Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 19
Polyethylene Glycol Loxenatide Selectively Reduces Adiposity While Preserving Lean Body Mass in Type 2 Diabetes: A 12-Week Clinical Study
Authors Gu R, Zhou Y, Kong X, Luo Y, Li H ![]() , Ma J
, Ma J ![]()
Received 10 January 2026
Accepted for publication 24 June 2026
Published 10 July 2026 Volume 2026:19 592044
DOI https://doi.org/10.2147/DMSO.S592044
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Halis Akturk
Rong Gu, Yunting Zhou, Xiaocen Kong, Yong Luo, Huiqin Li, Jianhua Ma
Department of Endocrinology, Nanjing First Hospital, Nanjing Medical University, Nanjing, 210012, People’s Republic of China
Correspondence: Huiqin Li, Email [email protected] Jianhua Ma, Email [email protected]
Objective: To investigate the effects of polyethylene glycol loxenatide (PEX168) on visceral and body fat, as well as glycolipid metabolism, in patients with type 2 diabetes mellitus (T2DM).
Methods: A prospective interventional study design was adopted. A total of 100 patients with type 2 diabetes mellitus (T2DM) who visited the outpatient clinic of the Department of Endocrinology, Nanjing First Hospital, Nanjing Medical University, between January and December 2023 were enrolled. On the basis of their original glucose-lowering regimen, polyethylene glycol loxenatide (PEX168) 0.2 mg was administered subcutaneously once weekly for 12 weeks. Ninety-nine patients (68 males, 31 females; mean age 53.48 ± 11.36 years) completed the 12-week treatment, while one patient was lost to follow-up. Among them, 16 patients extended treatment to one year. Glycemic parameters [glycosylated hemoglobin (HbA1c), fasting blood glucose (FBG)], continuous glucose monitoring profiles, and 25-hydroxyvitamin D (25-OH-VD) levels were assessed before and after treatment. Body composition, including visceral fat area (VFA), skeletal muscle mass, and lean body mass, was measured using bioelectrical impedance analysis. Paired t-test or Wilcoxon signed-rank test was used to compare differences before and after treatment.
Results: After 12 weeks of treatment compared with baseline, improvements were observed in glycosylated hemoglobin (8.8 ± 1.11% vs 6.9 ± 0.92%, P < 0.001), fasting blood glucose (9.6 ± 2.65 mmol/L vs 7.2 ± 1.71 mmol/L, P < 0.001), body weight (75.5 ± 12.67 kg vs 74.7 ± 12.78 kg, P = 0.003), BMI (27.1 ± 3.03 kg/m2 vs 26.8 ± 3.05 kg/m2, P = 0.025), body fat mass (23.9 ± 6.12 kg vs 23.0 ± 5.86 kg, P = 0.002), VFA (120.0 ± 36.04 cm2 vs 113.7 ± 32.90 cm2, P = 0.001), and 25-OH-VD levels (48.88 [41.99, 57.88] nmol/L vs 51.60 [45.55, 64.17] nmol/L, P = 0.002). Lean body mass (LBM) remained unchanged.
Conclusion: PEX168 treatment for 12 weeks not only effectively improves glycemic control, lipid profiles, and glycemic variability in patients with T2DM, but also significantly reduces visceral fat, ameliorates central obesity, and preserves skeletal muscle mass, thereby achieving “high-quality weight loss.”.
Clinical Trial Registration: www.clinicaltrials.gov identifier is NCT05611684.
Keywords: polyethylene glycol loxenatide, type 2 diabetes, visceral fat, lean body mass preservation
Introduction
Diabetes mellitus is a group of chronic endocrine and metabolic diseases characterized primarily by persistent hyperglycemia,1,2 with complex etiology involving the interaction between genetic and environmental factors. Both type 1 diabetes and type 2 diabetes are its clinical classifications, and recent studies have suggested that inflammatory responses play an important role in the development and progression of both subtypes.3,4 Energy metabolism imbalance is a key driver of type 2 diabetes,5 and insulin, as a core hormone regulating glucose homeostasis,6 exhibits dysfunction throughout the entire course of the disease. Studies show that the prevalence of diabetes in China has risen sharply, increasing from 7.53% in 2005 to 13.7% in 2023.7 According to the statistics of the International Diabetes Federation (IDF), in 2024, approximately 589 million adults aged 20 to 79 years worldwide were living with diabetes, a number projected to rise to 853 million by 2050.8 From 1990 to 2021, the global prevalence of overweight and obesity increased significantly—by 155.1% (95% uncertainty intervals [UI] 149.8–160.3) in men and 104.9% (95% UI 100.9–108.8) in women. By 2050, the global population affected by overweight and obesity is expected to reach 3.8 billion (95% UI 3.39–4.04), representing over half of the projected global adult population at that time. In 2021, China reported the highest absolute number of individuals with overweight and obesity globally, totaling 402 million. The prevalence rates were 36.6% in men and 42.5% in women, highlighting a pressing public health challenge.9
The primary pathophysiological feature of type 2 diabetes mellitus (T2DM) is relative insulin deficiency resulting from insulin resistance and β-cell dysfunction. Among diabetic patients, 95% have type 2 diabetes that is characterized by insulin resistance, βcell dysfunction, and obesity resulting from excess caloric intake and insufficient physical activity.10 T2DM is frequently accompanied by overweight and obesity, and abnormal accumulation and distribution of adipose tissue directly contribute to the onset and progression of the disease. In China, the proportions of diabetic patients with overweight, obesity, and central obesity are 41%, 24.3%, and 45.4%, respectively.11 A retrospective analysis of 25,454 patients diagnosed with T2DM before 2020 from the 3B (Blood glucose, Blood pressure, and Blood lipid) database revealed that the combined prevalence of overweight and obesity among Chinese T2DM patients was 58.3%.12
Epidemiological data indicate that obesity markedly elevates diabetes risk, with a 7-fold increase in men and a 12-fold increase in women.13 This association is mediated by adipocyte-derived free fatty acids, which contribute to insulin resistance and β-cell dysfunction.14 Given that approximately 90% of T2DM patients are overweight or obese,15 the synergistic effect of these conditions amplifies mortality risk 7-fold.16 Notably, conventional therapies including insulin and sulfonylureas often promote further weight gain, potentially counteracting metabolic benefits.15 In managing overweight and obesity in diabetic patients, treatment goals should extend beyond simple weight reduction to include optimizing body fat composition, reducing visceral fat area (VFA), and improving fat distribution patterns.
In recent years, since glucagon-like peptide-1 receptor agonists (GLP-1RAs) have significant hypoglycemic effects and multiple benefits for diabetic patients, they have been recommended in major guidelines.17 GLP-1 RAs are enteric insulinotropic hypoglycemic agents that promote insulin secretion in a glucose-dependent manner while inhibiting glucagon secretion. They delay gastric emptying and reduce food intake through centralized appetite suppression, thereby contributing to blood glucose reduction.18,19 In addition to their potent glucose-lowering effects and low risk of hypoglycemia when used alone, GLP-1 RAs also promote weight loss, reduce blood pressure, and improve lipid profiles.20 For example, the GLP-1 receptor agonist liraglutide has the capacity to reduce weight by modifying the structure of the gut microbiota.21 GLP-1RAs are known not only for their efficacy in reducing hyperglycemia and body weight in metabolic disorders such as T2DM and obesity but also for their growing role in regulating inflammatory signaling cascades that contribute to insulin resistance.22 For patients with T2DM and established atherosclerotic cardiovascular disease (ASCVD) or those at high risk for ASCVD, the 2026 American Diabetes Association (ADA) guidelines recommend prioritizing GLP-1 RAs or sodium-glucose cotransporter 2 inhibitors (SGLT2i) that have demonstrated evidence of cardiovascular benefit.23
Polyethylene glycol loxenatide (PEX168) is a novel member of the GLP-1RAs class derived from exenatide.24 The peptide backbone of PEX168 comprises 39 amino acids based on exendin‑4. Strategic modifications were introduced to mitigate DPP‑4‑mediated inactivation: Ala for Gly2, norleucine for Met14, Gln for Asn28, and Cys for Ser39. The introduced cysteine residue serves as an attachment site for branched polyethylene glycol (PEG), enhancing the molecule’s metabolic stability.25 PEG-168 has multiple therapeutic advantages. In terms of its mechanism of action, PEG-168 exerts hypoglycemic effects by stimulating insulin secretion, inhibiting glucagon secretion, improving insulin resistance, and enhancing β‑cell function via activation of the insulin phosphatidylinositol 3‑kinase/protein kinase B (PI3K/AKT) pathway.17 PEX168 was developed by Jiangsu Haosen Pharmaceuticals Co., Ltd. and is part of a series of GLP-1 RA preparations independently developed in China. Despite its therapeutic potential, there is limited research on the effects of GLP-1 RAs on visceral fat both in China and abroad. The purpose of this study was to investigate the effects of PEX168 on glucose and lipid metabolism, and visceral fat, in patients with T2DM.
Materials and Methods
Study Design
This was a single center study conducted between January 2023 and December 2023 at the Department of Endocrinology, Nanjing First Hospital, Nanjing Medical University, China. This study was approved by the Ethics Committee of Nanjing First Hospital (KY20230310-11). All procedures were conducted in accordance with the Declaration of Helsinki (1964), as revised in 2013. Informed consent was obtained from all participants. The study was registered at ClinicalTrial.gov under registration number NCT05611684.
Patient Population
Patients with type 2 diabetes mellitus (T2DM) who visited the Department of Endocrinology at Nanjing First Hospital, Nanjing Medical University, between January 2023 and December 2023 were enrolled in the study.
The inclusion criteria were as follows: (1) diagnosis of T2DM according to the 1999 WHO criteria;26 (2) patients who had received at least 8 weeks of simple dietary control and physical exercise before screening, with stable doses of oral antidiabetic drugs (thiazolidinedione, sulfonylurea, glinide, or α-glucosidase inhibitor) and/or insulin during the 8 weeks before screening; (3) patients with glycosylated hemoglobin (HbA1c) ≥7.5%; (4) patients with body mass index (BMI) >24 kg/m2; (5) patients who agreed to maintain stable dietary habits and regular physical activity levels during the study period, and to comply with the guidance provided by diabetes specialist nurses.
The exclusion criteria were as follows: (1) use of any of the following drugs or treatments within 1 year prior screening: GLP-1 RAs, glucagon-like peptide-1 (GLP-1) analogs, dipeptidyl peptidase-4 inhibitors, or any other incretin analogs; (2) Long-term use (more than 7 consecutive days) of intravenous, oral, or intra-articular corticosteroids within 2 months before screening; (3) used medications for weight control or underwent surgery that could cause body weight fluctuations within 2 months before screening or were currently enrolled in a weight loss program and had not yet reached the maintenance stage; (4) history of acute or chronic pancreatitis, history of medullary C cell carcinoma, multiple endocrine neoplasia (MEN) type 2A or 2B syndrome, or relevant family history; (5) clinically significant abnormal gastric emptying; (6) any treated or untreated malignant tumor of any organ system diagnosed within 5 years before screening (excluding non-melanoma skin cancer); (7) history of coronary angioplasty, coronary artery stenting, coronary artery bypass grafting, decompensated heart failure (New York Heart Association, NYHA class III or IV), stroke, transient ischemic attack, unstable angina pectoris, myocardial infarction, or persistent and clinically significant arrhythmia within 6 months before screening; (8) acute metabolic complications (eg., diabetic ketoacidosis, hyperosmolar hyperglycemic state) within 6 months before screening; (9) laboratory test indicators before screening meeting any of the following: alanine aminotransferase or aspartate aminotransferase >2.5 times the normal value, estimated glomerular filtration rate <45 mL/min/1.73 m2, fasting triglyceride >5.64 mmol/L.
Intervention
After enrollment, patients with T2DM routinely received training in diabetes self-management education and lifestyle interventions provided by the nursing staff of our department (with at least 5 years of clinical experience in diabetes care). Without altering their original hypoglycemic regimen, PEX168 at a dose of 0.2 mg was added as a subcutaneous injection once a week. The treatment duration was 12 weeks. Changes in various indicators before and after 12 weeks of treatment were observed. The primary endpoint of this protocol was the magnitude of change in visceral fat area from baseline after 12 weeks of treatment.
Data Collection
R.G and Y.Z collected the patients’ clinical data, including age, gender, duration of diabetes, and the types and dosages of hypoglycemic agents.
For height measurement: subjects were instructed to remove hats, shoes, coats, mobile phones, keys, and other items. They stood upright on a height‑weight scale with their back against the measuring ruler, eyes looking forward horizontally, and keeping the head, buttocks, and heels aligned. The observer’s line of sight was level with the measuring slider. Height (m) and body weight (kg) were recorded. Body mass index (BMI) was calculated as weight (kg) divided by height squared (m2).
For waist and hip circumference measurement:
Waist circumference (cm): Patients stood upright with feet separated. The measuring tape was placed horizontally at the midpoint between the upper border of the iliac crest and the lower border of the 12th rib (the narrowest part of the abdomen), and the circumference was measured.
Hip circumference (cm): Patients stood upright with legs together. The measuring tape was placed horizontally around the widest part of the buttocks, and the circumference was measured.
Blood samples were collected after an overnight fast of at least 8 hours.
Measurement of Glucose Metabolism-Related Indicators
Fasting blood glucose (FBG) was measured using the glucose oxidase method with a Beckman automatic biochemical analyzer (Au5800). HbA1c was determined by high-performance liquid chromatography (Bio-Rad D100). Fasting C-peptide (FC-P) and fasting insulin (FINS) levels were measured using chemiluminescence immunoassay (Abbott I2000).
Measurement of Lipid Metabolism-Related Indicators
Total cholesterol (TC), triglycerides (TG), high-density lipoprotein (HDL), low-density lipoprotein (LDL), serum total protein (TP), and albumin (ALB) were measured using enzymatic assays on the Beckman automatic biochemical detector (Au5800). Body composition analysis was performed on patients using the InBody 770 analyzer, which employs the bioelectrical impedance analysis method. The device utilizes multi-electrode and multi-frequency segmental measurements to determine impedance. Participants were required to be in a fasting state and to refrain from vigorous physical activity prior to testing. While wearing light clothing and having removed their shoes and socks, they stood with their feet placed on the foot-shaped electrodes and held the hand electrodes for 1–2 minutes to complete the measurement. The test results included parameters such as body weight, body fat percentage, visceral fat area (VFA), total muscle mass, skeletal muscle mass, and fat mass. Skeletal muscle mass index (SMI) was calculated as skeletal muscle mass of the limbs (kg)/height (m2), and fat mass index (FMI) as body fat mass (kg)/height (m2).
Measurement of Vitamin D
25-hydroxyvitamin D (25- OH-VD) was measured using enzyme-linked immunosorbent assay: The 25- OH-VD monoclonal antibody was immobilized on a solid-phase carrier, enabling qualitative or quantitative analysis based on the specific binding between the antibody and antigen.
Evaluation of Islet Function
The homeostasis model assessment for insulin resistance (HOMA-IR) was calculated as HOMA-IR = FINS × FBG / 22.5. The homeostasis model assessment for insulin sensitivity (HOMA-IS) was calculated as HOMA-IS = 1 / HOMA-IR. The homeostasis model assessment for pancreatic β-cell function (HOMA-β) was calculated as HOMA-β = 20 × FINS / (FBG – 3.5).
Statistical Analysis
All the data collected in this study were analyzed using SPSS Version 27.0. Normally distributed continuous variables were expressed as mean ± standard deviation (SD), while non-normally distributed variables were expressed as median (interquartile range). Comparisons were examined using the Student’s t-test and the Mann–Whitney U-test (nonparametric distribution). A P value < 0.05 was considered statistically significant.
Results
Baseline Characteristics
A total of 99 subjects completed the study (one patient was lost to follow-up), among whom 16 completed a one-year follow-up. (The study flowchart is presented in Figure 1).No adverse events leading to discontinuation or deaths occurred during the study. The baseline data, including age, gender, duration of diabetes, types and proportions of oral medications, HbA1c, and FBG, are presented in Table 1.
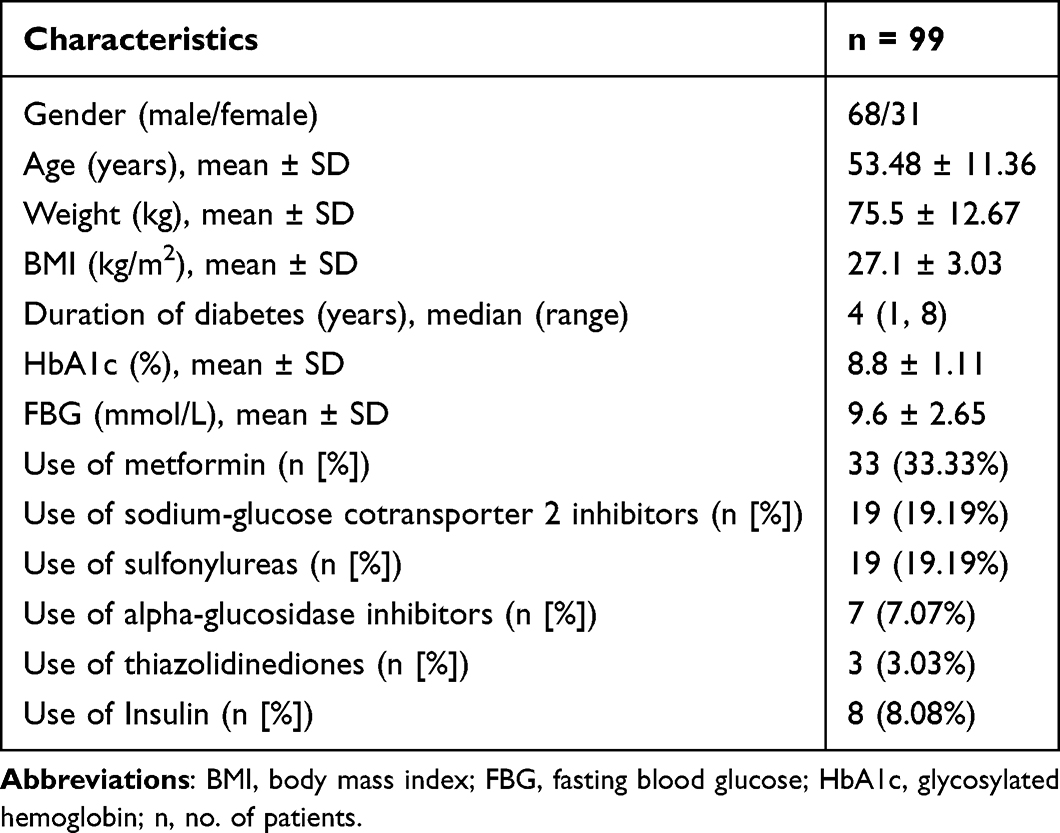 |
Table 1 Baseline Demographics and Clinical Characteristics of the Patients |
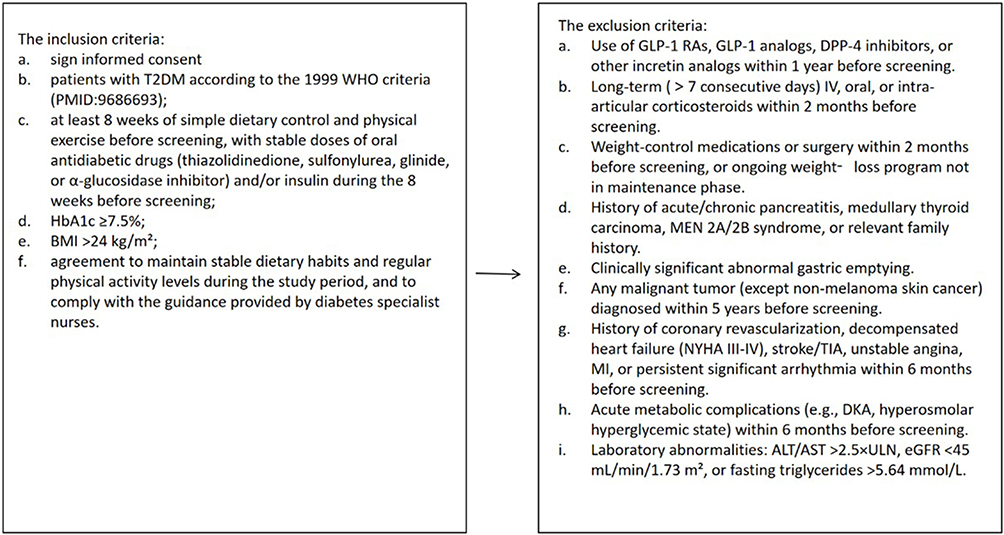 |
Figure 1 The study flowchart. |
Glucose Metabolism Analysis
After 12 weeks of intervention, patients with T2DM demonstrated statistically significant reductions in FBG, HbA1c, and HOMA-IR (P < 0.05). The levels of FC-P and HOMA-β increased, and the differences were statistically significant (P < 0.05). The details are presented in Table 2.
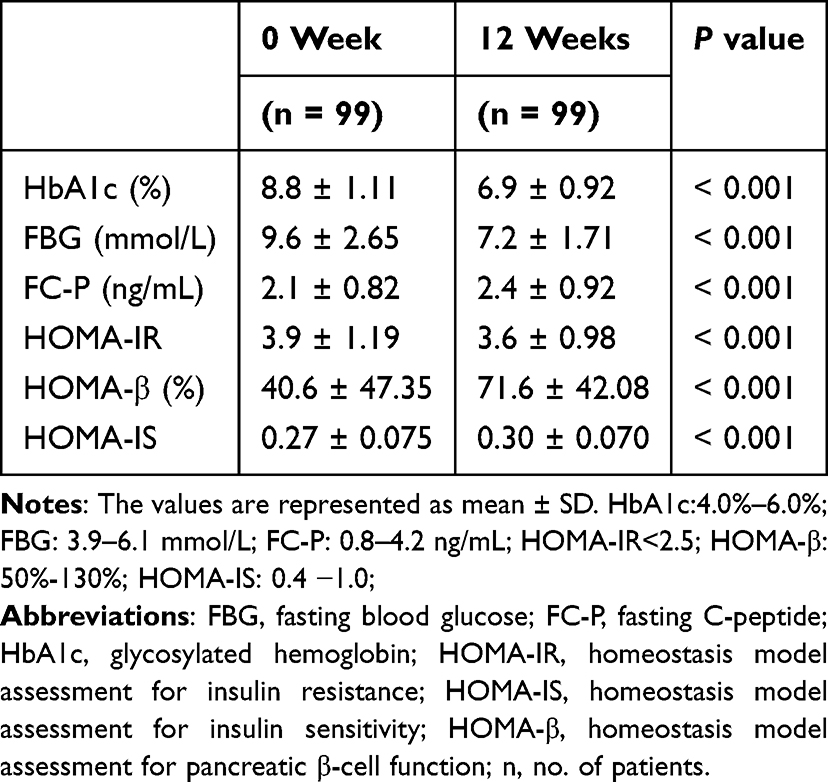 |
Table 2 Comparison of Glucose Metabolism–Related Indicators |
Body Composition Analysis
After 12 weeks of intervention, body weight, BMI, and waist-to-hip ratio of patients with T2DM significantly decreased compared with baseline. The differences were statistically significant (P < 0.05). The body fat mass, VFA, and FMI of patients with T2DM were significantly reduced compared with baseline values, and the differences were statistically significant (P < 0.05). The percentage of body fat decreased. Lean body mass (LBM) and skeletal muscle mass increased, but there was no statistical difference (P > 0.05). The details are presented in Table 3. Sixteen patients completed the 12-month treatment. The results showed that the lean body mass increased significantly from 51.41 ± 12.87 kg to 55.52 ± 11.44 kg (P < 0.05). The skeletal muscle mass increased from 29.24 ± 6.55 kg to 30.83 ± 6.81 kg, with a statistically significant difference (P < 0.05). The body fat percentage decreased from 32.34 ± 5.05 to 29.45 ± 6.84, with a statistically significant difference (P < 0.05). The visceral fat area, waist-to-hip ratio, and body fat mass decreased, but the differences were not statistically significant (P > 0.05). The details are presented in Table 4.
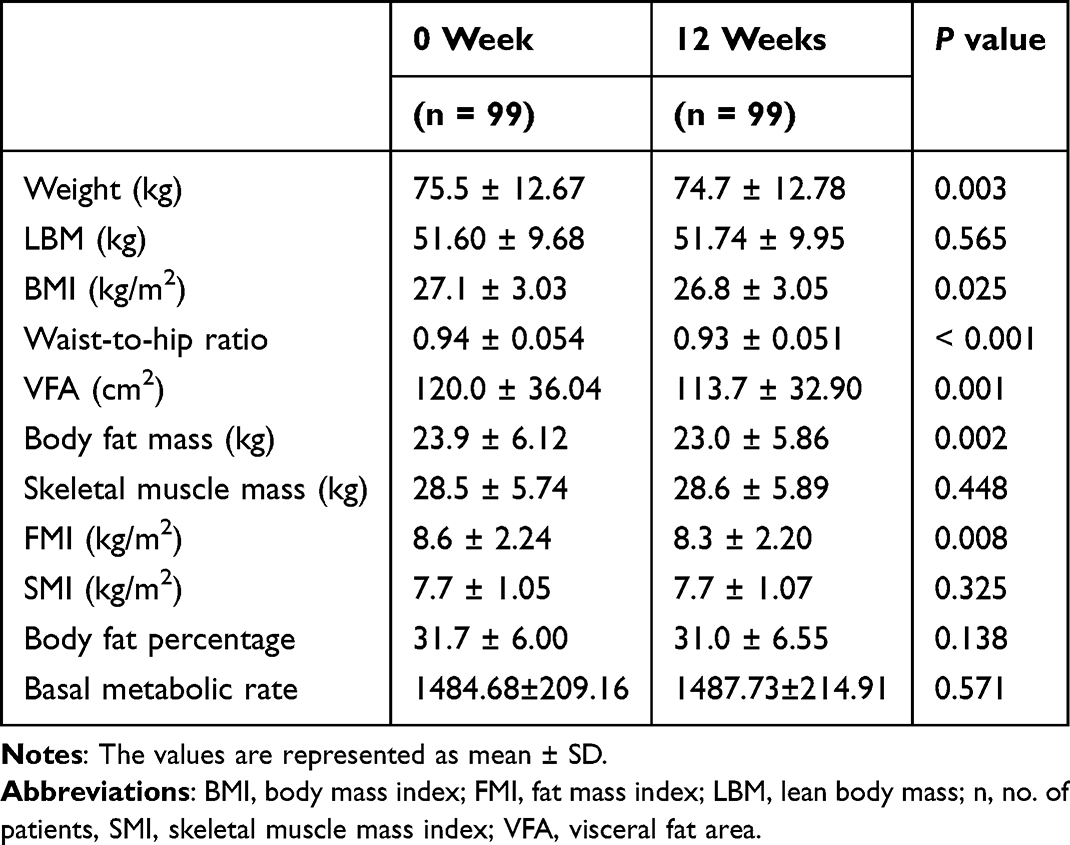 |
Table 3 Comparison of Body Composition Indicators |
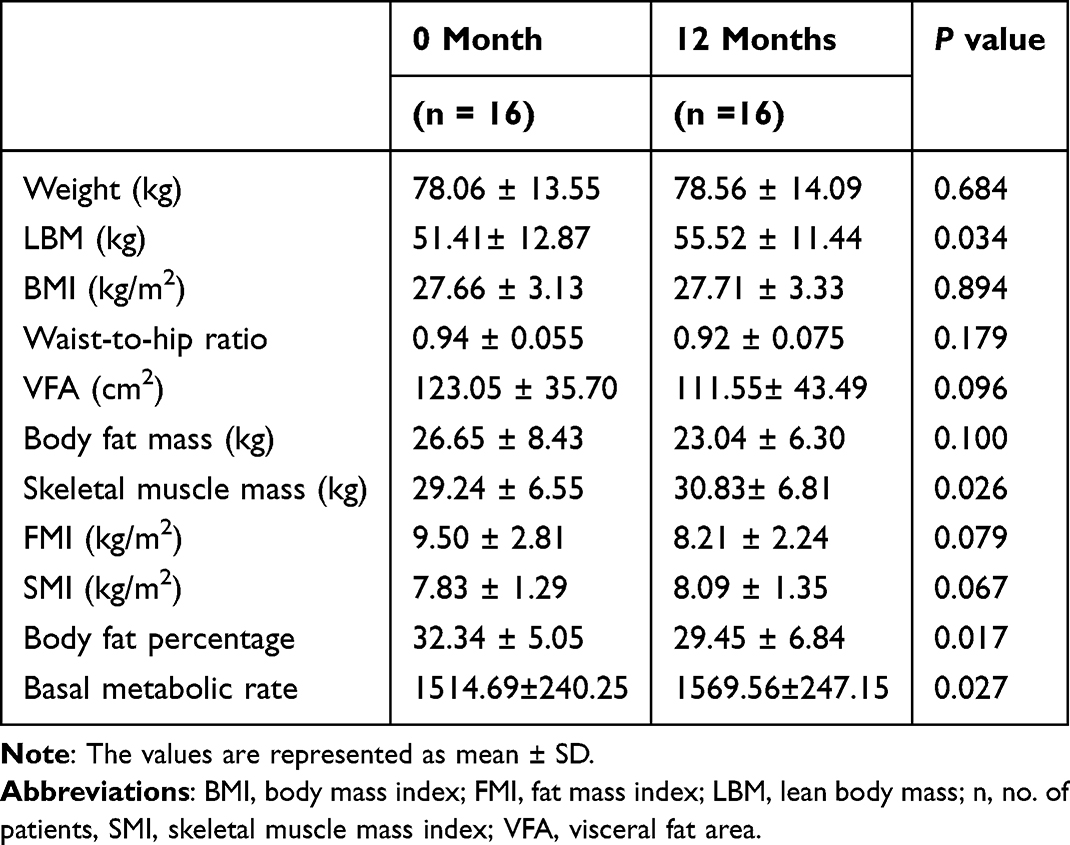 |
Table 4 Comparison of Body Composition Indicators After One Year |
Lipid Metabolism Analysis
After 12 weeks of treatment, the LDL level of the patients decreased from 3.05 ± 0.83 mmol/L to 2.87 ± 0.79 mmol/L, which was statistically significant (P < 0.05). The levels of TC and TG decreased, and the HDL increased, but the changes were not of statistical significance. The details are presented in Table 5.
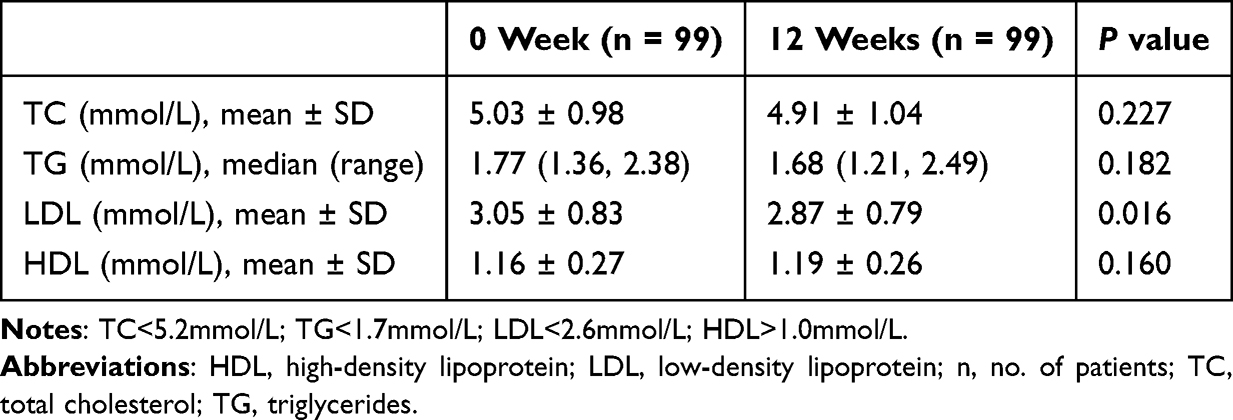 |
Table 5 Comparison of Blood Lipid Before and After Treatment |
Vitamin D
Compared with the baseline, 25-OH-VD level in patients with T2DM increased from 48.88 (41.99, 57.88) nmol/L to 51.60 (45.55, 64.17) nmol/L after treatment, and the difference was statistically significant (P < 0.05). The details are presented in Table 6.
 |
Table 6 Comparison of Vitamin D Before and After Treatment |
No serious adverse events were reported during the study period.
Discussion
Obesity is one of the main predisposing factors for T2DM, which can lead to the development of multiple cardiovascular risk factors and comorbidities. Excessive visceral adipose tissue significantly increases the risk of cardiovascular events and sudden death.27, Therefore, weight management, especially reducing abdominal fat, is of great significance for obese and patients with T2DM. For patients with T2DM and coexisting obesity, the selection of hypoglycemic drugs that also promote weight loss provides additional benefits. GLP-1 RAs are increasingly being chosen because of their remarkable hypoglycemic effects, ability to induce weight loss, improve blood lipid profiles, offer cardiorenal protection, and convenience of use.
Song et al (2023)28 conducted a study involving patients with T2DM who were overweight or obese, dividing them into a control group and a treatment group. The control group received metformin (1.5–2.0 g daily) orally along with subcutaneous insulin (initial dose of 12 U/day) injections, while the combination treatment group additionally received PEX168 (0.2 mg once weekly via subcutaneous injection). After 6 months of treatment, both groups showed reductions in FBG, 2-h postprandial blood glucose, FINS, and HbA1c levels. However, the combination treatment group exhibited statistically significant greater reductions compared with the control group (P < 0.05).
In another study by Shuai et al (2021), patients were randomized into a placebo group, a PEX168/100 μg group, and a PEX168/200 μg group. Compared with placebo, both doses of PEX168 achieved significantly greater reductions in HbA1c (P < 0.0001).25 Similarly, Gao et al (2020) randomized patients into three groups: metformin (500 mg three times daily)+ placebo, metformin + PEX168 100 μg, and metformin + PEX168 200 μg. After 24 weeks of treatment, the proportions of patients achieving HbA1c <7% were significantly higher in the PEX168 100 μg (37.4%) and PEX168 200 μg (40.6%) groups compared with the placebo group (16.8%; both P < 0.001).29 These studies confirm the superior glucose-lowering efficacy of PEX168, aligning with the findings of the present study.
In the present study, after PEX168 treatment, HbA1c levels decreased from 8.8 ± 1.11% to 6.9 ± 0.92%, and FBG levels decreased from 9.6 ± 2.65 mmol/L to 7.2 ± 1.71 mmol/L, both demonstrating statistically significant differences (P < 0.001).
Furthermore, Song et al (2023)28 reported that the combination treatment group showed a more pronounced reduction in HOMA-IR levels, with statistically significant differences (P < 0.05). Similarly, the current study demonstrated that PEX168 treatment increased FC-P levels and reduced HOMA-IR levels, suggesting that PEX168 improves insulin function in patients.
Obesity is not merely an increase in total body weight but also a manifestation of dysfunctional adipose tissue and abnormal fat distribution. Under conditions of obesity, visceral adipose tissue is more prone to abnormal deposition. The large amounts of free fatty acids released from visceral fat enter the liver and suppress insulin signaling pathways. Additionally, visceral fat secretes various inflammatory cytokines that impair normal insulin action, thereby contributing to the development of T2DM and cardiovascular diseases.30 Therefore, measuring visceral fat is particularly important, and reducing visceral fat content may provide significant benefits in T2DM treatment.
Forty-five obese women with polycystic ovary syndrome (PCOS) were randomly divided into three groups, receiving metformin 1000 mg twice daily, liraglutide 1.2 mg once daily, via subcutaneous injection, and roflumilast 500 μg once daily respectively for 12 weeks. The liraglutide group achieved an average weight loss of 3.1±3.5 kg (P = 0.006), which was superior to the metformin group with a weight loss of 0.2±1.83 kg (P = 0.735). Additionally, the liraglutide group showed a significant reduction in visceral adipose tissue area (P = 0.015).31
Thirty-five obese adults (17 receiving liraglutide and 18 receiving placebo) were included in the study. The liraglutide group had their dosage titrated weekly to 3 mg per day via subcutaneous injection, while the placebo group received a placebo. Both groups were combined with lifestyle interventions (dietary and behavioral counseling) for 16 weeks of continuous treatment. The results showed that the liraglutide group had significantly greater reductions in total fat, trunk fat, upper body fat, and lower body fat compared to the placebo group, without affecting lean body mass.32
In this study, after 12 weeks of treatment, 99 patients exhibited significant reductions in body weight, visceral fat area, and body fat mass. Among them, 16 patients who received 12-month treatment showed no significant change in body weight but had significant increases in lean body mass and skeletal muscle mass, along with a significant decrease in body fat percentage. Short-term treatment may be effective in reducing patients’ body weight; however, after one year of treatment, it was found that PEX168 had a minimal effect on body weight, while lean body mass and skeletal muscle mass were observed to be maintained. Nevertheless, the number of patients who received one-year treatment was small, which had a significant impact on the results, underscoring the need for larger-scale studies to validate these findings.
A study randomized patients into dulaglutide (0.75 mg/week) and semaglutide (0.25 mg/week) groups, showing that the semaglutide group achieved more significant reductions in BMI and VFA after 24 weeks of treatment (P < 0.05).33 A clinical study by Hongyu et al34 demonstrated that compared with metformin (1500 mg weekly), polyethylene glycol loxenatide (PEX 168, 0.3 mg weekly) significantly improved multiple cardiovascular risk factors, including BMI, waist circumference, VFA, and lipid profiles in overweight or obese T2DM patients. After 16 weeks of treatment, patients exhibited significant weight loss. TC, TG, and LDL-C levels were improved with PEG-Loxe treatment compared with metformin treatment (P < 0.001), suggesting that GLP-1 RAs can effectively reduce body weight and improve VFA. The difference between Hongyu’s study and the present study lies in the dosage and treatment duration of PEX 168: in Hongyu’s study, the dosage was 0.3 mg once weekly for 16 weeks, whereas in the present study, the dosage was 0.2 mg once weekly for 12 weeks. The innovation of this study is that middle-aged and elderly patients were selected as research subjects to analyze the effects of PEX 168 on body composition in elderly individuals.
GLP-1 RAs suppress appetite, delay gastric emptying, and reduce insulin resistance. By inducing a negative energy balance through caloric restriction, these agents promote lipolysis, thereby facilitating weight reduction and improving lipid profiles. The results of this study showed that PEX168 could reduce body weight, BMI, waist-to-hip ratio, VFA and FMI in patients with T2DM, consistent with previous research findings. PEX168 could help patients lose weight and improve visceral fat obesity. Reductions in body weight and visceral fat confer substantial benefits to obese patients, particularly those with central obesity.
The SURMOUNT-5 trial35 has demonstrated that tirzepatide (10 mg or 15 mg) exhibits superior weight-loss efficacy compared with semaglutide (1.7 mg or 2.4 mg) in adults with obesity without T2DM. At 72 weeks, the percentage of weight loss in the tirzepatide group reached −20.2%, with a reduction in waist circumference of 18.4 cm, whereas the semaglutide group showed a weight loss of −13.7% and a waist circumference reduction of 13 cm. This may be related to the simultaneous action of tirzepatide on both glucose-dependent insulinotropic polypeptide and GLP-1 receptors. The reduction in waist circumference was more significant in the tirzepatide group (−18.4 vs −13.0 cm), indicating a better improvement in central obesity. Dual-receptor agonists offer advantages over single-receptor agonists, providing key evidence for drug selection in the treatment of obesity.
Jing et al (2009)36 highlighted that individuals with the same BMI or body fat percentage may exhibit significant differences in body composition and metabolic status. Therefore, using FMI to measure and describe body composition may be more precise and effective compared with BMI or body fat percentage. In this study, the FMI of patients with T2DM decreased from 8.6 ± 2.24 to 8.3 ± 2.20 after 12 weeks of PEX168 treatment (P < 0.05), whereas LBM, skeletal muscle mass, and SMI showed no significant reduction, suggesting that PEX168 reduces body weight and fat mass without compromising skeletal muscle mass.
Li et al (2014)37 found that after 12 weeks of liraglutide treatment (0.6 mg once daily, titrated to 1.2 mg once daily after one week), patients with T2DM exhibited significant reductions in body weight, waist circumference, total fat, LBM, fat percentage, and abdominal VFA, with a 2.34% increase in relative total LBM (ie., LBM as a percentage of total body weight).
Volpe et al (2022)38 reported that after 3 months of semaglutide treatment (0.25 mg weekly for 4 weeks, then 0.5 mg weekly), patients with T2DM experienced reductions in body weight, VFA, and FMI, but no changes in SMI or muscle strength. Zhang et al39 conducted a clinical study in which 76 patients with T2DM with overweight/obesity were stratified into overweight, obese, and severely obese groups based on BMI. In addition to their original treatment, patients received exenatide(initial dose 5 μg twice daily by subcutaneous injection, increased to 10 μg twice daily after 1 week) or liraglutide (1.2 mg once daily by subcutaneous injection). The results showed the obese and severely obese patients showed significantly decreased percentage body fat (including both subcutaneous and visceral fat) and increased muscle mass after the treatment (P< 0.05). This demonstrates that the weight loss effects of GLP-1 RAs are not dependent on skeletal muscle reduction. On the contrary, although skeletal muscle mass may decrease during weight loss, the proportional increase in skeletal muscle relative to body composition is clearly evident.
Vitamin D is crucial for skeletal muscle health.40 Vitamin D deficiency can lead to sarcopenia, osteomalacia, osteoporosis, and an increased risk of falls and fractures.41 Conversely, skeletal muscle, being one of the body’s largest metabolic organs, may influence vitamin D metabolism, suggesting a bidirectional relationship between muscle function and vitamin D status. Compared with healthy individuals, patients with sarcopenia have lower circulating levels of 25-OH-VD.42 An Australian cross-sectional study found that in elderly men with low 25-OH-VD levels, the incidence of sarcopenia increased both in the next 2 and 5 years.43 Similarly, a Japanese study found that the vitamin D levels in the elderly population with sarcopenia were significantly lower than those in the normal control group.44 Furthermore, a meta-analysis by Du et al (2020), including 5081 patients with sarcopenia and 14,447 patients without, demonstrated that higher serum 25-OH-VD levels significantly improved muscle mass in the elderly, whereas higher HOMA-IR had a negative impact.45 Patients treated with GLP-1 RAs experienced reductions in body weight, fat mass, and visceral adipose tissue without significant loss of skeletal muscle.46–48 GLP-1 RAs improve endothelial function through both indirect (by improving blood glucose and insulin signaling) and direct (receptor agonism) mechanisms, thereby increasing microvascular perfusion in the muscles and stimulating angiogenesis. Of note, it has been reported that treating patients with insulin resistance with GLP-1 RAs can improve skeletal muscle microvascular perfusion.49
The increase in serum 25-OH-VD concentration induced by weight loss may be attributed to volumetric concentration effects50 or the release of vitamin D sequestered within adipocytes.51 In the present study, after 12 weeks of treatment, patients exhibited a significant reduction in visceral fat area accompanied by a marked increase in 25-OH-VD levels. This elevation in 25-OH-VD levels may be associated with favorable changes in the distribution or metabolism of the lipophilic vitamin D following weight loss and metabolic improvement.
Conclusion
In summary, PEX168 treatment effectively lowers blood glucose levels in patients with T2DM while achieving weight loss, improving BMI and waist-to-hip ratio, significantly reducing visceral fat area, and effectively ameliorating central obesity, with no adverse effects observed on skeletal muscle mass.
The major strength of this study lies in the systematic assessment of body composition using bioelectrical impedance analysis. However, several limitations should be acknowledged. First, this was a single-arm, open-label prospective study. Second, the sample size was relatively limited, particularly the small number of patients completing the one-year follow-up. Therefore, the findings warrant further validation through large-scale randomized controlled trials.
Compliance with Ethics Guidelines
Each participant provided written informed consent. This study protocol was approved by the Institutional Ethical Committee of Nanjing First Hospital in accordance with the Declaration of Helsinki guidelines (KY20230310-11). This trial is registered at Clinical Trials.gov (CT.gov identifier: NCT05611684).
Data Sharing Statement
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.
Author Contributions
R.G, Y.Z and X.K share co-first authorship. R.G: Data curation and Writing-original draft, Y.Z: Data curation and Formal analysis, X.K: Methodology and Supervision, Y.L: Software and Formal analysis, H. L: Visualization and Writing-review & editing. J.M: Conceptualization and Methodology. All authors took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agreed to be accountable for all aspects of the work.
Funding
The authors declare that they have received no funding for this paper.
Disclosure
The authors declare that there is no conflict of interest.
References
1. Liang J, He Y, Huang C, et al. The regulation of selenoproteins in diabetes: a new way to treat diabetes. Curr Pharm Des. 2024;30(20):1541–12. doi:10.2174/0113816128302667240422110226
2. Su M, Tang T, Tang W, et al. Astragalus improves intestinal barrier function and immunity by acting on intestinal microbiota to treat T2DM: a research review. Front Immunol. 2023;14:1243834. doi:10.3389/fimmu.2023.1243834
3. Mi W, Xia Y, Bian Y. The influence of ICAM1 rs5498 on diabetes mellitus risk: evidence from a meta-analysis. Inflammation Res. 2019;68(4):275–284. doi:10.1007/s00011-019-01220-4
4. Zhao M, Huang J, Yang H, et al. Engineered aggregation-induced emission luminogens-based framework with CO-releasing property for accelerating diabetic wound healing. Chem Eng J. 2025;524:12. doi:10.1016/j.cej.2025.168981
5. Shu Y, Yang F, Li W, et al. Changes and significance of central carbon metabolism before and after metformin treatment of type 2 diabetes based on mass spectrometry. Discov Med. 2024;36(183):678–689. doi:10.24976/Discov.Med.202436183.64
6. Tang L, Wang Y, Gong X, et al. Integrated transcriptome and metabolome analysis to investigate the mechanism of intranasal insulin treatment in a rat model of vascular dementia. Front Pharmacol. 2023;14:1182803. doi:10.3389/fphar.2023.1182803
7. Zhou YC, Liu JM, Zhao ZP, Zhou MG, Ng M. The national and provincial prevalence and non-fatal burdens of diabetes in China from 2005 to 2023 with projections of prevalence to 2050. Mil Med Res. 2025;12(1):28. doi:10.1186/s40779-025-00615-1
8. Genitsaridi I, Salpea P, Salim A, et al. 11th edition of the IDF diabetes atlas: global, regional, and national diabetes prevalence estimates for 2024 and projections for 2050. Lancet Diabetes Endocrinol. 2026;14(2):149–156. doi:10.1016/S2213-8587(25)00299-2
9. Abd-Elsalam S, Abdulkader RS, Abu-Rmeileh NM, et al. Global, regional, and national prevalence of adult overweight and obesity, 1990–2021, with forecasts to 2050: a forecasting study for the Global Burden of Disease Study 2021. Lancet. 2025;405(10481):813–838.
10. Ren W, Xia Y, Chen S, et al. Glutamine metabolism in macrophages: a novel target for obesity/type 2 diabetes. Adv Nutr. 2019;10(2):321–330. doi:10.1093/advances/nmy084
11. Hou X, Lu J, Weng J, et al. Impact of waist circumference and body mass index on risk of cardiometabolic disorder and cardiovascular disease in Chinese adults: a national diabetes and metabolic disorders survey. PLoS One. 2013;8(3):e57319. doi:10.1371/journal.pone.0057319
12. Ji Q, Chai S, Zhang R, et al. Prevalence and co-prevalence of comorbidities among Chinese adult patients with type 2 diabetes mellitus: a cross-sectional, multicenter, retrospective, observational study based on 3B study database. Front Endocrinol. 2024;15:1362433. doi:10.3389/fendo.2024.1362433
13. Guh DP, Zhang W, Bansback N, et al. The incidence of co-morbidities related to obesity and overweight: a systematic review and meta-analysis. BMC Public Health. 2009;9(1):88. doi:10.1186/1471-2458-9-88
14. Al-Goblan AS, Al-Alfi MA, Khan MZ. Mechanism linking diabetes mellitus and obesity. Diabetes Metab Syndr Obes. 2014;7:587–591. doi:10.2147/DMSO.S67400
15. Grant B, Sandelson M, Agyemang-Prempeh B, Zalin A. Managing obesity in people with type 2 diabetes. Clin Med. 2021;21(4):e327–e231. doi:10.7861/clinmed.2021-0370
16. Leitner DR, Frühbeck G, Yumuk V, et al. Obesity and type 2 diabetes: two diseases with a need for combined treatment strategies - EASO can lead the way. Obes Facts. 2017;10(5):483–492. doi:10.1159/000480525
17. Liu Y, Ma W, Fu H, et al. Efficacy of polyethylene glycol loxenatide for type 2 diabetes mellitus patients: a systematic review and meta-analysis. Front Pharmacol. 2024;15:1235639. doi:10.3389/fphar.2024.1235639
18. Drucker DJ. Mechanisms of action and therapeutic application of glucagon-like Peptide-1. Cell Metab. 2018;27(4):740–756. doi:10.1016/j.cmet.2018.03.001
19. Blundell J, Finlayson G, Axelsen M, et al. Effects of once-weekly semaglutide on appetite, energy intake, control of eating, food preference and body weight in subjects with obesity. Diabetes Obes Metab. 2017;19(9):1242–1251. doi:10.1111/dom.12932
20. Chinese SOE, Chinese DS. Consensus recommendations on utilizing glucagon-like peptide-1(GLP-1) receptor agonists in the treatment of type 2 diabetes mellitus. Chung-hua nei k‘o tsa chih. 2020;59(11):836–846.
21. Stepanova N. Type 2 diabetes mellitus and the gut microbiota: charting new territory for Sodium-Glucose Co-Transporter 2 inhibitors. Eurasian J Med Oncol. 2024;8(1):1. doi:10.14744/ejmo.2024.53968
22. Ngabea MA, Dimeji IY. GLP-1 receptor agonists and inflammatory pathway modulation: dual targeting of metabolic and immune dysfunction in insulin resistance. Biochem Biophys Res Commun. 2025;789:152822. doi:10.1016/j.bbrc.2025.152822
23. American Diabetes Association Professional Practice Committee, American Diabetes Association Professional Practice Committee.9. Pharmacologic approaches to glycemic treatment: standards of medical care in diabetes—2022. Diabetes Care. 2022;45(1):S125–S143. doi:10.2337/dc22-S009
24. Salamah HM, Marey A, Elsayed E, et al. Efficacy and safety of polyethylene glycol loxenatide in type 2 diabetic patients: a systematic review and meta-analysis of randomized controlled trials. Sci Rep. 2023;13(1):19041. doi:10.1038/s41598-023-46274-x
25. Shuai Y, Yang G, Zhang Q, et al. Efficacy and safety of polyethylene glycol loxenatide monotherapy in type 2 diabetes patients: a multicentre, randomized, double-blind, placebo-controlled phase 3a clinical trial. Diabetes Obesity Metab. 2021;23(1):116–124. doi:10.1111/dom.14198
26. Alberti KG, Zimmet PZ. Definition, diagnosis and classification of diabetes mellitus and its complications. Part 1: diagnosis and classification of diabetes mellitus provisional report of a WHO consultation. Diabet Med. 1998;15(7):539–553. doi:10.1002/(SICI)1096-9136(199807)15:7<539::AID-DIA668>3.0.CO;2-S
27. Piche MREE, Tchernof A, Despres JPER. Obesity phenotypes, diabetes, and cardiovascular diseases. Circ Res. 2020;126(11):1477–1500. doi:10.1161/CIRCRESAHA.120.316101
28. Song X, Yao M, Li Z, et al. Clinical efficacy of polyethylene glycol loxenatide in the treatment of obese or overweight patients with type 2 diabetes mellitus. J Coll Physicians Surg Pak. 2023;33(12):1390–1394. doi:10.29271/jcpsp.2023.12.1390
29. Gao F, Lv X, Mo Z, et al. Efficacy and safety of polyethylene glycol loxenatide as add-on to metformin in patients with type 2 diabetes: a multicentre, randomized, double-blind, placebo-controlled, phase 3b trial. Diabetes Obes Metab. 2020;22(12):2375–2383. doi:10.1111/dom.14163
30. Sakers A, De Siqueira MK, Seale P, Villanueva CJ. Adipose-tissue plasticity in health and disease. Cell. 2022;185(3):419–446. doi:10.1016/j.cell.2021.12.016
31. Jensterle M, Salamun V, Kocjan T, Vrtacnik Bokal E, Janez A. Short term monotherapy with GLP-1 receptor agonist liraglutide or PDE 4 inhibitor roflumilast is superior to metformin in weight loss in obese PCOS women: a pilot randomized study. J Ovarian Res. 2015;8:32. doi:10.1186/s13048-015-0161-3
32. Kadouh H, Chedid V, Halawi H, et al. GLP-1 analog modulates appetite, taste preference, gut hormones, and regional body fat stores in adults with obesity. J Clin Endocrinol Metab. 2020;105(5):1552–1563. doi:10.1210/clinem/dgz140
33. Kimura T, Katakura Y, Shimoda M, et al. Comparison of clinical efficacy and safety of weekly glucagon-like peptide-1 receptor agonists dulaglutide and semaglutide in Japanese patients with type 2 diabetes: randomized, parallel-group, multicentre, open-label trial (COMING study). Diabetes Obes Metab. 2023;25(12):3632–3647. doi:10.1111/dom.15258
34. Cai H, Chen Q, Duan Y, Zhao Y, Zhang X. Short-term effect of polyethylene glycol loxenatide on weight loss in overweight or obese patients with type 2 diabetes: an open-label, parallel-arm, randomized, metformin-controlled trial. Front Endocrinol. 2023;14:1106868. doi:10.3389/fendo.2023.1106868
35. Aronne LJ, Horn DB, le Roux CW, et al. Tirzepatide as compared with semaglutide for the treatment of obesity. N Engl J Med. 2025;393(1):26–36. doi:10.1056/NEJMoa2416394
36. Wang J, Rennie KL, Gu W, et al. Independent associations of body-size adjusted fat mass and fat-free mass with the metabolic syndrome in Chinese. Ann Hum Biol. 2009;36(1):110–121. doi:10.1080/03014460802585079
37. Li CJ, Yu Q, Yu P, et al. Changes in liraglutide-induced body composition are related to modifications in plasma cardiac natriuretic peptides levels in obese type 2 diabetic patients. Cardiovasc Diabetol. 2014;13:36. doi:10.1186/1475-2840-13-36
38. Volpe S, Lisco G, Racaniello D, et al. Once-Weekly semaglutide induces an early improvement in body composition in patients with type 2 diabetes: a 26-week prospective real-life study. Nutrients. 2022;14(12).
39. Zhang Y, Liu S, Fan C, et al. Effect of glucagon-like peptide 1 receptor agonists on body fat redistribution and muscle mass in overweight and obese type 2 diabetic patients. Nan fang yi ke da xue xue bao. 2019;39(4):450–455. doi:10.12122/j.issn.1673-4254.2019.04.11
40. Latham CM, Brightwell CR, Keeble AR, et al. Vitamin D promotes skeletal muscle regeneration and mitochondrial health. Front Physiol. 2021;12:660498. doi:10.3389/fphys.2021.660498
41. Kupisz-Urbanska M, Pludowski P, Marcinowska-Suchowierska E. Vitamin D deficiency in older patients-problems of sarcopenia, drug interactions, management in deficiency. Nutrients. 2021;13(4):1247. doi:10.3390/nu13041247
42. Luo J, Quan Z, Lin S, Cui L. The association between blood concentration of 25- hydroxyvitamin D and sarcopenia: a meta-analysis. Asia Pac J Clin Nutr. 2018;27(6):1258–1270. doi:10.6133/apjcn.201811_27(6).0013
43. Hirani V, Cumming RG, Naganathan V, et al. Longitudinal associations between Vitamin D metabolites and sarcopenia in older Australian men: the concord health and aging in men project. J Gerontol a Biol Sci Med Sci. 2017;73(1):131–138. doi:10.1093/gerona/glx086
44. Sato M, Morishita T, Katayama T, et al. Relationship between age-related decreases in serum 25-hydroxyvitamin D levels and skeletal muscle mass in Japanese women. J Med Invest. 2020;67(1.2):151–157. doi:10.2152/jmi.67.151
45. Du Y, Oh C, No J. Does vitamin D affect sarcopenia with insulin resistance in aging? Asia Pac J Clin Nutr. 2020;29(3):648–656. doi:10.6133/apjcn.202009_29(3).0025
46. Feng WH, Bi Y, Li P, et al. Effects of liraglutide, metformin and gliclazide on body composition in patients with both type 2 diabetes and non-alcoholic fatty liver disease: a randomized trial. J Diabetes Investig. 2019;10(2):399–407. doi:10.1111/jdi.12888
47. Gibbons C, Blundell J, Tetens Hoff S, et al. Effects of oral semaglutide on energy intake, food preference, appetite, control of eating and body weight in subjects with type 2 diabetes. Diabetes Obes Metab. 2021;23(2):581–588. doi:10.1111/dom.14255
48. Bouchi R, Nakano Y, Fukuda T, et al. Reduction of visceral fat by liraglutide is associated with ameliorations of hepatic steatosis, albuminuria, and micro-inflammation in type 2 diabetic patients with insulin treatment: a randomized control trial. Endocr J. 2017;64(3):269–281. doi:10.1507/endocrj.EJ16-0449
49. Love KM, Liu J, Regensteiner JG, Reusch JEB, Liu Z. GLP-1 and insulin regulation of skeletal and cardiac muscle microvascular perfusion in type 2 diabetes. J Diabetes. 2020;12(7):488–498. doi:10.1111/1753-0407.13045
50. Drincic AT, Armas LAG, Van Diest EE, Heaney RP. Volumetric dilution, rather than sequestration best explains the low vitamin D status of obesity. Obesity. 2012;20(7):1444–1448. doi:10.1038/oby.2011.404
51. Brouwer DA, van Beek J, Ferwerda H, et al. Rat adipose tissue rapidly accumulates and slowly releases an orally-administered high vitamin D dose. Br J Nutr. 1998;79(6):527–532. doi:10.1079/BJN19980091
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.