Back to Journals » Drug Design, Development and Therapy » Volume 20
Population Pharmacokinetics and Clinical Application of Vancomycin in Critically Ill Adults: A NONMEM-Based Review
Authors Husheng H, Wang Y, He Y ![]() , Shen F, Chen J
, Shen F, Chen J
Received 12 February 2026
Accepted for publication 5 May 2026
Published 14 May 2026 Volume 2026:20 603150
DOI https://doi.org/10.2147/DDDT.S603150
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Solomon Tadesse Zeleke
Huanran Husheng,1– 3 Ying Wang,1,4 Yan He,1– 3 Feng Shen,4 Jiyu Chen1– 3
1Clinical Trials Center & Key Laboratory of Clinical Pharmacology and Translational Research, the Affiliated Hospital of Guizhou Medical University, Guiyang, 550000, People’s Republic of China; 2School of Pharmacy, Guizhou Medical University, Guiyang, 550000, People’s Republic of China; 3Guizhou Provincial Key Laboratory for Digestive System Diseases, The Affiliated Hospital of Guizhou Medical University, Guiyang, 550000, People’s Republic of China; 4Department of Critical Care Medicine, Affiliated Hospital of Guizhou Medical University, Guiyang, 550004, People’s Republic of China
Correspondence: Jiyu Chen; Feng Shen, The Affiliated Hospital of Guizhou Medical University, Beijing Road, Yunyan District, Guiyang, Guizhou, 550004, People’s Republic of China, Email [email protected]; [email protected]
Abstract: Vancomycin remains an important treatment for severe Gram-positive infections in the intensive care unit (ICU), but critically ill adults show highly variable pharmacokinetics, making conventional dosing unreliable. This review aimed to summarize Nonlinear Mixed-Effects Modeling (NONMEM)-based population pharmacokinetic studies of vancomycin in critically ill adults and identify clinically relevant covariates associated with exposure variability. PubMed, Embase, and Google Scholar were searched from inception to January 2026. Twelve original studies met the inclusion criteria. All focused on adult ICU populations and used nonlinear mixed-effects modeling with NONMEM. One-compartment models were most commonly used, although parameter estimates varied substantially across populations. Typical clearance ranged from 1.19 to 5.15 L/h. Excluding volume estimates that needed to be normalized to actual body weight, reported typical values ranged from 29.2 to 107 L. Covariate analyses consistently identified renal function and body weight as important determinants of clearance, whereas continuous renal replacement therapy (CRRT)/high-volume hemofiltration (HVHF) intensity and residual renal function were particularly relevant in patients receiving extracorporeal support. Mechanical ventilation was retained as a covariate on clearance in some models. Overall, these findings highlight the marked heterogeneity of vancomycin pharmacokinetics in critical illness and support more individualized dosing strategies, ideally combining early therapeutic drug monitoring with model-informed precision dosing. Factors influencing drug clearance: demographics, pathology, treatment.The illustration shows factors influencing drug clearance and distribution volume in patients. On the left, a patient is depicted in a hospital bed connected to medical devices, including mechanical ventilation, continuous renal replacement therapy (CRRT) and high-volume hemofiltration (HVHF). Demographic factors such as weight, age and gender are highlighted. Pathological factors include multiple organ dysfunction, hemodynamic instability, renal function, hypoalbuminemia and capillary leak. On the right, patient factors affecting clearance include higher creatinine clearance and age over 65 years, which results in lower clearance. Distribution volume is influenced by higher total body weight. Treatment factors impacting clearance include higher CRRT intensity, higher residual urine volume and mechanical ventilation, which leads to lower clearance. Arrows indicate the relationship between these factors and their impact on clearance and distribution volume.
Keywords: vancomycin, population pharmacokinetics, critically ill adults, NONMEM, continuous renal replacement therapy, mechanical ventilation
Introduction
Vancomycin is a glycopeptide antibiotic widely used for severe Gram-positive infections, particularly methicillin-resistant Staphylococcus aureus (MRSA), Corynebacterium jeikeium, and multidrug-resistant Streptococcus pneumoniae. As a first-line agent for MRSA and other serious Gram-positive infections in critically ill patients, it is frequently used in sepsis, complicated infections, and septic shock. The clinical importance of this issue is underscored by the global burden of MRSA: in the latest GBD 2021 analysis, MRSA was associated with approximately 550,000 deaths globally and caused about 130,000 attributable deaths in 2021.1
Because vancomycin has a narrow therapeutic window, subtherapeutic exposure may lead to treatment failure and bacterial resistance, whereas excessive exposure increases the risk of nephrotoxicity and ototoxicity.
The 2020 ASHP/IDSA consensus guideline recommends AUC-guided monitoring with an AUC/MIC target of 400–600 for serious MRSA infections and no longer recommends trough-only monitoring targeting 15–20 mg/L.2 In critically ill adults, however, dose selection is particularly difficult because pharmacokinetics may change rapidly. Hemodynamic instability, multiorgan dysfunction, renal replacement therapy, capillary leak, fluid resuscitation, and unstable renal function can all alter vancomycin clearance and distribution, leading to marked between-patient variability.
The clinical relevance of this variability is amplified in ICU populations. In the multinational EPIC III study including 15,202 adult ICU patients from 88 countries, 54% had suspected or proven infection, and hospital mortality among infected patients was 30%.3 Under these conditions, dosing strategies based only on body weight or creatinine clearance(CrCl) often fail to achieve target exposure. Although TDM is essential, concentration data alone may still be hard to translate into individualized dosing without an appropriate pharmacokinetic framework, especially when only a few early samples are available in patients with rapidly changing pharmacokinetics.2,4,5 Population pharmacokinetic (PopPK) models, especially when combined with bayesian forecasting, help translate limited monitoring data and patient-specific covariates into individualized dosing decisions.4–6 Studies have been published, uncertainty remains regarding the most appropriate model structure, the most clinically relevant covariates, and the bedside applicability of existing ICU models. This review summarizes published NONMEM-based PopPK studies of vancomycin in critically ill adults and evaluates their implications for individualized dosing.
Materials and Methods
Search Strategy
The literature for this review was identified by searching PubMed (n = 54), the integrated database Embase (n = 103), and Google Scholar (n = 35). The search covered from the beginning of each database to January 2026. The search used Medical Subject Headings (MeSH) terms and keywords about vancomycin, PopPK, and critically ill adult patients. The specific search query for PubMed was: (“vancomycin”[Mesh]) AND (“population pharmacokinetic*”[Title/Abstract]) AND (“Intensive Care Units”[Mesh] OR “critically ill”[Title/Abstract]). For Embase and Google Scholar, the query was: vancomycin PopPK in critically ill. All retrieved articles were screened and independently reviewed in duplicate.
Inclusion and Exclusion Criteria
Studies were included if they met the following criteria: 1. The study population consisted of critically ill adult patients (aged 18 years or older); 2. Vancomycin was administered intravenously (IV); 3. The study employed a population pharmacokinetic modeling approach; 4. The article was an original research study with accessible data; 5. It was published in the English language. The exclusion criteria were as follows: 1. In vitro, animal, or pediatric studies; 2. Review articles, commentaries, or methodological papers; 3. Studies that did not utilize population pharmacokinetic modeling; 4. Studies that did not employ NONMEM for model development; 5. Simulation-only studies.
Data Extraction
For each included study, the following information was extracted: all literature meeting the inclusion criteria were collected, and relevant data were extracted, including: 1. Basic Information and Patient Demographics: first author and publication year, country of origin, study design type (prospective/retrospective), patient population characteristics (eg, type of severe infection, receipt of CRRT), sample size and gender distribution (male/female), age, body weight, BMI, CrCL and renal function status classification), serum albumin level, and disease severity scores (eg, SOFA score); 2 Vancomycin Dosing Regimen and Pharmacokinetic Sampling Information: loading dose and maintenance dose, route of administration and infusion duration, sampling time points and sampling strategy (intensive/sparse sampling), and method for measuring plasma concentrations; 3. Population Pharmacokinetic Modeling Methodology and Covariate Analysis: structural model type (eg, one-, two-, three-compartment model), covariate selection and testing procedures, and the model parameter estimation method; 4 Pharmacokinetic Parameter Estimates and Variability: estimates for CL and its between-subject variability (BSV), V and its BSV, and the type of residual variability (RV) model (eg, additive, proportional, exponential).
Quality Assessment
Two reviewers independently assessed the methodological quality of each included study using the National Institutes of Health (NIH) Study Quality Assessment Tool for Case Series Studies7 Because the included studies were observational population pharmacokinetic analyses rather than randomized comparative trials, this tool was applied as a pragmatic framework for evaluating population definition, methodological transparency, outcome assessment, and reporting completeness. Disagreements were resolved by discussion until consensus was reached.
Results
Literature Collection
According to the NIH Study Quality Assessment Tool for Case Series Studies, the included studies were generally of fair to good methodological quality, and none was rated as poor. Detailed item-level assessments are provided in Table S1.
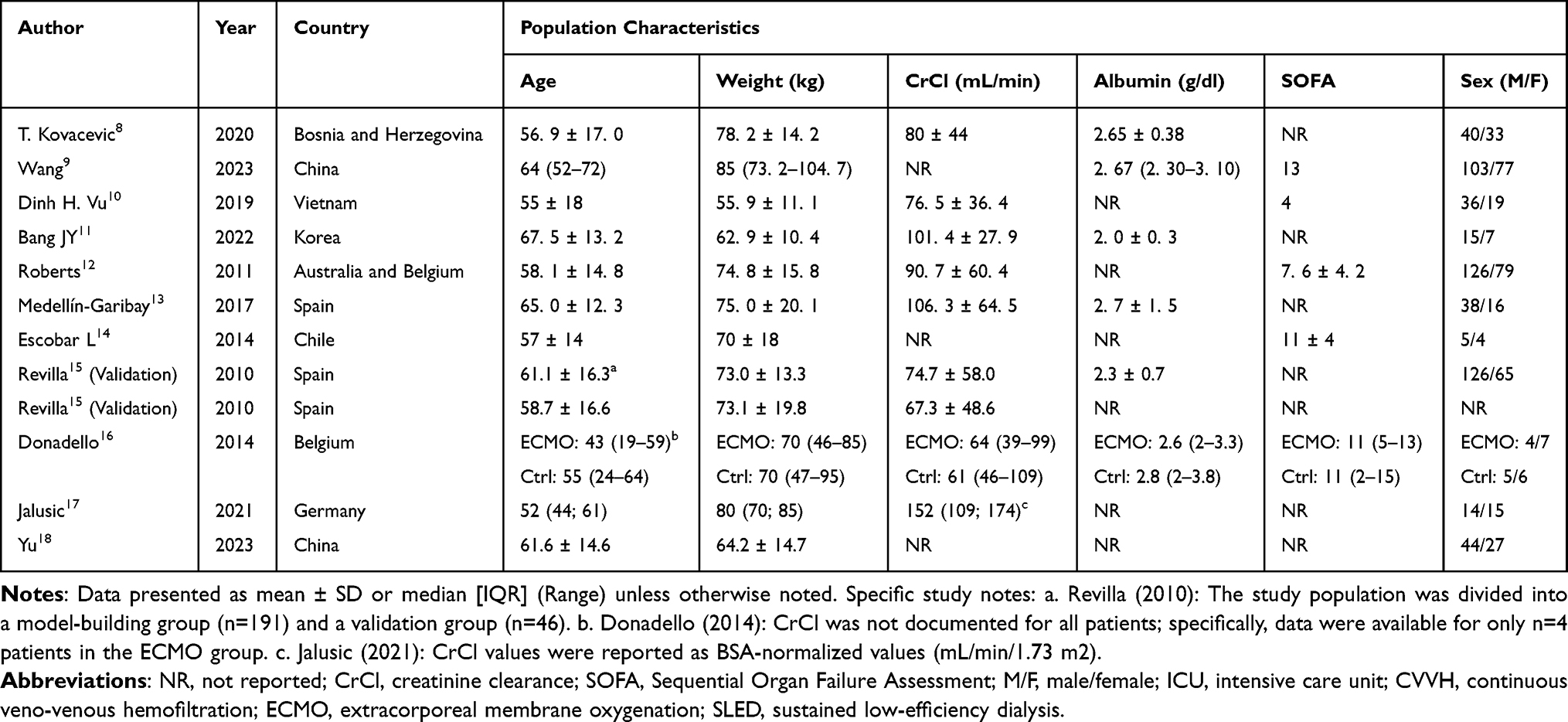 |
Table 1 Summary of Patients Demographics for All Population-Pharmacokinetic Studies Included in This Review |
The initial search yielded 192 potentially relevant articles. After screening based on titles and abstracts, 38 articles remained. Following full-text evaluation, 12 studies were included in this review (Figure 1, PRISMA). The characteristics of these 12 studies are summarized in Table 1. Geographically, the included studies were conducted across Asia, Europe, and South America, including China, South Korea, Vietnam, the Netherlands, Spain, Belgium, Bosnia and Herzegovina, Germany, and Chile. Many of the included cohorts involved patients with sepsis or septic shock, and several studies focused on patients receiving CRRT or other extracorporeal support.
 |
Figure 1 PRISMA 2020 flow diagram of study identification, screening, eligibility assessment, and inclusion for the present review. Adapted from Page MJ, et al. BMJ. 2021;372:n71, under the CC BY 4.0 licence. Abbreviation: PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses. |
Design and Methodological Characteristics of the Included Studies
All 12 PopPK studies included in this review focused on adult ICU patients and used NONMEM for population pharmacokinetic modeling. Among them, four studies employed a prospective design and eight were retrospective. Sample sizes varied considerably, ranging from 9 to 206 patients. Studies targeting specific physiological states, such as CRRT or septic shock, tended to have relatively smaller sample sizes; for example, Escobar collected 68 blood samples.14. Although all studies administered vancomycin intravenously, dosing regimens differed substantially. Udy, Vu, Medellin-Garibay, and the OLVG center in Roberts used continuous infusion,10,12,13,19 whereas other studies used intermittent dosing with loading and maintenance adjustment according to renal function. Kovacevic used a fixed regimen consisting of a 2 g loading dose followed by 1 g every 12 hours,8 and Escobar used a fixed daily dose of 1000 mg. Bang adopted a target-controlled infusion strategy after a 25 mg/kg loading dose to improve control of plasma concentrations.11,14
The sampling plans were mainly called “intensive sampling” or “sparse sampling.” Escobar used a very strict plan. They took samples when a 1-hour infusion started, and then at 0.5, 1, 2, 4, 6, 9, and 12 hours. Bang also took arterial blood samples at set times over 24 hours.14 Most studies utilized routine clinical TDM data. For instance, Kovacevic collected only a trough concentration before the 4th dose and a peak concentration 1-hour post-dose, while Udy routinely collected samples at 08:00 daily.8,19 For CRRT patients, the mean sampling interval in Wang was approximately 21.5 hours.9 The clinical characteristics of the studies are summarized in Table 2. The structural models, tested covariates, retained covariates, and evaluation methods of the included studies are summarized in Table 3.
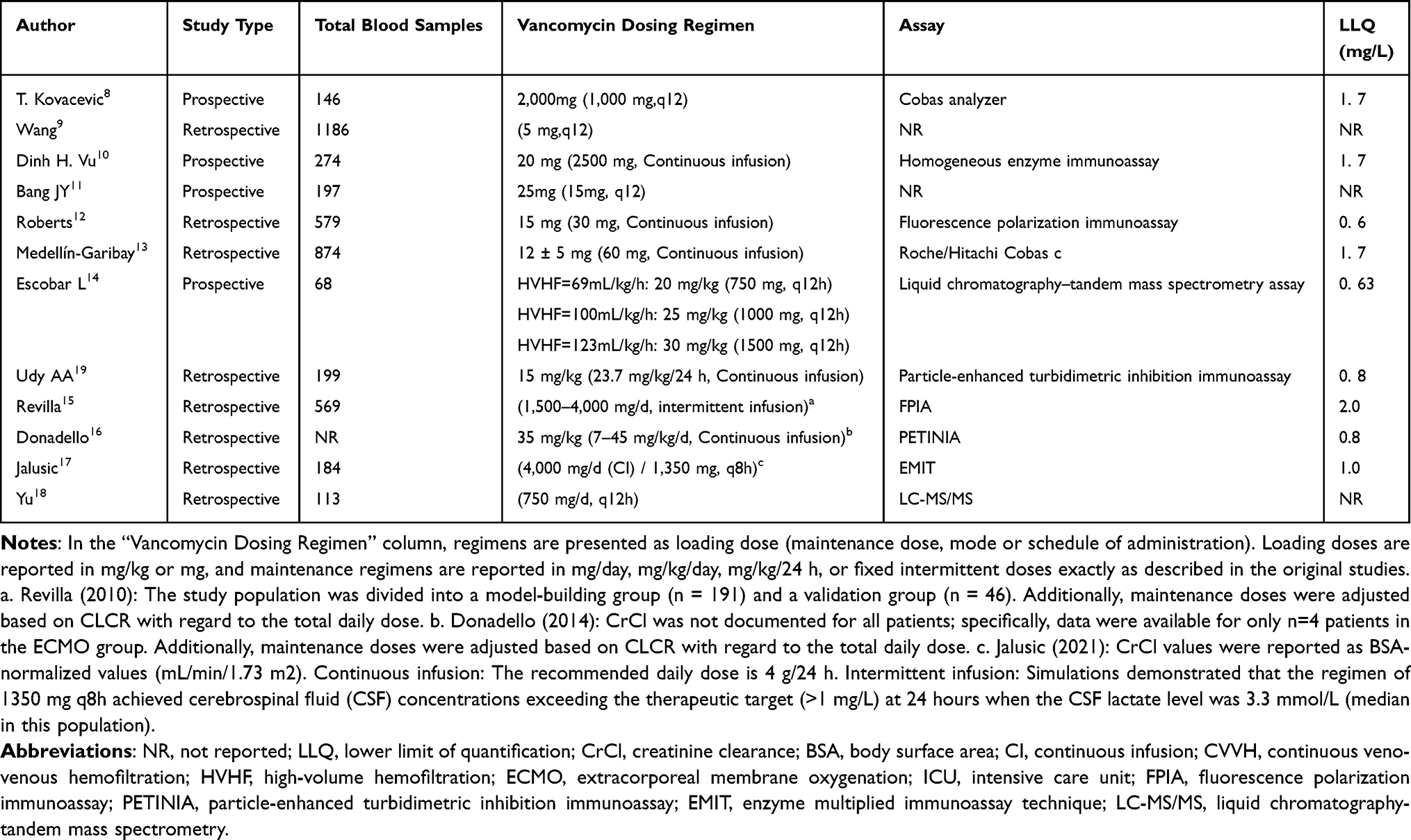 |
Table 2 Summary of the Clinical Protocols for Studies Included in This Review |
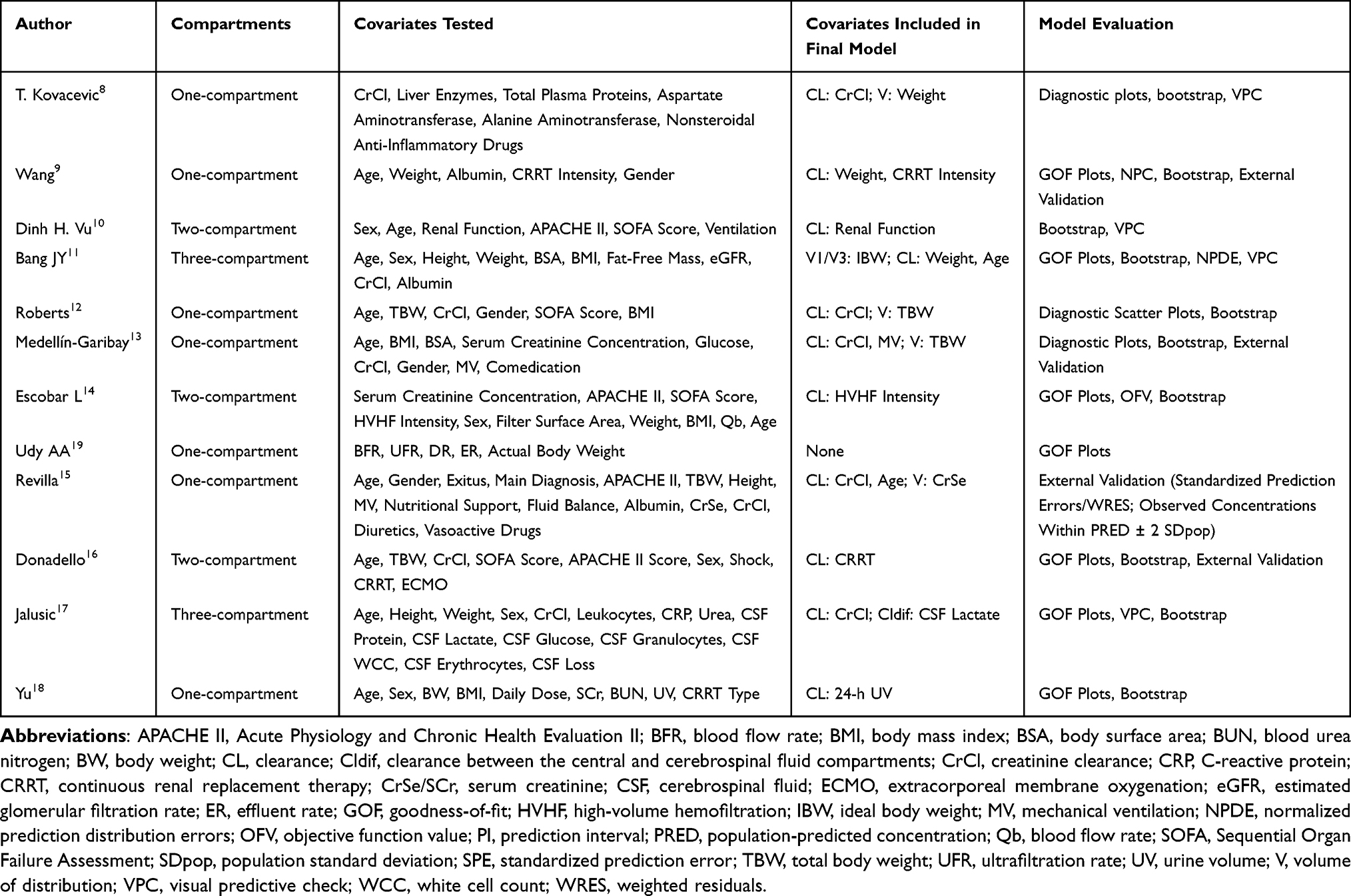 |
Table 3 Population Pharmacokinetic Modeling Methods, Tested and Retained Covariates by the Studies Included in the Review |
Population Pharmacokinetic Analysis
Across the twelve included studies, all PopPK models were developed in NONMEM using nonlinear mixed-effects modeling. Structural model selection appeared to depend largely on sampling design and clinical context. Studies based mainly on routine therapeutic drug monitoring (TDM) data and sparse sampling, such as those by Udy, Wang, Medellín-Garibay, and Kovacevic, generally used one-compartment models to support stable parameter estimation.8,9,13,19 By contrast, studies with richer sampling were more likely to support more complex structures. Vu and Escobar used two-compartment models, whereas Bang developed a three-compartment model in the setting of target-controlled infusion.10,11,14 This pattern is consistent with broader methodological reviews indicating that model structure in critically ill patients is shaped not only by software choice, but also by sampling density, renal support modality, and covariate quality.20,21
Clearance
Vancomycin clearance showed substantial between-study variability in critically ill adults, with typical values ranging from 1.19 to 4.58 L/h. Renal function remained the most consistent determinant of clearance, and several models identified CrCl as the dominant covariate, with higher CrCl generally associated with higher vancomycin clearance.8,12,13,15 However, creatinine-based estimates should be interpreted cautiously in critical illness because renal function is often unstable and serum creatinine may lag behind real-time changes in elimination.22 More recent evidence also suggests that cystatin C-based eGFR may improve prediction of vancomycin renal clearance in some settings, although this still requires confirmation in ICU populations.23
In patients receiving renal replacement therapy, treatment-related factors further contributed to clearance variability. Wang reported that increasing CRRT intensity was associated with increased clearance, whereas Escobar identified HVHF intensity as the only significant determinant of clearance, with values reaching 2.7 L/h under the highest filtration intensity.9,14 Bang also reported lower clearance in patients older than 65 years.11 Taken together, these findings suggest that vancomycin clearance in critically ill adults reflects both patient-specific renal function and treatment-related extracorporeal support, as also highlighted in broader evaluations of vancomycin dosing models in adults receiving renal replacement therapy.21,23 The effect of each covariate on clearance is shown in Figure 2. Figures 2 and 3 do not present absolute parameter estimates from individual studies. Instead, each retained covariate effect was normalized to a study-specific reference value, thereby facilitating qualitative comparisons to identify differences in the direction and magnitude of relative effects across studies. The numerical information underlying the relative effect ratios shown in Figures 2 and 3 including study-specific reference values, covariate ranges, and calculated ratios is provided in Tables S2 and S3, respectively.
 |
Figure 2 Study-specific relative effects of retained covariates on vancomycin clearance in critically ill adults. For each study, the typical clearance value was normalized to 1, and the horizontal interval represents the modeled relative change associated with the predefined covariate contrast within that study rather than a statistical confidence interval. Green lines denote renal-function-related covariates, pink lines denote organ-support-related covariates, and blue lines denote other modifiers. Open circles indicate studies that should be interpreted with additional caution because the included population differs from the general ICU setting. CrCl indicates creatinine clearance; UV indicates 24-hour urine volume; MV indicates mechanical ventilation; HVHF indicates high-volume hemofiltration; CRRT indicates continuous renal replacement therapy. Not all retained covariates identified across the reviewed studies are displayed in this panel. Covariates were preferentially included when the final model structure, covariate definition, and clinically interpretable contrast range could be reconstructed with sufficient confidence from the available source data. Reference numbers are shown as superscript Arabic numerals following the study names. Because retained covariates for clearance were more consistently defined across studies, a forest-style comparison was constructed for clearance only. A comparable plot was not generated for distribution-related parameters because the retained covariates were fewer and structurally heterogeneous across models (eg, V, V1, V3, TBW, IBW, and CrSe), which limited direct comparability. |
 |
Figure 3 Study-specific relative effects of retained covariates on vancomycin distribution-related parameters in critically ill adults. For each study, the typical distribution-related parameter value was normalized to 1, and the horizontal interval represents the modeled relative change associated with the predefined covariate contrast within that study rather than a statistical confidence interval. The panel highlights the most directly comparable body-size-related covariates retained across the included models. Additional distribution-related effects reported in some studies were not displayed in the main panel to preserve readability and comparability. Reference numbers are shown as superscript Arabic numerals following the study names. |
Volume of Distribution
In critically ill patients, capillary leak, inflammation, and fluid resuscitation can expand the extracellular fluid compartment and contribute to a relatively large apparent volume of distribution. Across the included studies, typical V estimates ranged from 29.2 to 107 L.9,12
Body-size descriptors were the most consistent covariates for V. Roberts identified total body weight (TBW) as a key determinant, with V increasing in proportion to body weight.12 Most studies likewise used TBW as the primary size descriptor, although Bang found that ideal body weight (IBW) reduced model variability, suggesting that the most appropriate size metric may vary by population and model structure.11 Studies with denser sampling, such as those by Vu and Escobar, were also better able to characterize distributional phases through two-compartment models.10,14
Model evaluation was most commonly based on bootstrap analysis, with visual predictive checks (VPC) and related predictive diagnostics also widely reported. External validation was performed in selected studies, including those by Wang, Medellín-Garibay, Revilla, and Donadello.9,13,15,16
This remains important in critically ill populations, where differences in renal support, sampling strategy, and case mix may limit model transportability across cohorts.21 The study-specific relative effects of retained covariates on vancomycin distribution-related parameters in critically ill adults are shown in Figure 3.
Discussion
This review aimed to summarize and identify key factors influencing vancomycin pharmacokinetics. By comparing published PopPK models, this review aimed to clarify the main sources of pharmacokinetic variability and their implications for precision dosing in different groups of critically ill patients.
A total of twelve PopPK analyses were included. These covered studies were published between 2010 and 2023. For modeling software, NONMEM was the most widely used tool. In contrast, for studies involving target-controlled infusion (TCI) or intensive sampling, two or three-compartment models proved to more accurately describe intercompartmental drug distribution. The estimated CL and V varied markedly across different target populations (Table 4). The included studies were predominantly prospective or retrospective analyses focusing on specific subgroups, such as critically ill patients with sepsis, acute kidney injury (AKI) receiving CRRT or HVHF. It is noteworthy that limited sample sizes and potential issues with sample representativeness may have constrained the ability of some studies to identify significant covariates.
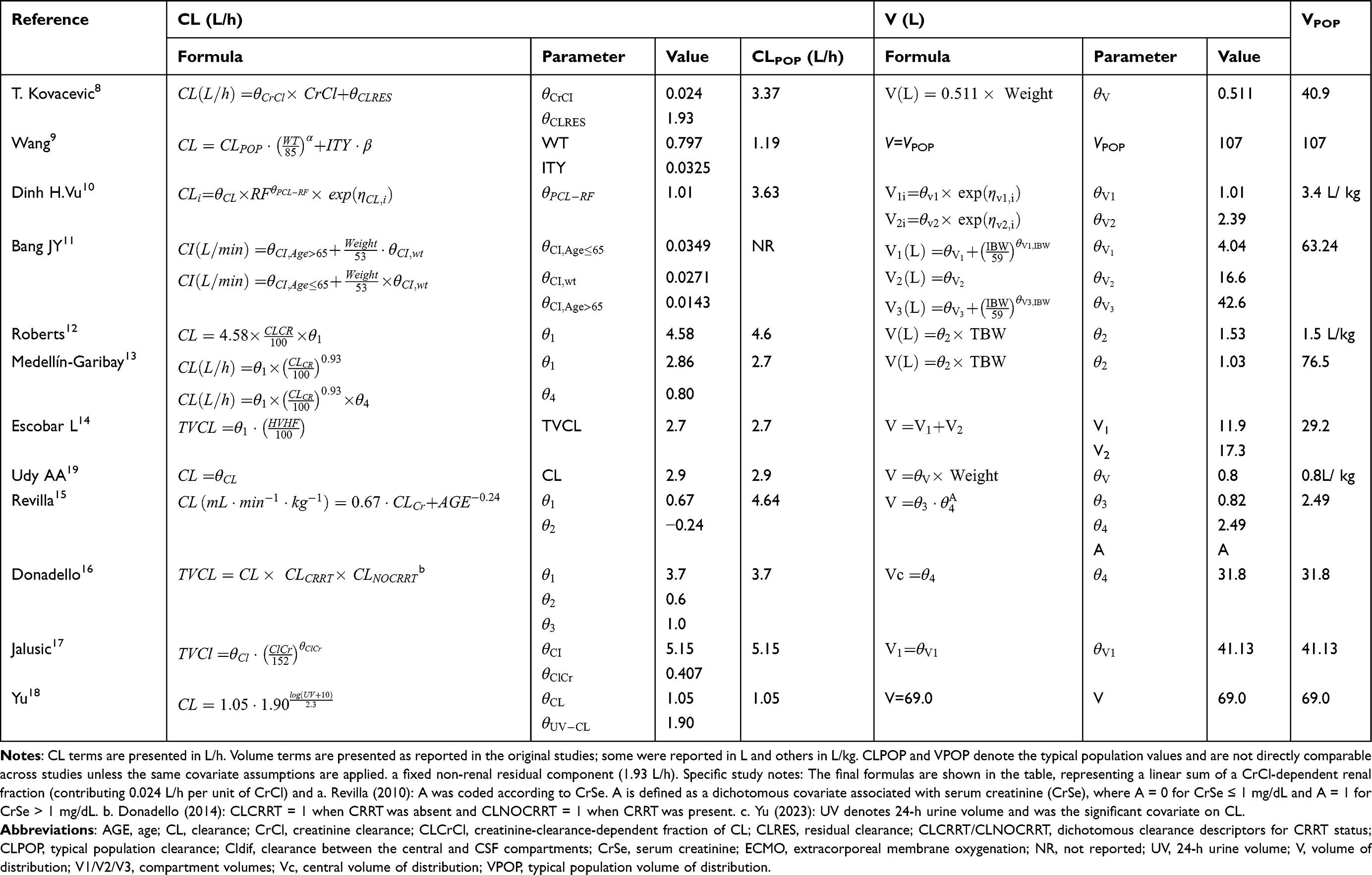 |
Table 4 A Summary of Final Models, Fixed and Random Effect Models Described in the Included Studies |
Core Advantages of NONMEM-Based Modeling
This review deliberately restricted study inclusion to population pharmacokinetic analyses developed using nonlinear mixed-effects modeling in NONMEM. NONMEM remains one of the most established and widely used platforms for population pharmacokinetic analysis and clinical pharmacometrics settings.24 Clarifying the methodological rationale for focusing on NONMEM is therefore important to the foundation of the present review.
In ICU settings, clinical pharmacokinetic data are often limited in sampling density and are accompanied by marked interindividual variability related to fluctuating renal function, fluid resuscitation, and organ support. Under such conditions, first-order conditional estimation with interaction (FOCE-I), as implemented in NONMEM, remains a commonly used and interpretable estimation approach, although its advantages are not absolute across all data structures.25 Compared with SAEM-based platforms, the main strengths of NONMEM lie less in universal statistical superiority and more in its long history of application, accumulated practical experience, and mature diagnostic and post-processing workflow.26
At the same time, alternative approaches also have value. For example, Pmetrics, which uses a nonparametric adaptive grid algorithm, may be more sensitive to multimodal distributions or atypical subpopulations and can be informative when log-normal parameter assumptions are difficult to justify.25 In practice, parametric and nonparametric methods serve different purposes. For most routine PopPK analyses, parametric platforms remain more mature in model interpretation, covariate evaluation, and standard reporting workflows, whereas nonparametric approaches may provide complementary information when latent subgroups or unusual parameter distributions are suspected.25
Another practical advantage of NONMEM is the breadth of its surrounding tool ecosystem, including widely used post-processing and diagnostic tools such as PsN and Xpose, which support internal evaluation procedures including bootstrap resampling, visual predictive checks, and numerical predictive checks.25,27 From the perspective of a systematic review, this methodological consistency improves comparability across studies. It also helps explain why NONMEM-based models, including those reported by Roberts, Wang, and others, have been particularly useful in identifying clinically relevant covariates in critically ill populations, such as CRRT intensity, residual urine output, and mechanical ventilation, within a relatively coherent analytic framework.9,12
Marked Between-Study Variability in Clearance and Volume of Distribution
The 12 studies included in this review showed substantial between-study variability in vancomycin population pharmacokinetic parameters. Typical clearance values ranged from approximately 1.19 to 4.58 L/h, whereas apparent volume of distribution ranged from 29.2 to 107 L. These differences are unlikely to reflect random variation alone. Rather, they probably arise from heterogeneity in patient pathophysiology, organ support strategies, and model-building approaches.
Systematic Differences in Renal Function Estimation and Sampling Strategy
One important source of clearance variability is the lack of uniformity in the way renal function was quantified across studies. As a hydrophilic drug eliminated predominantly by glomerular filtration, vancomycin clearance is closely linked to renal function. In studies such as those by Kovacevic and Medellín-Garibay, CrCl was primarily estimated using conventional formula-based approaches such as the Cockcroft-Gault equation.8,13 However, in the ICU, marked muscle wasting, aggressive fluid resuscitation, and the delayed response of serum creatinine during acute kidney injury can all reduce the reliability of estimated GFR derived from CG, MDRD, or CKD-EPI equations.
By contrast, the Roberts model used 24-hour urine collection to determine CrCl, which in theory better reflects dynamic renal elimination than a single serum creatinine-based estimate.12 That model also reported a comparatively high typical clearance and later showed relatively favorable predictive performance in external evaluation. Still, this should not be attributed solely to the method used to quantify renal function, since study population, dosing strategy, and model structure may also have contributed to its performance.
Organ Support and Extracorporeal Clearance
Organ support interventions, especially renal replacement therapy, represent another major source of clearance variability across studies. In the study by Wang, CRRT intensity emerged as an important covariate affecting vancomycin clearance, suggesting that increases in ultrafiltration and dialysate flow are associated with increased systemic clearance.9 Escobar further examined patients with refractory septic shock undergoing high-volume hemofiltration, with exchange rates as high as 100–123 mL/kg/h, and reported vancomycin clearance values approaching 2.7 L/h under these conditions.14 Dose simulations suggested that substantially higher regimens, such as 1000–1500 mg every 12 hours, might be needed to maintain minimum target concentrations in that setting.14 Not all extracorporeal support systems, however, increase clearance to the same extent. Yu showed that in patients receiving CRRT, 24-hour residual urine volume could explain interindividual variability in clearance better than machine settings alone.18 This finding implies that models based only on extracorporeal treatment parameters may have limited generalizability if residual renal function is not taken into account. Similarly, Medellín-Garibay reported that mechanical ventilation was associated with an approximately 20% reduction in vancomycin clearance, possibly reflecting hemodynamic changes induced by positive-pressure ventilation.13 In contrast, Donadello found no significant difference in either Vd or clearance between extracorporeal membrane oxygenation (ECMO) and non-ECMO patients.16 One plausible explanation is that the severe underlying illness in ECMO patients had already produced marked capillary leak and organ dysfunction, thereby attenuating the additional pharmacokinetic impact of the extracorporeal circuit itself.
Structural Model Complexity and Distributional Heterogeneity
Variability in volume of distribution is also likely related to differences in sampling design, structural model selection, and disease-related changes in tissue distribution. Most one-compartment models developed from sparse TDM data provide only a global estimate of apparent distribution volume. In addition, reported V values are not always directly comparable, because some studies expressed V in liters, whereas others reported V normalized to body weight.
By contrast, studies with denser sampling, such as those by Vu and Escobar, used two-compartment models that allowed central and peripheral distribution volumes to be distinguished.10,14 Jalusic went further by developing a three-compartment model in patients with ventriculitis associated with external ventricular drainage and found that cerebrospinal fluid lactate was associated with the parameter governing central-CSF distribution.17 This suggests that local inflammatory status may influence vancomycin penetration into the central nervous system. Even so, such findings were obtained in a specific infection phenotype and should be extrapolated to the general ICU population with caution.
Age
Age was retained as a covariate in some vancomycin population pharmacokinetic models, but it should be interpreted together with renal function, body size, comorbidity burden, and exposure monitoring. In the included studies, Bang found that age improved the clearance model more clearly when it was handled as a categorical covariate with a cutoff of 65 years than when it was treated as a continuous variable.11 Revilla also retained age as a predictor of clearance, which supports age as a real but not dominant covariate.15
On this basis, ≥65 years versus <65 years is a reasonable threshold for discussion in this review, and it fits the elderly literature better than a cutoff of 60 years.28–30 Even so, age should not be used on its own for dose selection.
Broader literature suggests that age mainly matters because it tracks with changes in renal function, body composition, and the limits of creatinine-based renal estimates. In older adults, these factors can lower vancomycin clearance and make exposure less predictable.30,31
Earlier comparative studies also reported lower clearance, longer half-life, and lower dose requirements in elderly and very elderly patients.28,29
By contrast, younger critically ill adults are more likely to have augmented renal clearance, which increases the risk of underexposure under standard dosing regimens.32,33
Clinically, patients younger than 65 years should be assessed for ARC-related underexposure, whereas those 65 years or older need closer monitoring for overexposure and nephrotoxicity, especially when trough concentrations are already high or AUC is approaching the upper end of the target range.34,35 Age stratification is useful, but dose selection still needs to be individualized with renal function, body weight, albumin, and TDM or MIPD-guided reassessment.
Mechanical Ventilation
In the model by Medellín-Garibay, mechanical ventilation was retained as a covariate on clearance, possibly because ventilation-associated changes in cardiac output and renal perfusion influence vancomycin elimination.13 A plausible physiological explanation is that positive-pressure ventilation, especially at higher levels of PEEP, may reduce venous return and increase right ventricular afterload, ultimately lowering cardiac output and secondarily renal blood flow.36,37 This may help explain why mechanically ventilated critically ill patients can show lower vancomycin clearance and greater uncertainty in early exposure. Dose individualization in this setting should therefore rely on early TDM and, when available, MIPD rather than on fixed empirical maintenance regimens alone.2,38,39 Although fluid shifts and capillary leak may also expand apparent volume of distribution in some ventilated ICU patients, the more consistent signal in the available PopPK literature concerns clearance rather than volume of distribution.
Sex
Across the included ICU PopPK studies, sex was not consistently retained as an independent covariate for vancomycin pharmacokinetics. In the Mangin model externally evaluated by Guo et al, male sex was associated with higher clearance than female sex, suggesting a possible sex-related difference in elimination in that specific model.40 However, in most other models assessed in the same analysis, including those by Udy, Roberts, and Medellín-Garibay, sex was not retained as a key determinant of clearance.12,13,19 This inconsistency suggests that any apparent sex effect is unlikely to represent a stable and generalizable biological determinant across critically ill populations.
In some models, sex may instead contribute indirectly through body size descriptors such as ideal body weight, rather than acting as a standalone pharmacokinetic covariate.11 Overall, current evidence does not support sex as a universal basis for vancomycin dose adjustment in critically ill adults, and any potential effect should be interpreted together with stronger determinants such as renal function and body size.
Liver Function Indices
Compared with renal function, CRRT intensity, and residual urine output, liver function indices have not emerged as stable and reproducible independent covariates in existing ICU vancomycin PopPK studies. In the studies included in this review, models such as those by Kovacevic and Medellín-Garibay evaluated liver enzymes or related biochemical variables, but these were not retained in the final models.8,13 This suggests that, in the critically ill setting, the contribution of routine hepatic markers to explaining vancomycin clearance and distribution is generally weaker than that of renal function, body weight, and organ support-related variables.
Mechanistically, this is not unexpected. Vancomycin is primarily eliminated through the kidneys, and hepatic function contributes only modestly to total drug clearance. As a result, variables such as ALT, AST, or bilirubin are often overshadowed by stronger determinants such as renal function and hemodynamic status in ICU models.41,42 That said, hepatic dysfunction should not be regarded as irrelevant. A more balanced interpretation is that liver dysfunction is more likely to affect vancomycin pharmacokinetics indirectly than to act as a stable direct covariate in final PopPK models. Severe liver disease or inflammation-related hepatic impairment is often accompanied by hypoalbuminemia, fluid shifts, and circulatory abnormalities, all of which may increase uncertainty in the distribution of hydrophilic drugs and weaken the interpretability of total drug concentrations.43
In addition, broader evidence from PopPK studies of antimicrobials in critically ill adults suggests that the variables most consistently retained in ICU models remain CrCl or GFR, body weight, urine output, renal replacement therapy, and albumin, whereas liver-related variables are reported and retained less frequently.44 Taken together, the current evidence does not support using routine hepatic function indices as core determinants for vancomycin dose adjustment in ICU patients. However, in patients with marked hypoalbuminemia, severe hepatic phenotype, or multiple organ dysfunction, greater reliance on early TDM and MIPD is still warranted, since empirical dosing alone may underestimate exposure variability.42,43
Hypoalbuminemia and Expansion of the Apparent Volume of Distribution
Hypoalbuminemia deserves discussion in critically ill patients because it often appears alongside severe infection, fluid resuscitation, and capillary leakage, all of which can complicate the interpretation of vancomycin exposure. Within the 12 included NONMEM studies, however, direct support for albumin as a stable independent covariate was limited. Albumin was considered during covariate screening in some studies, including those by Wang, Bang, and Revilla, but it was not retained in their final models, which instead favored variables such as body weight, CRRT intensity, CrCl, age, or serum creatinine.9,11,15 Taken at face value, the included studies do not support a uniform conclusion that albumin itself is a robust determinant of vancomycin clearance or distribution across ICU PopPK models.
Beyond the included studies, broader pharmacokinetic literature suggests that hypoalbuminemia may still influence vancomycin exposure in several ways. External reviews and mechanistic discussions have proposed that lower albumin concentrations can alter protein binding, increase the unbound fraction, and make total concentrations harder to interpret, especially in unstable ICU settings.43 Other external studies have also linked hypoalbuminemia to extravascular fluid shifts, net albumin leakage, and third-space expansion, which may increase the apparent volume of distribution of hydrophilic agents during severe infection or aggressive resuscitation.45,46 These external data help explain why albumin remains clinically relevant, but they should be interpreted as supportive rather than definitive in the context of this review.
Studies by Wang and Revilla have found that altered internal homeostasis, fluid imbalance, and severe illness can expand the apparent volume of distribution, but they did not establish albumin as the main driving factor.9,15 Accordingly, this review can only cautiously conclude that hypoalbuminemia may contribute to variability in volume of distribution and to difficulty interpreting total vancomycin concentrations in selected ICU settings, but its role appears less consistent than that of renal function, body weight, or extracorporeal support variables. Clinically, the main implication is not that albumin alone should guide dosing, but that patients with marked hypoalbuminemia and fluid shifts may require closer early TDM and, where available, MIPD-supported individualization to avoid misleading reliance on fixed empirical dosing.
Integration of MIPD Tools and Bayesian Posterior Estimation
As emphasized in both the abstract and conclusion of this review, identifying the main determinants of vancomycin pharmacokinetics in critical illness is ultimately intended to support model-informed precision dosing. Since publication of the 2020 ASHP/IDSA/PIDS/SIDP consensus guideline, vancomycin monitoring has progressively shifted away from simple trough-based adjustment toward an exposure-based strategy targeting an AUC24/MIC of 400–600. This shift is particularly relevant in the ICU, where rapid changes in renal function, fluid balance, and organ support often make single trough concentrations an unstable surrogate for true exposure.47
Within this context, bayesian forecasting has become one of the main technical foundations of MIPD. Rather than relying on a single observed concentration in isolation, bayesian approaches use a population pharmacokinetic model as the prior distribution and then update that model using individual patient covariates and measured drug concentrations to generate posterior exposure estimates that better reflect the patient’s actual clinical state.5 Unlike conventional approaches that usually wait until steady state before using trough measurements for dose adjustment, bayesian methods can integrate one or two early concentration samples, even before steady state is reached, to estimate AUC and predict future concentration trajectories. This has practical value in critically ill patients, in whom disease progression may be rapid and the therapeutic window is narrow.2,5,38
From a clinical perspective, the value of MIPD lies not in replacing clinical judgment, but in improving the timeliness and interpretability of early dosing decisions. Available studies suggest that bayesian posterior estimation can improve prediction of vancomycin exposure and increase the likelihood of achieving target exposure.38,39,48 For example, in a prospective ICU cohort, bayesian posterior estimation reduced prediction error substantially compared with prior-only or rule-based approaches, with RMSE decreasing from 45%–68% to 27%–37%.4,38 These findings suggest that, in critical illness, MIPD can serve as a practical link between population modeling and bedside individualization, especially in patients with rapidly changing renal function or those receiving CRRT or mechanical ventilation, where standard empiric dosing is often inadequate.
Nonetheless, the success of MIPD depends heavily on the suitability of the prior model, the quality of the input data, and the timing of concentration sampling. Bayesian tools do not eliminate model bias. If the prior model is poorly matched to the target population, or if measured concentrations are affected by timing errors, predictive performance may still be compromised.5,48 Future progress in precision dosing for vancomycin in critically ill patients will therefore depend not only on wider use of bayesian software, but also on continued refinement of ICU-specific PopPK models, stronger external validation, and closer integration of early TDM, bedside clinical assessment, and MIPD platforms.2,39,40
Limitations
Several limitations should be acknowledged. This review was limited to English-language studies and to models developed with NONMEM, so relevant vancomycin population pharmacokinetic studies using other platforms or identified through other sources may have been missed. In addition, only 12 studies met the inclusion criteria, and most were single-center retrospective studies with relatively small or selected patient cohorts. The included studies also differed considerably in both clinical setting and methodology, including patient case mix, renal support modality, dosing approach, sampling strategy, structural model, and covariate definition. This degree of heterogeneity makes direct comparison of parameter estimates difficult and does not allow quantitative synthesis. External validation was also uneven across studies, and only a limited number of reports linked model performance to clinically relevant outcomes such as target attainment, efficacy, or nephrotoxicity. For these reasons, the findings of this review should be regarded as a qualitative summary of the current NONMEM-based literature in critically ill adults rather than as support for a single preferred model or dosing algorithm.
Conclusion
This systematic review shows that vancomycin pharmacokinetics vary markedly in critically ill adults, shaped by organ dysfunction and the changing effects of extracorporeal support. The main clinical message is not just that individual covariates matter, but that fixed empiric dosing is often inadequate in ICU patients. Improving target attainment while limiting toxicity will likely require a shift away from traditional trough-based adjustment toward model-informed precision dosing (MIPD). In practice, this means combining pragmatic population models, including simple one-compartment models suitable for sparse data, with early therapeutic drug monitoring and bayesian forecasting at the bedside. At the same time, the current evidence base remains limited by retrospective study designs, small sample sizes, and limited external validation. Future work should therefore focus on larger multicenter prospective datasets, stronger external validation in specific ICU subgroups such as ECMO and continuous renal replacement therapy, and clinical studies testing whether bayesian MIPD improves patient-centered outcomes.
Acknowledgments
During the preparation of this work, the authors used DeepSeek for language polishing and data analysis, and Gemini 3 Pro to generate reference graphical abstracts to enhance logical structure. All AI-generated suggestions were reviewed and revised by the authors, who assume full responsibility for the final content.
Funding
This study was funded by the Science and Technology Planning Project of Guizhou Province (Qianke Science Support [2023] General 382); the Key Laboratory Construction Project of Affiliated Hospital of Guizhou Medical University (Contract No. 2025FYYJ(HX)-004); and the Guizhou Provincial Science and Technology Plan Project (Qiankehe Platform), Grant No. ZSYS[2025]021.
Disclosure
The author(s) report no conflicts of interest in this work.
References
1. Naghavi M, Vollset SE, Ikuta KS, et al. Global burden of bacterial antimicrobial resistance 1990–2021: a systematic analysis with forecasts to 2050. Lancet. 2024;404(10459):1199–16. doi:10.1016/S0140-6736(24)01867-1
2. Rybak MJ, Le J, Lodise TP, et al. Therapeutic monitoring of vancomycin for serious methicillin-resistant Staphylococcus aureus infections: a revised consensus guideline and review by the American Society of Health-System Pharmacists, the Infectious Diseases Society of America, the Pediatric Infectious Diseases Society, and the Society of Infectious Diseases Pharmacists. Am J Health-Syst Pharm. 2020;77(11):835–864. doi:10.1093/ajhp/zxaa036
3. Vincent JL, Sakr Y, Singer M, et al. Prevalence and Outcomes of Infection Among Patients in Intensive Care Units in 2017. JAMA. 2020;323(15):1478. doi:10.1001/jama.2020.2717
4. Narayan SW, Thoma Y, Drennan PG, et al. Predictive performance of Bayesian vancomycin monitoring in the critically ill. Crit Care Med. 2021;49(10):e952–e960. doi:10.1097/CCM.0000000000005062
5. Alnezary FS, Almutairi MS, Gonzales-Luna AJ, Thabit AK. The significance of Bayesian pharmacokinetics in dosing for critically ill patients: a primer for clinicians using vancomycin as an example. Antibiotics. 2023;12(9):1441. doi:10.3390/antibiotics12091441
6. Cunio CB, Uster DW, Carland JE, et al. Towards precision dosing of vancomycin in critically ill patients: an evaluation of the predictive performance of pharmacometric models in ICU patients. Clin Microbiol Infect. 2021;27(5):
7. National Heart, Lung, and Blood Institute. Study Quality Assessment Tools. 2013. Available from: https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools.
8. Kovacevic T, Miljkovic B, Kovacevic P, et al. Population pharmacokinetic model of vancomycin based on therapeutic drug monitoring data in critically ill septic patients. J Crit Care. 2020;55:116–121. doi:10.1016/j.jcrc.2019.10.012
9. Wang C, Chen J, Yang B, et al. Determination of vancomycin exposure target and individualized dosing recommendations for critically ill patients undergoing continuous renal replacement therapy. Pharmacotherapy. 2023;43(3):180–188. doi:10.1002/phar.2771
10. Vu Dinh H, Nguyen DA, Delattre IK, et al. Determination of optimal loading and maintenance doses for continuous infusion of vancomycin in critically ill patients: population pharmacokinetic modelling and simulations for improved dosing schemes. Int J Antimicrob Agents. 2019;54(6):702–708. doi:10.1016/j.ijantimicag.2019.09.018
11. Bang JY, Kang HI, Lee HJ, et al. Development of a new pharmacokinetic model for target-concentration controlled infusion of vancomycin in critically ill patients. Clin Exp Pharmacol Physiol. 2022;49(2):202–211. doi:10.1111/1440-1681.13597
12. Roberts JA, Taccone FS, Udy AA, Vincent JL, Jacobs F, Lipman J. Vancomycin dosing in critically ill patients: robust methods for improved continuous-infusion regimens. Antimicrob Agents Chemother. 2011;55(6):2704–2709. doi:10.1128/AAC.01708-10
13. Medellín-Garibay SE, Romano-Moreno S, Tejedor-Prado P, et al. Influence of mechanical ventilation on the pharmacokinetics of vancomycin administered by continuous infusion in critically ill patients. Antimicrob Agents Chemother. 2017;61(12):e01249–17. doi:10.1128/AAC.01249-17
14. Escobar L, Andresen M, Downey P, et al. Population pharmacokinetics and dose simulation of vancomycin in critically ill patients during high-volume haemofiltration. Int J Antimicrob Agents. 2014;44(2):163–167. doi:10.1016/j.ijantimicag.2014.03.009
15. Revilla N, Martín-Suárez A, Pérez MP, González FM, A E. Vancomycin dosing assessment in intensive care unit patients based on a population pharmacokinetic/pharmacodynamic simulation. Br J Clin Pharmacol. 2010;70(2):201–212. doi:10.1111/j.1365-2125.2010.03679.x
16. Donadello K, Roberts JA, Cristallini S, Beumier M, A E. Vancomycin population pharmacokinetics during extracorporeal membrane oxygenation therapy: a matched cohort study. Crit Care. 2014;18(6):632. doi:10.1186/s13054-014-0632-8
17. Jalusic KO, Hempel G, Arnemann PH, Spiekermann C, A E. Population pharmacokinetics of vancomycin in patients with external ventricular drain-associated ventriculitis. Br J Clin Pharmacol. 2020;87(6):2502–2510. doi:10.1111/bcp.14657
18. Yu Z, Liu J, Yu H, et al. Population pharmacokinetics and individualized dosing of vancomycin for critically ill patients receiving continuous renal replacement therapy: the role of residual diuresis. Front Pharmacol. 2023;14:1298397. doi:10.3389/fphar.2023.1298397
19. Udy AA, Covajes C, Taccone FS, et al. Can population pharmacokinetic modelling guide vancomycin dosing during continuous renal replacement therapy in critically ill patients? Int J Antimicrob Agents. 2013;41(6):564–568. doi:10.1016/j.ijantimicag.2013.01.018
20. Wieringa A, Smeets TJL, Ter Horst PGJ, et al. How to perform pharmacokinetic research of antimicrobial drugs in critically ill patients undergoing continuous renal replacement therapy: a scoping review of all relevant pharmacokinetic factors. Clin Microbiol Infect. 2025:S1198. doi:10.1016/j.cmi.2025.11.033
21. Yang P, Zhang H, Chen M, et al. Model-informed precision dosing of vancomycin in Chinese adult patients receiving renal replacement therapy: systematic evaluation of published pharmacokinetic models and dosing regimen simulations. Int J Antimicrob Agents. 2025;66(6):107608. doi:10.1016/j.ijantimicag.2025.107608
22. Ullah S, Zoller M, Jaehde U, et al. A model-based approach to assess unstable creatinine clearance in critically ill patients. Clin Pharmacol Ther. 2021;110(5):1240–1249. doi:10.1002/cpt.2341
23. Wansing EMA, Wicha SG, Bannas P, et al. Cystatin C-based eGFR better predicts renal vancomycin clearance than creatinine-based eGFR in patients with allogeneic stem cell transplantation. Clin Pharmacol Ther. 2025;119(3):669–677. doi:10.1002/cpt.70125
24. Yao Y, Zhang L, Chen D, Qin S, Meng M, Guo Q. Global research on the utilization of population pharmacokinetic model: a bibliometric analysis from 2000 to 2024. Front Pharmacol. 2025;16. doi:10.3389/fphar.2025.1548023.
25. Goutelle S, Woillard JB, Buclin T, et al. Parametric and nonparametric methods in population pharmacokinetics: experts’ discussion on use, strengths, and limitations. J Clin Pharmacol. 2022;62(2):158–170. doi:10.1002/jcph.1993
26. Combacte-Net Consortium, De Velde F, De Winter BCM, Neely MN, et al. Population pharmacokinetics of imipenem in critically ill patients: a parametric and nonparametric model converge on CKD-EPI estimated glomerular filtration rate as an impactful covariate. Clin Pharmacokinet. 2020;59(7):885–898. doi:10.1007/s40262-020-00859-1.
27. Bauer RJ, Guzy S, Ng C. A survey of population analysis methods and software for complex pharmacokinetic and pharmacodynamic models with examples. AAPS J. 2007;9(1):E60–E83. doi:10.1208/aapsj0901007
28. Guay DRP, Vance-Bryan K, Gilliland S, Rodvold K, Rotschafer J. Comparison of vancomycin pharmacokinetics in hospitalized elderly and young patients using a Bayesian forecaster. J Clin Pharmacol. 1993;33(10):918–922. doi:10.1002/j.1552-4604.1993.tb01922.x
29. Bourguignon L, Cazaubon Y, Debeurme G, Loue C, Ducher M, Goutelle S. Pharmacokinetics of vancomycin in elderly patients aged over 80 years. Antimicrob Agents Chemother. 2016;60(8):4563–4567. doi:10.1128/aac.00303-16
30. Barber KE, Bell AM, Stover KR, Wagner JL. Intravenous vancomycin dosing in the elderly: a focus on clinical issues and practical application. Drugs Aging. 2016;33(12):845–854. doi:10.1007/s40266-016-0420-z
31. Usman M, Fobker M, Hempel G. Investigation of the age dependency of vancomycin clearance by population pharmacokinetic modeling. Int J Clin Pharmacol Ther. 2018;56(02):56–63. doi:10.5414/cp203033
32. Bilbao-Meseguer I, Rodríguez-Gascón A, Barrasa H, Isla A, Solinís MÁ. Augmented renal clearance in critically ill patients: a systematic review. Clin Pharmacokinet. 2018;57(9):1107–1121. doi:10.1007/s40262-018-0636-7
33. Tesfamariam NS, Aboelezz A, Mahmoud SH. The impact of augmented renal clearance on vancomycin pharmacokinetics and pharmacodynamics in critically ill patients. J Clin Med. 2024;13(8):2317. doi:10.3390/jcm13082317
34. Xi L, Li S, Chen M, et al. Age-related differences in vancomycin-associated nephrotoxicity and efficacy in methicillin-resistant staphylococcus aureus infection: a comparative study between elderly and adult patients. Antibiotics. 2024;13(4):324. doi:10.3390/antibiotics13040324
35. Dai N, Jiang C, Wang Y. Relationship between vancomycin-induced nephrotoxicity and vancomycin trough concentration in older adults: a retrospective observational study. Indian J Pharmacol. 2023;55(3):155–161. doi:10.4103/ijp.ijp_634_22
36. Claisse G, Zufferey PJ, Trone JC, et al. Predicting the dose of vancomycin in ICU patients receiving different types of RRT therapy: a model-based meta-analytic approach. Br J Clin Pharmacol. 2019;85(6):1215–1226. doi:10.1111/bcp.13904
37. Cushway J, Murphy L, Chase JG, Shaw GM, Desaive T. Modelling patient specific cardiopulmonary interactions. Comput Biol Med. 2022;151:106235. doi:10.1016/j.compbiomed.2022.106235
38. Dreyse N, Salazar N, Munita JM, Rello J, López R. Vancomycin levels for Bayesian dose-optimization in critical care: a prospective cohort study. Front Med. 2025;12:1575224. doi:10.3389/fmed.2025.1575224
39. Hall NM, Brown ML, Edwards WS, Oster RA, Cordell W, Stripling J. Model-informed precision dosing improves outcomes in patients receiving vancomycin for gram-positive infections. OPEN Forum Infect Dis. 2024;11(1). doi:10.1093/ofid/ofae002
40. Guo T, Van Hest RM, Roggeveen LF, et al. External evaluation of population pharmacokinetic models of vancomycin in large cohorts of intensive care unit patients. Antimicrob Agents Chemother. 2019;63(5):e02543–18. doi:10.1128/AAC.02543-18
41. Glatard A, Bourguignon L, Jelliffe RW, Maire P, Neely MN, Goutelle S. Influence of renal function estimation on pharmacokinetic modeling of vancomycin in elderly patients. Antimicrob Agents Chemother. 2015;59(6):2986–2994. doi:10.1128/aac.04132-14
42. Martí R, Rosell M, Pou L, García L, Pascual C. Influence of biochemical parameters of liver function on vancomycin pharmacokinetics. Pharmacol Toxicol. 1996;79(2):55–59. doi:10.1111/j.1600-0773.1996.tb00242.x
43. Idasiak-Piechocka I, Lewandowski D, Świgut W, et al. Effect of hypoalbuminemia on drug pharmacokinetics. Front Pharmacol. 2025;16. doi:10.3389/fphar.2025.1546465
44. Hansel J, Mannan F, Robey R, et al. Covariates in population pharmacokinetic studies of critically ill adults receiving beta-lactam antimicrobials: a systematic review and narrative synthesis. JAC-Antimicrob Resist. 2023;6(1). doi:10.1093/jacamr/dlae030
45. Seldén D, Tardif N, Wernerman J, Rooyackers O, Norberg Å. Net albumin leakage in patients in the ICU with suspected sepsis. A prospective analysis using mass balance calculations. Crit Care. 2025;29(1). doi:10.1186/s13054-025-05323-9
46. Katip W, Jaruratanasirikul S, Pattharachayakul S, Wongpoowarak W, Jitsurong A, Lucksiri A. The pharmacokinetics of vancomycin during the initial loading dose in patients with septic shock. Infect Drug Resist. 2016;Volume 9:253–260. doi:10.2147/idr.s121513
47. Tanaka R. Pharmacokinetic variability and significance of therapeutic drug monitoring for broad-spectrum antimicrobials in critically ill patients. J Pharm Health Care Sci. 2025;11(1). doi:10.1186/s40780-025-00425-6
48. Bai G, Qi H, Huang Y, et al. Predictive performance of Bayesian dosing software for vancomycin in intensive care unit patients. Ther Drug Monit. 2025;47(5):594–602. doi:10.1097/ftd.0000000000001310
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.