Back to Journals » Vascular Health and Risk Management » Volume 18
Polyarteritis Nodosa with Cytomegalovirus Enteritis and Jejunoileal Perforation: Report of a Case with a Literature Review
Authors Waisayarat J ![]() , Niyasom C
, Niyasom C ![]() , Vilaiyuk S
, Vilaiyuk S ![]() , Molagool S
, Molagool S
Received 24 January 2022
Accepted for publication 19 July 2022
Published 28 July 2022 Volume 2022:18 Pages 595—601
DOI https://doi.org/10.2147/VHRM.S354548
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Pietro Scicchitano
Jariya Waisayarat,1 Chayakamon Niyasom,2 Soamarat Vilaiyuk,2 Sani Molagool3
1Department of Pathology, Faculty of Medicine Ramathibodi Hospital, Mahidol University, Bangkok, Thailand; 2Department of Pediatrics, Faculty of Medicine Ramathibodi Hospital, Mahidol University, Bangkok, Thailand; 3Department of Surgery, Faculty of Medicine Ramathibodi Hospital, Mahidol University, Bangkok, Thailand
Correspondence: Jariya Waisayarat, Department of Pathology, Faculty of Medicine, Ramathibodi Hospital, Mahidol University, 270 Rama VI Road, Rajathevee, Bangkok, 10400, Thailand, Tel +66 2 201 1432, Fax +66 2 354 7266, Email [email protected]
Abstract: Polyarteritis nodosa (PAN) is a rare systemic necrotizing vasculitis affecting small- to medium-sized arteries. The most common gastrointestinal manifestation of PAN is postprandial abdominal pain from mesenteric arteritis causing bowel ischemia. When transmural ischemia develops, there may be ischemic necrosis and perforation of the bowel wall, which are life-threatening. Severe, life-threatening gastrointestinal involvement is relatively rare in pediatric PAN and may require different management in adult patients. We report a pediatric PAN case in a patient who presented with acute abdominal pain and superimposed cytomegalovirus enteritis with jejunoileal perforation. The patient improved with emergency small intestinal resection followed by conventional immunosuppressive drugs of a corticosteroid and cyclophosphamide, and anti-viral drugs. Before increasing the immunosuppressive drug dosage, initial screening of infectious cytomegalovirus and comprehensive evaluation for surgical conditions are essential in pediatric PAN with severe gastrointestinal involvement. Early aggressive treatment for acute abdomen is useful in reducing morbidity and mortality in pediatric PAN.
Keywords: polyarteritis nodosa, cytomegalovirus enteritis, abdominal pain, bowel perforation
Introduction
Systemic polyarteritis nodosa (PAN) is a rare necrotizing vasculitis predominantly affecting small- to medium-sized blood vessels.1 Kussmaul and Maier first described an autopsy case of PAN in 1866.2 The diagnostic criteria of PAN are evidence of a necrotizing vasculitis or an angiographic abnormality of a medium- or small-sized artery and one of the following: skin involvement, myalgia/muscle tenderness, hypertension, peripheral neuropathy, and renal involvement.1,3–6 The annual incidence of PAN is estimated to be 0.9–8.0/million in European countries and it has a prevalence of 31/million. PAN can affect all ethnicities and often occurs in patients aged 40–60 years. Unlike other types of vasculitis, PAN has a male preponderance (male-to-female ratio of 1.5:1).3–5
PAN affects medium and small vessels, such as capillaries and small arterioles, but spares large vessels, such as the aorta and its major branches.7 Vascular lesions arise at the muscular arterial wall, mainly at bifurcations and branch points. Inflammation can start in the intima and progress to the entire arterial wall, including the internal and external elastic lamina, resulting in fibrinoid necrosis.7 When vessel walls are weak, aneurysms can develop, increasing the subsequent risk for rupture, hemorrhage, and thrombosis. As PAN progress, proliferation of the intima or media may result in obstruction, causing tissue ischemia or infarction.8 Approximately 50% of patients with PAN have gastrointestinal (GI) involvement, which indicates that it is a major morbidity and cause of mortality.9–11
Postprandial abdominal pain is the most common symptom of GI manifestations. This pain is characteristically intermittent and worsens after meals. The pain is caused by mesenteric arteritis and results in bowel ischemia, ulceration, or perforation.12 Adult PAN is associated with various viral infection, such as hepatitis B virus, but is less common in human immunodeficiency virus, cytomegalovirus (CMV), and parvovirus B19 infections.13,14 The cause of pediatric PAN is unknown and is rarely associated with hepatitis B virus owing to hepatitis immunization.7 A standard treatment of conventional PAN requires a combination of a corticosteroid and cyclophosphamide. Optional therapeutics for refractory PAN include intravenous immunoglobin, plasma exchange, infliximab, and rituximab (anti-CD20 monoclonal antibody).1,3–6 We report the case of a 6-year-old girl who was diagnosed with PAN. She developed recurrent acute abdominal pain with superimposed CMV enteritis and jejunoileal perforation. She successfully recovered after surgical intervention and a standard regimen of immunosuppressive drugs. Early recognition and appropriate decisions are essential for the management of pediatric PAN.
Case Report
A 6-year-old girl was referred to our tertiary care hospital with abdominal pain, hypertension, and recurrent stroke as shown by computed tomography (CT) and magnetic resonance imaging of the brain. At a previous hospital, she was diagnosed with PAN by CT angiography of the whole aorta. CT angiography showed multiple aneurysms at the spleen, both kidney vessels, the inferior gastroepiploic artery, the superior mesenteric artery, and the internal iliac artery. She had an elevated erythrocyte sediment rate of 42 mm/h. She received a high dose of methylprednisolone for 3 days as an initial induction therapy before being referred to our hospital.
On the first day of admission (D1), she was afebrile, partially cooperative, and had a blood pressure of 130/94 mmHg (no difference in blood pressure in the extremities), pulse rate of 100 beats/min, body weight of 13.5 kg, and height of 105 cm on a physical examination. An abdominal examination showed no distension, tenderness, or organomegaly. A neurological examination showed limited movements of the extraocular muscles of both eyes, limitation and ptosis of the left eye, and right hemiparesis with a muscle power grade of at least II/V. Pertinent laboratory values included a hemoglobin concentration of 10.6 g/dL, white blood cell count of 7900 cells/mm3 (neutrophils, 79%; lymphocytes, 20%), platelet count of 507,000/mm3, erythrocyte sediment rate of 5 mm/h, C-reactive protein concentration of 2.79 mg/L, lipase concentration of 40 U/L, amylase concentration of 78 U/L, and normal urine analysis. Additionally, antinuclear antibodies, antineutrophil cytoplasmic antibody, and antiphospholipid antibody were within the normal range. She received the first dose of cyclophosphamide 500 mg/body surface area by infusion. The methylprednisolone was tapered to 2 mg/kg/day. The abdominal pain improved after she received immunosuppressive treatment.
On D15 after admission, her abdominal pain worsened with a new onset of fever, but no diarrhea or GI bleeding was observed. A laboratory examination showed leukopenia, which included a hemoglobin concentration of 8.2 g/dL, white blood cell count of 3,600 cells/mm3 (neutrophils, 86%; lymphocytes, 4%), platelet count of 135,000/mm3, erythrocyte sediment rate of 24 mm/h, C-reactive protein concentration of 55.5 mg/L, and normal urine analysis. A repeated CT angiography of the whole aorta showed a slightly decreased size of some intra-abdominal arterial aneurysms with segments VI and VII of the liver and splenic infarctions. Therefore, an additional drug was prescribed as a single dose of infliximab. Six hours later, the patient had progressive severe abdominal pain, abdominal distension, decreased bowel sounds, generalized tenderness, and abdominal guarding, with the presence of pneumoperitoneum on supine abdominal plain film. An emergency pediatric surgery was performed, and it showed multiple hemorrhagic spots at the serosa of the proximal jejunum, which measured 60 cm in length, and a perforated ulcer (0.5 x 0.5 cm) at the terminal ileum 15 cm from the ileocecal valve. Pathological findings showed transmural suppurative enteritis with perforation and viral cytopathic change with typical “owl eye appearance” inclusion bodies, which was compatible with perforated CMV enteritis. No definite evidence of active vasculitis or thrombosis was identified (Figure 1).
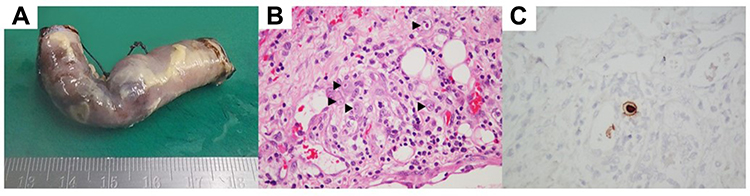 |
Figure 1 Cytomegaloviral enteritis with jejunoileal perforation. (A) Macroscopic findings. Serosal fibrinous exudate with perforation can be seen in the jejunoileum. (B) Microscopic findings. Cytomegalic cells with basophilic intranuclear inclusions can be seen (arrowheads, hematoxylin and eosin stain, 40×). (C) CMV-infected cells are shown by in situ hybridization. |
The patient’s blood CMV viral load examination showed 338,219 copies/mL. The patient’s clinical conditions improved postoperatively after a complete course of an anti-viral drug therapy (ganciclovir). The induction therapy was continued monthly with cyclophosphamide, but infliximab infusion for refractory PAN was stopped. Weaning of the steroid was planned according to a standard regimen.
Discussion
Our patient with PAN developed recurrent abdominal pain and a new episode of fever without diarrhea or GI bleeding on D15 after receiving immunosuppressive drugs. A complete blood count showed leukopenia and thrombocytopenia. She developed bowel perforation and underwent an emergency small intestinal resection. The pathological findings of the intestine showed CMV enteritis with jejunoileal perforation, but no evidence of active vasculitis. The patient likely developed CMV enteritis after receiving the high dose of immunosuppressive medications, which led to the recurrent abdominal pain. Even though the erythrocyte sedimentation rate was not high, the new onset of fever along with cytopenia were additional indicators of CMV infection in this patient. The lowered erythrocyte sedimentation rate after referral to our hospital was likely due to the administration of immunosuppressive drugs in the previous hospital. Conventional cases of PAN can be treated by initial therapy of a corticosteroid and cyclophosphamide, followed by maintenance therapy of azathioprine or mycophenolate mofetil.15
Approximately half of PAN cases present with GI involvement.16 In our case, the bowel perforation needed to be treated by surgery. This finding is similar to that in a study by Levine et al, who reported 24 patients diagnosed with PAN.17 In their study, 50% of all patients with GI involvement had acute abdominal pain, and most of the 13 patients with acute abdomen underwent surgery. There were eight episodes of a patient developing bowel infarction or perforation, and four had aneurysmal ruptures.17
Several previous cases of PAN presented with abdominal pain and multiple intestinal perforations of the small intestine, jejunum, or ileum.18–20 In a previous report, a 3-year-old girl had a prolonged fever without abdominal pain.21 A physical examination showed abdominal distension and rebound tenderness, and multiple free air fluid levels were detected on an abdominal X-ray. At surgery, there was fecal peritonitis with multiple gangrenous patches in the jejunoileum. The common sites of perforation of patients with PAN are the small intestine, jejunum, and ileum.22.
A review of 11 reports showed that severe, life-threatening GI involvement was found as small intestinal stricture, enteritis, colitis, ischemic necrosis, and its complications, such as obstruction, perforation, peritonitis, and mesenteric infarction.21,23–32 These pediatric patients with PAN who presented with aneurysms with or without rupture are shown in Table 1.
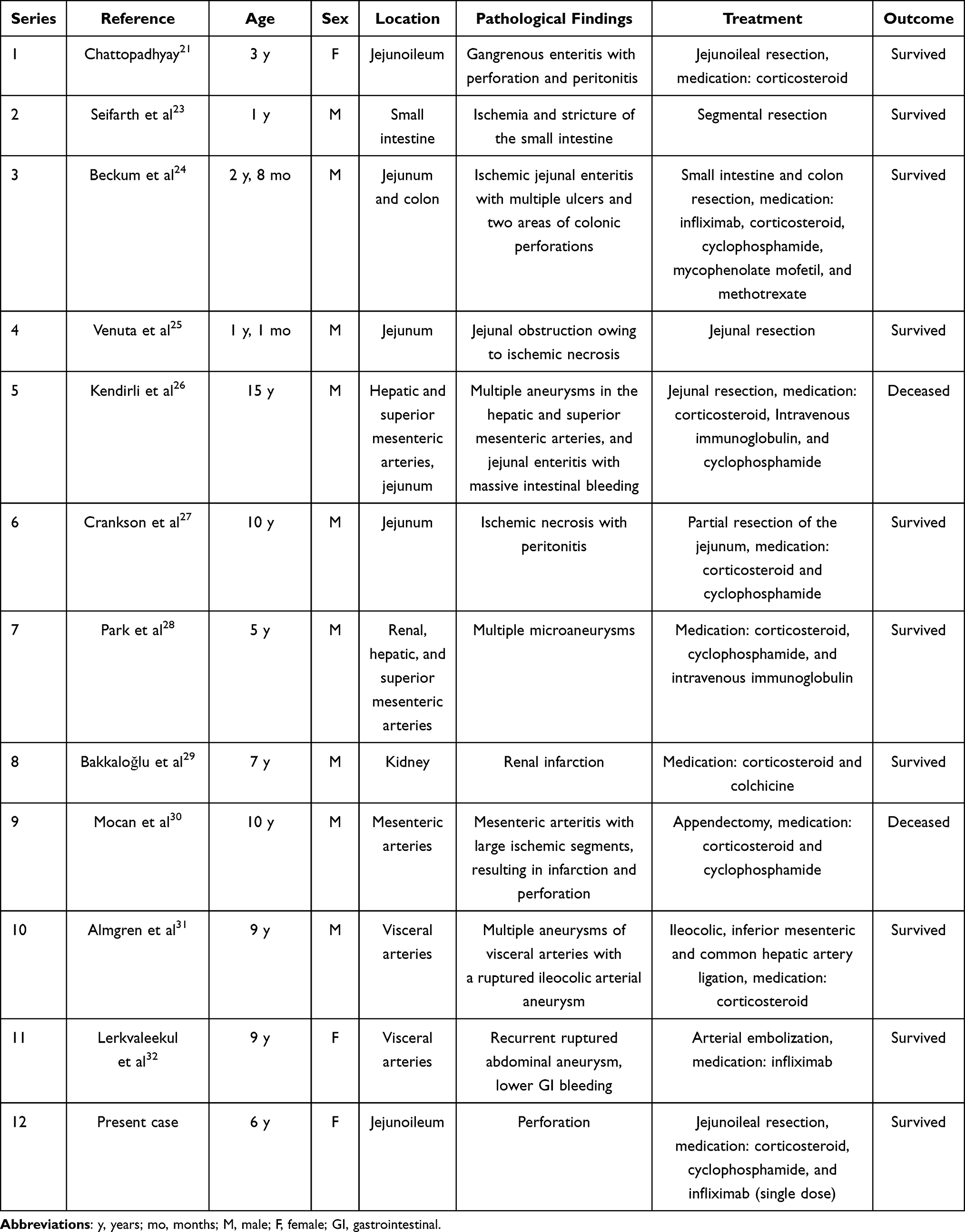 |
Table 1 Pediatric PAN Cases with Life-Threatening Gastrointestinal Involvement |
Uncommon GI involvement in these pediatric patients was treated with immunosuppressive drugs, intervention, or surgical resection. The outcome was survival in 10 out of 12 cases. Two of the patients were deceased. Kendirli et al reported catastrophic GI involvement in a 15-year-old boy with PAN and multiple aneurysms involving the hepatic and superior mesenteric arteries and jejunal enteritis with massive intestinal bleeding.26 This boy died from sepsis despite aggressive therapy. Mocan reported a fatal PAN in a 10-year-old boy who presented with acute abdomen and severe GI bleeding due to massive mesenteric arteritis, necrosis, and perforation.30 With regard to patients who survived PAN, Bakkaloğlu et al described a 7-year-old boy with familial Mediterranean fever complicated by PAN.29 Definite familial Mediterranean fever was diagnosed on the basis of typical attacks characterized by abdominal pain, fever, and an acute-phase response, including a homozygous MEFV mutation (M694 V/M694 V). Non-aneurysmal angiographic signs of PAN were present under renal angiography. The patient developed renal infarction and his condition was controlled with colchicine and a corticosteroid. Other PAN cases were improved after surgery, followed by corticosteroid, cyclophosphamide, or optional immunosuppressive drug therapy. Cases of pediatric PAN with life-threatening GI involvement are relatively rare and may require different management from adult patients.
Generally, GI CMV infection can occur in a healthy or an immunocompromised host. The most common involved site is the colon. The most common manifestation is diarrhea, followed by abdominal pain and rectal bleeding.33 However, the most frequent site of intestinal perforation in an immunocompromised patient is the distal ileum.34 A negative blood test for CMV does not exclude CMV colitis. Therefore, the gold standard for diagnosing CMV colitis is through histopathology. According to a study by Arnold et al, approximately 18% of patients with CMV infection showed peritonitis from multiple jejunoileal perforations, and the macroscopic manifestation was heterogeneous and varied according to the site of involvement.35 CMV can cause duodenal ulcers, antimesenteric perforations, and hemorrhagic ulceration.
In our study, the patient developed progressive severe abdominal pain with clinical signs of a systemic inflammatory response and peritonitis, and immediately underwent surgery. The operative findings were multiple hemorrhagic spots at the serosa of the proximal jejunum and a perforated ulcer at the terminal ileum. Additionally, the serology and histopathology were positive for CMV infection. Acute abdominal pain leading to perforation in this patient with PAN was caused by superimposed CMV infection.
In patients with PAN who receive conventional treatment, including corticosteroid and cyclophosphamide administration, the condition of the refractory disease or opportunistic infection should be evaluated when progressive abdominal pain develops. Therefore, infection should be excluded before increasing immunosuppressive medications. In refractory disease, anti-tumor necrosis factor therapy might be another treatment option for the refractory condition to prevent ongoing inflammation. However, early recognition of the patient’s condition with aggressive treatment is vital to reduce morbidity and mortality.
Conclusion
In conclusion, we report a 6-year-old girl with PAN who presented with abdominal pain, hypertension, and recurrent stroke. Initially, she improved with induction therapy and then developed recurrent acute abdominal pain with superimposed CMV enteritis and jejunoileal perforation. She underwent emergency jejunoileal resection, including an anti-viral drug, followed by the standard dosage of immunosuppressive drugs. The patient successfully recovered and was allowed to be discharged. Critical evaluation for secondary infection and early aggressive treatment for acute abdomen are important in reducing morbidity and mortality in pediatric PAN with severe life-threatening GI involvement.
Abbreviations
PAN, polyarteritis nodosa; GI, gastrointestinal; CMV, cytomegalovirus.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval
This study was approved by the Institutional Review Board of Mahidol University, in full compliance with International Guidelines for Human Research Protection, such as the Declaration of Helsinki, The Belmont Report, CIOMS Guidelines, and the International Conference on Harmonization in Good Clinical Practice (COA. MURA2022/10).
Consent for Publication
Written informed consent was obtained from the patient’s parents for this case report and any accompanying images.
Acknowledgments
We wish to thank the patient’s parents who provided consent for us to study their daughter for medical academic purposes. We acknowledge Mr. Phu Waisayarat, a medical student of the Faculty of Medicine, King Mongkut’s Institute of Technology Ladkrabang, Bangkok, Thailand for providing English proofreading services. We thank Ellen Knapp, PhD, from Edanz (https://edanz.com/ac) for editing a draft of this manuscript.
Author Contributions
All authors contributed toward data analysis, and drafting and revising the manuscript. All authors provided final approval of the version to be published and agree to be accountable for all aspects of the work. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors received no financial support for the research, authorship, or publication of this article.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Jennette JC, Falk RJ, Bacon PA, et al. 2012 revised International chapel hill consensus conference nomenclature of vasculitides. Arthritis Rheum. 2013;65(1):1–11. doi:10.1002/art.37715
2. Kussmaul A, Maier R. Ueber eine bisher nicht beschriebene eigenthümliche Arterienerkrankung (Periarteritis nodosa), die mit Morbus Brightii und rapid fortschreitender allgemeiner Muskellähmung einhergeht. Dtsch Arch Klin Med. 1866;1:484–518. German.
3. Stanton M, Tiwari V. Polyarteritis Nodosa. Treasure Island (FL): StatPearls Publishing; 2022.
4. De Virgilio A, Greco A, Magliulo G, et al. Polyarteritis nodosa: a contemporary overview. Autoimmun Rev. 2016;15(6):564–570. doi:10.1016/j.autrev.2016.02.015
5. Ozen S. The changing face of polyarteritis nodosa and necrotizing vasculitis. Nat Rev Rheumatol. 2017;13(6):381–386. doi:10.1038/nrrheum.2017.68
6. Hernández-Rodríguez J, Alba MA, Prieto-González S, Cid MC. Diagnosis and classification of polyarteritis nodosa. J Autoimmun. 2014;14:4849, 84–89. doi:10.1016/j.jaut.2014.01.029
7. Stone JH. Polyarteritis nodosa. JAMA. 2002;288(13):1632–1639. doi:10.1001/jama.288.13.1632
8. Colmegna I, Maldonado-Cocco JA. Polyarteritis nodosa revisited. Curr Rheumatol Rep. 2005;7(4):288–296. doi:10.1007/s11926-005-0039-2
9. Ebert EC, Hagspiel KD, Nagar M, Schlesinger N. Gastrointestinal involvement in polyarteritis nodosa. Clin Gastroenterol Hepatol. 2008;6(9):960–966. doi:10.1016/j.cgh.2008.04.004
10. Lee JS, Kim JG, Lee S. Clinical presentations and long term prognosis of childhood onset polyarteritis nodosa in single centre of Korea. Sci Rep. 2021;11(1):8393. doi:10.1038/s41598-021-87718-6
11. Merlin E, Mouy R, Pereira B, et al. Long-term outcome of children with pediatric-onset cutaneous and visceral polyarteritis nodosa. Joint Bone Spine. 2015;82(4):251–257. doi:10.1016/j.jbspin.2015.01.007
12. Lhote F, Cohen P, Guillevin L. Polyarteritis nodosa, microscopic polyangiitis and Churg-Strauss syndrome. Lupus. 1998;7(4):238–258. doi:10.1191/096120398678920055
13. Finkel TH, Török TJ, Ferguson PJ, et al. Chronic parvovirus B19 infection and systemic necrotising vasculitis: opportunistic infection or aetiological agent? Lancet. 1994;343(8908):1255–1258. doi:10.1016/S0140-6736(94)92152-0
14. Fernandes SR, Bértolo MB, Rossi CL, et al. Polyarteritis nodosa and cytomegalovirus: diagnosis by polymerase chain reaction. Clin Rheumatol. 1999;18(6):501–503. doi:10.1007/s100670050148
15. Eleftheriou D, Dillon MJ, Tullus K, et al. Systemic polyarteritis nodosa in the young: a single-center experience over thirty-two years. Arthritis Rheum. 2013;65(9):2476–2485. doi:10.1002/art.38024
16. de Carpi JM, Castejón E, Masiques L, Vilar P, Antón J, Varea V. Gastrointestinal involvement in pediatric polyarteritis nodosa. J Pediatr Gastroenterol Nutr. 2007;44(2):274–278. doi:10.1097/01.mpg.0000235753.37358.72
17. Levine SM, Hellmann DB, Stone JH. Gastrointestinal involvement in polyarteritis nodosa (1986–2000): presentation and outcomes in 24 patients. Am J Med. 2002;112(5):386–391. doi:10.1016/S0002-9343(01)01131-7
18. Miller DR, O’farrell TP. Perforation of the small intestine secondary to necrotizing vasculitis (periarteritis nodosa). Ann Surg. 1965;162(1):81–90. doi:10.1097/00000658-196507000-00013
19. Mousavie SH, Mirzaei R, Mahjoubi B, Azizi R. Successful management of multiple small bowel perforations due to polyarteritis nodosa. J Res Med Sci. 2014;19(3):276–278.
20. Buldukoglu OC, Koklu S, Koklu H, Uluoglu O, Kulduk G. Intestinal perforation as the initial presentation of polyarteritis nodosa in an older adult. Geriatr Gerontol Int. 2015;15(1):121–122. doi:10.1111/ggi.12266
21. Chattopadhyay A. Intestinal perforation due to polyarteritis nodosa. Indian J Pediatr. 2001;68(3):297–298. doi:10.1007/BF02723211
22. Takada T, Yoshida H, Tsukuda M, Katoh H. A case of classic polyarteritis nodosa presenting as acute abdomen. A review of 50 patients with PN involving small intestine undergone laparotomy in Japanese literature. Jpn J Gastroenterol Surg. 2003;36(1):51–56. doi:10.5833/jjgs.36.51
23. Seifarth FG, Ibrahim S, Spalding SJ, Reid JR. Intestinal obstruction secondary to infantile polyarteritis nodosa. Afr J Paediatr Surg. 2014;11(3):264–266. doi:10.4103/0189-6725.137339
24. Beckum KM, Kim DJ, Kelly DR, et al. Polyarteritis nodosa in childhood: recognition of early dermatologic signs may prevent morbidity. Pediatr Dermatol. 2014;31(1):e6–e9. doi:10.1111/pde.12207
25. Venuta A, Ceccarelli PL, Biondini D, Montanari F. Jejunal obstruction as initial presentation of polyarteritis nodosa in a 13-month-old boy. J Pediatr Surg. 2011;46(7):E27–E29. doi:10.1016/j.jpedsurg.2011.03.084
26. Kendirli T, Yüksel S, Oral M, et al. Fatal polyarteritis nodosa with gastrointestinal involvement in a child. Pediatr Emerg Care. 2006;22(12):810–812. doi:10.1097/01.pec.0000245172.38967.d0
27. Crankson SJ, Oda O, Al-Zaben AA, Suwairi WAI, Makanjoula D. Intestinal ischamemia in a child due to polyarteritis nodosa: a case report. Trop Gastroenterol. 2006;27(1):41–43.
28. Park H-J, Choi Y-J, Kim J-E, Ye Y-M, Park H-S, Suh C-H. Successful treatment of pediatric systemic polyarteritis nodosa with cholestatic hepatitis. Clin Rheumatol. 2007;26(1):122–124. doi:10.1007/s10067-005-0121-1
29. Bakkaloğlu SA, Muzaç S, Akpek S, Söylemezoğlu O, Buyan N, Hasanoğlu E. Polyarteritis nodosa in a case of familial Mediterranean fever. Pediatr Nephrol. 2004;19(5):536–538. doi:10.1007/s00467-003-1390-z
30. Mocan H, Mocan MC, Sen Y, Kuzey G, Civiloglu C. Fatal polyarteritis nodosa with massive mesenteric necrosis in a child. Clin Rheumatol. 1999;18(1):88–90. doi:10.1007/s100670050063
31. Almgren B, Eriksson I, Foucard T, Lörelius LE, Olsen L. Multiple aneurysms of visceral arteries in a child with polyarteritis nodosa. J Pediatr Surg. 1980;15(3):347–348. doi:10.1016/S0022-3468(80)80156-4
32. Lerkvaleekul B, Treepongkaruna S, Ruangwattanapaisarn N, Treesit T, Vilaiyuk S. Recurrent ruptured abdominal aneurysms in polyarteritis nodosa successfully treated with infliximab. Biologics. 2019;13:111–116. doi:10.2147/BTT.S204726
33. Le PH, Lin WR, Kuo CJ, et al. Clinical characteristics of cytomegalovirus colitis: a 15-year experience from a tertiary reference center. Ther Clin Risk Manag. 2017;13:1585–1593. doi:10.2147/TCRM.S151180
34. You DM, Johnson MD. Cytomegalovirus infection and the gastrointestinal tract. Curr Gastroenterol Rep. 2012;14(4):334–342. doi:10.1007/s11894-012-0266-4
35. Arnold M, Itzikowitz R, Young B, et al. Surgical manifestations of gastrointestinal cytomegalovirus infection in children: clinical audit and literature review. J Pediatr Surg. 2015;50:1874–1879.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.