Back to Journals » Infection and Drug Resistance » Volume 19
Polymicrobial Multidrug-Resistant Infection and Fatal Bowel Ischemic Perforation After Urgent Heart Transplantation in a VA-ECMO–Bridged Recipient: A Case Report
Received 24 February 2026
Accepted for publication 12 May 2026
Published 18 May 2026 Volume 2026:19 604688
DOI https://doi.org/10.2147/IDR.S604688
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Oliver Planz
Yangyang Jia,1,* Yue Zhu,2,* Hongliu Cai2
1Department of Infection Management, The First Affiliated Hospital, Zhejiang University School of Medicine, Hangzhou, 310003, People’s Republic of China; 2Department of Critical Care Medicine, the First Afliated Hospital, Zhejiang University School of Medicine, Hangzhou, 310003, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yue Zhu, Department of Critical Care Medicine, the First Afliated Hospital, Zhejiang University School of Medicine, Hangzhou, 310003, People’s Republic of China, Email [email protected]
Abstract: Post-transplant infection caused by multidrug-resistant organisms (MDROs) is a major challenge in heart transplantation, especially in recipients requiring veno-arterial extracorporeal membrane oxygenation (VA-ECMO) before surgery. We describe a 52-year-old man with non-ST-elevation myocardial infarction and refractory cardiogenic shock who required VA-ECMO, intra-aortic balloon pump support, continuous renal replacement therapy, and mechanical ventilation before urgent heart transplantation. Before transplantation, he had active pneumonia. Donor respiratory culture grew Acinetobacter baumannii, Pseudomonas aeruginosa, and Staphylococcus aureus, whereas donor blood culture and blood metagenomic next-generation sequencing (mNGS) were negative. After transplantation, serial mNGS and conventional cultures revealed rapidly progressive polymicrobial infection involving Stenotrophomonas maltophilia, Burkholderia multivorans, carbapenem-resistant Acinetobacter baumannii, carbapenem-resistant Klebsiella pneumoniae, and vancomycin-resistant Enterococcus faecium. Antimicrobial therapy was repeatedly adjusted, and VA-ECMO was successfully discontinued on postoperative day 13. However, on postoperative day 16, the patient developed bowel ischemia with gastrointestinal perforation, followed by feculent peritonitis, persistent septic shock, progressive multiorgan dysfunction syndrome, and death on postoperative day 24. This case shows that perioperative infection control in VA-ECMO-bridged urgent heart transplant recipients requires more than broad-spectrum antimicrobial escalation. It requires careful assessment of preoperative infection controllability, interpretation of mNGS in conjunction with culture-based susceptibility testing, and early investigation of occult abdominal ischemia when clinical deterioration is unexplained.
Keywords: heart transplantation, VA-ECMO, multidrug-resistant organisms, polymicrobial infection, metagenomic next-generation sequencing, gastrointestinal perforation, bowel ischemia, multiorgan dysfunction syndrome
Introduction
Infection is a major cause of adverse outcomes after heart transplantation. The risk is particularly high in critically ill recipients who require advanced mechanical circulatory support before transplantation, such as veno-arterial extracorporeal membrane oxygenation (VA-ECMO).1,2 In this population, pre-existing pulmonary infection, prolonged intensive care unit stay, repeated exposure to broad-spectrum antimicrobials, multiple invasive devices, and postoperative immunosuppression may act together to impair infection control. When multidrug-resistant organisms (MDROs) are involved, infection can progress rapidly and may become difficult to reverse, especially when the infectious source is not promptly identified or controlled.
Whether to proceed with urgent heart transplantation in a patient with active infection and ongoing extracorporeal support is a difficult clinical decision. The 2016 International Society for Heart and Lung Transplantation listing criteria recommend that infectious diseases should be incorporated into transplant candidate assessment, and active systemic infection is an important concern when postoperative immunosuppression is expected.3 However, for patients with refractory cardiogenic shock supported by VA-ECMO, intra-aortic balloon pump (IABP), and continuous renal replacement therapy (CRRT), waiting for complete microbiological clearance may not be feasible. In such circumstances, the transplant team must balance the immediate risk of death from cardiac failure against the possibility of uncontrolled infection after transplantation.
Donor microbiology further complicates this assessment. Respiratory tract colonization in the donor, even with MDROs, does not necessarily mean donor bloodstream infection, particularly when donor blood culture and blood metagenomic next-generation sequencing (mNGS) are negative. Nevertheless, these findings should influence donor-recipient infectious risk assessment, perioperative antimicrobial planning, and post-transplant surveillance.4–6 In the present case, the recipient had active pneumonia, non-ST-elevation myocardial infarction, refractory cardiogenic shock, and evolving multiorgan dysfunction while receiving VA-ECMO, IABP, CRRT, and mechanical ventilation before urgent transplantation. Donor respiratory culture grew Acinetobacter baumannii, Pseudomonas aeruginosa, and Staphylococcus aureus, whereas donor blood culture and blood mNGS were negative.
We describe a case of rapidly progressive polymicrobial MDRO infection after urgent heart transplantation in a VA-ECMO-bridged recipient. The postoperative course was complicated by bowel ischemia, gastrointestinal perforation, intra-abdominal sepsis, refractory septic shock, and fatal multiple organ dysfunction syndrome (MODS). The value of this case lies in the convergence of several risk factors within a short postoperative period: partially controlled recipient infection, extracorporeal support, donor respiratory MDRO colonization, postoperative immunosuppression, complex microbiological findings, and delayed definitive source control. This report therefore focuses on three practical issues: assessing whether infection is sufficiently controllable before urgent transplantation, interpreting mNGS together with culture-based susceptibility data, and maintaining early suspicion for occult abdominal complications in high-risk transplant recipients.7,8
Case Report
A 52-year-old man had experienced intermittent chest tightness and dull pain over the left anterior chest for approximately one month. The pain radiated to the left shoulder and back and was partly relieved by rest. At a local hospital, cardiac troponin I was elevated to 2.517 ng/mL, and electrocardiography showed ST-segment depression in leads I, aVL, and V5–V6. Coronary angiography was not performed at that time, and the patient received conservative treatment. His symptoms worsened over the following week, and he was admitted to another hospital on 8 March 2024.
Transthoracic echocardiography showed impaired left ventricular systolic function, with an ejection fraction of approximately 40%. Chest imaging suggested bilateral pneumonia. Despite anti-infective therapy, inotropic support, and diuretics, the patient developed progressive circulatory failure requiring high-dose vasoactive agents. On 14 March 2024, continuous renal replacement therapy (CRRT) and intra-aortic balloon pump (IABP) support were started because of worsening cardiorenal dysfunction and hemodynamic instability. Coronary angiography performed on 15 March showed multivessel coronary artery disease. Percutaneous coronary intervention with stent implantation was performed for severe lesions in the left circumflex territory, but cardiac function did not improve substantially, and IABP weaning was unsuccessful.
On 26 March 2024, refractory cardiogenic shock further worsened, and veno-arterial extracorporeal membrane oxygenation (VA-ECMO) was initiated for circulatory and oxygenation support. The patient was transferred to our institution on 27 March 2024 for advanced heart failure management and transplant evaluation while receiving VA-ECMO and IABP support. Piperacillin/tazobactam 4.5 g every 8 h was started empirically for suspected hospital-acquired pneumonia. Supportive treatment included dobutamine, continued CRRT, gastrointestinal protection, correction of electrolyte imbalance, and nutritional support.
On 31 March 2024, sputum culture showed abundant Klebsiella pneumoniae and moderate Stenotrophomonas maltophilia, accompanied by increasing inflammatory markers. Piperacillin/tazobactam was therefore changed to meropenem 1 g every 8 h. Vancomycin was added perioperatively because of the patient’s critical illness, multiple invasive devices, and risk of bloodstream infection.
Status on Admission
At admission to our institution, the patient was sedated and mechanically ventilated through a tracheostomy tube in pressure-control assist-control mode, with PEEP 8 cmH2O and FiO2 35%. Peripheral oxygen saturation was maintained at 100%. Hemodynamic support included norepinephrine at 1.13 μg/kg/min; blood pressure was 103/47 mmHg, and sinus tachycardia was present with a heart rate of 128 beats/min. VA-ECMO was running at 3600 rpm, with blood flow 3.0 L/min and sweep oxygen fraction 100%. IABP support was set at 1:2. Bilateral coarse breath sounds with mixed dry and moist rales were heard on auscultation. No lower limb edema was observed.
The patient had no known history of hypertension, diabetes mellitus, chronic viral hepatitis, tuberculosis, previous surgery, trauma, or blood transfusion. There was no known family history of genetic or infectious disease, and no drug or food allergy was reported.
Laboratory and Imaging Findings
Electrocardiography again showed ST-segment depression in leads I, aVL, and V5–V6. Non-contrast head CT did not show acute intracranial abnormalities. Chest CT demonstrated airway mucus plugs, exudative changes in both lower lobes, mild pericardial effusion, and coronary and aortic calcifications. Abdominal CT showed a left renal calculus, small pelvic effusion, and peritoneal exudative changes.
Laboratory testing showed a white blood cell count of 6.53 × 109/L, with neutrophils 84.1% and lymphocytes 0.69 × 109/L. Platelet count was 53 × 109/L. High-sensitivity C-reactive protein was 48.66 mg/L, procalcitonin 2.21 ng/mL, D-dimer 3990 μg/L, troponin I 1.336 ng/mL, and BNP 2779 pg/mL. Arterial lactate was 1.3 mmol/L. Serum albumin was 26.0 g/L, total bilirubin 41.5 μmol/L, and creatinine 293 μmol/L, corresponding to an estimated GFR of 20.2 mL/min.
Clinical Diagnosis
The working diagnoses were end-stage heart failure secondary to coronary artery disease with recent non-ST-elevation myocardial infarction, cardiogenic shock classified as Killip class IV, severe pneumonia with suspected bloodstream infection and evolving sepsis, multiple organ dysfunction, acute kidney injury requiring CRRT, coagulopathy, hypoalbuminemia, pleural and abdominal effusions, cholelithiasis, and renal calculi.
Heart Transplantation and Donor Information
Because the patient remained dependent on VA-ECMO and IABP support and had refractory cardiogenic shock with severely impaired biventricular function, he was evaluated for urgent heart transplantation. Preoperative echocardiography showed an ejection fraction of approximately 12% and a tricuspid annular plane systolic excursion of 7 mm. At the time of listing, he also had active pneumonia, CRRT-dependent acute kidney injury, hyperbilirubinemia, thrombocytopenia, and evolving multiorgan dysfunction. These findings were recognized as substantial perioperative risks, particularly because postoperative immunosuppression would be required.
After multidisciplinary discussion, the transplant team considered that much of the organ dysfunction was driven by refractory cardiogenic shock and was unlikely to improve without heart replacement. The infection-related risks were substantial, but the patient remained dependent on VA-ECMO and IABP support and had limited alternative treatment options. Urgent transplantation was therefore pursued after individualized risk-benefit assessment and detailed discussion with the family.
Before transplantation, VA-ECMO was maintained through peripheral femoral cannulation, with a 17-Fr femoral arterial cannula and a 23-Fr femoral venous cannula. IABP was used as the available left-sided unloading strategy. Additional left ventricular unloading was not performed because the patient’s infection appeared clinically improved after transfer to our center and the expected waiting time for a donor heart was short.
Orthotopic heart transplantation was performed on 3 April 2024 while the patient remained on VA-ECMO and IABP support. Intraoperative findings included marked cardiomegaly and extremely poor native cardiac contractility. The operative course was reported as uneventful, and donor graft function was considered acceptable at implantation. Delayed sternal closure was not required.
The donor was a 24-year-old male donor after brain death due to traumatic brain injury. Allocation was performed through the China Organ Transplant Response System (COTRS). Donor screening for HBV, HCV, HIV, and syphilis was negative. Donor blood culture and donor blood mNGS were also negative. Donor respiratory culture, however, grew carbapenem-resistant Acinetobacter baumannii, carbapenem-resistant Pseudomonas aeruginosa, and methicillin-susceptible Staphylococcus aureus, suggesting respiratory tract colonization or localized respiratory infection rather than documented systemic donor infection. Available donor susceptibility information was reviewed during perioperative risk assessment. Because the susceptibility patterns were not fully concordant with the recipient’s later isolates, donor-derived infection could not be established on the basis of available microbiological evidence. Perioperative antimicrobial planning and post-transplant surveillance were therefore considered in relation to both recipient and donor infectious risks.
Organ procurement began at 08:00 on 3 April 2024. Aortic cross-clamping was performed at 08:20, and preservation perfusion was completed at 08:29. The heart arrived at our center at 13:46, giving an estimated cold ischemia time of approximately 390 minutes. During the early postoperative period, norepinephrine was discontinued, only low-dose epinephrine was required, and lactate remained below 2 mmol/L. Postoperative echocardiography showed acceptable graft function, with an ejection fraction of approximately 50–55%.
Microbiological Findings and Antimicrobial Treatment
Because the patient had prolonged mechanical ventilation, VA-ECMO, IABP, CRRT, multiple invasive devices, and postoperative immunosuppression, microbiological surveillance and antimicrobial adjustment were performed repeatedly during the perioperative period.
Piperacillin/tazobactam was started empirically on admission to our institution on 27 March 2024. After sputum culture on 31 March showed abundant Klebsiella pneumoniae and moderate Stenotrophomonas maltophilia, with increased inflammatory markers, treatment was changed to meropenem. Vancomycin plus meropenem was continued perioperatively after transplantation. Repeated sputum cultures continued to show S. maltophilia, and fungal culture showed a small amount of Candida albicans. On 9 April, meropenem was replaced with cefoperazone/sulbactam according to susceptibility results.
On 12 April, abdominal drainage fluid culture yielded carbapenem-resistant Acinetobacter baumannii. Tigecycline was used during 12–13 April for suspected multidrug-resistant Gram-negative intra-abdominal infection, but was replaced after bilirubin increased markedly during treatment. In the setting of abdominal distension, abdominal hypertension, and suspected enterogenic septic shock, antimicrobial therapy was escalated from 14 April to eravacycline 50 mg every 12 h, imipenem/cilastatin 0.5 g every 6 h, intravenous colistin sulfate 0.75 million units every 12 h, and caspofungin 50 mg once daily.
Subsequent blood mNGS and cultures showed polymicrobial bloodstream infection involving Burkholderia multivorans, vancomycin-resistant Enterococcus faecium, and carbapenem-resistant Klebsiella pneumoniae. On 17 April, ceftazidime/avibactam 2.5 g every 8 h was started according to the susceptibility profile of carbapenem-resistant K. pneumoniae and was continued until 27 April. Antimicrobial therapy was further adjusted according to evolving pathogens, resistance patterns, organ function, and the patient’s clinical course. All mNGS results were interpreted together with conventional culture findings, susceptibility testing, imaging, inflammatory markers, and clinical deterioration. The detailed microbiological and antimicrobial timeline is shown in Table 1.
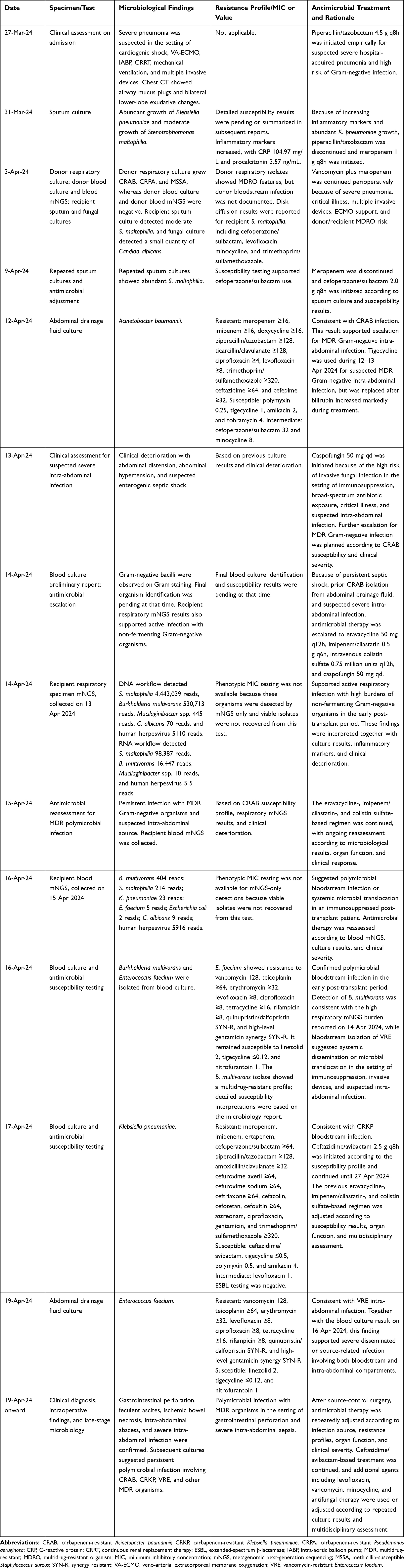 |
Table 1 Timeline of Microbiological Findings, Antimicrobial Susceptibility Profiles, and Antimicrobial Treatment Adjustments |
Postoperative Complications and Outcome
VA-ECMO was successfully weaned on 16 April 2024. During the following days, the patient developed worsening signs of systemic infection and abdominal involvement. On 19 April, head, chest, and abdominal CT revealed a right parieto-occipital cerebral infarction, a large right-sided pneumothorax, and free intraperitoneal gas suggestive of gastrointestinal perforation (Figure 1A–C).
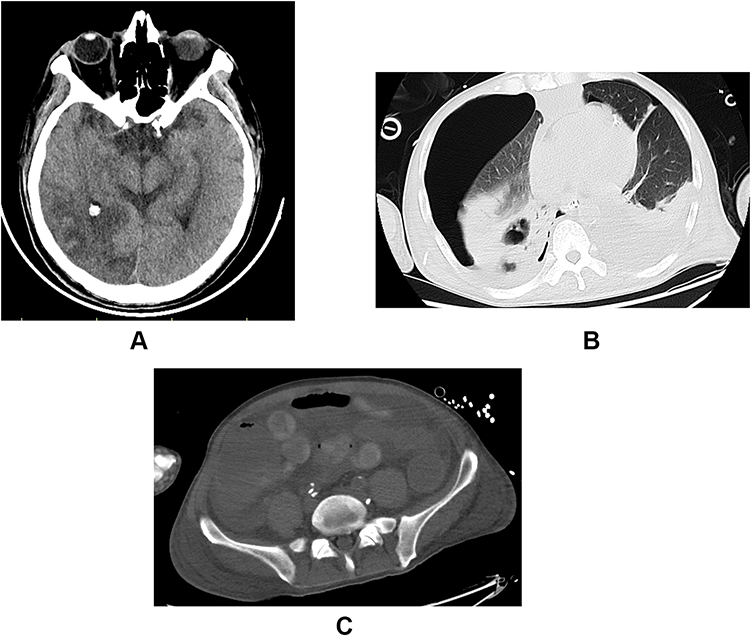 |
Figure 1 (A) Computed tomography findings on 19 April showing right parieto-occipital cerebral infarction. This finding reflected a major neurologic complication during the postoperative course and occurred in the setting of prolonged extracorporeal support, systemic infection, and coagulopathy. (B) Computed tomography findings on 19 April showing a large right-sided pneumothorax. This finding indicated acute respiratory deterioration after heart transplantation and contributed to the complexity of postoperative organ support. (C) Computed tomography findings on 19 April showing free intraperitoneal air, consistent with gastrointestinal perforation. Bowel wall edema and exudative changes in the abdominopelvic cavity were also observed. These findings prompted diagnostic abdominal paracentesis and emergency surgical source control. |
Abdominal paracentesis yielded feculent fluid, confirming enteric perforation and intra-abdominal contamination (Figure 2). Emergency laparotomy was performed, including right hemicolectomy, intra-abdominal abscess drainage, and ileostomy. Extensive ischemic bowel necrosis and severe intra-abdominal infection were found intraoperatively. Cholecystostomy was also performed. The overall clinical course, including microbiological findings, antimicrobial adjustments, major complications, and outcome, is summarized in Figure 3.
 |
Figure 2 Diagnostic abdominal paracentesis yielded feculent drainage fluid, providing direct clinical evidence of gastrointestinal perforation and enteric contamination. This finding supported the need for emergency source-control surgery, including right hemicolectomy, intra-abdominal abscess drainage, and ileostomy. |
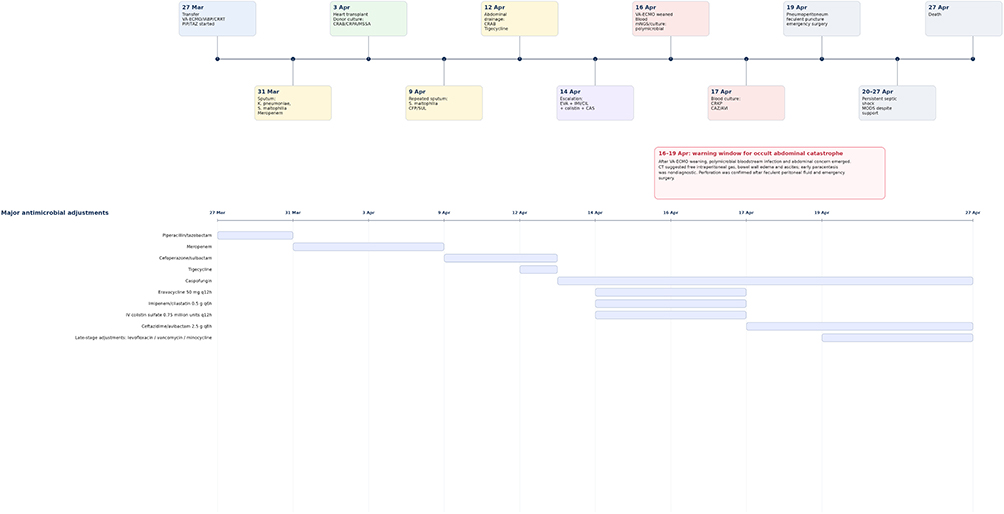 |
Figure 3 Clinical timeline of disease progression, microbiological findings, antimicrobial treatment, major complications, and outcome. The timeline shows the patient’s progression from refractory cardiogenic shock requiring IABP, VA-ECMO, and CRRT to urgent orthotopic heart transplantation, followed by polymicrobial multidrug-resistant infection, gastrointestinal perforation, emergency source-control surgery, persistent septic shock, MODS, and death. Donor respiratory culture grew CRAB, CRPA, and MSSA, while donor blood culture and blood mNGS were negative. The highlighted period from 16 to 19 April indicates the interval between VA-ECMO weaning and confirmed gastrointestinal perforation, during which polymicrobial bloodstream infection and abdominal concern emerged. The lower panel summarizes major antimicrobial treatment adjustments. Abbreviations: CAZ/AVI, ceftazidime/avibactam; CAS, caspofungin; CFP/SUL, cefoperazone/sulbactam; CRAB, carbapenem-resistant Acinetobacter baumannii; CRKP, carbapenem-resistant Klebsiella pneumoniae; CRPA, carbapenem-resistant Pseudomonas aeruginosa; CRRT, continuous renal replacement therapy; EVA, eravacycline; IABP, intra-aortic balloon pump; IMI/CIL, imipenem/cilastatin; mNGS, metagenomic next-generation sequencing; MODS, multiple organ dysfunction syndrome; MSSA, methicillin-susceptible Staphylococcus aureus; PIP/TAZ, piperacillin/tazobactam; VA-ECMO, veno-arterial extracorporeal membrane oxygenation. |
Despite vasopressor support, targeted antimicrobial therapy, source-control surgery, CRRT, plasma exchange, transfusion, and nutritional support, the patient developed refractory septic shock with progressive multiorgan dysfunction, particularly irreversible liver failure. His condition continued to deteriorate, and he died of circulatory failure on 27 April 2024.
Discussion
This case describes a rapidly progressive infectious deterioration after urgent heart transplantation in a recipient bridged with prolonged VA-ECMO.1,9 Before transplantation, the patient already had active pneumonia, prolonged ICU exposure, multiple invasive devices, broad antimicrobial exposure, and dependence on VA-ECMO, IABP, and CRRT. Although his condition appeared transiently stabilized before transplantation, he soon developed polymicrobial bloodstream infection, gastrointestinal perforation with feculent peritonitis, refractory septic shock, and fatal multiple organ dysfunction after surgery.
The clinical importance of this case lies in the convergence of several risks within a short postoperative period: partially controlled recipient infection, extracorporeal support, postoperative immunosuppression, donor respiratory MDRO colonization, intestinal hypoperfusion, and delayed definitive source control. The case also reflects a difficult decision commonly encountered in urgent transplantation: whether to proceed when infection has improved clinically but cannot be regarded as fully eradicated, and how donor respiratory MDRO findings should be incorporated into perioperative risk assessment and post-transplant surveillance.
Donor Respiratory MDRO Colonization and Its Implications
Donor respiratory microbiology was one of the key concerns in this case. Donor respiratory culture grew carbapenem-resistant Acinetobacter baumannii, carbapenem-resistant Pseudomonas aeruginosa, and methicillin-susceptible Staphylococcus aureus, whereas donor blood culture and blood mNGS were negative. The recipient subsequently developed carbapenem-resistant A. baumannii infection, making donor-derived transmission an important consideration. However, strain-level molecular typing between the donor respiratory A. baumannii isolate and the recipient post-transplant isolate was not performed. Therefore, donor-derived transmission could not be confirmed or excluded.
The available susceptibility profiles were not fully concordant between the donor respiratory isolates and the recipient’s later isolates, making direct donor transmission less certain based on available microbiological evidence. Even so, donor respiratory MDRO colonization remained clinically relevant. The recipient already had active pneumonia, prolonged ICU exposure, broad antimicrobial exposure, VA-ECMO/IABP support, CRRT, and evolving organ dysfunction; in this context, donor respiratory colonization further increased the complexity of perioperative infection risk assessment.
Respiratory colonization in a donor does not necessarily preclude organ use, especially when blood culture and blood mNGS show no evidence of systemic donor infection and the recipient has no durable alternative (4, 10). However, such findings should not be treated as incidental. They should prompt careful review of donor susceptibility data where available, adjustment of perioperative antimicrobial planning, closer post-transplant microbiological surveillance, and cautious interpretation of early postoperative MDRO emergence.11 In this case, the donor respiratory culture results were considered during donor-recipient risk assessment, but the absence of strain-level comparison limited the ability to determine whether subsequent recipient infection was donor-derived.
Transplant Candidacy in a Rapidly Deteriorating Recipient
The case also raises the question of transplant candidacy in VA-ECMO-supported patients with active infection and evolving organ dysfunction.3 Before transplantation, this patient had severe pneumonia, suspected bloodstream infection, CRRT-dependent acute kidney injury, hyperbilirubinemia, thrombocytopenia, and multiorgan dysfunction. These findings clearly increased perioperative risk, particularly under the immunosuppression required after transplantation.
The transplant team considered that much of the organ dysfunction was driven by refractory cardiogenic shock and was unlikely to reverse without heart replacement. In such situations, the decision is not simply whether infection is present, but whether infection is sufficiently controllable to justify transplantation in the face of otherwise fatal cardiac failure. This distinction is important because short-term clinical improvement does not necessarily mean microbiological eradication, especially in patients with invasive devices, respiratory colonization, and prolonged critical illness.
Mechanical support optimization is another issue raised by this case. The patient had severe left ventricular dysfunction while receiving VA-ECMO and IABP. IABP was used as the available left-sided unloading strategy, and additional unloading procedures such as transseptal left atrial drainage, direct LV venting, or Impella support were not performed. After transfer to our center, infection appeared clinically improved and the expected waiting time for donor heart availability was short. Nevertheless, in VA-ECMO-supported candidates with severe LV dysfunction, left ventricular distension, pulmonary congestion, and adequacy of unloading should be reassessed repeatedly. Insufficient unloading may worsen pulmonary edema and create a less favorable respiratory environment for infection control.12–14
Progression to Polymicrobial Sepsis and Critical Complications
Several factors likely contributed to the rapid infectious progression after transplantation. The patient had prolonged pre-transplant ICU exposure, mechanical ventilation, VA-ECMO, IABP, CRRT, and repeated broad-spectrum antimicrobial therapy. These factors favored MDRO acquisition and persistence. Postoperative immunosuppression further weakened host defense, and infection progressed from respiratory involvement to polymicrobial bloodstream infection involving Stenotrophomonas maltophilia, Burkholderia multivorans, carbapenem-resistant A. baumannii, carbapenem-resistant Klebsiella pneumoniae, and vancomycin-resistant Enterococcus faecium.
mNGS was useful in this setting because it revealed the breadth of potential pathogens earlier than conventional culture alone.8,15,16 However, the results required careful interpretation. In this case, mNGS was not used as a stand-alone basis for antimicrobial decisions. It was interpreted alongside conventional cultures, susceptibility testing, imaging findings, inflammatory markers, and clinical deterioration. Culture results remained essential because they confirmed viable pathogens and provided phenotypic susceptibility data. This distinction is particularly important in critically ill transplant recipients, because mNGS cannot reliably distinguish colonization, contamination, nonviable organisms, or invasive infection, and it does not provide MIC values.
Gastrointestinal perforation on postoperative day 16 became the decisive turning point. Pneumoperitoneum and feculent fluid on paracentesis confirmed enteric perforation with severe intra-abdominal contamination. Emergency surgery revealed ischemic bowel necrosis and severe peritonitis. Although surgical source control was attempted, the patient had already progressed to refractory septic shock and irreversible multiorgan failure. The intestinal ischemia was probably multifactorial, related to prolonged hypoperfusion, vasoactive therapy, coagulopathy, critical illness, and the effects of postoperative immunosuppression.17
The interval between VA-ECMO weaning on 16 April and confirmed gastrointestinal perforation on 19 April should be viewed as a warning period rather than a clinically silent interval. During this period, the patient developed abdominal distension, concern for intra-abdominal hypertension, gastrointestinal bleeding or positive fecal occult blood, elevated inflammatory markers, and rising lactate. Abdominal CT suggested free intraperitoneal gas, bowel wall edema, abdominopelvic exudative changes, and ascites. Early paracentesis did not confirm gastrointestinal perforation, and thoracic air tracking into the abdominal cavity after thoracic surgery was also considered. The diagnosis became definitive only after feculent peritoneal fluid was obtained and emergency surgery confirmed ischemic bowel necrosis and severe peritonitis. This sequence supports repeated abdominal examination, repeat imaging, and early surgical reassessment in VA-ECMO-supported transplant recipients with polymicrobial bacteremia, abdominal distension, gastrointestinal bleeding, rising lactate, or unexplained septic shock, even when an initial puncture is nondiagnostic.18
Neurologic Complication in the Setting of VA-ECMO and Sepsis
The right parieto-occipital cerebral infarction identified on 19 April was another clinically relevant complication. Neurologic events may occur during VA-ECMO support, particularly in the presence of systemic inflammation, coagulopathy, hemodynamic instability, and complex anticoagulation management.19,20 In this patient, the infarction likely reflected the broader thrombo-inflammatory and perfusion-related vulnerability during prolonged extracorporeal support and septic deterioration. Although it was not the immediate cause of death, it added to the overall burden of postoperative organ dysfunction.
Clinical Implications
Several clinical implications can be drawn from this case. Preoperative infection assessment in VA-ECMO-bridged candidates should not rely only on transient clinical improvement. The possibility of persistent infection or colonization under postoperative immunosuppression should be considered, particularly when MDROs, invasive devices, and prolonged ICU exposure are present. Donor respiratory MDRO colonization also deserves explicit consideration during organ acceptance and perioperative planning, even when donor blood testing is negative.
After transplantation, polymicrobial bacteremia, unexplained septic shock, abdominal distension, gastrointestinal bleeding, rising lactate, or escalating vasoactive requirements should prompt early evaluation for an occult abdominal source. In parallel, adequacy of left ventricular unloading during VA-ECMO support should be reassessed, since unresolved pulmonary congestion may worsen respiratory infection control. For patients with this level of complexity, infection management requires continuous coordination among transplant surgery, intensive care, infectious diseases, microbiology, and abdominal surgery teams.
Conclusions
Perioperative infection management in VA-ECMO-bridged heart transplant recipients cannot depend solely on broad-spectrum antimicrobial coverage. Donor respiratory MDRO colonization does not automatically preclude organ acceptance when donor blood testing is negative, but it should lead to careful donor-recipient risk assessment, tailored antimicrobial planning, and intensified post-transplant surveillance.
In candidates with active pneumonia, suspected bloodstream infection, or evolving organ dysfunction, “controlled infection” should be assessed dynamically rather than inferred from short-term clinical improvement alone. Persistent colonization, recent culture and mNGS findings, susceptibility profiles, invasive device burden, and feasibility of source control should be considered before urgent transplantation.
After transplantation, particularly after prolonged VA-ECMO support, clinicians should maintain a low threshold for evaluating occult abdominal complications. Polymicrobial bacteremia, unexplained septic shock, abdominal distension, escalating vasopressor requirements, rising lactate, increased nasogastric output, or elevated intra-abdominal pressure should prompt early assessment for mesenteric ischemia or gastrointestinal perforation. Close multidisciplinary collaboration is essential to optimize antimicrobial therapy, adjust immunosuppression, provide organ support, and achieve timely source control.
Statistical Analysis
No statistical analysis was performed because this study was a single-patient case report without group comparisons, hypothesis testing, or inferential analysis. Clinical, laboratory, microbiological, imaging, treatment, and outcome data were summarized descriptively.
Data Sharing Statement
All relevant data generated or analyzed during this case report are included in this article.
Ethics Approval and Consent to Participate
This case report was reviewed and approved by the Ethics Committee of the First Affiliated Hospital, Zhejiang University School of Medicine ([2025B] IIT Ethics Approval No. 0198). Institutional approval was required and obtained for publication of the case details. The patient was critically ill and lacked decision-making capacity during hospitalization and subsequently passed away.
Consent for Publication
Written informed consent for publication of this case report, including the case details and any accompanying clinical information or images, was obtained from the patient’s spouse, who was the legally authorized representative and next of kin. All patient-related data were anonymized and handled confidentially.
Acknowledgments
The authors would like to thank Director Wenqiao Yu and the treatment team of the Comprehensive Intensive Care Unit, The First Affiliated Hospital, Zhejiang University School of Medicine, for their invaluable expertise and support during the management of this case.
Author Contributions
Yangyang Jia, Yue Zhu, and Hongliu Cai contributed to validation. Yangyang Jia and Yue Zhu contributed to writing the original draft, review and editing, and visualization. Yue Zhu contributed to the methodology for diagnostic verification. All authors made a significant contribution to the work reported, whether in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
No external funding was received for this report.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Tan Z, Zeng LA. Post-operative infection in mechanical circulatory support patients. Ann Transl Med. 2020;8(13):831. doi:10.21037/atm-20-1748
2. Shah MM, Rando H, Polanco AR, Kilic A. ECMO as a bridge to heart transplantation: insights into stratification by heart failure etiology. JHLT Open. 2024;5:100097. doi:10.1016/j.jhlto.2024.100097
3. Mehra MR, Canter CE, Hannan MM, et al. The 2016 International Society for Heart Lung Transplantation listing criteria for heart transplantation: a 10-year update. J Heart Lung Transplant. 2016;35(1):1–14. doi:10.1016/j.healun.2015.10.023
4. Anesi JA, Blumberg EA, Han JH, et al. Impact of donor multidrug-resistant organisms on solid organ transplant recipient outcomes. Transpl Infect Dis. 2022;24(1):e13783. doi:10.1111/tid.13783
5. Bahakel H, Madan RP, Danziger-Isakov L. Approach to suspected donor-derived infections. Front Pediatr. 2023;11:1265023. doi:10.3389/fped.2023.1265023
6. Gardiner BJ, Ison MG. Donor-derived infections in heart and lung transplant recipients. JHLT Open. 2025;10:100376. doi:10.1016/j.jhlto.2025.100376
7. Wu H, Cao H, Gao X, et al. The role of metagenomic next-generation sequencing in diagnosing and managing post-kidney transplantation infections. Front Cell Infect Microbiol. 2024;14:1473068. doi:10.3389/fcimb.2024.1473068
8. Yang H, Xu N, Yan M, et al. Comparison of metagenomic next-generation sequencing and conventional culture for the diagnostic performance in febrile patients with suspected infections. BMC Infect Dis. 2024;24(1):350. doi:10.1186/s12879-024-09236-w
9. López-Vilella R, Pérez-Guillén M, Guerrero-Cervera B, et al. Comparative temporal analysis of morbidity and early mortality in heart transplantation with extracorporeal membrane oxygenation support: exploring trends over time. Biomedicines. 2024;12(9):2109. doi:10.3390/biomedicines12092109
10. Eldin C, Grossi PA, Manda V, et al. Updates on donor-derived infection in solid organ transplantation, report from the 2024 GTI (Infection and Transplantation Group) Annual Meeting. Transpl Int. 2025;38:14237. doi:10.3389/ti.2025.14237
11. Ison MG, Grossi P. AST Infectious Diseases Community of Practice. Donor-derived infections in solid organ transplantation. Am J Transplant. 2013;13(4):22–30. doi:10.1111/ajt.12095
12. Lorusso R, Meani P, Raffa GM, Kowalewski M. Extracorporeal membrane oxygenation and left ventricular unloading: what is the evidence? JTCVS Tech. 2022;13:101–114. doi:10.1016/j.xjtc.2022.02.039
13. Lim Y, Kim MC, Jeong IS. Left ventricle unloading during veno-arterial extracorporeal membrane oxygenation: review with updated evidence. Acute Crit Care. 2024;39(4):473–487. doi:10.4266/acc.2024.00801
14. Ezad SM, Ryan M, Donker DW, et al. Unloading the left ventricle in venoarterial ECMO: in whom, when, and how? Circulation. 2023;147(16):1237–1250. doi:10.1161/CIRCULATIONAHA.122.062371
15. Huang JF, Miao Q, Cheng JW, et al. Metagenomic next-generation sequencing versus traditional laboratory methods for the diagnosis and treatment of infection in liver transplantation. Front Cell Infect Microbiol. 2022;12:886359. doi:10.3389/fcimb.2022.886359
16. Wang Q, Ding H, Hao Z, Liao G. Metagenomic next-generation sequencing enhances diagnosis of fungal infections in kidney transplant recipients: a retrospective study. Front Cell Infect Microbiol. 2026;15:1667475. doi:10.3389/fcimb.2025.1667475
17. Renaudier M, de Roux Q, Bougouin W, et al. Acute mesenteric ischaemia in refractory shock on veno-arterial extracorporeal membrane oxygenation. Eur Heart J Acute Cardiovasc Care. 2021;10(1):62–70.
18. Reintam Blaser A, Coopersmith CM, Acosta S. Managing acute mesenteric ischaemia. Intensive Care Med. 2024;50(4):593–596. doi:10.1007/s00134-024-07363-1
19. Iacobelli R, Fletcher-Sandersjöö A, Lindblad C, et al. Predictors of brain infarction in adult patients on extracorporeal membrane oxygenation: an observational cohort study. Sci Rep. 2021;11(1):3809. doi:10.1038/s41598-021-83157-5
20. Pisano DV, Ortoleva JP, Wieruszewski PM. Short-term neurologic complications in patients undergoing extracorporeal membrane oxygenation support: a review on pathophysiology, incidence, risk factors, and outcomes. Pulm Ther. 2024;10(3):267–278. doi:10.1007/s41030-024-00265-z
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.