Back to Journals » Clinical Epidemiology » Volume 12
Positive Predictive Value of Benign Prostatic Hyperplasia and Acute Urinary Retention in the Danish National Patient Registry: A Validation Study
Authors Bengtsen MB ![]() , Heide-Jørgensen U
, Heide-Jørgensen U ![]() , Blichert-Refsgaard LS, Hjelholt TJ
, Blichert-Refsgaard LS, Hjelholt TJ ![]() , Borre M, Nørgaard M
, Borre M, Nørgaard M ![]()
Received 24 August 2020
Accepted for publication 22 October 2020
Published 16 November 2020 Volume 2020:12 Pages 1281—1285
DOI https://doi.org/10.2147/CLEP.S278554
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Irene Petersen
Maria Bisgaard Bengtsen,1 Uffe Heide-Jørgensen,1 Linea Sandfeld Blichert-Refsgaard,2 Thomas Johannesson Hjelholt,1 Michael Borre,2 Mette Nørgaard1
1Department of Clinical Epidemiology, Aarhus University Hospital, Aarhus N, Denmark; 2Department of Urology, Aarhus University Hospital, Aarhus N, Denmark
Correspondence: Maria Bisgaard Bengtsen
Department of Clinical Epidemiology, Aarhus University Hospital, Olof Palmes Allé 43-45, Aarhus N, Denmark
Tel +45 87155872
Fax +45 87167215
Email [email protected]
Background and Aim: Benign prostatic hyperplasia comprises a significant burden to ageing men due to frequently associated lower urinary tract symptoms and the risk of developing serious complications, such as acute urinary retention. Healthcare databases are a valuable source of epidemiological research; however, continuous validation of definitions is imperative. We examined the positive predictive values of International Classification of Diseases, 10th Revision (ICD-10), diagnostic coding for benign prostatic hyperplasia and acute urinary retention in men in the Danish National Patient Registry.
Methods: We investigated a random sample of 100 men diagnosed with benign prostatic hyperplasia and 100 men diagnosed with acute urinary retention between 2011 and 2017 in the Central Denmark Region. Using medical record review as reference standard, we estimated the positive predictive value with corresponding 95% confidence intervals (CI) overall and stratified by age, type of hospital (university hospital vs regional hospital), type of hospital contact (inpatient, outpatient or emergency room), calendar year group (2011– 2013, 2014– 2017), and department (department of urology, geriatrics, endocrinology or emergency room).
Results: Medical records were available for all 200 sampled patients. We found an overall positive predictive value (PPV) of 95% (95% CI: 89– 98%) for benign prostatic hyperplasia and 98% (95% CI: 93– 99%) for acute urinary retention. The PPVs were consistent across age, type of hospital, type of hospital contact, calendar year group, and department.
Conclusion: The PPVs of ICD-10 codes for benign prostatic hyperplasia and acute urinary retention recorded in the Danish National Patient Registry are high.
Keywords: epidemiology, benign prostatic hyperplasia, acute urinary retention, validity
Introduction
Benign prostatic hyperplasia (BPH) is common in the aging male population, affecting more than 50% of men above 60 years. It is an important cause of lower urinary tract symptoms (LUTS), and 15–25% of men aged 50–64 years report LUTS to a degree that has a substantial negative impact on their quality of life.1–3 Acute urinary retention (AUR) is a severe complication to BPH, characterized by a sudden, painful inability to void urine.4 Before the advent of medical therapy for BPH in the mid-1990’s, AUR was an absolute indication for BPH surgery, and today many men will still undergo surgery after an episode of AUR.5 A study from the UK, demonstrated that mortality in men hospitalized with AUR was 2–3 times higher than expected compared with the general population.6 The reason for this high mortality remains largely unknown. Previous population-based studies on incidence, risk factors and prognosis of BPH and AUR are sparse, despite an imperative need for more in-depth knowledge on these diagnoses. National hospital administrative healthcare registries are a potential valuable source of information on BPH and AUR. Many administrative healthcare registries are based on discharge diagnoses coded according to the International Classification of diseases, Tenth revision (ICD-10). The Danish National Patient Registry (DNPR) contains data on all hospital inpatient admissions since 1977 and emergency room and outpatient clinics since 1995.7 Since 1994, diagnoses in the DNPR are classified according to the ICD-10. However, the validity of ICD-10 diagnostic coding of BPH and AUR has not previously been assessed. We therefore investigated the positive predictive values (PPVs) of BPH and AUR in the DNPR.
Materials and Methods
Setting
Denmark is divided into five regions, each representative of the Danish population regarding basic sociodemographic characteristics and use of healthcare and medications.8 Each region typically has one major urologic department at a university hospital and one or several smaller urologic departments at regional hospitals. We conducted this study in the Central Denmark Region with a source population of 1.3 million residents. In the Central Denmark Region, urologic departments are present at Aarhus University Hospital and Regional Hospital Unit West Jutland. The Danish Healthcare Service provides free access to medical care for all Danish residents, including treatment at general practitioners, inpatient, outpatient and emergency room hospital visits, and reimbursement for prescription drugs.9 Data in the DNPR are prospectively collected and registered by the treating physician.7 Data from general practitioners are not included in the DNPR.
Study Population
From the DNPR, we identified all men above 50 years, diagnosed with BPH (ICD-10 code N40) and AUR (ICD-10 code R33) during 2011–2017 at the two hospitals in the Central Denmark Region with urologic departments. Given the homogeneity of the Danish healthcare system, we considered these hospitals to be representative of hospitals of similar size in other Danish regions.8 From departments of urology, acute medicine/emergency room, geriatrics, and endocrinology, we randomly sampled 100 patients diagnosed with BPH and 100 patients diagnosed with AUR. We included these departments because they were the five departments in which patients with BPH and AUR were most frequently diagnosed, in total covering ~90% of all diagnoses at the investigated hospitals.
Medical Record Review
Medical record review was considered reference standard. Three physicians (MBB, LBR and TJH) performed medical record review by entering information from medical records into a standardized form specially developed for the purpose. Each review was initiated by confirming the civil registration number and date of diagnosis. For each patient, we evaluated if the diagnosis recorded in the DNPR could be confirmed by medical record review. Presence of BPH was considered confirmed when a) patients had a history of LUTS or received BPH medication and no other causes of LUTS were specified in the medical record or b) BPH was confirmed by biopsy. We defined acute urinary retention as the acute inability to void urine. In cases of doubt, consultation with another physician (MBB or MN) was performed to reach consensus.
All data were entered into REDCap (Research Electronic Data Capture) tools hosted at Aarhus University.
Statistical Analysis
From the DNPR, we retrieved data on age, type of hospital contact (inpatient, outpatient or emergency room), and calendar year group (2011–2013 vs 2014–2017). We calculated the PPVs as the proportion of diagnoses in the DNPR confirmed by medical record review. Confidence intervals were computed using Wilson Score method.10 For each diagnosis, we computed PPVs stratified by age groups (50–69, 70–79, and 80+ years), type of hospital, type of hospital contact, calendar year group (2011–2013 and 2014–2017), and department (department of urology, geriatrics, endocrinology or emergency room).
Analyses were performed in R version 3.6.1 (R Foundation for Statistical Computing).
Results
Figure 1 shows a flowchart of the sampling process. From the DNPR, we identified 44,935 patients diagnosed with BPH and 41,868 patients diagnosed with AUR during 2011–2017, of which 3557 and 3232 were diagnosed at the investigated hospitals and departments. Medical records were available for all sampled patients.
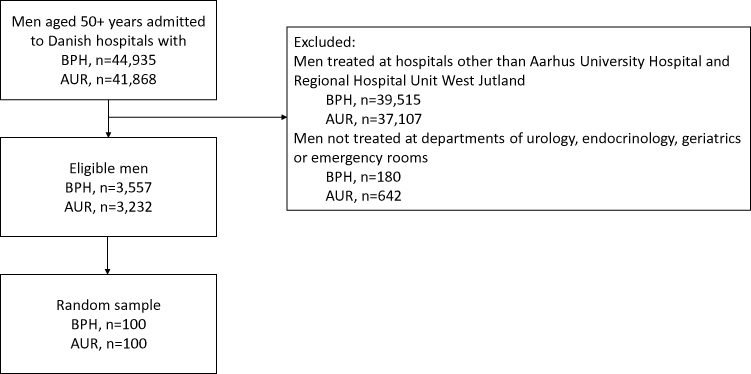 |
Figure 1 Flowchart of study population selection. |
The median age was 71 years (interquartile range (IQR): 65–79) for BPH patients and 78 years (IQR: 70–84) for AUR patients. Outpatient diagnoses comprised 92% of BPH diagnoses and 59% of AUR diagnoses. Overall, medical record review confirmed 95 BPH cases, resulting in a PPV of 95% (95% CI: 89–98%). The overall PPV for AUR was 98% (95% CI: 93–99%). The PPVs stratified by age, type of hospital, type of hospital contact, calendar year group and department were consistent with the main results (Figure 2).
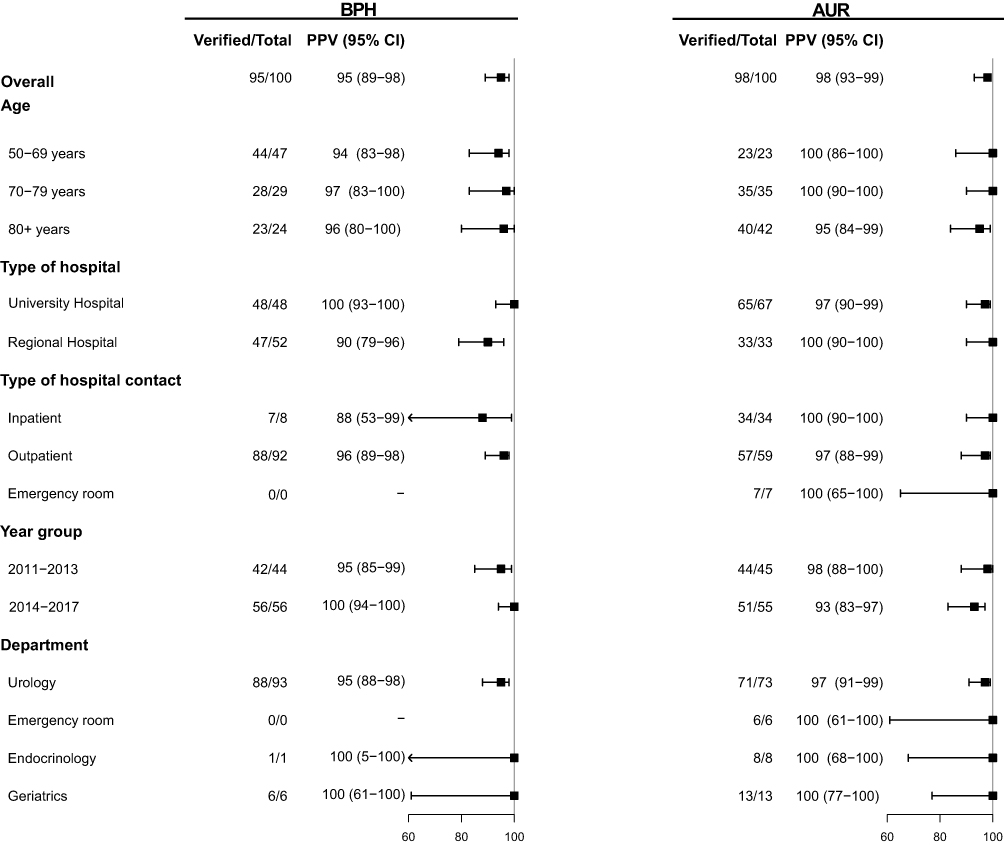 |
Figure 2 Positive predictive value of benign prostatic hyperplasia (BPH) and acute urinary retention (AUR) in the Danish National Patient Registry. |
Discussion
This study demonstrated high PPVs of AUR and BPH in the DNPR during 2011–2017, suggesting that the DNPR is a valid source for epidemiologic research of BPH and AUR.
Although administrative healthcare databases, such as the DNPR, are a valuable tool in epidemiological research, continuous validation is essential.7 In line with our results, previous studies validating other benign urogenital diseases in the DNPR, found PPV’s ranging from 77% to 100%.7 Our study is the first to validate BPH and AUR diagnoses recorded in the DNPR. A previous study reported a sensitivity and specificity of 95% and 91% of ICD-9 coding of AUR, based on emergency room diagnoses at one hospital in the US.11 To the best of our knowledge, no previous data exist of validity of BPH in healthcare administrative databases.
Our study has limitations. Data collection for this study was only made in one out of five Danish regions. However, due to the homogeneity of the country, our results are most likely generalizable to other Danish hospitals and regions.8 Our results may, however, not be applicable for other countries or other healthcare systems. The DNPR was established in 1977 and contains diagnoses classified according to ICD-8 until the end of 1993, and the 10th revision thereafter.7 Since we validated ICD-10 codes in the period 2011 to 2017, we cannot necessarily extrapolate our results to previous periods. Still, we found no substantial changes in the PPV across calendar year groups, suggesting that the reported validity is also applicable to other periods.
Although we were unable to confirm the BPH diagnosis through medical record review in five patients, this does not necessarily mean that these patients did not actually have BPH. We experienced that medical records of patients suspected of prostate cancer focused on presence or absence of cancer rather than BPH, and we could not confirm the BPH diagnosis unless it was specifically mentioned in the medical record by the treating physician. Thus, the PPV of BPH might have been slightly higher than reported.
Fifty-nine percent of patients with AUR were diagnosed at outpatient clinics, which correlates well with the structure of the Danish Health Care system. In Denmark, general practitioners serve as gatekeepers for all patients going into the hospital.12 Except for cases of 911-emergency, patients need a hospital referral from a general practitioner at all hours of the day. According to current guidelines, general practitioners should perform catheterization and then refer patients for further work-up at hospital, eg, subacute referral for outpatient clinic.13 Only in cases with failure of catheterization, risk of post-obstruction polyuria or if another underlying condition that requires acute hospitalization is suspected, patients will be referred directly to hospital.13
We used the PPV as a measure of validity. However, by design, we were unable to assess other measures of data quality, including sensitivity, specificity and negative predictive values because we lacked an independent sample of true BPH/AUR cases as well as a sample of non-cases. The importance of these different measures of data quality depends on the specific study aim and design. Thus, while a high PPV is important when studying prognosis, it cannot stand alone in studies of incidence.
Conclusion
The validity of BPH and AUR in the DNPR is high, confirming the potential of these diagnoses in epidemiologic research.
Ethics Approval
This study was approved by The Danish Data Protection Agency (journal number: 2016-051-000001), the Danish Patient Safety Authority (reference number: 3-3013-2925/1) and by the Head of each involved departments. In accordance with Danish law governing analysis of registry data, no Ethics Committee approval was required.
Acknowledgments
The authors wish to thank the head of each of the involved departments for their cooperation and Henriette Kristoffersen for practical assistance.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
Dr Thomas Johannesson Hjelholt reports grants from Novo Nordisk Foundation during the conduct of the study. The authors report no other potential conflicts of interest for this work.
References
1. Nørby B, Nordling J, Mortensen S. Lower urinary tract symptoms in the Danish Population: a population-based study of symptom prevalence, health-care seeking behavior and prevalence of treatment in elderly males and females. Eur Urol. 2005;47(6):817–823. doi:10.1016/j.eururo.2005.01.011
2. Girman CJ, Jacobsen SJ, Tsukamoto T, et al. Health-related quality of life associated with lower urinary tract symptoms in four countries. Urology. 1998;51(3):428–436. doi:10.1016/S0090-4295(97)00717-6
3. Batista-Miranda JE, Molinuevo B, Pardo Y. Impact of lower urinary tract symptoms on quality of life using functional assessment cancer therapy scale. Urology. 2007;69(2):285–288. doi:10.1016/j.urology.2006.09.054
4. Emberton M, Cornel EB, Bassi PF, Fourcade RO, Gómez JMF, Castro R. Benign prostatic hyperplasia as a progressive disease: a guide to the risk factors and options for medical management. Int J Clin Pract. 2008;62(7):1076–1086. doi:10.1111/j.1742-1241.2008.01785.x
5. Roehrborn CG. Acute urinary retention: risks and management. Rev Urol. 2005;7(Suppl4):S31–S41.
6. Armitage JN, Sibanda N, Cathcart PJ, Emberton M, van der Meulen JHP. Mortality in men admitted to hospital with acute urinary retention: database analysis. BMJ. 2007;335(7631):1199.
7. Schmidt M, Schmidt SAJ, Sandegaard JL, Ehrenstein V, Pedersen L, Sorensen HT. The Danish National Patient Registry: a review of content, data quality, and research potential. Clin Epidemiol. 2015;7:449–490. doi:10.2147/clep.S91125
8. Henriksen DP, Rasmussen L, Hansen MR, Hallas J, Pottegård A. Comparison of the Five Danish regions regarding demographic characteristics, healthcare utilization, and medication use—a descriptive cross-sectional study. Dalal K, ed. PLoS One. 2015;10(10):e0140197. doi:10.1371/journal.pone.0140197
9. Frank L. When an entire country is a cohort. Science. 2000;287(5462):2398–2399. doi:10.1126/science.287.5462.2398
10. Wilson EB. Probable inference, the law of succession, and statistical inference. J Am Stat Assoc. 1927;22(158):209–212. doi:10.1080/01621459.1927.10502953
11. Vouri SM, Strope S, Olsen M. Validating acute urinary retention using diagnosis and procedure codes. J Clin Transl Sci. 2017;1(S1):80. doi:10.1017/cts.2017.282
12. Healthcare Denmark, Ministry of Health. Healthcare in Denmark; 2016.
13. Danish College of General Practitioners. Klinisk Vejledning for Almen Praksis Udredning Og Behandling Af Nedre Urinvejssymptomer Hos Mænd Og Kvinder; 2009. [Clinical guidelines for general practitioners. Diagnostic work-up and treatment of lower urinary tract symptoms in men and women, 2009].
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.