Back to Archived Journals » Chronic Wound Care Management and Research » Volume 4
Platelet-rich plasma for the treatment of chronic wounds: evidence to date
Authors Conde-Montero E, de la Cueva Dobao P, Martínez González JM
Received 27 March 2017
Accepted for publication 21 June 2017
Published 4 September 2017 Volume 2017:4 Pages 107—120
DOI https://doi.org/10.2147/CWCMR.S118655
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Marco Romanelli
Elena Conde-Montero,1 Pablo de la Cueva Dobao,1 José María Martínez González2
1Department of Dermatology, Hospital Universitario Infanta Leonor, 2Faculty of Dentistry, Universidad Complutense de Madrid, Madrid, Spain
Abstract: Platelet-rich plasma (PRP) is a widely used throughout diverse fields of medicine for improving tissue regeneration. In dermatology, its main applications in the last few years have mainly been in antiaging treatment and wound healing. PRP contains platelets at higher concentrations than whole blood, and consequently represents a growth-factor pool. Chronic wounds are characterized by a prolonged inflammatory phase, involving a continuous destruction of matrix proteins and growth factors. Growth factors promote cell migration, proliferation, and differentiation, which are essential for wound healing. In this review, we explain the basic principles of PRP in wound healing and aim to offer an updated critical assessment of the available clinical evidence that supports the utility of PRP for the therapeutic challenge that chronic ulcers represent in our daily clinical practice.
Keywords: platelet-rich plasma, chronic wounds, growth factors, wound healing, platelet gel
Introduction
In recent years, the use of platelet-rich plasma (PRP) has increased notably in a range of diseases and settings, such as wound healing. Considering cutaneous ulcers, good outcomes have been found in case series and controlled studies in a wide variety of etiologies. After explaining the basic principles of PRP treatment, the authors aim to offer an updated review and critical assessment of the quality of the clinical evidence published to 2016 that supports the benefits of PRP in wound healing. More specifically, the following questions have been raised in this study:
- role of growth factors in wound healing
- PRP and its clinical application in wound healing
- safety of PRP application in wounds
- clinical evidence of PRP as adjunctive treatment for chronic wounds.
Role of growth factors in wound healing
Wound healing is a natural response to tissue injury, which involves a complex cascade of overlapped cellular events. However, in order to simplify the process, it has been traditionally explained as a series of four phases: hemostasis, inflammation, proliferation, and maturation. These stages may vary in length, due to different pathologic factors, such as infection, malnutrition, venous insufficiency, ischemia, and exogenous factors. Consensus has been reached such that a wound may be defined as chronic if complete healing has not been achieved in 6 weeks or no positive response to a treatment change is observed.1
Chronic cutaneous wound etiology is diverse. Leg ulcers, mainly secondary to venous insufficiency, are the most frequent. Other highly prevalent lesions include arterial, pressure, neuropathic ulcers, essentially secondary to diabetes or lepra reaction, and Martorell hypertensive ischemic leg ulcer.2
The biochemical microenvironment that promotes the chronicity of these lesions is characterized by an abnormally prolonged inflammatory phase, due to an increase in proinflammatory cytokines and high metalloprotease activity. Hypoxia and repeated infections promote this excessive amount of proteolytic enzymes and consequent growth factors and fibrin deficit, which impairs wound healing. Matrix metalloproteases, specifically MMP2 and MMP9, have been shown to be elevated in chronic wounds. Moreover, TIMP1 is decreased in nonhealing chronic wounds, which elevates levels of collagenolytic activity. Metalloproteinase concentration in a wound correlates with duration and chronification.3
An effective intervention must thus modify this environment that impedes healing, and is essential to induce the reparative phase of healing and shorten the prior inflammatory phase. In order to succeed, chronic-ulcer management should have a dual approach, including both underlying disease and local wound treatment. Consensus exists regarding the key points that should include any strategy that is suggested to enhance natural wound healing.4,5 However, to date, no robust scientific evidence exists to conclude that any dressing is superior to others, and conventional wound care does not supply the growth factors essential to the wound-healing process,6 which have been proven to be present in platelets.7 Platelets embedded within blood clots have a main role in the physiological process of wound healing, not only as hemostatic agents but also as regulators of inflammation, angiogenesis, cell migration, and proliferation.7,8 This biological basis supports treatment strategies that include the application of platelet concentrates on the wound, such as PRP.
Platelets are anucleate fragments of megakaryocytes that originate in the bone marrow and travel in the bloodstream for 7–10 days. These cellular elements contain a wide protein content in their secretory granules (dense granules, lysosomes, and mainly α-granules).7
During the physiological wound-healing process, platelets are activated in the injury site, and growth factors and cytokines are released over time during fibrin retraction. These proteins can bind to the fibrin matrix and to proteoglycans in the extracellular matrix, with the consequent establishment of a storage pool that can be secondarily released by proteinases.7
Each growth factor activates one or several response pathways, which depend on the cellular environment. Once the growth factor has bound to a cell-surface receptor, a second messenger cascade is triggered and the signal transmission remains active, even when growth factors disappear. Depending on the growth factor, a specific group of proteins is phosphorylated and a modification in cell activity takes place. The major families of growth factors that are released from platelets and are involved in wound healing are as follows:9
- EGF – stimulates fibroblasts to secrete collagenases, in order to degrade the extracellular matrix during the remodeling phase; encourages keratinocyte and fibroblast proliferation
- TGF
- TGFα – mitogenic and chemotactic for keratinocytes and fibroblasts
- TGFβ1 and TGFβ2 – promote angiogenesis, upregulate collagen production, inhibit degradation, stimulate chemoattraction of inflammatory cells
- VEGF – stimulates angiogenesis during tissue hypoxia
- FGF – promotes angiogenesis, granulation, and epithelialization via endothelial cell, fibroblast, and keratinocyte migration, respectively
- Platelet-derived growth factor (PDGF) – enhances migration of macrophages and fibroblasts; promotes collagen and proteoglycan synthesis.
Considering that PRP is a source of growth factors, and consequently has mitogenic, angiogenic, and chemotactic properties, it represents an interesting alternative adjunctive treatment for recalcitrant wounds. Moreover, PRP provides the wound with adhesive proteins, such as fibrinogen, which are essential in the healing process.9 Application of PRP has been demonstrated to be effective in both acute and chronic ulcers. Increased rates of cell proliferation and cell migration have been associated with the upregulation of different cell-cycle-regulatory proteins.10
Recombinant DNA technology has been used to produce PDGFs as nonautologous commercially prepared biotechnology products. Among these, the recombinant human PDGF becaplermin (Smith & Nephew Inc., London, UK) is the only product whose efficacy has been confirmed by well-designed studies, specifically in diabetic foot ulcers.11 However, it is important to highlight that isolated growth factors, in contrast to PRP, do not provide the wound with the complex pool of molecular signals in the multifunctional cell scaffold that potentially simulates physiological wound healing.8 This review is focused on clinical applications of PRP in wound healing, and not related to isolated growth factors.
PRP and its clinical application in wound healing
From a historical perspective, PRP application started in regenerative medicine the 1980s. At the end of the 1990s, taking advantage of the sealing and hemostatic properties of fibrin, PRP was progressively used in oral and maxillofacial medicine. After the first description of an ambulatory method for PRP obtainment by Anitua in 1999,12 various techniques and potential uses have been described. At present, different PRP cell-separation systems are commercially available.
The most commonly used technique is to obtain a blood simple from the patients themselves (autologous), but homologous techniques are also a valid option. The blood is centrifuged to separate the platelets from red and white blood cells. Depending on the author, single or double centrifugation under different centrifugation times and speed conditions may be used.13,14 The objective is achieving highly concentrated platelets and suspended in a small volume of plasma, which is consequently rich in growth factors. The mean blood platelet count in normal individuals ranges from 150,000 to 350,000/μL. Although a PRP platelet count of 1 million/µL (baseline levels ×5) has been postulated as the ideal therapeutic dose of PRP,15 others propose that platelet integrity is more important than platelet concentration and suggest that PRP should be defined as the volume of plasma that has more platelets than baseline blood.16
Depending on the author, different names are used to refer to autologous PRP: autologous platelet gel, plasma-rich growth factors, and autologous platelet concentrate. Moreover, various techniques are used to obtain the concentrates, which results in different final products. Platelet lysate is the resulting concentrate after breaking the platelet membrane by physical methods, such as freezing or sonication. Sonication is the process that disrupts cell membranes and releases cellular content using ultrasound. Platelet releasate is the resulting product after activation of the platelets by chemical methods with thrombin or calcium to liberate the cellular contents. Platelet-poor plasma refers to the fraction of plasma that lies over the platelet concentrate.
To date, there have been no correlations found among clinical results, platelet and growth-factor concentration, and PRP volume per treated area, and no consensus exists considering ideal PRP composition.13,17 Research has found that despite lower platelet concentration, similar and even higher growth-factor concentration than other systems can be achieved using low-force single-step centrifugation.18 We agree with this view, and propose that platelet integrity is more important than platelet concentration. Platelets that are exposed to less mechanical force maintain their viability.
Even if platelet concentration and capture efficiency may be similar between different preparation systems, significant compositional differences may be identified, such as white-cell concentration. The role of these compositional differences and their effect on clinical outcomes are unknown.19
Some authors have suggested that the more active platelets be mixed with a superior coat of red cells,15 so they include erythrocytes. However, others consider that erythrocytes may alter platelet aggregation. The presence of leukocytes in PRP is another point of disagreement.8 After centrifugation, leukocytes can be found mixed with platelets in the buffy coat, between erythrocyte and plasma fractions. Some authors consider that the presence of leukocytes is essential in PRP preparations, due to both their antibacterial activity20 and growth-factor release. On the contrary, some experts suggest that their inflammatory potential may impair wound healing.9 Consequently, depending on the method used, a different PRP fraction will be used.
When treating a lesion with PRP, the amount of bioavailable growth factors depends on both the platelet storage and the release into the microenvironment. This release relies on the kinetics of uptake and release from the PRP. Few studies have compared the kinetics of growth-factor release among PRP gels obtained by different methods.13 Differences are associated with platelet damage secondary to manipulation, variety in fibrin-mesh characteristics, which depend on the procoagulant molecule that has been used (calcium or thrombin), and growth factor-dependent factors. For example, ex vivo thrombin-activated PRP induces rapid clot formation/retraction and a sudden rise in molecular signals compared with Ca2+ or collagen.8 Considering that clotting cascade can be activated in situ without an exogenous activator, some methods use nonactivated platelets on the basis of potentially more efficient stimulation of wound healing.8
PRP application in wounds may be intralesional or topical. No studies compare the effects of both methods. Intralesional application will be limited by ulcer extent and patient pain tolerance. In our experience, considering pain tolerance, intralesional application of PRP should be restricted to small or neuropathic wounds.21 PRP injection should take place within the first 10 minutes after PRP activation with the procoagulant substance. PRP will be injected in wound edges in the wound bed. Topical application may be combined with intralesional use.
As happens with wound dressings and the different alternatives and advanced treatments, efficacy will mainly depend on the presence of a properly prepared wound bed. Prior to PRP application, the wound should be cleaned and adequately debrided. If there exists a high amount of necrotic or unviable tissue, it should be removed and PRP postponed until necessary. The choice of the secondary dressing depends on the amount of wound exudate. No studies have established the most appropriate frequency of PRP application. However, it is normally used on a weekly basis.12
In the last few years, several methods for obtaining PRP have been published and commercialized, with disposal kits at different prices. Products from these commercially available systems produce differing concentrations of growth factors and other bioactive molecules.22 Moreover, different techniques have been suggested to obtain PRP gel for topical application, normally physical, such as heating or stirring.23 The addition of bioactive excipients, both natural and synthetic, has also been suggested as a less time-consuming strategy. Different studies have shown the advantages of achieving a sustained release of growth factors, such as angiogenesis promotion, when PRP is mixed with bioactive polymers, such as hydrogels, before topical application.24 These polymers enhance the action of the fibrin mesh that is naturally obtained in the clot after PRP activation. Additionally, the use of these polymers for gelification enables an immediate production of PRP gel, which may be helpful in our daily clinical practice. However, no clinical trials comparing different polymers are available. Moreover, some are high in cost and difficult to obtain. The authors have suggested PRP gelification by adding a bioactive cellulose polymer, in order to promote sustained growth-factor release and facilitate topical application. This polymer is obtained with economic material and an easily reproducible technique, and it additionally enables an immediate production of PRP gel.18
Safety of PRP application in wounds
PRP can be considered a secure treatment. No adverse effects, such as increased risk of infection or hypersensitivity reactions, have been detected in clinical trials.25 Regarding oncogenic potential, when possible coincidences between carcinogenesis and the mitogenic pathways employed by growth factors have been evaluated, no evidence supports a possible tumoral triggering. Once a growth factor has joined its membrane receptor, intracellular signal cascades are activated, normal genetic expression is promoted, and different control mechanisms regulate this process. Growth factor overexpression could give rise to receptor mutation.26
It may be assumed that therapeutic growth-factor concentrates in PRP could act more as promoters than as initiators of carcinogenesis, favoring the division and proliferation of previously mutated cells. In tumor cells, the presence of an excessively large number of normal growth-factor-receptor copies induces increased sensitivity to the corresponding ligands, which even at very low concentrations may stimulate the cells and induce proliferation. Moreover, tumoral cells are unable adequately to suppress the continuously generated mitogenic signals.26 Consequently, as the use of growth factors is contraindicated in malignant wounds, a skin biopsy should be taken before starting PRP if malignancy cannot be completely excluded.
Clinical evidence of PRP as adjunctive treatment for chronic wounds
The first clinical application of platelet-derived preparations was in chronic leg ulcers. The lesions were covered with collagen embedded in platelet proteins. With this product, known as platelet-derived wound-healing formula, the formation of vascularized connective tissue was induced in these wounds.27 Since then, different platelet preparations have been tried for application in solution, gel, or by injection in wounds of different etiologies.25
Reports correspond mainly to individual cases or case series, although pilot studies and clinical trials have also been conducted. The outcomes of the isolated cases and small series published are often spectacular.28–30 These reports show noteworthy variability in the size and etiology of the lesions, as well as the method for obtaining and applying PRP. Wound etiologies that have been treated with PRP include diabetic, pressure, or venous ulcer, surgical or traumatic wounds, and wounds of other etiologies.
With the use of manual preparations, the published outcomes are similar to those obtained in case series treated with PRP obtained using commercial kits.31 Our experience confirms these findings.18 Considering the available evidence, the evaluation of the real utility of PRP use in chronic ulcers is complex. Regarding wound healing, it is difficult to design clinical trials with low risk of bias, and sample size is normally small. Moreover, as chronic ulcer management must have a dual approach, including both underlying disease and local wound treatment, it may be difficult to evaluate exclusively the role of a local treatment that additionally is not standardized. Consequently, in addition to evidence considering clinical trials,27,32–44 we have decided to include the results of large uncontrolled cohort studies,45–52 which are closer to real-life settings, despite their lower levels of evidence (Tables 1 and 2). Both descriptive and systematic reviews25,53–56 and clinical guidelines64–67 were also included.
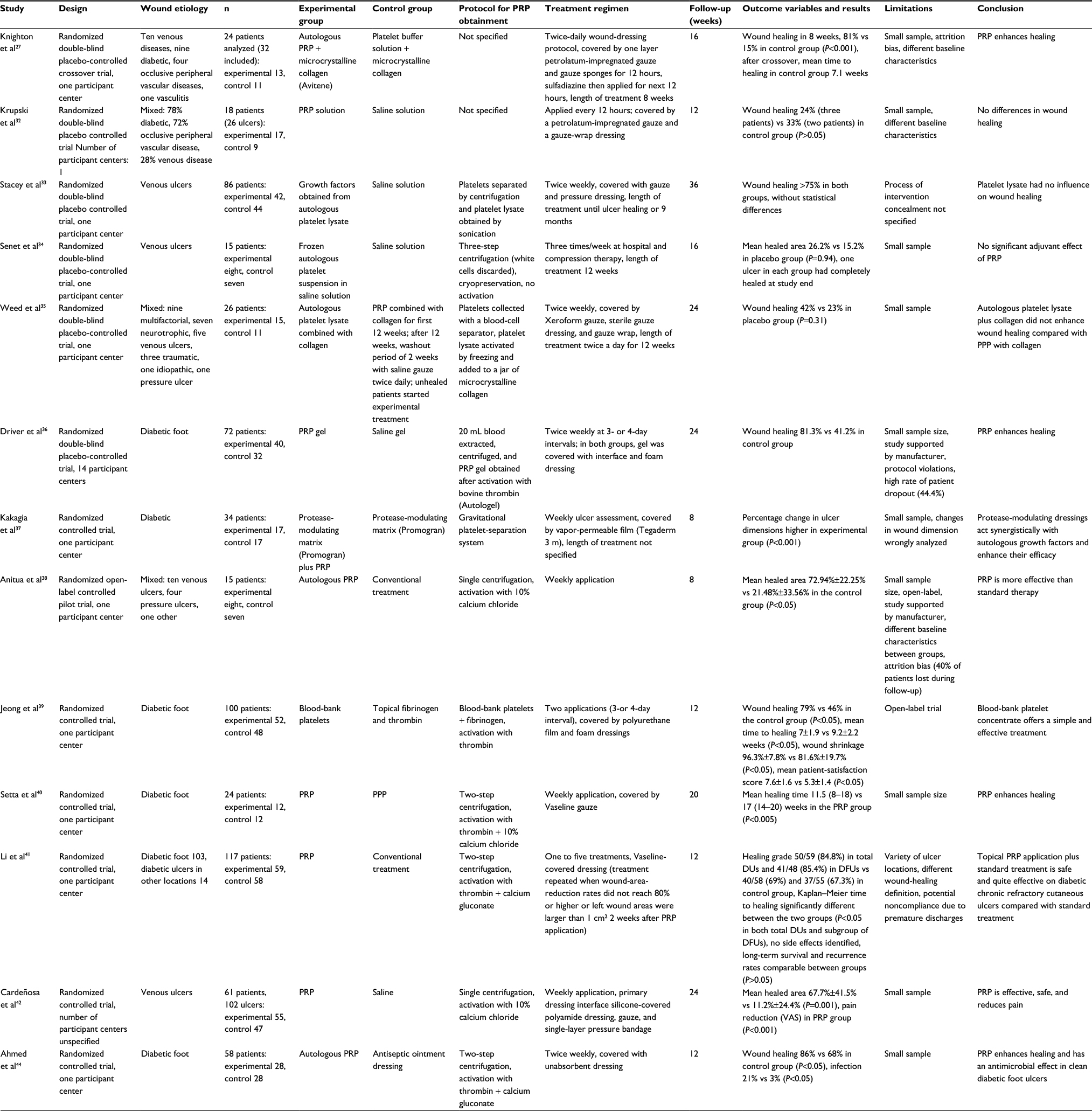
 | Table 1 Randomized controlled trials Note: Data presented as range, n (range) or mean ± standard deviation. Abbreviations: PRP, platelet-rich plasma; SF, Short Form (questionnaire); VAS, visual analogue scale. |
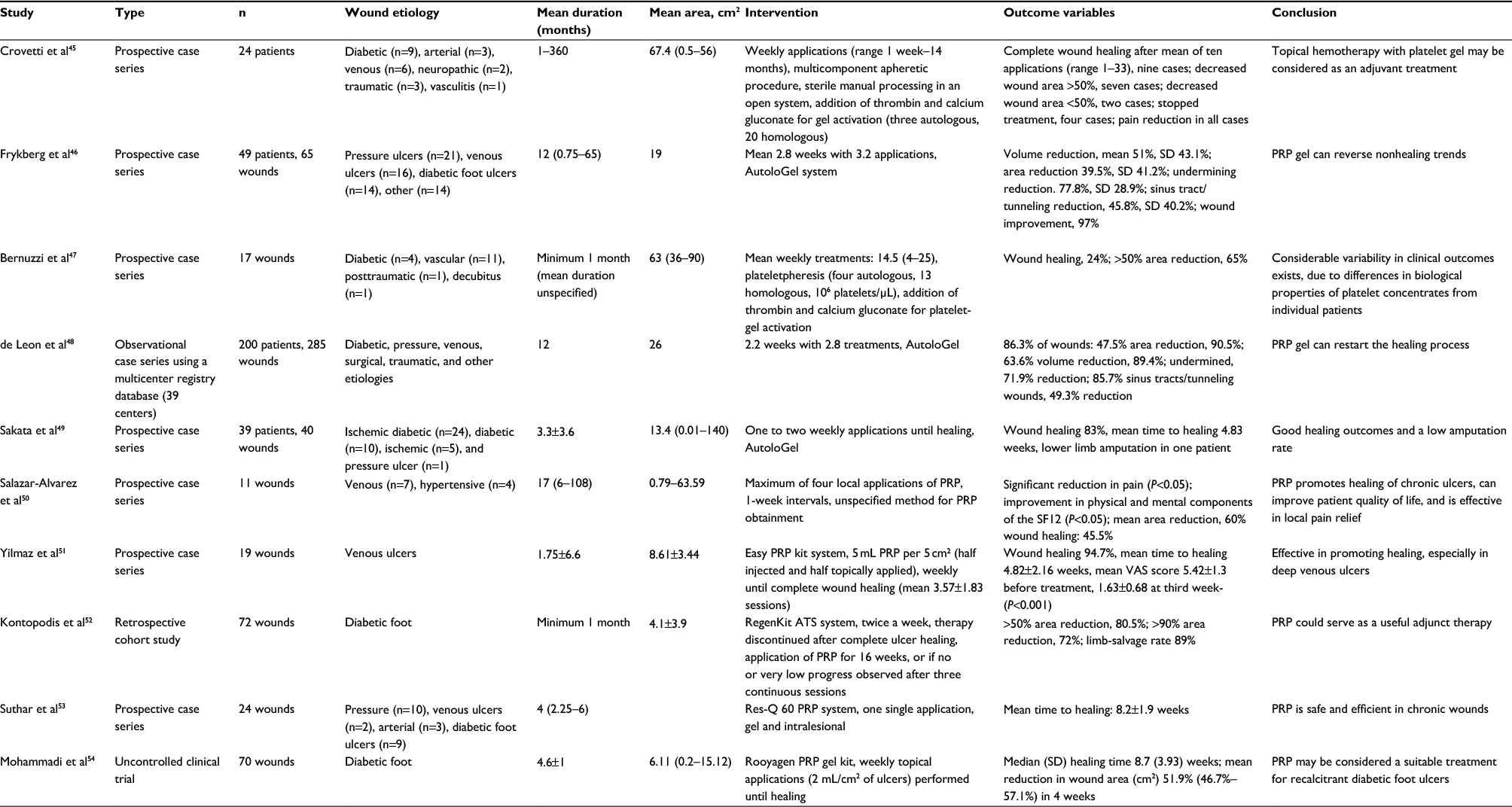
 | Table 2 Large-cohort studies Abbreviations: PRP, platelet-rich plasma; PPP, platelet-poor plasma; DUs, diabetic ulcers; DFUs, diabetic foot ulcers; VAS, visual analogue scale. |
The results of ten uncontrolled studies (seven prospective case series,45–47,49,50 one uncontrolled clinical trial,54 one retrospective cohort study,52 and one observational case series using a multicenter registry database48) are analyzed in this review (Table 1). Sample sizes range from eleven to 285 wounds. Both duration and baseline area of included ulcers were heterogeneous (1–17 months). Except for the studies by Yilmaz et al51 and Mohammadi et al,54 the rest of the series included ulcers of various etiologies. Yilmaz et al and Suthar et al53 applied both topical and injected PRP, whereas the other authors applied it just topically (PRP gel). Weekly application was the most frequent protocol. The number of treatment sessions was enormously variable, from 1 week to 14 months. The most frequently registered outcomes were wound healing and wound-area-reduction percentages. Salazar-Alvarez et al50 measured reduction and impact on quality of life, and found significant amelioration in both variables. PRP treatment had been associated with pain relief, showing a statistically significant reduction in the number of intravenous analgesics during PRP therapy. Asfaha et al59 associated this analgesic activity to the PAR4 pathway. Our clinical experience confirms this pain reduction and impact on quality of life in any wound etiology.18
Considering that both included ulcers and outcome variables are different among these studies, it is difficult to draw a concise summary of the results. Regarding mean wound-area reduction, in most of the studies it was superior to 50% at week 4. Mean time to healing ranged between 4 and 10 weeks. Wound-healing rates were highly variable inter- and intrastudy: 45%–95%. Bernuzzi et al,47 who included autologous and homologous PRP applications, posited that the variability in clinical outcomes of their series may have been due to differences in biological properties of platelet concentrates from individual patients.
Thirteen randomized clinical trials25,32–44 were also included in this review, six of which were double-blind placebo-controlled trials25,32–36 (Table 2). Regarding etiology, five of the studies recruited mixed-etiology ulcers,25,32,36,38,41 three considered venous ulcers,33,34,42 and the other five diabetic foot ulcers.36,37,39,40,44 Four studies, including mixed ulcers and venous ulcers, did not find clinical evidence to support the benefit of PRP in wound healing.32–35
The largest study considering just venous ulcers was conducted by Stacey et al,33 and included 86 patients (42 in the experimental and 44 in the control group). Autologous platelets were separated by centrifugation and platelet lysate was obtained by sonication. Platelet lysate was applied twice weekly until healing or for a 9-month period. Over the 36-week study period, the investigators did not find any improvement in wound healing with the use of platelet lysate (>75% in both groups without statistical differences).
Senet et al34 also studied the potential benefit of PRP in venous ulcers in a randomized double-blind clinical trial of 15 patients (eight in the experimental and seven in the control group). PRP treatment (frozen autologous platelet suspension in saline solution) was applied three times a week, together with hydrocolloids and standardized compression bandages, until either full epithelialization or 12 weeks of treatment. Mean percentage reduction in ulcer area was 26.2% in the group versus 15.2% in the placebo group (P=0.94). This study is especially interesting, because wound fluid was collected and local healing mediators measured. Even though TIMP1 concentrations increased significantly, growth-factor levels were not modified with PRP treatment. The authors of this study, which was essentially limited by a small sample, remarked that the absence of PRP healing effect could be explained by the destructive role of high levels of proteases found in wound fluid from chronic venous ulcers, and suggested the possible benefit of delivering platelet products together with protease inhibitors. The combined use of PRP and a protease-inhibitor polymeric device has shown healing promotion in a clinical trial with diabetic foot ulcers.37
Regarding clinical trials of only diabetic foot ulcers, we identified five,36–40 and the results in all were in favor of PRP treatment. Jeong et al39 conducted the largest study. A total of 52 patients were treated using a blood-bank platelet concentrate, and 48 were included in the control group (treatment with topical fibrinogen and thrombin). The use of those concentrates avoided the requirement of blood aspiration from the patient or posterior platelet separation. Complete wound healing was achieved in 79% of patients in the treatment group in comparison with 46% in the control group (P<0.05). The times required for complete healing were 7±1.9 and 9.2±2.2 weeks in the blood-bank platelet concentrate-treated and control groups, respectively (P<0.05). Patient satisfaction with treatment was also significantly higher in the interventional group (P<0.05). No adverse events related to the study treatment were identified.
Driver et al36 had previously designed a multicentric clinical trial on 72 diabetic foot ulcers. The study results were also better in the PRP group. Complete healing was achieved in 81.3% of the lesions treated with PRP gel, whereas just 42.1% of the lesions in the control group healed (P=0.036). However, these promising results were overshadowed by the study limitations, mainly the high rate of patient dropout (44.4%).
In light of all these findings, both in case series and controlled trials, we can make a specific comment regarding the efficacy of PRP in different chronic wounds. Whereas enhancement of wound healing has been found in both case series and clinical trials that have included diabetic feet, the beneficial results of PRP in venous leg ulcers found in case series have not been confirmed in clinical trials. Consequently, the authors suggest that even if all chronic wounds are characterized by a proinflammatory microenvironment, where growth factors are destroyed, the effect of providing the wound with a higher amount of these proteins depends on the etiology. The role that different factors play in the proteolytic microenvironment of chronic wounds should be further studied, in order to establish the real utility of adjuvant therapies in optimized etiological treatment (compression therapy in leg ulcers).
Considering the other main groups of chronic ulcers, arterial and pressure ulcers, no clinical trials have been performed specifically to analyze the effect of PRP application in these lesions. The limitations that characterize the published clinical trials prevent quantitative systematic reviews from obtaining strong and representative conclusions.
Various systematic reviews and meta-analysis25,55–58 have been conducted to evaluate the use of PRP for the treatment of cutaneous wounds compared to standard wound care (Table 3). All of them conclude that PRP therapy can positively impact wound healing, mainly in patients with nonhealing diabetic foot ulcers. However, all these reviews highlight the important limitations of the included studies, such as heterogeneous patient populations, small samples in clinical trials, lack of long-term follow-up, different types of products and regimens, and frequent study support by manufacturers.
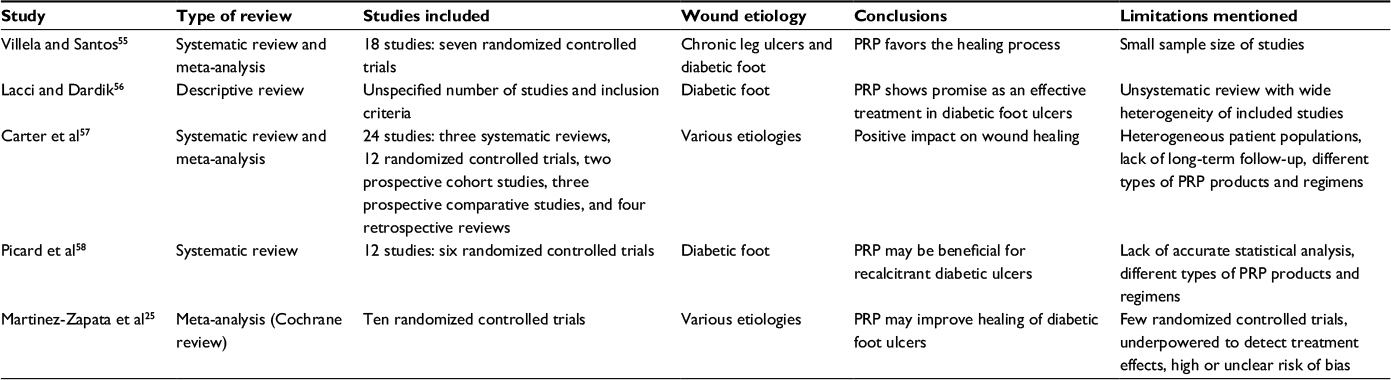 | Table 3 Descriptive and systematic reviews Abbreviation: PRP, platelet-rich plasma. |
A recent meta-analysis25 of ten randomized controlled trials with 442 patients (42% women), concluded that even if PRP may improve the healing of foot ulcers associated with diabetes, it is unclear whether PRP influences the healing of other chronic wounds. Nine of these ten studies have been included in Table 2. We did not include the trial by Rucigaj and Lunder,43 because of the limited information available in the conference abstract were the results were published. The median number of participants per randomized controlled trial was 29 (range 10–117), and autologous PRP was compared with placebo or alternative treatments. Considering etiology, four of the studies in the meta-analysis recruited mixed-etiology ulcers,25,32,35,38 three considered venous ulcers,33–4,43 and the three others diabetic foot ulcers.36,37,39 The average treatment duration was 12 weeks (8–40 weeks). Three studies reported wound complications, such as infection or dermatitis, but results showed no difference in the risk of adverse events in people treated with PRP or standard care. This systematic review presents important limitations, such as the risk of bias in most of the studies and the heterogeneity of the result variables that were measured (Table 2). Consequently, considering the favorable clinical response found in several studies, the authors suggest that powerful, well-designed clinical trials are needed to determine the real utility of PRP in chronic-ulcer healing. It has to be considered that variability exists in the obtainment and application of PRP, which may hinder the design and implementation of well-designed randomized controlled trials.
In addition to its benefits as a sole therapy, PRP has shown promising results when combined with other treatments, such as adipose-derived stem cells. In a randomized controlled trial with an 18-month follow-up period, 24 control-group patients with 31 chronic skin ulcers were treated with standard wound care, while 16 experimental-group patients with 21 chronic skin ulcers were treated with standard wound care and one combined PRP–adipose-derived stem-cell injection. The control and experimental groups had similar healing rates, but wound-closure rates were significantly different, favoring the experimental group.60
Considering the role of PRP as a delivery system of mitogenic and chemostatic factors, platelet gel has been used in small uncontrolled cohort studies combined with thin split-thickness skin grafts with or without fibrin glue (hemostatic tissue sealant that avoids the use of staples or sutures) to enhance skin-graft take. Recalcitrant ulcers of various etiologies were enrolled in the studies. No adverse reactions were observed.61,62 Negative-pressure wound therapy or light-emitting diodes have also been combined in small heterogeneous case series, with significant amelioration in different healing outcomes.63 To date, no robust evidence exists to enable the inclusion of reproducible standardized protocols for PRP treatment in chronic-wound guidelines.
In a diabetic inpatient clinical guideline, the National Institute for Health and Care Excellence recommended that autologous PRP gel should not be offered as treatment for diabetic foot problems unless part of a clinical trial.64 Regarding guidelines supported by the Wound Healing Society, indications refer to growth factors in general and no specific references to PRP can be found. For the treatment of diabetic ulcers, PDGF is effective in treating diabetic neurotrophic foot ulcers (evidence level I).65 In guidelines for the treatment of pressure ulcers, the Wound Healing Society states that the use of growth-factor therapy should be considered for pressure ulcers that are not responsive to initial comprehensive therapy and/or before surgical repair (level II).66 In guidelines for the treatment of venous ulcers, the Wound Healing Society states that cytokine growth factors have yet to be shown to demonstrate sufficient statistically significant results of effectiveness to recommend any of them for treatment of venous ulcers, although isolated reports suggest their potential usefulness (level I).67
In relation to health economics, PRP may be considered a cost-effective alternative. Studies that have analyzed the impact of the treatment of chronic wounds with PRP in comparison with conventional dressings have shown improvement in quality of life and cost reduction for the health system.68,69
Conclusion
Chronic wounds that do not respond to conventional treatment are not rare, and thus constitute a real challenge for the clinician. PRP represents a viable alternative treatment for recalcitrant chronic ulcers, whose efficacy has been demonstrated both in vitro and in vivo. However, stronger scientific evidence is required to support its potential benefit for use in chronic wounds. Even though several studies describe interesting results with PRP application in chronic ulcers, the absence of clinical protocols and guidelines is hindering the extension of use. As other published reviews have previously concluded, robust clinical trials are essential to determine the most accurate indications for use and the most recommended method of PRP obtainment and application.
The design of clinical protocols and the extension of PRP use in wound-care centers could have an important socioeconomic impact and see improvement in patients’ quality of life. Regenerative medicine in wound healing is a continuously innovative area. Its objectives are both providing essential elements for damaged-tissue replacement and enhancing intrinsic regenerative capacity. Clinical experience shows that combination of different regenerative techniques may enhance healing.
Disclosure
The authors report no conflicts of interest in this work.
References
Schreml S, Szeimies RM, Prantl L, Landthaler M, Babilas P. Wound healing in the 21st century. J Am Acad Dermatol. 2010;63:866–868. | ||
Phillips T. Ulceras. In: Bolognia JL, Jorizzo JL, Rapini RP, editors. Dermatologia. 2nd ed. London: Mosby; 2008:1597–1614. | ||
Lazaro JL, Izzo V, Meaume S, Davies AH, Lobmann R, Uccioli L. Elevated levels of matrix metalloproteinases and chronic wound healing: an updated review of clinical evidence. J Wound Care. 2016;25:277–287. | ||
Brölmann FE, Ubbink DT, Nelson EA, Munte AK, van der Horst CM, Vermeulen H. Evidence-based decisions for local and systemic wound care. Br J Surg. 2012;99:1172–1183. | ||
Flanagan M. Principles of wound management. In: Flanagan M, editor. Wound Healing and Skin Integrity. Oxford: Wiley-Blackwell; 2013:66–86. | ||
Skórkowska-Telichowska K, Czemplik M, Kulma A, Szopa J. The local treatment and available dressings designed for chronic wounds. J Am Acad Dermatol. 2013;68:e117–e126. | ||
Nurden AT, Nurden P, Sanchez M, Andia I, Anitua E. Platelets and wound healing. Front Biosci. 2008;13:3532–3548. | ||
Andia I, Abate M. Platelet rich plasma (PRP):underlying biology and clinical correlates. Regen Med. 2013;8:645–658. | ||
Sánchez M, Andia I, Anitua E, Sánchez P. Platelet rich plasma (PRP) biotechnology: concepts and therapeutic applications in orthopedics and sports medicine. In: Agbo EC, editor. Innovations in Biotechnology. Rijeka, Croatia: InTech; 2012:113–138. | ||
Kim SA, Ryu HW, Lee KS, Cho JW. Application of platelet-rich plasma accelerates the wound healing process in acute and chronic ulcers through rapid migration and upregulation of cyclin A and CDK4 in HaCaT cells. Mol Med Rep. 2013;7:476–480. | ||
Steed DL. Clinical evaluation of recombinant human platelet-derived growth factor for the treatment of lower extremity ulcers. Plast Reconstr Surg. 2006;117:143S–151S. | ||
Anitua E. Plasma rich in growth factors: preliminary results of use in the preparation of future sites for implants. Int J Oral Maxillofac Implants. 1999;14:529–535. | ||
Mazzucco L, Balbo V, Cattana E, Guaschino R, Borzini P. Not every PRP-gel is born equal: evaluation of growth factor availability for tissues through four PRP-gel preparations – Fibrinet, RegenPRP-kit, Plateltex and one manual procedure. Vox Sang. 2009;97:110–118. | ||
Zimmermann R, Jakubietz R, Jakubietz M, et al. Different preparation methods to obtain platelet components as a source of growth factors for local application. Transfusion. 2001;41:1217–1224. | ||
Marx RE. Platelet-rich plasma: evidence to support its use. J Oral Maxillofac Surg. 2004;62:489–496. | ||
Anitua E, Andia I, Ardanza B, Nurden P, Nurden AT. Autologous platelets as a source of proteins for healing and tissue regeneration. Thromb Haemost. 2004;91:4–15. | ||
Kaux JF, Le Goff C, Seidel L, et al. Comparative study of five techniques of preparation of platelet-rich plasma. Pathol Biol. 2011;59:157–160. | ||
Conde-Montero E. Validación de un Nuevo Método de Obtención de Plasma Rico en Plaquetas para su Aplicación en Úlceras Cutáneas Crónicas [doctoral thesis]. Madrid: Universidad Complutense de Madrid; 2016. | ||
Degen RM, Bernard JA, Oliver KS, Dines JS. Commercial separation systems designed for preparation of platelet-rich plasma yield differences in cellular composition. HSS J. 2017;13:75–80. | ||
Drago L, Bortolin M, Vassena C, Romanò CL, Taschieri S, Del Fabbro M. Plasma components and platelet activation are essential for the antimicrobial properties of autologous platelet-rich plasma: an in vitro study. PLoS One. 2014;9:e107813. | ||
Conde-Montero E, Horcajada-Reales C, Clavo P, Delgado-Sillero I, Suárez-Fernández R. Neuropathic ulcers in leprosy treated with intralesional platelet-rich plasma. Int Wound J. 2016;13:726–728. | ||
Castillo TN, Pouliot MA, Kim HJ, Dragoo JL. Comparison of growth factor and platelet concentration from commercial platelet-rich plasma separation systems. Am J Sports Med. 2011;39:266–271. | ||
Lopez-Fernandez R, Ramirez-Melgoza J, Martinez-Aguilar NE, Leon-Chavez A, Martinez-Fong D, Gonzalez-Barrios JA. Growth factor-enriched autologous plasma improves wound healing after surgical debridement in odontogenic necrotizing fasciitis: a case report. J Med Case Rep. 2011;5:98. | ||
Notodihardjo PV, Morimoto N, Kakudo N, et al. Gelatin hydrogel impregnated with platelet-rich plasma releasate promotes angiogenesis and wound healing in murine model. J Artif Organs. 2015;18:64–71. | ||
Martinez-Zapata MJ, Martí-Carvajal AJ, Solà I, et al. Autologous platelet-rich plasma for treating chronic wounds. Cochrane Database Syst Rev. 2016;5:CD006899. | ||
Martinez-Gonzalez JM, Cano-Sanchez J, Gonzalo-Lafuente JC, Campo-Trapero J, Esparza-Gomez G, Seoane J. Do ambulatory-use platelet-rich plasma (PRP) concentrates present risks? Med Oral. 2002;7:375–390. | ||
Knighton DR, Ciresi K, Fiegel VD, Schumerth S, Butler E, Cerra F. Stimulation of repair in chronic, nonhealing, cutaneous ulcers using platelet-derived wound healing formula. Surg Gynecol Obstet. 1990;170:56–60. | ||
Ficarelli E, Bernuzzi G, Tognetti E, et al. Treatment of chronic venous leg ulcers by platelet gel. Dermatol Ther. 2008;21:S13–S17. | ||
Sell SA, Ericksen JJ, Reis TW, Droste LR, Bhuiyan MB, Gater DR. A case report on the use of sustained release platelet-rich plasma for the treatment of chronic pressure ulcers. J Spinal Cord Med. 2011;34:122–127. | ||
Ramos-Torrecillas J, De Luna-Bertos E, García-Martínez O, Díaz-Rodríguez L, Ruiz C. Use of platelet-rich plasma to treat pressure ulcers: a case study. J Wound Ostomy Continence Nurs. 2013;40:198–202. | ||
Jeong KH, Shin MK, Kim NI. Refractory lipodermatosclerosis treated with intralesional platelet-rich plasma. J Am Acad Dermatol. 2011;65:e157–e158. | ||
Krupski WC, Reilly LM, Perez S, Moss KM, Crombleholme PA, Rapp JH. A prospective randomized trial of autologous platelet-derived wound healing factors for treatment of chronic nonhealing wounds: a preliminary report. J Vasc Surg. 1991;14:526–532. | ||
Stacey MC, Mata SD, Trengove NJ, Mather CA. Randomised double-blind placebo controlled trial of topical autologous platelet lysate in venous ulcer healing. Eur J Vasc Endovasc Surg. 2000;20:296–301. | ||
Senet P, Bon FX, Benbunan M, Bussel A, Traineau R, Calvo F. Randomized trial and local biological effect of autologous platelets used as adjuvant therapy for chronic venous leg ulcers. J Vasc Surg. 2003;38:1342–1348. | ||
Weed B, Davis MD, Felty CL, et al. Autologous platelet lysate product versus placebo in patients with chronic leg ulcerations: a pilot study using a randomized, double-blind, placebo controlled trial. Wounds. 2004;16:273–282. | ||
Driver VR, Hanft J, Fylling CP, Beriou JM. A prospective, randomized, controlled trial of autologous platelet-rich plasma gel for the treatment of diabetic foot ulcers. Ostomy Wound Manage. 2006;52:68–87. | ||
Kakagia D, Kazakos K, Xarchas K, et al. Synergistic action of protease-modulating matrix and autologous growth factors in healing diabetic foot ulcers: a prospective randomized trial. J Diabetes Complications. 2007;21:387–391. | ||
Anitua E, Aguirre JJ, Algorta J, et al. Effectiveness of autologous preparation rich in growth factors for the treatment of chronic cutaneous ulcers. J Biomed Mater Res B Appl Biomater. 2008;84:415–421. | ||
Jeong SH, Han SK, Kim WK. Treatment of diabetic foot ulcers using a blood bank platelet concentrate. Plast Reconstr Surg. 2010;125:944–952. | ||
Setta HS, Elshahat A, Elsherbiny K, Massoud K, Safe I. Platelet-rich plasma versus platelet-poor plasma in the management of chronic diabetic foot ulcers: a comparative study. Int Wound J. 2011;8:307–312. | ||
Li L, Chen DW, Wang C, et al. Autologous platelet-rich gel for treatment of diabetic chronic refractory cutaneous ulcers: a prospective, randomized clinical trial. Wound Repair Regen. 2015;23:495–505. | ||
Cardeñosa ME, Domínguez-Maldonado G, Córdoba-Fernández A. Efficacy and safety of the use of platelet-rich plasma to manage venous ulcers. J Tissue Viability. 2017;26:138–143. | ||
Rucigaj TP, Lunder T. Stimulation of venous leg ulcers with thrombocytic growth factors: a randomized study. Poster presented at: 17th Conference of the European Wound Management Association; May 2–4, 2007; Glasgow, Scotland. | ||
Ahmed M, Reffat SA, Hassan A, Eskander F. Platelet-rich plasma for the treatment of clean diabetic foot ulcers. Ann Vasc Surg. 2017;38:206–211. | ||
Crovetti G, Martinelli G, Issi M, et al. Platelet gel for healing cutaneous chronic wounds. Transfus Apher Sci. 2004;30:145–151. | ||
Frykberg RG, Driver VR, Carman D, et al. Chronic wounds treated with a physiologically relevant concentration of platelet-rich plasma gel: a prospective case series. Ostomy Wound Manage. 2010;56:36–44. | ||
Bernuzzi G, Tardito S, Bussolati O, et al. Platelet gel in the treatment of cutaneous ulcers: the experience of the Immunohaematology and Transfusion Center of Parma. Blood Transfus. 2010;8:237–247. | ||
de Leon JM, Driver VR, Fylling CP, et al. The clinical relevance of treating chronic wounds with an enhanced near-physiological concentration of platelet-rich plasma gel. Adv Skin Wound Care. 2011;24:357–368. | ||
Sakata J, Sasaki S, Handa K, et al. A retrospective, longitudinal study to evaluate healing lower extremity wounds in patients with diabetes mellitus and ischemia using standard protocols of care and platelet-rich plasma gel in a Japanese wound care program. Ostomy Wound Manage. 2012;58:36–49. | ||
Salazar-Alvarez AE, Riera-del-Moral LF, García-Arranz M, Alvarez-García J, Concepción-Rodriguez NA, Riera-de-Cubas L. Use of platelet-rich plasma in the healing of chronic ulcers of the lower extremity. Actas Dermosifiliogr. 2014;105:597–604. | ||
Yilmaz S, Aksoy E, Doganci S, Yalcinkaya A, Diken AI, Cagli K. Autologous platelet-rich plasma in treatment of chronic venous leg ulcers: a prospective case series. Vascular. 2015;23:580–585. | ||
Kontopodis N, Tavlas E, Papadopoulos G, et al. Effectiveness of platelet-rich plasma to enhance healing of diabetic foot ulcers in patients with concomitant peripheral arterial disease and critical limb ischemia. Int J Low Extrem Wounds. 2016;15:45–51. | ||
Suthar M, Gupta S, Bukhari S, Ponemone V. Treatment of chronic non-healing ulcers using autologous platelet rich plasma: a case series. J Biomed Sci. 2017;24:16. | ||
Mohammadi MH, Molavi B, Mohammadi S, et al. Evaluation of wound healing in diabetic foot ulcer using platelet-rich plasma gel: a single-arm clinical trial. Transfus Apher Sci. 2017;56:160–164. | ||
Villela DL, Santos VL. Evidence on the use of platelet-rich plasma for diabetic ulcer: a systematic review. Growth Factors. 2010;28:111–116. | ||
Lacci KM, Dardik A. Platelet-rich plasma: support for its use in wound healing. Yale J Biol Med. 2010;83:1–9. | ||
Carter MJ, Fylling CP, Li WW, et al. Analysis of run-in and treatment data in a wound outcomes registry: clinical impact of topical platelet-rich plasma gel on healing trajectory. Int Wound J. 2011;8:638–650. | ||
Picard F, Hersant B, Bosc R, Meningaud JP. The growing evidence for the use of platelet-rich plasma on diabetic chronic wounds: a review and a proposal for a new standard care. Wound Repair Regen. 2015;23:638–643. | ||
Asfaha S, Cenac N, Houle S, et al. Protease activated receptor-4: a novel mechanism of inflammatory pain modulation. Br J Pharmacol. 2007;150:176–185. | ||
Raposio E, Bertozzi N, Bonomini S, et al. Adipose-derived stem cells added to platelet-rich plasma for chronic skin ulcer therapy. Wounds. 2016;28:126–131. | ||
Tzeng YS, Deng SC, Wang CH, Tsai JC, Chen TM, Burnouf T. Treatment of nonhealing diabetic lower extremity ulcers with skin graft and autologous platelet gel: a case series. Biomed Res Int. 2013;2013:837620. | ||
Chen TM, Tsai JC, Burnouf T. A novel technique combining platelet gel, skin graft, and fibrin glue for healing recalcitrant lower extremity ulcers. Dermatol Surg. 2010;36:453–460. | ||
Park KY, Kim IS, Yeo IK, Kim BJ, Kim MN. Treatment of refractory venous stasis ulcers with autologous platelet-rich plasma and light-emitting diodes: a pilot study. J Dermatolog Treat. 2013;24:332–335. | ||
National Institute for Health and Care Excellence. Diabetic Foot Problems: Prevention and Management. London: NICE; 2015. | ||
Lavery LA, Davis KE, Berriman SJ, et al. WHS guidelines update: diabetic foot ulcer treatment guidelines. Wound Repair Regen. 2016;24:112–126. | ||
Gould L, Stuntz M, Giovannelli M, et al. Wound Healing Society 2015 update on guidelines for pressure ulcers. Wound Repair Regen. 2016;24:145–162. | ||
Marston W, Tang J, Kirsner RS, Ennis W. Wound Healing Society 2015 update on guidelines for venous ulcers. Wound Repair Regen. 2016;24:136–144. | ||
Dougherty EJ. An evidence-based model comparing the cost-effectiveness of platelet-rich plasma gel to alternative therapies for patients with nonhealing diabetic foot ulcers. Adv Skin Wound Care. 2008;21:568–575. | ||
Cobos R, Aizpuru F, Parraza N, Anitua E, Orive G. Effectiveness and efficiency of platelet rich plasma in the treatment of diabetic ulcers. Curr Pharm Biotechnol. 2015;16:630–634. |
 © 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.