Back to Journals » Journal of Multidisciplinary Healthcare » Volume 19
Poor Sleep Quality Associated with Impaired Postoperative Outcomes and Frailty Incidence in Elderly Patients After Total Hip Arthroplasty: A Severity Matched Case-Control Study
Authors Zhao L, Wu H, Wu Z, Li FY, Yan JF ![]()
Received 6 August 2025
Accepted for publication 9 January 2026
Published 15 May 2026 Volume 2026:19 558926
DOI https://doi.org/10.2147/JMDH.S558926
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Charles V Pollack
Le Zhao,1,* Haoran Wu,2,* Zhen Wu,3 Feng-Ying Li,4 Jian-Feng Yan1
1Department of Orthopedics, Affiliated Changshu Hospital to Nantong University, Changshu No. 2 People’s Hospital, Changshu, Jiangsu, People’s Republic of China; 2School of Medicine, Tongji University, Shanghai, People’s Republic of China; 3Department of Ear, Nose, and Throat, Affiliated Changshu Hospital to Nantong University, Changshu No. 2 People’s Hospital, Changshu, Jiangsu, People’s Republic of China; 4The First Hospital of Nanchang, Nanchang, Jiangxi, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jian-Feng Yan, Email [email protected]
Objective: This study aimed to assess the effect of preoperative sleep quality on postoperative pain, functional recovery, and weakness in THA patients and explore its interaction with other health issues.
Methods: This retrospective case-control study included 90 patients (45 with poor sleep PSQI> 5 and 45 with good sleep PSQI≤ 5) matched by age, sex, and the American Society of Anesthesiologists (ASA) classification. Data on sleep, hip function, pain, anxiety/depression, and weakness were collected preoperatively and 6 months postoperatively. Multiple logistic regression was used to analyze the postoperative frailty risk factors, adjusting for age, body mass index (BMI), diabetes, and osteoporosis history, with ORs and 95% CIs.
Results: Patients with poor preoperative sleep quality demonstrated significantly longer hospital stays (4.79± 1.47 vs 3.42± 0.89 days, P< 0.001) and higher pain scores at 3 months postoperatively (visual analog scale [VAS] 3.13± 1.04 vs 1.87± 0.87, P< 0.001). Multivariate analysis identified preoperative poor sleep as an independent predictor of postoperative frailty (OR=2.44, 95% CI 0.97– 4.20, P=0.002), along with age ≥ 65 years (OR=11.29) and osteoporosis history (OR=2.06). Two-way ANOVA revealed significant group-time interactions in PSQI scores (P< 0.001). While both groups showed postoperative PSQI improvement (poor sleep: 11.89± 2.92 to 6.56± 2.39; good sleep: 3.31± 1.57 to 2.29± 1.14), between-group differences remained significant (P< 0.001).
Conclusion: Poor preoperative sleep quality was associated with a higher risk of pain and frailty after THA, possibly due to a two-way relationship. Although this study has some limitations, preoperative sleep screening could be useful in improving perioperative care and requires further testing in future studies.
Keywords: sleep quality, THA, postoperative pain, frailty, frailty index
Introduction
THA surgery is rising due to aging populations and increasing osteoarthritis prevalence. By 2030, annual THA surgeries are expected to surge by 174% from 2005, with the US reaching 572,000 cases/year and Europe about 400,000 cases/year.1 Osteoarthritis is the most common indication for THA (70–80% of cases), followed by osteonecrosis of the femoral head (10–15%) and post-traumatic arthritis (5–10%).2 This increase is not only reflected in the volume of procedures but also carries a heavy economic burden: the direct medical cost of a single THA in the United States is as high as $48,000, and readmission for postoperative complications (eg, infections, loosening) costs an additional $23,000 per case.3 As one of the countries with the fastest aging populations, the demand for THA has risen dramatically in China. According to the National Joint Replacement Registry, the annual number of THA surgeries in China has increased from 45,000 in 2013 to 287,000 in 2020, with a compound annual growth rate of 30%.4 Among them, Femoral head necrosis (35–40%) and osteoarthritis (30–35%) are the main indications, which are significantly higher than the distribution of the disease spectrum in Western countries.5 Delayed diagnosis and treatment lead to a higher proportion (60%) of advanced hip pathology in rural areas compared to urban ones (30%), indicating unequal healthcare resources worsen surgical complexity and postoperative recovery challenges.6 THA improves patient function, but postoperative frailty incidence (15–25%) causes delayed recovery, readmission risk, and higher costs.7 Existing studies mainly focus on surgical techniques or short-term complications, with the link between preoperative factors (such as sleep quality) and postoperative frailty underexplored. Given THA’s growth and China’s unique disease profile, identifying preoperative risk markers and interventions is vital for public health.
According to a study, approximately 1.361 billion people worldwide suffer from sleep disorders, especially in men, older adults, and those with an elevated body mass index.8 Sleep disorders in surgical patients complicate perioperative care, linked to postoperative hypoxemia, pulmonary/cardiac issues, ICU transfers, longer stays, higher readmission rates, and increased resource use.9 Patients undergoing orthopedic surgery exhibit a higher prevalence of sleep disorders than those undergoing general surgery,10 and several studies have shown that sleep disorders adversely affect morbidity and mortality in the orthopedic population.10–14 Larsen et al studied sleep quality and chronic pain, while this study is the first to use a multidimensional assessment of postoperative frailty over 6 months to track its dynamic changes. Unlike Larsen et al’s Western-based study, this one focuses on elderly Chinese THA patients with unique sleep and comorbidity patterns, offering Asian-relevant evidence. Though Larsen et al’s RCT-based design was rigorous, it did not prioritize frailty as a geriatric surgical outcome. This study’s novelty lies in linking sleep quality to postoperative frailty risk and providing non-Western perioperative management evidence. Recent studies also show sleep quality affects postoperative pain and recovery in the elderly, with sleep-disordered THA patients facing longer stays, higher costs, pain rates, and complication risks.13,15,16 Therefore, it is crucial to perform early risk prediction focusing on older patients with preoperative sleep disorders.
Frailty, marked by reduced physiological reserves and stress resistance, presents as poor mobility, muscle loss, poor nutrition, and cognitive decline, and is a key risk factor for postoperative complications in older adults. The Fried frailty phenotype and clinical frailty scale, well validated in research and clinical practice,17 are commonly used tools for frailty assessment. Traditionally, frailty is seen as chronic and cumulative, but recent studies suggest “postoperative acquired frailty”, where surgical stress may rapidly worsen frailty, especially in the elderly.18 Petermann-Rocha et al (2023) found the Fried score rose by 1.5 items on average 6 months post major orthopedic surgery, correlating with preoperative inflammatory markers (such as IL-6).19 In this study, the increase in ΔFried=1.8 is consistent with this, supporting the clinical significance of short-term changes in postoperative frailty. Studies have shown that individuals with sleep disorders are at a higher risk of developing frailty.20 Sleep quality is assessed using the Pittsburgh Sleep Quality Index (PSQI). A PSQI total score exceeding 5 points is commonly employed as the clinical cut-off point distinguishing “good sleep quality” from “poor sleep quality”. This criterion is widely adopted globally and has demonstrated good reliability and validity across multiple studies.21 Although many studies have confirmed the association between sleep disorders and frailty in the elderly population, the dynamic evolution of this relationship in the orthopedic postoperative population and its clinical significance have not been fully explored. Patients undergoing total hip replacement (THA) may experience unique sleep-weakness interactions due to pain, limited mobility, and perioperative stress. However, the effect of sleep quality on the incidence of frailty after THA remains unclear. This study investigated the potential association between sleep quality and postoperative outcomes in older THA patients, and screened for risk factors associated with postoperative THA frailty.
Methods
Study Design and Population
This is a single-center, retrospective case-control study, non-randomised intervention trial. The case group included THA patients with poor sleep quality (PSQI>5 points) before surgery (n=45) and the good sleep quality group included patients with PSQI≤5 points (n=45). All patients underwent their first unilateral THA at our center between 2018 and 2022. The study was approved by the Medical Ethics Committee of Changshu No. 2 People’s Hospital (Ethics No. 2021-KYW-070; December 21, 2021), and written informed consent was obtained from all subjects participating in the trial. The study protocol was in compliance with the ethical guidelines of the Declaration of Helsinki. Adult patients undergoing selective THA at Changshu No. 2 Hospital were selected for this study, and patient eligibility was assessed at the pre-admission hospital visit before admission for surgery, with a 6-month postoperative follow-up. A total of 239 hospitalized THA patients were screened using the inclusion criteria shown in Figure 1. The exclusion criteria were as follows: 1. History of Drug Dependence. (1) Current or past 12 months meeting DSM-5 diagnostic criteria for substance use disorders (eg, opioid, benzodiazepine dependence) and (2) a history of illicit drug use (eg, cocaine, methamphetamine) or over-the-counter substance abuse within 6 months prior to surgery. Drug dependence status was assessed using a combination of the Structured Clinical Interview (SCID-5) and urine toxicology screening (within 48 h preoperatively); 2. History of previous THA surgery, 3. Other pain treatments outside standard care; and 4. BMI > 40 kg/m2; 5. Inability to understand or cooperate in the evaluation of the scales or questionnaires used in this study. During the follow-up period of this study, all 90 enrolled patients completed the six-month postoperative assessment with no cases lost to follow-up; consequently, there were no issues requiring missing data imputation. All patients were screened and included based on existing medical records after surgery.
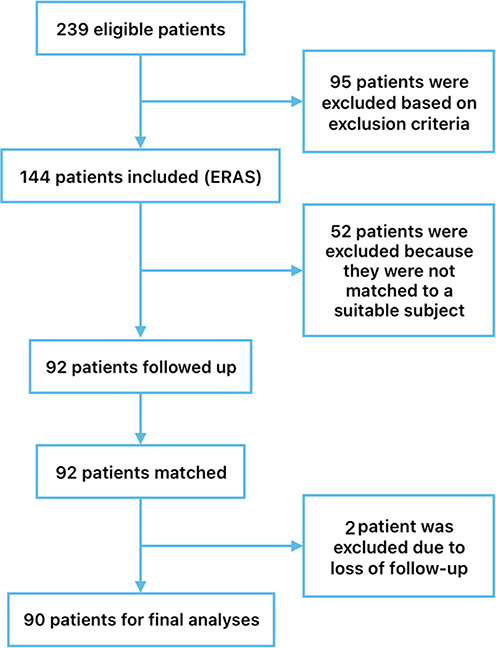 |
Figure 1 Flowchart for data incorporation. |
Patients with good and poor sleep quality were then included according to the PSQI and randomly selected and used as matched controls according to age at surgery (within 2 years), sex (corresponding match), and concordance with the American Society of Anesthesiologists (ASA) scores. If one of the matched controls was lost to follow-up, the patient was excluded. This study was approved by the Medical Ethics Committee and complied with the Declaration of Helsinki.
Data Collection and Definitions
Basic data on demographics, clinical characteristics, sleep quality (Pittsburgh Sleep Quality Index [PSQI]), ASA scores, HHS scores, and pain intensity (visual analog scale [VAS]) were collected by a professional staff. The HHS is a standardized tool widely used in the assessment of hip function and was proposed by Harris in 1969 to quantify pain, functional status, and mobility after hip surgery. Demographics included age, sex, and body mass index (BMI), which was calculated by dividing weight (kg) by height (m2). Hypertension was defined as a self-reported history of hypertension, current use of antihypertensive medication, or three or more consecutive measurements of diastolic blood pressure (BP) ≥90 mmHg and/or systolic BP ≥140 mmHg.22 History of diabetes, cardiovascular disease, osteoporosis, and chronic lung disease was obtained from self-report or clinical records. After surgery, the patients returned to the orthopedic wards with a standardized postoperative care and physical therapy program provided to both groups. Clinical data related to surgery were collected, including operative time, blood loss, intraoperative complications, use of postoperative analgesic medications (eg, analgesic pumps and opioids), hospitalization duration, and postoperative VAS pain intensity at 1 d. Patients were contacted by telephone at 1, 3, and 6 months postoperatively to record their HHS scores and VAS pain intensity. The occurrence of complications within 30 days of surgery, PSQI scores, anxiety and depression scores, and frailty status were collected using the same method six months after surgery. Different assessment frequencies are designed because multiple assessment tools (PSQI, VAS, HHS) capture dynamic changes: PSQI observes long-term sleep quality improvement post-surgery; VAS and HSS evaluate early postoperative recovery, hence intensive early follow-ups. Single-time postoperative tools (eg, Fried Frailty Phenotype) focus on cumulative incidence at six months, reflecting the overall state post-surgery. HADS serves as an endpoint for psychological status, aligned with primary outcomes to analyze its link with frailty. Single-time preoperative tools (MoCA, medical history) describe baseline and exclude severe confounders, crucial for grouping and adjusting covariates.
Sleep Quality
Preoperative sleep disorders were assessed using the PSQI, a globally recognized and widely used sleep questionnaire that accurately reflects the quality of a participant’s sleep over a 1-month period.23 The PSQI, with a total score of 21, measures 7 dimensions of sleep quality through 19 question items, including subjective sleep quality, sleep latency, sleep duration, sleep efficiency, sleep disorders, use of sleep medicine, and daytime dysfunction. Higher PSQI scores indicate poorer sleep quality, with a threshold of 5, which means that a PSQI score higher than 5 can be used to indicate the risk of having a preoperative sleep disorder.
Assessment of Postoperative Frailty
Postoperative frailty was evaluated using two methods. The frailty phenotype FP possesses five indicators: weight loss, fatigue, slowed walking speed, low grip strength, and decreased physical activity. Compliance with three or more phenotypes was considered frailty, 1–2 phenotypes as pre-frailty, and 0 as non-frailty.24,25 The Clinical Frailty Scale (CSF) consists of a 9-point scale in which patients are rated based on their functional ability, level of motor activity, and comorbid symptoms, with a score of 1 denoting very healthy (characterized as robust, active, energetic, and motivated), and a score of 9 indicating severe frailty (characterized as being completely dependent on others for daily living or suffering from a terminal illness).26
Anxiety and Depression
The Anxiety and Depression Scale (HADS) is recommended by the National Institute for Health and Clinical Excellence for the diagnosis of depression and anxiety in the United Kingdom27 and is used to determine preoperative levels of anxiety and depression. The scale is composed of 14 questions, with seven items assessing anxiety and seven evaluating depression. Each item was rated from 0 to 3 and summed to obtain separate scores for anxiety and depression.28
Measurement of Pain Intensity
Clinical pain intensity was defined as pain after 20 minutes of rest and was rated using a visual analog scale (VAS: 0–10 cm). Clinical pain intensity data were obtained at 1 d, 1 month, 3 months, and 6 months postoperatively. VAS scores ranged from 0 to 10, where 0 denoted no pain, 0–4 mild pain, and 4–10 indicated worst pain.29
Statistical Analysis
In this study, normality was tested using the Shapiro–Wilk test, Q-Q plots, and the Kolmogorov–Smirnov test, and descriptive statistics for normally distributed variables were expressed as mean ± standard deviation for non-normally distributed variables as median (interquartile spacing), and categorical variables as frequency (percentage); group comparison tests, such as the independent samples t-test, Mann–Whitney U-test, chi-square test, Fisher’s exact test, one-way ANOVA, Kruskal–Wallis H-test, paired t-test, and paired Wilcoxon signed-rank test; regression analyses using multiple logistic regressions and linear regressions to explore the relationship between risk factors and variables; assessment of the model through the AUC of the ROC curve, calculation of the VIF to avoid multicollinearity, Box-Cox transformation of continuous variables to satisfy the assumptions of linearity and normality, and optimization of the logistic regression model using penalized maximum likelihood estimation (and bootstrap resampling to validate the robustness of the model. Statistical significance was defined as p < 0.05.
Although previous studies have reported the effect of sleep quality on THA, the sample size was not sufficiently large. In this project, based on the study by Boye Larsen et al11 the preoperative anxiety data were selected and tested using the PASS software, with α value set as 0.05, β value (1-power) set as 0.2, and the ratio of the sample size of the experimental and good sleep quality groups was 1. The sample size of the experimental group was obtained using the R language according to the method of Chow et al30 which resulted in a sample size of 36 cases for the two groups. Considering the 20% loss to follow-up rate, 90 patients (45 in each group) were included, ensuring that an effect size of OR≥3.0 could be detected.
Baseline Clinical Characteristics
The MoCA score was assessed preoperatively and served as a core indicator of the patient’s preoperative cognitive status, ranging from 0 to 30 points, with scores below the threshold corresponding to the level of education indicating the presence of cognitive impairment. Assessments were completed by two independent researchers and arbitrated by a third neurologist when the difference in scores was greater than 2 points.
Results
Basic Characteristics
A total of 90 eligible THA surgical patients were enrolled and divided into two groups based on their Polysomnography Quality Index (PSQI) scores: a good sleep quality group (higher PSQI score) and a poor sleep quality group (lower PSQI score). The PSQI score in the poor sleep quality group was 11.89 ± 2.92, while the PSQI score in the good sleep quality group was 3.31 ± 1.57. The two groups were comparable in age, sex, ASA score, BMI, HHS score, and history of systemic diseases (P > 0.05). There was no significant difference in preoperative frailty scores between the two groups (P = 0.259). All patients had normal preoperative MoCA scores, with no significant difference between the two groups. Table 1 summarizes the detailed preoperative data of all THA patients.
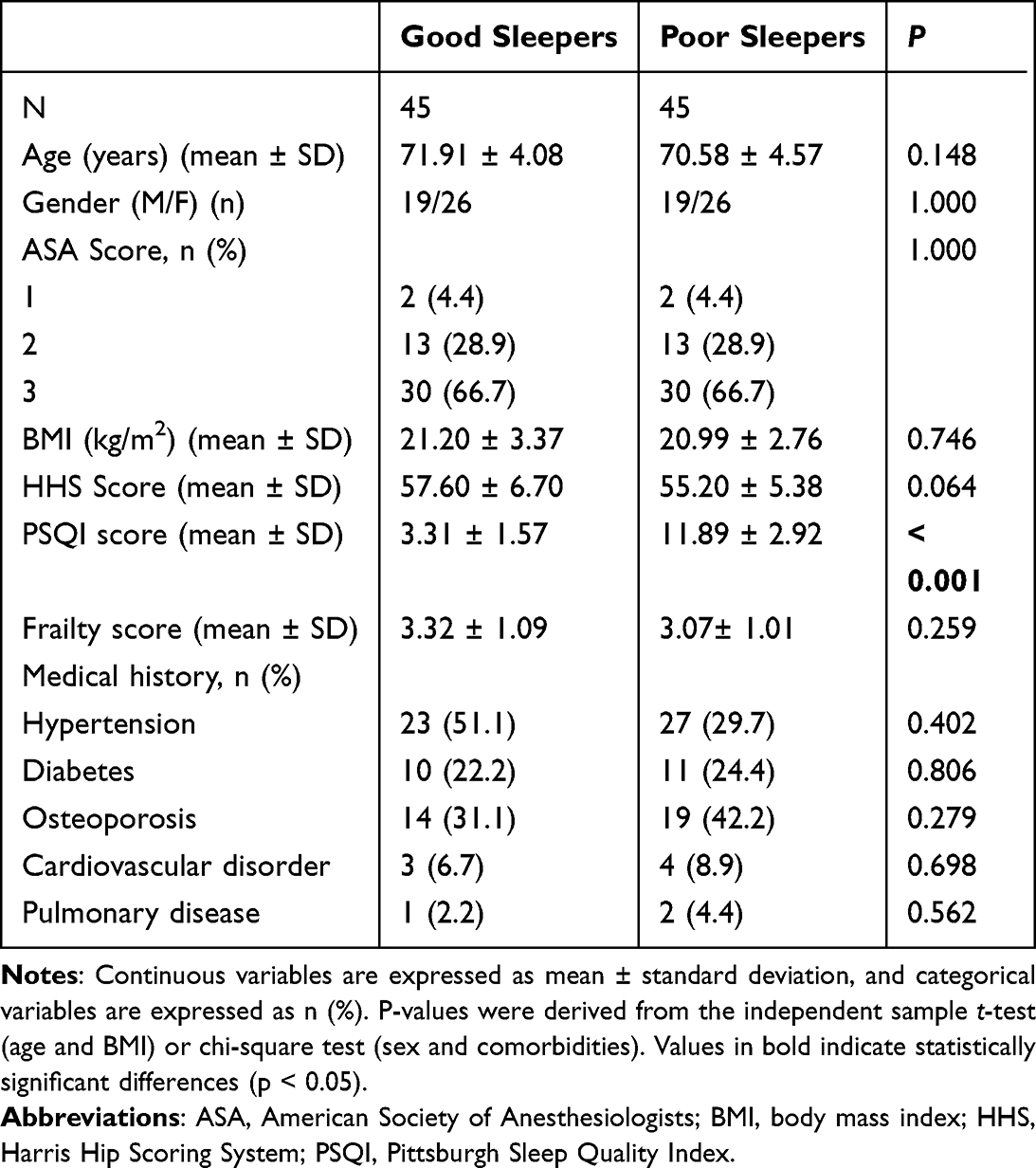 |
Table 1 Comparison of Basic Data on Patient Demographics and Clinical Characteristics Based on Sleep Quality |
Intergroup Comparison of Postoperative Opioid Utilisation Rates and Length of Hospital Stay
Although there was no significant difference in operative time (115.04 ± 16.66 vs. 116.44 ± 13.05 minutes, P = 0.658) and no difference in the rate of postoperative complications (22.2% vs. 8.9%, P = 0.083), there was a significant increase in the rate of opioid use in the poor sleep group (22.2% vs. 6.7%, P = 0.036) and a longer hospital stays (4.49 ± 1.47 vs. 3.42 ± 0.89 days, P < 0.001) (Table 2).
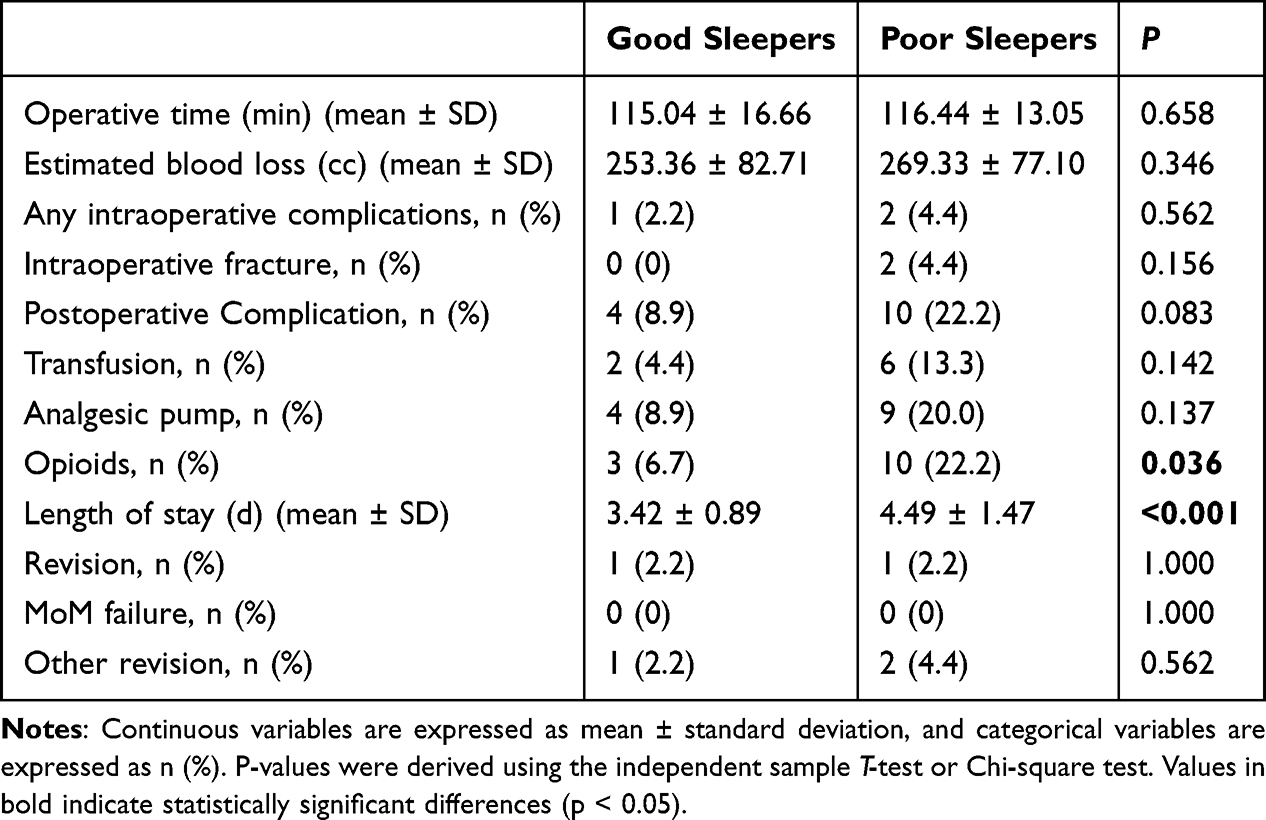 |
Table 2 Surgical Details, Hospital Outcomes and Complications (Short-Term and at 6 Months Post-Operatively) |
The Relationship Between Sleep Quality and Postoperative Pain, Functional Recovery, and Complications
Postoperative pain intensity was significantly higher in the group with poor sleep quality than in the group with good sleep quality at 1 d, 1 month, and 3 months postoperatively (with statistical differences), while tending toward convergence at six months postoperatively (Figure 2). The HHS scores of the two groups were not statistically different preoperatively, whereas the group with poor sleep quality was statistically higher than that of the group with good sleep quality one month after surgery. At 3 and 6 months postoperatively, no statistically significant difference was observed in the HHS scores between the two groups (Figure 3). Six months postoperatively, there was no difference in the prosthesis revision rate between the two groups (2.2% vs. 2.2%, P = 1.000), and the incidence of other complications (eg, aseptic loosening and infection) was similar (Table 2).
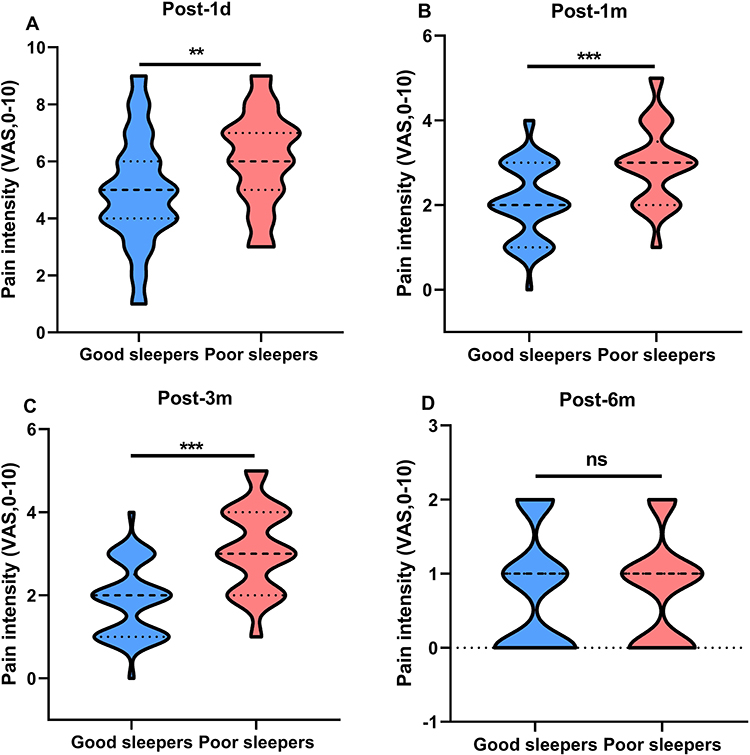 |
Figure 2 Comparison of pain intensity at 1 day, 1 month, 3 months and 6 months postoperatively according to sleep quality. Blue is the good sleep group, red is the poor sleep group. (A) preoperative; (B) post-1 month; (C) post-3 month; (D) post-6 month. ns indicates no significance; **P<0.01; ***P<0.001. |
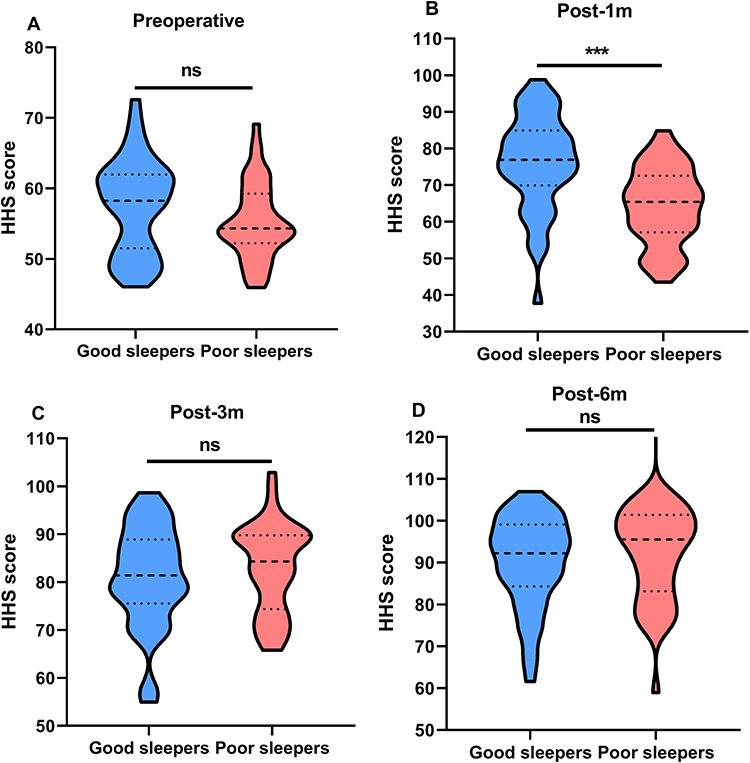 |
Figure 3 Comparison of HHS scores preoperatively, 1 month, 3 months and 6 months postoperatively according to sleep quality. (A) preoperative; (B) post-1 month; (C) post-3 month; (D) post-6 month. ns indicates no significance; ***P<0.001. |
The Impact of Sleep Quality on Postoperative Fatigue, Anxiety and Depression
The PSQI indices of both groups improved preoperatively and six months postoperatively, with a statistically significant difference (Figure 4). It could be observed that the PSQI indices of the poor sleep quality group decreased significantly postoperatively but remained lower than those of the good sleep quality group (Table 3). The incidence of frailty at 6 months after surgery was significantly higher in the poor sleep quality group than in the good sleep quality group (44.4% vs. 24.4%, p=0.024), and the Fried phenotypic score was higher (3.49±1.62 vs. 2.31±1.39, P<0.001). There were also significant differences in the rates of anxiety (HDS-A ≥8 score: 42.2% vs. 17.8%, p=0.009) and depression (HDS-D ≥8 score: 35.6% vs. 13.3%, P=0.011). At 3 months after surgery, the HADS-A score decreased less in the poor sleep group (ΔHADS-A=1.2±0.8 vs. 2.5±1.1, p=0.002), suggesting a delayed recovery of mental health.
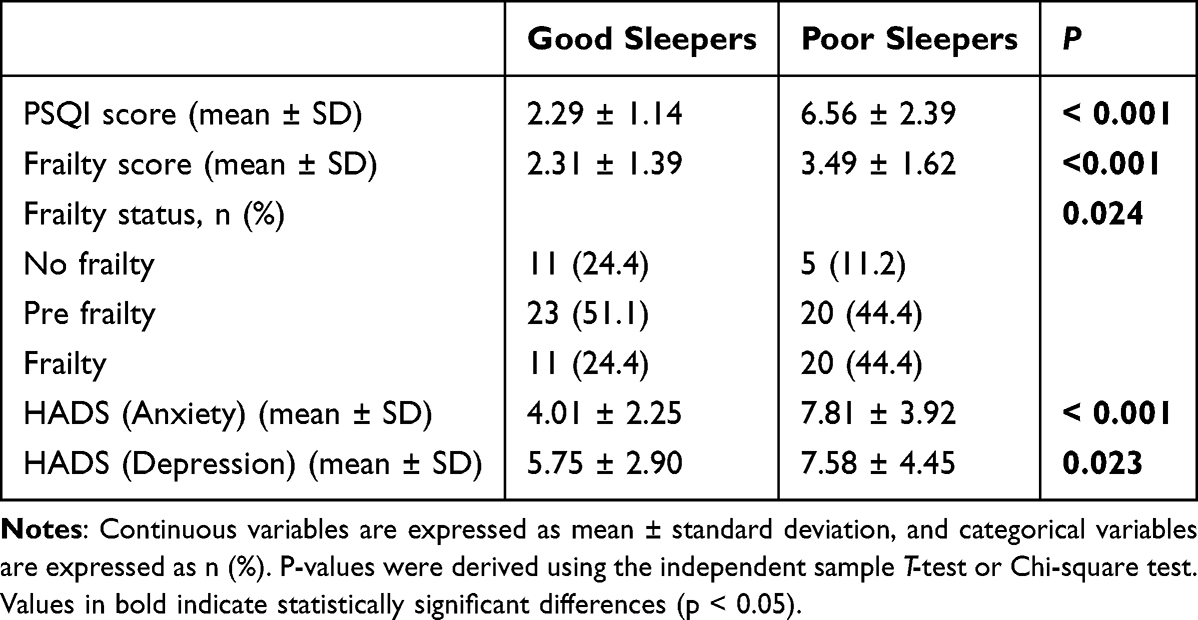 |
Table 3 PSQI Index, Frailty Status and Anxiety and Depression Index in Patients at 6 Months Postoperatively |
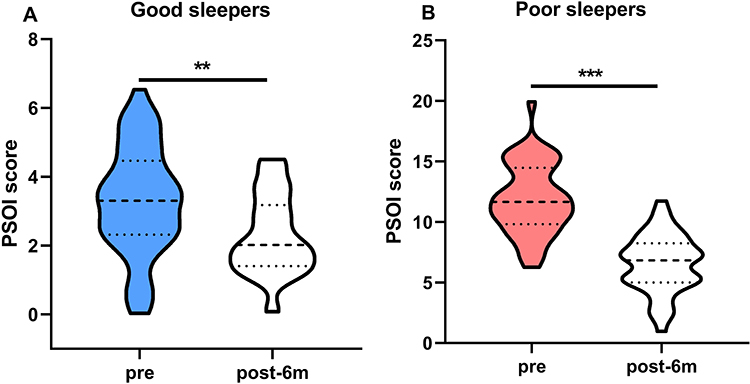 |
Figure 4 Comparison of changes in PSQI scores preoperatively and at 6 months postoperatively between groups. (A) good sleepers; (B) poor sleepers. **P<0.01; ***P<0.001. |
Screening and Multivariate Analysis of Factors Influencing Postoperative Frailty
Screening for factors influencing the prognosis of weakness six months after THA revealed that age, BMI, poor sleep quality, history of diabetes mellitus, and history of osteoporosis had potential influences on the occurrence of weakness six months after surgery (P<0.05, Table 4). Multiple logistic regression modeling of indicators with significant differences showed that poor sleep quality was an independent risk factor for poor prognosis of frailty in patients undergoing THA surgery, with a significant correlation with the primary outcome (OR=2.44, 95% CI: 0.97–4.20, p = 0.002) (Table 5).
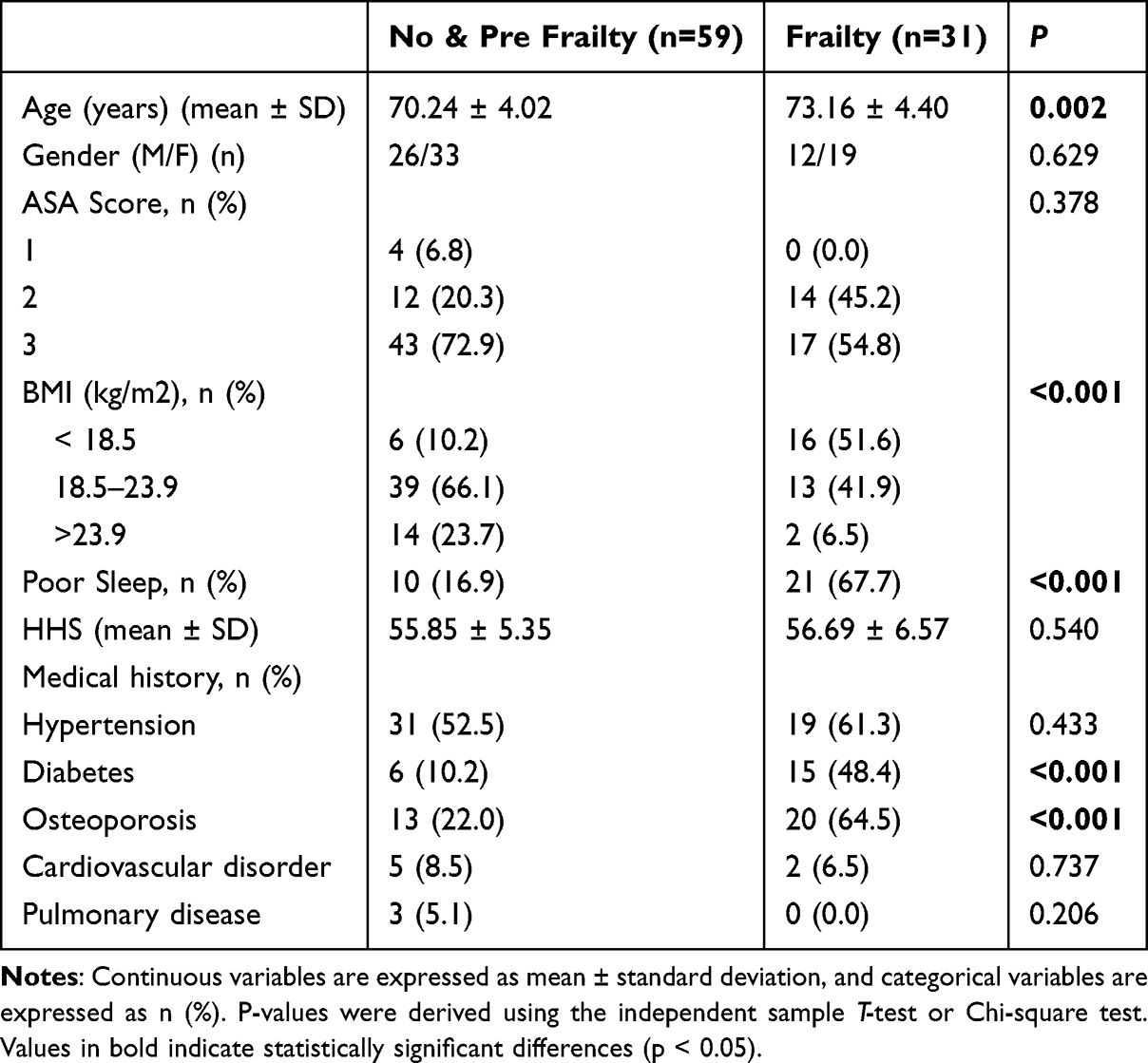 |
Table 4 Comparison of Baseline Characteristics Among Patients Grouped According to Frailty Status at 6 Months Post-Surgery |
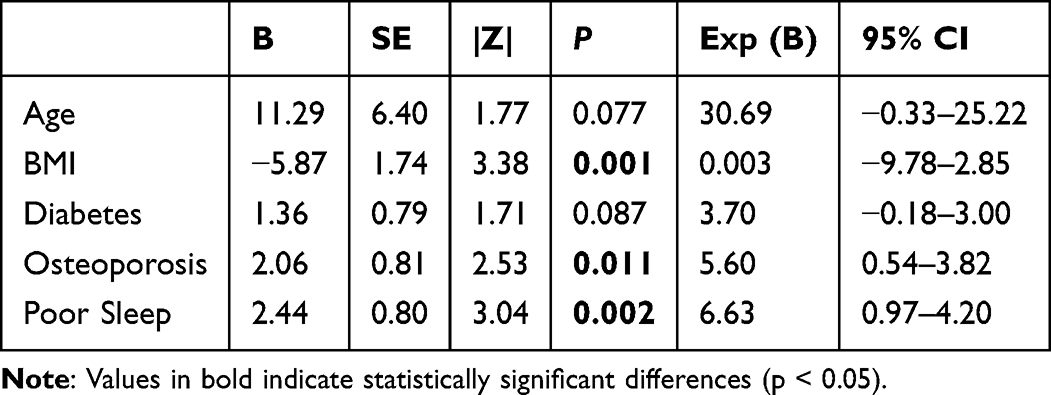 |
Table 5 Multivariate Logistic Regression Analysis of Independent Risk Factors for Frailty in Patients with THA 6 Months After Surgery |
Discussion
After adjusting for available confounders, preoperative poor sleep quality was significantly associated with a higher incidence of frailty at 6 months postoperatively. Risks included age, diabetes/osteoporosis, low BMI, and poor sleep (which independently affected frailty). THA improved outcomes. Identifying frailty factors after THA can guide both preoperative and intraoperative care. Several studies have demonstrated that age is one of the most important risk factors for poor prognosis. David’s study showed that one year after THA, younger patients (<55 years) had slightly worse pain/quality of life but better function, improving more than older patients (≥75 years) who maintained higher function. Age did not affect baseline function but predicted 1-year postoperative pain.31,32 However, no statistically significant differences were observed in the clinical data. Notably, older THA patients (median age = 82.5 years) with severe comorbidities (Charlson score ≥5) had a higher risk of postoperative mortality.33 Similarly, multivariate logistic regression analysis showed that age was significantly different between the postoperative frailty and non-frailty groups.
A history of diabetes and osteoporosis strongly affects THA prognosis. Hyperglycemia weakens immunity and microangiopathy delays wound healing in patients with diabetes. A meta-analysis of 3.5M+ hip arthroplasty cases linked diabetes to a 64% higher risk of periprosthetic joint infection post-THA.34 The WHO and CDC have highlighted strict glycemic control during surgery. Uncontrolled diabetes (blood glucose level >200 mg/dL or hemoglobin A1c level >7%) increases the risk of postoperative complications. The ADA advises delaying surgery for patients with Hgb A1c >7%.35 A recent study investigating 2.5 million patients demonstrated that age (older than 75), diabetes, and osteoporosis were clinical risks leading to postoperative THA fractures with higher mortality.36 Another study investigating 927 THA patients using univariate and multivariate logistic regression analyses showed that lower BMI and a history of osteoporosis were risk factors for anemia after THA.37 Furthermore, inflammatory markers (CRP) and increased blood coagulation (factor VIII and D-dimer) are associated with frailty.38 Examinations have found that the risk of frailty is highest at the lowest hemoglobin levels and lowest at moderate-to-normal hemoglobin levels, suggesting anemia as a risk factor for frailty.39 Consistent with our study, diabetes, history of osteoporosis, and lower BMI represent potential hazard factors that lead to adverse postoperative frailty.
Patients with poor preoperative sleep quality were associated with poorer postoperative recovery in patients with THA, and sleep disorders were linked to higher pain sensitivity, which correlated with poorer postoperative pain control and adverse effects on pain control six months postoperatively. Boye et al11 investigated 163 patients who underwent total joint replacement and showed that preoperative sleep disorders were associated with higher levels of preoperative anxiety and depression, inducing higher levels of postoperative pain. A study of 604 total joint replacement patients found that better preoperative sleep quality correlated with a higher likelihood of discharge within two days.12 Our findings suggest an association between poor preoperative sleep and post-THA frailty, independent of age, BMI, and specific comorbidities. Additionally, frailty is an independent risk factor for frailty. However, the connection between preoperative sleep and postoperative mental health is unclear because a smaller study found no association with anxiety or depression.40
Although frailty is often linked to aging, its definition is complex and variable. The absence of a widely accepted clinical definition complicates the understanding of its implications.41 Indeed, a relatively large number of patients undergoing THA present with frailty according to this definition. McIsaac et al42 concluded that frailty is one of the strongest risk factors for serious short-term adverse events after THA. Serious adverse events in these patients include heart attack, pneumonia, sepsis/shock, surgical bleeding, and pulmonary embolism. Research shows frailty is consistently tied to higher risks of illness, readmission, and death.39,43–45 Common frailty models (eg, Frailty Phenotype, Frailty Index) use similar methods; therefore, their accuracy in predicting surgical outcomes does not differ much.46 Sleep deprivation reduces exercise motivation and fatigue tolerance by altering brain chemistry and mitochondrial function, whereas chronic sleep disruption causes inflammation and muscle breakdown, and weakens physical abilities. We assessed 6-month postoperative frailty using validated scales (Frailty Phenotype, Clinical Frailty Scale).47
Preoperative sleep can predict postoperative frailty, yet frailty factors such as preoperative pain, activity limitations, and anxiety may also disrupt sleep. Postoperatively, surgical stress further impairs sleep; deteriorating sleep in turn hinders recovery and exacerbates frailty, creating a vicious cycle. Future longitudinal studies are required to unravel this complex relationship. This study offers clear clinical implications: incorporating sleep quality screening into routine preoperative assessment for total hip arthroplasty (THA) can identify high-risk patients. Implementing a multimodal prehabilitation programme—integrating sleep interventions alongside physical training and nutritional support—may break this vicious cycle. Optimising preoperative sleep could reduce postoperative frailty incidence and improve long-term outcomes. Given the increasing number of hip osteoarthritis cases and THA expenses, identifying the risk factors for poor recovery after THA is vital. This helps tailor care to improve outcomes and reduce readmission and cost. Based on these findings, it is necessary to conduct prospective interventional studies in the next phase, such as designing a randomised controlled trial to verify whether optimising preoperative sleep in total hip arthroplasty patients can effectively reduce the incidence of postoperative frailty and improve long-term functional outcomes.
Limitations
Our matched retrospective study, being non-interventional, risks incomplete data and has limited generalizability due to its small, single-center sample. Due to the limitations of the retrospective study design, we were unable to obtain and match patients’ preoperative baseline frailty status and anxiety/depression scores. While rigorous matching minimized confounding, multicenter, large-sample studies are needed to validate these findings across diverse populations.
A more refined matching scheme should address incomplete confounders such as the HHS index and BMI. The lack of preoperative assessments of anxiety, depression, frailty, and mental health status in our study may obscure the full impact of sleep disorders on recovery. Preoperative anxiety or depression can indirectly affect postoperative outcomes through sleep quality.
Future studies should comprehensively assess preoperative frailty and mental health in order to accurately gauge the independent effects of sleep quality on recovery. Given the limitations of the retrospective design, prospective studies with thorough baseline assessments are essential to optimize matching and reduce the bias from unmeasured variables.
Conclusion
This novel assessment (combining laboratory data, biomarkers and frailty scores) enables rapid evaluation of short-term risk in elderly total hip arthroplasty patients, facilitating swifter and more precise clinical decision-making. Elderly hip replacement patients with poor sleep quality constitute a frail population. THA improves sleep quality Identifying poor sleepers before surgery helps doctors to predict recovery and plan care.
Abbreviations
THA, total hip arthroplasty; ASA, the American Society of Anesthesiologists; BMI, body mass index; HHS, Harris Hip Scoring System; PSQI, Pittsburgh Sleep Quality Index; HADS, Anxiety and Depression Scale; VAS, Visual Analog Scale.
Data Sharing Statement
Data supporting the findings of this study are available from the corresponding author upon reasonable request.
Ethics Approval and Consent to Participate
The study protocol was approved by the Medical Ethics Committee of Changshu No. 2 People’s Hospital (Ethics No. 2021-KYW-070; December 21, 2021), and written informed consent was obtained from all subjects participating in the trial. The study protocol was in compliance with the ethical guidelines of the Declaration of Helsinki.
Acknowledgments
Le Zhao and Haoran Wu are co-first authors for this study. This paper has been uploaded to researchsquare as a preprint: https://www.researchsquare.com/article/rs-5377617/v1.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Kurtz S, Ong K, Lau E, Mowat F, Halpern M. Projections of primary and revision hip and knee arthroplasty in the United States from 2005 to 2030. J Bone Joint Surg. 2007;89(4):780–13. doi:10.2106/jbjs.F.00222
2. Dale H, Fenstad AM, Hallan G, et al. Increasing risk of revision due to infection after primary total hip arthroplasty: results from the nordic arthroplasty register association. Acta Orthopaedica. 2023;94:307–315. doi:10.2340/17453674.2023.13648
3. Maradit Kremers H, Larson DR, Crowson CS, et al. Prevalence of total hip and knee replacement in the United States. J Bone Joint Surg. 2015;97(17):1386–1397. doi:10.2106/jbjs.N.01141
4. Springer BD, Levine BR, Golladay GJ. Highlights of the 2020 American joint replacement registry annual report. Arthroplasty Today. 2021;9:141–142. doi:10.1016/j.artd.2021.06.004
5. Kang W, Yu J, Liang C, et al. Epidemiology and association rules analysis for pulmonary tuberculosis cases with extrapulmonary tuberculosis from age and gender perspective: a large-scale retrospective multicenter observational study in China. Int J Clin Pract. 2023;2023:1–8. doi:10.1155/2023/5562495
6. Hinman A, Chang R, Royse KE, Navarro R, Paxton E, Okike K. Utilization of total joint arthroplasty by rural-urban designation in patients with osteoarthritis in a universal coverage system. J Arthroplasty. 2023;38(12):2541–2548. doi:10.1016/j.arth.2023.08.030
7. Shaw JF, Budiansky D, Sharif F, McIsaac DI. The association of frailty with outcomes after cancer surgery: a systematic review and metaanalysis. Ann Surg Oncol. 2022;29(8):4690–4704. doi:10.1245/s10434-021-11321-2
8. Nagano A, Wakabayashi H, Maeda K, et al. Respiratory sarcopenia and sarcopenic respiratory disability: concepts, diagnosis, and treatment. J Nutr Health Aging. 2021;25(4):507–515. doi:10.1007/s12603-021-1587-5
9. Golaz R, Tangel VE, Lui B, Albrecht E, Pryor KO, White RS. Post-operative outcomes and anesthesia type in total hip arthroplasty in patients with obstructive sleep apnea: a retrospective analysis of the state inpatient databases. J Clin Anesth. 2021;69:110159. doi:10.1016/j.jclinane.2020.110159
10. Memtsoudis S, Liu SS, Ma Y, et al. Perioperative pulmonary outcomes in patients with sleep apnea after noncardiac surgery. Anesth Analg. 2011;112(1):113–121. doi:10.1213/ANE.0b013e3182009abf
11. Boye Larsen D, Laursen M, Simonsen O, Arendt-Nielsen L, Petersen KK. The association between sleep quality, preoperative risk factors for chronic postoperative pain and postoperative pain intensity 12 months after knee and hip arthroplasty. Br J Pain. 2021;15(4):486–496. doi:10.1177/20494637211005803
12. Ding Z, Li J, Xu B, Cao J, Li H, Zhou Z. Preoperative high sleep quality predicts further decrease in length of stay after total joint arthroplasty under enhanced recovery short-stay program: experience in 604 patients from a single team. Orthop Surg. 2022;14(9):1989–1997. doi:10.1111/os.13382
13. Golub IJ, Ng MK, Conway CA, Vakharia RM, Cannada LK, Kang KK. How does sleep apnea impact outcomes following primary total hip arthroplasty for femoral neck fractures: a matched-control analysis. Arch Orthop Trauma Surg. 2023;143(1):295–300. doi:10.1007/s00402-021-04070-0
14. Gupta RM, Parvizi J, Hanssen AD, Gay PC. Postoperative complications in patients with obstructive sleep apnea syndrome undergoing hip or knee replacement: a case-control study. Mayo Clin Proc. 2001;76(9):897–905. doi:10.4065/76.9.897
15. Tang S, Jin Y, Hou Y, et al. Predictors of chronic pain in elderly patients undergoing total knee and hip arthroplasty: a prospective observational study. J Arthroplasty. 2023;38(9):1693–1699. doi:10.1016/j.arth.2023.04.055
16. Vakharia RM, Cohen-Levy WB, Vakharia AM, Donnally CJ, Law TY, Roche MW. Sleep apnea increases ninety-day complications and cost following primary total joint arthroplasty. J Arthroplasty. 2019;34(5):959–964e1. doi:10.1016/j.arth.2018.12.018
17. Pearl A, Ismail A, Alsadi T, Crespi Z, Daher M, Saleh K. Frailty and pre-frailty in the setting of total joint arthroplasty: a narrative review. Geriatr Orthop Surg Rehabil. 2023;14:21514593231188864. doi:10.1177/21514593231188864
18. Wozniak SE, Coleman J, Katlic MR. The utility of preoperative frailty assessment. Curr Surg Reports. 2016;4(11). doi:10.1007/s40137-016-0156-z
19. Gu C, Lu A, Lei C, et al. Frailty index is useful for predicting postoperative morbidity in older patients undergoing gastrointestinal surgery: a prospective cohort study. BMC Surg. 2022;22(1). doi:10.1186/s12893-022-01471-9
20. Xue Z, Song S, Hu C, Zhao S, Wang J. Risk of sarcopenia and osteoporosis in elderly male patients with obstructive sleep apnea syndrome: a multicenter study. J Clin Densitom. 2024;27(2):101481. doi:10.1016/j.jocd.2024.101481
21. Du Z, Wang G, Yan D, Yang F, Bing D. Relationships between the Pittsburgh sleep quality index (PSQI) and vertigo outcome. Neurological Res. 2023;45(4):291–299. doi:10.1080/01616412.2022.2132728
22. Williams B, Mancia G, Spiering W, et al. 2018 ESC/ESH Guidelines for the management of arterial hypertension. Eur Heart J. 2018;39(33):3021–3104. doi:10.1093/eurheartj/ehy339
23. Tsai PS, Wang SY, Wang MY, et al. Psychometric evaluation of the Chinese version of the Pittsburgh sleep quality index (CPSQI) in primary insomnia and control subjects. Qual Life Res. 2005;14(8):1943–1952. doi:10.1007/s11136-005-4346-x
24. Abellan van Kan G, Rolland Y, Bergman H, Morley JE, Kritchevsky SB, Vellas B. The I.A.N.A Task Force on frailty assessment of older people in clinical practice. J Nutr Health Aging. 2008;12(1):29–37. doi:10.1007/BF02982161
25. Fried LP, Tangen CM, Walston J, et al. Frailty in older adults: evidence for a phenotype. J Gerontol a Biol Sci Med Sci. 2001;56(3):M146–56. doi:10.1093/gerona/56.3.m146
26. Rockwood K, Theou O. Using the clinical frailty scale in allocating scarce health care resources. Can Geriatr J. 2020;23(3):210–215. doi:10.5770/cgj.23.463
27. Kendrick T, Pilling S. Common mental health disorders--identification and pathways to care: NICE clinical guideline. Br J Gen Pract. 2012;62(594):47–49. doi:10.3399/bjgp12X616481
28. Snaith RP. The Hospital Anxiety and Depression Scale. Health Qual Life Outcomes. 2003;1:29. doi:10.1186/1477-7525-1-29
29. Reich A, Heisig M, Phan NQ, et al. Visual analogue scale: evaluation of the instrument for the assessment of pruritus. Acta Derm Venereol. 2012;92(5):497–501. doi:10.2340/00015555-1265
30. Chow S-C, Shao J, Wang H. Sample Size Calculations in Clinical Research.
31. Ayers DC, Yousef M, Yang W, Zheng H. Age-related differences in pain, function, and quality of life following primary total knee arthroplasty: results from a FORCE-TJR (Function and outcomes research for comparative effectiveness in total joint replacement) cohort. J Arthroplasty. 2023;38(7 Suppl 2):S169–S176. doi:10.1016/j.arth.2023.04.005
32. Ayers DC, Yousef M, Zheng H, Yang W, Franklin PD. Do patient outcomes vary by patient age following primary total hip arthroplasty? J Arthroplasty. 2022;37(7S):S510–S516. doi:10.1016/j.arth.2022.03.032
33. Schouten B, Baartmans M, van Eikenhorst L, et al. Fatal adverse events in femoral neck fracture patients undergoing hemiarthroplasty or total hip arthroplasty-a retrospective record review study in a nationwide sample of deceased patients. J Patient Saf. 2024;20(5):e59–e72. doi:10.1097/PTS.0000000000001226
34. Ren X, Ling L, Qi L, et al. Patients’ risk factors for periprosthetic joint infection in primary total Hip arthroplasty: a meta-analysis of 40 studies. BMC Musculoskelet Disord. 2021;22(1):776. doi:10.1186/s12891-021-04647-1
35. American Diabetes A. Standards of medical care in diabetes-2022 abridged for primary care providers. Clin Diabetes. 2022;40(1):10–38. doi:10.2337/cd22-as01
36. Walter N, Szymski D, Kurtz SM, et al. What are the mortality, infection, and nonunion rates after periprosthetic femoral fractures in the United States? Clin Orthop Relat Res. 2024;482(3):471–483. doi:10.1097/CORR.0000000000002825
37. Li X, Jiang HY, Zhao YJ, Liu SZ, Pan LX. Establishment and validation of a nomogram to predict postoperative anemia after total Hip arthroplasty. BMC Musculoskelet Disord. 2024;25(1):141. doi:10.1186/s12891-024-07264-w
38. Chaves PH, Semba RD, Leng SX, et al. Impact of anemia and cardiovascular disease on frailty status of community-dwelling older women: the women’s health and aging studies I and II. J Gerontol a Biol Sci Med Sci. 2005;60(6):729–735. doi:10.1093/gerona/60.6.729
39. Wilkes JG, Evans JL, Prato BS, Hess SA, MacGillivray DC, Fitzgerald TL. Frailty cost: economic impact of frailty in the elective surgical patient. J Am Coll Surg. 2019;228(6):861–870. doi:10.1016/j.jamcollsurg.2019.01.015
40. Longo UG, De Salvatore S, Greco A, et al. Influence of depression and sleep quality on postoperative outcomes after total hip arthroplasty: a prospective study. J Clin Med. 2022;11(13). doi:10.3390/jcm11133845
41. Rockwood K, Song X, MacKnight C, et al. A global clinical measure of fitness and frailty in elderly people. CMAJ. 2005;173(5):489–495. doi:10.1503/cmaj.050051
42. McIsaac DI, MacDonald DB, Aucoin SD. Frailty for perioperative clinicians: a narrative review. Anesth Analg. 2020;130(6):1450–1460. doi:10.1213/ANE.0000000000004602
43. Kim AG, Grits D, Zhong J, et al. 5-factor modified frailty index as a predictor of outcomes after hemiarthroplasty or total hip arthroplasty for femoral neck fracture. J Am Acad Orthop Surg. 2024;32(13):e634–e641. doi:10.5435/JAAOS-D-23-00936
44. Lin HS, Watts JN, Peel NM, Hubbard RE. Frailty and post-operative outcomes in older surgical patients: a systematic review. BMC Geriatr. 2016;16(1):157. doi:10.1186/s12877-016-0329-8
45. Beggs T, Sepehri A, Szwajcer A, Tangri N, Arora RC. Frailty and perioperative outcomes: a narrative review. Can J Anaesth. 2015;62(2):143–157. doi:10.1007/s12630-014-0273-z
46. Mitnitski AB, Mogilner AJ, Rockwood K. Accumulation of deficits as a proxy measure of aging. Scientific World J. 2001;1:323–336. doi:10.1100/tsw.2001.58
47. Li C, Tao M, Chen D, et al. Transcranial direct current stimulation for anxiety during laparoscopic colorectal cancer surgery: a randomized clinical trial. JAMA Network Open. 2024;7(4):e246589. doi:10.1001/jamanetworkopen.2024.6589
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.