Back to Journals » Patient Preference and Adherence » Volume 17
Portrait for Type 2 Diabetes with Goal-Achieved HbA1c Using Digital Diabetes Care Model: A Real-World 12-Month Study from China
Authors Li M, Zhang B, Guo L, Zhang Y, Du X, Wang B, Xu Z, Sun N, Chen R, Han W, Chen L ![]() , Song Z
, Song Z
Received 6 April 2023
Accepted for publication 22 August 2023
Published 7 September 2023 Volume 2023:17 Pages 2227—2235
DOI https://doi.org/10.2147/PPA.S416121
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jongwha Chang
Mingzhen Li,1 Bing Zhang,2 Lichuan Guo,2 Yuan Zhang,2 Xiaoyan Du,3 Bingyi Wang,3 Zheng Xu,4 Ning Sun,4 Ruibin Chen,4 Wanwen Han,4 Liming Chen,1 Zhenqiang Song1
1Department of Endocrinology, NHC Key Laboratory of Hormones and Development, Tianjin Key Laboratory of Metabolic Diseases, Chu Hsien-I Memorial Hospital & Tianjin Institute of Endocrinology, Tianjin Medical University, Tianjin, People’s Republic of China; 2Department of Information Management, NHC Key Laboratory of Hormones and Development, Tianjin Key Laboratory of Metabolic Diseases, Chu Hsien-I Memorial Hospital & Tianjin Institute of Endocrinology, Tianjin Medical University, Tianjin, People’s Republic of China; 3Department of Medical, Happy Life Technology Co Ltd, Beijing, People’s Republic of China; 4Department of Yutang, Andon Health Co., Ltd, Tianjin, People’s Republic of China
Correspondence: Zhenqiang Song, Department of Endocrinology, NHC Key Laboratory of Hormones and Development, Tianjin Key Laboratory of Metabolic Diseases, Chu Hsien-I Memorial Hospital & Tianjin Institute of Endocrinology, Tianjin Medical University, No. 6 North Huanrui Road, Beichen District, Tianjin, People’s Republic of China, Tel +86-18602276218, Fax +86-022-59562017, Email [email protected]
Background: Our previous study demonstrated that digital diabetes care model (DDCM) created by multidisciplinary care team (MDCT) can improve glycemic control for patients with diabetes than usual care. Therefore, we aimed to explore long-term glycemic control with DDCM and influencing factors in type 2 diabetic cohort, in order to make a portrait for diabetes with goal-achieved HbA1c in clinics.
Methods: A total of 1198 outpatients with type 2 diabetes using DDCM for at least 12 months were recruited as a cohort. Medical records and specific DDCM indexes were collected. The influencing factors for glycemic control were explored by multivariate logistic regression analysis, followed by an internal and external validation.
Results: A total of 887 patients were finally included. HbA1c target-achieving rate was increased from 39.83% at baseline to 71.79% after 3-month follow-up. A shorter duration of diabetes, more frequent self-monitoring of blood glucose, lower HbA1c level at baseline, and less frequent emergency out-of-hospital follow-ups were influencing factors for HbA1c < 7% at 12-month follow-up. AUC of the prediction model was 0.790, with a sensitivity of 69.7% and specificity of 76.1%. Internal and external validation in patients using the DDCM monitored by MDCT indicated that the DDCM was robust (AUC =0.783 and 0.723, respectively).
Conclusion: Our findings made a portrait for T2DM with goal-achieved HbA1c in our DDCM. It is important to recognize associated factors for health providers to make personalized intervention in clinical practice.
Keywords: digital diabetes care model, glycemic control, type 2 diabetes management
Introduction
Type 2 diabetes mellitus (T2DM) is a metabolic disorder caused by both genetic and environmental factors that has become a worldwide health issue due to the high prevalence and associated risks of disability and mortality. A report published by the International Diabetes Federation in 2021 states that approximately 537 million adults aged 20–79 years worldwide are living with T2DM, including 140.9 million in China, which accounts for the largest population by country.1 T2DM can lead to severe micro- and macro-vascular complications, such as blindness, diabetic kidney disease, cardiovascular disease, and diabetic foot, which further increase the risk of all-cause mortality.2,3 Due to the failure to stabilize diabetes prevalence and reduce mortality, global economic burden of diabetes in 2030 will be more greater, especially North America and East Asia and the Pacific region. Therefore, diabetes will likely pose an even larger burden to national health systems and economies than currently, and more effective management strategies for T2DM care are urgently needed.
Although various medications are available to effectively reduce hemoglobin A1c (HbA1c) levels in patients with T2DM, appropriate lifestyle interventions, such as low-fat diets, encouragement of physical activity, and weight loss programs, combined with integrated care, can achieve HbA1c goal.4,5 The development of new technologies has revolutionized treatment of T2DM. In addition, health education, real-time counseling, self-management, and regular follow-ups via smartphone applications are considered essential for the overall care of patients with T2DM and achieving target HbA1c concentrations of <7%.6,7 Since many complex factors are involved in comprehensive control of T2DM, a more effective care model is urgently needed.
Our multidisciplinary care team (MDCT) created a novel digital diabetes care model (DDCM) in 2016 forT2DM patients that combines the use of a unique smartphone application, smart wearable wireless blood glucose (BG) monitor, web platform, and data-sharing cloud platform. In addition to in-person clinical visits, consenting patients were enrolled in a digital system administrated through the smartphone application that was wirelessly connected to a glucose meter to allow convenient access to medical records and uninterrupted communication with the MDCT to receive information about diet and exercise, and obtain timely advice to address medical emergencies, such as severe hypo- and hyperglycemia.
A previous retrospective study conducted by our group of 37,913 patients with T2DM demonstrated improved glycemic outcomes with the DDCM (formerly called “mobile-based intervention”) versus routine clinical care.8,9 As a further work, the aim of the present study was to identify factors influencing glycemic control and make a portrait for HbA1c goal-achieved patients with the use of the DDCM over a 12-month period, in order to optimize management of T2DM patients.
Methods
Study Approval
The study protocol was approved by the Ethics Committee of Tianjin Medical University Chu Hsien-I Memorial Hospital (approval no. DXBYYhMEC2020-34) and conducted in accordance with the ethical principles for medical research involving human subjects described in the Declaration of Helsinki. Prior to inclusion in this study, written informed consent was obtained from all subjects.
Study Design
The medical records of 5168 outpatients who used the DDCM between June 2016 and January 2020 were retrieved from the electronic database of Tianjin Medical University Chu Hsien-I Memorial Hospital and retrospectively reviewed. The retrieved data included patient demographics, diagnoses, and clinical examination results. The inclusion criteria were a confirmed diagnosis of T2DM, age of 18–70 years, program enrollment for ≥12 months, and documented serial HbA1c measurements. The exclusion criteria were a diagnosis of prediabetes, type 1 diabetes, gestational diabetes, or other type of diabetes.
DDCM
The DDCM was created to provide continuous, real-time, personalized healthcare from the MDCT, which consisted of physicians, nurses, health educators, and dietitians. The DDCM is a unified T2DM management system consisting of a smartphone application, smart wearable wireless BG monitor, web platform, and data-sharing cloud platform.9 At each in-person clinical visit, the patients received routine healthcare, which included medical treatment by physicians and structured lectures about diet and physical activity by specialized educators. Data on daily glucose values, diets, and activities were continuously available from the cloud platform as well as feedback from the MDCT. In addition, the MDCT was available for immediate help with medical emergencies, such as severe hypo- and hyperglycemia.
Definition and Data Collection
Demographics (sex, age, education level, employment status, marital status, economic level, and medical insurance), medical history (comorbidities and surgery), vital signs, and results of routine laboratory examinations upon admission and at the 12-month follow-up were collected. In addition, relevant data retrieved from the DDCM were also collected, which included the frequency of BG self-monitoring, regularity of return visits, in-clinic healthcare education, frequency of online follow-ups and emergency, frequency of messages sent and received, and number of education articles read by the patient.
Frequency of BG self-monitoring was defined as the number of times the patient self-monitored BG levels. The regularity of return visits was defined as the number of visits to the outpatient clinic as recommended by the DDCM (ie, every 3 months). The number of in-clinic healthcare education sessions attended by the patient was also recorded. The frequency of out-of-hospital follow-ups was based on the documented BG test results. An urgent out-of-hospital follow-up was defined as receiving remote support from the MDCT for hyper- or hypoglycemia. Effective communication was defined as timely feedback from the MDCT. In addition, the number of articles on T2DMread by the patient from the smartphone application was recorded. The target of glycemic control for patients with T2DM was defined as HbA1c <7%.
Outcomes
The primary outcome was HbA1c control from baseline to 3, 6, 9, and 12 months with the use of the DDCM. Factors influencing HbA1c control were also investigated.
Statistical Analysis
The data are presented as the number and percentage or the median and interquartile range (IQR). The multiple imputations by chained equations method were used to meet statistical requirements for variables with a missing data rate <25%. Univariate logistic regression was used to compare data between the target and non-target groups. A probability (p) value <0.05 was considered statistically significant. Bootstrap sampling of all patients with T2DMwho used the DDCM was performed. A prediction model was constructed for internal validation of HbA1c <7% at the 12-month follow-up examination. In addition, internal and external validations were conducted of patients who used the DDCM from Tianjin Medical University Chu Hsien-I Memorial Hospital and Tianjin Yellow River Hospital. Multivariate logistic regression analysis of factors with significant differences by univariate analysis was performed to identify independent predictors of HbA1c <7% at the 12-month follow-up. The odds ratio (OR) and 95% confidence interval (CI) of the independent risk factors were calculated to create a prediction model. The area under the receiver operating characteristic curve (AUC) was chosen as the primary evaluation metric for the model. The Hosmer–Lemeshow test was used to evaluate the goodness of fit (R2) of the logistic regression model. A nomogram was generated of the probability of HbA1c <7% at the 12-month follow-up. All data analyses were conducted using R software version 3.6.3 (https://www.r-project.org/).
Results
Baseline Characteristics of Patients
Of 1198 patients with T2DM using the DDCM, 887 (74.0%) met the inclusion criteria. The median age of the included patients was 58(IQR, 49.0–65.0) years, the male-to-female ratio was 1.8:1, the mean HbA1c level at baseline was 7.2% (IQR 6.5%–8.6%), the mean duration of T2DM was 8 (IQR, 4.0–14.0) years, and 39.83% (337/887) had baseline HbA1c levels <7% (Table 1). The median number of regular outpatient visits was 3 [2.00, 4.00]. Two-way communication was the most common (86.9%) approach between patients and the MDCT (Table 1).
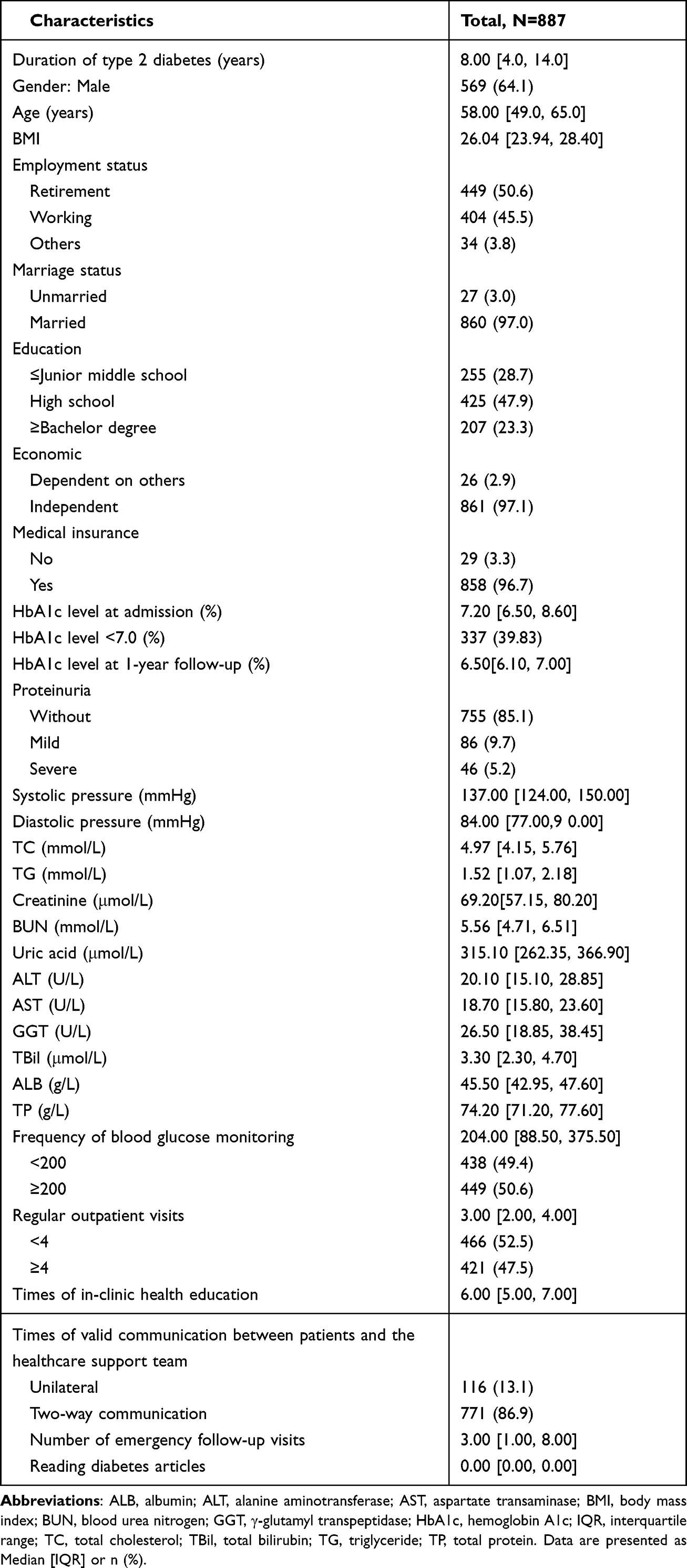 |
Table 1 Baseline Characteristics of All Patients |
Achievement of the HbA1c Target
Use of the DDCM was associated with significantly improved rates of achieving the target HbA1c level (71.79%, 72.86%, 73.66%, and 71.70% at 3, 6, 9, and 12 months, respectively).
From baseline to 12 months, the median HbA1c level of the outpatients decreased from 7.3% (IQR, 6.5%–8.6%) to 6.6% (IQR, 6.1%–7.0%). At 12 months, the medianHbA1c level of the target group decreased from 6.9% (IQR, 6.3%–8.1%) to 6.3% (IQR, 5.9%–6.6%), whereas that of the non-target group decreased from 8.0% (IQR, 7.2%–9%) to 7.5% (IQR, 7.2%–7.9%).
Comparisons of T2DM-Related Factors Between the Target and Non-Target Groups at 12 Months by Univariate Analysis
Baseline HbA1c levels were lower, disease duration was shorter, body mass index (BMI) was lower, education level was higher, frequency of BG self-monitoring was greater, frequency of regular outpatient visits was greater, and frequency of hospital and emergency follow-ups were fewer in the target vs non-target group. There were no significant differences in the male-to-female ratio, mean age, employment status, marriage status, economic level, mode of payment, number of short messages sent/received by patients, or number of articles read between the target and non-target groups (Table 2).
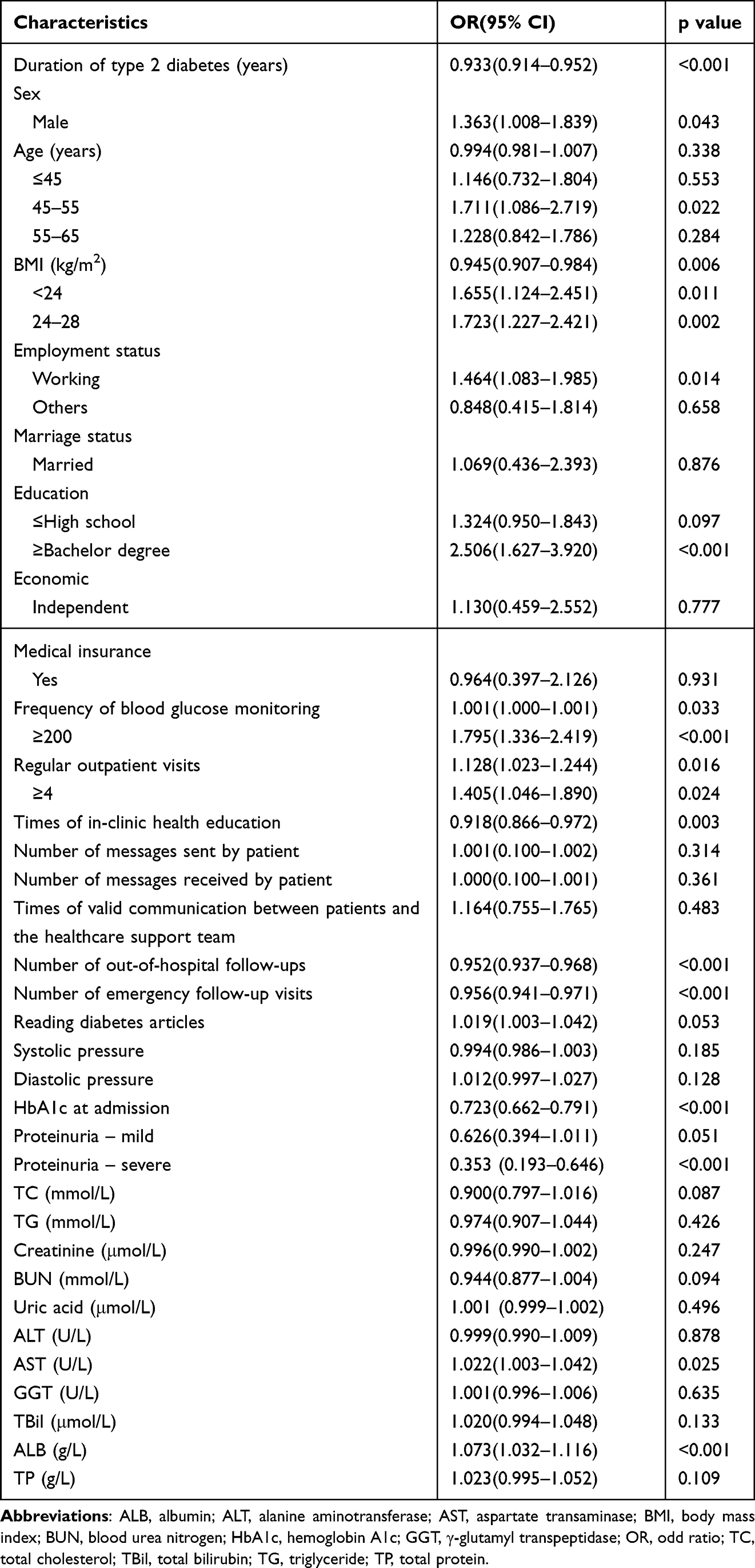 |
Table 2 Comparison Between the Two Groups by Univariate Analysis |
Factors Influencing the Target HbA1c Level <7% at 12 months
Significant variables identified by univariate analysis were used for multiple logistic regression analysis (Table 3). A nomogram was constructed to predict the probability of achieving the HbA1c target of <7% at 12 months with use of the DDCM. The independent risk factors for failure to achieve the target HbA1c level at 12 months included a longer duration of T2DM (OR = 0.939; 95% CI 0.916–0.962, p<0.001), higher HbA1c level at baseline (OR = 0.698, 95% CI = 0.630–0.771, p<0.001), lower frequency of BG self-monitoring (OR = 4.323, 95% CI = 2.891–6.576, p<0.001), and greater frequency of emergency online follow-ups (OR = 0.938, 95% CI = 0.917–0.959, p<0.001). The AUC was 0.790 with sensitivity of 69.7% and specificity of 76.1%. The R2 value obtained by the Hosmer–Lemeshow fit test was 6.733. Moreover, internal validation based on a bootstrap sampling of 887 cases and external validation based on 523 patients who used the DDCM monitored by the MDCT at Tianjin Yellow River Hospital indicated that the DDCM was robust (AUC=0.783 and 0.723, respectively).
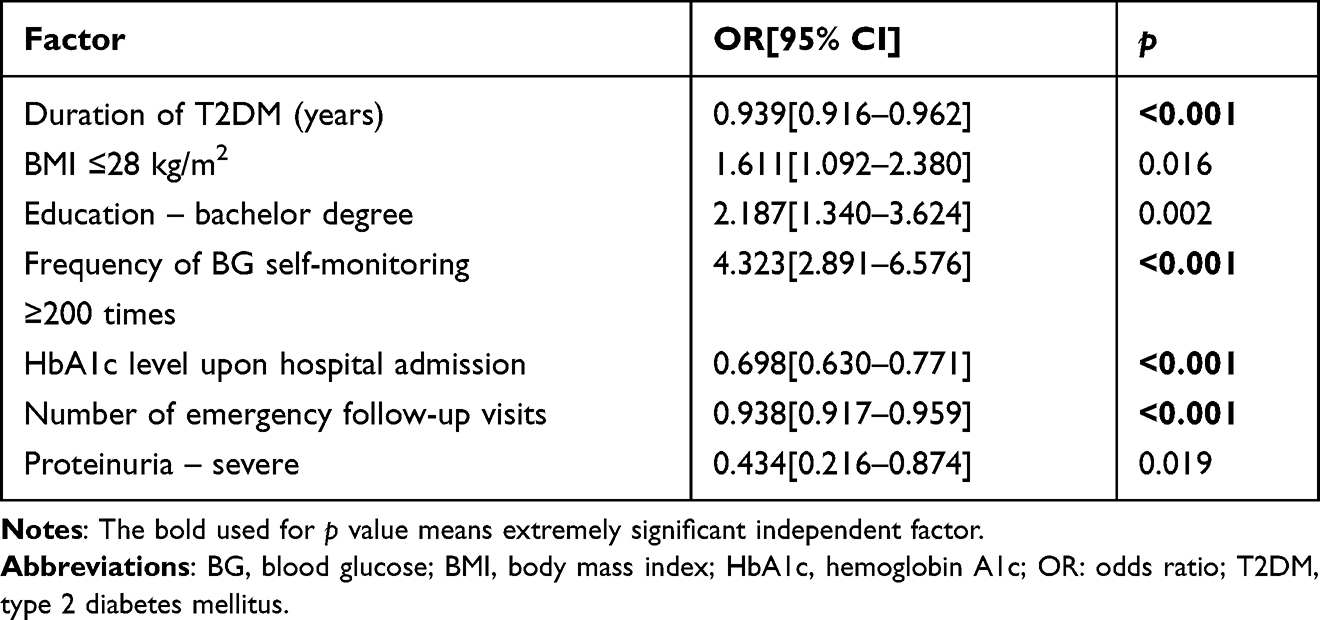 |
Table 3 Independent Factors Influencing Target HbA1c at 12 Months |
Discussion
Our group produced the DDCM as an innovative tool for comprehensive management of patients with T2DM. Use of the DDCM was shown to effectively improve HbA1c control after 3 months and levels were generally sustained for the 12-month study period. Overall, HbA1c levels were greatly improved and the proportion of patients achieving the HbA1ctarget of <7% was significantly increased at 12 months. Factors influencing achievement of the HbA1c target included short disease duration, high frequency of BG self-monitoring, lower HbA1c levels at baseline, and fewer online follow-ups. Our findings made a portrait for diabetic patients with goal-achieved HbA1c from DDCM and pave the way for further investigation of long-term clinical outcomes in T2DM.
Monitoring of HbA1c levels, as a gold standard for glycemic control, is especially important to prevent the development and progression of T2DM-related complications, as intensive glycemic control is strongly associated with diabetic complications and mortality.10 A previous prospective observational study11 reported that every 1% reduction in the mean HbA1c value was associated with a 21% reduction in the risk of T2DM-related complications. Although various new glucose-lowering drugs have been approved for T2DM, the rate of achieving HbA1c target levels was only 39.7% among diabetic patients in China in 2013, which was very disappointing.12 Since T2DM is a lifestyle-related chronic disease, alternative methods to drug intervention are needed.12
The proposed DDCM provides comprehensive management with both in-person and online services to reduce the need for doctor visits, lab work, and examinations by providing screening for complications, patient education, online follow-ups, dietary advice, instruction to improve physical activity, and timely consultations. In the present study, the HbA1c target rates achieved with the DDCM were ~70% from 3 to 12 months, which further confirmed the results of our previous reports.9,13
Since prior glucose control has sustained effects that persist even after return to more usual glycemic control, early hyperglycemia can cause subsequent damage to tissues and organs.14 Thus, from the perspective of clinical practice, it is important to achieve HbA1c target as soon as possible and maintain HbA1c levels for long periods to reduce the risk of diabetic complications. Therefore, it is important to identify factors that influence HbA1c control. The results of the present study showed that a shorter duration of T2DM, lower BMI, lower HbA1c levels at baseline, higher education level, greater frequency of BG self-monitoring, and fewer emergent follow-ups with the use of the proposed DDCM helped to achieve HbA1c target. However, self-management behaviors and awareness of BG monitoring greatly impact glucose control. Other factors identified in this study, including communication, patient-generated health data, education, and feedback, are similar to the findings of previous systematic reviews and meta-analyses.15
Altogether, our results demonstrated that DDCM can greatly increase the HbA1c goal-achieving rate in diabetes by enhancing the awareness of self-health-management. The earlier diabetic patients use DDCM after diagnosis, the better glycemic outcomes, less complications and lower healthcare cost they will have, since DDCM can provide timely, individualized and full cycle care from MDCT. There were some limitations to this study that should be addressed. First, this was a retrospective, single-center study; thus, prospective trials are needed to confirm the results. Second, although the model was externally validated, further verification is required with other populations. Third, a 12-month follow-up period is not sufficient to explore the long-term cardiovascular outcomes of the DDCM.
Conclusion
Patients with short disease duration, high frequency of BG self-monitoring, and low HbA1c baseline levels significantly improved HbA1c target with use of the DDCM. It is important to recognize associated factors for health providers to make personalized intervention in clinical practice. DDCM may be an optimized choice for diabetic patients after being diagnosed. Further studies are expected to explore the long-term effect of DDCM on diabetic complications and related mortalities.
Abbreviations
ALB, albumin; ALT, alanine aminotransferase; AST, aspartate transaminase; AUC, area under curve; BG, blood glucose; BMI, body mass index; BUN, blood urea nitrogen; CI, confidence interval; DDCM, digital diabetes care model; GGT, γ-glutamyl transpeptidase; HbA1c, hemoglobin A1c; IQR, interquartile range; MDCT, multidisciplinary care team; OR, odds ratio; TBil, total bilirubin; TC, total cholesterol; T2DM, Type 2 diabetes mellitus; TG, triglyceride; TP, total protein.
Acknowledgments
We thank LetPub (www.letpub.com) for linguistic assistance.
Funding
This work was supported by National Key R&D Plan Strategic International Science and Technology Innovation Cooperation Key Project (2018YFE0205000) and Tianjin Key Medical Discipline (Specialty) Construction Project (TJYXZDXK-032A).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Magliano DJ, Boyko EJ, IDF Diabetes Atlas 10th edition scientific committee. IDF Diabetes Atlas. IDF diabetes Atlas 2021,
2. Bragg F, Holmes MV, Iona A, et al. Association between diabetes and cause-specific mortality in rural and urban areas of China. JAMA J Am Med Assoc. 2017;317(3):280–289. doi:10.1001/jama.2016.19720
3. Xu G, Liu B, Sun Y, et al. Prevalence of diagnosed type 1 and type 2 diabetes among US adults in 2016 and 2017: population based study. BMJ. 2018;362:k1497. doi:10.1136/bmj.k1497
4. ADA. 6. obesity management for the treatment of type 2 diabetes. Diabetes Care. 2016;39(Suppl 1):S47–51. doi:10.2337/dc16-S009
5. Gorter KJ, Laar FA, Janssen P et al. Diabetes: glycaemic control in type 2 (drug treatments). BMJ Clin Evid. 2012;2012:0609.
6. Ayre J, Bonner C, Bramwell S, et al. Factors for supporting primary care physician engagement with patient apps for type 2 diabetes self-management that link to primary care: interview study. JMIR mHealth uHealth. 2019;7(1):e11885. doi:10.2196/11885
7. Dong Y, Wang P, Dai Z . Increased self-care activities and glycemic control rate in relation to health education via Wechat among diabetes patients: a randomized clinical trial. Medicine(Baltimore). 2018;97(50):e13632. doi:10.1097/MD.0000000000013632
8. Garabedian LF, Ross-Degnan D, Wharam JF. Mobile phone and smartphone technologies for diabetes care and self-management. Curr Diab Rep. 2015;15(12):109. doi:10.1007/s11892-015-0680-8
9. Li J, Sun L, Wang Y, et al. A mobile-based intervention for glycemic control in patients with type 2 diabetes: retrospective, propensity score-matched cohort study. JMIR mHealth uHealth. 2020;8(3):e15390. doi:10.2196/15390
10. Zinman B, Genuth S, Nathan DM. The diabetes control and complications trial/epidemiology of diabetes interventions and complications study: 30th anniversary presentations. Diabetes Care. 2014;37(1):8. doi:10.2337/dc13-2111
11. Stratton IM, Adler AI, Neil HA et al. Association of glycaemia with macrovascular and microvascular complications of type 2 diabetes (UKPDS 35): prospective observational study. BMJ. 2000;321(7258): ;405–412. doi:10.1136/bmj.321.7258.405
12. Xu Y, Wang L, He J et al. Prevalence and control of diabetes in Chinese adults. JAMA. 2013;310(9):948–959. doi:10.1001/jama.2013.168118
13. Shen Y, Wang F, Zhang X et al. Effectiveness of internet-based interventions on glycemic control in patients with type 2 diabetes: meta-analysis of randomized controlled trials. J Med Internet Res. 2018;20(5):e172. doi:10.2196/jmir.9133
14. Yin H, Liang S, Hua HE et al. Progress in therapeutic strategy for high glucose induced metabolic memory. Progress Pharmaceutical Sci. 2018;42(08):599–607.
15. Greenwood DA, Gee PM, Fatkin KJ et al. A systematic review of reviews evaluating technology-enabled diabetes self-management education and support. J Diabetes Sci Technol. 2017;11(5) :1015–1027. doi:10.1177/1932296817713506
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.