from four hospitals in Taiwan, the presence of ICD-10-CM codes for DME in any position of the outpatient diagnosis carried a PPV of 26.4% (95% CI: 0.23-0.30). The PPV did not significantly improve when the code position was restricted to the primary diagnosis column. However, combining ICD-10-CM diagnosis codes with the use of intravitreal anti-VEGF drugs for DME achieved a perfect PPV, with all identified cases classified as center-involved DME.
Comparison with the Literature
In the present study, the PPV of ICD-10-CM codes for identifying DME was substantially lower than that reported by Bearelly et al for ICD-9-CM codes in U.S. claims data (26.4% vs. 92.1%).7 Several factors may explain this discrepancy, including differences in coding practices and sample selection. First, our review of electronic medical records revealed that a large proportion of the false positives consisted of tentative diagnoses (94.2%, or 516/548). This may reflect a common practice in Taiwan, where ophthalmologists provisionally assign DME codes to patients with diabetic retinopathy who present symptoms such as blurred vision, metamorphopsia, or central scotoma. To improve coding accuracy, ophthalmologists could consider reserving ICD-10 CM DME diagnostic codes for cases with objective evidence of macular edema, preferably OCT-confirmed (and/or FA-supported when indicated), and use alternative codes (eg., diabetic retinopathy without macular edema or symptom-only codes) when DME remains only a tentative diagnosis pending imaging confirmation. Second, Bearelly et al used a convenience sample drawn from ophthalmologists who voluntarily submitted records, with only 22 of 43 agreeing to participate, potentially introducing selection bias due to better documentation practices. In contrast, our study was based on a random sample of patients with ICD-10-CM DME codes across multiple hospital levels, reducing the potential for selection bias related to physician participation. These findings underscore the critical need to validate the accuracy of ICD-10-CM codes before using secondary databases for DME research.
Implications for Future Researchers
Our results indicated that only about one out of every four patients assigned an ICD-10-CM diagnosis code for DME was actually an ascertainable DME case. Since the accuracy of ICD-10-CM codes to define DME is therefore suboptimal, future researchers relying on these codes face significant risks of misclassification. For example, when defining study populations, the use of inaccurate ICD-10-CM codes may lead to the inclusion of patients who do not truly have the disease (false positives) or the exclusion of true cases (false negatives), leading to selection bias and reduced generalizability. When defining covariates, misclassified comorbidities can result in inadequate confounding adjustment. When defining outcomes, low ICD-10-CM coding accuracy may lead to misclassification of clinical events, biasing effect estimates and threatening internal validity. Hence, it is imperative that researchers use validated ICD-10-CM coding algorithms with high PPVs, whereby we suggest combining diagnostic codes with the use of related medications, such as combining ICD-10-CM DME diagnosis codes with intravitreal anti-VEGF drugs to improve the accuracy of DME identification using Taiwan’s NHI data or other secondary healthcare data sources.
Strengths and Limitations
A major strength of this study is its use of a random sample from four hospitals of varying levels in Taiwan, enhancing the representativeness of the patient population. Among the 745 patients examined, 197 true DME cases were identified, all of whom underwent ophthalmological examinations (fundus photography or OCT). Moreover, all 55 patients who received NHI-covered intravitreal anti-VEGF drugs had an ascertained diagnosis of center-involved DME, consistent with current clinical guidelines, thereby supporting the internal validity of our study.
Some limitations of our study must also be acknowledged. First, because the target population was first identified from the electronic medical records database in our validation study step, we were unable to evaluate the sensitivity, specificity, or negative predictive value of the ICD-10-CM codes for DME. Second, the generalizability of our findings to other countries should be approached with caution, as Taiwan operates under a single-payer NHI system. For instance, intravitreal anti-VEGF drugs for DME are reimbursed under specific criteria in Taiwan, including that best-corrected visual acuity must be between 0.05 and 0.5, with central retinal thickness ≥ 300 μm. Moreover, HbA1c level within the three months prior to initiation of intravitreal anti-VEGF drugs must be under 10%. This HbA1c requirement may lead to the exclusion of patients with poorly controlled diabetes and, consequently, may disproportionately exclude those with more severe diabetic retinopathy. However, as these criteria largely reflect the inclusion criteria of Phase 3 clinical trials for these drugs,25–27 variability in the prescribing patterns of intravitreal anti-VEGF drugs for DME among ophthalmologists worldwide is likely to be minimal.
Conclusion
The accuracy of ICD-10-CM codes alone for identifying DME was found to be suboptimal in Taiwan. However, when combined with records of intravitreal anti-VEGF drug use, the ICD-10-CM codes reliably identified DME cases, particularly those with center-involved DME, in routine clinical practice in Taiwan. These findings provide a valuable reference for future claims-based research requiring the identification of DME cases in Taiwan.
Data Sharing Statement
Data sharing is not applicable because the analyses were performed via remote access on a secure statistical server at Chang Gung Medical Foundation, Taiwan, to ensure data privacy and security. Further enquiries may be directed to Dr. Ling Yeung ([email protected]).
Statement of Ethics
All of the included patient data used in the study were handled in strict accordance with applicable data protection and privacy regulations. Access to the data was restricted to authorized investigators only.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported in part by grants from Keelung Chang Gung Memorial Hospital, Keelung, Taiwan (CMRPG2P0152).
Disclosure
The authors report no conflicts of interest with regard to this work.
References
1. Teo ZL, Tham YC, Yu M, et al. Global prevalence of diabetic retinopathy and projection of burden through 2045: systematic review and meta-analysis. Ophthalmology. 2021;128(11):1580–8. doi:10.1016/j.ophtha.2021.04.027
2. Boyer DS, Hopkins JJ, Sorof J, Ehrlich JS. Anti-vascular endothelial growth factor therapy for diabetic macular edema. Ther Adv Endocrinol Metab. 2013;4(6):151–169. doi:10.1177/2042018813512360
3. Mitchell P, Wong TY, Diabetic Macular Edema Treatment Guideline Working Group. Management paradigms for diabetic macular edema. Am J Ophthalmol. 2014;157(3):505–13.e138. doi:10.1016/j.ajo.2013.11.012
4. Lundeen EA, Andes LJ, Rein DB, et al. Trends in prevalence and treatment of diabetic macular edema and vision-threatening diabetic retinopathy among medicare part B fee-for-service beneficiaries. JAMA Ophthalmol. 2022;140(4):345–353. doi:10.1001/jamaophthalmol.2022.0052
5. Lee WA, Shao SC, Hsieh MH, Liao TC, Lin SJ, Lai EC. Adverse renal events between ranibizumab and aflibercept in patients with diabetic macular oedema in Taiwan: a comparative cohort study. Br J Ophthalmol. 2025;109(10):1171–1178. doi:10.1136/bjo-2024-325509
6. Ehrenstein V, Petersen I, Smeeth L, et al. Helping everyone do better: a call for validation studies of routinely recorded health data. Clin Epidemiol. 2016;8:49–51. doi:10.2147/CLEP.S104448
7. Bearelly S, Mruthyunjaya P, Tzeng JP, et al. Identification of patients with diabetic macular edema from claims data: a validation study. Arch Ophthalmol. 2008;126(7):986–989. doi:10.1001/archopht.126.7.986
8. Hernandez-Ibarburu G, Perez-Rey D, Alonso-Oset E, et al. ICD-10-CM extension with ICD-9 diagnosis codes to support integrated access to clinical legacy data. Int J Med Inform. 2019;129:189–197. doi:10.1016/j.ijmedinf.2019.06.010
9. Steindel SJ. International classification of diseases, 10th edition, clinical modification and procedure coding system: descriptive overview of the next generation HIPAA code sets. J Am Med Inform Assoc. 2010;17(3):274–282. doi:10.1136/jamia.2009.001230
10. Shao SC, Chan YY, Kao Yang YH, et al. The Chang Gung Research Database-A multi-institutional electronic medical records database for real-world epidemiological studies in Taiwan. Pharmacoepidemiol Drug Saf. 2019;28(5):593–600. doi:10.1002/pds.4713
11. Tsai DH, Chuang AT, Liu KH, Shao SC, Lai EC. Sodium-glucose cotransporter 2 (SGLT2) inhibitors and risk of chronic kidney disease-mineral and bone disorders in patients with type 2 diabetes mellitus and stage 1-3 chronic kidney disease. CMAJ. 2025;197(7):E178–E189. doi:10.1503/cmaj.240922
12. Hu JC, Shao SC, Tsai DH, Chuang AT, Liu KH, Lai EC. Use of SGLT2 inhibitors vs GLP-1 RAs and anemia in patients with diabetes and CKD. JAMA Network Open. 2024;7(3):e240946. doi:10.1001/jamanetworkopen.2024.0946
13. Shao SC, Chang KC, Lin SJ, et al. Differences in outcomes of hospitalizations for heart failure after SGLT2 inhibitor treatment: effect modification by atherosclerotic cardiovascular disease. Cardiovasc Diabetol. 2021;20(1):213. doi:10.1186/s12933-021-01406-3
14. Su YC, Hung JH, Chang KC, et al. Comparison of Sodium-Glucose cotransporter 2 inhibitors vs glucagonlike Peptide-1 receptor agonists and incidence of dry eye disease in patients with type 2 diabetes in Taiwan. JAMA Network Open. 2022;5(9):e2232584. doi:10.1001/jamanetworkopen.2022.32584
15. Shao SC, Su YC, Lai EC, et al. Association between sodium glucose co-transporter 2 inhibitors and incident glaucoma in patients with type 2 diabetes: a multi-institutional cohort study in Taiwan. Diabetes Metab. 2022;48(1):101318. doi:10.1016/j.diabet.2022.101318
16. Su YC, Shao SC, Lai EC, et al. Risk of diabetic macular oedema with sodium-glucose cotransporter-2 inhibitors in type 2 diabetes patients: a multi-institutional cohort study in Taiwan. Diabetes Obes Metab. 2021;23(9):2067–2076. doi:10.1111/dom.14445
17. Hsieh CY, Shao SC, Sung SF, et al. Taiwan’s National Health Insurance Research Database (NHIRD): in the era of artificial intelligence, causal inference, and data security. Clin Epidemiol. 2025;17:967–981. doi:10.2147/CLEP.S553894
18. Liao SC, Shao SC, Lai EC, Lin SJ, Huang WI, Hsieh CY. Positive predictive value of ICD-10 codes for cerebral venous sinus thrombosis in taiwan’s national health insurance claims database. Clin Epidemiol. 2022;14:1–7. doi:10.2147/CLEP.S335517
19. Wu LY, Shao SC, Liao SC. Positive predictive value of ICD-10-CM codes for myocarditis in claims data: a multi-institutional study in Taiwan. Clin Epidemiol. 2023;15:459–468. doi:10.2147/CLEP.S405660
20. Chang C, Liao SC, Shao SC. Positive predictive values of anaphylaxis diagnosis in claims data: a multi-institutional study in Taiwan. J Med Syst. 2023;47(1):97. doi:10.1007/s10916-023-01989-2
21. Chiang MY, Shao SC, Liao SC. Validation of diagnostic codes to identify carbon monoxide poisoning in taiwan’s claims data. Front Pharmacol. 2022;13:882632. doi:10.3389/fphar.2022.882632
22. Hsieh CY, Chen PT, Shao SC, Lin SJ, Liao SC, Lai EC. Validating ICD-10 diagnosis codes for guillain-barré syndrome in Taiwan’s national health insurance claims database. Clin Epidemiol. 2024;16:733–742. doi:10.2147/CLEP.S485953
23. Lu PT, Tsai TH, Lai CC, Chuang LH, Shao SC. Validation of diagnostic codes to identify glaucoma in taiwan’s claims data: a multi-institutional study. Clin Epidemiol. 2024;16:227–234. doi:10.2147/CLEP.S443872
24. Wong TY, Sun J, Kawasaki R, et al. Guidelines on diabetic eye care: the international council of ophthalmology recommendations for screening, follow-up, referral, and treatment based on resource settings. Ophthalmology. 2018;125(10):1608–1622. doi:10.1016/j.ophtha.2018.04.007
25. Heier JS, Korobelnik JF, Brown DM, et al. Intravitreal aflibercept for diabetic macular edema: 148-week results from the vista and VIVID studies. Ophthalmology. 2016;123(11):2376–2385. doi:10.1016/j.ophtha.2016.07.032
26. Nguyen QD, Brown DM, Marcus DM, et al. Ranibizumab for diabetic macular edema: results from 2 Phase III randomized trials: RISE and RIDE. Ophthalmology. 2012;119(4):789–801. doi:10.1016/j.ophtha.2011.12.039
27. Wong TY, Haskova Z, Asik K, et al. Faricimab treat-and-extend for diabetic macular edema: two-year results from the randomized phase 3 YOSEMITE and RHINE trials. Ophthalmology. 2024;131(6):708–723. doi:10.1016/j.ophtha.2023.12.026
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.