Back to Journals » Vascular Health and Risk Management » Volume 15
Polysaccharide peptide (PsP) Ganoderma lucidum: a potential inducer for vascular repair in type 2 diabetes mellitus model
Authors Heriansyah T ![]() , Nurwidyaningtyas W
, Nurwidyaningtyas W ![]() , Sargowo D, Tjahjono CT, Wihastuti TA
, Sargowo D, Tjahjono CT, Wihastuti TA ![]()
Received 19 February 2019
Accepted for publication 29 August 2019
Published 3 October 2019 Volume 2019:15 Pages 419—427
DOI https://doi.org/10.2147/VHRM.S205996
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Konstantinos Tziomalos
Teuku Heriansyah,1 Wiwit Nurwidyaningtyas,2 Djanggan Sargowo,3 Cholid Tri Tjahjono,3 Titin Andri Wihastuti4
1Department of Cardiology, Faculty of Medicine, Syah Kuala University, Banda Aceh, Indonesia; 2Department of Biomedical Nursing Science, STIKES Kendedes, Malang, East Java, Indonesia; 3Department of Cardiology, Faculty of Medicine, Brawijaya University, Malang, Indonesia; 4Department of Biomedical Nursing Science, Faculty of Medicine, Brawijaya University, Malang, Indonesia
Correspondence: Titin Andri Wihastuti
Department of Biomedical Nursing Science, Faculty of Medicine, Brawijaya University, Malang 65145, Indonesia
Tel +62 8 180 510 1827
Email [email protected]
Introduction: The increasing blood glucose level due to insulin resistance which occurs in diabetes mellitus (DM) may cause vascular damage. This study aims to prove the effect of the polysaccharide peptide (PsP) Ganoderma lucidum on improving vascular damage through an increase of circulating endothelial cells and circulating endothelial cells (CEC) ratio, decreased H2O2, triglyceride (TG), total cholesterol (TC) and insulin resistance in type 2 DM.
Methods: Our study is a true experimental study with randomized posttest control group design that used 35 Wistar rats divided into five groups: normal, control (+) and three groups of different variant PsP doses 50, 150 and 300 mg/kg BW (n=7).
Results: By using one-way ANOVA and post-hoc Duncan test, the results show a significant increase of endothelial progenitor cell (EPC) concentration (p=0.000) and ratio EPC:CEC (0.000) by dose-dependent fashion and also reduced CEC concentration (p=0.001), H2O2 (p=0.03), TG (p=0.001), TC (p=0.01) and insulin resistance (p=0.003).
Conclusion: In this study, PsP induced endothelial repairing process and reduced the risk factor with 300 mg/kg BW as optimum dose. However, further research on EPC and CEC detection markers is important. Further research on PsP and clinical trial for commercial uses is also needed.
Keywords: EC, EPC, polysaccharide peptide, type 2 diabetes mellitus, vascular repair
Corrigendum for this paper has been published
Introduction
Type 2 diabetes mellitus (DMT2) is one of the major risk factors of cardiovascular diseases.28 Previous research reported that patients with diabetes mellitus (DM) have a decreased life expectancy up to 7–8 years compared to those without DM.4 The number of patients with DM increased to 422 million in 2014 and caused 1.5 million deaths in 2015.1,2,5,29 Oxidative stress in DMT2 is caused by the accumulation of unstable residual DMT2, which is a major problem worldwide.10,15,46 Based on basic health research 2013, the prevalence of diabetes in Indonesia increased twice than that in 2007 (1.1–2.1%).3 The mortality in DMT2 is related to the complications, impact on vascular circumstances initiated by circulating cell at an early state.30,31 In fact, vascular walls have enzymatic systems capable of producing ROS, for example, mitochondrial electron transport chain, NADPH oxidases and xanthine oxidase.7,9–11 Excess vascular production of ROS increased glucose metabolism and another form of sugar through polyol pathway, increased production of advanced glycation end products (AGEs), increased expression of the receptor for AGEs (RAGE), activated protein kinase C (PKC) isoforms and over-activated the hexosamine pathway.6,13,14
The increase of ROS level has a harmful effect on endothelial function.12 Excessive ROS causes accelerated damages to the lipid membranes, enzymes and nucleic acids.10,13 It lowered nitric oxide (NO) level and contributed to endothelial dysfunction, low-grade inflammation, platelet hyperactivity, tissue hypoxia, apoptosis and thrombogenesis.6,16 It starts the formation of atherosclerosis plaque.14 While the apoptosis of endothelial cells began, it lost their attachments from basal membranes and circulated in the blood, called circulating endothelial cell (CEC).17,32 As a response to repaired damages, bone marrow released myeloid cells which contribute to re-endothelialization, known as endothelial progenitor cell (EPC).18
Their mobilization and differentiation are triggered by many proinflammatory chemoattractants produced by traumatic and hypoxic tissue response.10,12,15 Some chemical modulators influenced its concentration, such as physical training, erythropoietin, estrogen, granulocyte macrophage colony-stimulating factor (GM-CSF), stromal cell-derived factor −1 (SDF-1) and vascular endothelial growth factor (VEGF).19 Accumulating data suggests that the vasculoprotective functions of EPCs may be used as cellular biomarkers for endothelial damage or may be pharmacologically modulated to enhance the body’s defense to atherosclerosis.20
EPC and CEC concentrations were measured using flow cytometry.21 Higher EPC level within the ratio of EPC:CEC denotes the increase of vascular repair activity.20,47 An innovation using polysaccharide peptide (PsP) isolated from Ganoderma lucidum fungi was developed. This fungus is commonly known as Chinese traditional herb for many years for treating hepatitis, hypertension, chronic bronchitis and cancer.22,27,29 It has antioxidant and anti-inflammatory properties expected to improve the vascular repair activity and further inhibition in atherogenesis processes by altering the ratio of EPC:CEC.23 This research is aimed to determine whether PsP has an effect on improved conditions for insulin resistance through the measurement of oxidative stress status (measurement of H2O2) and indicators of circulating cell visibility changes which are indicators of vascular status (cEPC and CEC).
Materials and methods
Experimental subject
Thirty-five 8-week-old Wistar rats (Rattus norvegicus) weighing 150–200 g were taken from CV Gamma Scientific Biolab located in Malang, Indonesia, and then randomized and classified into five groups. Every group consisted of seven rats. The groups included the normal group, DMT2 group, DMT2 groups with three treatment doses of PsP (50, 150 and 300 mg/kg BW). High-cholesterol diet (HCD) was fed for 12 weeks and streptozotocin (STZ) 30 mg/kg body weight (Bio World Products Inc., Visalia, CA, USA from the Laboratory of Physiology, Brawijaya University) was injected once after 4 weeks of HCD to create DMT2.
Polysaccharide peptide of Ganoderma lucidum
PsP of Ganoderma lucidum was packed in a capsule which contained 250 mg of G. lucidum extract supplied by “Sahabat Lingkungan Hidup” Partner Labs, Surabaya, Indonesia. Each gram of PsP contained 200 mg of β-D-glucan. PsP was administered to DMT2 animal models once in a day by oral gavage 4 weeks prior to sacrifice.
Blood glucose measurement
After STZ induction, the blood glucose level of animal models was measured using a GlucoDR blood glucose test meter (All Medicus Co. Ltd, Dongan-gu, Anyang-si, Korea). When the level reached >200 mg/dL, the animals were declared as DMT2 condition.
H2O2 measurement
H2O2 levels in the plasma were analyzed by colorimetric H2O2 kit of Assay Design by Abcam, Cambridge, MA, USA and identified at 570 nm using an ELISA Kit by Boehringer-Mannheim GMBH, Mannheim, Germany.
Insulin resistance measurement
Insulin resistance assay was performed to diagnose whether the rat had DMT2.23,24 The insulin levels in plasma were analyzed using ELISA Kit (Boehringer, Mannheim) afterward the measurement of the level of blood glucose. The levels of fasting insulin in plasma were at a normal value of below 2500 pg/mL. Moreover, insulin resistance was measured by insulin sensitivity index (ISI) formula as follows:

where FBG = fasting blood glucose and FINS = fasting plasma insulin. The insulin resistance is indicated when the value of ISI is lower than 1.23–25
Lipid profile level measurement
Lipid profiles of serum were analyzed by the use of a Cobas Mira Analyzer by PT Roche Indonesia, Jakarta, Indonesia.
Isolation of EPC and CEC
Heparinized peripheral blood from healthy and treated rats was aseptically collected by puncturing a heart vein. We further used Ficoll-based gradient aimed to produce more PBMCs than using the RBC lysis-based preparation method.47 Cells were analyzed with a fluorophore-labeled antibody [specific surface antigen] before sorting flow cytometer.
Measurement of EPC
The number of EPC was obtained by flow cytometry. The EPC was detected by CD 34 per CP Santa Cruz SC-19,621 and CD 133 FITC (Fluorescein isothiocyanate) Bioss bs-0395R-FITC marker.32,33,47
Measurement of CEC
The number of CEC was obtained by flow cytometry. CEC was detected by CD 45 per CP Santa Cruz SC-19,621 and CD 146 FITC (Fluorescein isothiocyanate) Bioss bs-0395R-FITCmarker.12,32,33,47
Ethic
Ethics approval for this study was obtained from Ethical Committee of Medical Faculty, University of Brawijaya, Indonesia number 462/EC/KEPK/08/2013), and the IACUC (Institutional Animal Care and Use Committee) guidelines were followed for the animal experiments.
Analysis of statistical data
The levels of EPC, CEC, EPC:CEC ratio, H2O2, lipid profile and insulin resistance in DMT2 rats were analyzed using ANOVA test; SPSS software version 20 (IBM Corporation, New York, NY, USA) was used to determine the difference among groups of intervention and control.
Result
Table 1 presents the results with one-way ANOVA and posthoc Duncan Test of PsP effect in all parameters of vascular state in diabetic models for each group. There was a significant reduction in some endothelial cell dysfunction parameters after administration of PsP, including H2O2, total cholesterol (TC) and triglyceride (TG) as lipid profile, CEC and insulin resistance levels (one-way ANOVA p=0.000). The lipid profile level indicated by TC and TG showed the highest in the DMT2 group (139,65 mg/dL and 661,60 mg/dL, respectively) and the lowest in the normal group at 47,20 mg/dL and 76,20 mg/dL, respectively respectively. Moreover, the insulin resistance was identified at −1.18 in the DMT2 group.
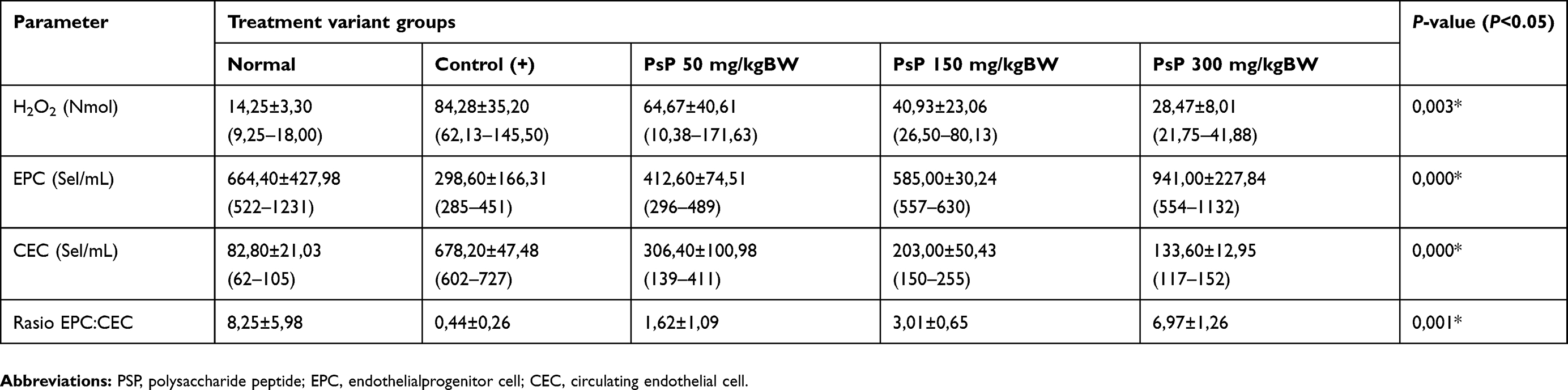 |
Table 1 Result in each group with one-way ANOVA and posthoc duncan test |
This study showed that a HCD and STZ administration were able to induce insulin resistance in the DMT2 group and increase the lipid profile level with the significance value of <0.05.
To assess the downstream effects of insulin-resistant conditions on the modulation of oxidative stress, measurements of plasma H2O2 levels in the control group (+) showed the highest number (84.28±35.20) compared to the other groups. Another impact of increasing plasma glucose is the inhibition of the activity of the DDHA enzyme causing an increase in asymmetric dimethylarginine (ADMA). ADMA is one of the results of methylation of arginine, which is competitive binding with arginine (material for NO synthesis) in eNOS. Change NO availability impacted on the endothelial structure.36 To validate this concept, the researchers performed measurements of the number of CEC and cEPC which were indicators of endothelial damage and repair due to a decrease NO. The data show that insulin resistance in this model causes the release of endothelial cells to the circulation by 678.20±47.48.
This amount was followed by identification of cEPC, although initially we used double markers for cEPC identification but the results of this study indicate that the double-positive cell population is very low. Fluctuations in the population of CD 133+ showed significant differences (p-value 0.000) in all observation groups. We did not use VEGFR2/KDR markers in this study as used in many publications because basically defining cEPC is varied depending on the source of cEPC isolation itself or the selection of marker surfaces. The results of this study indicate the effect of PsP on increasing the number of niche populations of cEPC as a form of response to improvement. In the insulin resistance group, there was a decline in the CD133+ population which decreased in the range of 298.60±166.31. The results of this study are similar to those of previous research, indicating that the progression of type I/II DM will cause oxidative stress conditions that modulate endothelial dysfunction including reducing the potential cEPC.30,46
Furthermore, the researchers examined the effect of PSP on improving vascular circumstances which contributed to improve oxidative stress, increase repopulation of cEPC as an indicator of improvement in endothelial dysfunction and block conditions for endothelial dysfunction.12,33 There was a significant reduction in some endothelial cell dysfunction parameters after administration of PsP, including H2O2, TCand TG as lipid profile, CEC and insulin resistance levels. The most significant level was observed in the control(+) group and the lowest value at the normal group.
The posthoc Duncan test results show a significant difference in the concentration between control (+) group with the normal group and PsP 300 mg/kg BW group. However, there was no significant difference with PsP 50 mg/kg BW and PsP 150 mg/kg BW. This means the parameter value after administration of PsP 300 mg/kg BW was closer to the normal value. EPC:CEC ratio was measured by EPC number divided by CEC number detected by flow cytometry. EPC number is determined through CD133(+) marker (cells that spread at the lower right quadrant). The result ranged from 285 to 1231 cells/mL. EPC cells spreading pattern show a significant rise of number in the PsP treatment groups. The lowest average number was found at control (+) group with 298 cells/mL and the highest average at PsP 300 mg/kgBW group (941 cells/mL). EPC number under PsP 300 mg/kg BW treatment had a higher level compared to the normal group (P=0.000).
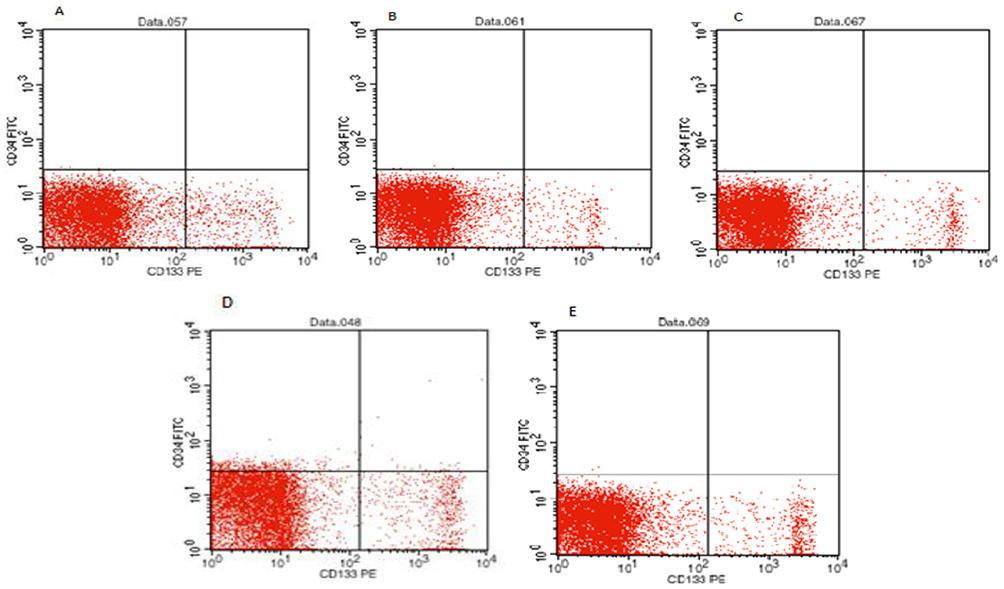 |
Figure 1 The result of flow cytometry of EPC counted by CD 133(+)-dominant cells located at the lower right quadrant of the graph. Notes: (A) Normal group, (B) insulin resistance models, (C) group with administration 50 mg/kgBW dose of PsP, (D) group with administration 150 mg/kgBW dose of PsP, (E) group with administration 300 mg/kgBW dose of PsP. Abbreviations: EPC, endothelial progenitor cell; BW, body weight; PsP, polysaccharide peptide. |
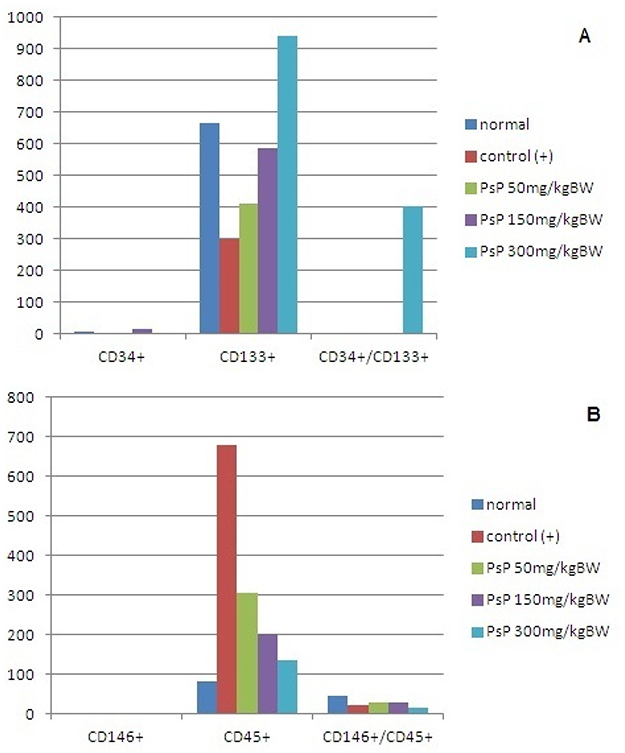 |
Figure 2 Single and double staining representative circulating cell target as well as vascular repair indicator. Note: (A) Marker used for circulating endothelial progenitor cell identification, (B) marker used for circulating endothelial cell identification. Abbreviation: CD, cluster of differentiation. |
Display data that we presented in Figure 2 are the result of the validation results of staining for identification cEPC and CEC. It appears that the cEPC single marker with CD133+ is very dominant in almost all groups and is the cell population with the most visible variation in changes after the administration of PsP Ganoderma lucidum compared to positive controls. Likewise with the CEC marker that we use, the CD45+ cell population (mononuclear cell marker) actually provides information on the negative effects of the PsP Ganoderma lucidum on the CD45+ cell population.
The enhancement of cEPC was followed by reduction of CEC number in PsP treatment group compared to the control (+) group. CEC was detected through CD45(-) and CD146(+) by flow cytometry. The lowest average was found in PsP 300 mg/kgBW group (p=0.000). Alteration of the ratio depends on EPC and/or CEC number in each milliliter of blood. The increases in EPC would increase the ratio. Inversely, the increase in CEC would decrease the ratio. Therefore, the ratio of EPC:CEC tends to increase along with the addition of PsP doses. The flow cytometry results of EPC and CEC cell spreading pattern in each group can be seen in Figures 1 and 3.
Antioxidant effect was confirmed using differences in H2O2 level between control(+) group and PsP intervention groups of 50 mg/kg BW, 150 mg/kg BW and 300 mg/kg BW. There was a significant increase of H2O2 level in the control(+) group compared to the normal group. H2O2 level in normal group is 14.25 nmol/mL and increased 12 folds in control(+) group. H2O2 level decreased in PsP treatment group in accordance to dose escalation. Based on one-way ANOVA test and post-hoc Duncan test, it was concluded that there was a significant difference of H2O2 level (p=0.003) between control(+) group, normal group and PsP 300 mg/kg BW group. These results confirm the potentiated antioxidant effect of 300 mg/kg BW PsP which reduced the H2O2 level almost to the normal value.
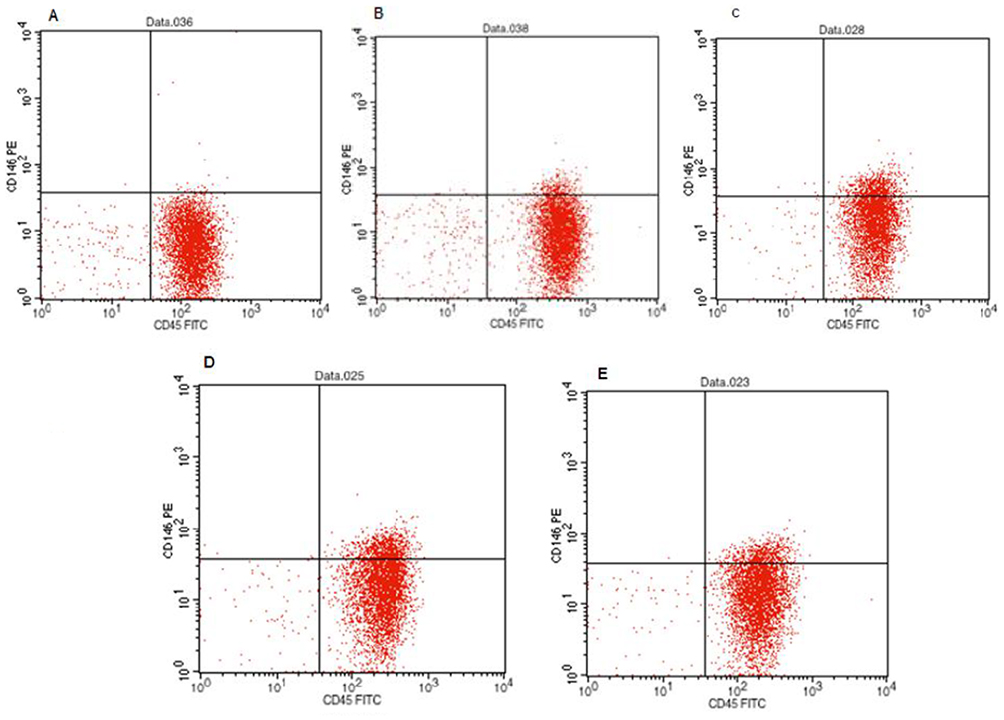 |
Figure 3 The result of flow cytometry of CEC counted by CD 146(+)/CD45(-) cells located at the upper left quadrant of the graph. Notes: (A) Normal group, (B) insulin resistance models, (C) group with administration 50 mg/kgBW dose of PsP, (D) group with administration 150 mg/kgBW dose of PsP, (E) group with administration 300 mg/kgBW dose of PsP. Abbreviations: CEC, circulating endothelial cell; BW, body weight; PsP, Pplysaccharide peptide. |
PsP intervention has been found to improve the TG level and TC level. One-way ANOVA test results show significant differences in lipid profile in each group (p=0.01 and p=0.001). The highest level of TG and TC was observed at control(+) group, the group with HCD and the lowest measured at normal diet group. PsP has also been found to improve insulin resistance in DMT2 rats, proved by one-way ANOVA test with 95% confidence interval (p=0.003). Insulin sensitivity index <1 is regarded as insulin resistance. The lowest value of insulin sensitivity index was found in the control(+) group with the average of −1.18 which means that it had insulin resistance and confirmed the development of DMT2. Posthoc test analysis demonstrated that PsP 300 mg/kgBW has a significant difference in control(+) groups and PsP 50 mg/kg BW group, and the level of insulin resistance increased around normal value in PsP 300 mg/kg BW group.
Discussion
Basic studies have shown the evidence regarding the innate complex mechanisms underlying changes that occur in the vasculature during DM and lead to CV risk associated with macrovascular and microvascular complications of DM.25,28,44 More importantly, during the formation of arteriosclerosis, vascular cell homeostasis plays a significant role.15,42 Endothelial dysfunction is a consistent finding across the spectrum of insulin-resistant states, characterized by reduced NO bioavailability leading to an increase in the number of circulating endothelial cells. EPCs are circulating cells which have been identified as mediators of endothelial repair. Several abnormalities associated with insulin resistance, including reduced NO bioavailability, increased production of RO and downregulation of intracellular signaling pathways, have the potential to disrupt EPC function.41 EPCs have a protective impact on the vasculature.44
This study observes the effects of Ganoderma lucidum PsP that was investigated to have antioxidant and anti-inflammatory properties which are expected to improve the vascular repair activity and further inhibition.23 Improved vascular capacity occurs with maximum doses of PsP (300 mg/kg BW), reducing the amount of CEC lower than the control group (+) with disparity point at 544.60 cells/mL. However, 50.80 cells/mL were higher compared to that of the normal group. It can be concluded that the administration of PSP has been proven to reduce endothelial dysfunction shown by the decreased CEC count.
Endothelial dysfunction in the insulin resistance model is associated with oxidative stress due to an increase in plasma glucose levels.10,12,23,28,46 Reduction of CEC was an indicator of improvement in endothelial dysfunction in this study, associated with a decrease of H2O2 levels in the maximum dose of PSP group. Reduction of H2O2 at the maximum dose showed the lowest levels compared to the group with another dose or in the control group (+).
NO, produced from L-arginine by eNOS [endothelial NOS (NO synthase)], is perhaps the most important compound, possessing vasodilatory, anti-inflammatory, antiplatelet and antioxidant properties.41 NO is rapidly inactivated in the vessel wall by ROS. The relative production by endothelial cells of NO and ROS is, therefore, of critical importance in vascular homeostasis.41 Based on that statement, antioxidants in the PSP Ganoderma lucidum are thought to have the same effect as NO. So, they can reduce H2O2 at the level 21.75–41.88 Nmol. Coexisting vascular risk factors and many biochemical changes associated with insulin resistance, including inflammation, ROS, altered secretion of cytokines by adipocytes and increased NEFAs, may contribute to endothelial dysfunction indirectly.41 Endothelial dysfunction is an imbalance in the production of vasodilator factors. When this balance is disrupted, it predisposes the vasculature toward prothrombotic and pro-atherogenic effects.45 From some of the statements above, it can be concluded that the PSP Ganoderma lucidum can reduce ROS (H2O2) so that endothelial disrupted (increased number of CEC) can be inhibited through the antioxidant effects of PsP.
STZ-induced diabetes: Diabetes reduced the release of SDF in wounds, reduced circulating EPCs and impaired EPC mobilization due to reduced bone marrow eNOS phosphorylation. Hyperoxia and SDF administration acted synergistically to abrogate these defects.39 Decreasing intracellular superoxide by transgenic overexpression of MnSOD prevented the reduced eNOS and CXCR4 expression usually seen in diabetic EPCs exposed to hypoxia or hyperglycemia.40
Several abnormalities associated with insulin resistance, including reduced NO bioavailability, increased production of ROS, and downregulation of intracellular signaling pathways, have the potential to disrupt EPC function.46 In endothelial cells, ROS exert direct cytotoxic effects, react with NO to diminish NO bioavailability and form peroxynitrite anions, which are powerful oxidants. Although EPCs from healthy individuals are postulated to be relatively resistant to oxidant stress, increased ROS, resulting from increased production or diminished endogenous antioxidant defenses, may lead to EPC dysfunction in those at risk of cardiovascular disease. In animal models, conditions characterized by increased ROS are associated with reduced number of circulating EPCs.23,26,41
This study shows that a high-fat diet and STZ induction can modulate the increase of H2O2 that occurs in the control group (+) compared to the entire observation group. Increased H2O2 has an impact on the amount of EPC in circulation. The number of cEPC in the control group (+) shows the lowest number (298.60 cells/mL) compared to the entire observation group. PsP intervention showed improvement in cEPC (CD133+) repopulation in this study. PsP administration at the maximum dose showed vascular improvement in the resistant insulin model. It appears that the CD133 (+) repopulation shows the highest number compared to all observation groups with a significance value of 0.000. CD133 is a marker of hematopoietic cells derived from bone marrow, and repopulation of cells with these markers can be increased due to exposure to inflammatory mediators. CD133 which is becoming a major overview of the results of our study is basically an indicator of the characteristics of stem cells hematopoetic are abundant in the bone marrow and have the ability to differentiate into different types of cells mononuclear another one of them is the EPC.34
Many previous studies mention that the decrease in NO in the insulin resistance model causes endothelial dysfunction. Endothelial dysfunction is an imbalance in the production of vasodilator factors, and when this balance is disrupted, it predisposes the vasculature toward prothrombotic and pro-atherogenic effects.45 This study did not measure NO as a mediator that induced improvement in endothelial dysfunction through the administration of PsP Ganoderma lucidum.
Analysis of the EPC and CEC ratios in the entire observation group is an indicator of improvement in vascular status in the insulin resistance model. Vascular repair with those indicated by EPC and CEC ratio data can be seen in the group given PsP Ganoderma lucidum. So, it can be concluded, based on this study, that the PsP Ganoderma lucidum have a positive effect to improve vascular damage through an increase of EPC/CEC ratio and decreased oxidant, TG, TC and insulin resistance in type 2 diabetes in the rat model.
Geolocation information
Laboratorium Sentral Ilmu Hayati (LSIH) and Biomedical Laboratory, Medical Faculty Brawijaya University, East Java, Indonesia.
Acknowledgments
This study was supported by Medical Faculty of Brawijaya University, Indonesia. The authors are grateful to the Syiah Kuala University for its participation and the Ministry of Research, Technology and Higher Education of the Republic of Indonesia for funding this experiment. We gratefully acknowledge all participants of this study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Mozaffarian D, Bejamin EJ, Go AS, et al; American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Executive summary: heart disease and stroke statistics–2016 update: a report from the American Heart Association. Circulation. 2016;133:447–454.
2. World Health Organization Geneva. (2017). Fact sheet on Diabetes. [
3. Dasar RK. Badan Penelitian Dan Pengembangan Kesehatan. Jakarta: Kementerian Kesehatan Republik Indonesia; 2013:85–90.
4. Santos ADL, Cecílio HPM, Teston EF, Arruda GOD, Peternella FMN, Marcon SS. Microvascular complications in type 2 diabetes and associated factors: a telephone survey of self-reported morbidity. Cien Saude Colet. 2015;20(3):761–770. doi:10.1590/1413-81232015203.12182014
5. Ulutas KT, Dokuyucu R, Sefil F, et al. Evaluation of mean platelet volume in patients with type 2 diabetes mellitus and blood glucose regulation: a marker for atherosclerosis? Int J Clin Exp Med. 2014;7(4):955–961.
6. Sena CM, Pereira AM, Seiça R. Endothelial dysfunction - a major mediator of diabetic vascular disease.Biochim Biophys Acta. 2013;1832:2216–2231. doi:10.1016/j.bbadis.2013.08.006
7. Lassegue B, Griendling KK. NADPH oxidases: functions and pathologies in the vasculature, Arterioscler. Thromb Vasc Biol. 2010;30:653–661. doi:10.1161/ATVBAHA.108.181610
8. Jezek P, Hlavata L. Mitochondria in homeostasis of reactive oxygen species in cell, tissues, and organism, Int. J Biochem Cell Biol. 2005;37:2478–2503. doi:10.1016/j.biocel.2005.05.013
9. Turrens JF. Mitochondrial formation of reactive oxygen species, J. Physiol. 2003;552:335–344. doi:10.1113/jphysiol.2003.049478
10. Chung HY, Baek BS, Song SH, et al. Xanthine dehydrogenase/xanthine oxidase and oxidative stress. Age. 1997;20(3):127–140. doi:10.1007/s11357-997-0012-2
11. J-M L, Lin PH, Yao Q, Chen C. Chemical and molecular mechanisms of antioxidants: experimental approaches and model systems. J Cell Mol Med. 2010;14(4):840–860. doi:10.1111/j.1582-4934.2009.00897
12. Cai H, Harrison DG. Endothelial dysfunction in cardiovascular diseases: the role of oxidant stress. Circ Res. 2000;87:840–844. doi:10.1161/01.res.87.6.480
13. Brownlee M. The pathobiology of diabetes complications: a unifying mechanism. Diabetes. 2005;54:1615–1625. doi:10.2337/diabetes.54.6.1615
14. Wihastuti TA, Sargowo D, Tjokroprawiro A, Permatasari N, Widodo MA, Soeharto S. Vasa Vasorum Anti-angiogenesis through H2O2, HIF-1α, NF-kB, and iNOS inhibition by mango-steen pericarp ethanolic extract (Garcinia mangostana Linn) inhipercholesterol diet given Rattus novergicus Wistar strain. Vasc Health Risk Manag. 2014;10:523–531. doi:10.2147/VHRM.S61736
15. Boamponsem AK, Boamponsem LK. The role of inflammation in atherosclerosis. Pelagia Res Lib. 2011;2(4):194−207.
16. Sabatier F, Camoin-Jau L, Anfosso F, Sampol J, Dignat-George F. Circulating endothelial cells, microparticles and progenitors: key players towards the definition of vascular competence. J Cell Mol Med. 2009;13(3):454–457. doi:10.1111/j.1582-4934.2008.00639.x
17. Du F, Zhou J, Gong R, et al. Endothelial progenitor cells in atherosclerosis. Front Biosci. 2012;17:2327–2349. doi:10.2741/4055
18. Liu P, Zhou B, Gu D, Zhang L, Han Z. Endothelial progenitor cell therapy in atherosclerosis: A double-edged sword? Ageing Res Rev. 2009;8;pp:83–93. doi:10.1016/0006-2952(75)90029-5
19. Pompilio G, Capogrossi MC, Pesce M, et al. Review: endothelial progenitor cells and cardiovascular homeostasis: clinical implications. Int J Cardiol. 2009;131:156–167. doi:10.1016/j.ijcard.2008.11.048
20. Schmidt-Lucke C, Fichtlscherer S, Aicher A, et al. Quantification of circulating endothelial progenitor cells using the modified ISHAGE protocol. PLoS One. 2010;5(11):e13790. doi:10.1371/journal.pone.0013790
21. Xu Z, Chen X, Zhong Z, et al. Ganoderma lucidum polysaccharides: immunomodulation and potential anti-tumor activities. Am J Chin Med. 2011;39:15–27. doi:10.1142/S0192415X11008610
22. Wihastuti TA, Heriansyah T. The inhibitory effects of polysaccharide peptides (PsP) of Ganoderma lucidum against atherosclerosis in rats with dyslipidemia. Heart Int. 2017;12(1):e1–e7.
23. American Diabetes Association. Diagnosis and classification of diabetes mellitus. Diabetes Care. 2014;37(Suppl. 1):81–90. doi:10.2337/dc14-S081
24. Baynes HW. Classification, pathophysiology, diagnosis and management of diabetes mellitus. J Diabetes Metab. 2015;6:541. doi:10.4172/2155-6156.1000541
25. Perkumpulan Endokrinologi Indonesia. Konsensus Pengendalian Dan Pencegahan Diabetes Mellitus Tipe 2 Di Indonesia. Jakarta: PB. PERKENI; 2015:11–14.
26. Teramoto T, Sasaki J, Ishibashi S, et al. Diagnostic criteria for dyslipidemia executive summary of the Japan Atherosclerosis Society (JAS) guidelines for the diagnosis and prevention of atherosclerotic cardiovascular diseases. 2012 Japan version. Journal of Atherosclerosis and Thrombosis, 20(8), 655-660. https://doi.org/10.5551/jat.17152.
27. Seto SW, Lam TY, Tam HL, et al. Novel hypoglycemic effects of Ganoderma lucidum water-extract in obese/diabetic (+db/+db) mice. Phytomedicine. 2009;16(5):426–436. doi:10.1016/j.phymed.2008.10.004
28. Gleissner CA, Galkina E, Nadler JL, Ley K. Mechanisms by which diabetes increases cardiovascular disease. Drug Discov Today Dis Mech. 2007;4(3):131–140. doi:10.1016/j.ddmec.2007.12.005
29. Benzie IFF, Wachtel-Galor S. Herbal Medicine: Biomolecular and Clinical Aspects.
30. Ferraro F, Lymperi S, Méndez-Ferrer S, et al. Diabetes impairs hematopoietic stem cell mobilization through alteration of niche function. Sci Transl Med. 2011;3(104):104ra101. doi:10.1126/scitranslmed.3002191
31. Kumar A; Fausto. Pathologic Basis of Disease.
32. Lampka M, Grąbczewska Z, Jendryczka-Maćkiewicz E, et al. Circulating endothelial cells in coronary artery disease. Kardiol Pol. 2010;68(10):1100–1105.
33. Liu P, Zhou B, Gu D, Zhang L, Han Z. Endothelial progenitor cell therapy in atherosclerosis : a double-edged sword? Ageing Res Rev. 2009;8:83–93. doi:10.1016/j.arr.2008.11.002
34. Hristov M, Erl W, Weber PC. Endothelial Progenitor Cell. Arterioscler Thromb Vasc Biol. 2003;23:1185–1189. doi:10.1161/01.ATV.0000073832.49290.B5
35. Yu C-G, Zhang N, Yuan -S-S, et al. Endothelial progenitor cells in diabetic microvascular complications: friends or foes? Stem Cells Int. 2016;1803989. doi:10.1155/2016/1803989
36. Hamed S. Endothelial Progenitor Cell Dysfunction in Diabetes Mellitus Type-2: Focus on Nitric Oxide System, Medical Complications of Type 2 Diabetes, Dr. Colleen Croniger (Ed.), ISBN: 978-953-307-363-7, InTech. 2010. Available from: http://www.intechopen.com/books/medical-complications-of-type-2-diabetes/endothelial-progenitor-cell-dysfunction-in-diabetes-mellitus-type-2-focus-on-nitric-oxide-system
37. Lombardo MF, Iacopino P, Cuzzola M, et al. Type 2 diabetes mellitus impairs the maturation of endothelial progenitor cells and increases the number of circulating endothelial cells in peripheral blood. Cytometry. 2012;81A:856–864. doi:10.1002/cyto.a.22109
38. Nelwan EJ, Widjajanto E, Andarini S, Djati MS. Modified risk factors for Coronary Heart Disease In Minahasa Ethnic Group, Manado. J Exp Life Sci. 2016;6(2):88–94. doi:10.21776/ub.jels.2016.006.02.06
39. Gallagher KA, Liu ZJ, Xiao M, et al. Diabetic impairments in NO-mediated endothelial progenitor cell mobilization and homing are reversed by hyperoxia and SDF-1α. J Clin Invest. 2007;117:1249–1259. doi:10.1172/JCI29710
40. Ceradini DJ, Yao D, Grogan RH, et al. Decreasing intracellular superoxide corrects defective ischemia-induced new vessel formation in diabetic mice. J Biol Chem. 2008;283:10930–10938. doi:10.1074/jbc.M707451200
41. CUBBON RM, Kahn MB, Wheatcroft SB. Effects of insulin resistance on endothelial progenitor cells and vascular repair. Clin Sci. 2009;117:173–190. doi:10.1042/CS20080263; Printed in Great Britain.
42. Zhou B, Andriana Margariti L, Margariti A, Zeng L, Xu Q. Role of histone deacetylases in vascular cell homeostasis and arteriosclerosis. Cardiovasc Res. 2011;90:413–420. doi:10.1093/cvr/cvr003
43. BAZZONI GIANFRANCO, DEJANA ELISABETTA. Endothelial cell-to-cell junctions: molecular organization and role in vascular homeostasis. Physiol Rev. 2004;84:869–901. doi:10.1152/physrev.00035.2003
44. Berezin AE. Endothelial progenitor cells dysfunction in diabetes mellitus. ARC J Diabetes Endocrinol. 2016;2(1):29–37. doi:10.20431/2455-5983.0201005.
45. Dhananjayan R, Srivani Koundinya KS. Endothelial Dysfunction in Type 2 Diabetes Mellitus. Ind J Clin Biochem. 2016;31(4):372–379. doi:10.1007/s12291-015-0516-y
46. Desouza CV, Frederick G, Hamel FG, Bidasee K, O’Connell K. Role of inflammation and insulin resistance in endothelial progenitor cell dysfunction. DIABETES. 2011;60.doi:10.2337/db10-0875.
47. Huizer K, Mustafa DAM, Mustafa DA, Spelt JC, et al. Improving the characterization of endothelial progenitor cell subsets by an optimized FACS protocol. PLoS One. 2017;12(9):e0184895. doi:10.1371/journal.pone.0184895
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.