Back to Journals » Journal of Pain Research » Volume 13
Platelet-Rich Plasma-Derived Growth Factor vs Hyaluronic Acid Injection in the Individuals with Knee Osteoarthritis: A One Year Randomized Clinical Trial
Authors Raeissadat SA, Gharooee Ahangar A, Rayegani SM ![]() , Minator Sajjadi M, Ebrahimpour A, Yavari P
, Minator Sajjadi M, Ebrahimpour A, Yavari P
Received 1 April 2019
Accepted for publication 27 May 2020
Published 8 July 2020 Volume 2020:13 Pages 1699—1711
DOI https://doi.org/10.2147/JPR.S210715
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Michael Schatman
Seyed Ahmad Raeissadat,1 Azadeh Gharooee Ahangar,2 Seyed Mansoor Rayegani,1 Mohammadreza Minator Sajjadi,3 Adel Ebrahimpour,3 Pegah Yavari1
1Physical Medicine and Rehabilitation Research Center, Clinical Research Development Center of Shahid Modarres Hospital, Shahid Beheshti University of Medical Sciences, Tehran, Iran; 2Department of Orthopedic Surgery, Zanjan University of Medical Sciences, Zanjan, Iran; 3Taleghani Hospital, Shahid Beheshti University of Medical Sciences, Tehran, Iran
Correspondence: Pegah Yavari
Physical Medicine and Rehabilitation Research Center, Clinical Research Development Center of Shahid Modarres Hospital, Shahid Beheshti University of Medical Sciences, Tehran, Iran
Tel + 98 912 299 7782
Email [email protected]
Objective: In this study, we aimed at performing a comparison between intra-articular injections of PRP-derived growth factor (PGRF) and hyaluronic acid regarding their effect on pain and patient’s function in knee osteoarthritis, as well as their safety profiles.
Methods: During our single-masked randomized clinical trial, the candidates with symptomatic knee osteoarthritis received two intra-articular injections of PRGF with 3 weeks apart or received three weekly injections of HA. The mean improvements from before treatment until the second, sixth, and twelfth months post-intervention in scores obtained by visual analog scale (VAS), Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC), and Lequesne index were our primary outcomes.
Results: A total of 102 candidates were finally included in the study. Patients’ mean age was 57.08± 7.3 years old in the PRGF group compared to the mean age of 58.63± 7.09 years old in HA patients. In the PRGF group, total WOMAC index decreased from 41.96± 11.71 to 27.10± 12.3 (P = 0.02), and from 39.71± 10.4 to 32.41± 11.8 in the HA group after 12 months (P > 0.05). Regarding the Lequesne index, pain, ADL, and global scores significantly decreased after 12 months in the PRGF group compared to the HA group (P< 0.001). There was also a meaningful higher rate of satisfaction in the PRGF group compared to the HA group after 12 months of treatment (P< 0.001).
Conclusion: Besides significantly higher satisfaction belonging to the PRGF group, there was a statistically significant improvement in VAS score and global, pain, and ADL score of Lequesne by passing 12 months from injection in PRGF compared to HA.
Keywords: knee, osteoarthritis, PRP, PRP-derived growth factor, hyaluronic acid, intra-articular injections
Introduction
Osteoarthritis (OA) is a joint disease with the highest prevalence worldwide. Accordingly, its characteristic signs are as follows: increasing the loss of joint cartilage, synovial membrane changes, and reduction in the synovial fluid viscosity.1 In this regard, at first, erosion of articular cartilage and exposure of the bone under the cartilage occur in OA, resulting in the inflammation of the surrounding tissues. This complication may involve any joint, with cartilage destruction being the trademark sign of osteoarthritis.2–4
Since, at the moment, osteoarthritis lacks a definite cure, symptomatic relief is the foundation of treatment; however, reducing the pain and disability and maintaining or improving joint mobility is the mainstay management. Also, non-surgical modalities such as exercise and weight reduction, are preferred due to having less satisfactory symptomatic and functional results of surgery.6–8 On the other hand, patient compliance with non-surgical approaches is weak, while some medications such as standard painkillers and NSAIDs may have the risk of adverse effects.5,10,11
Recent studies have worked on new non-surgical approaches including Intra-Articular Injection (IAI) of hyaluronic acid (HA), ozone therapy, prolotherapy, intra-articular botulinum toxin administration, and platelet-rich plasma (PRP), which are considered as the favored candidates among the existing management options for knee OA.12–16
HA is a chief viscoelastic constituent of the synovial fluid present inside the joints with lubricant and cushioning properties. In an OA-affected patient, a reduction occurs in the concentration and molecular weight of HA, which as a result, affects its properties. In clinical practice, it was shown that, infiltration of HA in the joint can temporarily restore the joint’s normal function, giving the patient symptom relief. Also, the effectiveness of HA in knee OA treatment has been shown in a number of clinical trials.17–20 Moreover, HA has a longer-lasting effect compared to corticosteroid infiltrations.21,22 Considering the direct costs and the costs associated with the potential side effects, the cost-effectiveness of HA compared to oral NSAIDs, physical therapy, and assistive devices has been reported in the literature. Despite the lack of certain evidence on the recent guidelines, intra-articular HA has been used for several years, which is considered as the standard treatment in knee OA.19,20
PRP is a blood component with non-transfusion usage, utilized to treat many pathologies as a topical agent, as injections for tendons or ligament injury, IA injections in osteoarthritis or very recently in carpal tunnel syndrome.24 PRP is collected from the blood of each patient and is used for that patient; so, it is considered as a safe practice.25,26 PRP treatment efficacy have been reported in several studies, particularly in the first years of treatment.27–31 It is also possible to perform PRP injections in the office. Accordingly, its therapeutic benefits are thought to be resulted from the increased concentration of the platelet-derived growth factors in the alpha granules of the platelets injected into the knee.32–34 The roles of these growth factors are affecting the chondrocytes, promoting the synthesis of the cartilage matrix, increasing the growth and migration of cells, and facilitating protein transcription. The theory behind the use of PRGF is the supra-physiological amounts of platelet-derived factors that are directly delivered at the site of the damaged cartilage such as OA, and can trigger the natural healing process and tissue regeneration as well as facilitation of the anti-inflammatory response.
Of many biologic treatments employed for modifying symptoms in OA treatment, plasma rich in growth factors (PRGF) articular injection has proven its safety and efficacy as an autologous treatment method.36–38 The role of PRGF” preparation rich the followings in growth factors: a low-concentrate PRP with no leukocytes on OA synoviocytes with or without exposition to IL-1ß, to mimic the overproduction of pro-inflammatory cytokines in the joint environment during OA progression”, which was investigated by Anitua et al Accordingly, their results showed significant enhancement of HA secretion relative to PRP, and irrespective of IL-1b. It also modified angiogenesis to a more balanced status.
Moreover, this concentrated platelet suspension in plasma leads to the formation of an in situ matrix of fibrin and also facilitates the delivery of growth factors, cytokines, and morphogens 40 (IGF-1, TGFB1, HGF, PDGF, VEGF, NGF, BDNF, CTGF, BMPs, vitronectin, fibronectin, SDF-1, and PF4 among others), all of which proven chondroprotective, anabolic, anti-inflammatory, and immunomodulatory properties.41–45 This product showed encouraging results in knee OA, while it indicates lower complications such as pain and swelling after injection. In contrast to PRP, which has been compared with placebo or HA in many studies in the literature showing conflicting results,38,46-48 the evidence is scarce when it comes to investigate the use of PGRF articular injection in improving long term outcome, compared to HA in the patients with knee OA.26,49
Our previous study demonstrated that, the pain reduction and functional improvement effects of PGRF and HA are very close in those patients suffering from mild to moderate knee OA. In this regard, both products retained their positive effect up to 6 months, while showing no meaningful difference. The goal of the present study was to compare the 12-month clinical efficacy and safety of intra-articular injections of PRP-derived growth factor (PRGF) with HA on the patients with knee OA using WOMAC, LEQUESNE, and VAS scores used as the outcome measures.
Materials and Methods
The present study conducted a long-term follow-up on the existing clinical trials published in our department. Our randomized clinical trial (RCT) was performed in Moddares Medical Center of Tehran, Iran, from July 2016 to September 2018. The institutional review board approved this RCT design and methodology, which were then registered in the Iranian Registry of Clinical Trials (www.irct.ir), regulatory representative of the World Health Organization for Iranian clinical trials, with registration code of IRCT2016071513442N11.
The main purpose of this comparative RCT was assessing the efficacy of these two therapeutic groups treated by intraarticular injection of plasma rich in growth factor (PRGF) and hyaluronic acid (HA) in the patients with knee osteoarthritis (OA) at the 2nd, 6th, and 12th months after injection.
Patient Selection and Randomization
The signed written informed consent was obtained from all research units prior to participation in this RCT. A knee x-ray was prepared in anteroposterior weight-bearing, and lateral views to diagnosing and grading OA. A specialist in physical medicine and rehabilitation explained the study design, objectives, advantages, and side effects for those patients who met the inclusion criteria. Subsequently, the selected subjects were assigned into two groups (Group I: received IAIs with PRGFs and Group II: received IAIs with HA) using the permuted block randomization method. An assistant who was a resident in physical medicine and rehabilitation, and was also unaware of the group allocation, performed the recruitment and randomization.
The inclusion criteria were the age of 40–70 years old, suffering from knee pain in the past six months, history of complaints for at least one month, the need for painkillers, and knee osteoarthritis confirmed by radiography (Kellgren-Lawrence classification grade 2–3). In addition, the exclusion criteria were the presence of systemic disorders (ie, diabetes mellitus, immunodeficiency, and collagen vascular diseases), the history of malignancy, the history of autoimmune diseases or platelet disorders, body mass index of over 33 kg/m2, and the use of nonsteroidal anti-inflammatory drugs (NSAIDs) within the past two days or aspirin within the seven days before the injection, the use of anticoagulant or antiplatelet medications within ten days before the injection, the history of systemic steroids in two weeks before the injection, the presence of IAIs within the past three months before the injection, the hemoglobin level of less than 12 g/dl or platelet count of less than 150 000/μl36, the history of a recently occurred severe knee trauma, knee septic arthritis, the active ulcer or septic arthritis of knee, genu varum or valgum of over 20°, allergy to proteins of egg and chicken or HA, and the use of ginger or turmeric within a week before the injection.
Product Preparation
In the present study, the Group I separately received two and three weeks of IAIs with platelet-rich plasma (PRP)-derived growth factor (PRGF), which were prepared in terms of the following protocol. At first, the PRP was produced from the participants who were referred to the laboratory of the hospital using Rooyagen Kit (Arya MabnaTashkhis Corporation, RN: 312,569) with the behind principle of a dual-spin system aseptically. To fulfil this, 35 CC of blood samples were taken from the patients to obtain PRP having a concentration of 4 to 6 times more than the mean normal values, which were then added by 5 mL of citric acid dextrose solution A for anticoagulation. Complete blood count (CBC) was also measured using 1 mL of the collected samples. Afterward, the blood samples were centrifuged for 15 min at 1600 rpm, resulting in three phases of red blood cells (lower), white blood cells (middle), and plasma (upper). The two uppermost layers were centrifuged again for 7 minutes at 3500 rpm. The final resulting product contained 8 mL of plasma with 4.6 ± 0.7 times more than the platelet concentration.
Next, 1.5 mL of platelet-activating factor (Rooyagen) containing epinephrine and calcium chloride (25mmol/l) was poured, stirred, and then placed in warm water for 20–30 min at 40±1°C to release the platelet factors, which occurs due to platelet activation, in which fibrin interacts with platelets through glycoprotein IIa/IIIb surface proteins, hereby producing growth factors by platelets.
In this step, two phases were formed in a plasma preparation named as the supernatant liquid phase (PRGF) and the solid phase (platelet clumps+fibrin network). The third centrifugation stage was performed for 4 minutes at 4000 rpm to separate platelets and fibrin stick attached to the bottom of the tubes. The remaining fluid (5 mL) was injected within 20 minutes of its preparation, and no local anesthetics were used before plasma product injection.
The level of various growth factors present in the final product PRGF was evaluated in 10 volunteers of the PRGF group, which resulted in vascular endothelial growth factor (312±23.2ng/mL), PDGF (279±52.1ng/mL), IGF (1.3±0.7ng/mL), TGF-β1 (2.0±0.1ng/mL), and TGF-β 2 (1.1±0.3ng/mL). Also, no platelet or WBCs was found in our product, and the hepatocyte growth factor level was measured as 321pg/mL, using an enzyme-linked immunosorbent assay method.
Interventions
After disinfection, the lateral mid-patellar injection of PRGF was performed using G21 needles with the knee extended. Moreover, an anteromedial method with flexed knee was applied for a patient, because of inadequate space. Active knee flexion and extension were prescribed after a 20-min rest for the injected fluid dispersion inside the entire synovial space. After three weeks, the same injection settings were repeated for the second time, and the number of injections was determined in terms of the experiences of the authors due to having no consensus in this regard. The group II underwent three injections of HA weekly (Hyalgan®, FidiaFarmaceutici S.p.A., Abano Terme, Italy). In case of feeling any pain, a single dose of acetaminophen (500 mg, oral) was given to the patients two hours after the injection.
The content of each prefilled syringe was the active ingredient sodium hyaluronate (20 mg) in the liquid (2 mL) with a molecular weight of 500 to 730 kDa. The injection of hyalgan syringes was aseptically performed via G21 needles based on the same above-mentioned protocol. After injections, the subjects were requested for their knee flexion and extension for several times. The same injection processes were performed for the second and third injections with a week of interval. A similarly skilled specialist in physical medicine and rehabilitation, who was not blinded to group allocation, performed the IAIs in these two groups.
Follow-Up After Interventions
The discharge of the patients was after a rest time of 10–15 min. Besides, only mild physical activities and limited weight-bearing over the involved lower limb were instructed for the patients.
The therapeutic exercise was administered to the patients in both groups. One week after the first injection, the patients were asked to report the exercise process. Moreover, one month after the first injection, the patients were asked again via phone call. In follow-ups, the patients were also asked about their exercise to make sure that the patients were regularly performing the exercise.
Accordingly, they were also recommended to use an ice pack daily for 10 minutes every 8 hours, through the first two days. Moreover, up to four 500-mg acetaminophen tablets were proscribed for the possible mild to moderate pain, or codeine/acetaminophen for the persisted pain. Other analgesics were also prohibited up to 5 days after injection. This research authors recommended routine knee-oriented exercise therapy for both groups.
Another blinded resident assistant followed up all the subjects at the clinic after the 2nd, 6th, and 12th months of injections. The intensity of pain, joint stiffness, and problems with the injection site were monitored, and the number of painkillers consumed was then checked continuously. A 24-h phone line was considered in case of any emergent condition. The reason for the absence of each patient in timely visits was followed up for any possible exclusion from the study.
Outcome Measures
At the baseline, we collected demographic profiles (sex, age, body mass index BMI), clinical characteristics, and degree of osteoarthritis measured by with Kellgren-Lawrence score, laterality, and side effects. Additional measures were also performed at baseline and at the 2nd, 6th, and 12th months of follow-up. Primary outcomes in our study were considered as a reduction of pain and an improvement of function by assessing the decreased global score of the WOMAC Index (Western Ontario and McMaster University Osteoarthritis Index) 51 along with the subscales of pain, stiffness, and physical function, and the decreased global score of LEQUESNE Index 52 and the relevant subscales of pain, maximum walking distance (MWD) and activities of daily living (ADL), as well as Visual Analogue Scale (VAS) at the baseline and at the 2nd, 6th, and 12th months (48 weeks) after the injection.
The secondary outcome was considered as the patients’ satisfaction after 12 months and the injection-related complications.
Safety Assessments
We analyzed and then documented the grade of severity, received treatment, and complications for each visit. The patient’s diaries consisted of a daily usage of rescue medication.
Sample Size Calculation
The sample size was 50 in each group by considering the results from the earlier study 50 regarding a significant mean difference in the decreased scores of WOMAC and LEQUESNE, the equation for calculating the sample size to compare two means, and the test power of 80% at the significance level of 0.5. The difference between the efficacies of these two therapeutic methods was described as effect size (raw mean difference [RMD]) and then analyzed using Mann–Whitney U-test.
Statistical Analysis
A medical statistics expert who was blinded to the group allocation inserted the attained data from pre/post-treatment to the computer and then analyzed them by SPSS v.16 software using Shapiro–Wilk or Kolmogorov–Smirnov for the evaluation of data normality, independent samples t-test for comparing the mean scores between these two groups, and the repeated measures analysis of variance (ANOVA) for assessing the intra/inter-group changes.
Results
Patient Characteristics
From 211 candidates with knee osteoarthritis who were eligible to participate in our study, 92 patients were excluded, and 119 candidates were then included in this study and had IAIs (PRGF=60, HA=59). During the 12 months of this study, 7 patients in HA group and 10 patients in PRGF group were excluded from the study (because of missing follow up, total knee arthroplasty, the increased knee pain, IAI ozone therapy, and PT) and 50 patients in PRGF and 52 in Hyalgan groups completed the study protocol (Figure 1). The candidates’ mean age was 57.81 ± 7.2 years old (43–70), 71.6% of the patients were female, and 21 (73.9%) patients were obese or overweight. The initial characteristics of this study subjects are shown in Table 1. As can be observed, the subjects were statistically matched between the two groups.
 |
Table 1 Initial Characteristics of the Study Subjects |
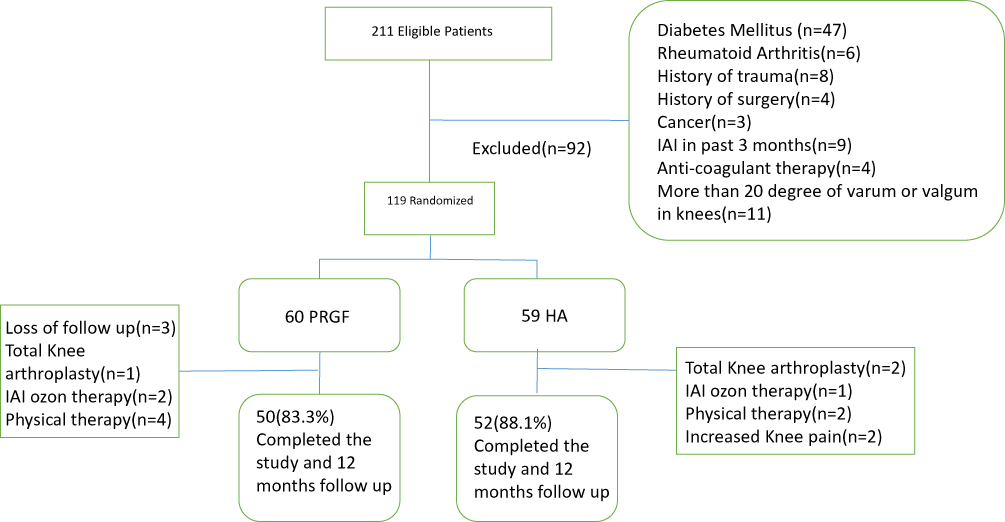 |
Figure 1 Enrollment and allocation diagram. IAI, intra-articular injection; HA, hyaluronic acid; PRGF, plasma rich in growth factor. |
Outcomes
The VAS for pain, WOMAC, and Lequesne instrument mean scores acquired by the subjects at baseline and at the 2nd, 6th, and 12th months after injection are shown in Tables 2 and 3.
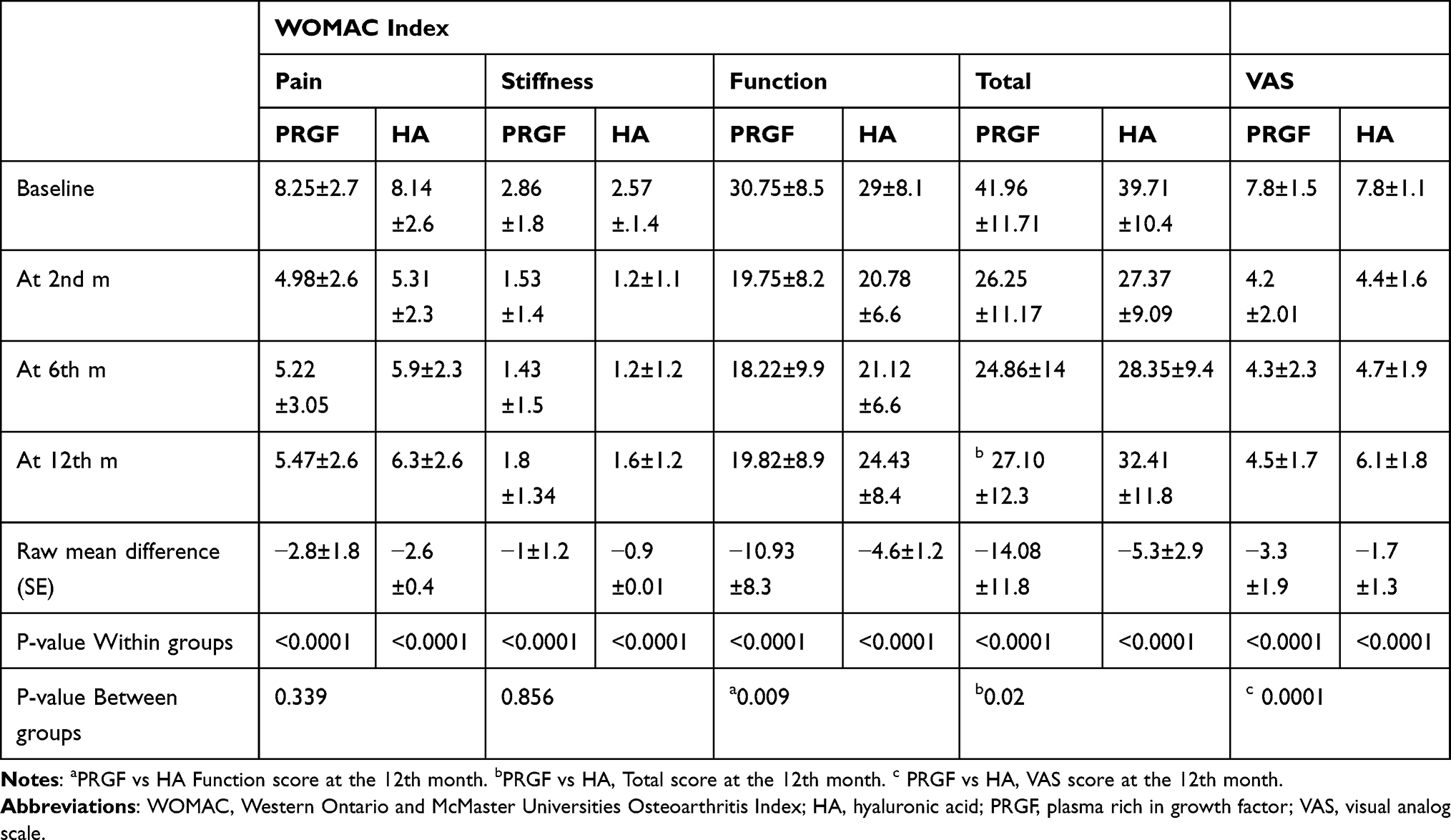 |
Table 2 WOMAC and VAS Mean Scores at Baseline, and at the 2nd, 6th, and 12th Months After Injection |
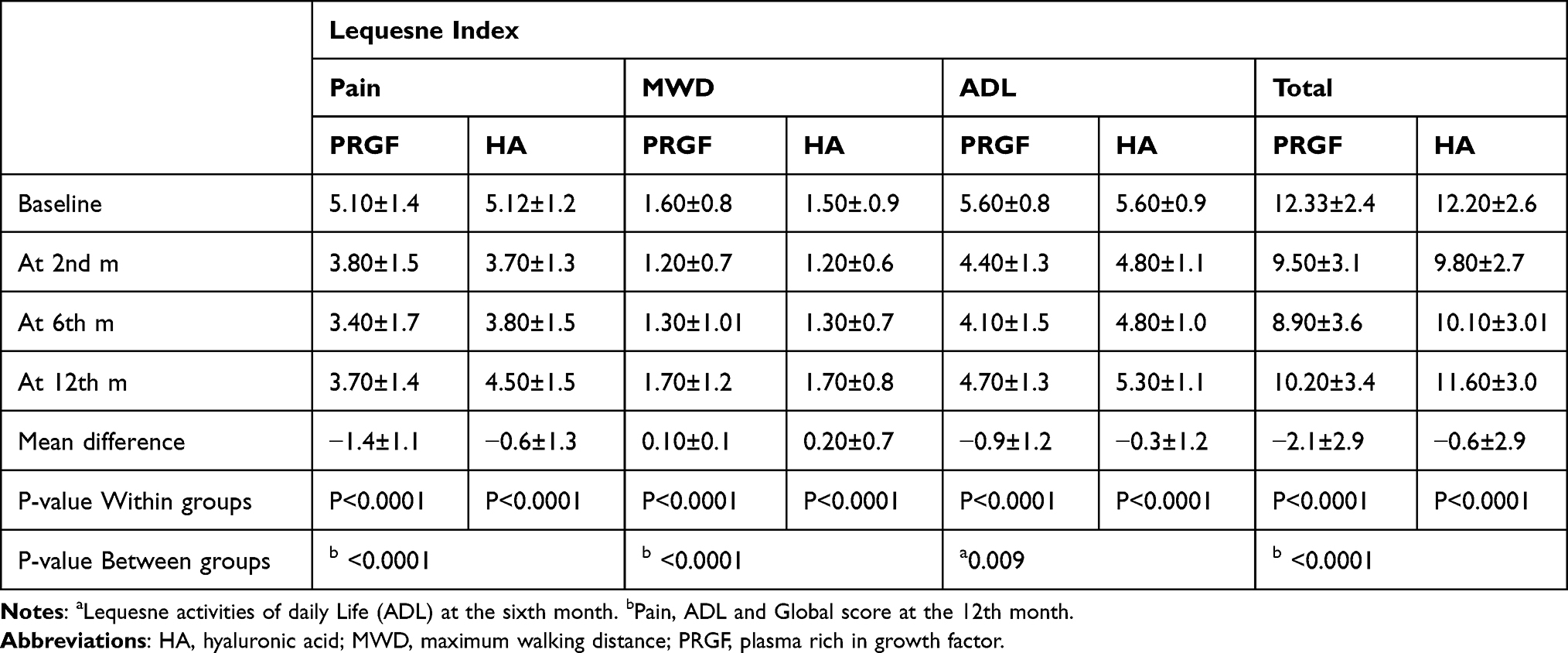 |
Table 3 Lequesne Mean Scores at Baseline, and at the 2nd, 6th, and 12th Months After Injection |
Based on ANOVA for the repeated measures, the decreased pattern observed in WOMAC and VAS was statistically significant within each group during the study time (F=108.8, P<0.001).
During 12-month follow-up, VAS score was significantly higher in the HA group (PRGF vs HA, 4.59: 6.18) (F = 0.02, P < 0.0001). Also, HA group had significantly higher scores in sub-score of function in the WOMAC index (PRGF vs HA, 19.82: 24.43) (F = 0.2, P = 0.009). The WOMAC global score was also significantly higher in the HA group compared to the PRGF group (27.1: 34. PRGF vs HA) (F = 0.1, P = 0.02).
The %change from baseline was calculated with the following formula:
([Baseline score – 12th month score/Baseline score] *100).
According to Table 3, there was no statistically significant difference between these two groups at baseline and after two months of injection in each one of the scores (p> 0.05). By passing 6 months from injection, a significant difference was observed in the subscale of Lequesne activities of daily life (ADL), which shows that HA injection group had a higher score (F = 3.7, P = 0.009).
Also, after 12 months, significant differences were observed in Lequesne global, pain, and ADL sub-scales scores between these two groups. HA group had a higher score in pain (PRGF vs HA, 3.71: 4.58), ADL (PRGF vs HA, 4.78: 5.36) and the global score (PRGF vs HA, 10.20: 11.67), (P <0.05). Figures 2–4 show the changes of total WOMAC, Lequesne, and VAS scores during 12 months of study in both groups.
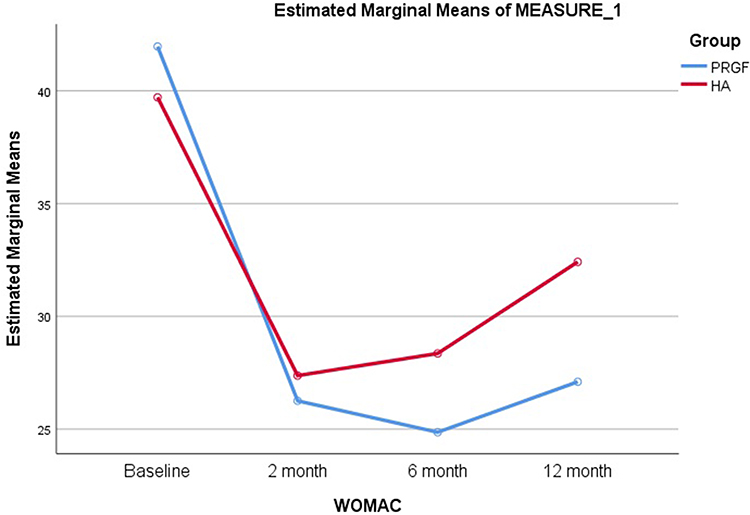 |
Figure 2 Means of WOMAC total scores at baseline, and at the 2nd, 6th, and 12th months after injection. PRGF, plasma rich in growth factor; WOMAC, Western Ontario and McMaster Universities Osteoarthritis Index; HA, hyaluronic acid. |
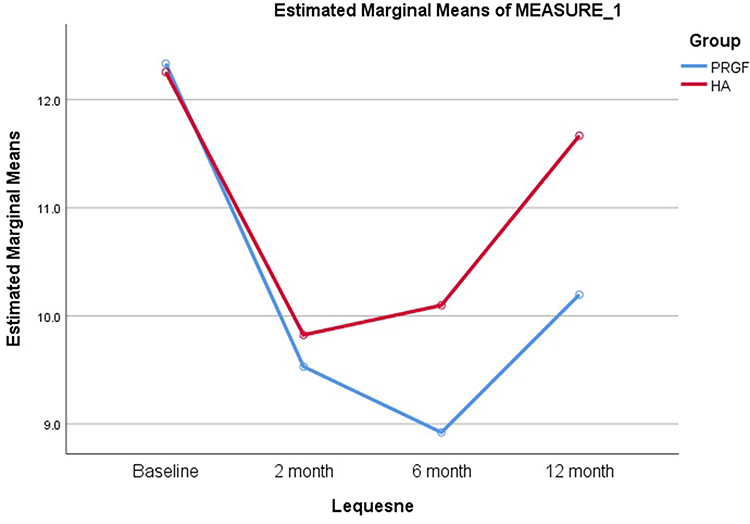 |
Figure 3 Mean values of Lequesne total at baseline, and at the 2nd, 6th, and 12th months after injection. PRGF, plasma rich in growth factor; HA, hyaluronic acid. |
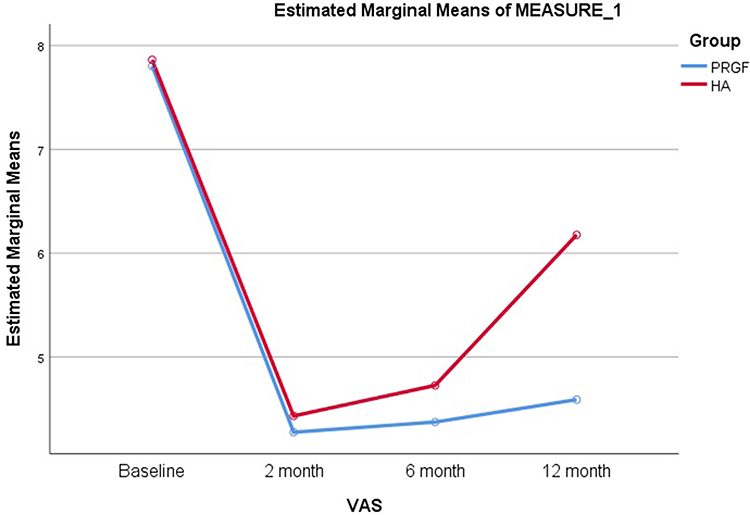 |
Figure 4 Means of VAS at baseline, and at the 2nd, 6th, and 12th months after injection. Abbreviations: PRGF, plasma rich in growth factor; VAS, visual analog scale; HA, hyaluronic acid. |
The success rates of both interventions were defined as any reduction of approximately 30% or higher from baseline scores, when assessed for the third time by passing 12 months from the intervention. According to this definition, success rates for each scale were as follows (PRGF vs Hyalgan): WOMAC total 72.5% vs 22.4% (P < 0.001), WOMAC pain 68.6% vs 74.5% (P =.661), WOMAC stiffness 74.5% vs 19.6% (P < 0.001), and WOMAC function 74.5% vs 19.6% (P < 0.001). By considering P values, there were significantly higher success rates in total, stiffness, and function scores of WOMAC in the PRGF group. In this regard, Table 2 shows WOMAC subscale scores before, and after the 2nd, 6th, and 12th months of intervention in both groups.
Based on the Lequesne scale scores, the rates of success regarding various subscales (PRGF vs HA) were as follows: 21.6% vs 7.8% for total (P =.091), 45.1% vs 19.6% for pain (P =.011), 92.2% vs 96.1% (P =.408) for walk, and 21.6% vs 3.9% for the activities of daily life (P =.015). At the end of the follow-up, the mean satisfaction scores within a range of 0 to 5 were 2.43 ± 1.25 and 1.33 ± 1.07 in PRGF and Hyalgan group, respectively (P <.001). In PRGF study groups, 54.9% and in the HA group, and 15.7% of the subjects had a good or very good satisfaction regarding the procedure they had undergone. The rate of satisfaction is presented in Table 4.
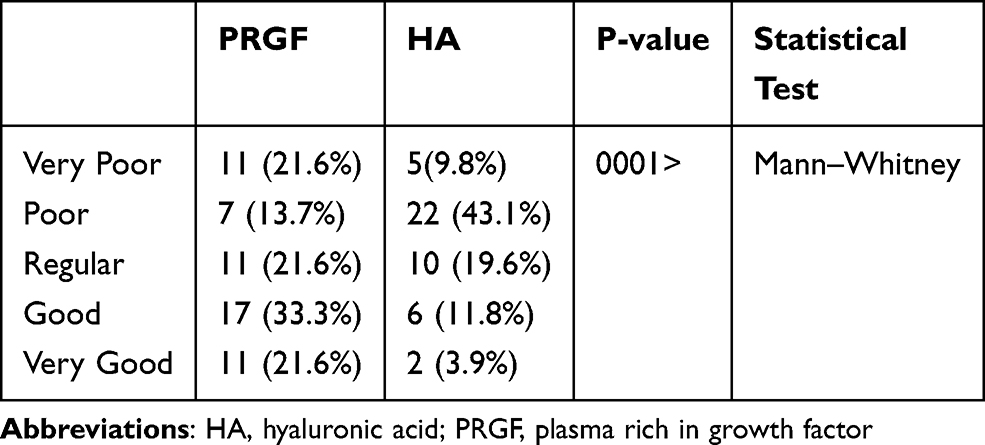 |
Table 4 Rate of the Patient’s Satisfaction 12 Months Post-Injection |
Minor complications because of injection occurred in 10 (19.6%) and 3 (5.9%) subjects in PRGF and Hyalgan groups, respectively (P =.076). In this regard, swelling (one in PRGF vs none in Hyalgan) or stiffness and heaviness of injection site (other cases) were the mentioned ones.
Discussion
This was a single-blinded randomized controlled study comparing intra-articular injections of a newly developed PRGF compared to HA. Also, the results of this study show that, in the HA group, WOMAC, Lequesne and VAS scores significantly reduced after two months but then increased in 6 and 12 months post-injection; however, they were significantly lower in comparison to baseline scores. In PRGF groups, WOMAC and Lequesne scores significant reduction continued up to the sixth month and then increased up to 12th month after injection that were significantly lower in comparison to baseline scores. Beside significantly higher satisfaction in the PRGF group, there were statistically significant improvements after 12 months’ post-injection in VAS score and global, pain, and ADL score of Lequesne test in PRGF compared to HA.
Previous studies performed in vitro and in vivo have also found that, PRP and its consisting growth factors including HGF, IGF-1, and PDGF, have a suppressive effect on the activation of macrophages, fibroblasts, and chondrocytes by inhibiting the NFkB signaling pathway;40–43 thus controlling the catabolic loop. As a result, the inflammatory responses of the synovial and articular cartilage will be blunted when exposed to pro-inflammatory cytokines, abnormal mechanical stress, and DAMPs, which are the characteristics of the OA conditions.4 Also, the considerable concentration of endogenous cannabinoids within PRP 53 might play the role of ligands for cannabinoid receptor 1 (CB1) and 2 (CB2) of chondrocyte and synovium cells of the OA patients 54,55 thereby assisting pain reduction through the endogenous cannabinoid system.53,54
The positive results of HA may be related to the improved impermanent lubrication due to the viscoelasticity and the improvement of the intra-articular environment by repairing the space between the synovial membrane and the articular surface. Moreover, the growth factors secreted from active platelets play an essential role in stimulating proliferation and differentiation of chondrocytes, regulating collagenase secretion, and regeneration of cartilage.
An abundance of clinical studies has also shown that, HA relieves joint pain as well as improving the joint function.58–60
Although several studies have been conducted on comparing the effects of PRP and HA on knee OA, limited clinical trials have been conducted on examining the long term outcomes of PRGF and HA in OA. Moreover, our previous study showed that, our newly developed PRGF, as well as HA, are both effective options on decreasing pain and improvement of function in the patients with symptomatic mild to moderate knee osteoarthritis by passing six months from injection.
This meaningful clinical improvement assessed by both LEQUESNE and WOMAC scores in the patients with knee OA treated with intra-articular injections of PRGF, was observed in this study, which is in line with the previously reported results. The Duymus et al’s study showed that, in the 6th month, while the clinical efficacies of PRP and HA were similar and continued, and at the end of the 12th month, PRP was determined to be both statistically and clinically superior to HA (p < 0.001). In agreement with that, the Dai et al’s study indicated that, compared with HA and saline, intra-articular PRP injection may be more beneficial on pain relief and functional improvement in the patients with symptomatic knee OA at 12 months post-injection.62
In a retrospective cohort study performed by Sánchez et al, success rates by the 5th week for the pain subscale reached 33.4% for the PRGF group and 10% for the hyaluronan group.26 In another study, Vaquerizo et al reported that, PRGF-Endoret is safe and significantly superior to HA in primary and secondary efficacy analysis both at the 24th and 48th weeks that provided a significant clinical improvement, reduced the patients’ pain, and improved joint stiffness and physical function compared to basal levels in the patients with knee OA.38 Wang-Saegusa et al also showed that, six months following intra-articular infiltration of PRGF in patients with OA of the knee, function, and quality of life improvements were acknowledged by OA-specific and general clinical assessment instruments.
The results of all these studies indicate that, PRGF, despite being effective on improving the symptoms of the patients, may not have superior efficacy in comparison with HA over 6 months, while in the longer duration, it can significantly increase the patient’s physical function and satisfaction compared with HA.
Some studies have reported several contrary results to ours. In this regard, Filardo et al reported that, both groups had clinical improvement at follow-up evaluation, but the comparison between these two groups showed no statistically significant difference in all scores evaluated.36,48 In the study by Sanchez et al, the rate of response to PRGF-Endoret was 14.1% higher than that of HA (95% CI, 0.5–27.6; P = 0.044). Regarding the secondary outcome measures, the rate of response to PRGF-Endoret was higher than that of HA in all the cases; however, the difference did not reach statistical significance. In another study by Montañez-Heredia E, both PRP and HA treatments improved pain in knee osteoarthritis patients with no statistically significant differences between them.
Different factors should be considered when comparing the results of studies that have contradicted our study. Variations in results could have resulted from the preparation techniques (frequency/speed/length of centrifugation or the use of ancillary activating/anticoagulant agents). There are some ways of extracting plasma products such as PRP and PRGF. Also, different methods and concentrations exist, which result in different end products even though they have similarities in their names.58 Accordingly, this difference is largely related to the concentration of platelets, leukocytes, and growth factors, all of which are responsible for the effectiveness on converting a joint destructive environment into repairing or regenerating status. Moreover, production of PRGF was used, which employs triple centrifuges to clear the end product of any cell or material except growth factors.
Another factor is the type of administration techniques (volume/frequency/delivery regarding means of administration), as well as post-administration rehabilitation protocols. In a wide variety of studies performed, there has been a variety of injections from one injection to multiple, along with weekly to every 3 or 4 week schedules.59,63 As observed in other studies, no general agreement exists among the researchers regarding a standard frequency of injections. Therefore, according to our previous plasma product experiences 26,33 and while trying to maintain a balance between these 2 groups regarding the costs as well, a two-injection schedule was selected. Follow-up duration is another differentiating factor among these studies. A large number of researchers claimed that, there is no difference between HA and plasma products until two and six months post-injection, while the important difference was observed at the 12 month post-injection. Other factors such as baseline characteristics (age, sex, activity level or OA grade) also affect the results.36,46,64
Limitation
Our study’s first limitation was having no placebo group, which could mean that, there is no clear evidence that PRGF is indeed effective on the degenerative cartilage lesions. Most (75%) of the overall treatment effect on OA RCTs can be due to contextual effects rather than to the specific effect of treatments.65
Failing to blind subjects was another limitation that was due to the extraction of PRGF from patient blood samples and different injection schedules. Also it was possible, but not ethical to take blood from the patients and then to throw away the collected blood in the HA group. It was insisted by the ethics committee that blood should not be collected from the subjects in the HA group. However, the data analyst as well as the physician performing follow-up interviews and visits, were kept blinded to the allocation.
Conclusion
In conclusion, our study demonstrate that, besides a significantly higher satisfaction in the PRGF group, there was a statistically significant improvement after 12 months post-injection in VAS score and global, pain, and ADL score of Lequesne test in PRGF compared to HA.
Data Sharing Statement
Acknowledgments
The abstract of this paper was presented at the EULAR 2019 Annual European Congress of Rheumatology as a poster presentation/conference talk with interim findings. The poster’s abstract was published in ‘Poster Abstracts’ in Annals of Rheumatic Diseases: https://ard.bmj.com/content/78/Suppl_2/499.1
The authors would like to thank their dear colleagues from the Physical Medicine and Rehabilitation Research Center and Clinical Research Developmental Center of Shahid Moddares Hospital, Mehrnaz Mehrabi for her cooperation in data collection. This article has been extracted from the thesis written by Dr. Pegah Yavari in the School of Medicine of Shahid Beheshti University of Medical Sciences.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Wearing SC, Hennig EM, Byrne NM, Steele JR, Hills AP Musculoskeletal disorders associated with obesity: a biomechanical perspective. Obesity Rev. 2006;7(3):239–250. doi: 10.1111/j.1467-789X.2006.00251.x
2. Berenbaum F Osteoarthritis as an inflammatory disease (osteoarthritis is not osteoarthrosis!). Osteoarthritis Cartilage. 2013;21(1):16–21. doi: 10.1016/j.joca.2012.11.012
3. Loeser RF, Goldring SR, Scanzello CR, Goldring MB Osteoarthritis: a disease of the joint as an organ. Arthritis Rheum. 2012;64(6):1697–1707. doi: 10.1002/art.34453
4. Scanzello CR, Goldring SR The role of synovitis in osteoarthritis pathogenesis. Bone. 2012;51(2):249–257. doi: 10.1016/j.bone.2012.02.012
5. Harvey WF, Hunter DJ The role of analgesics and intra-articular injections in disease management. Med Clin North Am. 2009;93(1):201–211, xii. doi: 10.1016/j.mcna.2008.07.010
6. Bourne RB, Chesworth BM, Davis AM, Mahomed NN, Charron KDJ Patient satisfaction after total knee arthroplasty: who is satisfied and who is not? Clin Orthop Relat Res. 2010;468(1):57–63. doi: 10.1007/s11999-009-1119-9
7. Rayegani SM, Raeissadat SA, Heidari S. Safety M-JM and effectiveness of low-level laser therapy in patients with knee osteoarthritis: a systematic review and meta-analysis. J Lasers Med Sci. 2017;8(Suppl 1):S12–S19. doi: 10.15171/jlms.2017.s3
8. Sedighipour L, Raeissadat SA, Rayegani SM, Bossaghzadeh Z, Abdollahzadeh MH, Malayi F AB0973 The efficacy of electromyographic biofeedback on pain, function and maximal thickness of vastus medialis oblique muscle in patients with knee osteoarthritis: a randomised clinical trial. Ann Rheum Dis. 2018;77(Suppl 2):1610. doi: 10.1136/annrheumdis-2017-212762
9. Fransen M, McConnell S Exercise for osteoarthritis of the knee. Cochrane Database Sys Rev. 2008;4:Cd004376.
10. Bjordal JM, Ljunggren AE, Klovning A, Slordal L Non-steroidal anti-inflammatory drugs, including cyclo-oxygenase-2 inhibitors, in osteoarthritic knee pain: meta-analysis of randomised placebo controlled trials. BMJ. 2004;329(7478):1317.
11. Zhang W, Moskowitz RW, Nuki G, et al. OARSI recommendations for the management of hip and knee osteoarthritis, part II: OARSI evidence-based, expert consensus guidelines. Osteoarthritis Cartilage. 2008;16(2):137–162. doi: 10.1016/j.joca.2007.12.013
12. Marx RE Platelet-rich plasma (PRP): what is PRP and what is not PRP? Implant Dent. 2001;10(4):225–228. doi: 10.1097/00008505-200110000-00002
13. Raeissadat SA, Rayegani SM, Hassanabadi H, et al. Knee osteoarthritis injection choices: platelet- rich plasma (PRP) versus hyaluronic acid (A one-year randomized clinical trial). Clin Med Insights Arthritis Musculoskelet Disord. 2015;8:1–8. doi: 10.4137/CMAMD.S17894
14. Raeissadat SA, Rayegani SM, Babaee M, Ghorbani E The effect of platelet-rich plasma on pain, function, and quality of life of patients with knee osteoarthritis. Pain Res Treat. 2013;2013:7. doi: 10.1155/2013/165967
15. Raeissadat SA, Rayegani SM, Tabibian E, Rahimi Dehgolan S Intra-articular ozone injection efficacy in knee osteoarthritis: A systematic review with meta-analysis. Ann Phys Rehabil Med. 2018;61:e132–e133. doi: 10.1016/j.rehab.2018.05.294
16. Rezasoltani Z, Taheri M, Mofrad MK, Mohajerani SA Periarticular dextrose prolotherapy instead of intra-articular injection for pain and functional improvement in knee osteoarthritis. J Pain Res. 2017;10:1179–1187. doi: 10.2147/JPR.S127633
17. Conrozier T, Jerosch J, Beks P, et al. Prospective, multi-centre, randomised evaluation of the safety and efficacy of five dosing regimens of viscosupplementation with hylan G-F 20 in patients with symptomatic tibio-femoral osteoarthritis: a pilot study. Arch Orthop Trauma Surg. 2009;129(3):417–423. doi: 10.1007/s00402-008-0601-2
18. Navarro-Sarabia F, Coronel P, Collantes E, et al. A 40-month multicentre, randomised placebo-controlled study to assess the efficacy and carry-over effect of repeated intra-articular injections of hyaluronic acid in knee osteoarthritis: the AMELIA project. Ann Rheum Dis. 2011;70(11):1957–1962. doi: 10.1136/ard.2011.152017
19. Altman RD, Rosen JE, Bloch DA, Hatoum HT Safety and efficacy of retreatment with a bioengineered hyaluronate for painful osteoarthritis of the knee: results of the open-label extension study of the FLEXX trial. Osteoarthritis Cartilage. 2011;19(10):1169–1175. doi: 10.1016/j.joca.2011.07.001
20. Pal S, Thuppal S, Reddy KJ, et al. Long-term (1-year) safety and efficacy of a single 6-mL injection of hylan G-F 20 in indian patients with symptomatic knee osteoarthritis. Open Rheumatol J. 2014;8:54–68. doi: 10.2174/1874312901408010054
21. Askari A, Gholami T, NaghiZadeh MM, Farjam M, Kouhpayeh SA, Shahabfard Z Hyaluronic acid compared with corticosteroid injections for the treatment of osteoarthritis of the knee: a randomized control trail. Springer Plus. 2016;5:442. doi: 10.1186/s40064-016-2020-0
22. Bruyere O, Cooper C, Pelletier JP, et al. An algorithm recommendation for the management of knee osteoarthritis in Europe and internationally: a report from a task force of the European Society for Clinical and Economic Aspects of Osteoporosis and Osteoarthritis (ESCEO). Semin Arthritis Rheum. 2014;44(3):253–263. doi: 10.1016/j.semarthrit.2014.05.014
23. Hatoum HT, Fierlinger AL, Lin SJ, Altman RD Cost-effectiveness analysis of intra-articular injections of a high molecular weight bioengineered hyaluronic acid for the treatment of osteoarthritis knee pain. J Med Econ. 2014;17(5):326–337. doi: 10.3111/13696998.2014.902843
24. Raeissadat SA, Karimzadeh A, Hashemi M, Bagherzadeh L Safety and efficacy of platelet-rich plasma in treatment of carpal tunnel syndrome; a randomized controlled trial. BMC Musculoskelet Disord. 2018;19(1):49.
25. Kon E, Filardo G, Delcogliano M, et al. Platelet autologous growth factors decrease the osteochondral regeneration capability of a collagen-hydroxyapatite scaffold in a sheep model. BMC Musculoskelet Disord. 2010;11:220. doi: 10.1186/1471-2474-11-220
26. Sanchez M, Fiz N, Azofra J, et al. A randomized clinical trial evaluating plasma rich in growth factors (PRGF-Endoret) versus hyaluronic acid in the short-term treatment of symptomatic knee osteoarthritis. Arthroscopy. 2012;28(8):1070–1078.
27. Kon E, Buda R, Filardo G, et al. Platelet-rich plasma: intra-articular knee injections produced favorable results on degenerative cartilage lesions. Knee Surgery Sports Traumatol Arthroscopy. 2010;18(4):472–479. doi: 10.1007/s00167-009-0940-8
28. Sampson S, Reed M, Silvers H, Meng M, Mandelbaum B Injection of platelet-rich plasma in patients with primary and secondary knee osteoarthritis: a pilot study. Am j Phy Med Rehab. 2010;89(12):961–969. doi: 10.1097/PHM.0b013e3181fc7edf
29. Saad Setta H, Elshahat A, Elsherbiny K, Massoud K, Safe I Platelet-rich plasma versus platelet-poor plasma in the management of chronic diabetic foot ulcers: a comparative study. Int Wound J. 2011;8(3):307–312. doi: 10.1111/j.1742-481X.2011.00797.x
30. Wang-Saegusa A, Cugat R, Ares O, Seijas R, Cusco X, Garcia-Balletbo M Infiltration of plasma rich in growth factors for osteoarthritis of the knee short-term effects on function and quality of life. Arch Orthop Trauma Surg. 2011;131(3):311–317. doi: 10.1007/s00402-010-1167-3
31. Raeissadat SA, Babaee M, Rayegani SM, et al. An overview of platelet products (PRP, PRGF, PRF, etc.) in the Iranian studies. Future Science OA. 2017;3(4):FSO231. doi: 10.4155/fsoa-2017-0045
32. Andia I, Sanchez M, Maffulli N Joint pathology and platelet-rich plasma therapies. Expert Opin Biol Ther. 2012;12(1):7–22. doi: 10.1517/14712598.2012.632765
33. Cole BJ, Seroyer ST, Filardo G, Bajaj S, Fortier LA Platelet-rich plasma: where are we now and where are we going? Sports Health. 2010;2(3):203–210. doi: 10.1177/1941738110366385
34. Kon E, Filardo G, Di Martino A, Marcacci M Platelet-rich plasma (PRP) to treat sports injuries: evidence to support its use. Knee Surgery Sports Traumatol Arthroscopy. 2011;19(4):516–527. doi: 10.1007/s00167-010-1306-y
35. Mascarenhas R, Saltzman BM, Fortier LA, Cole BJ Role of platelet-rich plasma in articular cartilage injury and disease. J Knee Surg. 2015;28(1):3–10. doi: 10.1055/s-0034-1384672
36. Filardo G, Kon E, Pereira Ruiz MT, et al. Platelet-rich plasma intra-articular injections for cartilage degeneration and osteoarthritis: single- versus double-spinning approach. Knee Surgery Sports Traumatol Arthroscopy. 2012;20(10):2082–2091. doi: 10.1007/s00167-011-1837-x
37. Sanchez M, Anitua E, Azofra J, Aguirre JJ, Andia I Intra-articular injection of an autologous preparation rich in growth factors for the treatment of knee OA: a retrospective cohort study. Clin Exp Rheumatol. 2008;26(5):910–913.
38. Vaquerizo V, Plasencia MA, Arribas I, et al. Comparison of intra-articular injections of plasma rich in growth factors (PRGF-Endoret) versus Durolane hyaluronic acid in the treatment of patients with symptomatic osteoarthritis: a randomized controlled trial. Arthroscopy. 2013;29(10):1635–1643. doi: 10.1016/j.arthro.2013.07.264
39. Anitua E, Sanchez M, Nurden AT, et al. Platelet-released growth factors enhance the secretion of hyaluronic acid and induce hepatocyte growth factor production by synovial fibroblasts from arthritic patients. Rheumatology. 2007;46(12):1769–1772. doi: 10.1093/rheumatology/kem234
40. Anitua E, Zalduendo MM, Prado R, Alkhraisat MH, Orive G Morphogen and proinflammatory cytokine release kinetics from PRGF-Endoret fibrin scaffolds: evaluation of the effect of leukocyte inclusion. J Biomed Mater Res A. 2015;103(3):1011–1020. doi: 10.1002/jbm.a.35244
41. Bendinelli P, Matteucci E, Dogliotti G, et al. Molecular basis of anti-inflammatory action of platelet-rich plasma on human chondrocytes: mechanisms of NF-kappaB inhibition via HGF. J Cell Physiol. 2010;225(3):757–766. doi: 10.1002/jcp.22274
42. Coudriet GM, He J, Trucco M, Mars WM, Piganelli JD Hepatocyte growth factor modulates interleukin-6 production in bone marrow derived macrophages: implications for inflammatory mediated diseases. PLoS One. 2010;5(11):e15384. doi: 10.1371/journal.pone.0015384
43. Montaseri A, Busch F, Mobasheri A, et al. IGF-1 and PDGF-bb suppress IL-1β-induced cartilage degradation through down-regulation of NF-κB signaling: involvement of Src/PI-3K/AKT pathway. PLoS One. 2011;6(12):e28663. doi: 10.1371/journal.pone.0028663
44. Sakata R, McNary SM, Miyatake K, et al. Stimulation of the superficial zone protein and lubrication in the articular cartilage by human platelet-rich plasma. Am J Sports Med. 2015;43(6):1467–1473. doi: 10.1177/0363546515575023
45. Wu CC, Chen WH, Zao B, et al. Regenerative potentials of platelet-rich plasma enhanced by collagen in retrieving pro-inflammatory cytokine-inhibited chondrogenesis. Biomaterials. 2011;32(25):5847–5854. doi: 10.1016/j.biomaterials.2011.05.002
46. Montanez-Heredia E, Irizar S, Huertas PJ, et al. Intra-articular injections of platelet-rich plasma versus hyaluronic acid in the treatment of osteoarthritic knee pain: a randomized clinical trial in the context of the spanish national health care system. Int J Mol Sci. 2016;17(7). doi: 10.3390/ijms17071064
47. Patel S, Dhillon MS, Aggarwal S, Marwaha N, Jain A Treatment with platelet-rich plasma is more effective than placebo for knee osteoarthritis: a prospective, double-blind, randomized trial. Am J Sports Med. 2013;41(2):356–364. doi: 10.1177/0363546512471299
48. Filardo G, Di Matteo B, Di Martino A, et al. Platelet-rich plasma intra-articular knee injections show no superiority versus viscosupplementation: a randomized controlled trial. Am J Sports Med. 2015;43(7):1575–1582. doi: 10.1177/0363546515582027
49. Anitua E, Sanchez M, Aguirre JJ, Prado R, Padilla S, Orive G Efficacy and safety of plasma rich in growth factors intra-articular infiltrations in the treatment of knee osteoarthritis. Arthroscopy. 2014;30(8):1006–1017.
50. Raeissadat SA, Rayegani SM, Ahangar AG, Abadi PH, Mojgani P, Ahangar OG Efficacy of intra-articular injection of a newly developed Plasma Rich in Growth Factor (PRGF) versus hyaluronic acid on pain and function of patients with knee osteoarthritis: a single-blinded randomized clinical trial. Clin Med Insights Arthritis Musculoskelet Disord. 2017;10:1179544117733452. doi: 10.1177/1179544117733452
51. Bellamy N, Buchanan WW, Goldsmith CH, Campbell J, Stitt LW Validation study of WOMAC: a health status instrument for measuring clinically important patient relevant outcomes to antirheumatic drug therapy in patients with osteoarthritis of the hip or knee. J Rheumatol. 1988;15(12):1833–1840.
52. Lequesne MG, Mery C, Samson M, Gerard P Indexes of severity for osteoarthritis of the hip and knee. Validation–value in comparison with other assessment tests. Scand J Rheumatol Suppl. 1987;65:85–89. doi: 10.3109/03009748709102182
53. Descalzi F, Ulivi V, Cancedda R, et al. Platelet-rich plasma exerts antinociceptive activity by a peripheral endocannabinoid-related mechanism. Tissue Eng Part A. 2013; 19 (19–20): 2120–2129. doi: 10.1089/ten.tea.2012.0557
54. Dray A, Read SJ Arthritis and pain. Future targets to control osteoarthritis pain. Arthritis Res Ther. 2007;9(3):212. doi: 10.1186/ar2178
55. Richardson D, Pearson RG, Kurian N, et al. Characterisation of the cannabinoid receptor system in synovial tissue and fluid in patients with osteoarthritis and rheumatoid arthritis. Arthritis Res Ther. 2008;10(2):R43.
56. Namiki O, Toyoshima H, Morisaki N Therapeutic effect of intra-articular injection of high molecular weight hyaluronic acid on osteoarthritis of the knee. Int J Clin Pharmacol Ther Toxicol. 1982;20(11):501–507.
57. Leitner GC, Gruber R, Neumuller J, et al. Platelet content and growth factor release in platelet-rich plasma: a comparison of four different systems. Vox Sang. 2006;91(2):135–139. doi: 10.1111/j.1423-0410.2006.00815.x
58. Hunter DJ, Lo GH The management of osteoarthritis: an overview and call to appropriate conservative treatment. Med Clin North Am. 2009;93(1):127–143, xi. doi: 10.1016/j.mcna.2008.07.009
59. Campbell J, Bellamy N, Gee T Differences between systematic reviews/meta-analyses of hyaluronic acid/hyaluronan/hylan in osteoarthritis of the knee. Osteoarthritis Cartilage. 2007;15(12):1424–1436. doi: 10.1016/j.joca.2007.01.022
60. Miller LE, Block JE US-approved intra-articular hyaluronic acid injections are safe and effective in patients with knee osteoarthritis: systematic review and meta-analysis of randomized, saline-controlled trials. Clin Med Insights Arthritis Musculoskelet Disord. 2013;6:57–63. doi: 10.4137/CMAMD.S12743
61. Duymus TM, Mutlu S, Dernek B, Komur B, Aydogmus S, Kesiktas FN Choice of intra-articular injection in treatment of knee osteoarthritis: platelet-rich plasma, hyaluronic acid or ozone options. Knee Surgery Sports Traumatol arthroscopy. 2017;25(2):485–492. doi: 10.1007/s00167-016-4110-5
62. Dai WL, Zhou AG, Zhang H, Zhang J Efficacy of platelet-rich plasma in the treatment of knee osteoarthritis: a meta-analysis of randomized controlled trials. Arthroscopy. 2017;33(3):659–670.e651.
63. Say F, Gurler D, Yener K, Bulbul M, Malkoc M Platelet-rich plasma injection is more effective than hyaluronic acid in the treatment of knee osteoarthritis. Acta Chir Orthop Traumatol Cech. 2013;80(4):278–283.
64. Cerza F, Carni S, Carcangiu A, et al. Comparison between hyaluronic acid and platelet-rich plasma, intra-articular infiltration in the treatment of gonarthrosis. Am J Sports Med. 2012;40(12):2822–2827. doi: 10.1177/0363546512461902
65. Zou K, Wong J, Abdullah N, et al. Examination of overall treatment effect and the proportion attributable to contextual effect in osteoarthritis: meta-analysis of randomised controlled trials. Ann Rheum Dis. 2016;75(11):1964–1970. doi: 10.1136/annrheumdis-2015-208387
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.